Embed Size (px)
Citation preview

0 1984 Alan R. Liss, Inc. Cytometry 5:636-643 (1984)
Flow Cytometry of Postmortem Human Testicular Tissue in Cases of Atherosclerosis'
Richard Klein and Peter Pfitzer Department of Cytopathology, University of Diisseldorf, D-4000 Diisseldorf, Federal Republic of Germany
Received for publication July 29, 1983; accepted June 12, 1984
From forty-seven autopsy cases of athero- sclerosis flow cytometry (FCM) of DNA and histology of both testes are compared with the histological sections of their supplying vessels arteriae testiculares and arteriae ductus de- ferentis at different levels. By this method, changes of spermatogenesis are judged sepa- rately for each side and the results can be related to the local conditions of blood supply. Four young men, dead after traffic accidents, served as control. In the majority of cases, the computer-assisted evaluations of the mei- otic DNA histograms show no differences be- tween the right and left testis, even when dif-
ferences of the arterial diameters are found by histology. On the other hand, cases with distinct differences in the histograms can show insignificant pathological alterations of the vessels. Though most excessive forms of macroscopic and microscopic atherosclerosis do not necessarily lead to a significant reduc- tion in spermatogenesis, some cases with moderate forms show a strong reduction or even a total loss. This discrepancy can best be explained by superposition of other diseases.
Key terms: Human testicular tissue, meiotic division, atherosclerosis
A considerable amount of cytophotometric work has been done on human sperm (5,6,8,11,12,21,23). A smaller number of papers were published concerning testicular biopsies (4,20,25,26), but ethics limit these investiga- tions to patients with andrological irregularities or the symptoms of a malignant tumor. Cases with other dis- eases can only be studied on postmortem material. For- mer investigations of postmortem testicular tissue with flow cytometry (FCM) (7,13,14) had shown restrictions of spermatogenesis under the influence of liver cirrhosis, fatty liver degeneration, acute and prolonged circulatory shock, and chronic inflammation. However, the investi- gated cases of malignant tumors (3) and atherosclerosis had irregular results and did not allow a definite conclusion.
It seemed probable that the degree in the reduction of spermatogenesis could be negatively correlated to the degree of pathological changes in the testicular arteries. The present investigation tries to estimate this correla- tion between spermatogenesis and the conditions of tes- ticular blood supply. An investigation of the arteria testicularis over its whole length was performed. The data in the literature are confined to the vessels in the testis itself (1,9) except for one angiological study (24). Naturally, it was not possible to limit this study to pure cases of atherosclerosis since multimorbidity usually is responsible for the patient's death.
MATERIALS AND METHODS
Whenever possible, the right and left testis and the complete testicular vessels from 51 autopsies performed 18-48 h postmortem are used for this investigation. Of this number, four control cases of young men dead after traffic accidents are included as control for the normal histological conditions of blood supply.
Histological sections of the formalin-fixed testicular arteries and the testes are made for each case. Stains are hematoxylin-eosin and elastica v. Gieson (EVG). Im- prints from fresh unfixed testicular tissue are taken and stained by May-Grunwald-Giemsa (16).
For the FCM, the testicular tissue is separated from the tunica albuginea, prepared as described, and stained with ethidium bromide and mithramycin (2,14). For analysis, the ICP 11 PHYWE is used. Each histogram comprises between 30,000 and 100,000 registrations and is analyzed with computer assistance (15,22).
'With the support of the Paul-Kuth-Stiftung, Wuppertal, Federal Republic of Germany. Presented at the International Conference of Analytical Cytology and Cytometry IX, Elmau, Federal Republic of Germany, October, 1982.
Address reprint requests to Prof. Dr. Peter Pfitzer, Department of Cytopathology, Moorenstrasse 5, D-4000 Diisseldorf, Federal Republic of Germany.

FCM OF TESTICULAR TISSUE AND ATHEROSCLEROSIS 637
Since some of the patients had only one testis at time of death, and in other cases the criteria of the investiga- tion are only valid for one side, the “number of cases” refers to the number of testes.
