Embed Size (px)
Citation preview

FLUID AND ELECTROLYTE BALANCE
John M. Burke, Pharm.D.St. Louis College of Pharmacy
Veterans Administration Medical Center

FLUID BALANCE
I. IntroductionII. Physiology of Body FluidsIII. Assessing Fluid StatusIV. Use of IV fluidsV. Hypernatremia

Body Fluid Distribution
Extracellular fluid Intracellular Fluid
= Sodium
= Potassium

ASSESSING FLUID BALANCEBASAL FLUID REQUIREMENTS
WEIGHT00--10 Kg10 Kg 100100 mLmL/Kg/Kg1010--20 kg20 kg 10001000 mLmL + 50+ 50 mLmL/kg (Wt/kg (Wt--10)10)>20 Kg>20 Kg 15001500 mLmL + 20+ 20 mLmL/kg (Wt/kg (Wt--20)20)
Body Surface Area 1500 ml/m2

ASSESSING FLUID BALANCEBASAL FLUID REQUIREMENTS
ESTIMATE THE DAILY FLUID REQUIREMENTS FOR AEUVOLEMIC PATIENT WITH A BODY WEIGHT OF 70 KG

ASSESSING FLUID BALANCEBASAL FLUID REQUIREMENTS
ESTIMATE THE DAILY FLUID REQUIREMENTS FOR AEUVOLEMIC PATIENT WITH A BODY WEIGHT OF 70 KG
10 kg10 kg 1000 ml/day1000 ml/day20 kg20 kg 1500 ml/day1500 ml/day60 kg60 kg 2300 ml/day2300 ml/day80 kg80 kg 2700 ml/day2700 ml/day
OTHER EXAMPLES
1500 ml + 20 ml/kg (70 kg - 20 kg)1500 ml + 20 (50)2500 ml/day = 104 ml/hr

ASSESSING FLUID BALANCE
SYMPTOMS DRY MOUTHEDEMACHANGES IN URINE OUTPUT

ASSESSING FLUID BALANCE
PHYSICAL FINDINGSWEIGHT CHANGESTEMPERATUREBP, ORTHOSTASIS, HEART RATEMUCOUS MEMBRANESJVD (PRESENCE/ABSENCE)PULM: RALESEDEMA (PRESENCE/ABSENCE)

ASSESSING FLUID BALANCEMONITORING FLUID STATUS
LABORATORYBUN, SERUM CREATININEURINE OSMOLALITYSERUM OSMOLALITYUna, FeNa

ASSESSING FLUID BALANCEMONITORING FLUID STATUS
Sensible losses: intake/output; urine output Insensible losses: 500-1000 ml/dayWeight

Fractional Excretion of Sodium
Calculate the FeNa for a 96 y/o female with CHF, diuretic therapy.Una = 11; Sna = 140; Ucr = 13.6; Scr = 2.1
FeNa = (Urine Na) / (Urine Cr) x 100(Serum Na) / (Serum Cr)

Fractional Excretion of Sodium
Calculate the FeNa for a 96 y/o female with CHF, diuretic therapy.Una = 11; Sna = 140; Ucr = 13.6; Scr = 2.1
FeNa = (11) / (13.6) x 100 = 1.2%(140) / (2.1)

FLUID BALANCE
SERUM OSMOLALITY
SOSM = 2[Na+] + BUN/2.8 + GLUCOSE/18
Normal serum osmolality: 280-300 mOsm/kg

ASSESSING FLUID BALANCEPLASMA OSMOLALITY
ASSESSING FLUID BALANCEPLASMA OSMOLALITY
Calculate Sosm for a patient with:Sodium 135 mEq/LBUN 12 mg/dlGlucose: 90 mg/dl

ASSESSING FLUID BALANCEPLASMA OSMOLALITY
SOSM = 2[Na+] + BUN/2.8 + GLUCOSE/18
= 2(135)= 2(135) + 12/2.8+ 12/2.8 + 90/18+ 90/18
= 270= 270 + 4+ 4 + 5+ 5
= 279= 279 mOsmmOsm/kg/kg

