Embed Size (px)
Citation preview

Fluid and Electrolyte Balance during Injury
Zohair Al Aseri. MD. FCEM(UK).FRCPC (EM&CCM)
Chairman ,National Emergency Medicine Committee
Coordinatoor MPH-DME Master
Consultant, ICU Department of Critical Care
Chairman, Department of Emergency Medicine
College of Medicine, King Saud University Medical City.
Riyadh, KSA.
http://fac.ksu.edu.sa/zalaseri

Fluid and Electrolyte Balance during Injury
Objectives Understand normal regulation of fluid balance Fluid Imbalance In Shock State Fluid Therapy (Types) & Indication Electrolyte disturbances in trauma and surgery Acid base in surgery patients

Case 1
39 year old male involved in MVC brought to ED by EMT, he is unconscious, heart rate 120 beat per minute blood pressure of 80/50, intubated in the scene, what is your immediate action
a)Take further history
b)Start him on dextrose 5% with NS
c)Start him in colloid
d)Start him in Normal saline

Case2
A recovery nurse calling you to see a 70 year old male, 7 hours post appendicictomy, because he is drowsy and unresponsive, his vital signs are normal and oxygen saturation 92% on room air? What is the most likely diagnosis?
a)Intracranial bleeding
b)Stroke
c)Acute renal failure
d)Respiratory failure

Case3
70 year old male, admitted for elective hernia repair, kept NPO and started in D5 ½ normal saline 24 hour ago, his current electrolyte showed k of 5 mmol and Na of 128 mmol What is the most likely diagnosis?
a)DI
b)SAIDH
c)Acute renal failure
d)Iatrogenic hyponatremia

HypovolaemiaReduced circulating volume
CausesLoss of blood, electrolyte-containing fluid or water.Third-space loss due to increased vascular permeability.
Fluid and Electrolyte Balance during Injury

Hypovoluemia will reduce oxygen and nutrient delivery
Leads to
increase healing and recovery times.

Fluid-conserving measures
Oliguria and sodium and water retention
Due to the release ADH and aldosterone after major surgery or injury
May persist even after normal circulating volume has been restored.
Fluid and Electrolyte Balance during Injury

Fluid-conserving measures:Increased ADH Secretion from the posterior pituitary is response to Afferent nerve impulses from the site of injury Atrial stretch receptors (responding to reduced volume) & aortic and carotid baroreceptors (responding to reduced pressure)Increased plasma osmolality (principally the result of an increase in sodium ions) detected by hypothalamic osmoreceptors.Input from higher centres in the brain (responding to pain, emotion and anxiety).
Fluid and Electrolyte Balance during Injury

Fluid-conserving measures:ADH promotes retention of free water (without electrolytes) by cells of the distal renal tubules and collecting ducts.
Fluid and Electrolyte Balance during Injury

Aldosterone secretion from the adrenal cortex is increased by: Activation of the renin-angiotensin system. Renin is released from afferent arteriolar cells in the kidney in response to reduced blood pressure and activation of the renal sympathetic nerves.
Fluid and Electrolyte Balance during Injury

Aldosterone secretion from the adrenal cortex is increased by:
Renin converts circulating angiotensinogen to angiotensin AT-1.AT-1 is converted by angiotsion converting enzyme (ACE) in plasma and tissues (particularly the lung) to AT-2 which cause arteriolar vasoconstriction and aldosterone secretion
Fluid and Electrolyte Balance during Injury

Adrenocorticotropic hormone (ACTH) Increased by the anterior pituitary in response to hypovolaemia and hypotension via afferent nerve impulses from stretch receptors in the atria, aorta and carotid arteries. lt is also raised by ADH.Direct stimulation of the adrenal cortex by hyponatraemia or hyperkalaemia.
Fluid and Electrolyte Balance during Injury

Aldosterone increases the reabsorption of both sodium
and water by distal renal tubular
+ simul taneous excretion of hydrogen and
potassium ions into the urine.
Fluid and Electrolyte Balance during Injury

Duration of increased ADH and aldosterone secretion following injury? Usually lasts 48-72 hours during which time urine volume is reduced and osmolality increased.
Fluid and Electrolyte Balance during Injury