RESULTS As criteria for normal testicular DNA histograms the
results of an earlier investigation in our institute are used (14). They are cons+tent with the data of Thorud et al. (20). The control values had been obtained from 20 healthy men who died in accidents or were examined
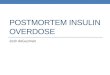
FIG. la,b. Age 76 years, sudden death from cardiac infarction. a) Computer-analyzed normal histogram; b) arteria testicularis with ath- erosclerosis; EVG, x80.
postmortem in forensic medicine. Their DNA histo- grams are characterized by four main peaks correspond- ing to the meiotic cell classes and attaining the following average values for normal spermatogenesis: elongated spermatids ( 1 c A ) 11.8 * 1.3%, round spermatids (1c~) 25.1 f 1.5%, diploid nuclei (2C) 32.7 * 2.3%, 4C nuclei ( 4 0 12.6 f 0.7%. The sum does not equal 100% because small intermediate peaks in the computer-assisted anal- ysis are not included in the main classes. Between 2C and 4C they correspond partly to the S phase and partly they are a consequence of asymmetry of peaks observa- ble also between 1C and 2C or in the haploid range. For this reason S phase is not calculated separately. Figure l a presents such a normal histogram in the case of a man aged 76 and suffering from severe atherosclerosis in the testicular arteries (Fig. lb). The patient had no other superposing diseases. The four main peaks are clearly differentiated: The first on the left side is a “subhaploid” DNA group (1CA) representing elongated spermatids that are more condensed and therefore un- derstained in comparison to the, equally haploid nuclei of the round spermatids in the second peak ( ~ C B ) . The third peak represents the total group of normal diploid cells including spermatogonia and spermatocytes I1 after the first meiotic division. The fourth peak has the value of 4C and includes the premitotic diploid cells but espe- cially the premeiotic and early meiotic spermatocytes I. The distribution shows a clear predominance of the spermatids. As a contrast, a histogram with distinctly reduced
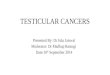
spermatogenesis in the case of a man 73 years old is shown (Fig. 2a). The patient suffered from severe ather- osclerosis (Fig. 2b) but with superposing diseases. As a consequence of the reduction of the haploid class we find a distinct dominance of the diploid values (ZC), mainly caused by connective tissues.
The histological evaluation of the conditions in the supplying testicular arteries is decisive for the judge- ment of spermatogenesis in cases of atherosclerosis. The 47 cases of atherosclerosis with 92 testes could be sub- divided into three groups according to the protocols of the autopsies, which refer above all to the situation in the great arteries of the elastic type and the coronaries.
Fifty-eight testes came from patients with general ath- erosclerosis judged as excessive (group I), 24 testes from cases with moderate to severe atherosclerosis (group 111, and 10 testes from patients with atherosclerosis present- ing only slight to moderate changes (group 111). Indepen- dently, we differentiated between severe and excessive atherosclerosis on the one hand and moderate forms on the other according to the histology of the supplying testicular vessels (Figs. lb,2b). In 48 testes from group I we find severe or excessive atherosclerosis also in the testicular arteries, but the same degree of atheroscle- rosis is found in 25% of group I1 and in 10% of group 111 (Table 1). Thus, atherosclerosis in the testicular vessels correlates only partly with the degree of general ather- osclerosis. Furthermore, it becomes evident that the al- terations in the small arteries of the muscular type must

638 KLEIN AND PFITZER
Table 1 Correlation Between General Atherosclerosis and Atherosclerosis of the Testicular Arteries
Cases of excessive or severe atherosclerosis
Group Degrees of general atherosclerosis N in the testicular arteries
I Excessive 58 28 (48%) I1 Moderate to severe 24 6 (25%) I11 Slight to moderate 10 1(10%)
Total 92 35
not be as severe as the alterations in the great arteries of the elastic type.
