Embed Size (px)
Citation preview
Thorax 1983;38:609-615
Flow-volume curves and sleep-disordered breathing:therapeutic implicationsEDWARD F HAPONIK, PHILIP L SMITH, JOSEPH KAPLAN,EUGENE R BLEECKER
From the Pulmonary Division and the Baltimore Regional Sleep Disorders Center, Department ofMedicine,Baltimore City Hospitals and Johns Hopkins Medical Institutions, Baltimore, Maryland, USA
ABSTRACT To assess the relationship of abnormal flow-volume curves during awake periods tothe clinical severity of sleep-disordered breathing and the need for surgical treatment of obstructivesleep apnoea, flow-volume curves were measured in 72 adults with obstructive apnoea. Patients inwhom surgery was recommended for standard clinical indications had significantly lowerinspiratory flow rates (p < 0.01) and a higher incidence of flow-volume curves indicatingextrathoracic airway obstruction (p < 0.01) than did non-surgical patients. These abnormal flow-volume curves correlated with an increased severity of nocturnal oxygen desaturation (p < 0.01).Furthermore, increases in inspiratory flow rates measured serially in 22 patients were related toimprovement in their polysomnography (p < 0.05), suggesting that alterations of airway functionduring awake periods correlate with changes in the severity of sleep apnoea.
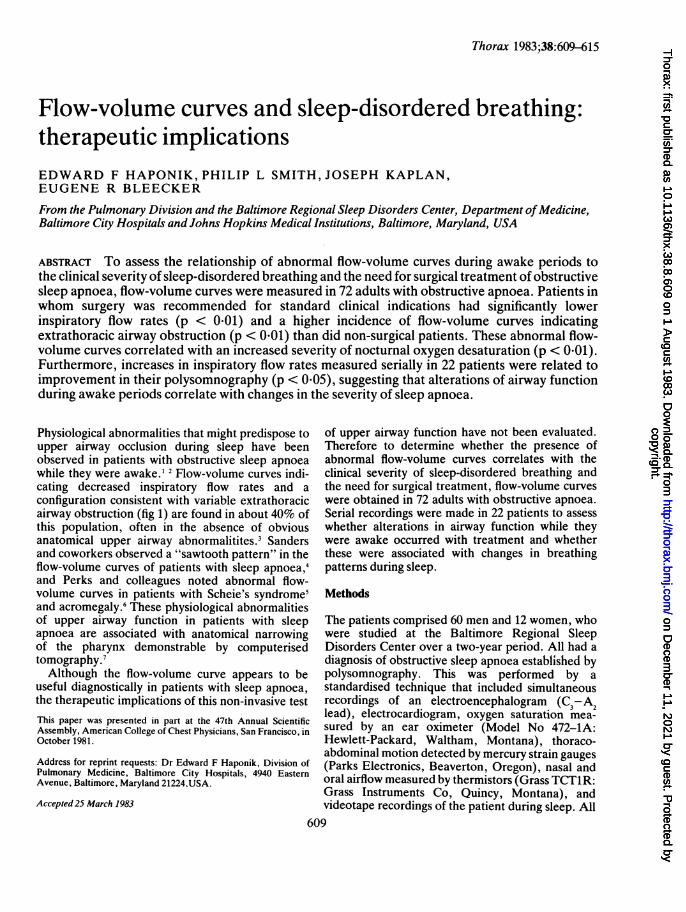
Physiological abnormalities that might predispose toupper airway occlusion during sleep have beenobserved in patients with obstructive sleep apnoeawhile they were awake.' 2 Flow-volume curves indi-cating decreased inspiratory flow rates and aconfiguration consistent with variable extrathoracicairway obstruction (fig 1) are found in about 40% ofthis population, often in the absence of obviousanatomical upper airway abnormalitites.3 Sandersand coworkers observed a "sawtooth pattern" in theflow-volume curves of patients with sleep apnoea,4and Perks and colleagues noted abnormal flow-volume curves in patients with Scheie's syndrome'and acromegaly.6 These physiological abnormalitiesof upper airway function in patients with sleepapnoea are associated with anatomical narrowingof the pharynx demonstrable by computerisedtomography.7Although the flow-volume curve appears to be
useful diagnostically in patients with sleep apnoea,the therapeutic implications of this non-invasive testThis paper was presented in part at the 47th Annual ScientificAssembly, American College of Chest Physicians, San Francisco, inOctober 1981.
Address for reprint requests: Dr Edward F Haponik, Division ofPulmonary Medicine, Baltimore City Hospitals, 4940 EasternAvenue, Baltimore, Maryland 21224,USA.
