Embed Size (px)
Citation preview
FLEX THERAPIST CEUs 1422 Monterey Street, Suite C-102
San Luis Obispo, Ca 93401
Ph (805) 543-5100 Fax (805) 543-5106
www.flextherapistceus.com
Shoulder - Glenohumeral & Scapulothoracic Rehab with Specific Consideration for Anterior
Capsulolabral Repairs & Throwing Injuries
Table of Contents
1. Glenohumeral/Scapulothoracic Rehab Pages 105 - 117
2. Anterior Joint Repair Rehab Pages 155 – 168
3. Shoulder Injuries in the Overhead Athlete Pages 38 - 54
journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 105
[ CLINICAL COMMENTARY ]
1Coordinator of Rehabilitation Research and Education, Department of Orthopedic Surgery, Division of Sports Medicine, Massachusetts General Hospital, Boston, MA; RehabilitationCoordinator/Assistant Athletic Trainer, Boston Red Sox Baseball Club, Boston, MA. 2Professor, Department of Physical Therapy, California State University, Sacramento, Sacramento,CA. 3Clinical Director, Champion Sports Medicine, Director of Rehabilitative Research, American Sports Medicine Institute, Birmingham, AL. Address correspondence to Dr MichaelM. Reinold, Rehabilitation Coordinator/Assistant Athletic Trainer, Boston Red Sox Baseball Club, Fenway Park, 4 Yawkey Way, Boston, MA 02215. Email: [email protected]
MICHAEL M. REINOLD, PT, DPT, ATC, CSCS¹ PT, PhD, CSCS, FACSM² PT, DPT³
Current Concepts in the Scientificand Clinical Rationale Behind
Exercises for Glenohumeral andScapulothoracic Musculature
The biomechanical analysis of rehabilitation exercises hasgained recent attention. As our knowledge of specific musclebiomechanics and function has increased, we have seena gradual progression towards more scientifically based
rehabilitation exercises. Several investigators have sought to describecommon rehabilitation exercises using kinematics, kinetics, andelectromyographic (EMG) data in an attempt to better understand theimplications of each exercise on the soft tissues of the glenohumeraland scapulothoracic joints. Advances in the understanding of
advantageous rehabilitation programs.The purpose of this paper is to provide
an overview of the biomechanical andclinical implications associated with therehabilitation of the glenohumeral andscapulothoracic joints. We will reviewthe function and biomechanics of eachmuscle, with specific emphasis on manycommonly performed rehabilitation ex-ercises. The goal of this is to provide theclinician with a thorough overview of theavailable information to develop safe,potentially effective, and appropriate ex-ercise programs for injury rehabilitationand prevention.
The rotator cuff has been shownto be a substantial dynamic stabiliz-er of the glenohumeral joint in mul-
tiple shoulder positions.49,88 Appropriaterehabilitation progression and strength-ening of the rotator cuff muscles areimportant to provide appropriate forceto help elevate and move the arm, com-press and center the humeral head withinthe glenoid fossa during shoulder move-ments (providing dynamic stability), andprovide a counterforce to humeral headsuperior translation resulting from del-
the biomechanical factors of rehabilita-tion have led to the enhancement ofrehabilitation programs that seekto facilitate recovery, while plac-ing minimal strain on specifichealing structures.
Though the fields of orthope-dics and sports medicine have evolved
to emphasize the necessity of evidence-based practice, few studies have been
conducted to determine the efficacyof specific shoulder rehabilitationexercises. Thus, knowledge ofanatomy, biomechanics, and func-
tion of specific musculature is criti-cal in an attempt to develop the most
The biomechanical analysis of re-habilitation exercises has led to more scientificallybased rehabilitation programs. Several investiga-tors have sought to quantify the biomechanics andelectromyographic data of common rehabilitationexercises in an attempt to fully understand theirclinical indications and usefulness. Furthermore,the effect of pathology on normal shoulder bio-mechanics has been documented. It is importantto consider the anatomical, biomechanical, andclinical implications when designing exercise
programs. The purpose of this paper is to providethe clinician with a thorough overview of the avail-able literature relevant to develop safe, effective,and appropriate exercise programs for injuryrehabilitation and prevention of the glenohumeraland scapulothoracic joints.
Level 5. J Orthop SportsPhys Ther 2009; 39(2):105-117. doi:10.2519/jospt.2009.2835
electromyography, infraspinatus,serratus anterior, supraspinatus, trapezius
106 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]toid activity (minimizing subacromialimpingement).6,8,9,21,34,50,60,65,74 In addi-tion, rotator cuff muscles are frequentlytreated either conservatively or surgicallysecondary to injuries.
Exercise designed to strengthen themuscles of the rotator cuff are often pre-scribed to patients with pathologies suchas subacromial impingement. Duringscapular plane abduction in healthy sub-jects, the humeral head translates 1 to 3mm in the superior direction from 0° to30° of abduction, slightly inferiorly from30° to 60° of abduction, and in the su-perior or inferior direction during 60° to90° of abduction.26,50,67 Other data dem-onstrate that, during passive scapularplane abduction, the humeral head trans-lates superiorly 0.6 to 1.8 mm between0° to 150°.25,26 But during active scapularplane abduction the humeral head re-mains nearly centered in the glenoid fos-sa throughout the range of movement.26
These data illustrate the importance ofrotator cuff strength and muscle balanceto resist humeral head superior transla-tion and help center the humeral headwithin the glenoid fossa during shoulderelevation.74 With rotator cuff pathology,altered kinematics and muscle activ-ity are present,31 and superior humeralhead translation increases and subacro-mial space decreases.24 Moreover, duringscapular plane shoulder abduction from30° to 90°, infraspinatus and subscapu-laris activity was found to be significantlyless in individuals with subacromial im-pingement compared to those withoutimpingement.68
Subjects with shoulder laxity and in-stability have also been shown to havealtered kinematics and firing patterns ofthe rotator cuff.7,35,45,46,55,64,72 Compared tohealthy subjects, patients with general-ized joint laxity demonstrated increasedsubscapularis activity during internalrotation (IR) exercise and decreased su-praspinatus and subscapularis activityduring external rotation (ER) exercise.7,43
Compared to healthy subjects, those withanterior instability exhibited less su-praspinatus activity between 30° to 60°
of shoulder elevation during abductionand scaption exercises.59
These EMG data clearly illustrateaberrant muscle-firing patterns in in-dividuals with shoulder pathology. It isoften the goal of rehabilitation special-ists to prescribe exercises to normalize orprevent these abnormal firing patterns.Proper selection of exercises to activatemuscle function for each muscle of therotator cuff should be considered duringrehabilitation.
The supraspinatus compresses, abducts,and generates a small ER torque to theglenohumeral joint. Supraspinatus activi-ty increases as resistance increases duringabduction/scaption movements, peakingat 30° to 60° of elevation for any givenresistance. At lower elevation angles, su-praspinatus activity increases, providingadditional humeral head compressionwithin the glenoid fossa to counter thehumeral head superior translation occur-ring with contraction of the deltoid.1 Dueto a decreasing moment arm with abduc-tion, the supraspinatus is a more effectiveabductor in the scapular plane at smallerabduction angles.34,50,65
Relatively high supraspinatus activityhas been measured in several commonrotator cuff exercises3,5,17,33,54,63,70,75,79,87
and in several exercises that are notcommonly thought of as rotator cuff ex-ercises, such as standing forward scap-ular punch, rowing exercises, push-upexercises, and 2-hand overhead medi-cine ball throws.13,17,32,81 These resultssuggest the importance of the rotatorcuff in providing dynamic glenohumeralstability by centering the humeral headwithin the glenoid fossa during all up-per extremity functional movements.This is an important concept for theclinician to understand. The muscle’sability to generate abduction torque inthe scapular plane appears to be great-est with the shoulder in neutral rotationor in slight IR or ER.50,65 This biome-chanical advantage has led to the devel-opment of exercises in the plane of the
scapula to specifically strengthen thesupraspinatus.38
Jobe38 was the first to recommend ele-vation in the scapular plane (30° anteriorto the frontal plane) with glenohumer-al IR, or the “empty can” exercise, tostrengthen the supraspinatus muscle.Other authors37,40,66,69,70,77 have suggestedthe “full can” position, or elevation in thescapular plane with glenohumeral ER,to best strengthen and test the supraspi-natus muscle. Furthermore, comparedto the empty can exercise, Blackburn5
reported significantly greater supraspi-natus activity during prone horizontalabduction at 100° with full ER, or pronefull can, position. The results of studiescomparing these exercises provide in-consistent results due to methodologicallimitations, including lack of statisticalanalysis,38,79 lack of data for all 3 exercis-es,40,54,79,87 and absence of data on deltoidmuscle activity.87
Recently, Reinold et al69 comprehen-sively evaluated the EMG signal of thesupraspinatus and deltoid musculatureduring the full can, empty can, andprone full can exercises in an attemptto clarify the muscular activation duringthese exercises. The results showed thatall 3 exercises provide a similar amountof supraspinatus activity ranging from62% to 67% of maximal voluntary iso-metric contraction (MVIC). However,the full can exercise demonstrated asignificantly lower amount of middleand posterior deltoid activity comparedto the 2 other exercises. This is clinicallysignificant when trying to strengthenthe supraspinatus while simultaneouslyminimizing potentially disadvanta-geous superior sheer force due to del-toid activity.
In patients with shoulder pain,weakness of the rotator cuff, or inef-ficient dynamic stabilization, it is theauthors’ opinion that activities thatproduce higher levels of deltoid activ-ity in relation to supraspinatus activity,such as the empty can and prone fullcan exercise, may be detrimental. Thisis due to the increased amount of supe-
journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 107
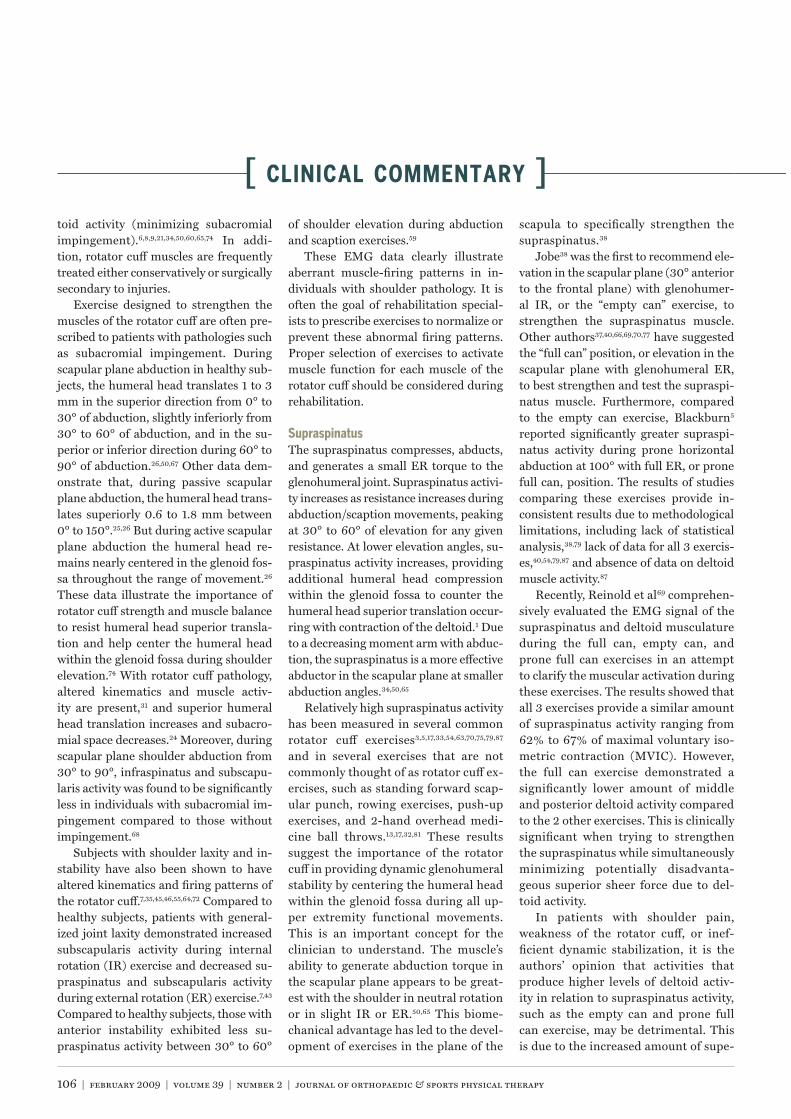
rior humeral head migration that maybe observed when the rotator cuff doesnot adequately compress the humeruswithin the glenoid fossa to counteract,or oppose, the superior pull of the del-toid ( ).61 Poppen and Walker66
have shown that the empty can exerciseresults in a greater superior-orientatedforce vector than the full can exercise( ). This superior humeral headmigration may result in subacromialimpingement, subdeltoid bursa trauma,
bursal thickening, and may result intendon degeneration and eventual fail-ure.21 Clinically, superior humeral headmigration may be disadvantageous topatients with rotator cuff pathology ora deficiency in glenohumeral dynamicstabilization that are symptomatic. Thismay partially explain why the empty canposition often elicits a certain amountof pain and discomfort in patients.
In addition to the altered ratio of su-praspinatus to deltoid muscle activity,
there are several reasons why the fullcan exercise may be preferred over theempty can exercise during rehabilitationand supraspinatus testing. Anatomically,the IR of the humerus during the emptycan exercise does not allow the greatertuberosity to clear from under the acro-mion during arm elevation, which mayincrease subacromial impingement riskbecause of decreased subacromial spacewidth.15,23,71
Biomechanically, shoulder abductionperformed in extreme IR progressivelydecreases the abduction moment arm ofthe supraspinatus from 0° to 90° of ab-duction.50 A diminished mechanical ad-vantage may result in the supraspinatusneeding to generate more force, thus in-creasing the tensile stresses in the injuredor healing tendon. This may also makethe exercise more challenging for patientswith weakness, facilitating compensatorymovements such as a shoulder “shrug.”
Scapular kinematics are also differentbetween these exercises, with scapularIR, or “winging” (which occurs in thetransverse plane with the scapular me-dial border moving posterior away fromthe trunk) and anterior tilt (which occursin the sagittal plane with the scapular in-ferior angle moving posterior away fromthe trunk) being greater with the emptycan compared to the full can exercise.78
This occurs in part because IR of thehumerus in the empty can position ten-sions both the posteroinferior capsule ofthe glenohumeral joint and the rotatorcuff (primarily the infraspinatus). Ten-sion in these structures contributes toanterior tilt and IR of the scapula, whichcontribute to scapular protraction. Thisis clinically important because scapularprotraction has been shown to decreasethe width of the subacromial space, in-creasing the risk of subacromial impinge-ment.76 In contrast, scapular retractionhas been shown to both increase sub-acromial space width76 and increase su-praspinatus strength potential (enhancedmechanical advantage), when comparedto a more protracted position.41 Thesedata also emphasize the importance of
Direction of the magnitude of the resultant force vector for different glenohumeral joint positions as afunction of different muscle activity, (A) deltoid activity, (B) rotator cuff activity, (C) combined deltoid and rotatorcuff activity. Reprinted with permission from Morrey et al.61
The position of the resultant force vector of the rotator cuff and deltoid for different positions of armelevation with (N) neutral rotation, (I) internal rotation, and (X) external rotation. Reprinted with permission fromPoppen and Walker.66

108 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]until it is about 1.3 cm at 60° abduction.65
These data imply that the infraspinatus isa more effective external rotator at lowershoulder abduction angles. The teres mi-nor has a relatively constant ER momentarm (approximately 2.1 cm) and the abil-ity to generate torque throughout shoul-der abduction movement, which impliesthat shoulder abduction angle does notaffect the effectiveness of the teres minorto generate ER torque.65
Several studies have been designed totest the results of the model; but, as instudies on the supraspinatus, variationsin experimental methodology have result-ed in conflicting results and controversyin exercise selection.3,5,17,19,27,33,44,54,63,70,77,79,81
Several exercises have been recommend-ed based on EMG data, including shoul-der ER in the side-lying,3,70,79 standing,27,70
or prone3,70 positions performed at 0°,3,70
45°,27,70 and 90°3,70 of abduction. Anotherexercise that has been shown to generatea high EMG signal of the infraspinatusand teres minor is prone horizontal ab-duction with ER.5,79
Reinold et al70 analyzed several dif-ferent exercises commonly used tostrengthen the shoulder external rota-tors to determine the most effectiveexercise and position to recruit muscleactivity of the posterior rotator cuff. Theauthors report that the exercise that elic-ited the most combined EMG signal forthe infraspinatus and teres minor wasshoulder ER in side-lying (infraspina-tus, 62% maximal voluntary isometriccontraction [MVIC]; teres minor, 67%MVIC), followed closely by standing ERin the scapular plane at 45° of abduction(infraspinatus, 53% MVIC; teres minor,55% MVIC), and finally prone ER in the90° abducted position (infraspinatus,50% MVIC; teres minor, 48% MVIC).
