Embed Size (px)
Citation preview

Maarten S. van Leeuwen, MD, PhD #{149}Jos Noordzij, MD #{149}Michiel A. M. Feldberg, MD, PhDAdriaan H. Hennipman, MD, PhD #{149}Heleen Doornewaard, MD
Focal Liver Lesions: Characterizationwith Triphasic Spiral CT’
327
PURPOSE: To assess whether tripha-sic spiral CT enables characterizationof a wide range of focal liver lesions.
MATERIALS AND METHODS: Onehundred five patients with suspectedfocal liver disease underwent tripha-sic liver CT. After injection of con-trast material, the liver was scannedin arterial (scanning delay, 22-27 sec-onds), portal (scanning delay, 49-73seconds), and equilibrium (scanningdelay, 8-10 minutes) phases. Enhance-ment of each lesion in each phasewas evaluated, and the lesions weretabulated according to one of 11 en-hancement patterns.
RESULTS: In 94 patients, 375 liverlesions were detected. The nature ofthe lesion was confirmed in 326 le-sions (87%). Six of 11 enhancementpatterns were always due to benigndisease and caused by areas withhyper- or hypoperfusion, hemangio-mas, cysts, focal nodular hyperplasias,or benign but nonspecified lesions.Two of 11 patterns were always dueto malignant disease, and one patternwas due to malignant disease in 38(97%) of 39 patients with known ma-lignancy elsewhere or with chronicliver disease. The other two patternswere seen in metastases and partlyfibrosed hemangiomas.
CONCLUSION: Triphasic liver CTenables characterization of a widerange of focal liver lesions, includingthe benign liver lesions that occurmost frequently.
S PIRAL computed tomography (CT)has rapidly gained acceptance as
the preferred CT technique for routineliver evaluation because it providesimage acquisition at peak enhance-
ment of the liver parenchyma duringa single breath hold (1-4). In addition,the fast data acquisition allows suc-
cessive scanning of the entire liver at
different moments after injection ofcontrast material, thus creating the
possibility of multiphasic liver CT.
Recent studies have reported an im-provement in lesion detection if arte-nat phase imaging is performed in
addition to portal venous imaging,especially in the presence of hyper-
vascular neoptasms, such as hepato-
cellular carcinoma (HCC) (5-8).In the current study, we evaluated
a triphasic spiral CT technique thatallows imaging of the entire liver
in arterial, portal, and equilibrium
phases. The rationale behind the pro-
tocol was that the portal phase is the
most sensitive phase for lesion detec-
tion, whereas the arterial and equilib-rium phases can supply additionalinformation on the vascutarity of he-
sions that may help to clarify the na-
ture of lesions. The study was de-signed to assess whether triphasic
spiral liver CT enables characteriza-
tion of a wide range of liver lesions,
also in the presence of multilevel dis-
ease and in the coexistence of differ-
ent pathologic conditions.
MATERIALS AND METHODS
Patients
From February 1993 to July 1994, 105nonconsecutive patients (45 men, 60women; age range, 25-84 years; medianage, 55 years) were examined with a tn-
phasic liver CT protocol. Patients wereincluded if focal liver disease was sus-pected clinically or if previous imagingstudies depicted hepatic lesions with anonspecific appearance. Fifty-eight pa-tients were referred with a known pni-many malignancy: colorectal carcinoma(1? = 36), carcinoid (,z = 4), breast carci-noma (n = 3), pancreatic endocrine tu-mors (n = 3), renal carcinoma (ii = 3),melanoma (it = 2), leiomyosarcoma (n =
2), and bronchogenic carcinoma, gastric
carcinoma, germ cell carcinoma, medul-lary thyroid carcinoma, and tongue basecarcinoma (one each). Among these fifty-eight patients, the reason for referral wassuspected metastatic disease or quantifica-tion of known metastatic disease. Thirty-one patients without a known primarymalignancy were referred because ultra-sound (US) or conventional CT demon-strated one or several hepatic lesions thatcould not be characterized. Eight patientswith chronic liver disease were referredbecause of possible HCC. In three patients,a focal liver mass was suspected at physi-cal examination. In three patients, abnor-mal liver function test results were thereason for referral. In one patient, a gall-bladder carcinoma was suspected at US,and in one patient the reason for referralwas unknown.
Index terms: Computed tomography (CT), tissue characterization, 761.91 #{149}Liver, CT, 761.12113,
761.12114, 761.12115 #{149}Liver, cysts, 761.312 #{149}Liver, focal nodular hyperplasia, 761.3198 #{149}Liven
neoplasms, 761.30 #{149}Liver neoplasms, secondary, 761.332
Abbreviations: FNH = focal nodular hyperplasia, HCC = hepatocellulan carcinoma.
Radiology 1996; 201:327-336
I From the Departments of Diagnostic Radiology (M.S.v.L., iN., M.A.M.F.), Surgery (A.H.H.), and
Pathology (H.D.), University Hospital Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The Nether-lands. Received September 28, 1994; revision requested November 18; final revision received April30, 1996; accepted May 14. Address reprint requests to M.S.v.L.
, RSNA, 1996

328 #{149}Radiology November 1996
CT Acquisition
A triphasic liver CT protocol was devel-oped in which we used a spiral CT scanner
with a 5.2 mega heat unit, or MHU, x-raytube, capable of 50 consecutive 1-secondrotations with 225 mAs and 140 kV (modelSR 70()0; Philips Medical Systems, Best,The Netherlands). Images were recon-
structed with a 180#{176}linear interpolationreconstruction algorithm.
With the tniphasic liver CT protocol, theentire liver was scanned successively inarterial, portal, and equilibrium phases.After obtaining a digital scout view, anunenhanced scan of the liver was acquiredwith 10 mm/sec table speed, 10-mm colti-mation, and 10-mm reconstruction index.On the unenhanced scan, the craniocau-dat extent of the liver was measured, and
2 cm was added to this distance to allow
for small differences in inspiration. Tominimize partial volume effects on theportal phase images, 5-mm collimationand 5 mm/sec table speed were used, with
a 2-mm reconstruction index. Because thescanner allowed a maximum of 50 rota-tions before a waiting period, acquisitionin arterial and portal phases together waslimited to these 50 rotations. The cranio-caudal extent of the liver determined thenumber of required rotations in portalphase. The remaining number of rotations(50 minus the number of portal phase ro-tations) were used for the arterial phase,and table speed and collimation were ad-
justed to cover the entire liver. Dependingon the craniocaudat extent of the liver,
5-mm collimation with 10 mm/sec tablespeed and 5-mm reconstruction index or10-mm collimation with 20 mm/sec tablespeed and 10-mm reconstruction indexwere used in the arterial phase.