Accepted 25 March 1983
of upper airway function have not been evaluated.Therefore to determine whether the presence ofabnormal flow-volume curves correlates with theclinical severity of sleep-disordered breathing andthe need for surgical treatment, flow-volume curveswere obtained in 72 adults with obstructive apnoea.Serial recordings were made in 22 patients to assesswhether alterations in airway function while theywere awake occurred with treatment and whetherthese were associated with changes in breathingpatterns during sleep.
Methods
The patients comprised 60 men and 12 women, whowere studied at the Baltimore Regional SleepDisorders Center over a two-year period. All had adiagnosis of obstructive sleep apnoea established bypolysomnography. This was performed by astandardised technique that included simultaneousrecordings of an electroencephalogram (C3-Alead), electrocardiogram, oxygen saturation mea-sured by an ear oximeter (Model No 472-1A:Hewlett-Packard, Waltham, Montana), thoraco-abdominal motion detected by mercury strain gauges(Parks Electronics, Beaverton, Oregon), nasal andoral airflow measured by thermistors (Grass TCT1R:Grass Instruments Co, Quincy, Montana), andvideotape recordings of the patient during sleep. All
609
copyright. on D
ecember 11, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.8.609 on 1 A
ugust 1983. Dow
nloaded from
copyright. on D
ecember 11, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.8.609 on 1 A
ugust 1983. Dow
nloaded from
copyright. on D
ecember 11, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.8.609 on 1 A
ugust 1983. Dow
nloaded from
610
physiological variables were recorded on either aBeckman DM dynograph (Beckman Instruments,Schiller Park, Illinois) or a Grass polygraph (GrassInstruments Co). The study was interpreted accord-ing to conventional criteria,8 independently of theresults of flow-volume curves.
Sleep-disordered breathing events were cate-gorised as apnoea or hypopnoea. Apnoea wasdefined as cessation of respiratory airflow for 10seconds or longer. Central apnoea was defined assimultaneous absence of airflow and thoraco-abdominal motion and obstructive apnoea as~theabsence of airflow despite persistent and usuallyprogressively accentuated thoracoabdominal move-ments. These events were usually terminated by aresuscitative snort with subsequent restoration ofairflow and arousal according to the EEG.Hypopnoea was defined by decreased nasal and oralairflow with continued thoracoabdominal move-ment, accompanied by EEG signs of arousal and afall in oxygen saturation of at least 4% from thebaseline level while the patients were awake andsupine. At least 30 episodes of apnoea or hypopnoeaduring a six-hour nocturnal sleep period, or a rateexceeding five episodes an hour, were required tomake the diagnosis of sleep-disordered breathing.The frequency of all episodes was expressed as thedisordered-breathing rate. The severity of oxygendesaturation during the sleep study was expressed asthe maximum fall in oxygen saturation from thebaseline level when patients were awake andsupine(ASao2%).Three reproducible flow-volume curves were ob-
tained in the sitting position in all patients. Thesewere derived by differentiation of the volume signalfrom a Stead Wells spirometer equipped with alinear potentiometer (Warren E Collins, Braintree,Montana), which was displayed on a storage oscillo-scope (Tektronix, Beaverton, Oregon) and photo-graphed with a polaroid camera. Two reviewersinterpreted the studies without knowledge of theoutcome of polysomnography or therapeutic recom-mendations. The flow-volume curves were cate-gorised as consistent with variable extrathoracicairway obstruction if the ratio of forced expiratoryflow at 50% of the vital capacity to forced inspiratoryflow at 50% of the vital capacity (FEF50/FIF5,)exceeded 1-09-" (fig 1). A sawtooth pattern of theflow-volume curve was recognised from the distinct,regular oscillations of flow.4Recommendations for treatment were made with-
out consideration of the flow-volume curve data.Indications for surgery included the presence of anobvious anatomical upper airway obstruction (identi-fied during routine physical examination, indirectlaryngoscopy, or fibreoptic nasopharyngoscopy),
Haponik, Smith, Kaplan, Bleecker
potentially life-threatening cardiovascular abnor-malities associated with the sleep-related breathingdisorders, and excessive daytime somnolence thatwas both incapacitating and unresponsive to medicaltreatment. Cardiovascular complications includedcor pulmonale and cardiac arrhythmias (atrio-ventricular block, sinus arrest, premature atrial orventricular contractions). Shifts from sinus brady-cardia to sinus tachycardia were not regarded as anindication for surgery, since these rhythm changesare frequently associated with apnoea episodes.
Serial polysomnography and pulmonary functionstudies were carried out before and after treatment in22 patients. Follow-up polysomnograms were com-pared with the original ones, and were considered toshow improvement if there was at least a 20%decrease in disordered-breathing rate and also a 10%improvement in maximum ASao2% during bothnon-rapid-eye-movement and rapid-eye-movementsleep.