Urinary sodium excretion decreases to 10-20 mmol /24hrs (normal 50-80mmol /24 hrs)
Urinary potassium excretion increases to > 100 mmol/24 hrs (normal 50-80mmol /24 hrs).
Fluid and Electrolyte Balance during Injury

Blood flow-conserving measures:Hypovolaemia
Reduces cardiac preload which leads to a fall in cardiac output.
Increased sympathetic activity results in a compensatory increase in cardiac output, peripheral vaso constriction and a rise in blood pressure.
Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury
FLUID AND ELECTROLYTE BALANCE:
May be altered in the surgical patient for several reasons:ADH and aldosterone secretion as described above.Loss from the GI tract (e.g. bowel preparation, ileus, stomas, fistulae).Reduced oral fluid intake in the perioperative period

Fluid and Electrolyte Balance during Injury
FLUID AND ELECTROLYTE BALANCE:Insensible losses (e.g. sweating secondary to fever).Third space losses.Surgical drains.Medications (e.g. diuretics).Underlying chronic illness (e.g. cardiac failure, portal hypertension).

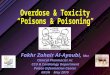
Normal water and electrolyte balance:Water forms about 60% of total body weight in men and 55% in women. Approximately two-thirds is intracellular, one-third extracellular. Extracellular water is distributed between the plasma and the interstitial space
Fluid and Electrolyte Balance during Injury

Regulation of Fluid Balance
TOTAL BODY FLUID(40) liters;60%TBW
Red cell volume(2 liters)
Plasma volume(3 liters,5 %)
Extracellular(15 liters,20%)
Blood volume (5 liters)
Intracellular(25 liters,40%)
The intracellular and The intracellular and extracellular compartments extracellular compartments
are separated by are separated by water-permeable water-permeable cell membranes.cell membranes.

IC. WATER ECF2/3 intrest. 1/3 blood
25 150 15 0.01 2 6 50
Na K Mg Ca Cl Hco3 Phos
140 4.5 1.2 2.4 100 25 1.2
Fluid & Electrolyte Balance

Regulation of Fluid Balance
ECC OsmolarityECC OsmolarityECF VolumeECF Volume
Prevent swelling or Prevent swelling or shrinking of the cellsshrinking of the cells
Maintain BPMaintain BP

Osmolality of extracellular fluid normally 275-295 mOsmol/kg determined primarily by sodium and chloride ion concentrations.
Fluid and Electrolyte Balance during Injury

Normal water and electrolyte balance:
Plasma oncotic pressure is primarily determined by albumin.
Fluid and Electrolyte Balance during Injury

Normal water and electrolyte balance:
In adults, Normal daily fluid requirement is 30-35ml / kg (-2500 ml /day).
In newborn babies and chil dren Contain proportionately more water than adults.Daily maintenance fluid requirement at birth is about 75ml/ kg, increasing to 150 ml/ kg during the first weeks of life.
Fluid and Electrolyte Balance during Injury

Normal water and electrolyte balance:After first month of life, fluid requirements decrease and the '4/2/1' formula can be used to estimate maintenance fluid requirements: first l0 kg of body weight requires 4ml /kg/h; the next 10kg 2ml /kg/ h; thereafter each kg of body requires 1ml/kg/h.
Fluid and Electrolyte Balance during Injury

The estimated maintenance fluid requirements of a 35 kg child would therefore be:(10 X 4) + (10 X 2) + (15 X 1) = 75 mljh.150 .
The daily requirement for both sodium and potassium in children is about 2-3mmol/kg.
Fluid and Electrolyte Balance during Injury

Assessing losses in the surgical patient:
Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury
Assessing losses in the surgical patient:
Normal Daily Losses and requirements for Fluid and Electrolytes
Volume (ml)
Na+ (mmol) K+ (mmol)
Urine 2000 80 60Insensible losses from skin and respiratory tract
700 - -
Faeces 300 - 10Less water created from metabolism
300 - -
Total 2700 80 70