Exercises in the 90° abducted posi-tion are often incorporated to simulatethe position and strain on the shoulderduring overhead activities such as throw-ing. This position produced moderateactivity of the external rotators but alsoincreased activity of the deltoid and su-praspinatus. It appears that the amount
of infraspinatus and teres minor activityprogressively decreases as the shouldermoves into an abducted position, whileactivity of the supraspinatus and deltoidincreases. This suggests that as the armmoves into a position of increased vulner-ability away from the body, the supraspi-natus and deltoid are active to assist inthe ER movement, while providing somedegree of glenohumeral stability throughmuscular contraction.
While standing ER exercises per-formed at 90° of shoulder abduction mayhave a functional advantage over exercis-es performed at 0° of shoulder abductionor performed in the scapular plane, dueto the close replication in sporting activi-ties, the combination of shoulder abduc-tion and ER places strain on the shouldercapsule, particularly the anterior band ofthe inferior glenohumeral ligament.30,85,86
The clinician must carefully consider thiswhen designing programs for patientswith capsulolabral pathology.
Side-lying ER may be the optimal ex-ercise to strengthen the external rotatorsbased on the previously mentioned stud-ies. The inclusion of this exercise shouldbe considered in all exercise programsattempting to increase ER strength ordecrease capsular strain.
Theoretically, ER performed at 0° ofshoulder abduction with a towel roll be-tween the rib cage and the arm providesboth the low capsular strain and also agood balance between the muscles thatexternally rotate the arm and the musclesthat adduct the arm to hold the towel.Our clinical experience has shown thatadding a towel roll to the ER exerciseprovides assistance to the patient by en-suring that proper technique is observedwithout muscle substitution. Reinold etal70 report that adding a towel roll to theexercise consistently exhibited a tendencytowards higher activity of the posteriorrotator cuff muscles as well. An increaseof 20% to 25% in EMG signal of the in-fraspinatus and teres minor was notedwhen using the towel roll compared tono towel roll.
What is not readily apparent is the
strengthening the scapular retractors andmaintaining a scapular retracted postureduring shoulder exercises. The authorsroutinely instruct patients to emphasizean upright posture and a retracted posi-tion of the scapula during all shoulderand scapula strengthening exercises.
Thus, the full can exercise appears tobe the most advantageous exercise whilethe empty can exercise is not commonlyrecommended. The prone full can exer-cise warrants further consideration be-cause the exercise results in greater EMGsignal of the posterior deltoid than themiddle deltoid, which may result in lesssuperior sheer force. The prone full canexercise may also be beneficial because ofscapular muscle recruitment.
The infraspinatus and teres minor com-prise the posterior cuff, which providesglenohumeral compression and resistssuperior and anterior humeral headtranslation by exerting an inferoposteri-or force on the humeral head.74 The pos-terior cuff muscles provide glenohumeralER, which functionally helps clear thegreater tuberosity from under the cora-coacromial arch during overhead move-ments, thus minimizing subacromialimpingement.
Based on 3-D biomechanical shouldermodels, the maximum predicted isomet-ric infraspinatus force was 723 N for ERat 90° of abduction and 909 N for ER at0° of abduction.34 The maximum predict-ed teres minor force was much less thanfor the infraspinatus during maximumER at both 90° (111 N) and 0° abduction(159 N).34 The effectiveness of the musclesof the posterior rotator cuff to externallyrotate the arm depends on glenohumeralposition. The superior, middle, and infe-rior heads of the infraspinatus have theirlargest ER moment arm (approximate-ly 2.2 cm) and generate their greatesttorque at 0° abduction.65 As the abduc-tion angle increases, the moment arms ofthe inferior and middle heads stay rela-tively constant, while the moment arm ofthe superior head progressively decreases

journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 109
significant role of the infraspinatus asa shoulder abductor in the scapularplane.34,50,65 From 3-D biomechanicalshoulder models, predicted infraspina-tus force during maximum isometriceffort scapular plane abduction (90°position) was 205 N, nearly twice thepredicted force from the supraspinatusin this position.34 Liu et al50 reportedthat in scapular plane abduction withneutral rotation the infraspinatus has anabductor moment arm that was small at0° abduction, but increased to 1 cm at15° abduction, and remained fairly con-stant throughout increasing abductionangles. Moreover, infraspinatus activityincreases as resistance increases, peakingat 30° to 60° for any given resistance.1 Asresistance increases, infraspinatus activ-ity increases to help generate a highershoulder scapular abduction torque, and,at lower elevation angles, infraspinatusactivity increases to resist superior hu-meral head translation due to the actionof the deltoid.74
In contrast to the infraspinatus, theteres minor generates a weak shoulderadductor torque due to its relativelylower attachments to the scapula and hu-merus.34,50,65 A 3-D biomechanical mod-el of the shoulder reveals that the teresminor does not generate scapular planeabduction torque when it contracts, but,rather, generates an adduction torqueand 94 N of force during maximum effortscapular plane adduction.34 In addition,Otis et al65 reported that the adductormoment arm of the teres minor was ap-proximately 0.2 cm at 45° of IR and ap-proximately 0.1 cm at 45° of ER. Thesedata imply that the teres minor is a weakadductor of the humerus, regardless ofthe rotational position of the humerus.In addition, because of its posterior posi-tion at the shoulder, it also helps gener-ate a weak horizontal abduction torque.Therefore, although its activity is simi-lar to the infraspinatus during ER, it ishypothesized that the teres minor wouldnot be as active as the infraspinatus dur-ing scapular abduction, abduction, andflexion movements, but would show ac-
tivity similar to that of the infraspina-tus during horizontal abduction. Thishypothesis is supported by EMG andmagnetic resonance imaging data, whichshow that teres minor activity duringflexion, abduction, and scapular abduc-tion is drastically less than infraspinatusactivity.1,3,5,54,77,79 Even though the teresminor generates an adduction torque, itis active during these different elevation-type movements, as it likely acts to en-hance joint stability by resisting superiorhumeral head translation and providinghumeral head compression within theglenoid fossa.74 This is especially likelythe case at lower shoulder abductionangles and when abduction and scapu-lar abduction movements are performedagainst greater resistance.1 In contrast tothe movements of shoulder abduction,scapular abduction, and flexion, teres mi-nor activity is much higher during pronehorizontal abduction at 100° abductionwith ER, exhibiting similar activity as theinfraspinatus.5,54,70,77,79
The subscapularis provides glenohumer-al compression, IR, and anterior stabilityof the shoulder. From 3-D biomechanicalshoulder models, predicted subscapu-laris force during maximum effort IRwas 1725 N at 90° abduction and 1297N at 0° abduction.34 Its superior, middle,and inferior heads all have their larg-est IR moment arm (approximately 2.5cm) and torque generation at 0° abduc-tion.65 As the abduction angle increases,the moment arms of the inferior andmiddle heads stay relatively constant,while the moment arm of the superiorhead progressively decreases until it isabout 1.3 cm at 60° abduction.65 Thesedata imply that the upper portion of thesubscapularis muscle (innervated by theupper subscapularis nerve) may be amore effective internal rotator at lowerabduction angles compared to higher ab-duction angles. However, there is no sig-nificant difference in upper subscapularisactivity among IR exercises performed at0°, 45°, or 90° abduction.17,39 Abduction
angle does not appear to affect the abilityof the lower subscapularis (innervated bythe lower subscapularis nerve) to gener-ate IR torque.65 However, lower sub-scapularis muscle activity is affected byabduction angle, where some EMG datashow significantly greater activity withIR at 0° abduction compared to IR at 90°abduction,17 while EMG data of anotherstudy show greater activity with IR ex-ercise performed at 90° compared to 0°abduction.39 Performing IR at 0° abduc-tion produces similar amounts of upperand lower subscapularis activity.17,28,39
Although biomechanical data remaininconclusive as to which position to per-form IR exercises (0° versus 90° abduc-tion), during IR at 0° abduction the actionof the subscapularis is assisted by severallarge muscles, such as the pectoralis ma-jor, latissimus dorsi, and teres major.17
Clinically, this may allow for compensa-tion of larger muscles during the exercisein the presence of subscapularis weak-ness. Decker et al17 demonstrated that IRat 90° abduction produced less pectoralismajor activity compared to 0° abduction.The authors’ findings revealed that pecto-ralis major and latissimus dorsi activityincreased when performing IR exercisesin an adducted position or while mov-ing into an adducted position during theexercise. Thus, IR at 90° abduction maybe performed if attempting to strengthenthe subscapularis while minimizing larg-er muscle group activity.
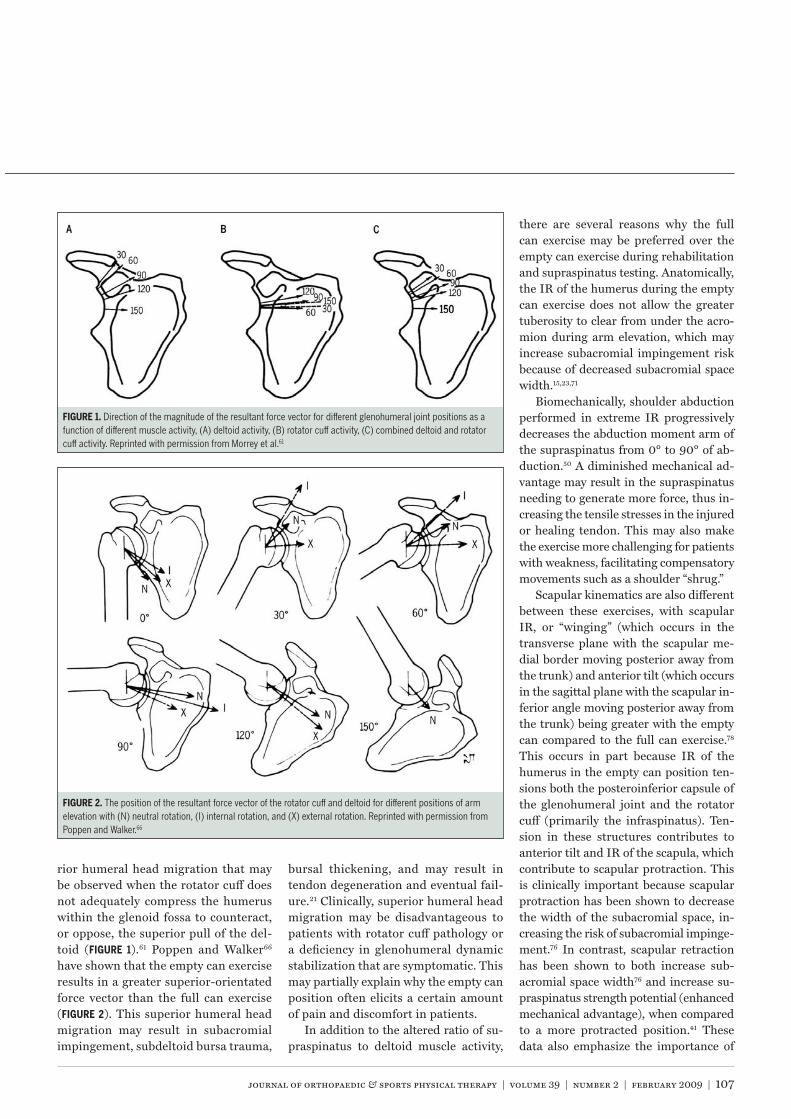
The subscapularis is active in numer-ous shoulder exercises other than specificIR of the shoulder. Decker et al17 reportedhigh subscapularis activity during thepush-up with plus and dynamic-hug ex-ercises. These authors also described an-other exercise that consistently producedhigh levels of subscapularis activity, whichthey called the “diagonal exercise” (3). Relatively high subscapularis activ-ity has been measured while performingside-lying shoulder abduction, standingshoulder extension from 90° to 0°, mili-tary press, D2 diagonal proprioceptiveneuromuscular facilitation (PNF) patternflexion and extension, and PNF scapular

110 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
clock, depression, elevation, protraction,and retraction movements.17,33,44,63,75,79
The subscapularis also generatesan abduction torque during arm eleva-tion.50,65 From 3-D biomechanical shoul-der models, predicted subscapularis forceduring maximum effort scapular planeabduction at 90° was 283 N, approxi-mately 2.5 times the predicted force forthe supraspinatus in this position.34 Thiswas similar to that of the infraspinatus,highlighting the theoretical force couplethat the 2 muscles provide to center thehumeral head within the glenoid fossaduring abduction. Liu et al50 reportedthat in scapular plane abduction withneutral rotation the subscapularis had apeak abductor moment arm of 1 cm at 0°abduction, which slowly decreased to 0cm at 60° abduction. Moreover, the ab-ductor moment arm of the subscapularisgenerally decreased as abduction was per-formed with greater shoulder IR,50 suchas performing the empty can exercise. Incontrast, the abductor moment arm ofthe subscapularis generally increased asabduction was performed with greatershoulder ER, similar to performing thefull can exercise.
Otis et al65 reported that the superior,middle, and inferior heads of the sub-
scapularis all have an abductor momentarm (greatest for the superior head andleast for the inferior head) that varies as afunction of humeral rotation. The lengthsof the moment arm for the 3 muscle headsare approximately 0.4 to 2.2 cm at 45° ofER, 0.4 to 1.4 cm in neutral rotation, and0.4 to 0.5 cm at 45° of IR. These data sug-gest that the subscapularis is most effec-tive as a scapular plane abductor with theshoulder in ER and least effective withthe shoulder in IR. Therefore, the simul-taneous activation of the subscapularisand infraspinatus during arm elevationgenerates both an abductor moment andan inferiorly directed force to the humer-al head to resist superior humeral headtranslation.74 In addition, a simultane-ous activation neutralizes the IR and ERtorques these muscles generate, furtherenhancing joint stability.
DELTOID
The deltoid plays an importantrole in shoulder biomechanics andduring glenohumeral and scapu-
lothoracic exercises. Extensive researchhas been conducted on deltoid activityduring upper extremity weight-liftingexercises, such as bench press, dumb-
bell flys, military press, and push-ups.4,13,16,19,44,57,63,79,81,83
The abductor moment arm is ap-proximately 0 cm for the anterior del-toid and 1.4 cm for the middle deltoidwhen the shoulder is in 0° abductionand neutral rotation in the scapularplane.50,65 The magnitude of these mo-ment arms progressively increases withshoulder abduction, such that, by 60°of abduction, they are approximately1.5 to 2 cm for the anterior deltoid and2.7 to 3.2 cm for the middle deltoid.From 0° to 40°of abduction the momentarms for the anterior and middle del-toids are less than the moment arms forthe supraspinatus, subscapularis, andinfraspinatus.50,65 These data suggestthat the anterior and middle deltoidare not effective shoulder abductors atlow abduction angles and the shoulderin neutral rotation, especially the ante-rior deltoid. This is in contrast to thesupraspinatus and to a lesser extent theinfraspinatus and subscapularis, whichare more effective shoulder abductorsat low abduction angles. These biome-chanical data are consistent with EMGdata, in which anterior and middle del-toid activity generally peaks between60° to 90° of abduction in the scapularplane, while supraspinatus, infraspina-tus, and subscapularis activity generallypeaks between 30° and 60° of shoulderabduction in the scapular plane.1
The abductor moment arm for theanterior deltoid changes considerablywith humeral rotation, increasing withER and decreasing with IR.50 At 60° ERand 0° abduction, a position similar tothe beginning of the full can exercise, theanterior deltoid moment arm is 1.5 cm(compared to 0 cm in neutral rotation),which makes the anterior deltoid an ef-fective abductor even at small abductionangles.50 By 60° abduction with ER, itsmoment arm increased to approximately2.5 cm (compared to approximately 1.5to 2 cm in neutral rotation).50 In con-trast, at 60° IR at 0° abduction, a po-sition similar to the beginning of theempty can exercise, its moment arm was
Diagnonal exercise for the subscapularis begins in shoulder external rotation at 90° abduction in thecoronal plane (A) and internal rotation and horizontal adduction are performed simultaneously (B), similar to atennis swing.

journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 111
0 cm (the same as with neutral rotation),which suggests that in this positionthe anterior deltoid is not an effectiveabductor.50
It has been reported that, given a peakisometric abduction torque of 25 N·m at0° abduction and neutral rotation, up to35% to 65% of this torque may be gener-ated by the middle deltoid, 30% by thesubscapularis, 25% by the supraspinatus,10% by the infraspinatus, 2% by the an-terior deltoid, and 0% by the posteriordeltoid.50 Interestingly, the rotator cuffprovides a significant contribution to theabduction torque. The ineffectivenessof the anterior and posterior deltoids togenerate abduction torque with neutralrotation may appear surprising.50,65 How-ever, it is important to understand thatthe low abduction torque for the anteriordeltoid does not mean that this muscle isonly minimally active. In fact, because theanterior deltoid has an abductor momentarm near 0 cm, the muscle could be veryactive and generate very high force butvery little torque (in 0° abduction thisforce attempts to translate the humeralhead superiorly).
The aforementioned torque data arecomplemented and supported by muscleforce data from Hughes and An.34 Theseauthors reported predicted forces fromthe deltoid and rotator cuff during maxi-mum effort abduction with the arm 90°abducted and in neutral rotation. Poste-rior deltoid and teres minor forces wereonly 2 N and 0 N, respectively, whichfurther demonstrates the ineffectivenessof these muscles as shoulder abductors.In contrast, middle deltoid force was thehighest at 434 N, which suggests a highcontribution of this muscle during abduc-tion. The anterior deltoid generated thesecond highest force of 323 N. This mayappear surprising given the low abductortorque for this muscle reported above,but it should be re-emphasized that forceand torque are not the same, and that theshoulder was positioned at 90° abductionin the study by Hughes and An,34 in con-trast to 0° abduction in the study by Liuet al.50 As previously mentioned, the mo-
ment arm of the anterior deltoid progres-sively increases as abduction increases,and it becomes a more effective abduc-tor. It is also important to rememberthat muscle force is generated not only togenerate joint torque, but also to providestabilization, such as joint compression.Also of interest is the 608-N force that,collectively, the subscapularis (283 N),infraspinatus (205 N), and supraspinatus(117 N) generate. These larges forces aregenerated not only to abduct the shoul-der but also to compress and stabilizethe joint, and neutralize the superiorlydirected force generated by the deltoid atlower abduction angles.
It should also be noted that deltoidmuscle force in different shoulder posi-tions may also affect shoulder stability.All 3 heads of the deltoid generate a forcethat increases shoulder stability at 60°abduction in the scapular plane (helps tostabilize the humeral head in the glenoidfossa) but decreases shoulder stability at60° abduction in the frontal plane (tendsto translate the humeral head anterior).48
These data provide evidence for the useof scapular abduction exercises instead ofabduction exercises for individuals withanterior instability.
Thus, it appears that the 3 heads ofthe deltoid have different roles duringupper extremity movements and, there-fore, different implications for exerciseselection. The middle deltoid may havethe most significant impact on superiorhumeral head migration, and exerciseswith high levels of middle deltoid activity(as well as anterior deltoid activity), suchas the empty can exercise, should likelybe minimized for most patients. Con-versely, high levels of posterior deltoidactivity may not be as disadvantageousas high levels of middle or anterior del-toid activity. It does not appear that theposterior deltoid has a significant role inproviding abduction or superior humeralhead migration. Thus, exercises such asthe prone full can, which generates highlevels of rotator cuff and posterior deltoidactivity, may be both safe and effective forrotator cuff strengthening.
The primary muscles that con-trol scapular movements include thetrapezius, serratus anterior, levator
scapulae, rhomboids, and pectoralis mi-nor. Appropriate scapular muscle strengthand balance are important because thescapula and humerus move together incoordination during arm movement,referred to as scapulohumeral rhythm.During humeral elevation, the scapulaupwardly rotates in the frontal plane,rotating approximately 1° for every 2°of humeral elevation until 120° humeralelevation, and thereafter rotates approxi-mately 1° for every 1° humeral elevationuntil maximal arm elevation, achievingat least 45° to 55° of upward rotation.52,58
During humeral elevation, in addition toscapular upward rotation, the scapula alsonormally tilts posteriorly approximately20° to 40° in the sagittal plane and exter-nally rotates approximately 15° to 35° inthe transverse plane.52,58
When the normal 3-D scapular move-ments are disrupted by abnormal scapularmuscle-firing patterns, fatigue, or injury,it has been hypothesized that the shouldercomplex functions less efficiently, leadingto injuries to the shoulder, including theglenohumeral joint.10,11,12,18,58,76,80,82 Duringarm elevation in the scapular plane, in-dividuals with subacromial impingementexhibit decreased scapular upward rota-tion, increased scapular IR (winging) andanterior tilt, and decreased subacromialspace width, compared to those withoutsubacromial impingement.24,51 Alteredscapular muscle activity is commonly as-sociated with impingement syndrome.For example, upper and lower trapeziusactivity increased and serratus anterioractivity decreased in individuals with im-pingement as compared to those withoutimpingement.51 Therefore, it is importantto include the scapulothoracic muscula-ture in the rehabilitation of patients withshoulder pathology.42
The serratus anterior works with the

112 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
pectoralis minor to protract the scapulaand with the upper and lower trapeziusto upwardly rotate the scapula. The ser-ratus anterior is an important muscle be-cause it contributes to all components ofnormal 3-D scapular movements duringarm elevation, which includes upwardrotation, posterior tilt, and external ro-tation.52,58 The serratus anterior is alsoimportant in athletics, such as duringoverhead throwing, to accelerate thescapula during the acceleration phase ofthrowing. The serratus anterior also helpsstabilize the medial border and inferiorangle of the scapula, preventing scapularIR (winging) and anterior tilt.
Several exercises elicit high serratusanterior activity, such as D1 and D2 di-agonal PNF pattern flexion, D2 diagonalPNF pattern extension, supine scapularprotraction, supine upward scapularpunch, military press, push-up plus, gle-nohumeral IR and ER at 90° abduction,and shoulder flexion, abduction, and
scaption with ER above 120°.16,20,32,62,63
Serratus anterior activity tends to increasein a somewhat linear fashion with arm el-evation.2,20,29,52,62 However, increasing armelevation increases subacromial impinge-ment risk,15,71 and arm elevation at lowerabduction angles also generates relativelyhigh serratus anterior activity.20
It is interesting that performingshoulder IR and ER at 90° of abductiongenerates relatively high serratus ante-rior activity, because these exercises areusually thought to primarily work rotatorcuff muscles.20,63 However, during IR andER at 90° abduction the serratus ante-rior helps stabilize the scapula. It shouldbe noted that the rotator cuff musclesalso act to move the scapula (where theyoriginate) in addition to the humerus.For example, the force exerted by the su-praspinatus at the supraspinous fossa hasthe ability to downwardly rotate the scap-ula if this force is not counterbalanced bythe scapulothoracic musculature.
Not surprising is high serratus ante-rior activity generated during a push-upexercise. When performing the stan-dard push-up, push-up on knees, andwall push-up, serratus anterior activityis greater when full scapular protrac-
tion occurs after the elbows fully extend(push-up plus).53 Moreover, serratusanterior activity was lowest in the wallpush-up plus, exhibited moderate activi-ty during the push-up plus on knees, andrelatively high activity during the stan-dard push-up plus.16,53 Compared to thestandard push-up, performing a push-up plus with the feet elevated producedsignificantly greater serratus anterioractivity.47 These findings demonstratethat serratus anterior activity increasesas the positional (gravitational) chal-lenge increases.
Decker et al16 compared several com-mon exercises designed to recruit the ser-ratus anterior. The authors identified thatthe 3 exercises that produced the great-est serratus anterior EMG signal were thepush-up with a plus, dynamic hug (4), and punch exercises (similar to a jab-bing protraction motion).
Ekstrom20 also looked at the activityof the serratus anterior during commonexercises. His data indicated that theserratus anterior is more active whenperforming a movement that simultane-ously creates scapular upward rotationand protraction, as with the serratus an-terior punch performed at 120° of abduc-
Dynamic hug exercise for the serratusanterior begins with the elbows in approximately 45°of flexion, the shoulder abducted 60° and internallyrotated 45° (A). The humerus is then horizontallyadducted by following an arc movement similar toa hugging action, until full shoulder protraction isreached (B).
Bilateral serratus anterior punch to 120° abduction begins with hands by the side (A) before extendingelbows and elevating shoulders up to 120° of elevation and full protraction (B).

journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 113
tion and during a diagonal exercise thatincorporated protraction with shoulderflexion, horizontal adduction, and exter-nal rotation. It appears that the punch ex-ercise can be enhanced by starting at 0°abduction and extending the elbow, whileelevating and protracting the shoulder( ).
Hardwick et al29 compared the wallpush-up plus, full can, and a wall slideexercise. The wall slide begins by slightlyleaning against the wall with the ulnarborder of the forearms in contact withthe wall, elbows flexed 90°, and shoul-ders abducted 90° in the scapular plane.From this position the arms slide up thewall in the scapular plane, while leaninginto the wall. Interestingly, the wall slideproduce similar serratus anterior activitycompared to scapular abduction above120° abduction with no resistance. Oneadvantage of the wall slide compared toscapular abduction is that, anecdotally,patients report that the wall slide is lesspainful to perform.29 This may be be-cause during the wall slide the upper ex-tremities are supported against the wall,making it easier to perform while also as-sisting with compression of the humeralhead within the glenoid. Thus, this maybe an effective exercise to perform dur-ing the earlier protective phases of somerehabilitation programs.
General functions of the trapezius includescapular upward rotation and elevationfor the upper trapezius, retraction for themiddle trapezius, and upward rotationand depression for the lower trapezius.In addition, the inferomedial-directedfibers of the lower trapezius may alsocontribute to posterior tilt and externalrotation of the scapula during arm eleva-tion,52 which decreases subacromial im-pingement risk24,51 and makes the lowertrapezius an important area of focus inrehabilitation. Relatively high uppertrapezius activity occurs in the shouldershrug, prone rowing, prone horizontalabduction at 90° and 135° of abductionwith ER and IR, D1 diagonal PNF pat-
tern flexion, standing scapular dynamichug, PNF scapular clock, military press,2-hand overhead medicine ball throw,and scapular abduction and abductionbelow 80°, at 90°, and above 120° withER.13,16,20,62,75 During scapular abduction,upper trapezius activity progressively in-creases from 0° to 60°, remains relativelyconstant from 60° to 120°, and contin-ues to progressively increase from 120°to 180°.2
Relatively high middle trapezius ac-tivity occurs with shoulder shrug, pronerowing, and prone horizontal abductionat 90° and 135° abduction with ER andIR.20,62 Some authors have reported rela-tively high middle trapezius activity dur-ing scapular abduction at 90° and above120°,2,16,20 while authors of another studyshowed low EMG signal amplitude of themiddle trapezius during this exercise.62
Relatively high lower trapezius activityoccurs in the prone rowing, prone hori-zontal abduction at 90° and 135° abduc-tion with ER and IR, prone and standingER at 90° abduction, D2 diagonal PNFpattern flexion and extension, PNF scap-ular clock, standing high scapular rows,and scapular abduction, flexion, and ab-duction below 80° and above 120° withER.20,62,63,75 Lower trapezius activity tendsto be relatively low at angles less than 90°of scapular abduction, abduction, andflexion, and then increases exponentially
from 90° to 180°.2,20,29,62,75,84 Significantlygreater lower trapezius activity has beenreported during the prone ER at 90° ab-duction exercise compared to the emptycan exercise.3 As previously mentioned,the lower trapezius is an extremely im-portant muscle in shoulder function dueto its role in scapular upward rotation,external rotation, and posterior tilt.
Ekstrom et al20 reported that the great-est EMG signal amplitude of the lowertrapezius occurred during the prone fullcan, prone ER at 90°, and prone horizon-tal abduction at 90° with ER exercises.Based on these results, it appears thatthe prone full can exercise should not beperformed at a set degree of abduction,but should be individualized based on thealignment of the lower trapezius fibers( ). In the authors’ experience, thisis typically around 120° of abduction butmay fluctuate, depending on the specificpatient and body type.
It is often clinically beneficial to en-hance the ratio of lower trapezius-to-up-per trapezius strength.11 In the opinion ofthe authors, poor posture and muscle im-balance often seen in patients with a va-riety of shoulder pathologies is often theresult of poor muscle balance betweenthe upper and lower trapezius, with theupper trapezius being more dominant.McCabe et al56 report that bilateral ERat 0° abduction resulted in the greatestlower trapezius-upper trapezius ratiocompared to several other similar trape-zius exercises ( ). Cools et al11 alsoidentified side-lying ER and prone hori-zontal abduction at 90° abduction andER as 2 beneficial exercises to enhancethe ratio of lower trapezius to upper tra-pezius activity.
Both the rhomboids and levator scap-ulae function as scapular retractors,downward rotators, and elevators. Ex-ercises used to strengthen rotator cuffand scapulothoracic musculature arealso effective in eliciting activity of therhomboids and levator scapulae. Rela-tively high rhomboid activity has been
The proper alignment of the upperextremity during the prone horizontal abductionexercise with external rotation. Note how the upperextremity is aligned with the muscle fiber orientationof the lower trapezius.

114 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
reported during D2 diagonal PNF pat-tern flexion and extension, standingshoulder ER at 0° and 90° abduction,standing shoulder IR at 90° abduction,standing shoulder extension from 90°to 0°, prone shoulder horizontal abduc-tion at 90° abduction with IR, scapularabduction, abduction, and shoulder flex-ion above 120° with ER, prone rowing,and standing high, mid, and low scapu-lar rows.62,63 Relatively high rhomboidsand levator scapulae activity has beenreported with scapular abduction above120° with ER, prone horizontal abduc-tion at 90° abduction with ER and IR,prone rowing, and prone extension at90° flexion.62 Therefore, the prone ex-tension exercise may be performed inaddition to many of the previously men-tioned exercises for other scapulotho-racic muscles. Other specific exercisesto activate the rhomboids and levatorscapulae muscles are not often neces-sary to perform.
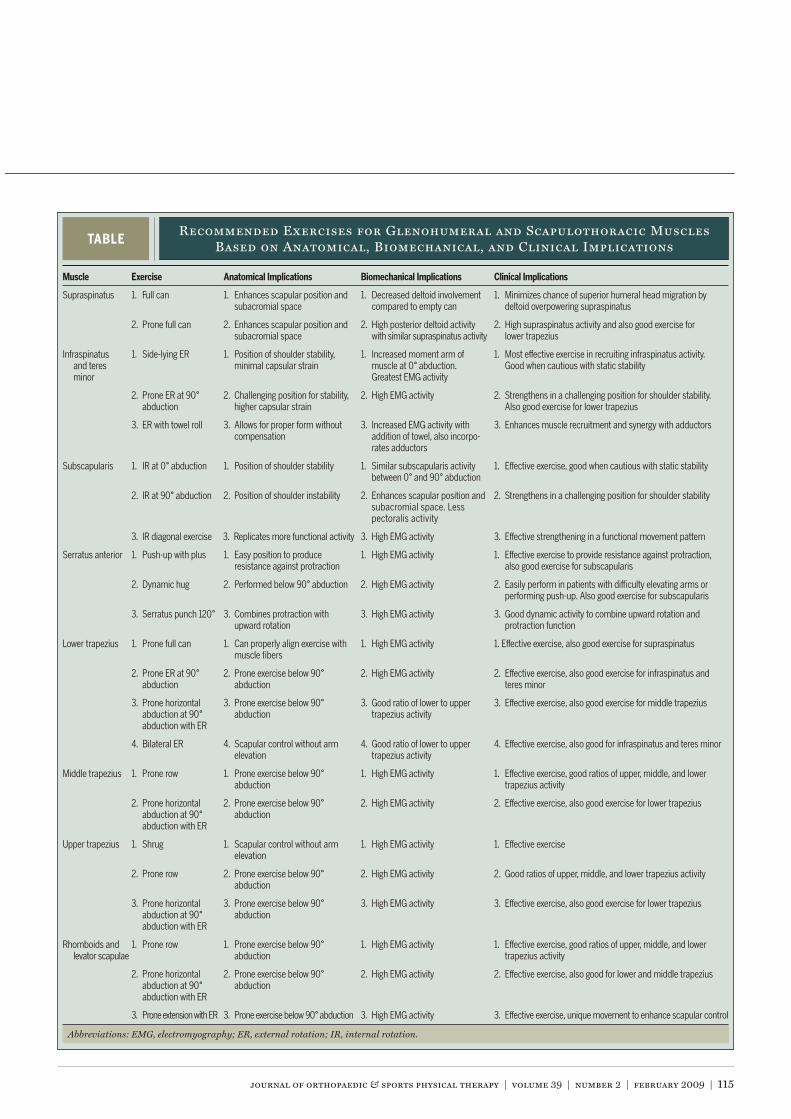
The preceding review can be usedto identify appropriate rehabilitationexercises for specific muscles. Based
on the reported studies and the collectiveexperience of the authors, we recommendthat exercises should be selected based onthe appropriate anatomical, biomechani-cal, and clinical implications. We haveidentified a set of exercises that the cur-rent authors use clinically for rehabilita-tion and injury prevention (TABLE). Theseexercises have been selected based on theresults of the numerous studies previous-ly cited and take into consideration theseimplications for each exercise described.Furthermore, the authors encourage theclinician to carefully consider emphasiz-ing posture and scapular retraction dur-ing the performance of glenohumeral andscapulothoracic exercises.
