Embed Size (px)
Citation preview

Focus onProstate Cancer
(Relates to Chapter 55, “Nursing Management:
Male Reproductive Problems,” in the textbook)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Significance
Malignant tumor of the prostate
Estimated 192,280 new cases diagnosed and 27,360 deaths annually
1 in every 5 men will develop it in their lifetime.
2Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Etiology and Pathophysiology
Androgen-dependent adenocarcinoma
Majority of tumors occur in outer aspect of the gland.
Usually slow growing
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 3

Etiology and Pathophysiology
Spreads by three routesDirect extensionThrough lymph systemThrough bloodstream
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 4

Etiology and Pathophysiology
Direct extension involves seminal vesicles, urethral mucosa, bladder wall, and external sphincter.
Cancer later spreads through lymphatic system to the regional lymph nodes.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 5

Etiology and Pathophysiology
Veins from the prostate seem to be mode of spread toPelvic bonesHead of femurLower lumbar spineLiverLungs
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 6

Etiology and Pathophysiology
Age, ethnicity, and family history are nonmodifiable risk factors.
Incidence rises markedly after age 50.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 7

Etiology and Pathophysiology
African Americans have highest incidence.
Having a first-degree relative with prostate cancer increases risk.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 8

Etiology and Pathophysiology
High-fat diet is associated with increased risk.
Exposure to certain chemicals may be associated with higher risk.
History of BPH is NOT a risk factor.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 9

Clinical Manifestations
Usually asymptomatic in early stages
Eventually may experience symptoms similar to BPHDysuriaHesitancyDribblingFrequency
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 10

Clinical Manifestations
Symptoms similar to BPHUrgency HematuriaNocturiaRetention Interruption of urinary
streamInability to urinate
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 11

Clinical ManifestationsPain in lumbosacral area that
radiates to hips or legs, when coupled with urinary symptoms, could indicate metastasis.
Once cancer has spread to distant sites, pain management becomes major problem.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 12

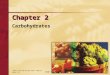
Metastasis of Prostate Cancer to the Pelvis and Lumbar Spine
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 13
Fig. 55-4. Metastasis of prostate cancer to the pelvis and lumbar spine.

Diagnostic Studies
Two primary screening toolsPSA (prostate-specific antigen)
blood test•Elevated levels indicate prostatic pathology—not necessarily cancer.•Marker of tumor volume when cancer exists•Also used to monitor success of treatment
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 14

Diagnostic Studies
Two primary screening toolsDRE (digital rectal
examination)•Abnormal prostate findings include hardness, nodular and asymmetric.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 15

Diagnostic Studies
Elevated levels of PAP (prostatic acid phosphatase) also indicate prostate cancer.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 16

Diagnostic Studies
Neither a PSA nor DRE is a definitive diagnostic test.
Biopsy of prostate tissue is necessary to confirm diagnosis.Done using TRUS to allow
physician to visualize and pinpoint abnormalities
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 17

Diagnostic Studies
Bone scan, CT, MRI with endorectal probe, and TRUS are used to determine location and spread.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 18

Collaborative Care
Whitmore-Jewett and tumor, node, metastasis (TNM) system used to stage prostate cancerBased on size (volume) and
spread
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 19

Collaborative Care
Grading of tumor is done using Gleason scale.Tumors are graded from 1
(well differentiated) to 5 (undifferentiated).
Grades are given to the two most common patterns of cells and are added together.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 20

Collaborative Care
Conservative therapyWatchful waiting when•Life expectancy is less than 10 years•Presence of low-grade, low-stage tumor
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 21

Collaborative Care
Surgical therapyRadical prostatectomy•Entire gland, seminal vesicles, and part of bladder neck are moved.•Retroperineal lymph node dissection usually is done.•Considered most effective for long-term survival
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 22

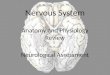
Prostatectomy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 23
Fig. 55-5. Common approaches used to perform a prostatectomy. A, Retropubic approach involves a midlineabdominal incision. B, Perineal approach involves an incision between the scrotum and anus.

Collaborative Care
Radical prostatectomy •Patient catheterized for a couple of days•Stay in hospital for 1 to 3 days•Major complications are erectile dysfunction and incontinence.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 24

Collaborative Care
Other complications of radical prostatectomyHemorrhageUrinary retentionInfectionWound dehiscenceDVTPulmonary emboli
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 25

Collaborative Care
Nerve-sparing surgical procedureSpares nerves responsible
for erectionOnly for cancer confined to
prostateNo guarantee that potency
will be maintained
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 26

Collaborative Care
CryosurgerySurgical technique that
destroys cancer cells by freezing the tissue
Initial and second-line treatment after radiation fails
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 27

Collaborative Care
CryosurgeryComplications include damage
to urethra, urethrorectal fistula, and urethrocutaneous fistula.
Tissue sloughing, ED, urinary incontinence, prostatitis, and hemorrhage have also been reported.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 28

Collaborative Care
Radiation therapyExternal beam radiation•Most widely used method of radiation for prostate cancer•Used to treat cancer confined to prostate and/or surrounding tissue•Side effects can be acute or delayed.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 29

Collaborative Care
Radiation therapyBrachytherapy •Implantation of radioactive seed into prostate gland•Spares surrounding tissue•Placement guided by transrectal ultrasound
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 30

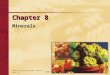
Brachytherapy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 31
Fig. 55-6. A, Prostate brachytherapy. Implantation of seeds with a needle guided by ultrasound and atemplate grid. B, Radioactive seeds.