The patient was asked to hyperventilate
during 30 seconds before arterial scan-fling. A total of 194 mL of nonionic con-trast material (iohexot [Omnipaque; Ny-corned, Princeton, NJ], 350 rng of iodineper milliliter; ioversot [Optiray; Guerbet,Aulnay-sous-Bois, France], 350 mg of io-dine per milliliter; or joprornide [Ultravist;Schering, Berlin, Germany], 300 or 370 mgof iodine per milliliter) was injected with apower injector (model CT 9000 Digital In-jection System; Liebel Flarsheim, Cinci-natti, Ohio) at 4 mL/sec into an antecubi-tat vein by using an 18-gauge needle. After
22 or 27 seconds (22 seconds in patientsyounger than 40 years and 27 seconds inpatients older than 40 years), the entire
liver was scanned in arterial phase.Twenty seconds after the end of the ar-
teniat phase, the liver was scanned in por-
tat phase with 5-mm collimation, 5 mm/sec table speed, and 2-mm reconstructionindex. The 20-second interscan delay be-tween the end of the arterial phase andthe onset of the portal phase acquisitionwas needed to give the patient a chance torebreathe and to reposition the scan plane
cephalad to the liver. As a result, portalphase acquisition started between 0 and24 seconds after the end of injection ofcontrast material.
After reconstruction of arterial phase
images (reconstruction time, 8 seconds persection) and saving of the raw data of por-tal phase sections, a third scan was obtainedin the equilibrium phase, 8-10 minutesafter injection of contrast material, with10-mm collimation, 10 mm/sec tablespeed, and 5-mm reconstruction index.The number of rotations was adjustedto cover the entire abdominal cavity.
Alt scans were obtained in the cranio-caudal direction and during breath hold.Patients were allowed to breathe slowlyduring the latter part of the equilibriumacquisition, when the lower abdomen andpelvis were scanned. Total examinationtime, including reconstruction, filming,and data storage varied between 45 and50 minutes.
Eight (8%) of 105 examinations wereperformed with a different protocol, either
due to a technical fault or to human error
in the implementation of the protocol. Allthese errors occurred in the first 50 pa-tients. Among these eight examinations,no equilibrium phase of the liver was ac-
quired in six examinations, no arterialphase was acquired in one examination,and 10-mm collimation instead of 5-mmwas used for portal phase imaging in oneexamination.
Image Interpretation
Initially, images were reviewed as hardcopies, with every other image printed onfilm. Thus, 10-mm arterial and equilibriumphase sections were presented as contigu-ous images, and 5-mm portal phase sec-tions were presented at 4-mm intervals.During the course of the study, an off-lineworkstation (Easy-vision CT/MR; PhilipsMedical Systems) became available, whichallowed dynamic viewing of all recon-structed images in interactive cine mode.Comparison of the sections at the sameanatomic level in the three different phases
of contrast enhancement was facilitated by
using a proprietary “Compare” functionin the workstation.
Each study was interpreted by two radi-otogists (M.S.v.L., J.N.) in consensus. Mostreadings were performed in a blindedfashion, but in a number of patients theresults of previous imaging studies wereknown because one of the radiologists had
performed the previous study. In alt pa-
tients but one, the reason for referral wasknown. First, the enhancement character-istics of each phase were assessed by grad-ing the attenuation of the arterial and por-tal venous system at the level of the portahepatis in comparison to liver paren-chyma. Second, arterial, portal, and equi-libnum phase images were reviewed for
the presence of focal liver lesions. The ap-pearance of each lesion in each phase was
described on the basis of the attenuationand the homogeneity of the lesion in corn-parison to surrounding parenchyma in
that phase and was expressed as one offive possible states, with an abbreviatedname for each state: (a) area of water at-tenuation, homogeneous: hypo-(cyst),(b) area of soft-tissue attenuation, often
slightly mnhomogeneous: Iiypo-, (c) inho-mogeneous mixture of hypo- and hyperat-tenuation, but less hyperattenuating thanthe arterial system: mixed, (d )area of hyper-attenuation, but less hyperattenuating thanthe arterial system: hyper-, and (e) isoatten-uating compared with the arterial system:arterial. Moreover, the presence of a con-tinuous, hyperattenuating rim, less hyper-attenuating than the arterial system, wasnoted in the arterial phase, hyper-(rim). Afterdescribing the state of each lesion in eachphase, the pattern of enhancement overtime of each lesion was described as a
three-part pattern name that incorporatedthe appearance of the lesion in each phase(eg, hypo-/hypo-/hypo-). Additional fea-tures, defined by typical location, appear-ance, or size of the lesion, were used to
define subtype enhancement patterns.According to the literature (6,9-23) and
previous experience with dynamic liverCT, 11 different enhancement patternswere defined that belonged to one of twogeneral groups, either hypoattenuatingpatterns, which demonstrated less con-trast enhancement than normal paren-chyma during the arterial and portalphases, or hyperattenuating patterns,which demonstrated more contrast en-hancement than normal parenchyma dun-ing the arterial phase (Table 1). Percent-ages were rounded off to the nearestwhole number.
Standard of Reference
After all studies were interpreted, astandard of reference for each detectedlesion was determined. To this purpose,medical history, results of other imagingstudies, biopsy findings, and surgical find-
ings were collected. A total of 375 lesionswere detected in 94 patients. In 326 lesions(87%), a standard of reference concerning
the nature of the lesion was available(Table 2). These 326 lesions were includedfor further analysis. The following infor-mation was accepted as the standard ofreference: (a) Findings at surgery andhistopathologic examination (ii = 74).(b) Findings at percutaneous biopsy (;i =
137). If, in a patient with multiple lesions,biopsy was performed of one lesion, altlesions with the same appearance at CT
as the biopsy lesion were considered torepresent the same pathologic finding.(c) Findings at US (ii = 32). An anechoiclesion with posterior acoustic enhancementwas considered proof of a cyst. (d) Find-ings at magnetic resonance (MR) imaging(n = 31). A sharply demarcated lesion withhomogeneous high signal intensity onheavily T2-weighted images was consid-ered proof for the presence of a cyst or ahemangioma. (e) Findings at follow-up(n = 52). When a patient with a proved
malignancy developed solid lesions in theliver that increased in size over time, thelesions were considered to be metastasesof the primary tumor. Conversely, if a he-sion did not show any change after aminimum of 1-year follow-up, the lesionwas considered to be benign but unchar-acterized as to its pathologic nature.

Table 2Standard of Reference in 326 of the 375 Lesions Detected with Triphasic Liver CT
MRSurgery Biopsy Imaging US Follow-up
Noncolorectal metastases (103 lesions/14 patients) 6/2 87/11 . . . . . . 10/1Colorectal metastases (62 lesions/25 patients) 33/15 18/5 . . . . . . 11/5HCC (18 lesions/5 patients) 2/2 16/3 . . . . . . ...