IV FLUIDS
ContentDistribution of IV fluidsBasal fluid requirementsCorrecting fluid deficitsReplacing free water deficits

IV Fluids
1 literD5W
Dextrose50 g
1 liter¼ NS
NaCl 38.5 mEq
1 literNS
NaCl154 mEq
1 liter1/2 NS
NaCl77 mEq
1 literRingers
NaCl147 mEqK 4Ca 4
308mOsm/l
154mOsm/l
77mOsm/l
250mOsm/l
310mOsm/l

Distribution of Normal Saline
Extracellular fluid Intracellular Fluid
= Sodium
= Potassium
NaCl
154 mEq

Distribution of D5W
Extracellular fluid Intracellular Fluid
= Sodium
= Potassium
Dextrose
50 g

DISTRIBUTION OF IV FLUIDS
DISTRIBUTION OF IV FLUIDS
What percentage of the fluid administered would What percentage of the fluid administered would stay in the EXTRAstay in the EXTRA--cellular space?cellular space?
normal saline normal saline = __= __100_100____%___%1/2 NS1/2 NS = ___= ___7373___%___%1/4 NS1/4 NS = ___= ___5555___%___%D5WD5W = ___= ___4040___%___%RingersRingers = ___97___%= ___97___%LRLR = ___= ___8686___%___%

DISTRIBUTION OF IV FLUIDS
DISTRIBUTION OF IV FLUIDS
How would you expect the addition of dextrose to an IV fluid to change the distribution?
Example: Normal saline vs Normal saline with D5W
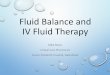
IV Fluids
1 literNS
NaCl154 mEq
1 literD5NS
NaCl154mEq
Dextrose50 g

Providing Basal Fluid Requirements
Choice of IV Fluids½ Normal SalineD5 ½NS¼ Normal SalineD5 ¼NS
Rationale for choice: provides some sodiumsome free water

Providing Basal Fluid Requirements
IV fluid rate
ml/hr = basal fluid requirements/ 24 hours
AdditivesKCl: 20 mEq/l IVF (if serum K is normal)

Example55 y/o male. Ht 6’0”, Wt 78 kgNPO.EuvolemicBasal fluid requirements?

Example55 y/o male. Ht 6’0”, Wt 78 kgNPO.EuvolemicBasal fluid requirements?
Dextrose 5%/0.45% sodium chloride With 20 mEq KCl/L IVFInfused at 110 ml/hr
(see previous basal fluid requirement calculations)

Correction of Hypovolemia
Choice of IV FluidsNormal SalineLactated RingersRingers solution
Rationale for choice:

Correction of HypovolemiaIV Fluid rateSevere hypovolemia:500-1000 ml/hr until hemodynamically stablefollowed by a lower rateModerate hypovolemia2-3 times maintenance fluid requirementsMild hypovolemia1-2 times maintenance fluid requirements

ExampleBasal fluid requirements are 2000 ml/dayIf 20 mEq KCl is added to each liter, how much fluid would the patient receive?
Rate for maintenance fluids?
What if patient is hypovolemic?
What if patient is volume overloaded?

ExampleBasal fluid requirements are 2000 ml/dayIf 20 mEq KCl is added to each liter, how much fluid would the patient receive?
Rate for maintenance fluids?83 ml/hr; 40 mEq KCl per dayWhat if patient is hypovolemic?125-150 ml/hr; 60-72 mEq per dayWhat if patient is volume overloaded?