In order to estimate the special influence of the path- ological alterations in the vessels on spermatogenesis, those cases with significantly different histology be- tween right and left testicular artery are compared. Only nine of the 47 cases have such a difference. How- ever, none of these nine cases has a corresponding differ- ence in the histograms of the testicular tissues, i.e., in spermatogenesis.
FIG. 2a,b. Age 73 years, death after embolism of the lung and prolonged circulatory shock. a) Histogram with reduced spermatoge- nesis; b) arteria ductus deferentis with severe stenosis; EVG, ~ 8 0 .
This is a first indication for the small effect of patho- logical alterations in the arteriae testiculares upon spermatogenesis.
Histology of the testes is normal in 61 of 92 cases (66%), 22 have a beginning atrophy (24%), and nine show a complete atrophy (10%). On the other hand, only 35 vessels demonstrate severe alterations: 29 combined with normal histology of the testis, five combined with beginning atrophy, and one with total atrophy (Table 2). Therefore, in many cases with severe or excessive path- ological alterations of the testicular arteries testes still have a normal aspect.
The case of a patient 71 years old offers an example for such contradictory results: On the left side heavy atherosclerosis (Fig. 3b) is combined with normal testic- ular histology (Fig. 3c) and a normal DNA histogram (Fig. 3a). However, on the right side an extreme ather- osclerotic plaque covers the ostium of the testicular ar- tery (Fig. 3e), and testicular histology (Fig. 3f l as well as the DNA histogram (Fig. 3d) show severe damage, which could be interpreted as a negative correlation between atherosclerosis and spermatogenesis. However, this is a single case.
Comparing all the sections of the testicular arteries, it can be stated that they are not equally struck by ather- osclerosis (Figs. lb,3b,e,4b). In 84 cases the two arteries could be compared (Table 3) and in only one-third (32%) are the changes equally strong, whereas in 45 (54%) changes predominate in the arteriae ductus deferentis and only in 12 (24%) in the arteriae testicularis.
A further analysis can be tried by dividing all cases into two groups according to the histological conditions in the testicular vessels (Table 4). Thirty-five vessels with severe or excessive alterations show normal sper- matogenesis in 54%, whereas 50 vessels with moderate alterations have normal spermatogenesis in only 34%. This is inconsistent with the expectation.
After this negative result concerning atherosclerosis we analyzed our cases according to four diseases that
Table 2 Correlation Between the Histology of the Testes and the
Atherosclerosis of the Supplying Arteries
Excessive or severe atherosclerosis in the testicular arteries Histology of the testes
Normal 29 (83%) Beginning atrophy 5 (14%) Total atrophy 1( 3%)
Total 35

FCM OF TESTICULAR TISSUE AND ATHEROSCLEROSIS 639
a
FIG. 3a-f. Age 71 years, sudden death from acute failure of the left side of the heart. a) Normal histogram of the left testis; b) Left arteria testicularis: section near the ostium with strongly reduced diameter; EVG, ~ 8 0 . c) Normal left testis; EVG, X80. d) Histogram of the right
testis with reduction of spermatogenesis; e) Ostium of the right A. testicularis with stenosis and atherosclerotic plaque in the aorta; EVG, X45. D Beginning atrophy in the right testis; EVG, ~ 8 0 .

640 KLEIN AND PFITZER
FIG. 4a,b. Age 62 years, death from heart failure after pneumonia. a) Normal histogram; b) arteria ductus deferentis showing recanaliza- tion after complete thrombotic stenosis; EVG X 80.
have a proven influence on spermatogenesis: acute cir- culatory shock, prolonged circulatory shock, liver cirrho- sis, and severe lung emphysema (7,13,14,17,18). There is by chance a significantly higher rate of these four fac- tors in the group of men with moderate alterations in their testicular arteries (74%) than in the group of men with severe vessel disease (40%).