A common recommendation in reha-bilitation is to limit the amount of weightused during glenohumeral and scapu-lothoracic exercises to assure that the ap-propriate muscles are being utilized andnot larger compensatory muscles. Tworecent studies have analyzed this theoryand appear to prove the recommenda-tion inaccurate and not necessary. Alpertet al7 studied the rotator cuff and deltoidmuscles during scapular plane elevationand noted that EMG signal amplitudeof the smaller rotator cuff muscles andlarger deltoid muscles increased linearlyin relation to the amount of weight used.This finding is consistent with that ofDark et al,14 who showed similar resultsfor the rotator cuff, deltoid, pectoralis,and latissimus dorsi during ER and IRat 0° abduction. Thus, it appears thatlarger muscle groups do not overpowersmaller groups, such as the rotator cuff.Weight selection should be based on theindividual goals and performance of eachpatient. It does not appear necessary tolimit the amount of weight performedduring these rotator cuff exercises.
As our understanding of the anatomi-cal and biomechanical implications asso-ciated with exercise selection continues
to grow, we are seeing advances in exer-cise selection and the integration of thewhole-body kinetic-chain approach tostrengthening and rehabilitating injuries.This may involve strengthening multiplejoints simultaneously and during move-ment patterns that mimic athletic andfunctional daily activities of living. Theauthors often employ these techniqueswhen our patients improve in strengthyet continue to have symptoms duringactivities. In addition, we often attemptto further challenge our patients by per-forming many of the recommended exer-cise on various unstable surfaces (such asfoam or physioballs), with altered basesof support (such as sitting, standing, orsingle-leg balancing), in an attempt torecruit whole-body muscle patterns thatinteract together to perform active rangeof motion while stabilizing other areas ofthe body. We believe that these conceptsare important to consider in addition tostraight-plane, isolated movements ofspecific muscle groups, and that strength,posture, balance, and neuromuscularcontrol are all vital components to anyinjury prevention of rehabilitation pro-gram. Future research on the validity ofthese techniques is needed to justify theiruse. We believe that this is the next stepin the evolution of research on the clini-cal and biomechanical implications ofexercise selection for the glenohumeraland scapulothoracic musculature.
Athorough understanding ofthe biomechanical factors as-sociated with normal shoulder
movement, as well as during commonlyperformed exercises, is necessary tosafely and effectively design appropriateprograms. We have reviewed the normalbiomechanics of the glenohumeral andscapulothoracic muscles during func-tional activities, common exercises, andin the presence of pathology. These find-ings can be used by the clinician to designappropriate rehabilitation and injuryprevention programs.
Bilateral external rotation for infraspinatusand lower trapezius strengthening involves graspingexercise tubing with both hands and externallyrotating. Emphasis should be placed on providingscapular retraction and posterior tilting.
journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 115
TABLERecommended Exercises for Glenohumeral and Scapulothoracic Muscles
Based on Anatomical, Biomechanical, and Clinical Implications
Abbreviations: EMG, electromyography; ER, external rotation; IR, internal rotation.
Supraspinatus 1. Full can 1. Enhances scapular position andsubacromial space
1. Decreased deltoid involvementcompared to empty can
1. Minimizes chance of superior humeral head migration bydeltoid overpowering supraspinatus
2. Prone full can 2. Enhances scapular position andsubacromial space
2. High posterior deltoid activitywith similar supraspinatus activity
2. High supraspinatus activity and also good exercise forlower trapezius
Infraspinatusand teresminor
1. Side-lying ER 1. Position of shoulder stability,minimal capsular strain
1. Increased moment arm ofmuscle at 0° abduction.Greatest EMG activity
1. Most effective exercise in recruiting infraspinatus activity.Good when cautious with static stability
2. Prone ER at 90°abduction
2. Challenging position for stability,higher capsular strain
2. High EMG activity 2. Strengthens in a challenging position for shoulder stability.Also good exercise for lower trapezius
3. ER with towel roll 3. Allows for proper form withoutcompensation
3. Increased EMG activity withaddition of towel, also incorpo-rates adductors
3. Enhances muscle recruitment and synergy with adductors
Subscapularis 1. IR at 0° abduction 1. Position of shoulder stability 1. Similar subscapularis activitybetween 0° and 90° abduction
1. Effective exercise, good when cautious with static stability
2. IR at 90° abduction 2. Position of shoulder instability 2. Enhances scapular position andsubacromial space. Lesspectoralis activity
2. Strengthens in a challenging position for shoulder stability
3. IR diagonal exercise 3. Replicates more functional activity 3. High EMG activity 3. Effective strengthening in a functional movement pattern
Serratus anterior 1. Push-up with plus 1. Easy position to produceresistance against protraction
1. High EMG activity 1. Effective exercise to provide resistance against protraction,also good exercise for subscapularis
2. Dynamic hug 2. Performed below 90° abduction 2. High EMG activity 2. Easily perform in patients with difficulty elevating arms orperforming push-up. Also good exercise for subscapularis
3. Serratus punch 120° 3. Combines protraction withupward rotation
3. High EMG activity 3. Good dynamic activity to combine upward rotation andprotraction function
Lower trapezius 1. Prone full can 1. Can properly align exercise withmuscle fibers
1. High EMG activity 1. Effective exercise, also good exercise for supraspinatus
2. Prone ER at 90°abduction
2. Prone exercise below 90°abduction
2. High EMG activity 2. Effective exercise, also good exercise for infraspinatus andteres minor
3. Prone horizontalabduction at 90°abduction with ER
3. Prone exercise below 90°abduction
3. Good ratio of lower to uppertrapezius activity
3. Effective exercise, also good exercise for middle trapezius
4. Bilateral ER 4. Scapular control without armelevation
4. Good ratio of lower to uppertrapezius activity
4. Effective exercise, also good for infraspinatus and teres minor
Middle trapezius 1. Prone row 1. Prone exercise below 90°abduction
1. High EMG activity 1. Effective exercise, good ratios of upper, middle, and lowertrapezius activity
2. Prone horizontalabduction at 90°abduction with ER
2. Prone exercise below 90°abduction
2. High EMG activity 2. Effective exercise, also good exercise for lower trapezius
Upper trapezius 1. Shrug 1. Scapular control without armelevation
1. High EMG activity 1. Effective exercise
2. Prone row 2. Prone exercise below 90°abduction
2. High EMG activity 2. Good ratios of upper, middle, and lower trapezius activity
3. Prone horizontalabduction at 90°abduction with ER
3. Prone exercise below 90°abduction
3. High EMG activity 3. Effective exercise, also good exercise for lower trapezius
Rhomboids andlevator scapulae
1. Prone row 1. Prone exercise below 90°abduction
1. High EMG activity 1. Effective exercise, good ratios of upper, middle, and lowertrapezius activity
2. Prone horizontalabduction at 90°abduction with ER
2. Prone exercise below 90°abduction
2. High EMG activity 2. Effective exercise, also good for lower and middle trapezius
3. Prone extension with ER 3. Prone exercise below 90° abduction 3. High EMG activity 3. Effective exercise, unique movement to enhance scapular control
116 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
1. Alpert SW, Pink MM, Jobe FW, McMahon PJ, Ma-thiyakom W. Electromyographic analysis of deltoidand rotator cuff function under varying loads andspeeds. J Shoulder Elbow Surg. 2000;9:47-58.
2. Bagg SD, Forrest WJ. Electromyographic study ofthe scapular rotators during arm abduction in thescapular plane. Am J Phys Med. 1986;65:111-124.
3. Ballantyne BT, O’Hare SJ, Paschall JL, Et al.Electromyographic activity of selected shouldermuscles in commonly used therapeutic exercises.Phys Ther. 1993;73:668-682.
4. Barnett C, Kippers V, Turner P. Effects of variationsof the pench press exercise on the EMG activityof five shoulder muscles. J Strength Cond Res.1995;9:222-227.Blackburn TA, McLeod WD, White B, Wofford L.EMG analysis of posterior rotator cuff exercises.Athl Train J Natl Athl Train Assoc. 1990;25:40-45.Brossmann J, Preidler KW, Pedowitz RA, WhiteLM, Trudell D, Resnick D. Shoulder impingementsyndrome: influence of shoulder position on rota-tor cuff impingement—an anatomic study. AJRAm J Roentgenol. 1996;167:1511-1515.Brostrom LA, Kronberg M, Nemeth G. Muscleactivity during shoulder dislocation. Acta OrthopScand. 1989;60:639-641.
8. Burke WS, Vangsness CT, Powers CM. Strengthen-ing the supraspinatus: a clinical and biomechani-cal review. Clin Orthop Relat Res. 2002;292-298.
9. Cain PR, Mutschler TA, Fu FH, Lee SK. Anteriorstability of the glenohumeral joint. A dynamicmodel. Am J Sports Med. 1987;15:144-148.
10. Cools AM, Declercq GA, Cambier DC, Mahieu NN,Witvrouw EE. Trapezius activity and intramuscularbalance during isokinetic exercise in overheadathletes with impingement symptoms. ScandJ Med Sci Sports. 2007;17:25-33. http://dx.doi.org/10.1111/j.1600-0838.2006.00570.x
11. Cools AM, Dewitte V, Lanszweert F, et al.Rehabilitation of scapular muscle balance:which exercises to prescribe? Am J SportsMed. 2007;35:1744-1751. http://dx.doi.org/10.1177/0363546507303560
12. Cools AM, Witvrouw EE, Declercq GA, DanneelsLA, Cambier DC. Scapular muscle recruitmentpatterns: trapezius muscle latency with and with-out impingement symptoms. Am J Sports Med.2003;31:542-549.
13. Cordasco FA, Wolfe IN, Wootten ME, Bigliani LU.An electromyographic analysis of the shoulderduring a medicine ball rehabilitation program. AmJ Sports Med. 1996;24:386-392.
14. Dark A, Ginn KA, Halaki M. Shoulder musclerecruitment patterns during commonly used rota-tor cuff exercises: an electromyographic study.Phys Ther. 2007;87:1039-1046. http://dx.doi.org/10.2522/ptj.20060068De Wilde L, Plasschaert F, Berghs B, Van HoeckeM, Verstraete K, Verdonk R. Quantified measure-ment of subacromial impingement. J ShoulderElbow Surg. 2003;12:346-349. http://dx.doi.
org/10.1016/mse.2003.S1058274603000387Decker MJ, Hintermeister RA, Faber KJ, HawkinsRJ. Serratus anterior muscle activity during se-lected rehabilitation exercises. Am J Sports Med.1999;27:784-791.Decker MJ, Tokish JM, Ellis HB, Torry MR, HawkinsRJ. Subscapularis muscle activity during selectedrehabilitation exercises. Am J Sports Med.2003;31:126-134.
18. Ebaugh DD, McClure PW, Karduna AR. Scapu-lothoracic and glenohumeral kinematics followingan external rotation fatigue protocol. J OrthopSports Phys Ther. 2006;36:557-571. http://dx.doi.org/10.2519/jospt.2006.2189
19. Ekholm J, Arborelius UP, Hillered L, Ortqvist A.Shoulder muscle EMG and resisting momentduring diagonal exercise movements resisted byweight-and-pulley-circuit. Scand J Rehabil Med.1978;10:179-185.
20. Ekstrom RA, Donatelli RA, Soderberg GL. Surfaceelectromyographic analysis of exercises for thetrapezius and serratus anterior muscles. J OrthopSports Phys Ther. 2003;33:247-258.
21. Flatow EL, Soslowsky LJ, Ticker JB, et al. Excur-sion of the rotator cuff under the acromion. Pat-terns of subacromial contact. Am J Sports Med.1994;22:779-788.
22. Glousman R, Jobe F, Tibone J, Moynes D, Antonel-li D, Perry J. Dynamic electromyographic analysisof the throwing shoulder with glenohumeral insta-bility. J Bone Joint Surg Am. 1988;70:220-226.
23. Graichen H, Bonel H, Stammberger T, EnglmeierKH, Reiser M, Eckstein F. Subacromial spacewidth changes during abduction and rotation--a 3-D MR imaging study. Surg Radiol Anat.1999;21:59-64.
24. Graichen H, Bonel H, Stammberger T, et al. Three-dimensional analysis of the width of the subacro-mial space in healthy subjects and patients withimpingement syndrome. AJR Am J Roentgenol.1999;172:1081-1086.Graichen H, Hinterwimmer S, von Eisenhart-Rothe R, Vogl T, Englmeier KH, Eckstein F. Effectof abducting and adducting muscle activity onglenohumeral translation, scapular kinematicsand subacromial space width in vivo. J Biomech.2005;38:755-760. http://dx.doi.org/10.1016/j.jbiomech.2004.05.020Graichen H, Stammberger T, Bonel H, Karl-HansE, Reiser M, Eckstein F. Glenohumeral transla-tion during active and passive elevation of theshoulder: a 3D open-MRI study. J Biomech.2000;33:609-613.Greenfield BH, Donatelli R, Wooden MJ, WilkesJ. Isokinetic evaluation of shoulder rotationalstrength between the plane of scapula and thefrontal plane. Am J Sports Med. 1990;18:124-128.
28. Greis PE, Kuhn JE, Schultheis J, Hintermeister R,Hawkins R. Validation of the lift-off test and analy-sis of subscapularis activity during maximal inter-nal rotation. Am J Sports Med. 1996;24:589-593.
29. Hardwick DH, Beebe JA, McDonnell MK, LangCE. A comparison of serratus anterior muscleactivation during a wall slide exercise and othertraditional exercises. J Orthop Sports Phys Ther.
2006;36:903-910. http://dx.doi.org/10.2519/jospt.2006.2306
30. Harryman DT, 2nd, Sidles JA, Clark JM, McQuadeKJ, Gibb TD, Matsen FA, 3rd. Translation ofthe humeral head on the glenoid with passiveglenohumeral motion. J Bone Joint Surg Am.1990;72:1334-1343.
31. Hess SA, Richardson C, Darnell R, Friis P, Lisle D,Myers P. Timing of rotator cuff activation duringshoulder external rotation in throwers with andwithout symptoms of pain. J Orthop Sports PhysTher. 2005;35:812-820. http://dx.doi.org/10.2519/jospt.2005.2134
32. Hintermeister RA, Lange GW, Schultheis JM, BeyMJ, Hawkins RJ. Electromyographic activity andapplied load during shoulder rehabilitation exer-cises using elastic resistance. Am J Sports Med.1998;26:210-220.
33. Horrigan JM, Shellock FG, Mink JH, DeutschAL. Magnetic resonance imaging evaluation ofmuscle usage associated with three exercises forrotator cuff rehabilitation. Med Sci Sports Exerc.1999;31:1361-1366.
