Embed Size (px)
Citation preview

DOI: 10.1542/pir.33-5-2262012;33;226Pediatrics in Review
Kamakshya P. Patra and Donald W. LewisFocus on Diagnosis : Electroencephalography: A Primer
http://pedsinreview.aappublications.org/content/33/5/226located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pedsinreview.aappublications.org/content/suppl/2012/05/15/33.5.226.DC1.htmlData Supplement (unedited) at:
Pediatrics. All rights reserved. Print ISSN: 0191-9601. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
by Rachel Boykan on October 8, 2012http://pedsinreview.aappublications.org/Downloaded from

Author Disclosure
Drs Patra and Lewis have disclosed no
financial relationships relevant to this
article. This commentary does not
contain a discussion of an
unapproved/investigative use of
a commercial product/device.
Electroencephalography: A PrimerKamakshya P. Patra, MD,* Donald W. Lewis, MD†
IntroductionElectroencephalography is the record-ing of electrical activity along the scalpproduced by the firing of neuronswithin the brain. The first recordingswere made by Hans Berger in 1929.
PhysiologyEEG activity is due to charge move-ment across neuronal membranes.This activity reflects the summationof excitatory and inhibitory postsyn-aptic potentials in apical dendrites ofpyramidal neurons of the cortex.
UsesEEG tracings can serve manyfunctions:
1. To differentiate epileptic seizuresfrom pseudoseizures, syncope, be-havioral disorders, movement dis-orders, and migraine variants;
2. To distinguish organic or meta-bolic encephalopathy from primarypsychiatric syndromes;
3. To define seizure semiology, prog-nostication, and characterizationfor treatment;
4. To localize the epileptic focus forpossible respective surgery;
5. To monitor status epilepticus (es-pecially nonconvulsive) in ICUs;
6. To determine whether to weanantiepileptic drugs;
7. To make the diagnosis of braindeath; and
8. To investigate parasomnias (sleepdisorders).
Twenty-one electrodes are usuallyplaced on specific positions on thescalp to measure voltage fluctuationsover time. The manner in which pairsof electrodes are connected to eachamplifier of the EEGmachine is calleda montage. Primary generalized epi-lepsy is suggested by spike-and-wavedischarges that are spread widely overboth hemispheres of the brain. Spikesand sharp waves in a local area of thebrain, such as the left temporal lobe,indicate that partial seizures are begin-ning in that area.
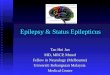
Case Vignette 1A 6-year-old girl is brought to you byher mother, because her teacher hasobservedmultiple daily staring episodesin which the child is unresponsive toverbal and tactile cues. These episodeslastw10 to 15 seconds and occurw10to 20 times a day. Immediately afterthe episode, she resumes normal activ-ity with no recollection of the event.The teacher has also noted facialtwitching and fluttering of the eyelidswith some of these episodes. Therehas been a recent decline in schoolperformance, and the diagnosis of at-tention deficit hyperactivity disorder issuggested. Results of physical exami-nation are normal. EEG demonstrates3 per second generalized spike-and-wave activity (Fig 1). This activity isprovoked by hyperventilation.
The diagnosis in this case is ab-sence seizures.
Absence seizures have an age ofonset of w5 to 6 years and are char-acterized by brief lapses in conscious-ness that occur multiple times perday. No aura or postictal state occurswith these seizures, and the spells canbe provoked by hyperventilation orphotic stimulation. EEG is diagnostic
*Children’s Hospital of Shreveport, Louisiana State
University Health Sciences Center, Shreveport, LA;
currently affiliated with the Department of Pediatrics,
Mayo Clinic, Rochester, MN.†Division of Pediatric Neurology, Children’s Hospital
of the King’s Daughters, Norfolk, VA.
focus on diagnosis
226 Pediatrics in Review Vol.33 No.5 May 2012
by Rachel Boykan on October 8, 2012http://pedsinreview.aappublications.org/Downloaded from