Statistical analysis was performed by X2 test andStudent's t test for unpaired and paired variablesrespectively. 12
Results
Non-surgical treatment was recommended in 47patients, and included nocturnal oxygen,"3 weightreduction, or drug treatment with protriptyline1'17 ormedroxyprogesterone.18 Surgical treatment was ad-
I 86
4 ExpFlow
2 (Ifs)
2 InspFlow
! (Ifs)
Fig 1 Flow-volume curve in a patient with obstructive sleepapnoea. The plateau of inspiratoryflow rates and an FEF5JFIF50> 1-0 are consistent with variable extrathoracic airwayobstruction. Sawtoothing is present on the expiratory curve.
The vertical broken line denotes 50% of the vital capacity.TLC-total lung capacity; RV-residual volume.
I
copyright. on D
ecember 11, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.8.609 on 1 A
ugust 1983. Dow
nloaded from
Flow-volume curves and sleep-disordered breathing: therapeutic implicationsTable 1 Obstructive sleep apnoea: indications for surgeryIndication No of
patientsAnatomical obstruction 6*Tumour 1Laryngeal web 1Micrognathia 2Tonsillar hypertrophy 2
Cardiovascular complications 7*Arrhythmias 4Cor pulmonale 3
Incapacitating hypersomnolence 16*
*More than one major criterion was present in four patients.
vised in the remaining 25 patients and includedtracheostomy"9 20 in 16 patients, tonsillectomy in twopatients, and uvulopalatopharyngoplasty21 in sevenpatients.The indications for surgery are outlined in table 1.
Six patients had obvious anatomical upper airwayobstruction. One patient had a benign tumour(lymphangioma), one had a laryngeal web, twopatients had micrognathia with a bird-like face asdescribed by Coccagnia et al,22 and two patients hadmassive tonsillar hypertrophy.23 Cardiovascular com-plications were present in four of these patients, andin three who did not have anatomical abnormalities.Four patients had cardiac arrhythmias associatedwith episodes of oxygen desaturation; these includedfrequent sinus arrests of up to 12 seconds in onepatient, paroxysmal atrial tachycardia in another,and frequent multifocal premature ventricular con-tractions in two. All the cardiac arrhythmias occurredin patients with a history of heart disease. Threepatients had cor pulmonale, presumably because ofobstructive sleep apnoea and the associated noctur-nal oxygen desaturation. Thus surgery was advocatedas initial treatment in the nine patients with anatomi-cal obstruction or cardiac complications or both.Four of these patients, all with anatomical upperairway obstruction, refused this treatment. Eitheruvulopalatopharyngoplasty or tracheostomy was re-commended in 16 other patients because of persistentand incapacitating daytime somnolence that wasunrelieved by medical treatment, and 13 of these hadsurgery.The clinical characteristics of the patients, includ-
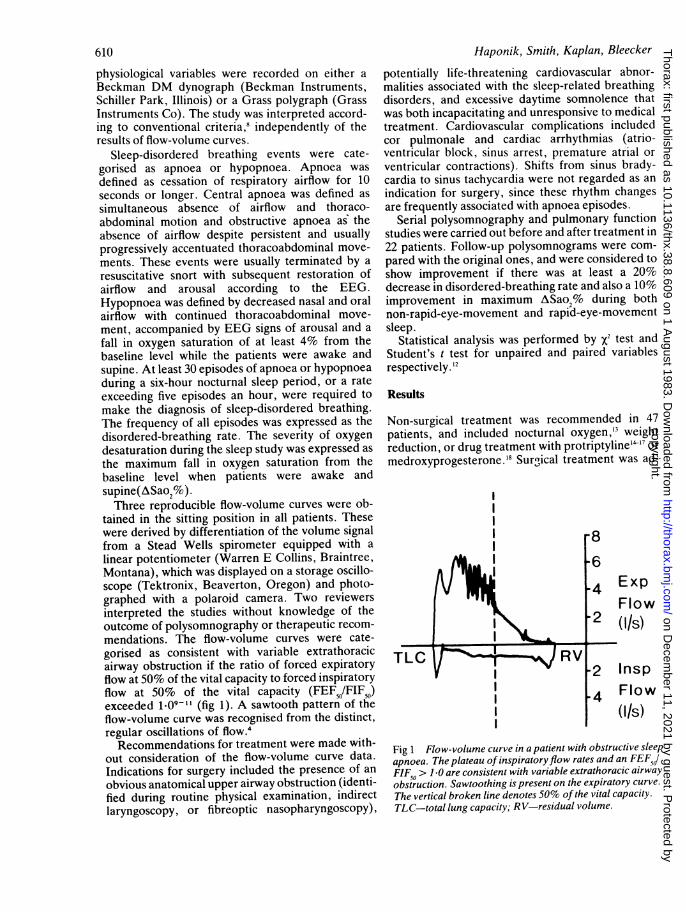
ing age, disordered breathing rate, and the maximumfall of oxygen saturation in non-REM sleep from thebaseline level when they were awake and supine areshown in fig 2. The surgical and non-surgical groupswere of similar age and had a similar number ofdisordered-breathing episodes per hour of sleep. Allpatients experienced clinically important falls inoxygen saturation and these were significantly moresevere in the patients who had surgery (p < 0.01).