34. Hughes RE, An KN. Force analysis of rotator cuffmuscles. Clin Orthop Relat Res. 1996;75-83.
Illyes A, Kiss RM. Electromyographic analysis in pa-tients with multidirectional shoulder instability duringpull, forward punch, elevation and overhead throw.Knee Surg Sports Traumatol Arthrosc. 2007;15:624-631. http://dx.doi.org/10.1007/s00167-006-0163-1Itoi E, Berglund LJ, Grabowski JJ, et al. Tensileproperties of the supraspinatus tendon. J OrthopRes. 1995;13:578-584. http://dx.doi.org/10.1002/jor.1100130413Itoi E, Kido T, Sano A, Urayama M, Sato K. Whichis more useful, the “full can test” or the “emptycan test,” in detecting the torn supraspinatustendon? Am J Sports Med. 1999;27:65-68.
38. Jobe FW, Moynes DR. Delineation of diagnosticcriteria and a rehabilitation program for rotatorcuff injuries. Am J Sports Med. 1982;10:336-339.
39. Kadaba MP, Cole A, Wootten ME, et al. Intramus-cular wire electromyography of the subscapularis.J Orthop Res. 1992;10:394-397. http://dx.doi.org/10.1002/jor.1100100312
40. Kelly BT, Kadrmas WR, Speer KP. The manualmuscle examination for rotator cuff strength. Anelectromyographic investigation. Am J SportsMed. 1996;24:581-588.
41. Kibler WB, Sciascia A, Dome D. Evaluationof apparent and absolute supraspinatusstrength in patients with shoulder injury us-ing the scapular retraction test. Am J SportsMed. 2006;34:1643-1647. http://dx.doi.org/10.1177/0363546506288728
42. Konrad GG, Jolly JT, Labriola JE, McMahon PJ,Debski RE. Thoracohumeral muscle activityalters glenohumeral joint biomechanics duringactive abduction. J Orthop Res. 2006;24:748-756.http://dx.doi.org/10.1002/jor.20062
43. Kronberg M, Brostrom LA, Nemeth G. Differencesin shoulder muscle activity between patients withgeneralized joint laxity and normal controls. ClinOrthop Relat Res. 1991;181-192.
44. Kronberg M, Nemeth G, Brostrom LA. Muscle ac-
journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 117
@ WWW.JOSPT.ORG
J. Comparative electromyographic analysis ofshoulder muscles during planar motions: anteriorglenohumeral instability versus normal. J Shoul-der Elbow Surg. 1996;5:118-123.Meskers CG, van der Helm FC, Rozing PM. Thesize of the supraspinatus outlet during elevationof the arm in the frontal and sagittal plane: a3-D model study. Clin Biomech (Bristol, Avon).2002;17:257-266.
Morrey BF, Itoi E, An KN. Biomechanics of the shoul-der. In: Rockwood CA, Matsen FA, 3rd, eds. TheShoulder. Philadelphia: Saunders; 1998:233-276.Moseley JB, Jr., Jobe FW, Pink M, Perry J, TiboneJ. EMG analysis of the scapular muscles duringa shoulder rehabilitation program. Am J SportsMed. 1992;20:128-134.Myers JB, Pasquale MR, Laudner KG, Sell TC,Bradley JP, Lephart SM. On-the-field resistance-tubing exercises for throwers: an electromyo-graphic analysis. J Athl Train. 2005;40:15-22.Ogston JB, Ludewig PM. Differences in 3-dimen-sional shoulder kinematics between persons withmultidirectional instability and asymptomaticcontrols. Am J Sports Med. 2007;35:1361-1370.http://dx.doi.org/10.1177/0363546507300820
Otis JC, Jiang CC, Wickiewicz TL, Peterson MG, War-ren RF, Santner TJ. Changes in the moment arms ofthe rotator cuff and deltoid muscles with abductionand rotation. J Bone Joint Surg Am. 1994;76:667-676.Poppen NK, Walker PS. Forces at the gle-nohumeral joint in abduction. Clin Orthop RelatRes. 1978;165-170.Poppen NK, Walker PS. Normal and abnormalmotion of the shoulder. J Bone Joint Surg Am.1976;58:195-201.Reddy AS, Mohr KJ, Pink MM, Jobe FW. Electro-myographic analysis of the deltoid and rotator cuffmuscles in persons with subacromial impinge-ment. J Shoulder Elbow Surg. 2000;9:519-523.Reinold MM, Macrina LC, Wilk KE, et al. Electro-myographic analysis of the supraspinatus anddeltoid muscles during 3 common rehabilitationexercises. J Athl Train. 2007;42:464-469.Reinold MM, Wilk KE, Fleisig GS, et al. Elec-tromyographic analysis of the rotator cuff anddeltoid musculature during common shoulderexternal rotation exercises. J Orthop SportsPhys Ther. 2004;34:385-394. http://dx.doi.org/10.2519/jospt.2004.0665Roberts CS, Davila JN, Hushek SG, Tillett ED, Cor-rigan TM. Magnetic resonance imaging analysisof the subacromial space in the impingement signpositions. J Shoulder Elbow Surg. 2002;11:595-599. http://dx.doi.org/10.1067/mse.2002.127095Santos MJ, Belangero WD, Almeida GL. The effectof joint instability on latency and recruitment or-der of the shoulder muscles. J Electromyogr Kine-siol. 2007;17:167-175. http://dx.doi.org/10.1016/j.jelekin.2006.01.010Scovazzo ML, Browne A, Pink M, Jobe FW, Kerri-gan J. The painful shoulder during freestyle swim-ming. An electromyographic cinematographicanalysis of twelve muscles. Am J Sports Med.1991;19:577-582.Sharkey NA, Marder RA. The rotator cuff opposes
tivity and coordination in the normal shoulder. Anelectromyographic study. Clin Orthop Relat Res.1990;76-85.Labriola JE, Jolly JT, McMahon PJ, Debski RE. Ac-tive stability of the glenohumeral joint decreasesin the apprehension position. Clin Biomech(Bristol, Avon). 2004;19:801-809. http://dx.doi.org/10.1016/j.clinbiomech.2004.05.008Labriola JE, Lee TQ, Debski RE, McMahon PJ. Sta-bility and instability of the glenohumeral joint: therole of shoulder muscles. J Shoulder Elbow Surg.2005;14:32S-38S. http://dx.doi.org/10.1016/j.jse.2004.09.014Lear LJ, Gross MT. An electromyographical analy-sis of the scapular stabilizing synergists during apush-up progression. J Orthop Sports Phys Ther.1998;28:146-157.
48. Lee SB, An KN. Dynamic glenohumeral stabilityprovided by three heads of the deltoid muscle.Clin Orthop Relat Res. 2002;40-47.
49. Lee SB, Kim KJ, O’Driscoll SW, Morrey BF, AnKN. Dynamic glenohumeral stability providedby the rotator cuff muscles in the mid-range andend-range of motion. A study in cadavera. J BoneJoint Surg Am. 2000;82:849-857.Liu J, Hughes RE, Smutz WP, Niebur G, Nan-AnK. Roles of deltoid and rotator cuff muscles inshoulder elevation. Clin Biomech (Bristol, Avon).1997;12:32-38.Ludewig PM, Cook TM. Alterations in shoulderkinematics and associated muscle activity inpeople with symptoms of shoulder impingement.Phys Ther. 2000;80:276-291.Ludewig PM, Cook TM, Nawoczenski DA. Three-dimensional scapular orientation and muscle ac-tivity at selected positions of humeral elevation. JOrthop Sports Phys Ther. 1996;24:57-65.Ludewig PM, Hoff MS, Osowski EE, MeschkeSA, Rundquist PJ. Relative balance of serratusanterior and upper trapezius muscle activityduring push-up exercises. Am J Sports Med.2004;32:484-493.Malanga GA, Jenp YN, Growney ES, An KN. EMGanalysis of shoulder positioning in testing andstrengthening the supraspinatus. Med Sci SportsExerc. 1996;28:661-664.Matias R, Pascoal AG. The unstable shoulder inarm elevation: a three-dimensional and electro-myographic study in subjects with glenohumeralinstability. Clin Biomech (Bristol, Avon). 2006;21Suppl 1:S52-58. http://dx.doi.org/10.1016/j.clinbiomech.2005.09.014
McCabe RA. Surface electromyographic analysis ofthe lower trapezius muscle during exercises performedbelow ninety degrees of shoulder elevation in healthysubjects. N Am J Sports Phys Ther. 2007;2:34-43.McCaw ST, Friday JJ. A comparison of muscleactivity between a free weight and machine benchpress. J Strength Cond Res. 1994;8:259-264.McClure PW, Michener LA, Sennett BJ, KardunaAR. Direct 3-dimensional measurement ofscapular kinematics during dynamic movementsin vivo. J Shoulder Elbow Surg. 2001;10:269-277.http://dx.doi.org/10.1067/mse.2001.112954McMahon PJ, Jobe FW, Pink MM, Brault JR, Perry
superior translation of the humeral head. Am JSports Med. 1995;23:270-275.Smith J, Dahm DL, Kaufman KR, et al. Electro-myographic activity in the immobilized shouldergirdle musculature during scapulothoracic exer-cises. Arch Phys Med Rehabil. 2006;87:923-927.http://dx.doi.org/10.1016/j.apmr.2006.03.013Solem-Bertoft E, Thuomas KA, Westerberg CE.The influence of scapular retraction and protrac-tion on the width of the subacromial space. AnMRI study. Clin Orthop Relat Res. 1993;99-103.Takeda Y, Kashiwaguchi S, Endo K, Matsuura T, SasaT. The most effective exercise for strengthening thesupraspinatus muscle: evaluation by magnetic reso-nance imaging. Am J Sports Med. 2002;30:374-381.Thigpen CA, Padua DA, Morgan N, Kreps C,Karas SG. Scapular kinematics during supraspi-natus rehabilitation exercise: a comparison offull-can versus empty-can techniques. Am JSports Med. 2006;34:644-652. http://dx.doi.org/10.1177/0363546505281797Townsend H, Jobe FW, Pink M, Perry J. Elec-tromyographic analysis of the glenohumeralmuscles during a baseball rehabilitation program.Am J Sports Med. 1991;19:264-272.
80. Tsai NT, McClure PW, Karduna AR. Effects of mus-cle fatigue on 3-dimensional scapular kinematics.Arch Phys Med Rehabil. 2003;84:1000-1005.
81. Uhl TL, Carver TJ, Mattacola CG, Mair SD, Nitz AJ.Shoulder musculature activation during upper ex-tremity weight-bearing exercise. J Orthop SportsPhys Ther. 2003;33:109-117.
82. Warner JJ, Micheli LJ, Arslanian LE, KennedyJ, Kennedy R. Patterns of flexibility, laxity, andstrength in normal shoulders and shoulders withinstability and impingement. Am J Sports Med.1990;18:366-375.
83. Welsch EA, Bird M, Mayhew JL. Electromyograph-ic activity of the pectoralis major and anteriordeltoid muscles during three upper-body lifts.J Strength Cond Res. 2005;19:449-452. http://dx.doi.org/10.1519/14513.1
84. Wiedenbauer MM, Mortensen OA. An electromyo-graphic study of the trapezius muscle. Am J PhysMed. 1952;31:363-372.Wilk KE, Andrews JR, Arrigo CA. The physical ex-amination of the glenohumeral joint: emphasis onthe stabilizing structures. J Orthop Sports PhysTher. 1997;25:380-389.Wilk KE, Arrigo CA, Andrews JR. Currentconcepts: the stabilizing structures of theglenohumeral joint. J Orthop Sports Phys Ther.1997;25:364-379.Worrell TW, Corey BJ, York SL, Santiestaban J. Ananalysis of supraspinatus EMG activity and shoul-der isometric force development. Med Sci SportsExerc. 1992;24:744-748.
88. Wuelker N, Korell M, Thren K. Dynamic gle-nohumeral joint stability. J Shoulder Elbow Surg.1998;7:43-52.
journal of orthopaedic & sports physical therapy | volume 40 | number 3 | march 2010 | 155
[ clinical commentary ]
1 Director of Physical Therapy, HPRC at St Francis Rehabilitation Center, Columbus, GA. 2 Coordinator of Sports Rehabilitation University of Iowa Sports Medicine, Clinical Specialist Department of Rehabilitation Therapies University of Iowa Hospitals and Clinics, Iowa City, IA. 3 Associate Professor and Chair, Department of Interdisciplinary Health Sciences, A. T. Still University, Mesa, AZ. 4 Associate Professor Department of Physical Therapy, Virginia Commonwealth University-MCV Campus, Richmond, VA. 5 Director, St Francis Shoulder Center, St Francis Orthopaedic Institute, Columbus, GA. 6 Clinical Research Scientist, Proaxis Therapy, Greenville, SC. 7 Assistant Consulting Professor, Doctor of Physical Therapy Division, Department of Community and Family Medicine, Duke University School of Medicine, Durham, NC. Address correspondence to Bryce Gaunt, HPRC at St Francis Rehabilitation Center, PO Box 8068, Columbus, GA 31908-8068. E-mail: [email protected]
Bryce W. Gaunt, PT, SCS1 • Michael a. Shaffer, MSPT, OCS, ATC2 • eric l. SauerS, PhD, ATC3 lori a. Michener, PT, PhD, ATC, SCS4 • GeorGe M. MccluSkey iii, MD5 • chuck a. ThiGpen, PT, PhD, ATC6,7
The American Society of Shoulder and Elbow Therapists’ Consensus Rehabilitation
Guideline for Arthroscopic Anterior Capsulolabral Repair of the Shoulder
the maintenance of shoulder stability is the result of a complex interplay of static and dynamic factors. Shoulder instability may require surgical stabilization to resolve the anatomical deficits causing the instability and to restore shoulder function.
A variety of surgical techniques exist. The chronicity, magnitude (dislocations or subluxations), and direction (anterior, posterior, or multidirectional) of instability are the key factors considered during preoperative planning. In addition, patient factors, such as a need for mobility in the case of an overhead athlete, must be considered.