and is characterized by frequent 3 persecond generalized spike-and-waveactivity. The condition is treated withethosuximide, valproate, or lamotri-gine and typically is outgrown bythe early teenage years.
Absence seizures may be mistakenfor complex partial seizures. In the lat-ter, spells usually last longer than 30 sec-onds, have a more gradual onset andtermination, occur only once or twicedaily, and commonly are associatedwith an aura or automatism or postic-tal confusion. EEG demonstrates focalepileptiform discharges, commonly inthe temporal lobe. EEG changes arenot precipitated by hyperventilation.
Case Vignette 2A 15-year-old girl presents to the clinicwith concerns of morning twitches.
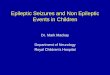
These jerky spells occur within a fewminutes of awakening. She becomesvery tremulous, her arm jolts, and thenshe drops her toothbrush and comb.She remains conscious during these ep-isodes. On the day of presentation, shehas had a generalized tonic-clonic sei-zure. There is history of idiopathic pri-marily generalized epilepsy in hermother. The adolescent onset ofmorn-ing myoclonus coupled with general-ized convulsive seizures and an EEGstudy that demonstrates 4 to 5 cyclesper second generalized polyspike andwave pattern (Fig 2) is consistent withjuvenile myoclonic epilepsy (JME). Pa-tients with JME also may have absenceseizures in addition to their morningmyoclonic seizures and generalizedconvulsions, some of which may beprecipitated by photic stimulation.
JME is an inherited generalizedepilepsy that is typically lifelong, asopposed to absence seizures, whichare “outgrown” during adolescence.Several different genetic linkages havebeen discovered, many on chromo-some 6. Patients with JME need tobe particularly careful about avoidingsleep deprivation and alcohol. In gen-eral, treatment of JME is a broad spec-trum antiepileptic drug (AED), such asvalproate, levetiracetam, topiramate, orlamotrigine. Myoclonic seizures areprecipitated with photic stimulation.
Case Vignette 3A 6-month-old African Americanboy presents with a history of clustersof head nods and sudden forwardflexion of the upper torso, along withflaring of arms outward, then inward.
Figure 1. Three-hertz spike-and-wave discharges, the hallmark of absence epilepsy.
focus on diagnosis
Pediatrics in Review Vol.33 No.5 May 2012 227
by Rachel Boykan on October 8, 2012http://pedsinreview.aappublications.org/Downloaded from

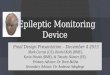
These clusters occur >20 times perday. Skin examination reveals ash leafmacules. Infantile spasms are suspected.The patient is placed on continuousEEG monitoring, which demonstratesmodified hypsarrhythmia with low-amplitude and less fast activity (Fig 3).MRI of the brain reveals the presenceof tubers suggestive of tuberous sclero-sis. Tuberous sclerosis complex presentsoften as infantile spasms. Treatmentchoices include corticotropin, corti-costeroids, and vigabatrin or otherbroad-spectrum AEDs.
Case Vignette 4A 7-year-old girl experiences threeepisodes of seizures within a span of1 month characterized by paresthesiasof themouth followed by clonic move-ments of the mouth, face, and right
arm. The seizures last forw30 secondsto 1 minute without loss of conscious-ness. There is no family history of fe-brile seizures, epilepsy, or any otherneurologic illness. The results of herneurologic examination are normal.An EEG shows bilateral centrotempo-ral spikes (Fig 4). A gentle tapping onthe volar aspect of her thumbwith a ten-don hammer produces spikes above thecontralateral centrotemporal regions.
Benign rolandic epilepsy, or be-nign childhood epilepsy with centro-temporal spikes, is a common partialepilepsy that causes oropharyngeal,motor, and somatosensory symptomsconfined to the face and ipsilateral ex-tremity. The condition begins at anaverage age of 7 to 9 years (range,2–14) and occurs mostly during sleepat night. Neurologic examination
results are normal, and intelligenceis unaffected. The EEG pattern is di-agnostic and demonstrates bilateralspikes in the centrotemporal or ro-landic area with normal backgroundactivity. Neuroimaging results arenormal. Anticonvulsants usually arenot indicated because the seizuresare infrequent and resolve spontane-ously by w15 years of age. Carbama-zepine may be prescribed if seizuresare frequent.
Case Vignette 5A 13-month-old boy is referred for re-fractory seizures. He is having inter-mittent episodes of extension of hisneck associated with rolling of his eye-balls. These episodes occur w5 to 10times a day and are not associated withloss of consciousness or postural tone.
Figure 2. Four- to 6-Hz poly spike-and-wave activity is seen with generalized myoclonic seizures.
focus on diagnosis
228 Pediatrics in Review Vol.33 No.5 May 2012
by Rachel Boykan on October 8, 2012http://pedsinreview.aappublications.org/Downloaded from