Non-Hodgkin lymphoma (1 lesion/i patient) . . . i/i . . . . . . ...
Hemangioma (59 lesions/32 patients)Arterial/arterial/arterial (51 lesions/25 patients) 6/5 3/2 18/6 . . . 24/12hypo-/hypo-/hyper (3 lesions/3 patients) 1/1 . . . 2/2 . . . ...
hypo-/hypo-/hypo (5 lesions/5 patients) 1/1 1/1 1/1 . . . 2/2Cyst (51 lesions/i3 patients) 6/3 . . . 10/1 32/7 3/2FNH (7 lesions/6 patients) 3/3 4/3 . . . . . . ...
Adenoma (4 lesions/3 patients) . . . 2/2 . . . . . . 2/1Focal fat deposit (1 lesion/i patient) i/I . . . . . . . . . . .
Benign, but not characterized as to pathologicnature (20 lesions/9 patients) 15/7 5/2 . . . . . . ...
Note.-Data are presented as no. of lesions/no. of patients. FNH = focal nodular hyperplasia.
was visually compared and graded.Arterial phase images were acquired
in 104 patients. The arterial system
was intensely opacified throughout
Table 1
-�-.--� -�� �-.--.-�--�-�-- --fl
Volume 201 #{149}Number 2 Radiology #{149}329
Enhancement Patterns
Attenuation for Arterial!Portal!Equilibnium Phases
.
Arterial Phase Portal Phase Equilibrium Phase
Hypo-/hypo-/hypo-
Hypo-/hypo-(FL)!hypo-�
Hypen-(nim)/hypo-!hypo-
Hypo-! hypo-/hypen-Hypo-/hypo-(cyst)/hypo-
Small hypo-/hypo-(cyst)!hypo-�
Artenial/anterial/artenialllLarge
Small
Hyper�!A/A#
l-Iyper-!A/A (cleft)**
Hypen�(wedge)!iso�/iso�**
Mixed/mixed/mixed
Hypoattenuating Patterns*
Hypo- or isoattenuating
Hypo- or isoattenuating
Hypo- or isoattenuating, hyperat-tenuating rim
Hypo- or isoattenuatingHypo- or isoattenuating
Hypo- or isoattenuating
Hypoattenuating
Hypoattenuating, no mass effect,adjacent to FL
Hypoattenuating
HypoattenuatingHypoattenuating, water attenua-
tion; sharp marginHypoattenuating, near water
attenuation; sharp margin; � 5mm
Hypo- or isoattenuating, possiblehypoattenuating rim
Hypo- or isoattenuating
Hypo- or isoattenuating, possiblehypoattenuating rim
HyperattenuatingHypo- or isoattenuating
Hypo- or isoattenuating
Hyperattenuating I’atterns*
Peripheral nodular enhancement ofarterial attenuation or hypoat-tenuating
Complete enhancement of arterialattenuation or hypoattenuating
Hyperattenuating but less hyperat-tenuating than arterial space
Hyperattenuating but less hyperat-tenuating than arterial space, cen-tral hypoattenuating cleft
Wedge-shaped area of hypenattenu-
ation, less hyperattenuating thanvascular system; no accompa-flying lesion
Partly hypoattenuating, partlyhyperattenuating
Peripheral nodular enhancement ofvascular attenuation, progressivein a centropetal fashion
Complete enhancement of vascularattenuation
1-lyper-, iso-, or hypoattenuating
Hyper-, iso-, or hypoattenuating;central hypoattenuating cleft
Isoattenuating, no lesion
Partly hvpoattenuating, partly
hypenattenuating
Hyperattenuating with possible cen-tnal hypoattenuation on isoattenu-ating (if vascular space is isoat-tenuating)
Complete enhancement of vascularattenuation or isoattenuating
Iso- or hypoattenuating
Iso- or hypoattenuating, centralhypoattenuating cleft
lsoattenuating, no lesion
Partly hypoattenuating. partly
hyperattenuating
Notc.-Hypo-, iso-, and hyperattenuating refer to relative attenuation in comparison to that of the surrounding liver parenchyma.
* Lesions showed less enhancement in the arterial and portal phases than that of liver panenchyma.
7 Subtype of pattern hypo-!hypo-!hypo-. FL = falciform ligament.� Subtype of pattern hypo-!hypo- (cyst)!hypo-.
� S Lesions showed more enhancement in the arterial phase than that of liver parenchyma.[his pattern, with arterial attenuation in all phases, had two appearances depending on the size of the lesions.
� I This pattern was defined by its appearance in arterial phase only, irrespective of the enhancement in the other phases. A -hypo-. ist-. on hyperattenuating.� ** Subtypeof hyper=!A!A.
Abnormality
RESULTS
The relative enhancement of the
arterial and portal venous systems
the entire arterial phase on 98 (94%)
of the 104 scans. In this arterial phase,
the splenic vein demonstrated van-
able enhancement depending on the
splenic circulation time. As a result, 21
patients (20%) demonstrated enhance-
ment of the intrahepatic portal system
slightly less than or equivalent to that
of the arterial space. Parenchymal en-
hancement, however, was always
well below the enhancement seen in
the portal phase. In the other 83 pa-
tients (80%), the intrahepatic portal
system was not, or only slightly, en-hanced. Apparently, the chosen tim-
ing for the arterial scanning delay re-
sulted in a true arterial phase in most
patients.
Portal phase images were acquired
in all 105 patients. Visually, good en-
hancement of liven parenchyma was
present in all patients. In 53 (50%) of
the 105 patients, the enhancement of
the portal system at the level of the
porta hepatis was more intense com-

Table 3
330 #{149}Radiology November 1996
Clinical Importance and Pathologic Correlation of Hypo- and Hyperattenuating Enhancement Patterns
Enhancement Pattern
Malignancy Benignancy
No. of Lesions Pathologic Diagnosis No. of Lesions Pathologic Diagnosis
Hypo-/hypo-/hypo- (n = 89)
Hypoattenuating Patterns (196 Lesions)
84 (94) Colorectal metastases (n = 31) 5 (6) Hemangiomas, partly fibnosed (ti = 5)Noncolorectal metastases (n = 53)
Carcinoid (n = 25)PET(n= 12)Renal carcinoma (n = 10)MTC (n =3)Breast carcinoma (ii = 3)
Hyper-(rim)/hypo-/hypo (n = 29) 29 (100) Colorectal metastases (n = 24) 0 (0) ...