Table 3 Distribution of Estimated Pathological Changes in the Arteria
ductus deferentis and the Arteria testicularis in 84 Cases
More changes in the
More changes in the
Equal changes in both arteries
A. ductus deferentis 45 (54%)
A. testicularis 12 (14%) 27 (32%)
Total 84
If the two groups in Table 4 are divided into two divisions each according to superposing diseases (Table 5), the groups show normal spermatogenesis indepen- dent of pathological changes in the vessels when super- posing diseases are missing. An example is the case of an 82-year-old patient who died immediately after fresh cardiac infarction (Fig. 5). However, reduced spermato- genesis is observed when other diseases superpose (14).
An expected result is that in cases with hypertension the alterations in small vessels are more severe than in cases without (Fig. 6) (19). So, in the total group of 47 men, we find 17 hypertensives, 60% of them with severe or excessive testicular vessel alterations, whereas 30 men without hypertension have severe vessel altera- tions in only 30%. Nevertheless, we find normal sper- matogenesis even in the group of hypertensives with severe alterations when superposing diseases are miss- ing (Table 5, Fig. 6a,b). These results support that even severely altered vessels in cases of atherosclerosis can be combined with normal spermatogenesis.
DISCUSSION First reports confirmed that postmortem material of
the testes can be examined by FCM (7,13,14). Only in a few cases of the former investigations was the testicular tissue totally autolytic at time of preparation. In the present examination such cases have been excluded. The evaluation of the histograms by computer assist- ance establishing a Gaussian distribution for each peak (12,191 allows a quantitative comparison of the FCM results. However, possible autolytical influences make it recommendable to neglect the small intermediate peaks, attaining a few percent only and not definitely belonging to one of the main classes. On the other hand the differentiation of the haploid class in understained elongated spermatids and 1C spermatids is based on the
Table 4 Haploid Values of Spermatogenesis and Vessel Disease
Slightly Moderately Strongly Nearly Normal reduced reduced reduced total loss
Vessels with N 1cTot. (40%) lcTo,. (30-40%) 1cTot, (20-30%) 1cT& (10-20%) 1cTo,, (()-lo%) Severe or
excessive alterations 35 19 (54.3%) 0 5 (14.3%) 6 (17.1%) 5 (14.3%)
alterations 50 17(34%) 1(2%) 9 (18%) 7 (14%) 16 (32%) Moderate

641
r
1 I
I I
1 I
FCM OF TESTICULAR TISSUE AND ATHEROSCLEROSIS
~
FIG. 6a,h. Age 78 years, hypertension. a) Normal histogram; h) arteria testicularis with severe atherosclerosis; EVG, x 80.
FIG. 5a-c. Age 82 years, sudden death from fresh cardiac infarc- tion. a) Normal histogram; b) atherosclerotic alteration in an enlarged ieft Arteria testicularis; c) right Arteria testicularis after former orchi- dectomy; EVG, ~ 8 0 .
comparison of separately prepared epididymal and tes- ticular material (7).
The difficulty in the present investigation consists of a very limited number of cases with pure atheroscle- rosis, i.e., cases with no influence on spermatogenesis other than atherosclerotic reduction in blood supply. For
example, men with severe general atherosclerosis who die of cardiac infarction but are otherwise healthy are extremely rare. In reality, men with cardiac infarction often have a survival time of a few days under intensive care and die then in a state of prolonged circulatory shock.
After a longer survival time of a few weeks, factors like pneumonia and other forms of respiratory insuffi- ciency (17) influence the patient's history. For this rea- son spermatogenesis must always be regarded under the clinical aspects as a whole. Naturally, psychological in- fluences cannot be taken into account in such a study.
As mentioned above the earlier results of FCM in cases of atherosclerosis had been very inconsistent. The influence of altered blood supply was proved for cases of circulatory shock in a former investigation in our insti- tute (13,141. The present investigation was started under the expectation that it would be possible to correlate the reduction of spermatogenesis to the degree of pathologi- cal alterations in the testicular arteries or perhaps to the local conditions at the ostium in a pathologically altered aorta.