DISORDERS OF SODIUM BALANCE
VOLUME STATUSHYPOVOLEMIC
SODIUMSODIUMmEqmEq/L/L
< 135< 135
135135--145145
> 145> 145
ISOVOLEMIC HYPERVOLEMIC
NORMAL

FLUID/ELECTROLYTE DISORDERSHYPERNATREMIA
FLUID/ELECTROLYTE DISORDERSHYPERNATREMIA
DEVELOPMENT OF HYPERNATREMIAWater LossSodium Retention
Intact Thirst mechanism provides protection

ASSESSMENT OF THE PATIENT WITH HYPERNATREMIAASSESSMENT OF THE PATIENT WITH HYPERNATREMIA
HYPERVOLEMICHYPERVOLEMICHYPERNATREMIAHYPERNATREMIA
DETERMINE SERUM OSMOLALITYDETERMINE SERUM OSMOLALITY
ASSESS VOLUME STATUSASSESS VOLUME STATUS
HYPOVOLEMICHYPOVOLEMICHYPERNATREMIAHYPERNATREMIA
ISOVOLEMICISOVOLEMICHYPERNATREMIAHYPERNATREMIA
Renal lossesdiureticsglucosuriaARF/CRFpartial post-renal obst
Adrenal insufficiencyGI lossesResp lossesInsensible loss
Diabetes insipidus Renal FailureIatrogenicMineralocorticoid excess

FLUID/ELECTROLYTE DISORDERSASSESSMENT OF HYPERNATREMIA
HYPOHYPO--VOLEMICVOLEMIC EUVOLEMICEUVOLEMIC
H20 LOSS > Na LOSSH20 LOSS > Na LOSSnormal Nanormal NaSlSl H20 DEFICITH20 DEFICIT Na EXCESS >Na EXCESS >
H20 EXCESSH20 EXCESS
HYPERVOLEMICHYPERVOLEMIC
Diabetes InsipidusFluid Loss Renal FailureLiver FailureCHF

HypernatremiaClinical Manifestations
CNS dysfunction: restlessness irritabilitytremulousness spasticityhyperreflexia ataxiaseizures coma, death
polyuria if due to diabetes insipiduspolydipsia
Severity based on severity and rate of development

HypernatremiaClinical Manifestations
Urine osmolalityvariablebased on cause of hypernatremia
Volume statusvariablebased on cause


NormalBrainNormalosmolality
Water Loss
Highosmolality
Accumulationof electrolytes
Highosmolality
Accumulationof organicosmoles
CerebralEdema
Immediate effect ofhypertonic state
RapidAdaptation
SlowAdaptationRapid
correction ofhypertonicity
Slow Correctionof hypertonicity
water
Adrogue HJ. N Engl J Med 2000; 342: 1493-9.

HypernatremiaECF Volume
Low Normal/increased
Uvol < 3 l/day Uvol > 3 l/day
Uosm > 450 Uosm
> 300
Postural Hypotension
Na/H20 depletion 1º H20depletion
Uvol > 3 l/day
Uosm < 250 Uosm > 300
Osmotic diuresisDI
Responseto ADH
CentralDI
NephrogenicDI
yes noyes no
Osmoticdiuresis

Hypernatremia
Assessment of Free Water deficit
deficit (liters) = (Wt)(0.6) (Serum Na - 1)140

Correction of Hypernatremia
VOLUME STATUSHYPOVOLEMIC
SODIUMSODIUMmEqmEq/L/L
< 135< 135
135135--145145
> 145> 145
ISOVOLEMIC HYPERVOLEMIC
NORMAL

DISORDERS OF SODIUM BALANCE
VOLUME STATUSHYPOVOLEMIC
SODIUMSODIUMmEqmEq/L/L
< 135< 135
135135--145145
> 145> 145
ISOVOLEMIC HYPERVOLEMIC
NORMAL

Hypovolemic Hypernatremia
Etiologies:Renal lossesadrenal insufficiencyGI lossesRespiratory lossesInsensible losses
excessive loss of sodium and water [Na+] = Na
H2O

Extracellular fluid Intracellular Fluid
Hypovolemic Hypernatremia

HYPERNATREMIA
Hypovolemic HypernatremiaStep 1: Replace ECVStep 2: Replace free water deficit
Hypovolemia

Hypovolemic HypernatremiaSeverity of Hypovolemia
2 Normal Saline Normal Saline
Persistent Hypernatremia
¼ Normal SalineDextrose 5% in Water
SevereMild/Mod

