Embed Size (px)
Citation preview

The Alphabet Soup The Alphabet Soup of Traumatic Brain of Traumatic Brain InjuryInjury

DefinitionDefinition
Traumatic brain injury Refers to injuries that result directly from impact.
Injuries include contusions, lacerations, brainstem injuries, and diffuse axonal injury
ENA, 2010


Traumatic Brain InjuryTraumatic Brain Injury
Leading cause of death due to trauma
Outcomes are greatly affected by the severity of the initial injury and the time elapsed to definitive care.
Therefore, rapid interfacility transport is crucial.
Holleran, 2010, p. 311


Secondary Brain InjurySecondary Brain Injury
Injuries caused by pathophysiologic processes which add to the primary injury during a delay—such as transferring the patient to a higher level of care
These include expanding hematomas, increasing cerebral oedema, rising ICP and seizures
ENA, 2010

The Key Problem:The Key Problem:
The combination of primary and secondary damage leads to compromised cerebral perfusion (CPP)

HOW IS CEREBRAL HOW IS CEREBRAL PERFUSION PERFUSION SUPPOSED SUPPOSED TO TO FUNCTION?FUNCTION?
(OR, How is the (OR, How is the alphabet soup alphabet soup supposed to look?)supposed to look?)

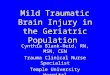
Normal Volume Normal Volume RelationshipsRelationships
• Contents of the skull are:–Cerebrospinal fluid (150 ml)
–Blood (1400 ml) –Brain tissue (1400 ml)
Holleran, 2010, p. 387

Skull ContentsSkull Contents
Brain Tissue
Venous Blood
ArterialBlood
CSF

Cerebral Blood Flow Cerebral Blood Flow AutoregulationAutoregulation
Arterial blood flow and volume is controlled by the autoregulation process◦Cerebral arteries constrict when systemic
BP rises or when PaCO2 decreases and PaO2 increases
◦Cerebral arteries dilate when systemic BP falls or when PaO2 decreases and PaCO2 increases
The brain has the ability to maintain constant blood flow with arterial pressures between 60 and150mmHg (MAP)
Holleran, 2010, p. 389

Pressure-Volume Pressure-Volume Relationships with Acute Relationships with Acute Brain Injury Brain Injury
• Any increase in the volume of one of the components within the skull without a decrease in the volume of the other two results in increased pressure
Holleran, 2010, p. 387

Autoregulation FailureAutoregulation Failure
As ICP increases, autoregulation fails, and CBF (cerebral blood flow) decreases, resulting in decreased tissue perfusion and ischaemia.
Decreased perfusion leads to cerebral hypoxia, which disrupts cellular metabolism and the blood-brain barrier
This leads to further cerebral oedema through fluid leaking from capillaries into brain tissue
ENA, 2010


Normal Cerebral PerfusionNormal Cerebral Perfusion
Brain receives about 15 to 35% of cardiac output
Goal is to maintain a cerebral perfusion pressure (CPP) between 70 and 90 mmHg
ENA, 2010

What’s so important about What’s so important about CPP?CPP? Brain lacks metabolic reserves and depends on arterial flow (cerebral perfusion) to meet it’s needs
Factors that influence CPP include: PaO2, PaCO2, cerebral blood volume, systemic BP, cerebral oedema and ICP.
ENA, 2010

Calculating Cerebral Calculating Cerebral Perfusion PressurePerfusion Pressure
CPP = MAP – ICP Compare to cardiac preload-afterload calculations:
MAP is like blood going in (preload)
ICP is like resistance to blood flow (afterload)

A Calculation Example:A Calculation Example:MAP = (2xDP)+SP 3
Normal BP: 120/70 2x70 = 140 + 120
= 260 260/3 = 87 MAP

How Do I Measure ICP How Do I Measure ICP Directly?Directly?
ICP monitor into the cranial cavity
Measured in mmHgNormally 7-15 mmHg for a healthy, supine adult
Only available in ICU or sometimes during interfacility transfers

Assessing ICP Without an ICP Assessing ICP Without an ICP MonitorMonitor
Since it isn’t always able to be directly measured in the air transfer environment, ICP may be indirectly assessed by physical findings
How do we assess ICP physiologically?