There is no postictal confusion. Theseepisodes are more frequent afterfeeding. There is a family history ofseizures. The boy’s birth and develop-ment have been normal. Neurologicassessment is within normal limits.The results of a previous EEG werenormal, and the boy has been treatedwith valproate and levetiracetam withno effect. He is admitted for a videoEEG. Videotaping of these episodesshows recurrent episodes of dystonicmovements of the neck. Sandifer syn-drome is suspected and confirmed byesophageal pHprobe studies.His symp-toms resolve completely with antirefluxtherapy.
Sandifer syndrome is characterizedby spasmodic torticollis and dystoniaassociated with gastroesophageal reflux
or hiatal hernia. The episodes may beconfused with infantile spasms. A tem-poral relationship with feeding and aneurologic examination with normalresults may help in arriving at the di-agnosis. Treatment is antireflux ther-apy or correction of the hiatal hernia.
Case Vignette 6An 8-year-old white girl has presentedwith intractable seizures since infancy.She was born at term, and global de-velopmental delay was noted early inchildhood. She experienced a multi-plicity of seizure types, including atyp-ical absence, generalized tonic clonic,myoclonic, and drop attacks. Multipleantiepileptic drugs, including val-proate, clonazepam, clobazam, gaba-pentin, and levetiracetam, were used,
but to no avail. Interictal EEG revealsgeneralized slow spike-and-wave ab-normality. The diagnosis is Lennox-Gestaut syndrome.
Lennox-Gestaut syndrome is char-acterized by a triad of intractable seiz-ures of multiple types, interictal EEGabnormalities, and mental retardation.The condition usually begins at 2 to 4years of age and may be preceded byinfantile spasms. Seizures are resis-tant to therapy. Valproate, clonazepam,vigabatrin, lamotrigine, felbamate, andtopiramate have been used. A keto-genic diet should be considered in pa-tients refractory to AEDs.
Case Vignette 7A 10-day-old girl born at termpresents with multiple episodes of
Figure 3. Repetitive spike focus localized in the centrotemporal or rolandic area with a normal background activity, typical ofbenign rolandic epilepsy.
focus on diagnosis
Pediatrics in Review Vol.33 No.5 May 2012 229
by Rachel Boykan on October 8, 2012http://pedsinreview.aappublications.org/Downloaded from

abnormal jerks affecting all fourlimbs. In between the episodes,she is active and feeding well. Thereis no history of fever. The pregnancyand delivery were uneventful. Theinfant is breastfed exclusively. Thephysical examination is within nor-mal limits. Blood levels of glucose,electrolytes, calcium, and magnesiumare normal. The results of a septicevaluation are negative. Computedtomography scan of the brain andEEG have normal results. A tentativediagnosis of benign sleep myoclonusis made. The myoclonic jerks occurduring sleep only and disappearwhen the infant is awake. This find-ing is corroborated by the nurse. Pa-rents are reassured, and the infantdischarged from the hospital. The
myoclonus disappears by 3 monthsof age. Follow-up at 1 year of agereveals normal neurologic findingsand development.
Benign neonatal sleep myoclo-nus is a nonepileptic, self-limitedparasomnia that begins typicallyduring the neonatal period. It oc-curs during sleep and stops whenthe baby is awake. The myoclonusmay be induced by repetitive soundstimuli or rocking the baby. Theseepisodes may be confused with in-fantile spasms but can be distin-guished from the latter by theabsence of EEG findings. The prog-nosis is good, with no sequelae andcessation of myoclonus by 2 yearsof age. Antiepileptic therapy is notindicated.
Case Vignette 8A 16-year-old girl is referred for re-fractory seizures. She was admittedfor video EEG monitoring. Resultsof her neurologic examination arenormal. One of the episodes capturedduring video EEG reveals a gradualonset of facial grimacing followedby forward pelvic thrusting. She ap-pears unresponsive. No urinary in-continence, frothing from mouth,cyanosis, or tongue bite is noted. Herpupils remain normal, and she hasnormal muscle tone and flexor plantarresponse. She recollects the episodeand had no lethargy or confusion afterthe episode. EEG shows excess mus-cle artifacts with a normal back-ground activity devoid of epilepticdischarges.
Figure 4. Hypsarrhythmia, which consists of a chaotic pattern of high voltage, bilaterally asynchronous, slow wave activity,characteristic of infantile spasms.
focus on diagnosis
230 Pediatrics in Review Vol.33 No.5 May 2012
by Rachel Boykan on October 8, 2012http://pedsinreview.aappublications.org/Downloaded from