100
80
60
40
20
NS
i
NS p(.001
I
- _mu - _- I - - I
Age DBR ASao2,%Fig 2 Clinical characteristics ofpatients with obstructivesleep apnoea. Surgical and non-surgical patients weresimilar with regard to age and disordered-breathing rate(DBR), but surgical patients had more severe falls in oxygensaturation (ASao2, %). The values recorded are thoseobtained during non-rapid-eye-movement sleep.0 Surgical; C non-surgical. The vertical axis indicatesnumbers ofpatients.
The results of flow-volume curves are shown intable 2. Twenty-five of the 72 patients (35%) hadflow-volume curves that were consistent with vari-able extrathoracic airway obstruction. This findingwas not associated with a significantly higher disor-dered-breathing rate, but was associated with a moresevere fall in oxygen saturation. Patients withextrathoracic obstruction had a maximum fall inSao2I% of 33*0 (20-8) (mean and SD) while thosewithout extrathoracic obstruction had a fall in Sao2%of only 20.9 (12.3) (p < 0.01). Abnormal curves wereobtained in only eight of 47 (17%) referred formedical treatment, but in 17 of 25 (68%) in whomsurgery was recommended. This relationship wassignificant, but might have been accounted for by thepatients with obvious anatomical upper airwayabnormalities, all of whom had decreased inspiratoryflow rates. The association of abnormal flow-volumecurves with the requirement for surgery remainssignificant, however, if analysis is limited to patientswithout apparent anatomical obstruction (p < 0.01),or if those who refused surgery are excluded(p < 0-01). The relationship between treatmentrecommendations and the results of flow-volumecurve measurements are shown in fig 3. Peakexpiratory flow rates (PEF) in surgical patients were
hmmmh..
611
copyright. on D
ecember 11, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.8.609 on 1 A
ugust 1983. Dow
nloaded from
Table 2 Relationship betweenflow-volume curve abnormalities and clinical severity ofsleep apnoeaNo of Disordered Maximum ASao2 No with surgicalpatients breathing rate (%, mean (SE)) indications
(mean (SE)episodeslh)
Extrathoric airway obstructionPresent 25 56-6 28-8) 33-0 (20-8) 17Absent 47 54-2 28.7) 20-9 (12-3) 8p NS p<0-01 p<04C
Sawtooth patternPresent 36 59-3 (26-9) 25-9 (17-2) 15Absent 36 51-3 (28-9) 24-4 (16-8) 10p NS NS NS
ASao2-change in percentage oxygen saturation of arterial blood; NS-not significant.
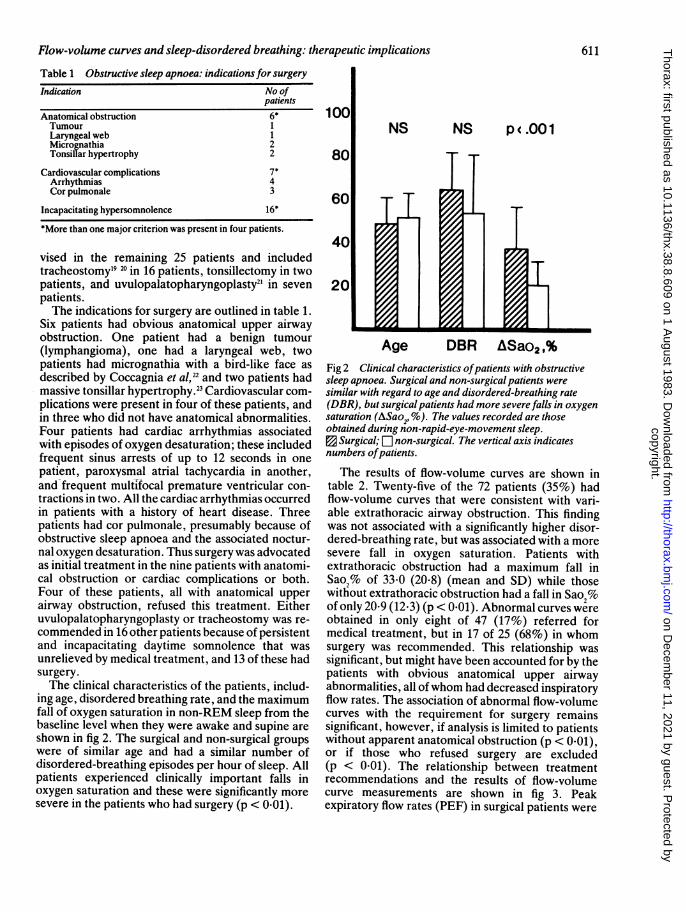
not significantly different from those of non-surgicalpatients. Their peak inspiratory flow rates (PIF),however (4.08 (1.8) I/s), were lower (p < 0.01) andthe ratio of FEF, to FIFw (1-41 (0-88)) was higher(p < 0.001) than that of non-surgical patients (5-55(2.3) 1/s and 0-82 (0-36) respectively). The surgicalpatients were slightly more obese, with higherweight:height ratios than non-surgical patients, butobesity itself did not correlate with the flow volumemeasurements.A sawtooth pattern of the flow-volume curve4 was
present on the expiratory curves of 36 patients(50%), and occurred more often in surgical (15/25,60%) than non-surgical patients (21/47, 44-7%).Sawtoothing did not correlate with either the disor-
p(.05 NS p .01 p .001
Wt/Ht PEF PIF FEF50 /FII50Fig 3 Flow-volume curve measurements in patients withobstructive apnoea. Peak expiratoryflow rate (PRU) wassimilar in both groups, butpeak inspiratoryflow rate (PIF)was lower and the ratio offorced expiratoryflow at50%vital capacity toforced inspiratoryflow at50% vitalcapacity (FEFQJFIFd) was higher in surgicalpatients.a Surgical; ji non-surgical. Units ofPEFand PIF are lls.