642 KLEIN AND PFITZER
Table 5 FCM Results in the Main Classes of Spermatogenesis (%I
Group N 1CA 1CB 1CTOt. 2 c 4c
12.6 k 0.7 Control cases 20 11.8 k 1.3 25.1 k 1.5 40.0 k 1.9 32.7 k 2.3 Severe or
excessive vessel alterations in cases 21 18.7 k 1.1 25.4 k 2.1 44.1 + 2.7 30.8 & 2.1 6.7 k 0.5 without superposing diseases
With superposing diseases
Moderate vessel alterations in cases without superposing diseases
With superposing diseases
Hypertonics with severe or excessive vessel alterations 13 17.9 k 1.6 23.4 k 3.0 41.3 k 3.9 31.3 k 3.2 7.3 k 0.7 in cases without superposing diseases
14 5.9 + 0.9 10.0 * 1.9 15.9 k 2.6 57.0 + 3.4 11.8 k 1.2
13 16.0 + 2.6 23.0 k 3.5 39.0 k 5.6 36.7 k 4.5 7.8 k 0.9
30 9.6 k 1.3 12.9 1.7 22.5 + 2.8 51.5 k 2.8 9.3 k 0.5
However, we find normal spermatogenesis in a remark- able number of cases with severe vessel alterations evi- dently independent of the degree of stenosis. It is remarkable that, in our material of 47 patients with ath- erosclerosis, there is only one case where atherosclerotic vessels alone are responsible for a total loss or even a re- duction of spermatogenesis. This result is inconsistent with our working hypothesis. A total stoppage of blood supply in both testicular arteries without collaterals would naturally stop spermatogenesis, and necrosis would be the result. This makes it clear that atheroscle- rosis should have an effect on the reduction of spermato- genesis, but only in cases of extreme stenosis. However, what we observe is a large tolerance of atherosclerotic al- terations in the testicular vessels before restrictions of the organic function are observed,
The fact that the arteria ductus deferentis is struck more than the arteria testicularis may be a further reason for the small influence of atherosclerosis on sper- matogenesis, since the arteria testicularis is the more important vessel for the blood supply of the testis.
In cases with strong reduction or total loss of sperma- togenesis it seems certain that other events like pro- longed or acute circulatory shock, toxic influences by chronical inflammations, pulmonary insufficiency (171, liver diseases, and hormonal factors dominate the influ- ence of atherosclerosis. The influence of hormonal fac- tors has not been taken into consideration in the present investigation since there were not sufficient data in the patients’ histories. Disturbances of spermatogenesis are known from cases of prolactinome (10).
However, since hormonal factors are not regularly dis- balanced in old age, it seems improbable that the occa- sionally observed reductions of spermatogenesis in advanced age should be directly correlated to hormonal factors. Our results support that atherosclerosis alone,
often correlated with age, does not lead to the expected reduction of spermatogenesis.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
LITERATURE CITED Andres TL, Trainer TD, Lapenas D J Small vessel alterations in the testes of infertile men with varicocele. Am J Clin Pathol 76:378-384, 1981. Barlogie B, Zante J, Drewinko B, Schumann J, Biichner T, Gahde W, Hart JS, Johnston DA The use of mithramycin in pulse-cyto- photometry. In: Pulse cytophotometry, Gijhde W, Schumann J, Biichner T (eds) Ghent, European Press, 1976, pp 125-136. Bohm N, Sandritter W: DNA in human tumors: A cytophotometric study. Curr Top Path01 60:151-219, 1975. Clausen OPF, Abyholm T: Desoxyribonucleic acid flow cytometry of germ cells in the investigation of male infertility. Fertil Steril 