Collaborative Care
Brachytherapy (cont’d)•Best suited for stage A or B•Irritative or obstructive urinary problems are common side effects.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 32

Collaborative Care
Drug therapyHormonal therapy•Androgen deprivation is primary therapeutic approach.•Focused on reducing levels of androgens to reduce tumor growth•Can be used before surgery or radiation to reduce tumor size and in advanced disease
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 33

Collaborative Care
Hormone therapy“Hormone refractory”•Tumors become resistant to therapy within a few years.•Elevated PSA level is often first sign that therapy is no longer effective.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 34

Collaborative Care
Types of hormonal therapyLuteinizing hormone–
releasing hormone agonists Androgen receptor blockersEstrogen
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 35

Collaborative CareLuteinizing hormone–releasing
hormone agonists With continued administration, LH
and testosterone levels decrease.Produces a chemical castration
similar to orchiectomySide effects include hot flashes,
gynecomastia, loss of libido, and ED.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 36

Collaborative Care
Androgen receptor blockersCompete with circulating
androgens at receptor sitesCan be combined with LH-RH
agonistsSide effects include loss of
libido, ED, hot flashes, breast pain, and gynecomastia.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 37

Collaborative Care
EstrogenUsed as a form of androgen
deprivation therapyDeclining because of
cardiovascular complications (MI, DVT, cerebrovascular disease) and new therapies
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 38

Collaborative Care
OrchiectomySurgical removal of testes
for advanced stages of prostate cancer
May be done alone or with prostatectomy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 39

Collaborative Care
OrchiectomyReduces circulating
testosterone by 90%Side effects include hot
flashes, ED, loss of libido, irritability, weight gain, loss of muscle mass, and osteoporosis.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 40

Collaborative Care
ChemotherapyPrimarily limited to
treatment for those with hormone-resistant prostate cancer (HRPC) in late stages
Goal is palliation, as prostate cancer has responded poorly to chemotherapy.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 41

Nursing AssessmentHealth history
Medications, especially testosterone supplements, morphine, anticholinergics, monoamine oxidase inhibitors and tricyclic antidepressants
Family historyHigh-fat diet, anorexia, weight
loss
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 42

Nursing Assessment
Health historyUrinary urgency, frequency,
retention with dribbling, hematuria, nocturia
Dysuria, low back pain radiating to legs or pelvis, bone pain
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 43

Nursing AssessmentObjective data
Anxiety Distended bladder on palpation;
unilaterally hard, enlarged fixed prostate on rectal examination
High PSA, PAP nodular irregularities on ultrasonography, positive biopsy results, anemia
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 44

Nursing Diagnoses
Decisional conflictAcute pain Urinary retentionImpaired urinary
elimination
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 45

Nursing Diagnoses
ConstipationDiarrheaSexual dysfunctionAnxiety
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 46

Planning
Will be active participant in therapeutic plan
Will have satisfactory pain control
Will follow therapeutic plan on sexual dysfunction
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 47

Planning
Understand the effect of treatment on sexual function.
Find a satisfactory way to manage impact on bladder or bowel function.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 48

Nursing Implementation
Encourage DRE and PSA screenings.
Provide sensitive, caring support to patient and family.
Encourage joining a support group and seeking information.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 49

Nursing Implementation
Teach catheter care.Teach pelvic floor
exercises.Administer pain
medication.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 50

Evaluation
Actively participate in treatment plan
Have satisfactory pain control
Follow therapeutic plan
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 51

Evaluation
Accept effect of treatment on sexual function
Find satisfactory way to manage impact on bladder or bowel function
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 52

After radical perineal prostatectomy for advanced cancer of the prostate, the priority nursing diagnosis for the patient is:
1. Risk for infection.2. Risk for situational low self-esteem.3. Sexual dysfunction.4. Total urinary incontinence.
Audience Response Question
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 53

Case Study
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.54

Case Study
70-year-old man presents to clinic with urinary urgency, difficulty initiating stream, and urinary retention.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 55

Case Study
Symptoms began 6 months ago.
His last PSA with digital rectal examination was 10 years ago.Results were normal.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 56

Case Study
Current digital rectal examination finds the prostate hard and nodular.
His current PSA is 12 ng/mL.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 57

Case Study
A biopsy is performed and indicates cancer.
He decides to undergo radical prostatectomy.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 58

Discussion Questions
1. What should you tell him about the surgical procedure?
2. What side effects of the treatment should he be aware of?
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 59

Discussion Questions
3. You notice that he is embarrassed to discuss sexual dysfunction. What approach should you take?
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 60