Noncotorectal metastases (n = 4)PET (n = 3)Carcinoid (n = 1)
Lymphoma (n = 1)Hypo-/hypo-/hyper- (ii = 8) 5 (62) Colorectat metastases (n = 5) 3 (38) Hemangiomas (it = 3)Hypo-/hypo-(cyst)/hypo- (n = 51) 0 (0) . . . 51 (100) Cysts (n = 51)Small hypo-/hypo-(cyst)/hypo- (0 = 15) 0 (0) . . . 15 (100) Focal fat (,i = 1)
Benign at follow-up (n = 8)
No abnormality (n = 6)
Hypo-/hypo-(FL)/hypo- (ii = 4)
Arterial/arterial/arterial (n = 51)
0 (0) . . . 4 (100) No abnormality (it = 4)
Hyperattenuating Patterns (130 Lesions)
0 (0) . . . 51 (100) Hemangiomas (n = 51)Hyper-/A/A (n = 45) 38 (84) Noncolorectal metastases (n = 20) 7 (16) Adenomas (n = 4)
Carcinoid (n = 10) FNH (n = 2)MTC (n = 7) Benign at follow-up (n = 1)Renal carcinoma (n = 3)
HCC (n = 18)Hyper-/A/A (cleft) (n = 5)Hyper-(wedge)/iso-/iso- (n = 1)Mixed/mixed/mixed (n = 28)
0 (0)0 (0)
28 (100)
. . . 5 (100) FNH (n = 5)
. . . 1 (100) No abnormality (n = 1)Noncotorectal metastases (n = 26) 0 (0) ...
Carcinoid (n = 15)Breast carcinoma (�i = 10)Leiomyosarcoma (n = 1)
Colorectal metastases (n = 2)
Note-Numbers in parentheses are percentages. MTC - medullary thyroid cardnoma, PET = pancreatic endocrine tumor.
pared with that of the arterial system,and in 53 patients (50%) enhance-ment was equal.
During the equilibrium phase, thevascular spaces and parenchyma couldbe distinguished in 92 (93%) of the
99 patients in whom equilibriumphase scans were obtained; in seven
patients (7%), the vascular structures
were isoattenuating compared withliver parenchyma. To assess the utilityof tnphasic liver CT for charactenza-
tion of liver lesions, data were ana-lyzed in two formats. First, the 11 pat-terns of enhancement were compared
with the standard of reference toquantify the clinical relevance of each
of the 11 patterns. These data and thepathologic counterpart of the 11 en-hancement patterns are presented in
Table 3.
Second, the abnormalities were com-
pared with their patterns of enhance-ment to understand the correlationbetween different pathologic entitiesand their tniphasic liver CT appear-ance. These findings are presentedin Tables 4-7.
DISCUSSION
Because of the high frequency ofbenign focal liver lesions such as cysts,hemangiomas, and FM!-! (24-27), char-
acterization of these lesions is essen-tial. In addition, in many patients who
are referred for liver CT, one does notknow what kind of abnormality will
be present. Consequently, the pre-
ferred liver CT technique should com-
bine a high sensitivity for lesion de-tection with a good ability for lesioncharacterization, to differentiate le-sions that do need further diagnostic
tests or treatment from lesions that
do not. To meet these requirements,a triphasic spiral CT technique wasdeveloped to image the entire liverin arterial, portal, and equilibrium
phases. A monophasic, high-volume
(194 mL), high-injection-rate (4 mL/
sec) contrast material protocol was
used to achieve sufficient arterial opaci-
fication during the arterial phase, in-tense parenchymal opacification in
the portal phase, and hyperattenuat-
ing vascular space in the equilibrium
phase.
Hypoattenuating EnhancementPatterns
The characterization of hypoat-tenuating liver lesions is often diffi-
cult, especially when lesions are small
(ie, < 1.5 cm in diameter). Although
such lesions are seldom malignant if
found in a patient without a knownprimary tumor, the chance of malig-
nancy in patients with a known pri-
mary tumor is reported to be as high
as 34% (27).
The first distinction to be made is
between cysts and hypoattenuatingsolid lesions. All hypo-/hypo-(cyst)/
hypo- lesions (n = 51) were confirmed
to be cysts. Because of their sharper
margin and homogeneous hypoattenu-
ation, 5-10-mm hypo-/hypo-(cyst)/
hypo- lesions (n = 26) could be confi-
dently differentiated from subcentimeter
hypo-/hypo-/hypo- lesions (n = 30),greatly reducing the need for confir-
matory US or follow-up of these small
cysts. The subtype small hypo-/hypo-
(cyst)/hypo- was used for hypo-/hypo-
(cyst)/hypo- lesions less than 5 mm in
diameter. We defined this subtype

Table 4
ObservedEnhancement Patterns of 184 Malignant Lesions
Pathologic Diagnosis No. of Lesions �nhancemcrnt Patterns
Colorectal metastases (n = 62) 31 (50) Hypo-/hypo-/hypo-24 (39)
5 (8)
Hyper-(rim)/hypo-/hypo-
Hypo-/hypo-/hyper-2 (3) Mixed-/mixed-/mixed-
Noncolonectal metastases (n = 103)* 53 (51)
26 (25)20 (19)
4 (4)
Hypo-/hypo-/hypo-
Mixed/mixed/mixedHyper-/A/AHyper-(nim)/hypo-/hypo-
HCC (,z = 18) 18 (100) Hyper-/A/ANon-Hodgkin lymphoma (,z = 1) 1 (100) Hyper-(rim)/hypo-/hypo-
Note-Numbers in parentheses are percentages. Of 14 patients who had more than one colorectal� metastasis, eight patients demonstrated different CT appearances of the metastases; two different ap-� peanances in five patients and three different appearances in three patients. Likewise, of 12 patients� who had more than one noncolorectal metastasis, four patients demonstrated two different CT appear-� ances of the metastases.� * Carcinoid (�i = 51), pancreatic endocrine carcinoma (ii = 15), breast carcinoma (n = 13), renal carci-� noma (;: = 13). medullary thyroid carcinoma (tz = 10), and leiomyosarcoma (ti = 1).
Volume 201 #{149}Number 2 Radiology #{149}331
Table5Size Distribu lion o f Malig nant Lesions
Pathologic 0-1.0 1.1-2.0 2.1-3.0 >3.0Diagnosis cm cm cm cm
Colorectalmetastases(�z=62) 11 13 15 23
Noncotorectalmetastases(n 103) 33 32 18 20
HCC(n=18) ii 5 1 1Non-Hodgkin
l�mphoma(s:=i) 0 1 0 0
because we judged that we could not
make a certain diagnosis of benignancy
in these small lesions. However, all 15
small hypo-/hypo-(cyst)/hypo- lesionswith a sta ndard-of-reference diagno-
sis represented benign disease (Fig 1).
Hypoattenuating noncystic lesions
were grouped in one of four enhance-
ment patterns, which all demonstrated
hypoattenuation in the portal phase,
often somewhat inhomogeneous.When these lesions demonstrated
no enhancement in other phases (ie,
hypo-/hypo-/hypo- pattern), 84(94%)
of 89 lesions were malignant (Table 3).