34:369-374, 1980. Dean PN, Pinkel D, Mendelsohn ML: Hydrodynamic orientation of sperm heads for flow cytometry. Biophys J 23:7-13, 1978. Gall WE, Ohsumi Y: Decondensation of sperm nuclei in vitro. Exp Cell Res 102:349-358, 1976. Gilbert P, Pfitzer P: Retrospektive Fertilitatskontrolle durch DNA- Messungen am menschlichen Hoden. Verh DG Urol 32:399-401, 198 1. Gledhill BL, Lake S, Steinmetz LL, Gray JW, Crawford JR, Dean PN, Van Dilla MA: Flow microfluorometric analysis of sperm DNA content: Effect of cell shape on the fluorescence distribution. J Cell Physiol 87:367-376, 1976. Glindemann JR, Manzke H: Histologisch-histometrische Untersu- chungen an normalem und pathologischem menschlichem Testes- gewebe unter besonderer Beriicksichtigung der GefaBe. Dissertation, Med Fak Diisseldorf, 1980. Joplin GF: Endokrine Impotenz und Sterilitat. Hexagon Rocke 1O:l-8, 1982. Krieg K, Gerlach R, Rost D: Impulszytophotometrische Spermaun- tersuchungen zum Nachweis von Fertilitats-storungen. Z Gynokol 99:1217-1224, 1977. Otto FL, Hacker U, Zante J, Schumann J, Gohde W, Meistrich ML: Flow cytometry of human spermatozoa. Histochemistry 61:249-254, 1979. Pfitzer P, Gilbert P, Rolz G Fertilitatskontrolle durch DNA-Mes- sungen am menschlichen Hoden. Verh DG Pathol65:388, 1981. Pfitzer P, Gilbert P, Rolz G, Vyska K: Flow cytometry of human

FCM OF TESTICULAR TISSUE AND ATHEROSCLEROSIS 643
testicular tissue. Cytometry 3:116-122, 1982. 15. Hitzer P, Vyska K, Stecher G: Zur Analyse van DNA-Histogram-
men durch Computer. Beitr Pathol 159:157-187, 1976. 16. Schenk U, Schill WB: Vergleichende Untersuchung zwischen Hod-
enbiopsie und Biopsieausstrich bei Azoospermie. Andrologica
17. Semple PDA, Beastall GH, Watson WS, Hume R: Serum Testoster- one depression associated with hypoxia in respiratory failure. Clin Sci 58:105-106,1980,
18. Soderstrom KO, Suominen J Histopathology and ultrastructure of meiotic arrest in human spermatogenesis. Arch Pathol Lab Med 104:476-482,1980,
19. Suzuki T, Oboshi S, Sat0 R: Periarteritis nodosa in spontaneously hypertensive rats: Morphology of the arterial lesion with special reference to the initial changes. Acta Pathol Jpn 292353-864,1979.
20. Thorud E, Clausen OPF, Abyholm T Fine needle aspiration biop- sies from human testes evaluated by DNA flow cytometry. Flow
12268-275, 1980.
Cytom 4:175-177, 1980. 21. Van Dilla MA, Pinkel D, Gledhill BL, Lake S, Watchmaker G,
Wyrobek A J Flow cytometry of mammalian sperm: Progress re- port. Flow Cytom 4279-283, 1980.
22. Vyska K, Pfitzer P, Kraushaar J Computeranaiyse van DNA- Histogrammen. Verh DH Pathol 61:479, 1977.
23. Zante J, Schumann J, Gohde W, Hacker U: DNA fluorometry of mammalian sperm. Histochemistry 54:l-7, 1977.
24. Zemp H. Postmortem angiography of the testis. Path Res Pract 167:380-192,1980,
24. Zemp H: Postmortem angiography of the testis. Path Res Pract 167:380-392,1980,
25. Zimmermann A, Truss F: Die DNA-Bestimmung bei der Diagnos- tik der Hodenerkrankungen. Verh DG Urol31:362-363,1979.
26. Zimmermann A, Truss F: The prognostic power of flowthrough cytophotometry DNA determinations for testicular diseases. Anal Quant Cytol2:247-251,1980.


























![Isolated Testicular Tuberculosis Mimicking Testicular ... involvement, but testicular involvement is an unusual clinical condition [3]. In this report, a case with isolated testicular](https://img.pdfslide.us/doc/110x75/5f3d57bf74280d66ef795ba2/isolated-testicular-tuberculosis-mimicking-testicular-involvement-but-testicular.jpg)