Hypovolemic Hypernatremia
Desired rate of correction of hypernatremia0.5 mEq/L per hour

Replacement of Free Water
Choice of IV FluidsD5W: 100% free water¼NS: 75% free water½NS: 50% free water

Free Water Deficit
Assessment of Free Water deficit
deficit (liters) = (Wt)(%TBW) (Serum Na - 1)140
%TBW: 0.6 l/kg for children, men < 70 yrs%TBW: 0.5 l/kg for men > 70 yrs, females < 70%TBW: 0.45 l/kg for women > 70 yrs

Calculation of Free Water Deficit
Calculate free water deficit for a 75 y/o male (wt: 60 kg) with serum sodium of 160 mEq/l

Calculation of Free Water Deficit
Calculate free water deficit for a 75 y/o male (wt: 60 kg) with serum sodium of 160 mEq/l
deficit (liters) = (Wt)(%TBW) (Serum Na - 1)140
= (60 kg)(0.5)(160 - 1) = 4.3 L140

Replacement of free water deficit
Replacement of free water deficit is based on calculated deficit and free water contentTo replace 4.3 Liters of free water:
4.3 Liters of D5W5.7 Liters of ¼ NS8.6 Liters of ½ NS

Correction of IV FluidIV rate (ml/hr) = (free water deficit)(1000ml/L)
(Serum Na - 140) (% of free water in IVF)(0.5 mEq/l/hr)
Calculate IVF rate for:75 y/o male with weight 70 kg and serum Na of 160 mEq/L
1. Normal saline2. ½ normal saline3. ¼ normal saline4. Dextrose 5% in Water

Correction of IV Fluid
IV rate (ml/hr) = (5.0 L)(1000ml/L) (160 - 140) (% of free water in IVF)(0.5 mEq/l/hr)
Calculate IVF rate for: 75 y/o male with weight 70 kg and serum Na of 160 mEq/L
1. Normal saline (0) rate = XXXXX2. ½ normal saline (0.5) rate = 250 ml/hr3. ¼ normal saline (0.75) rate = 167 ml/hr4. Dextrose 5% in Water (1.0) rate = 125 ml/hr

DISORDERS OF POTASSIUM BALANCEDISORDERS OF POTASSIUM BALANCE

HYPOKALEMIAHYPOKALEMIA
CELLULAR METABOLISM
Em = - 61 log r[K]c + 0.01[Na]cr[K]e + 0.01[Na]e
Distribution of serum potassium

Action Potential

Distribution of potassiumSerum Cell
insulin
insulin
Epi/NE
pH
pH
Sosm
Sosm

Distribution of potassiumSerum Cell
insulin
insulin
Epi/NE
pH
pH
Sosm
Sosm

Etiology of Hypokalemia
Beta agonistIntracellular shift of potassiumTheophyllineIntracellular shift of potassiumInsulinIntracellular shift of potassiumDiuretics (HCTZ, furosemide)enhanced renal excretion

Etiology of Hypokalemia
High dose penicillinEnhanced renal excretionMineralocorticoidsEnhanced renal excretionAminoglycosidesEnhanced renal excretionAmphoterecin-BEnhanced renal excretion

Etiology of Hypokalemia
Cis-Platinumenhanced renal excretionSodium polystyrene sulfonateEnhanced fecal eliminationSorbitolEnhanced fecal eliminationDiarrheaEnhanced fecal elimination

Etiology of Hypokalemia
Vomiting/NG suctionIncreased GI eliminationHypomagnesemiaDecreased intracellular potassiumEnhanced renal eliminationMetabolic alkalosisIntracellular shift of potassium
HYPOKALEMIAHYPOKALEMIA
ETIOLOGYRe-Distribution of potassium
Metabolic AlkalosisInsulin
Decreased intake

HYPOKALEMIAHYPOKALEMIA
ETIOLOGYINCREASED LOSSES
GI lossesSkin lossesRenal Losses
Increased renin activityIncreased mineralocorticoid activity