When an enhancing rim in the arterial
phase was observed (ie, hyper-(nim)/
hypo-/hypo- pattern), all lesions (29
of 29 lesions) were malignant. The
hypervascular rim of hyper-(nim)/
hypo-/hypo- lesions has been well
described (10,15,16,28,29) and prob-
ably represents the well-perfused vi-
able periphery of tumor tissue. Theselesions often demonstrated a reversed
enhancement pattern in equilibrium
phase (ie, a hypoattenuating peniph-
eral rim surrounding a hyperattenuat-
ing center) (Fig 2), a phenomenon
already known as “the washout sign”
(17,30). Others have observed rim en-
hancement around abscesses (31), which� were not present in the current study.
Conversely, if a hypoattenuatinglesion in the portal phase demonstrated
� homogeneous enhancement in theequilibrium phase (ie, hypo-/hypo-/hyper- pattern), only five (62%) of the
eight lesions were malignant (Table
3). The remaining 6% of hypo-/hypo-/
hypo- lesions and 38% of hypo-/hypo-/
hyper- lesions probably represented
� completely, or partly, fibrosed heman-giomas. Honda et al (15) reported a
lack of enhancement during bolos
phase in 15% of hemangiomas and
hypoattenuation after 6-7 minutes in5% of hemangiomas. In that study, no
explanation was given for these find-ings. Whereas the central fibrocarti-
laginous scar in large hemangiomas
does not cause diagnostic difficulties,
the fibrosis in these smaller lesionsgives them a nonspecific hypoattenu-
ating appearance. Four of eight hem-
angiomas with these nonspecific ap-
pearances were found in patients
with a history of colorectal tumor,
emphasizing the problem of lack ofspecificity of these enhancement pat-terns in the studied population.
To avoid confusion between thehyper-(nim)/hypo-/hypo- pattern and
the peripheral enhancement in hem-angiomas, it is essential to differenti-
ate the fairly homogeneous, continu-
ous rim hyperattenuation with
parenchyma but less hyperattenuat-
ing than the vascular spaces that char-
acterizes hyper-(rim)/hypo-/hypo-
lesions (Fig 2) from the globular,
peripheral enhancement, isoattenua-
tion with the arterial system that isthe hallmark of hemangiomas (9,12-
14) (Fig 3).
A subtype enhancement pattern (ie,
hypo-/hypo-[FL]/hypo-) refers to a
hypo-/hypo-/hypo- lesion to the right
of the falciform ligament, on the ante-nor surface of the liver, without mass
effect. No focal abnormality was found
in any of these lesions. The same en-
hancement pattern has been describedas a perfusion defect during CT ante-
nat portography (20,32) on an area of
focal fatty infiltration (21,22). Interest-
ingly, in two of 12 hypo-/hypo-(FL)/
hypo- lesions observed in total during
1 the study period, the hypoattenuationwas also appreciated on unenhanced
images and during the arterial and
equilibrium phases, while the other 10hypo-/hypo-(FL)/hypo- lesions were
only perceived in the portal phase.�, , Possibly, the persistent hypo-/hypo-
(FL)/hypo- lesions were caused by
focal fatty infiltration, whereas the
lesions only perceived in portal phase
may be caused by a variant blood sup-
ply (23).
Hyperattenuating EnhancementPatterns
Recent studies have reported an
improvement in lesion detection if
arterial phase imaging is performed in
addition to portal venous scanning,
especially for hypervascutar lesions
(5-8). However, characterization ofthese lesions as to their clinical impor-tance has so far received little atten-tion.
Hyperattenuation in the arterial
phase has to be differentiated in terms
of arterial attenuation or less than an-tenial attenuation. If a lesion demon-
strates arterial attenuation, either
complete and in alt phases or peniph-eral globular and extending in a cen-tropetat fashion in subsequent phases,
the appearance is pathognomonic for
hemangioma (9,12-14). Marked differ-
ences in perfusion pattern were seen
between the hemangiomas that pre-sented as arterial/arterial/arterial he-
sions. Some hemangiomas did notshow any enhancement in the arterialphase and only started to enhance in
the portal phase, whereas others dem-
onstrated complete enhancement in
both the arterial and portal phases. In
the equilibrium phase, 16 (31%) of 51
arterial/arterial/arterial lesions were
hyperattenuating compared with thevascular system (Fig 3), a phenom-
enon already described by Freeny
and Marks (9). Apparently, due to
slow perfusion, concentration of con-
trast material in the lesion still cx-
ceeded the concentration in the vas-cular system.

Table 6Observed Enhancement Patterns of 131 Benign Lesions and 11 Areas with NoAbnormality
Pathologic Diagnosis No. of Lesions Enhancement Pattern
Hemangiomas (n = 59) 51 (86) Arterial/arterial/arterial5 (8) Hypo-/hypo-/hypo-3 (5) Hypo-/hypo-/hyper-
Cysts (n = 51) 51 (100) Hypo-/hypo-(cyst)/hypo-FNH (n = 7) 5 (71)
2 (29)Hyper-/A/A (cleft)Hyper-/A/A
Adenoma (n = 4) 4 (100) Hyper-/A/AFocal fat (n = 1) 1 (100) Small hypo-/hypo-(cyst)/hypo-Benign at biopsy or follow-up, but not 8 (89) Small hypo-/hypo-(cyst)/hypo-
characterized (71 = 9) 1 (11) Hyper-/A/ANo abnormality (H = 11) 6 (55)
4 (36)1 (9)
Small hypo-/hypo-(cyst)/hypo-Hypo-/hypo-(FL)/hypo-Hyper-(wedge)/iso-/iso-
Note-Numbers in parentheses are percentages. Of 12 patients who had more than one hemangi-oma, four patients demonstrated different �T appearances of the hemangiomas; two different appear-ances in three patients and three different appearances in one patient. In equilibrium phase, only 72%of arterial/arterial/arterial lesions demonstrated the typical appearance of a homogeneous hyperattenu-ating lesion. A persistent central hypoattenuation was seen in 24% of arterial/arterial/arterial lesions,one-fourth of which were less than 3 cm in diameter (Fig 3). In addition, two arterial/arterial/arteriallesions (0.9 and 1.8 cm) were invisible in equilibrium phase, both in patients with only slightly hyperat-
� tenuating vascular spaces.