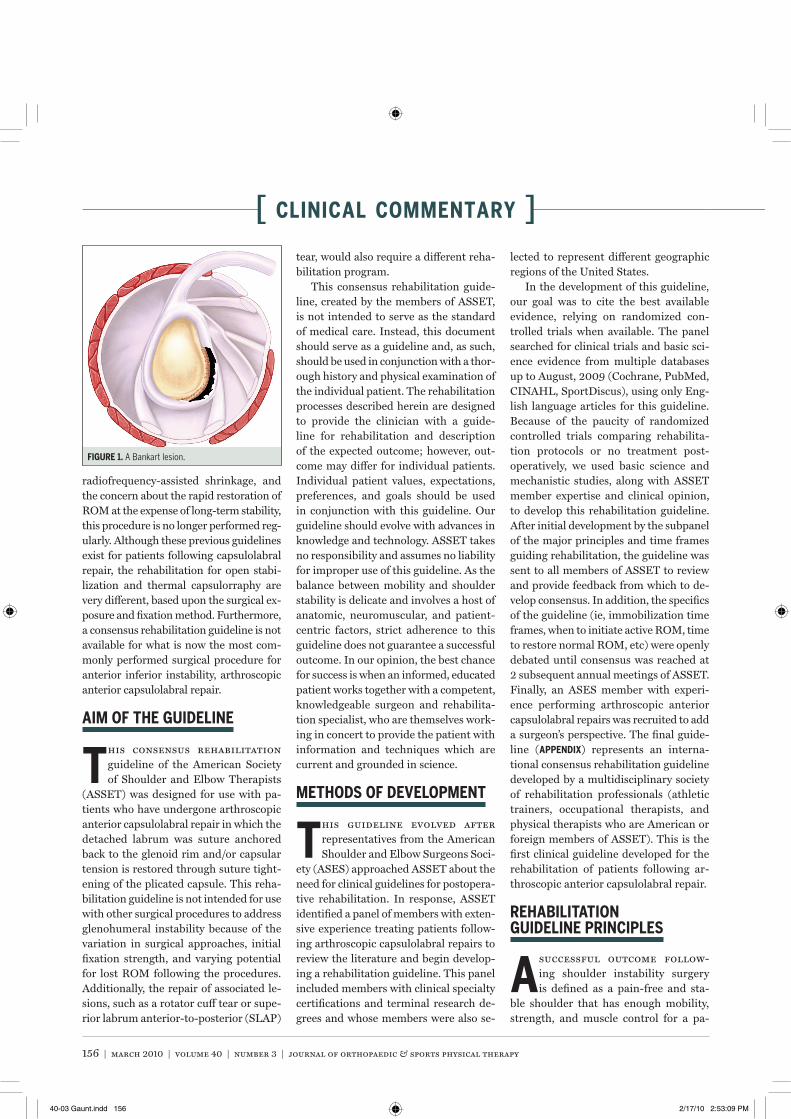
store shoulder stability by suturing back to the glenoid the detached or unstable anterior inferior labrum, known as a Ban-kart lesion (fiGure 1). In addition to a Ban-kart repair, capsular plication is added as necessary to address permanent plastic deformation of the glenohumeral joint capsule that often accompanies recurrent anterior inferior dislocations.6,31 Rehabili-tation following the surgery must balance the restoration of motion and function with the desired result of an appropriately taut capsulolabral complex.23,34
Blackburn and Guido7 published a re-habilitation guideline in 2000 for patients following open anterior shoulder stabiliza-tion, which at the time was the most com-monly performed stabilization procedure. However, due to the less invasive nature of arthroscopic procedures, patients under-going arthroscopic repair today generally regain range of motion (ROM) more easily and with less risk of permanent restriction than patients following comparable open surgeries.23,34 In 2002, Wilk et al95 pub-lished a rehabilitation protocol follow-ing thermal-assisted capsulorraphy. Due to concerns about the long-term health of capsular tissue treated with laser- or
As the majority of patients with an-terior instability have injuries to their capsulolabral complex, the arthroscopic
anterior capsulolabral repair is a com-monly utilized procedure. Arthroscopic anterior capsulolabral repair seeks to re-
t SynopSiS: This manuscript describes the consensus rehabilitation guideline developed by the American Society of Shoulder and Elbow Therapists. The purpose of this guideline is to facilitate clinical decision making during the reha-bilitation of patients following arthroscopic anterior capsulolabral repair of the shoulder. This guideline is centered on the principle of the gradual applica-tion of stress to the healing capsulolabral repair through appropriate integration of range of motion, strengthening, and shoulder girdle stabilization exercises during rehabilitation and daily activities. Components of this guideline include a 0- to 4-week period of absolute immobilization, a staged recovery of full range of motion over a 3-month
period, a strengthening progression beginning at postoperative week 6, and a functional progression for return to athletic or demanding work activities between postoperative months 4 and 6. This docu-ment represents the first consensus rehabilita-tion guideline developed by a multidisciplinary society of international rehabilitation professionals specifically for the postoperative care of patients following arthroscopic anterior capsulolabral repair of the shoulder. J Orthop Sports Phys Ther 2010;40(3):155-168. doi:10.2519/jospt.2010.3186
t key WorDS: Bankart repair, capsular plica-tion, postoperative rehabilitation, shoulder instabil-ity, therapeutic exercise
40-03 Gaunt.indd 155 2/17/10 2:53:08 PM
156 | march 2010 | volume 40 | number 3 | journal of orthopaedic & sports physical therapy
[ clinical commentary ]
radiofrequency-assisted shrinkage, and the concern about the rapid restoration of ROM at the expense of long-term stability, this procedure is no longer performed reg-ularly. Although these previous guidelines exist for patients following capsulolabral repair, the rehabilitation for open stabi-lization and thermal capsulorraphy are very different, based upon the surgical ex-posure and fixation method. Furthermore, a consensus rehabilitation guideline is not available for what is now the most com-monly performed surgical procedure for anterior inferior instability, arthroscopic anterior capsulolabral repair.
aiM of The GuiDeline
this consensus rehabilitation guideline of the American Society of Shoulder and Elbow Therapists
(ASSET) was designed for use with pa-tients who have undergone arthroscopic anterior capsulolabral repair in which the detached labrum was suture anchored back to the glenoid rim and/or capsular tension is restored through suture tight-ening of the plicated capsule. This reha-bilitation guideline is not intended for use with other surgical procedures to address glenohumeral instability because of the variation in surgical approaches, initial fixation strength, and varying potential for lost ROM following the procedures. Additionally, the repair of associated le-sions, such as a rotator cuff tear or supe-rior labrum anterior-to-posterior (SLAP)
tear, would also require a different reha-bilitation program.
This consensus rehabilitation guide-line, created by the members of ASSET, is not intended to serve as the standard of medical care. Instead, this document should serve as a guideline and, as such, should be used in conjunction with a thor-ough history and physical examination of the individual patient. The rehabilitation processes described herein are designed to provide the clinician with a guide-line for rehabilitation and description of the expected outcome; however, out-come may differ for individual patients. Individual patient values, expectations, preferences, and goals should be used in conjunction with this guideline. Our guideline should evolve with advances in knowledge and technology. ASSET takes no responsibility and assumes no liability for improper use of this guideline. As the balance between mobility and shoulder stability is delicate and involves a host of anatomic, neuromuscular, and patient-centric factors, strict adherence to this guideline does not guarantee a successful outcome. In our opinion, the best chance for success is when an informed, educated patient works together with a competent, knowledgeable surgeon and rehabilita-tion specialist, who are themselves work-ing in concert to provide the patient with information and techniques which are current and grounded in science.
MeThoDS of DeVelopMenT
this guideline evolved after representatives from the American Shoulder and Elbow Surgeons Soci-
ety (ASES) approached ASSET about the need for clinical guidelines for postopera-tive rehabilitation. In response, ASSET identified a panel of members with exten-sive experience treating patients follow-ing arthroscopic capsulolabral repairs to review the literature and begin develop-ing a rehabilitation guideline. This panel included members with clinical specialty certifications and terminal research de-grees and whose members were also se-
lected to represent different geographic regions of the United States.
In the development of this guideline, our goal was to cite the best available evidence, relying on randomized con-trolled trials when available. The panel searched for clinical trials and basic sci-ence evidence from multiple databases up to August, 2009 (Cochrane, PubMed, CINAHL, SportDiscus), using only Eng-lish language articles for this guideline. Because of the paucity of randomized controlled trials comparing rehabilita-tion protocols or no treatment post-operatively, we used basic science and mechanistic studies, along with ASSET member expertise and clinical opinion, to develop this rehabilitation guideline. After initial development by the subpanel of the major principles and time frames guiding rehabilitation, the guideline was sent to all members of ASSET to review and provide feedback from which to de-velop consensus. In addition, the specifics of the guideline (ie, immobilization time frames, when to initiate active ROM, time to restore normal ROM, etc) were openly debated until consensus was reached at 2 subsequent annual meetings of ASSET. Finally, an ASES member with experi-ence performing arthroscopic anterior capsulolabral repairs was recruited to add a surgeon’s perspective. The final guide-line (appenDiX) represents an interna-tional consensus rehabilitation guideline developed by a multidisciplinary society of rehabilitation professionals (athletic trainers, occupational therapists, and physical therapists who are American or foreign members of ASSET). This is the first clinical guideline developed for the rehabilitation of patients following ar-throscopic anterior capsulolabral repair.
rehaBiliTaTion GuiDeline principleS
a successful outcome follow-ing shoulder instability surgery is defined as a pain-free and sta-
ble shoulder that has enough mobility, strength, and muscle control for a pa-
fiGure 1. A Bankart lesion.
40-03 Gaunt.indd 156 2/17/10 2:53:09 PM
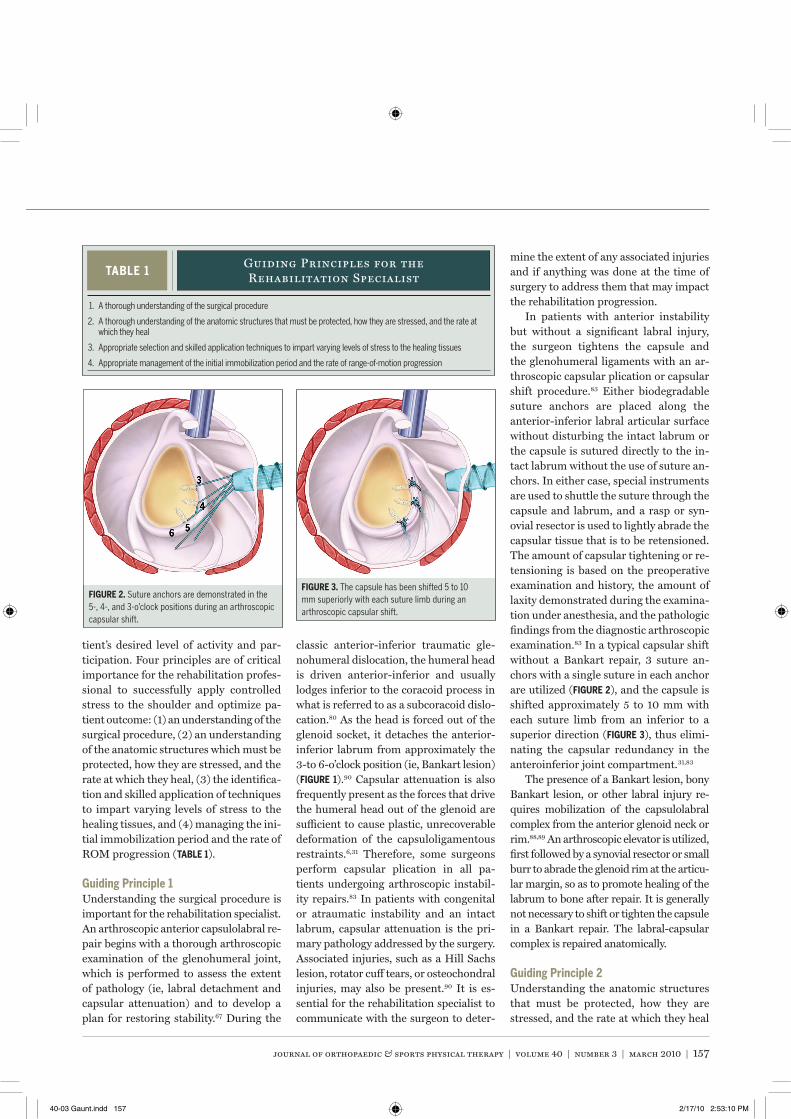
journal of orthopaedic & sports physical therapy | volume 40 | number 3 | march 2010 | 157
tient’s desired level of activity and par-ticipation. Four principles are of critical importance for the rehabilitation profes-sional to successfully apply controlled stress to the shoulder and optimize pa-tient outcome: (1) an understanding of the surgical procedure, (2) an understanding of the anatomic structures which must be protected, how they are stressed, and the rate at which they heal, (3) the identifica-tion and skilled application of techniques to impart varying levels of stress to the healing tissues, and (4) managing the ini-tial immobilization period and the rate of ROM progression (TaBle 1).
Guiding principle 1Understanding the surgical procedure is important for the rehabilitation specialist. An arthroscopic anterior capsulolabral re-pair begins with a thorough arthroscopic examination of the glenohumeral joint, which is performed to assess the extent of pathology (ie, labral detachment and capsular attenuation) and to develop a plan for restoring stability.67 During the
classic anterior-inferior traumatic gle-nohumeral dislocation, the humeral head is driven anterior-inferior and usually lodges inferior to the coracoid process in what is referred to as a subcoracoid dislo-cation.80 As the head is forced out of the glenoid socket, it detaches the anterior-inferior labrum from approximately the 3-to 6-o’clock position (ie, Bankart lesion) (fiGure 1).90 Capsular attenuation is also frequently present as the forces that drive the humeral head out of the glenoid are sufficient to cause plastic, unrecoverable deformation of the capsuloligamentous restraints.6,31 Therefore, some surgeons perform capsular plication in all pa-tients undergoing arthroscopic instabil-ity repairs.83 In patients with congenital or atraumatic instability and an intact labrum, capsular attenuation is the pri-mary pathology addressed by the surgery. Associated injuries, such as a Hill Sachs lesion, rotator cuff tears, or osteochondral injuries, may also be present.90 It is es-sential for the rehabilitation specialist to communicate with the surgeon to deter-
mine the extent of any associated injuries and if anything was done at the time of surgery to address them that may impact the rehabilitation progression.
In patients with anterior instability but without a significant labral injury, the surgeon tightens the capsule and the glenohumeral ligaments with an ar-throscopic capsular plication or capsular shift procedure.83 Either biodegradable suture anchors are placed along the anterior-inferior labral articular surface without disturbing the intact labrum or the capsule is sutured directly to the in-tact labrum without the use of suture an-chors. In either case, special instruments are used to shuttle the suture through the capsule and labrum, and a rasp or syn-ovial resector is used to lightly abrade the capsular tissue that is to be retensioned. The amount of capsular tightening or re-tensioning is based on the preoperative examination and history, the amount of laxity demonstrated during the examina-tion under anesthesia, and the pathologic findings from the diagnostic arthroscopic examination.83 In a typical capsular shift without a Bankart repair, 3 suture an-chors with a single suture in each anchor are utilized (fiGure 2), and the capsule is shifted approximately 5 to 10 mm with each suture limb from an inferior to a superior direction (fiGure 3), thus elimi-nating the capsular redundancy in the anteroinferior joint compartment.31,83
The presence of a Bankart lesion, bony Bankart lesion, or other labral injury re-quires mobilization of the capsulolabral complex from the anterior glenoid neck or rim.88,89 An arthroscopic elevator is utilized, first followed by a synovial resector or small burr to abrade the glenoid rim at the articu-lar margin, so as to promote healing of the labrum to bone after repair. It is generally not necessary to shift or tighten the capsule in a Bankart repair. The labral-capsular complex is repaired anatomically.
Guiding principle 2Understanding the anatomic structures that must be protected, how they are stressed, and the rate at which they heal
fiGure 2. Suture anchors are demonstrated in the 5-, 4-, and 3-o’clock positions during an arthroscopic capsular shift.
fiGure 3. The capsule has been shifted 5 to 10 mm superiorly with each suture limb during an arthroscopic capsular shift.
TaBle 1Guiding Principles for the Rehabilitation Specialist
1. A thorough understanding of the surgical procedure
2. A thorough understanding of the anatomic structures that must be protected, how they are stressed, and the rate at which they heal
3. Appropriate selection and skilled application techniques to impart varying levels of stress to the healing tissues
4. Appropriate management of the initial immobilization period and the rate of range-of-motion progression
40-03 Gaunt.indd 157 2/17/10 2:53:10 PM

158 | march 2010 | volume 40 | number 3 | journal of orthopaedic & sports physical therapy
[ clinical commentary ]The rehabilitation process is divided
into 3 phases of 6 to 12 weeks in duration, because we believe these time frames co-incide with the healing and clinical mile-stones. The first 6 weeks postoperative include the inflammatory and the prolif-erative (fibroplasia and wound contrac-tion) phases and the beginning of the scar maturation phase of tissue healing.19 Scar maturation and remodeling of the tissue likely continues throughout the rehabili-tation process and may not be complete until 40 to 50 weeks after surgery.53,96
Other factors, such as the patient’s age and the presence of comorbidities, may affect tissue healing and should be considered when deciding how quickly to progress an individual patient. Diabetes mellitus, peripheral vascular disease, and connective tissue disorders may impair healing; therefore patients with these diseases may have or require a slower re-habilitation progression. No studies have examined the influence of comorbidities on shoulder function following capsulo-labral repair. Comorbidities do negatively influence outcome following rotator cuff repair and shoulder athroplasty,11,35 there-fore it is possible that comorbidities may negatively impact rehabilitation and out-comes after capsulolabral repair.
Guiding principle 3Correct selection and use of techniques to apply varying levels of stress to the sur-gical repair is important for a successful outcome. Following surgical repair, the healing capsulolabral structures require appropriate stress to stimulate optimal healing, while protecting the repair from excessive tension. The gradual applica-tion of stress is a stimulus for further proliferation and differentiation of fibro-blasts.19,35 A gradual increase in applied stress, in a process analogous to Wollf ’s law of bone healing,96 results in enhanced structural integrity of the capsulolabral complex as additional collagen fibers are laid down in response to controlled stresses. However, it is equally important to understand that with excessive stress to the capsulolabral complex, either in
terms of magnitude or timing, the tissues will be unable to adequately adapt,32,92 and damage will result to either the heal-ing tissues or the suture anchors. During rehabilitation, there are 3 mechanisms by which rehabilitation providers apply stress to the surgical repair to positively affect patient outcome: (1) absolute ROM, (2) controlled submaximal tissue loading, and (3) dynamic stabilization.