dered-breathing rate or the severity of oxygendesaturation (table 2).
Serial pulmonary function studies and poly-somnography were performed in 22 patients. All hadexcessive daytime somnolence, abnormal disor-dered-breathing rates, and large falls in oxygensaturation during sleep. Treatment consisted of thefollowing: 16 patients received drug treatment (14protriptyline, two amitriptyline), three had upperairway surgery (one tonsillectomy, two uvulopala-topharyngoplasty), one with obvious tonsillarhypertrophy refused surgery and was treated with acervical collar, and two refused all treatment.According to the criteria previously described, 11 ofthese patients (seven having drugs, three who hadsurgery, and one who had a collar) had improvedpolysomnograms. Their mean disordered-breathingrates fell significantly from 63-8 (20-8) episodes anhour to 30-8 (19-7) episodes an hour (p < 0-01) andthe maximum percentage fall in oxygen saturationduring apnoeic periods in non-REM sleep wasreduced from 36-9 (19-2) to 12-6 (10-2) (p < 0.01).Eleven patients had no improvement in poly-somnography: their disordered-breathing rates didnot change (55-3 (20-7) baseline, 52-6 (33-8) follow-up; p > 0-5), and their maximum percentage fall inoxygen saturation was unchanged (25-1% (16-1%)baseline, 26-1 (18-7%) follow-up, p > 0-5).The relationship of serial measurements of inspira-
tory flow rates when the patients were awake to theresults of polysomnography is summarised in table 3.PIF and FIF N increased significantly (p < 0-05) inpatients with improvement in their sleep-disorderedbreathing. PIF worsened (p < 0-05), and FIF.0 wasunchanged in patients without polysomnographicimprovement at the time of their follow-up examina-tion. Mean FEF5O:FIF 5 was unchanged in bothgroups, but changes in the configuration of flow-volume curves occurred in eight patients. In six thebaseline flow-volume curves were consistent withupper airway obstruction and reverted to a normalpattern after treatment, and all of these had im-proved polysomnograms. One patient whose sleep
612 Haponik, Smith, Kaplan, Bleecker
copyright. on D
ecember 11, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.8.609 on 1 A
ugust 1983. Dow
nloaded from
Flow-volume curves and sleep-disordered breathing: therapeutic implicationsTable 3 Association ofserialflow-volume curvemeasurements* (means and SD) with polysomnographicfindingsFlow-volume curve Polysomnogram result
Improved Unimproved(n=ll) (n=11)
Peak inspiratory flow rateBaseline 5-5 (2-1) 5-4 1-9)Follow-up 6-4 (1-8)t 4-4 15)t
FIFeaseline 5-2 (2-1)t 4-8 (1-9)Follow-up 6-2 1-8 4-1(1-6
FEF 5WF-IF5IJBaseline 0-97 (0-3 1-1 11Follow-up 0-83 (0-4) 1-3 1.0
*Flow rates expressed in I/s.tDifference between baseline and follow-up results significant:p<O.05.FIF,0-forced inspiratory flow at 50% vital capacity; FEF,0-forced expiratory flow at 50% vital capacity.
apnoea worsened had curves at follow-up suggestingextrathoracic obstruction that was not present at thetime of the initial study. Another patient had lessapnoea but an increased FEF.1/FIF., an apparentdiscrepancy related to the patient's severe obstruc-tive pulmonary disease (which considerably loweredthe FEF, in his baseline expiratory curve). In the 21patients without obstructive pulmonary disease con-version of the flow-volume curve to a normal patterncorrelated (p < 0-05) with polysomnographic im-provement.