332 #{149}Radiology November 1996
The combination of all phases al-
lowed us a confident diagnosis of he-
mangioma in 86% of alt hemangiomas
present (Table 6). Since 25 (42%) of
the 59 hemangiomas were 2 cm orsmaller, this is a good result and com-
pares favorably with the findings of a
biphasic CT study designed to differ-
entiate hemangiomas from malignantlesions (10). In that study, bolus dy-
namic phase combined with delayed
scanning (5-60 minutes after injection
of contrast material) allowed a confi-
dent diagnosis in 53.7% of hemangio-
mas. In addition, the criteria used
were not specific, since one pancreaticcarcinoma metastasis was erroneously
characterized as hemangioma. We
believe that the better results in thecurrent study were achieved because
the triphasic spiral CT technique al-
lows optimal use of contrast dynamics
due to the speed of data acquisition.Overlapping reconstructions allow
centering of the plane of reconstruc-
tion with respect to lesions and, thus,
leads to a higher percentage of typical
appearances. More stringent criteria
for the “ typical hemangioma appear-
ance” were adopted to prevent false-positive diagnoses. The ability of tn-
phasic liver CT to facilitate confident
characterization of most hemangio-
mas, irrespective of their size, poten-
tially can lead to a substantial reduc-
tion in confirmatory tests, such as T2-
weighted MR imaging, red blood cellscintignaphy, or histologic biopsy, as
advocated in patients suspected of
having hemangiomas (14).
The second group of lesions withhyperattenuation in the arterial phase
demonstrated enhancement less than
arterial space attenuation. Hyper-/
A/A lesions are nonspecific hypervas-
cular lesions found in malignant and
benign disease. Most (84%) hyper-/
A/A lesions were malignant and rep-resented metastases from hypervascu-
lan tumors or HCC (Table 3, Fig 4).
Although 90 (87%) of 103 noncolo-rectal metastases represented metas-
tases from hypervascular primary
tumors, only 44% presented as hyper-
attenuating lesions in the arterial
phase (19% hyper-/A/A and 25%
mixed/mixed/mixed); the remainder(51% hypo-/hypo-/hypo- and 4%
hyper-(nim)/hypo-/hypo-) were indis-
tinguishable from hypovascular cob-
rectal metastases (Table 4). Whether
metastases from hypervascular pri-
many tumors are well depicted on anincremental bolus dynamic scan is amatter of discussion (33-35). If lesion
detection is the only issue, portalphase images alone would have al-
bowed detection of all hypervascularmetastases. However, 13 (65%) of 20
hypervascular metastases that ap-
peared as hyper-/A/A lesions were
better delineated on arterial phase
images, while the other seven (35%)
hyper-/A/A hypervascular metastases
were better delineated on portal phaseimages owing to a small hypoattenu-
ating rim that surrounded the other-
wise isoattenuating lesion (Fig 4).
All 18 HCC lesions presented as
hyper-/A/A; three lesions were only
visible in the arterial phase, five le-
sions were hypoattenuating in the
portal phase, and 10 lesions (presentin one patient) were hyperattenuat-
Table 7Size Distribution of Benign Lesions
Pathologic 0-1 1.1-2.0 2.1-3.0 >3
Diagnosis cm cm cm cm
Hemangiomas(n=59)
Artenial/arte-rial/arterial 8 17 9 17
Hypo-/hypo-/hypo- 3 1 1 0
Hypo-/hypo-/hyper- 1 1 0 1
Cysts(n=51) 26 18 3 4FNH(n=7) 0 1 1 5Adenoma (n = 4) 1 0 0 3
Figure 1. Portal phase image shows a smallhypoattenuating lesion (arrow) in the dorsalaspect of the right side of the liver with a smallhypo-/hypo-(cyst)/hypo- appearance. Theright side of the liver was resected for a largehemangioma at a more cranial level. At histo-pathologic examination, a focal fat depositwas found at the location of the small hypo/hypo-(cyst)/hypo- lesion.
ing in the portal phase and better vi-
sualized than in the arterial phase.
These findings are in keeping with
the well-known hypervascularity of
HCC (15,24,36). However, larger stud-ies are needed to confirm if all hyper-/
A/A lesions occurring in patients with
chronic liver disease truly represent
HCC lesions.Only 16% of hyper-/A/A lesions
were benign and represented adeno-mas, FNHs, or a benign lesion with
unknown histologic diagnosis (Table3). Interpretation of a hyper-/A/A be-
sion should be done in a clinical con-
text; all malignant hyper-/A/A lesionsoccurred in patients with chronic liverdisease or in patients with a known
hypervascular primary malignancy.
Conversely, all benign hyper-/A/A
lesions occurred in patients without
such a history, except orie lesion in a
patient with a history of melanoma.Consequently, aspiration biopsy was

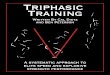
a.Figure 2. Colorectal metastasis with hyper-(rim)/hypo-/hypo- appearance. (a) Arterial phase image shows a homogeneously enhanced hyper-attenuating rim (arrows). (b) Portal phase image shows that the lesion was homogeneously hypoattenuating. (c) Equilibrium phase image shows that
the periphery of the metastasis is hypoattenuating (arrows) relative to the enhanced center of the lesion and the surrounding liver parenchyma.
d. e. f.
Volume 201 #{149}Number 2 Radiology #{149}333
Figure 3. Tniphasic liver CT images at two anatomic levels. (a-c) In the anterior segment of the left lobe, a lesion is present with the appear-ance of a large arterial/arterial/arterial lesion. (d-f) In the right lobe, a small subcapsulan lesion is present (arrow) that showed intense and
complete enhancement in the arterial (d) and portal (e) phases, consistent with a small arterial/arterial/arterial lesion. Both lesions demon-
strated complete enhancement in the equilibrium phase (c, f larrowl), hyperattenuating compared with the vascular system. Two hemangio-
mas were confirmed at tapanotomy.

a. b. c.Figure 4. (a) Arterial, (b) portal, and (c) equilibrium phase sections in a patient with metastases from medutlary thyroid carcinoma. In the arte-nat and equilibrium phases, metastases were only slightly hyperattenuating and some were faintly visible (arrows in a and c) only due to a subtle
hypoattenuating rim. In the portal phase, metastases in the right side of the liver were slightly hyperattenuating and surrounded with a well-
demarcated hypoattenuating rim. One metastasis in the left side of the liver was hypoattenuating (arrow in b). The metastases in the right side
of the liver were interpreted as (atypical) hyper-/A/A lesions, whereas the metastasis in the left side of the liver was consistent with a hypo-/
hypo-/hypo- lesion.
334 #{149}Radiology November 1996
essential for differentiating melanoma
metastasis from adenoma or FNH.