Transtubular Potassium Gradient
TTKG = [K+] urine / (Uosm/Sosm)[K+] serum
Normal = 6-8

Transtubular potassium Gradient
Sosm
Uosm
KDT
[K+] urine
[K+]

ProminentU Wave
BiphasicT wave
ST depression
Manifestations of Hypokalemia

HYPOKALEMIAHYPOKALEMIA
CLINICAL MANIFESTATIONSCardiovascular
ArrhythmiasOrthostatic hypotension
MuscularWeakness, myalgiasCramps, ParalysisRhabdomyolysis

HYPOKALEMIAHYPOKALEMIA
CLINICAL MANIFESTATIONSMetabolic
Abnormal carbohydrate metabolismHypercalcemiaHypomagnesemiaHyperlipidemiaAchlohydria

HYPOKALEMIAHYPOKALEMIA
CLINICAL MANIFESTATIONSRENAL
Nephrogenic diabetes insipidusNegative nitrogen balancedecreased protein synthesisIncreased ammonia production by kidneys

HYPOKALEMIAHYPOKALEMIA
NON-PHARMACOLOGIC THERAPYHighest content
dried figs, molassesVery High content
dried fruit, nuts, avocados, lima beansHigh Content
vegetables: spinach, tomatoes,carrotsbananas, oranges, mangos, watermelonmeat: beef, pork, lamb, veal

Potassium Supplementation
Why is serum potassium an imprecise measure of total body potassium?
How does this influence your estimate of need for supplementation?

HYPOKALEMIAHYPOKALEMIA
SELECT/RECOMMEND THERAPYTOTAL DOSE REQUIREDESTIMATE for ACUTE Replacement:10 mEq per 0.1 mEq/L rise desired
1 mEq/L requires about 100 mEq K

HYPOKALEMIAHYPOKALEMIA
Choice of salt formPotassium bicarbonate 6.5 mEq, 25 mEq
Potassium chloridecapsulesfor solutionsolutiontablet

Management of Hypokalemia[K+]
3.5-4.0mEq/L
Salt subsitutesDietary sources
3-3.5mEq/L
?Cardiacdisease
none 40-100mEq20 mEq/day
For prevention
2.5-3.0mEq/L
?Symptoms
PO IV
no yes
< 2.5mEq/L
IV
intolerant

HYPOKALEMIAHYPOKALEMIA
SELECT/RECOMMEND THERAPYROUTE/RATE OF ADMINISTRATIONORAL

HYPOKALEMIAHYPOKALEMIA
SELECT/RECOMMEND THERAPYROUTE/RATE OF ADMINISTRATIONORALCHOICE AFFECTED BY SEVERITY AND GI TOLERABILITY20-40 mEq doses at 4 hour intervals PRN

HYPOKALEMIAHYPOKALEMIA
SELECT/RECOMMEND THERAPYROUTE/RATE OF ADMINISTRATIONINTRAVENOUSPREFERRED 10 mEq/HRMAXIMUM 20 mEq/HR WITH EKG MONITOR

HYPOKALEMIAHYPOKALEMIA
ADJUNCTIVE THERAPYTRIAMTERENEAMILORIDESPIRONOLACTONEMAGNESIUM SUPPLEMENTATION
HYPERKALEMIAHYPERKALEMIAETIOLOGY
Increased IntakeRedistribution (ICF to ECF)Decreased urinary excretionrenal failure RTAvolume depletion ACE Inhibitorshypoaldosteronism TMP/SMXK-sparing agentsNSAID’s
Hyperkalemia
Muscle weakness
Cardiac Arrhythmias
HYPERKALEMIAHYPERKALEMIA

Assessment of Hyperkalemia
Assess the patient for symptoms, i.e. EKGConfirm true hyperkalemiaEvaluate for possible reversible causesEvaluate renal functionTranstubular potassium gradient (TTKG)Fractional excretion of potassium (FeK)