Discussion
These data further confirm the relationship thatexists between upper airway function while patientsare awake and the presence of an abnormal breathingpattern with oxygen desaturation during sleep.3 I I
Abnormalities of flow-volume curves not only wereassociated with obstructive sleep apnoea but alsocorrelated with its severity. Patients with airwaydysfunction while awake had more severe nocturnalhypoxaemia and more medical complications thatrequired surgical intervention. Furthermore, im-provement in upper airway function while they wereawake was associated with a decrease in the severityof the sleep-related breathing disorder.
Increased awareness has resulted in the morefrequent diagnosis of obstructive sleep apnoea.Treatment for this disorder continues to evolve,however, and there are no absolute guidelines forsurgery. Tracheostomy"9 20 has become the estab-lished mode of treatment for patients with obviousanatomical upper airway obstruction or life-threaten-ing cardiovascular complications. The latter occurredin only seven (9.7%) of our patients, and was less
common than previously suspected." In patients withless severe clinical manifestations of sleep apnoeatracheostomy may be unacceptable. Furthermore,the availability of less invasive forms of treat-ment 1348 21 25-29 may further modify the need forsurgery. In our group of patients hypersomnolencewas the major reason for surgery and accounted for64% of those in whom such treatment was recom-mended. The fact that the degree of oxygendesaturation was more severe in this group than inthe non-surgical patients with fewer symptomssupports the hypothesis that hypoxaemia may beresponsible for much of the excessive somnolenceassociated with obstructive apnoea.10 31The relationship between the results of flow-
volume curves and polysomnography might havebeen anticipated in patients with obvious anatomicalupper airway abnormalities, but they representedonly 8% of our patients, and only 24% of those inwhom surgery was advised. This low frequency ofupper airway abnormalities apparent in the patientswhen awake probably reflects the relative insensitiv-ity of conventional techniques for the assessment ofthe upper airway. When computed tomography isused for evaluation of pharyngeal structure, airwaynarrowing is detectable during awake periods in mostpatients with obstructive sleep apnoea.7 We believethat the flow-volume curves reflect this upper airwaynarrowing and, in addition, the tendency for theairway to collapse during forced inspiration.
Since flow-volume curves are useful in the assess-ment of upper airway function, we might predict thatimproved flows would correlate with improvementsin obstructive apnoea. As can be seen, increasedinspiratory flow rates were associated with decreasesin the disordered-breathing rate and in the degree ofnocturnal oxygen desaturation. Furthermore, theconversion of an abnormal configuration of the flow-volume curve to a normal pattern, suggesting adecrease in upper airway obstruction, correlated withpolysomnographic improvement. Even though thechanges in inspiratory flow rates were small, theywere associated with significant improvement in theseverity of obstructive apnoea, emphasising thedelicate balance that exists between the forcesmaintaining upper airway patency and those produc-ing airway occlusion.
It was not surprising that improvement both ofinspiratory flow rates when patients were awake andof sleep-disordered breathing occurred after thesurgical correction of obvious anatomical upperairway obstruction in three of our patients. Similarpostoperative changes in flow-volume curves havebeen seen in patients without sleep apnoea.32 Theincreased PIF and FIF50 of the patient treated with acervical collar are also consistent with improvement
613copyright.
on Decem
ber 11, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.38.8.609 on 1 August 1983. D
ownloaded from
614
in anatomical upper airway obstruction and withreported effects of head position on upper airwayresistance. Inspiratory flow rates also increased insome ofthe patients treated with protriptyline, a non-
sedating tricyclic antidepressant, which has beenused successfully for the treatment of patients withmoderately severe sleep-disordered breathing.IllAlthough this drug is thought to block competitivelypresynaptic a-receptors and has major anticho-linergic properties, its mechanism of action inpatients with obstructive apnoea remains unclear.The increases in inspiratory flow rates while theywere awake in patients whose sleep-disorderedbreathing improved with protriptyline might beexplained by altered tone of the upper airwaymusculature, improved function or co-ordination ofother inspiratory muscles, or changes in neural or
cortical control.Anatomical or functional upper airway obstruction
detectable while patients are awake occurs more
commonly in obstructive sleep apnoea than isgenerally appreciated. We do not suggest that theabnormal flow-volume curve represents an indepen-dent indication for surgical treatment; but we believethat this simple, reproducible test provides pro-gnostic as well as diagnostic information and mightprove useful in guiding decisions about management.Experience with patients with obstructive sleepapnoea indicates that objective analysis of sleep isrequired to assess the effects of treatment. Flow-volume measurements may also have a role inmonitoring the clinical course of patients withobstructive apnoea, although at present there is nosubstitute for the careful physiological assessment ofsleep.