Hyper-/A/A(cleft) refers to a sub-
type pattern wherein a central hypo-
attenuating cleft is observed in the
arterial phase, and the cleft enhances
in the equilibrium phase. This cleftmay be stellate, round, or linear. In all
hyper-/A/A(cteft) lesions with a stan-
dard of reference, the diagnosis ofFNH was confirmed (Fig 5). Conversely,
a hyper-/A/A(cteft) appearance was
found in 71 % of FNH (Table 6), whichcompares favorably with angiogra-
phy, and reported to be characteristic
in 73% (11). In view of the associated
risk of hemorrhage in adenomas, it is
important to differentiate adenomas
from FNH. In our limited experience
so far, a hyper-/A/A(cleft) lesion ex-
cludes the possibility of adenoma,
thus potentially limiting the need for
further imaging procedures.
In one patient, a wedge-shaped areaof hyperattenuation was observed in
the arterial phase, in an area whereno abnormality was found at surgery.
It is important to differentiate such a
hyper-(wedge)/iso-/iso- pattern, with-
out any sign of focal disease, from
subsegmentat areas of contrast en-
hancement, which may accompany
focal liver lesions, probably due to
increased arterial supply to the liver
region that contains the lesions (7,37).All mixed/mixed/mixed lesions
represented malignant disease, the
majority (26 lesions [93%]) being non-
colorectal metastases (Table 3). Prob-
ably, the combination of enhancing
tumor with interspersed areas of ne-
crosis was the cause of this appear-
ance.
Study Limitations
A number of limitations are present
in our study. The study was not blinded;
the clinical history of all but one pa-
tient and the results of other imaging
studies in some patients were known.
The reported data are only relevant to
the studied population, wherein some
abnormalities were not represented
(eg, infectious disease). Some of the
standards of reference used can be
criticized. In some patients with mul-tiple lesions, biopsy was performed of
only one lesion, and coexisting lesions
with the same CT appearance were
assumed to represent the same abnor-
mality as the biopsy lesion. Preferably,each lesion would have been corre-bated with surgery or biopsy, but this
would exclude a large amount of le-
sions from the study and introduce a
selection bias. We are unable to quan-
titate the addition value of arterial
and equilibrium phase sections rela-
tive to portal phase sections alone for
two reasons. First, sections of the three
phases were interpreted concurrently,
and second, section geometry of the
three phases differed. If all three phases
would have been acquired with thesame section geometry, comparison of
the value of the three separate phases
would have been meaningful. How-
ever, with the scanner used, this could
only have been achieved by scanning
all phases with 10-mm collimationand 10 mm/sec table speed. Instead,
we chose 5-mm collimation and 5
mm/sec table speed for the portal sec-
tions to minimize partial volume aver-
aging. Other scanners, and the most
recent version of the scanner used,
offer the possibility of identical sec-
tion geometry in all phases, with use
of 7- or 8-mm collimation; however,
this would still result in an increase in
partial volume averaging in portal
phase sections.
By strictly defining the 11 CT ap-
pearances, an objective characteriza-
tion system is implied. In our experi-
ence, the definitions of the various CT
appearances do fit the vast majority of
lesions; however, some lesions are
difficult to classify because they do
not strictly follow the definition of the
various CT appearances. In these
cases, one has to judge which appear-
ance best fits the lesion under study.
Conclusions
Triphasic spiral liver CT is a stan-
danized CT procedure, designed to
enable detection and characterization
of a large variety of liver lesions, also
in the presence of different pathologic
conditions and multilevel disease. The
5-mm portal phase images, recon-
structed at 2-mm intervals, acquired
at the peak of liver enhancement are
the centerpiece of the protocol andare essential for lesion detection. Ante-nat phase images are helpful in the
detection of hypervascular lesions
and are essential for the characteniza-
tion of a large proportion of lesions.
Equilibrium phase images further aid

a. b. c.Figure 5. Triphasic liver CT scans of a patient with two FNHs. (a) Arterial phase image shows that the lesions (arrows) have a tobutated, ho-mogeneous area of hyperattenuation with radiating linear areas of hypoattenuation in their centers. (b) Portal phase image shows that the te-sions are almost isoattenuating (small arrows), with the exception of a small area of hypoattenuation (large arrow) in the central part of the
caudate lobe lesion. The ventral lesion also demonstrated such a hypoattenuation at a slightly higher level (not shown). (c) Equilibrium phase
image shows that the lesions are isoattenuating, except for the central part which has become hyperattenuating (arrow). The findings were
consistent with a hyper-/A/A(cteft) pattern.
Volume 201 #{149}Number 2 Radiology #{149}335
in lesion characterization. Our results
demonstrate that characterization of
frequently occurring benign focal
liver lesions, such as hemangioma,cyst, and FNH, which represented 117
(36%) of the 326 focal liver lesions
with a standard of reference, was sat-
isfactony (51 [86%] of 59 hemangio-
mas, 51 [100%] of 51 cysts, and five
[71%] of seven FNHs). All lesions with
a small hypo-/hypo-(cyst)/hypo- ap-
pearance were also benign. Conversely,
all hyper-(nim)/hypo-/hypo- lesions,
all mixed/mixed/mixed lesions, and
all but one hyper-/A/A lesions in pa-
tients with a hypervascular primary
tumor or chronic liver disease repre-
sented malignant disease. Hypo-/
hypo-/hypo- and hypo-/hypo-/hyper-
lesions need to be interpreted with
caution. A small proportion of hypo-/
hypo-/hypo- lesions (6%) and a large
proportion of hypo-/hypo-/hyper-
lesions (38%) were due to probably
fibrosed hemangiomas; the remainder
were due to both colorectal and non-
colorectal metastases.
In clinical practice, one has to de-
cide in which patients to use triphasic
liver CT. The liven is scanned four
times, with resultant increased radia-
tion exposure. In addition, the proce-
dune takes more time and is more
costly than (single-phase) spiral CTbecause of the large number of im-
ages acquired that all have to be re-
constructed and interpreted. There-
fore, one has to limit its use to patients
who are likely to gain from this addi-
tional burden.
In our clinic, patients with unclassi-
tied lesions at US or monophasic CT,
possible resectable colorectat metasta-
ses or metastases from hypenvascular
primary tumors, and suspected HCC
constitute the vast majority of those
who undergo tniphasic liver CT. In
these patients, triphasic liver CT, per-
formed as an outpatient procedure,
is likely to provide most information
needed for clinical management. #{149}
Acknowledgments: We thank Willeke Rauwfor helping to translate ideas into practical pro-tocols, Jacques Steenbeek, BSc, (Philips MedicalSystems) for technical advice, and Wouter vanEs, MD, and Evan Dillon, MD, for critical reviewof the manuscript.
References1. Bluemke DA, Fishman EK. Spiral CT of
the liver. AIR 1993; 160:787-792.2. Zeman RK, Fox SH, Silverman PM, et al.
Helical (spiral) CT of the abdomen. AJR1993; 160:719-725.
3. Zeman RK, Zeiberg AS, Davros WJ, et al.Routine helical CT of the abdomen: imagequality considerations. Radiology 1993;189:395-400.