Typical Losses per
24hrsFactors Modifying Volume
Insensible Losses
700-2000mlLosses associated with pyrexia,
sweating and use of non-humidified
Urine1000-
2500ml With aldosterone and DH secretion; With diuretic Therapy
Gut 300-1000ml Losses with obstruction, ileus, fistulae and diarrhea (may increase substantially)
Third spaces Losses
0-4000mlLosses with greater extent of surgery and tissue trauma
Fluid and Electrolyte Balance during Injury
Source of Fluid Loss in Surgical Patients

Insensible fluid losses:Hyperventilation increases insensible water loss is not usually large unless the normal mechanisms for humidifying inhaled air (the nasal passages and upper airways) are compromised.
this occurs in intubated patients or in those receiving non humidified high-flow oxygen. In these situations inspired gases should be humidified routinely.
Fluid and Electrolyte Balance during Injury

Insensible fluid losses:Pyrexia 200ml/day for each 1°C rise in temperature.
Sweating May increase fluid loss by up to 1 litre/hourSweat also contains significant amounts of sodium (20-70mmol/l) and potassium (10mmol/l).
Fluid and Electrolyte Balance during Injury

The effect of surgery:
The stress responseADH leads to water retention and a reduction in urine volume for 2-3days following major surgery.
Aldosterone conserves both sodium and water, further contributing to oliguria.
Urinary sodium excretion falls while urinary potassium excretion increases, predisposing to hypokalaemia.
Fluid and Electrolyte Balance during Injury

'Third-space' losses:if tissue injury is severe, widespread and/or prolonged then the loss of water, electrolytes and colloid particles into the interstitial space can amount to many litres and can significantly decrease circulating blood volume following trauma and surgery.
Fluid and Electrolyte Balance during Injury

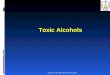
Regulation of Fluid BalanceRegulation of Fluid Balance
Q=K[(Pc-Pi)-@(Oc-Oi)]Q=K[(Pc-Pi)-@(Oc-Oi)]
17Mm Hg
Oncotic P=25
37mm Hg
VenuleArteriole
Pnet =(37-1)+(0-25)=11
InterstitialHydrostatic P=1 Pnet =(17-1)+(0-25)=-9

'Third-space' losses:Colloid oncotic pressure throughout the lumen of the capillary is 25mmHg. The hydrostatic pressure is 1 mmHg in the interstitium.Hydrostatic pressure on the arteriolar side of the capillary falls from 37 mmHg to 17 mmHg on the venular side.net outward pressure on the arteriolar side (37 - 1 - 25 = 11)net inward pressure (25 -17-1= 9) on the venular side.
Fluid and Electrolyte Balance during Injury

Hydrostatic Hydrostatic pressurepressure
Oncotic Oncotic pressurepressure
tending to move fluid tending to move fluid out of the capillariesout of the capillaries
tending to keep fluid tending to keep fluid within the capillarieswithin the capillaries
THE STARLING EQUATION
Excess fluid filtered is collected through the lymphatic circulation and returned to the Systemic circulation
Regulation of Fluid Balance

Third-space' losses:Oedema is formed if
hydrostatic pressure increases on the venu lar side as in heart failure or
colloid oncotic pressure falls due to liver or kidney disease or
permeability is increased as in sepsis and /or injury.
Fluid and Electrolyte Balance during Injury

Loss from the gastrointestinal tractThe magnitude and content of fluid losses depends on the site of loss or lntestinal obstruction.
ln general, the higher an obstruction occurs in the intestine, the greater the fluid loss
Fluid and Electrolyte Balance during Injury

Volume Na+ K+ Cl- HCO3Plasma - 140 5 100 25Gastric Secretions
2500 50 10 80 40
Intestinal Fluid (Upper)
3000 140 10 100 25
Bile and Pancreatic secretions
1500 140 5 80 60
Mature ileostomy 500 50 5 20 25Diarrhoea (Inflammatory)
- 110 40 100 40
Mixed Gastric Aspirate
- 120 10 - -
The approximate daily volumes (ml) and electrolyte concentrations (mmol/l) of various gastrointestinal fluids.