The writers thank Betty Giacomazza and LorenaClary for their secretarial assistance; Pam Hipler,Sandra McCawley, Garry Roberts, and NormanChubert for technical assistance; and Pam Mason andJennifer Grago for the statistical analyses andfigures.
References
Anch AM, Remmers JE. Upper airway resistance duringwaking and sleep in the Pickwickian syndrome. AmRev Respir Dis 1980;121,Suppl: 310.
2 Martin RJ, Pennock BE, Orr WC, Sanders MH, RogersRM. Respiratory mechanics and timing during sleep inocclusive sleep apnea. J Appl Physiol 1980;48:432-7.
Haponik EF, Bleecker ER, Allen RP, Smith PL, KaplanJ. Abnormal inspiratory flow volume curves in patientswith sleep-disordered breathing. Am Rev Respir Dis1981;124:571-4.
Sanders MH, Martin RJ, Pennock BE, Rogers RM. The
detection of sleep apnea in the awake patient. JAMA1981;245:2414-8.
Haponik, Smith, Kaplan, Bleecker
Perks WH, Cooper RA, Bradbury S, et al. Sleep apnoea inScheie's syndrome. Thorax 1980;35:85-91.
6 Perks WH, Horrocks P, Cooper RA, et al. Sleep apnea inacromegaly. Am Rev Respir Dis 1980;121, Suppl: 175.
Haponik EF, Smith PL, Bohlman ME, Allen RP,Goldman SM, Bleecker ER. Computerized tomo-graphy in obstructive sleep apnea: correlation ofairway size with physiology during sleep and wakeful-ness. Am Rev Respir Dis 1983;127:221-6.
8 Rechtschaffen A, Kalas A. A manual of standardizedterminology, techniques, and scoring system for sleepstages of human subjects. Los Angeles:BlS/BRI,University of California at Los Angeles, 1968:4-11.
9 Miller RD, Hyatt RE. Obstructing lesions of the larynxand trachea; clinical and physiologic characteristics.Mayo Clin Proc 1969;44:145-61.
10 Rotman HH, Liss HP, Weg JG. Diagnosis of upperairway obstruction by pulmonary function testing.Chest 1975;68:796-9.
Sackner MA. Physiologic features of upper airwayobstruction. Chest 1972;62:414-7.
12 Snedecor GW, Cochron WG. Statistical methods. 6th ed.Ames: Iowa State University Press, 1967.
13 Martin RJ, Sanders MH, Gray BA, Pennock BE. Acuteand long-term ventilatory effects of hyperoxia in theadult sleep apnea syndrome. Am Rev Respir Dis1982;125:175-80.
14 Smith PL, Haponik EF, Allen RP, Bleecker ER. Theeffects of protriptyline in sleep-disordered breathing.Am Rev Respir Dis 1983;127:8-13.
15 Clark RW, Schmidt HS, Schaal SF, Boudoulas H,Schuller DE. Sleep apnea: treatment with pro-triptyline. Neurology 1979;29:1287-92.
16 Conway WA, Zorick F, Piccione P, Roth T. Protriptylinein the treatment of sleep apnoea. Thorax 1982;37:49-53.
17 Brownell LG, West P, Sweatman P, Acres JC, KrygerMH. Protriptyline in obstructive sleep apnea: a double-blind trial. N Engl J Med 1982;307:1037-42.
18 Strohl KP, Hensley MJ, Saunders NA, Scharf SM, BrownR, Ingram RH. Progesterone administration andprogressive sleep apneas. JAMA 1981;245:1230-2.
19 Motta J, Guilleminault C, Schroeder JS, Dement WC.Tracheostomy and hemodynamic changes in sleep-induced apnea. Am Intern Med 1978;89:454-8.
20 Tilkian AG, Guilleminault C, Schroeder JS, LehrmanKL, Simmons FB, Dement WC. Sleep-induced apneasyndrome: prevalence of cardiac arrhythmias and theirreversal after tracheostomy. Am J Med 1977;63:348-58.
21 Conway W, Fujita S, Zorick F, Roth T, Hartse K,Piccione P. Uvulopalatopharyngoplasty in treatmentof upper airway sleep apnea. Am Rev Respir Dis1980;121, Suppl:121.
22 Coccagna G, Cirignotta F, Lugaresi E. The bird-like facesyndrome (acquired micrognathia, hypersomnia, andsleep apnea). In: Guilleminault C, Dement WC, eds.Sleep apnea syndromes. New York: Alan R Liss,1978:259-71.