4. Bluemke DA, Urban BA, Fishman EK.Spiral CT of the liver: current applications.Semin Ultrasound CT MR 1994; 15:107-121.
5. Baron RL, Dodd GD III, Holbert BL, OliverJH III, Cam B. Helical biphasic contrastCT in evaluation of hepatocellular carci-noma (abstr). Radiology 1994; l93(P):435.
6. Murakami T, Kim T, Oi H, et al. Detect-ability of hypervascular hepatocellular can-cinoma by arterial phase images of MR andspinal CT. Acta Radiol 1995; 36:372-376.
7. Hollett MD, Brooke Jeffrey R, Nino-MurciaM, Jorgensen MJ, Harris DP. Dual-phasehelical CT of the liver: value of arterial
phase scans in the detection of small ( < 1.5cm) malignant hepatic neoplasms. AJR1995; 164:879-884.
8. Bonaldi VM, Bret I’M, Reinhold C, Atni M.Helical CT of the liver: value ot an earlyhepatic arterial phase. Radiology 1995; 197:357-363.
9. Freeny PC, Marks WM. Hepatic hemangi-
oma: dynamic bolus CT. AJR 1986; 147:71 1-719.
10. Freeny PC, Marks WM. Patterns of con-trast enhancement of benign and malig-nant hepatic neoplasms during bolus dy-namic and delayed CT. Radiology 1986;160:613-618.
11. Mathieu D, Bruneton JN, Dnouilland J,Pointreau CC, Vasile N. Hepatic adeno-mas and focal nodular hyperplasia: dy-namic CT study. Radiology 1986; 160:53-58.
12. Ashida C, Fishman EK, Zenhouni EA,Siegelman SS. Computed tomography ofhepatic cavernous hemangioma. J ComputAssist Tomogn 1987; 11:455-461).
13. Quinn SF, Benjamin GG. Hepatic cavern-
ous hemangiomas: simple diagnostic signwith dynamic bolus CT. Radiology 1992;182:545-548.
14. Nelson RC, Chezmar JL. Diagnostic ap-proach to hepatic hemangiomas. Radiology
1990; 176:11-13.15. Honda H, Matsuura Y, Onitsuka H, et al.
Differential diagnosis of hepatic tumors(hepatoma, hemangioma, and metastasis)with CT: value of two-phase incrementalimaging. AJR 1992; 159:735-740.
16. Munamatsu Y, Takayasu KT, Moniyama N,et al. Peripheral low-density area of he-patic tumors: CT-pathologic correlation.
Radiology 1986; 160:49-52.17. Lin G, Gustafson T, Hagenstnand I, Lunden-
quist A. CT demonstration ot low densityring in liver metastases. J Comput AssistTomogr 1984; 8:450-452.
18. Kihana Y, Tamuna 5, Yuki Y, et al. Opti-mal timing for delineation of hepatocellu-Ian carcinoma in dynamic CT. J ComputAssist Tomogn 1993; 17:719-722.
19. Yoshikawa J, Matsui 0, Kadoya M, et al.Delayed enhancement of fibrotic areas inhepatic masses: CT-pathologic correlation.I Comput Assist Tomogr 1992; 16:206-211.
20. Peterson MS, Baron RL, Dodd GD III, et al.

336 #{149}Radiology November 1996
Hepatic parenchymal perfusion defectsdetected with CTAP: imaging-pathologiccorrelation. Radology 1992; 185:149-155.
21. Yoshikawa J, Matsui 0, Takashima T, et al.Focal fatty change of the liver adjacent tothe falsiform ligament: CT and sonographicfindings in five surgically confirmed cases.AJR 1987; 165:419-423.
22. Paulson EK, Baker ME, Spritzer CE, LederRA, Gulliver DJ, Meyers WC. Focal fattyinfiltration: a cause of nontumorous defectsin the left hepatic lobe during CT arterial
portography. J Comput Assist Tomogr1993; 17:590-595.
23. Arai K, Matsui 0, Takashima T, Ida M,Nishida Y. Focal spared areas in fattyliver caused by regional decreased portalflow. AJR 1988; 151 :300-302.
24. Craig JR, Peters RL, Edmondson HA. Tu-mors of the liver and intrahepatic bile
ducts. Atlas of tumor pathology, fasc 26, ser2. Washington, DC: Armed Forces Institute
of Pathology, 1989.
25. Karhunen PJ, Pentilla A, Liesto K, MannikoA, Mottonen, M. Benign bile duct tu-
mours, non-paracytic liver cysts and liverdamage in males. J Hepatol 1986; 2:89-99.
26. Karhunen PJ. Benign hepatic tumoursand tumour-like conditions in men. J ClinPathol 1986; 39:183-188.
27. Jones EC, ChezmarJL, Nelson RC, Bernar-dino ME. The frequency and significance
of small ( < 15 mm) hepatic lesions detectedby CT. AJR 1992; 158:535-539.
28. Freeny PC, Marks WM. Computed to-mography arteriography of the liver. Radi-ology 1983; 148:193-197.
29. Freeny PC, Marks WM. Hepatic perfu-sion abnormalities during CT angiography:detection and interpretation. Radiology1986; 159:685-691.
30. Mahfouz AE, Hamm B, Wolf KJ. Penph-eral washout: a sign of malignancy on dy-namic gadolinium-enhanced MR images offocal liverlesions. Radiology 1994; 190:49-52.
31. Brooke JR. Dual phase abdominal spiral(helical) CT. In: Syllabus annual course So-ciety of Computed Body Tomography andMagnetic Resonance, Rochester, Minn: So-ciety of Computed Body Tomography andMagnetic Resonance; 1996; 19-23.
32. Nelson RC, Thompson GH, ChezmarJL,Harned RK II, Fernandez MP. CT duringarterial portography: diagnostic pitfalls.RadioGraphics 1992; 12:705-718.
33. Bressler EL, Alpern MB, Glazer GM, Francis
IR, Ensminger WD. Hypervascular he-patic metastases: CT evaluation. Radiology1987; 162:49-51.
34. Patten RM, Byun JY, Freeny PC. CT of
hypervascular hepatic tumors: are unen-hanced scans necessary for diagnosis? AIR
1993; 161:979-984.35. Miketic LM. Are contrast-enhanced scans
necessary? (comment). AIR 1993; 161:984.
36. Choi BI, Takayasu K, Han MC. Small he-patocellular carcinomas and associated
nodular lesions of the liver: pathology,pathogenesis, and imaging findings. AJR1993; 160:1177-1187.
37. Itai Y, Moss AA, Goldberg HI. Transienthepatic attenuation difference of lobar orsegmental distribution detected by dy-namic computed tomography. Radiology1982; 144:835-839.