Loss from the gastrointestinal tractParalytic ileus.Propulsion in the small intestine ceases, has numerous causes.
Resolves within 1-2days of the operation.
Fluid and Electrolyte Balance during Injury

Loss from the gastrointestinal tract:
Intestinal fistulaassociated with the greatest fluid and electrolyte losses.
Fluid and Electrolyte Balance during Injury

Loss from the gastrointestinal tract:
Diarrhoea. Patients may present with diarrhoea or develop it during the perioperative period. Fluid and electrolyte losses may be considerable.
Fluid and Electrolyte Balance during Injury

Intravenous fluid administration:
When choosing and administering intravenous fluids it is important to consider:
what fluid deficiencies are present. fluid compartments requiring replacement. electrolyte disturbances present . which fluid is most appropriate.
Fluid and Electrolyte Balance during Injury

Types of intravenous fluid:
Dextrose After the IV administration of 1000 ml 5% dextrose solution, about 670ml of water will be added to the lFC and about 330 ml of water to the EFC, of which about 70ml will be intravascular.
thereforeDextrose solutions are of little value as resuscitation fluids to expand intravascular volume
Fluid and Electrolyte Balance during Injury


CrystalloidsSodium chloride 0.9%(NS) and Hartmann' s solution (Ringer) are isotonic solutions Sodium chloride NS 0.9 contains 9g of sodium chloride dissolved in l000ml of water.(Ringer's lactate) has a more composition, containing lactate, potassium and calcium addition to sodium and chloride ions.
Fluid and Electrolyte Balance during Injury

Crystalloids
Both normal saline and Ringer solution have an osmolality similar to extracellular fluid (about 300m0sm/l)
distribute rapidly to ECF compartment after venous administration .
Fluid and Electrolyte Balance during Injury

One liter of isotonic saline contains 154 meq of sodium and an equivalent number of chloride ions.
Fluid and Electrolyte Balance during Injury

Balanced solutions, such as Ringer's lactate closely match the composition of extracellular
fluid by providing physiological concentrations of sodium and lactate in place of bicarbonate.
After administration the lactate is metabolized, resulting in bicarbonate generation.
Fluid and Electrolyte Balance during Injury

Balanced solutions, such as Ringer's lactate Decrease the risk of hyperchloraermia,
which can occur following large volumes of fluids NS.
Fluid and Electrolyte Balance during Injury

Hypertonic saline solutionsInduce a shift of fluid from the IFC to the EFCReducing brain water and increasing intra vascular volume and serum sodium concentration.
Potential indications cerebral oedema raised intracranial pressure hyponatraemic seizures 'small volume' resuscitation of hypovolaemic shock.
Fluid and Electrolyte Balance during Injury

Dextrose saline solutionsCommercially available 5% dextrose with 0.9% normal saline is a hypertonic solution (twice the osmolarity of plasma) and should be used with caution.
Fluid and Electrolyte Balance during Injury

Colloids:albumin or be synthetically modified (e.g. gelatins, hydroxyethyl starches [HES], dextrans).
When administered, colloid remains largely within the intravascular space until the colloid particles are removed by the reticuloendothelial system.
Fluid and Electrolyte Balance during Injury

Colloids:The intravascular half-life is usually between 6 and 24 hours and such solutions are therefore appropriate for fluid resuscitation.
Electrolyte-containing solution distributes throughout the EFC.
But No Evidence
Fluid and Electrolyte Balance during Injury

Colloids:Synthetic colloids are more expensive than crystalloids and have variable side effect profiles.
Recognized risks Coagulopathy Reticuloendothelial system dysfunc tion Pruritus and anaphylactic reactions Renal failure when used for resuscitation in
patients with septic shock.
Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury

Maintenance fluid requirementsunder normal conditions, adult daily sodium requirements (80mmol) may be provided by the administration of 500-1000ml of 0.9% sodium chloride. The remaining requirement to maintain fluid balance (2000-2500ml).., typically provided as 5% dextrose.
Fluid and Electrolyte Balance during Injury