Transtubular potassium Gradientin Hyperkalemia
Sosm
Uosm
KDT
[K+] urine
[K+]
Low-hypoaldosteronsim
High-renal failure

Hyperkalemia
Hyperkalemia
Mild
Monitor Na PolystyreneSulfonate
Moderate Severe
IV CalciumIV NaHCO3IV insulin/dextrose
Hemodialysis

HYPERKALEMIAHYPERKALEMIA
THERAPY FOR MILD HYPERKALEMIANo therapyIdentify reversible causesDietary potassium restrictionDiuretics

Hyperkalemia
Sodium polystyrene sulfonateA non-absorbable ion-exchange resin which binds potassium in the GI tract to enhance excretion of potassiumOnset: 2-3 hoursDose: 25-50 g PO or PR prn

Management of HyperkalemiaAbnormal EKG? IV Calcium
Continuous EKG monitoring
Hyperglycemia? IV insulin° BS
IV insulin + dextrose
Consider albuterol or NaHCO3
Sodium polystyrene sulfonate or Dialysis
Monitor [K] q 2 hrs until < 5.5 mEq/L
yesno
yesno

HYPERKALEMIAHYPERKALEMIACalciumRaises the threshold potential (less negative) and restores cardiac excitability
HYPERKALEMIAHYPERKALEMIA
CalciumOnset: 1-2 minutesDuration: 10-30 minutesDose: CaGluc 1 gm (4.7 mEq) IV over 5 mins

HYPERKALEMIAHYPERKALEMIA
Insulin/glucoseStimulates cellular uptake of potassium, redistributing total body stores of potassiumOnset: 30 minutesDuration: 2-6 hoursDose: D50W 50 ml (25 g) IV over 5 min with
10 units of regular insulin IV/SQOr D10W with 25-50 units insulin/L at 100-500 ml/hr

HYPERKALEMIAHYPERKALEMIA
Sodium BicarbonateIncreases serum pH and stimulates redistribution of potassium intracellularlyOnset: 30 minutesDuration: 2-6 hoursDose: 50-100 mEq IV over 2-5 minutes

Hyperkalemia
AlbuterolBeta stimulation promotes intracellular distribution of potassiumOnset: 30 minutesDuration: 1-2 hoursDose: 10-20 mg via nebulizer over 10 mins

Hyperkalemia
HemodialysisIncreases potassium eliminationOnset of effect: immediateDuration of dialysis: variable (2-4 hrs)

MAGNESIUM BALANCEMAGNESIUM BALANCE
Jack Burke, Pharm.D.

HYPOMAGNESEMIAHYPOMAGNESEMIA
MAGNESIUM PHYSIOLOGY
MAGNESIUM IS AN Intra-CELLULARCATION AND ONLY 1% IS PRESENT EXTRACELLULARLY.

HYPOMAGNESEMIAHYPOMAGNESEMIA
EtiologyCommon disordersGastrointestinalRenalInternal redistributionMiscellaneousDrugs

HYPOMAGNESEMIAHYPOMAGNESEMIA
DRUG-INDUCED CAUSESAminoglycosides (gentamicin, etc)Amphoterecin BCyclosporineDiureticsdigoxinCis-Platinumethanol