Detailed psychological evaluationreveals a deep fear of her mathematicsteacher and possibility of sexual abuse.She experienced two such episodesat school just before mathematicsclass. She is diagnosed with nonepilep-tic seizures (pseudoseizures or psycho-genic seizures) and anticonvulsants arestopped.
Pseudoseizures are more frequentin adolescent girls. A more gradualonset; bizarre and variable patternof episodes; verbalizations; lack of cy-anosis; normal pupillary light reflex;flexor plantar responses; absence ofsphincter incontinence, tongue bite,or body injury; response to noxiousstimuli; and memory for the episodemay help distinguish a pseudoseizurefrom a true seizure. Often these pa-tients have a past history of epilepsy.Serum prolactin level is unchangedfrom baseline after a pseudoseizure,
unlike in a true seizure in which caseit is increased.
Video EEG has a high yield indistinguishing seizures from nonepi-leptic events, in classifying seizures,and in determining candidacy for ep-ileptic surgery. In one study, videoEEG resulted in an alteration of clin-ical management in 45% of pediatricpatients. (1)
LimitationsThe sensitivity and specificity of EEGin diagnosing epilepsy is w25% to56% and 78% to 98%, respectively.EEG is less sensitive to pick up signalsgenerated from the deeper structures(eg, hippocampus, basal ganglia).Normal EEG results are seen in10% to 20% children with epilepsy.EEG abnormalities may be found in2% to 4% of healthy children with
no known history of seizures. Ap-proximately 50% patients with epi-lepsy have a normal first EEG.
Reference1. Chen LS, Mitchell WG, Horton EJ,Snead OC III. Clinical utility of video-EEG monitoring. Pediatr Neurol. 1995;12(3):220–224
Suggested ReadingEbersole JS, Pedley TA, eds. Current Prac-
tice of Clinical Electroencephalography.3rd ed. Philadelphia, PA: LippincottWilliams and Wilkins;2003
Guerrini R. Epilepsy in children. Lancet.2006;367:499–524
Major P, Thiele EA. Seizures in children:laboratory diagnosis and manage-ment. Pediatr Rev. 2007;28(11):405–414
Smith SJM. EEG in the diagnosis, classifi-cation, and management of patients withepilepsy. J Neurol Neurosurg Psychiatry.2005;76:ii2–ii7
Condolences
The staff of Pediatrics in Review would like to express our sorrow at the death of Dr. Donald
Lewis, co-author of this article, a highly respected colleague, and valuable member of our
Editorial Board.
focus on diagnosis
Pediatrics in Review Vol.33 No.5 May 2012 231
by Rachel Boykan on October 8, 2012http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.33-5-2262012;33;226Pediatrics in Review
Kamakshya P. Patra and Donald W. LewisFocus on Diagnosis : Electroencephalography: A Primer
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/33/5/226including high resolution figures, can be found at:
References
http://pedsinreview.aappublications.org/content/33/5/226#BIBL
This article cites 4 articles, 2 of which you can access for free at:
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by Rachel Boykan on October 8, 2012http://pedsinreview.aappublications.org/Downloaded from