Maintenance fluid requirementsDaily potassium requirements (60-80mmol) are usually met by adding potassium chloride to maintenance fluids, but the amount added can be titrated to measured plasma concentrations.
“potassium should not be administered at a rate greater than 10-20 mmol/h except in severe potassium deficiency.
Fluid and Electrolyte Balance during Injury

Maintenance fluid requirement:The provision of total parenteral nutrition should also be considered in this situation.
Fluid and Electrolyte Balance during Injury

Treatment of postoperative hypovolaemia and/or hypotension:Hpovolaemia is common in the postoperative period and may present with one or more of the following: tachycardia, pallor, clammy skin, collapsed peripheral pulsesoliguria and / or hypotension.
Fluid and Electrolyte Balance during Injury

Treatment of postoperative hypovolaemia and/or hypotension:Intravascular volume should be rapidly restored with a series of fluid boluses (e.g. 250-500 ml) with the clinical response being assessed after each bolus.
Fluid and Electrolyte Balance during Injury

Crystalloids Versus ColloidsCrystalloids Versus Colloids
Crystalloids or colloids in fluid therapy?? Crystalloids or colloids in fluid therapy??

Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury

Water depletionPure water depletion is common in surgical practice, and is usually combined with sodium loss.The most frequent causes are inadequate intake or excessive gastrointestinal losses.
Fluid and Electrolyte Balance during Injury

Water excess
common in patients who receive large volumes of intravenous 5% dextrose in the early postoperative period.
Such patients have an increased extracellular volume and are commonly hyponatraemic.
Fluid and Electrolyte Balance during Injury

Water Excess:
Difficult to detect clinically Patients with water excess usually remain well Oedema may not be evident until the extracellular volume has increased by more than 4 litres.
Fluid and Electrolyte Balance during Injury

Hypernatraemia:
Normal sodium levels are in range 136-144mmol/l.
Hypernatraemia (>145mmol) results from either water or hypotonic fluid loss or sodium gain.
Fluid and Electrolyte Balance during Injury

Hypernatraemia:
Water loss is commonly caused by reduced water intakevomiting, diarrheadiuresis, burnssweating and insensible losses from the respiratory tract diabetes insipidus.
Fluid and Electrolyte Balance during Injury
Typically associated with hypovolaemia

Hypernatraemia:
Sodium gain is usually caused by excess sodium administration in hypertonic intravenous fluids
Typically associated with hypervolaemia.
Fluid and Electrolyte Balance during Injury

Hypovolaemic Hypernatraemia
is treated with isotonic crystalloid
followed by the more gradual administration of water to correct the relative water deficit.
We can use 5%dextrose,1/2 NS or 1/4 NS
Fluid and Electrolyte Balance during Injury

Cells, particularly brain cells, adapt to a high sodium concentration in extracellular fluid, and once this adaptation has occurred, rapid correction of severe hypernatraemia can result in a rapid rise in intracellular volume, cerebral oedema, seizures and permanent neurological injury.
Fluid and Electrolyte Balance during Injury

Hyponatraemia
(Na- < 135mmolfl) can occur with high, low or normal extracellular volume.
The commonest cause is the administration of hypotonic intravenous fluids (as intravenous 5% dextrose) is administered in the postoperative period (dilutional hyponatraemia).
Fluid and Electrolyte Balance during Injury

Hyponatraemia
Other causes include diuretic use and (SIADH)
Co-morbidities associated with secondary hyperaldosteronism, such as cirrhosis and congestive cardiac failure.
Fluid and Electrolyte Balance during Injury

Sodium deficit
This can be calculated as follows:
140- measured sodium x 0.2 x weight in kg
where 0.2 refers to the 20% extracellular space which represents the compartment in which sodium is the main cation.
Fluid and Electrolyte Balance during Injury

Hyponatraemia
Treatment depends on correct identification of the cause:
If ECF volume is normal or increased, the most likely cause is excessive intravenous water administration and this will correct spontaneously if water intake is reduced.
Fluid and Electrolyte Balance during Injury

Hyponatraemia
Although less common in surgical patients,
SIADH promotes the renal tubular reabsorption of water independently of sodium concentration, resulting in inappropriately concentrated urine (osmolality> 100m0sm / l) in the face of hypotonic plasma (osmolality< 290m0sm/ l).
Fluid and Electrolyte Balance during Injury