HypomagnesemiaDescribe the mechanism responsible for hypomagnesemia:Prolonged NG suctionPancreatic insufficiencyRenal tubular acidosisCis-platinHyperaldosteronismNephrotic syndromeDiureticsGlucose, insulin, AA admin
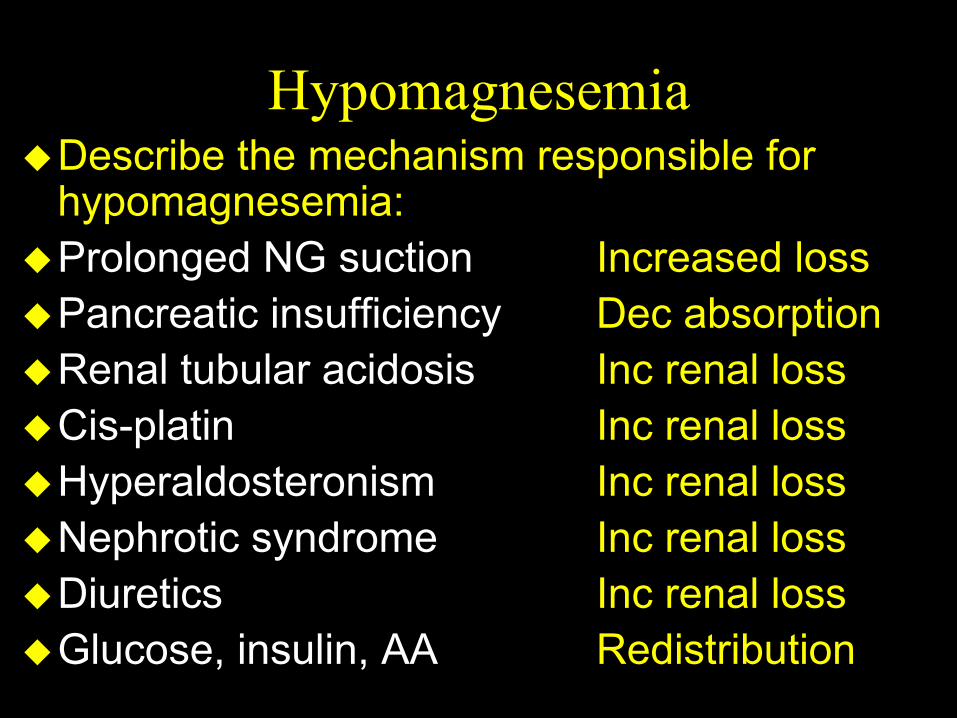
HypomagnesemiaDescribe the mechanism responsible for hypomagnesemia:Prolonged NG suction Increased lossPancreatic insufficiency Dec absorptionRenal tubular acidosis Inc renal lossCis-platin Inc renal lossHyperaldosteronism Inc renal lossNephrotic syndrome Inc renal lossDiuretics Inc renal lossGlucose, insulin, AA Redistribution

HYPOMAGNESEMIAHYPOMAGNESEMIA
CLINICAL MANIFESTATIONSNEUROMUSCULAR
Muscle Twitching TremorHyper-reflexia ParesthesiasTetany SeizuresComa NystagmusAtaxia Vertigo

HYPOMAGNESEMIAHYPOMAGNESEMIA
CLINICAL MANIFESTATIONSPychiatric
ApathyDepressionDeliriumAgitationConfusionHallucinations

HYPOMAGNESEMIAHYPOMAGNESEMIA
CLINICAL MANIFESTATIONSCardiac
PVC’s, V.Fib V.TachTorsade de PointesPredisposition to digoxin toxicityEKG : PR, QT prolongation,
wide QRSCoronary Spasm