Immediately following surgery, the re-pair is completely reliant on the mechani-cal strength of the sutures and/or suture anchors. Therefore, the absolute ROM limit that is initially deemed safe is based upon the surgical fixation and structural integrity of the repair. As time passes, the repaired tissues begin to heal through fi-brous scar formation and gradually in-crease in tensile strength. In the case of a Bankart lesion, the labrum develops immature connective tissue links to the glenoid rim, and in the case of a capsu-lar plication, the plicated layers of the capsule initiate formation of immature connective tissue links to one another. Excessive stretching during ROM activi-ties may overload the structural integrity of these immature cross-links in the heal-ing tissues.30,68,81,86
Much in the same way micromotion prevents bony union during fracture healing, submaximal tissue loading also has the potential to disrupt the tenuous tissue healing bonds between the labrum and bone and between the plicated layers of the capsule.32,92 Repeated submaximal stress of a ligament plication in an ani-mal model has been shown to negatively affect mechanical resistance properties, even as late as postoperative week 12.32 While direct extrapolation cannot be made to a pathologic human condition, these findings are similar to the effects of submaximal loading in human cadavers. Repetitive submaximal loading has been shown to increase the length and decrease the subsequent load to failure of the an-terior inferior glenohumeral ligament.71 The exact effect of submaximal loading during various rehabilitation interven-tions is currently unknown. Thus, clini-
is also important before rehabilitation begins. Arthroscopic anterior capsulo-labral repair involves a direct repair of damaged capsular and labral structures. Repair is achieved via suture and/or su-ture anchor reattachment, which requires protection from excessive stresses to fa-cilitate appropriate tissue healing.62,75 It is well documented that specific portions of the capsule and labrum are selectively tensioned with specific glenohumeral motions.68,81,86 A standard anterior cap-sulolabral repair, addressing attenuation of the anterior inferior capsule, is most directly stressed by external rotation, particularly above 90° of abduction.68,86 In a cadaveric model, Itoi et al37 dem-onstrated that with the arm by the side, external rotation to 30° could safely be applied to the shoulder without separat-ing a simulated Bankart lesion.
Forward flexion stresses the inferior part of the glenohumeral joint capsule. Therefore, based on the stress to the in-ferior capsule, we recommend limiting flexion to less than 90° until 3 weeks postsurgery, then gradually increasing flexion to 135° through postoperative week 6.
During the classic open Bankart re-pair, the subscapularis is either detached or split to access the capsule and is then subsequently reattached or closed with sutures, necessitating protection from active internal rotation during the early postoperative period.39,50 However, dur-ing the standard arthroscopic anterior capsulolabral repair, the subscapularis is not detached or split, therefore it does not need specific protection from ex-cessive stress during the rehabilitation program.15
It is imperative that activities be lim-ited to those which produce less stress to the healing tissues than the failure strength of the repair.93 The challenge for guiding rehabilitation based upon the tissue healing is the limited ability for clinicians to measure tissue heal-ing. Moreover, the amount of stress im-parted by many rehabilitation activities remains unknown.
40-03 Gaunt.indd 158 2/17/10 2:53:11 PM

journal of orthopaedic & sports physical therapy | volume 40 | number 3 | march 2010 | 159
cians should keep in mind that repeated and excessive submaximal tensioning of the repair during the remodeling phases of tissue healing may theoretically cause the capsule to heal at a longer length. Therefore, even though they are below the failure strength of the capsulolabral tissues, repetitive submaximal stresses should be carefully controlled as they pose a potential threat to capsuloliga-mentous integrity.
While excessive submaximal loading may be detrimental, dynamic stabiliza-tion or active stabilization of a joint by the muscles directly surrounding it provides protection to the surgical repair9,13,49,51 by supporting the joint capsule,14 increas-ing joint compression forces,42,49 and resisting joint displacement.55 It is vital to understand that these 3 mechanisms (absolute ROM, submaximal tissue load-ing, and dynamic stabilization) do not occur in isolation but are interrelated in all rehabilitation activities and should be the primary considerations when select-ing interventions during rehabilitation.
Guiding principle 4Appropriate management of the initial immobilization period and ROM pro-gression are also important for the reha-bilitation specialist because the tensile strength of the arthroscopic anterior capsulolabral repair is reduced through the first 12 postoperative weeks.32 There-fore, it is important to protect the surgi-cal repair from undue stress during the first 2 phases of this rehabilitation guide-line (12 weeks total) by controlling the rate at which ROM is regained. Gaining ROM too quickly can limit the normal tissue-healing process and lead to cap-suloligamentous attenuation.93 There-fore, an initial period of immobilization is common after arthroscopic anterior capsulolabral repair to facilitate healing of the surgically repaired tissues,40,45,52,65,76 theoretically allowing the surgically reat-tached labrum a chance to bind to the glenoid and the plicated layers of capsule to heal to each other.
Absolute immobilization (no gle-
nohumeral ROM exercises and constant sling use) in the first 6 weeks following arthroscopic capsulolabral repair of the shoulder was advocated during the in-fancy of these procedures,40,65 when surgi-cal techniques were rapidly evolving and failure rates were high.27 However, stud-ies advocating absolute immobilization as a means to decrease long-term failure rates utilized surgical procedures such as transglenoid sutures27,84 or staple repair40 that are no longer common. Current sur-gical methods typically employ sutures and suture anchors to repair the labrum and retension the glenohumeral liga-ments,3,10,45,52 producing outcomes similar to open instability repair.3,23,44 Therefore, the need for absolute immobilization af-ter arthroscopic Bankart repair has been reexamined in recent years.
Studies have shown short periods of absolute immobilization result in no greater recurrence rate of shoulder insta-bility and have demonstrated improved ROM over the course of recovery.3,46 In a randomized controlled trial comparing 3 weeks of absolute immobilization to im-mediate staged ROM in a select group of patients undergoing Bankart repair, Kim et al46 found that immediate ROM yielded no greater recurrence rate in dis-location, or difference in pain or function scores. These results apply to patients with recurrent (nonacute) instability brought on by a traumatic event, and a Bankart lesion only without the pres-ence of a bony fragment (bony Bankart). These results do not apply to those pa-tients actively participating in sports, or to those patients with multidirectional or posterior instability, other labral lesions, a rotator cuff tear, or a larger bony Ban-kart lesion involving greater than 30% of the glenoid. Additionally, considering that the capsulolabral complex appears to be within the safe boundaries of stress with the arm in adduction and up to 30° of external rotation,37 immediate postop-erative ROM in this range is safe.46
Based on this evidence and our sig-nificant clinical experience rehabilitat-ing patients following this surgery, we
recommend a variable period between 0 up to 4 weeks of absolute immobiliza-tion following an arthroscopic anterior capsulolabral repair, in which sutures or suture anchors are utilized. Relative immobilization (out of sling only for ROM exercises or short periods of sit-ting or standing) is recommended for 6 weeks, followed by sling use for comfort. We offer ranges of immobilization as a general guideline because we recognize that surgeon preference plays a major role in the postoperative immobilization time frames for patients undergoing this procedure and want to provide a wide range that is safe, both in terms of early motion and protecting the repair, and restricted motion in terms of preventing contractures and adhesions. Immobiliza-tion periods should be determined by the surgeon and rehabilitation provider for each individual patient, considering the extent of the pathology, the integrity or the repair, as well as the patient’s goals, age, and comorbidities.
Regardless of the period of absolute and relative immobilization, controlling the rate of ROM progression is vitally important. The integrity of the surgi-cal repair is thought to be negatively affected by the patient regaining ROM too quickly during the first 8 to 12 weeks postoperatively.32,62,75 Staged ROM goals are an effective tool to guide the rate of ROM progression.46,52 We have proposed a general guideline for staged ROM goals that we were able to achieve consensus on from our multidisciplinary team of shoul-der rehabilitation specialists (TaBle 2). As with the specific period of immobiliza-tion, ROM goals may be modified by the surgeon or rehabilitation provider, based on the individual patient. The ROM goals have the patient comfortably progressing their ROM to the specified angle. If the patient’s ROM is less than the targeted range, gentle stretching should be imple-mented to facilitate ROM gains to the targeted range and to prevent the devel-opment of contractures and adhesions. On the other hand, if the targeted ROM is easily obtained, then stretching in the
40-03 Gaunt.indd 159 2/17/10 2:53:12 PM
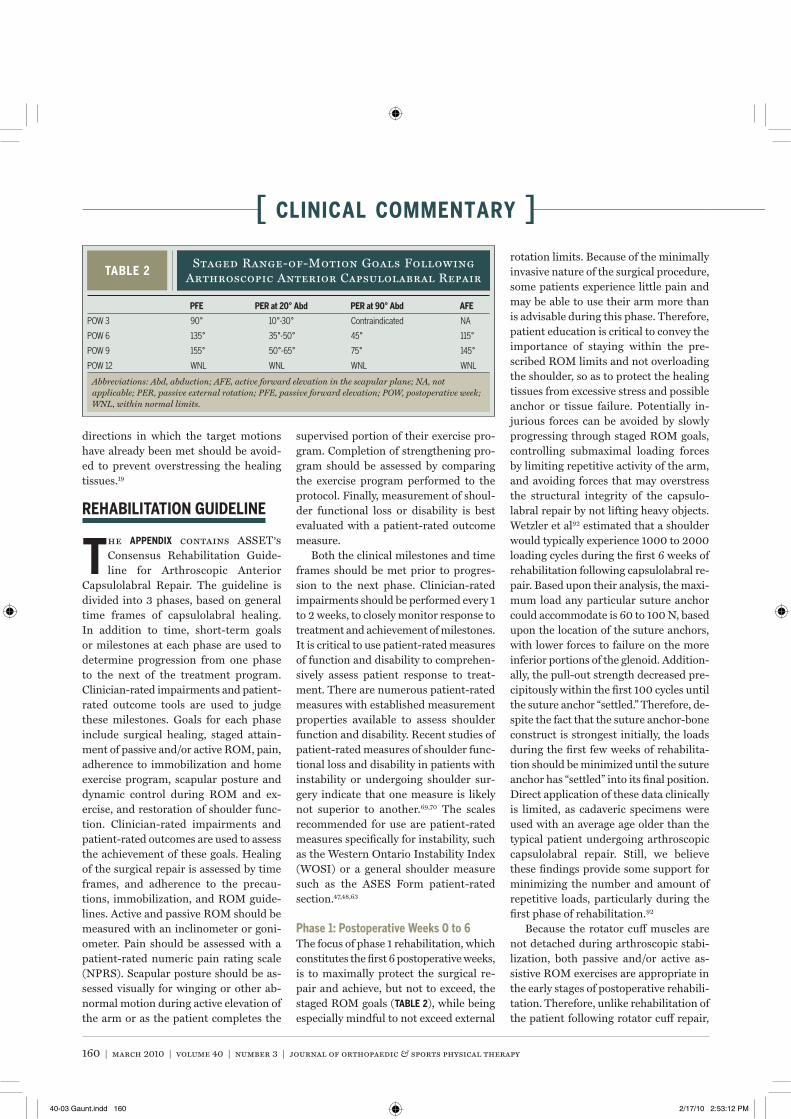
160 | march 2010 | volume 40 | number 3 | journal of orthopaedic & sports physical therapy
[ clinical commentary ]
directions in which the target motions have already been met should be avoid-ed to prevent overstressing the healing tissues.19
rehaBiliTaTion GuiDeline
the appenDiX contains ASSET’s Consensus Rehabilitation Guide-line for Arthroscopic Anterior
Capsulolabral Repair. The guideline is divided into 3 phases, based on general time frames of capsulolabral healing. In addition to time, short-term goals or milestones at each phase are used to determine progression from one phase to the next of the treatment program. Clinician-rated impairments and patient-rated outcome tools are used to judge these milestones. Goals for each phase include surgical healing, staged attain-ment of passive and/or active ROM, pain, adherence to immobilization and home exercise program, scapular posture and dynamic control during ROM and ex-ercise, and restoration of shoulder func-tion. Clinician-rated impairments and patient-rated outcomes are used to assess the achievement of these goals. Healing of the surgical repair is assessed by time frames, and adherence to the precau-tions, immobilization, and ROM guide-lines. Active and passive ROM should be measured with an inclinometer or goni-ometer. Pain should be assessed with a patient-rated numeric pain rating scale (NPRS). Scapular posture should be as-sessed visually for winging or other ab-normal motion during active elevation of the arm or as the patient completes the
supervised portion of their exercise pro-gram. Completion of strengthening pro-gram should be assessed by comparing the exercise program performed to the protocol. Finally, measurement of shoul-der functional loss or disability is best evaluated with a patient-rated outcome measure.
Both the clinical milestones and time frames should be met prior to progres-sion to the next phase. Clinician-rated impairments should be performed every 1 to 2 weeks, to closely monitor response to treatment and achievement of milestones. It is critical to use patient-rated measures of function and disability to comprehen-sively assess patient response to treat-ment. There are numerous patient-rated measures with established measurement properties available to assess shoulder function and disability. Recent studies of patient-rated measures of shoulder func-tional loss and disability in patients with instability or undergoing shoulder sur-gery indicate that one measure is likely not superior to another.69,70 The scales recommended for use are patient-rated measures specifically for instability, such as the Western Ontario Instability Index (WOSI) or a general shoulder measure such as the ASES Form patient-rated section.47,48,63
phase 1: postoperative Weeks 0 to 6The focus of phase 1 rehabilitation, which constitutes the first 6 postoperative weeks, is to maximally protect the surgical re-pair and achieve, but not to exceed, the staged ROM goals (TaBle 2), while being especially mindful to not exceed external
rotation limits. Because of the minimally invasive nature of the surgical procedure, some patients experience little pain and may be able to use their arm more than is advisable during this phase. Therefore, patient education is critical to convey the importance of staying within the pre-scribed ROM limits and not overloading the shoulder, so as to protect the healing tissues from excessive stress and possible anchor or tissue failure. Potentially in-jurious forces can be avoided by slowly progressing through staged ROM goals, controlling submaximal loading forces by limiting repetitive activity of the arm, and avoiding forces that may overstress the structural integrity of the capsulo-labral repair by not lifting heavy objects. Wetzler et al92 estimated that a shoulder would typically experience 1000 to 2000 loading cycles during the first 6 weeks of rehabilitation following capsulolabral re-pair. Based upon their analysis, the maxi-mum load any particular suture anchor could accommodate is 60 to 100 N, based upon the location of the suture anchors, with lower forces to failure on the more inferior portions of the glenoid. Addition-ally, the pull-out strength decreased pre-cipitously within the first 100 cycles until the suture anchor “settled.” Therefore, de-spite the fact that the suture anchor-bone construct is strongest initially, the loads during the first few weeks of rehabilita-tion should be minimized until the suture anchor has “settled” into its final position. Direct application of these data clinically is limited, as cadaveric specimens were used with an average age older than the typical patient undergoing arthroscopic capsulolabral repair. Still, we believe these findings provide some support for minimizing the number and amount of repetitive loads, particularly during the first phase of rehabilitation.92
Because the rotator cuff muscles are not detached during arthroscopic stabi-lization, both passive and/or active as-sistive ROM exercises are appropriate in the early stages of postoperative rehabili-tation. Therefore, unlike rehabilitation of the patient following rotator cuff repair,
TaBle 2Staged Range-of-Motion Goals Following
Arthroscopic Anterior Capsulolabral Repair
Abbreviations: Abd, abduction; AFE, active forward elevation in the scapular plane; NA, not applicable; PER, passive external rotation; PFE, passive forward elevation; POW, postoperative week; WNL, within normal limits.
pfe per at 20° abd per at 90° abd afe
POW 3 90° 10°-30° Contraindicated NA
POW 6 135° 35°-50° 45° 115°
POW 9 155° 50°-65° 75° 145°
POW 12 WNL WNL WNL WNL
40-03 Gaunt.indd 160 2/17/10 2:53:12 PM

journal of orthopaedic & sports physical therapy | volume 40 | number 3 | march 2010 | 161
active assistive exercises can be performed immediately for the patient following ar-throscopic capsulolabral repair.