Hyponatraemia
The urine osmolality helps to distinguish inappropriate ADH secretion from excessive water administration.
'Spot‘ measurement of urine sodium will be high.
Fluid and Electrolyte Balance during Injury

Hyponatraemia
In patients with decreased ECF volume,
hyponatracmia usually indicates combined water and sodium deficiency.
This is most frequently the result of DiuresisDiarrheaAdrenal insufficiency
Treatment by 0.9 sodium chloride
Fluid and Electrolyte Balance during Injury

Hyponatraemia
severe hyponatraemia (< 120mmol/ l) associated with confusion, seizures and coma.
Fluid and Electrolyte Balance during Injury

Hyponatraemia
Rapid correction of sodium concentration can precipitate an irreversible demyelinating condition known as central pontine myelinolysis
Sodium concentration should not increase by more than 0.5 mmol/h.
Fluid and Electrolyte Balance during Injury

Hyponatraemia
This can usually be achieved by the cautious administration of isotonic (0.9%) sodium chloride, occasionally combined with the use of a loop diuretic (e.g. furosemide).
Hypertonic saline solutions only for sever hyponatremia with CNS manifestation like seizure
Fluid and Electrolyte Balance during Injury


Potassium
98% of total body potassium (around 3500mmol) is intracellular
serum potassium concentration (normally 3.5-5 mmol/ l) is a poor indicator of total body potassium.
Fluid and Electrolyte Balance during Injury

Potassium
no absolute formula to determine K deficit.
When the serum K is < 2.5mmol/ l about 100-200mmol of KCL will be needed in a 70kg adult.
Serial monitoring of serum K is necessary to prevent overcorrection
Fluid and Electrolyte Balance during Injury

Potassium
Once the serum K comes above
3.0 mmol /1, K supplements can be reduced.
Acidosis reduces Na+/kATpase activity and results in a net efflux of potassium from cells and hyperkalaemia.
Conversely, alkalosis results in an influx of potassium into cells and hypokalaemia.
Fluid and Electrolyte Balance during Injury

Hyperkalaemia
This is a potentially life-threatening condition.
caused by exogenous administration of K release of K from cells (transcellular shift) as a result of tissue damage or changes in the Na / K-ATPase function impaired renal excretion.
Fluid and Electrolyte Balance during Injury

Hyperkalaemia
Mild hyperkalaemia (K" < 6mmol/l) is often asymptomatic.
High K cause progressive slowing of electrical conduction in the heart and the development of significant cardiac arrhythmias.
So ECG is mandatory in all suspected hyperkalaemia
Fluid and Electrolyte Balance during Injury

Hyperkalaemia
ECG FindingTall 'tented' T-waves in the precordial leads are the earliest flattening (or loss) of the P wavesprolonged PR intervalwidening of the QRS asystole.
Fluid and Electrolyte Balance during Injury



Hyperkalaemia
Severe hyperkalaemia (K > 7m mmol/l) requires immediate treatment
Fluid and Electrolyte Balance during Injury

Treatment of hyperkalaemia

Hypokalaemia
common in surgical patients.
Dietary intake of k is normally 60-80 mmol / day.
Under normal conditions, the majority of k loss (> 85%) is via the kidneys
Maintenance of K balance largely depends on normal renal tubular regulation.
Fluid and Electrolyte Balance during Injury

Hypokalaemia
K excretion is increased by Metabolic alkalosisDiuresisIncreased aldosterone release Increased losses from the GI tract.
Fluid and Electrolyte Balance during Injury

Hypokalaemia
Diagnostic features
Muscle weaknessParalytic ileusFlattening of T waves Prominent u waves
Fluid and Electrolyte Balance during Injury


Hypokalaemia
For every 3 K ions that come out from the intracellular compartment, one H and two Na ions are exchanged causing extracellular alkalosis and intracellular acidosis.
Fluid and Electrolyte Balance during Injury

Hypokalaemia
Treatment
Oral or NG potassium replacement in mild hypokalaemia.
Severe (K" < 2.5 mmol/1) or symptomatic hypokalaemia requires IV replacement.
Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury

