-
8/11/2019 Fluid Therapy and Electrolite
1/36
Fluid therapyand electrolite
-
8/11/2019 Fluid Therapy and Electrolite
2/36
TBW = 60% BB
-
8/11/2019 Fluid Therapy and Electrolite
3/36
Fluid composition differs between
compartments
-
8/11/2019 Fluid Therapy and Electrolite
4/36
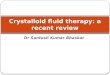
Starlings equation
Qf= Kf [(Pc-Pi) d(c-i)]
-
8/11/2019 Fluid Therapy and Electrolite
5/36
Microvascular fluid exchange
-
8/11/2019 Fluid Therapy and Electrolite
6/36
Hydrostatic and oncotic pressure
-
8/11/2019 Fluid Therapy and Electrolite
7/36
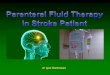
Resuscitation Maintenance
NutritionCristalloid
Replace acute losses(hemorrhage,
GI loss, 3 rdspace)
1. Normal requirement(IWL + urine + feses)
2. Nutritional support
Fluid therapy
Colloid Elektrolite
Repair
-
8/11/2019 Fluid Therapy and Electrolite
8/36
Crystalloids
-
8/11/2019 Fluid Therapy and Electrolite
9/36
Colloid
High molecular weight substance that
largely remain in the intravascular
compartment, thereby generating anoncotic pressure. To have a
greater
intravascular persistence when
compare to cristalloids
-
8/11/2019 Fluid Therapy and Electrolite
10/36
Colloid
-
8/11/2019 Fluid Therapy and Electrolite
11/36
Advantages
-
8/11/2019 Fluid Therapy and Electrolite
12/36
Disadvantages
-
8/11/2019 Fluid Therapy and Electrolite
13/36
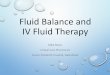
Sodium
The main determinant of ECF osmolality
The body fluid osmolality is 285 295
mOsm/kgCalculated ECF osmolality is
2 x Na + glucose / 18
-
8/11/2019 Fluid Therapy and Electrolite
14/36
Hypernatremia
Na > 145 mmol / L
Hypertonicity and absolute or relative
water deficitNeurologic effect ( altered mental status,
coma and seizure )
-
8/11/2019 Fluid Therapy and Electrolite
15/36
Caused
Hypovolemic hypernatremia
Loss of hypotonic fluids
Euvolemic hypernatremiaNet loss of free water
Hypervolemic hypernatremia
Gain of hypertonic fluid
-
8/11/2019 Fluid Therapy and Electrolite
16/36
Treatment
In hypovolemic replace volume deficit
with isotonic saline then correct hyper
Na with hypotonic fluids ( 0,45 % NaCl or
D5W ) In hypervolemic, enhance removal of
excess Na with loop diuretic
Correction < 0.5 mmol/hr for chronic and
< 1 mmol/hr for acute, and no more than10 mmol for 24 hrs
-
8/11/2019 Fluid Therapy and Electrolite
17/36
Current TBW x current Na = normal TBW x normal Na
Current TBW = normal TBW x ( 140 / current Na )
TBW deficit = normal TBW current TBW
= 0.6 BB current TBW
= ( 0.6 BB ) ( 1 140 / current Na )
Treat underlying disease
-
8/11/2019 Fluid Therapy and Electrolite
18/36
Hyponatremia
Na < 135 mmol / L
Pseudo hyponatremia : normal or
increase plasma osmolality True hyponatremia : increase free
water
relative to sodium
-
8/11/2019 Fluid Therapy and Electrolite
19/36
Treatment
1. Low ECFAsymptomatic : isotonic saline
Symptomatic : Hypertonic saline
2. Normal ECF
Asymptomatic : furosemide + isotonicsaline
Symptomatic : furosemide + hypertonicsaline
3. High ECF
Asymptomatic : furosemide
Symptomatic : furosemide + hypertonic
saline
-
8/11/2019 Fluid Therapy and Electrolite
20/36
Na deficit = TBW x ( desired Na current Na )= ( 0.6 BB ) ( 130
current Na )
3% NaCl = 513 mmol Na0.9% NaCl = 154 mmol Na
-
8/11/2019 Fluid Therapy and Electrolite
21/36
Potassium
Predominant intracellular
< 2% potassium in the ECF fluid
-
8/11/2019 Fluid Therapy and Electrolite
22/36
Hypokalemia
T inverted, U wave, atrial and ventricular
arrhythmias
Muscle weakness, ileus and paralysis
Nefrogenic DI
-
8/11/2019 Fluid Therapy and Electrolite
23/36
Treatment
Potassium replacement are hyperosmolar
and should preferable through CVC
Replacement rate 10 30 mEq/hr diluted in
100 200 ml NS/D5%
-
8/11/2019 Fluid Therapy and Electrolite
24/36
Hyperkalemia
Tall peaked T wave, prolonged PR
interval, flattened P wave, Widened QRS
complex, VT, VF and cardiac arrestNeuromuscular weakness,
areflexia,
paralysis and paresthesia
-
8/11/2019 Fluid Therapy and Electrolite
25/36
Treatment
IV Ca gluconate or CaCl2 10 20 ml in 5
minutes
IV Dextrose 50% 50 ml + IV 5 10 U
regular insulin in 10 minutes
IV NaHCO350 100 meq in 10 minutes
Hemodialysis / CRRT
-
8/11/2019 Fluid Therapy and Electrolite
26/36
Calcium
In extracellular, calcium is free or bound
to albumin
The ionized ( free ) is biologically active
Acidosis decreases bindingAlkalosis increases binding
-
8/11/2019 Fluid Therapy and Electrolite
27/36
Hypercalcemia
Mental manifestation vary from stupor to
coma
Neurologic effects ( redices muscle tone
and reflexes ) Vomiting, polyuria, polydipsia and
constipation
Arrhythmias
-
8/11/2019 Fluid Therapy and Electrolite
28/36
Treatment
Hydration to achieve urine 3 5 L / day
Furosemide
Calcitonin
Biphosphonates
-
8/11/2019 Fluid Therapy and Electrolite
29/36
Hypocalcemia
Neurologic manifestations include
hyperreflexia and tetany
-
8/11/2019 Fluid Therapy and Electrolite
30/36
Treatment
Ca gluconate or Ca chloride 10 ml in 50
ml Dx 5% over 10 min
Infusion of 1 2 mg calcium / kg / hour
until ionized calcium is 4.5 mg / dL ortotal calcium is 7 mg /
dL
Vitamin D
-
8/11/2019 Fluid Therapy and Electrolite
31/36
Magnesium
Free form 70%, 30% bound to albumin
Magnesium level depend on intestinal
absorption and renal excretion
-
8/11/2019 Fluid Therapy and Electrolite
32/36
Hypermagnesemia
Decreased reflexes, flaccid paralysis,
stupor and coma
Most common caused is renal failure
and aggravated use of magnesium
-
8/11/2019 Fluid Therapy and Electrolite
33/36
Treatment
Dialysis when renal function is impaired
Diuretic to increased urine production
Ca gluconate 10 ml in 50 ml Dx 5% over
10 minutes
-
8/11/2019 Fluid Therapy and Electrolite
34/36
Hypomagnesemia
Secondary effect of hypocalcemia. Lowmagnesium impairs PTH
secretion which
result in hypocalcemia
-
8/11/2019 Fluid Therapy and Electrolite
35/36
Treatment
1 2 gr MgSO4 over 5 10 minutes
Can be followed by infusion 1 5 gr over
4 6 hours.
-
8/11/2019 Fluid Therapy and Electrolite
36/36