Signs of Increasing ICPSigns of Increasing ICP Early recognition of increased ICP is vital
to preserving brain function Early warnings: Change in LOC,
irritability, mild confusion, pupillary change and decreased Glasgow Coma Score.
Late: Very difficult to arouse, coma, posturing, fixed pupils or blown pupils and ECG changes, Cushings response Cushing triad is (systolic) hypertension
with widened pulse pressure, bradycardia and respiratory depression.
ENA, 2010

Brain Injury AssessmentBrain Injury Assessment
Level of consciousnessPupil size and reactivity
Cranial nerve activityMotor activityRespiratory pattern
Holleran, 2010, p. 315

Level of ConsciousnessLevel of ConsciousnessAlert – responds readily but may be
confusedLethargic – drowsy but can be arousedObtunded – difficult to arouse, cannot
make a complete sentence, requires repeated stimulation
Stuporous – no verbal response, may moan, responds to pain by moving extremities
Comatose – no evidence of awareness
Holleran, 2010, p. 315

Berry, 1995

Pupil ResponsePupil Response
Cranial nerve IIIInjury to parasympathetic system
dilates pupilsInjury to sympathetic system
constricts pupilsBilateral fixed and dilated pupils
usually indicate global hypoxia or herniation from cerebral oedema
Holleran, 2010, p. 317


Cranial Nerve ActivityCranial Nerve ActivityII Optic nerve
◦“can you see me?”III Oculomotor nerve
◦“look up, look down”, pupil response
XI Spinal accessory nerve ◦“shrug your shoulders”
XII Hypoglossal nerve ◦“stick out your tongue”


Motor ActivityMotor ActivityConscious patient
◦Grip your hands◦Push feet against your hands
Unconscious patient◦Motor activity in response to pain Purposeful withdrawal General extremity movement
Holleran, 2010, p 317

Respiratory PatternRespiratory PatternInitial hypoventilationCheyne-stokes (crescendo-de-
crescendo)Brainstem lesions – irregular,
shallow, slowing rateMedullary lesions – respiratory
paralysisCentral neurogenic
hyperventilationHolleran, 2010, p 318

Berry, 1995

Treatment of Increased Treatment of Increased ICPICP
Keep head midline with HOB elevated to 45°
Decrease stimulation Administer Mannitol or Frusemide
per order Sedate (neuromuscular blockades/
barbiturates): decreases the metabolic rate
Temperature control
ENA, 2010


Other Possible In-flight Other Possible In-flight InterventionsInterventions
• IV fluids to maintain BP over 90 systolic to perfuse brain
• Treat seizures as needed• Continue ventilation with 100% O2
to oxygenate brain • Initial (only) hyperventilation, to
lower ICP• Prolonged hyperventilation not
recommended unless:–Dilated pupils or Extensor posturing
Holleran, 2010, p 320


Conclusion - Alphabet Conclusion - Alphabet SoupSoup
Brain trauma (CHI) happensMaintaining cerebral perfusion
(CPP) is the goalCerebral oedema (ICP)
compromises cerebral perfusionAssessment for cerebral oedema
(PERL, LOC, GCS, RR)Treatment for cerebral oedema
(BP, O2, IV)


ReferencesReferences
Berry, S. (1995). I’m still not an ambulance driver. S. Berry, Publisher.
Emergency Nurses Association. (2010). http://www.ena.org/ coursesandeducation/CATNII-ENPC-TNCC/tncc/Pages/Default.aspx
Holleran, R. (2010). ASTNA Patient transport principles and practice (4th Edition). Mosby. St. Louis, Missouri.