Calcium
Clinically significant abnormalities in endocrine surgery.
Fluid and Electrolyte Balance during Injury

Magnesium
Hypomagnesaemia is common in
restricted oral intake intra venous fluids for several days
Fluid and Electrolyte Balance during Injury

Magnesium
It is frequently associated with other electrolyte abnormalities, notably hypokalaemia,
hypocalcaemia and hypophosphataemia.
Fluid and Electrolyte Balance during Injury

Hypomagnesaemia
associated with arrhythmias (most notably torsades de pointes (polymorphic ventricular tachycardia) and atrial fibrillation)
Manifestations of are nonspecific
(muscle weakness, muscle cramps, altered mentation, tremors, hyperreflexia and generalized seizures).
Fluid and Electrolyte Balance during Injury

When hypokalaemia and hypomagnesaemia coexist it may be difficult to correct the former without correcting the latter.
Fluid and Electrolyte Balance during Injury
Hypomagnesaemia

Phosphate
Phosphate is a critical component in many biochemical processes such as ATP synthesis, cell signaling and nucleic acid synthesis.
Fluid and Electrolyte Balance during Injury

Hypophosphataemia
common in surgical patients
Severe (< 0.4 mmol/1) causes widespread cell dysfunction, muscle weakness, impaired myocardial contractility, reduced cardiac outputaltered sensorium.
Fluid and Electrolyte Balance during Injury

Hypophosphataemia
most commonly occurs in malnourished and/ or alcoholic patients commencing enteral or parenteral nutrition.
Sepsis is another situation in which marked hypophosphataemia can be seen
Fluid and Electrolyte Balance during Injury

Hypophosphataemia
refeeding syndrome
Hypophosphataemia accompanied by fluid retention and an increase in ECF volume
To avoid it
feeding should be established gradually with measurement and supplementation of serum electrolytes (phosphate, magnesium and potassium).
Fluid and Electrolyte Balance during Injury

Hypophosphataemia
Treatment
Phosphate can be supplemented orally or by slow intravenous infusion.
Fluid and Electrolyte Balance during Injury

Acid-base balance
Acidosis ('acidaemia' if plasma pH< 7.35)
Alkalosis ('alkalaemia' if plasma pH> 7.45).
Both acidosis and alkalosis may be respiratory or metabolic in origin.
Fluid and Electrolyte Balance during Injury

Acid-base balance
VBG is good,
ABG is more accurate
coupled with measurement of blood lactate concentration
Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury

Acid-base balance
Acid-base abnormalities are tackled by the body by means of blood buffersrespiratory systemkidneys.
Fluid and Electrolyte Balance during Injury

Acid-base balance
When the cause is metabolic, respiratory compensation is the most rapid (minutes) followed by the buffering systems hours) and kidneys (days).
Fluid and Electrolyte Balance during Injury

Acid-base balance
Bicarbonate buffer is the most important in the blood (65%) followed by the protein buffers (30%).
Fluid and Electrolyte Balance during Injury

Acid-base balance
Bicarbonate buffer (buffer is an acid-base combination where the acid is only partially dissociated) moves from left to right or vice versa depending on the addition of or loss of acid load with an aim to keep the HCO3/ H2CO3 ratio at 20:1.
Fluid and Electrolyte Balance during Injury

Metabolic acidosis
increase in plasma hydrogen ions in conjunction with a decrease in bicarbonate concentration.
A rise in plasma hydrogen ion concentratlon stimulates chemoreceptors in the medulla resulting in a compensatory respiratory alkalosis an increase in minute volume and a fall in PaCO2
Fluid and Electrolyte Balance during Injury

Metabolic acidosis
Causes
Endogenous acid (e.g. lactic acid or ketone bodies) referred to as 'increased anion gap acidosis' or
Increased loss of bicarbonate (e.g. intestinal fistula, hyperchloraemic acidosis) which leads to 'normal anion gap acidosis'.
Fluid and Electrolyte Balance during Injury