HYPOMAGNESEMIAHYPOMAGNESEMIA
CLINICAL MANIFESTATIONSRefractory hypocalcemiaRefractory hypokalemia
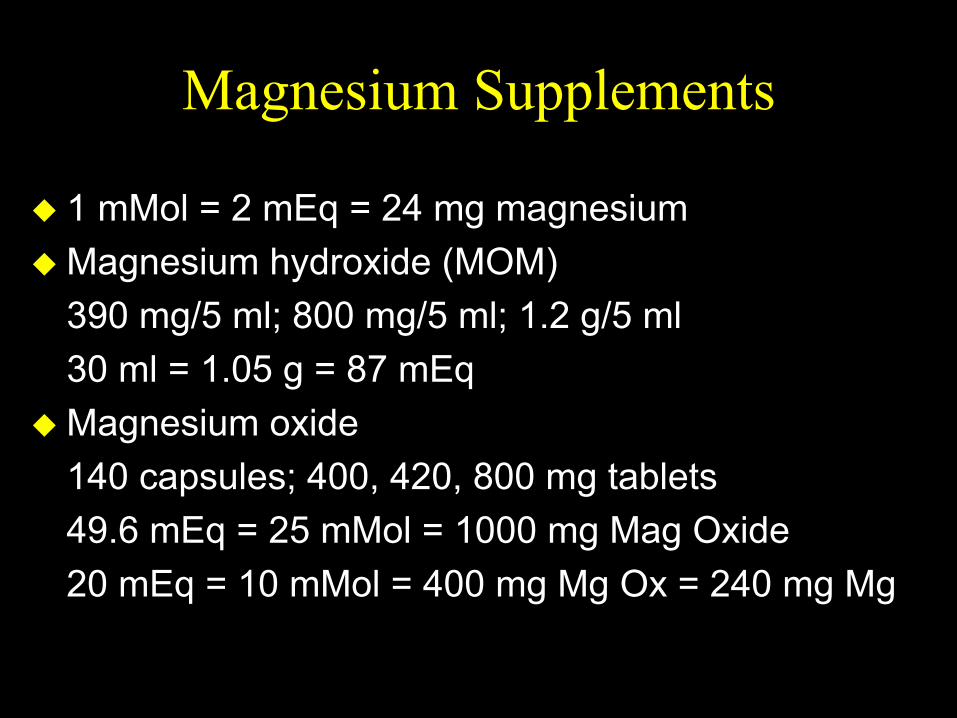
Magnesium Supplements
1 mMol = 2 mEq = 24 mg magnesiumMagnesium hydroxide (MOM)390 mg/5 ml; 800 mg/5 ml; 1.2 g/5 ml30 ml = 1.05 g = 87 mEqMagnesium oxide 140 capsules; 400, 420, 800 mg tablets49.6 mEq = 25 mMol = 1000 mg Mag Oxide20 mEq = 10 mMol = 400 mg Mg Ox = 240 mg Mg

HYPOMAGNESEMIAHYPOMAGNESEMIA
SERUM Mg CONCENTRATION
< 1 mEq/L 1-1.5 mEq/L + aSx
Life-threatening Sx?
MgSO4 2 gm1 mEq/kg/day
1 mEq/kg IV0.5 mEq/kg
yes no
MOM 5 ml QIDMOM 5 ml QIDMgOxide MgOxide 400 mg BID400 mg BID--QIDQID

HYPERMAGNESEMIAHYPERMAGNESEMIA
EtiologyDecreased renal excretion
Acute/chronic renal failureExcessive intake
CatharticsTreatment of toxemia of pregnancy
MiscellaneousLithium hypothyroidismMilk-Alkali Syn Addison’s diseaseViral hepatitis Acute DKA

HYPERMAGNESEMIAHYPERMAGNESEMIA
CLINICAL MANIFESTATIONS> 3 mEq/L hypotension, vasodilation> 4 QT prolongation> 4.5 bradycardia, heart blocks> 5 QRS prolongation, sedation> 7 somnolence, decreased reflexes> 10 coma, respiratory depression> 14 complete heart block>15 asystole

HYPERMAGNESEMIAHYPERMAGNESEMIA
Which patients should be treated?Severely elevated concentrations
Significant neuromuscular or cardiovascular symptoms

Hypermagnesemia
Acute treatmentElemental Ca 100-200 mg IV
Calcium Gluconate 90 mg (4.5 mEq) per gCalcium chloride 270 mg (13.5 mEq) per g
Onset: immediateDuration: transient (1-2 hrs)

CALCIUM BALANCECALCIUM BALANCE
Normal calcium: 8.5-10.5 mg/dl
Calcium Balance
Ca++
Ca++- Albumin
MeasuredIn Serum
(active)

Calcium Balance
correction for hypoalbuminemiaFor every 1 g/dl albumin falls below 4 g/dl
add 0.8 g/dl to the measured CalciumExample
Serum Calcium 7.0 mg/dl Serum Albumin 2 g/dl
What is the corrected calcium concentration?