23 Orr WC, Martin RJ. Obstructive sleep apnea associatedwith tonsillar hypertrophy in adults. Arch Intern Med1981;141:990-2.
24 Miller WP, Cardiac arrhythmias and conduction distur-bances in the sleep apnea syndrome: prevalence andsignificance. Am J Med 1982;73:317-21.
copyright. on D
ecember 11, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.8.609 on 1 A
ugust 1983. Dow
nloaded from

Flow-volume curves and sleep-disordered breathing: therapeutic implications25 Afzelius LE, Elmqvist D, Hougaard K, Laurin S, Nilsson
B, Risberg AM. Sleep apnea syndrome: an alter-native treatment to tracheostomy. Laryngoscope1981 ;91:285-91.
26 Sullivan CE, Issa FG, Jones MB, Eves L. Reversal ofobstructive sleep apnoea by continuous positive airwaypressure applied through the nares. Lancet 1981 ;i:862-5.
27 Rapoport DM, Sorkin B, Garay SM, Goldring RM.Reversal of the "Pickwickian syndrome" by long-termuse of nocturnal nasal-airway pressure. N Engl J Med1982;307:931-3.
28 Sanders MH, Moore SE, Eveslage J. CPAP via nasalmask: a treatment for occlusive sleep apnea. Chest1983;83: 144-5.
615
29 Cartwright RD, Samelson CF. The effects of anonsurgical treatment for obstructive sleep apnea: thetongue-retaining device. JAMA 1982;248:705-9.
30 Orr WC, Martin RJ, Imes NK, Rogers RM, Stahl ML.Hypersomnolent and nonhypersomnolent patientswith upper airway obstruction during sleep. Chest1979;75:418-22.
31 Harman E, Wynne JW, Block AJ, Malloy-Fisher L.Sleep-disordered breathing and oxygen desaturation inobese patients. Chest 1981;79:256-60.
32 Cormier Y, Kashima H, Summer W, Menkes H. Airflowin unilateral vocal cord paralysis before and after tefloninjection. Thorax 1978;33:57-61.
copyright. on D
ecember 11, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.8.609 on 1 A
ugust 1983. Dow
nloaded from

Thorax 1983;38:800
Book noticePulmonary Function Testing Guidelines and Controversies.JL Clausen (ed). (Pp 368; $39-95.) Academic Press, 1982.
This is essentially a practical manual covering the detailedmethods of pulmonary function testing with recommendednormal reference data. Particularly welcome are theemphasis on quality control and trouble shooting and honestdiscussion of areas of uncertainty and controversy. Thestyle is necessarily didactic, but largely based on commonsense. Although written primarily for an American audi-ence, most of the information and opinions travel well andthe references are comprehensive and up to date. Thecriterion for inclusion of a test is its popularity in variouslaboratories rather than a critical appraisal of its clinicalrole, and a further volume is promised on the more difficultand controversial area of clinical interpretation and useful-ness. Unconventional inclusions such as radiographic esti-mation of lung volume and measurements in the intensivecare unit are offset by surprising omissions, including peakflow, Kco, and mixed venous carbon dioxide tension asmeasured by rebreathing; and the important area ofradioisotope studies is not covered. Despite these deficien-cies, physicians and senior technicians concerned with clin-ical lung function testing will find much of interest andvalue in this book and they will be reassured to discoverthat their everyday practical problems are shared byothers.
NoticeAnnual meeting of the European Academy of Allergologyand Clinical ImmunologyThe annual meeting of the European Academy of Aller-gology and Clinical Immunology 1984 will be held in Brus-sels on 16-19 May. The themes will be the immunologicalaspects of asthma, occupational allergy, and immunomodu-lation, with a postgraduate course on the treatment ofallergic diseases. Further information from Professor RPauwels, Department of Respiratory Diseases, De Pin-telaan 185, B 9000 Ghent, Belgium.
CorrectionsFlow-volume curves and sleep-disordered breathingWe regret the following errors in the paper by Dr EFHaponik and others (August 1983, pp 609-15): On p 609,col 2, para 2, lines 10 and 14; and p 610, col 1, para 3,line 6, "Montana" should be "Massachusetts." In table 2,2nd and 3rd column headings, "SE" should be "SD."
Respiratory muscle and pulmonary function inpolymyositis and other proximal myopathiesWe regret the following errors in the paper by Dr NMTBraun and others (August 1983, pp 616-23): On p 617,col 1, para 2, line 3, "Montana" should be "Mas-sachusetts." In table 4, 2nd line of heading, "observations"should be "subjects."





