Metabolic acidosis
Anion gap 12-l5mmol/l.
Na - (Cl + HCO3)
Fluid and Electrolyte Balance during Injury

Metabolic acidosis
In surgery or trauma lactic acidosis is the communist cause
Fluid and Electrolyte Balance during Injury

Metabolic acidosis
Base deficit is a measure of the amount of bicarbonate required to correct acidosis and is calculated as follows:
Base deficit=
normal bicarbonate- measured bicarbonate x0.2 x weight in kg.
where 0.2 refers to the extracellular compartment.
Fluid and Electrolyte Balance during Injury

Metabolic acidosis
Treatment is directed towards restoring circulating blood volume and tissue perfusion.
Blood gas analysis should be repeated every 4-6 hours to assess the requirement for further corrections
Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury

Metabolic alkalosis
A decrease in plasma hydrogen ion concentration and an increase in bicarbonate concentration.
A rise in PaCO2 occurs as a consequence of the rise in bicarbonate concentration, resulting in a compensatory respiratory acidosis.
Fluid and Electrolyte Balance during Injury

Metabolic alkalosis in surgery
Mainly due to
hypokalaemia and hypochloraemia.
The kidney has an enormous capacity to generate bicarbonate ions and this is stimulated by chloride loss.
Fluid and Electrolyte Balance during Injury

Metabolic alkalosis
Example
Metabolic alkalosis seen following significant (chloride-rich) losses from the GI tract when combined with loss of acid from conditions such as gastric outlet obstruction.
Fluid and Electrolyte Balance during Injury

Metabolic alkalosis
Treatment
Adequate fluid replacementCorrection of electrolyte disturbances, notably hypokalaemia and hypochloraemiaTreatment of the primary cause.
Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury

Respiratory acidosis
common postoperative problem
Increased PC02 and plasma bicarbonate concentrations.
Hypoventilation
Fluid and Electrolyte Balance during Injury
Examplesgeneral anaesthesiaexcessive opiate administration

Respiratory acidosis
Hypoventilation respiratory acidosis require ventilatory support
Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury

Respiratory alkalosis
Respiratory alkalosis is caused by excessive excretion of CO2 as a result of hyperventilation.
PCO2 and hydrogen ion-concentration decrease.
Respiratory alkalosis is rarely chronic and usually does not need specific treatment.
Fluid and Electrolyte Balance during Injury

Fluid and Electrolyte Balance during Injury

Mixed patterns of acid-base imbalance
Mixed patterns of acid-base disturbance are common, particularly in very sick patients.
Fluid and Electrolyte Balance during Injury

Case 1
39 year old male involved in MVC brought to ED by EMT, he is unconscious, hr 120 bp 80/50, intubated in the scene, what is your immediate action
a)Take further history
b)Start him on dextrose 5% with NS
c)Start him in colloid
d)Start him in Normal saline

Case2
A recovery nurse calling you to see a 70 year old male, 7 hours post appendicictomy, because he is drowsy and unresponsive, his vital signs are normal and oxygen saturation 92% on room air? What is the most likely diagnosis?
a)Intracranial bleeding
b)Stroke
c)Acute renal failure
d)Respiratory failure

Case3
70 year old male, admitted for elective hernia repair, kept NPO and started in D5 ½ normal saline 24 hour ago, his current electrolyte showed k of 5 mmol and Na of 128 mmol What is the most likely diagnosis?
a)DI
b)SAIDH
c)Acute renal failure
d)Iatrogenic hyponatremia

Fluid and Electrolyte Balance during Injury
Summary Understand of The Normal Regulation of Fluid Balance Fluid Imbalance In Shock State Early Hemodynamic Optimization Fluid Therapy (Types) & Indication Electrolyte disturbances in trauma and surgery Acid base in surgery patients

Thank you
??







![West Midlands FCEM Course - Health Education England · West Midlands FCEM Course August 2009 Clinical SAQ Paper 2 QUESTION 1 [A] A 21 yr old British resident travelled to Bolivia](https://img.pdfslide.us/doc/110x75/5e801184225c0b1120656645/west-midlands-fcem-course-health-education-england-west-midlands-fcem-course-august.jpg)