Forward elevation and external rota-tion in slight abduction within the pre-scribed ROM limits are the glenohumeral motions performed during phase 1, as they allow for glenohumeral ROM without adversely stressing the surgi-cal repair. Exercises to regain forward elevation may include rope-and-pulley-assisted elevation, self-assisted elevation in the supine position, or wand-assisted elevation in the supine position. A table step-back exercise (fiGure 4), where the patient’s hands remain stationary on a surface, while the patient slowly walks his or her body back, bending at the waist to achieve forward elevation, may be help-ful for patients who have difficulty relax-ing. To regain external rotation ROM, the clinician or family member may perform passive external rotation with the arm at the side, or the patient could perform ac-tive assisted external rotation with a cane or bar to assure that ROM limits are not exceeded and the shoulder is not posi-tioned in extension during any external rotation ROM exercise.
To protect the surgical repair, ROM should never be forceful during phase 1. During phase 1, it is recommended that stretching exercises stop at the point when the patient experiences a sensation of a light stretch, as long as the ROM is less than the staged ROM goals. If ROM exceeds the staged goals without any sensation of stretch, then the pa-tient no longer has a ROM deficit. If this circumstance occurs, ROM exercises in this plane are discontinued until ROM is consistent with the staged goals. Dur-ing phase 1, ROM exercises should not be used that stretch into end range external rotation, particularly at 90° of abduction, have the patient positioned in shoulder extension, or stretch into straight-plane abduction, with or without humeral ex-ternal rotation, because they directly stress the anterior or anterior inferior glenohumeral capsule.86
Scapular exercises and active motion
of the uninvolved joints of the upper ex-tremity, such as the elbow or wrist, are recommended during phase 1 but are considered supplementary activities. Exercises to achieve scapular control are encouraged; however, positions and exer-cises that stress the capsulolabral struc-tures should be avoided, such as scapular protraction with concomitant horizontal abduction of the shoulder. Postures or exercises that include scapular retraction should be encouraged, as scapular retrac-tion minimizes the amount of shoulder extension needed for functional tasks and therefore limits stress on the anterior-inferior capsule and labrum.91 However, even though scapular elevation and re-traction are relatively safe, these activities should only be completed with very light or no resistance.
Although the rotator cuff does not specifically require protection following arthroscopic stabilization, glenohumeral active ROM and rotator cuff strengthen-ing are purposefully de-emphasized dur-ing the early postoperative period because of the potentially detrimental effect to the healing tissues.32,92 Light strengthening and active ROM within the staged ROM goals would not likely result in excessive loading; however, in our opinion, it sends an inconsistent message to the patient during this early postoperative period that some strengthening is approved yet significant restrictions of activities of
daily living and immobilization are nec-essary. We believe this inconsistency can lead to excessive arm use, in terms of both loading and ROM, resulting in too much stress to the surgical repair. Heal-ing is the first priority in phase 1. During phase 1, the only form of strengthening recommended is submaximal isometric strengthening of the shoulder and elbow, with the arm adducted to the side in neu-tral rotation.
phase 2: postoperative Weeks 6 to 12Phase 2 begins at postoperative week 6 and after the clinical milestones identified in phase 1 (appenDiX) have been achieved. The focus of this phase is continued pa-tient education regarding postoperative activity limitations, staged ROM goals (TaBle 2), and the initiation of rotator cuff and scapular neuromuscular control activities within the allowed ROM. This is achieved by gradual increase in ROM, submaximal tissue loading, and dynamic stabilization.
The goal is to achieve full ROM in all planes at 12 weeks postoperative, with the exception of end range external rotation at 90° of abduction. The motions of forward elevation and external rotation in slight abduction remain the focus of this phase, and it is also important to measure and, if limited, begin interventions to increase glenohumeral joint horizontal adduction and internal rotation. Posterior shoulder
fiGure 4. (A) Starting position and (B) 90° of shoulder elevation for the table step back exercise.
40-03 Gaunt.indd 161 2/17/10 2:53:14 PM

162 | march 2010 | volume 40 | number 3 | journal of orthopaedic & sports physical therapy
[ clinical commentary ]mobility is important to maintaining nor-mal arthrokinematics of the glenohumeral joint, as a tightness of the posterior shoul-der has been shown to increase superior humeral head migration, which may lead to impingement.28 Cross-body stretching has been shown to yield superior gains in internal rotation ROM when compared to a “sleeper” stretch.60
If forward elevation or external rota-tion ROM lag behind staged ROM goals, joint mobilizations or stretching can be performed. Based upon data regarding fatigue properties of suture anchors,92 rehabilitation professionals should be cautious during the use of joint mobili-zations. We recommend their use only when active assisted and passive ROM has not allowed the patient to achieve staged ROM goals.
In addition, there is an often theo-rized link between anterior glenohumer-al laxity and excessive external rotation ROM, particularly in overhead athletes. Increased laxity5,77 and greater external rotation ROM77 have been found in the dominant shoulders of professional base-ball pitchers. However, this finding is far from universal, as several authors have demonstrated no asymmetry in laxity between the dominant and nondominant shoulders of professional pitchers.12,16 The most direct evidence linking capsular loading, laxity, and ROM may have been provided by Mihata et al,64 who demon-strated a linear increase in length of the inferior glenohumeral ligament and the amount of glenohumeral anterior trans-lation as a result of a prolonged, excessive stretch into external rotation. Therefore, it is important to remember not to per-form passive stretching to gain end range external rotation or external rotation at 90° of abduction unless significant tight-ness is present, as these are the motions that impart the greatest stress to the heal-ing capsulolabral repair.68,86
As ROM targets are met, the focus of rehabilitation can shift to neuromuscu-lar retraining. A program which focuses on scapular stability and maintaining the humeral head in a centralized posi-
tion within the glenoid fossa has been shown to minimize strain on the cap-sule and thereby offers a protective ef-fect for the surgical repair.9,13,49,51 The neuromuscular retraining must be car-ried out within the staged ROM goals, and must provide a stepwise increase in muscular demand. If muscular demand is increased too quickly, abnormal move-ment patterns are likely to occur at the scapulothoracic and glenohumeral joints. We recommend exercises for which the magnitude of specific muscle activation has been documented through electro-myographic studies, to provide the clini-cian with the ability to objectively apply gradually increasing loads to specific muscles.4,8,17,18,20,22,33,36,38,43,54,57,58,66,72,73,85,87 A strengthening program that integrates the ROM progression, progressively in-creasing muscular activity levels, and re-petitive submaximal loading is detailed in the phase 2 strength and endurance section of the appendix.
Progression to active and resistive el-evation activities should be performed in phase 2. We advocate elevation in the scapular plane because, compared to frontal or sagittal plane elevation, scapular plane elevation provides mini-mal capsular stress,21 better subacromial clearance,41 and a more optimal length-tension relationship for the scapula and rotator cuff muscles.56 We advocate us-ing the thumb-up (“full can”) position for active and resisted elevation activities because it provides better subacromial clearance,25 better scapula mechanics,82 and equal rotator cuff activation8 com-pared to the thumb-down (“empty can”) position.
Exercises with weight bearing applied through the upper extremities can be help-ful to achieve correct static and dynamic scapular mechanics; however, the stresses that these exercises place on the surgical repair can be high. Appropriate weight-bearing scapular exercises during phase 2 include maintaining scapular alignment in the quadruped position progressing to 3-point and finally 2-point stabilization.87 While it is tempting to extrapolate this
information to a true push-up exercise, in our opinion, traditional push-ups are not appropriate during phase 2 because they produce relatively high loads on the shoulder and stress the anterior capsule when the arm is brought in horizontal abduction (“down position”). Push-ups performed in standing with hands placed on the wall (ie, wall push-ups, would be appropriate at this time frame). But to the best of our knowledge, the benefits of this exercise have not been quantified in published research.
Patient education regarding appropri-ate positions and loading is crucial during phase 2 so the patient understands that, even though his or her shoulder may be starting to feel much better, there should be no uncontrolled end range stretching, heavy lifting, or quick motions performed with the surgical arm. Loading of the surgical repair must be controlled dur-ing rehabilitation and during activities of daily living as well. The impact of this cannot be overstated, as the patient will spend more time performing activities of daily living than directly performing rehabilitation exercises. Patient educa-tion should stress that tissue healing is incomplete through 12 weeks32 and may not be complete until 40 to 50 weeks postoperatively.30,96
phase 3: postoperative Weeks 12 to 24Phase 3 rehabilitation begins at approxi-mately postoperative week 12, once the criteria to progress to phase 3 (appenDiX) are met. The primary focus of this final phase of rehabilitation is normalizing neuromuscular function with strength-ening, endurance, power, and dynamic stability exercises. This must be contin-ued in a way that assures gradual ad-vancement of stress to the capsulolabral structures through graded progressions of ROM, repetitive submaximal loading, and dynamic stabilization. Any remain-ing limitations in ROM should be di-rectly addressed early in phase 3 through low-load, prolonged stretching and joint mobilizations.
Time frame for the initiation of high-
40-03 Gaunt.indd 162 2/17/10 2:53:14 PM

journal of orthopaedic & sports physical therapy | volume 40 | number 3 | march 2010 | 163
loading exercises and activities following capsular plication or labral repair have not been established.10,44,46 A 12-week pe-riod is often cited as the minimum post-operative time frame to begin vigorous activities,7,23,45,61,94 and this time frame is consistent with our review of the litera-ture for healing rates of the capsulolabral complex.19,96 No clinical trial evidence supports this recommendation, only con-sensus from a multidisciplinary group of rehabilitation specialists. Prior to initiat-ing any high-load activities, the patient should demonstrate excellent shoulder girdle strength, endurance, and neuro-muscular control.
The ultimate goal of rehabilitation is to maximize the patient’s ability to return to full activities of daily living, work, and recreational activities. Setting appropri-ate goals should occur early in the reha-bilitation process and result from a team effort between the patient, physician, and rehabilitation specialist. Because each patient’s goals are different, phase 3 interventions should be tailored to each patient. For example, an athlete who de-sires a return to competitive baseball will require a greater amount of external rota-tion ROM in the 90° abducted position, an ability to control the shoulder girdle at high speeds, and endurance and power of the entire upper extremity, torso, and lower body. In contrast, a patient who desires a return to work on an assembly line may require the ability to lift heavy loads at waist level and moderate loads repeatedly to shoulder level. A patient who desires only to return to normal dai-ly activities would not require extreme ROM and would not require high levels of strength, endurance, and neuromuscu-lar control needed for overhead sport or repetitive work demands.
Although these patients have the same entry point into this last phase of rehabili-tation, every patient is unique and will re-quire goal-specific phase 3 programs. The final rehabilitation step for the sedentary person may be establishing a home exer-cise routine consisting of selected phase 2 exercises. Rehabilitation of the assembly
line worker would emphasize endurance through general weight lifting, as well a progressive routine of functional lifting. Rehabilitation of the throwing athlete would emphasize activities with pro-gressively higher speed and multiplanar sport-specific movements. Examples in-clude exercises performed rapidly against elastic resistance (fiGure 5) and progres-sive plyometrics.24,26,29,59
Due to the extremely high sport-spe-cific stresses placed on the upper quarter with overhead activities, it is necessary to progress to sport-specific programs.1,2,74 These programs should incorporate a gradual build-up in volume and intensi-ty, and include adequate rest.1,2,74 Return to sporting activities should be made in consultation with the surgeon and pa-tient and should not occur until specific milestones are achieved. Athletes must be symptom free and should not return to sport until they have demonstrated appropriate ROM, strength, control, en-durance, and power necessary for their particular sport or activity.
concluSion
aSSET developed this consen-sus rehabilitation guideline based upon 4 critical principles (TaBle 1),
to guide the rehabilitation process and optimize patient outcome. Each funda-mental principle has been reviewed and incorporated into the development of the consensus guideline for which the staged ROM goals (TaBle 2) and time frames of this consensus guideline are based. The graded application of stress to the heal-ing capsulolabral tissues guides reha-bilitation; this stress can be modulated through absolute ROM limits, repeti-tive submaximal loading, and dynamic stabilization.
This document represents a consensus guideline for the typical patient; modifi-cations to the specific application of the guideline may be required, based on the individual patient’s pathology, goals, age, or comorbidities. Because of the wide vari-ety of patients who undergo arthroscopic capsulolabral repair, we feel that final re-
fiGure 5. (A) Starting position and (B) ending position for a high-speed elastic resistance exercise replicating the throwing motion.
40-03 Gaunt.indd 163 2/17/10 2:53:16 PM
164 | march 2010 | volume 40 | number 3 | journal of orthopaedic & sports physical therapy
[ clinical commentary ]
referenceS
1. Axe MJ, Snyder-Mackler L, Konin JG, Strube MJ. Development of a distance-based interval throw-ing program for Little League-aged athletes. Am J Sports Med. 1996;24:594-602.
2. Axe MJ, Windley TC, Snyder-Mackler L. Data-based interval throwing programs for collegiate softball players. J Athl Train. 2002;37:194-203.
3. Bacilla P, Field LD, Savoie FH. Arthroscopic Ban-kart repair in a high-demand patient population. J Arthroscopic and Rel Surg. 1997;13:51-60.
4. Ballantyne BT, O’Hare SJ, Paschall JL, et al. Electromyographic activity of selected shoulder muscles in commonly used therapeutic exer-cises. Phys Ther. 1993;73:668-677.
5. Bigliani LU, Codd TP, Connor PM, Levine WN, Littlefield MA, Hershon SJ. Shoulder motion and laxity in the professional baseball player. Am J Sports Med. 1997;25:609-613.
6. Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC. Tensile properties of the inferior glenohumeral ligament. J Orthop Res. 1992;10:187-197. http://dx.doi.org/10.1002/jor.1100100205
7. Blackburn TA, Guido JA. Rehabilitation after liga-ment and labrum surgery of the shoulder: guid-ing rehabilitation concepts. Journal of Athletic Training. 2000;35:373-381.
8. Blackburn TA, White B, McLeod WD, Wofford L. EMG analysis of posterior rotator cuff exercises. Athl Training. 1990;25:40-45.
9. Blasier RB, Guldberg RE, Rothman ED. Anterior shoulder instability: contribution of rotator cuff
1994;22:779-788. 26. Goldbeck TG, Davies GJ. Test-Retest reliability of
the closed kinetic chain upper extremity stabil-ity test: a clinical field test. Journal of Sports Rehabilitation. 2000;9:35-45.
27. Grana WA, Buckley PD, Yates CK. Arthroscopic Bankart suture repair. Am J Sports Med. 1993;21:348-353.
28. Harryman DT, 2nd, Sidles JA, Clark JM, Mc-Quade KJ, Gibb TD, Matsen FA, 3rd. Translation of the humeral head on the glenoid with passive glenohumeral motion. J Bone Joint Surg Am. 1990;72:1334-1343.
29. Heiderscheit BC, McLean KP, Davies GJ. The effects of isokinetic versus plyometric training of the shoulder internal rotators. J Orthop Sports Phys Ther. 1996;23:125-133.
30. Hiemstra LA, Sasyniuk TM, Mohtadi NG, Fick GH. Shoulder strength after open versus arthroscopic stabilization. Am J Sports Med. 2008;36:861-867. http://dx.doi.org/10.1177/0363546508314429
31. Higgins LD, Warner JJ. Arthroscopic Bankart repair. Operative technique and surgical pitfalls. Clin Sports Med. 2000;19:49-62.
32. Hill AM, Jones IT, Hansen U, et al. Treatment of ligament laxity by electrothermal shrinkage or surgical plication: a morphologic and me-chanical comparison. J Shoulder Elbow Surg. 2007;16:95-100. http://dx.doi.org/10.1016/j.jse.2006.03.003
33. Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ. Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med. 1998;26:210-220.
34. Hubbell JD, Ahmad S, Bezenoff LS, Fond J, Pettrone FA. Comparison of shoulder sta-bilization using arthroscopic transglenoid sutures versus open capsulolabral repairs: a 5-year minimum follow-up. Am J Sports Med. 2004;32:650-654.
35. Humphries W, Jain N, Pietrobon R, Socolowski F, Cook C, Higgins L. Effect of the Deyo score on outcomes and costs in shoulder arthro-plasty patients. J Orthop Surg (Hong Kong). 2008;16:186-191.
36. Illyes A, Kiss RM. Electromyographic analysis in patients with multidirectional shoulder instabil-ity during pull, forward punch, elevation and overhead throw. Knee Surg Sports Traumatol Arthrosc. 2007;15:624-631. http://dx.doi.org/10.1007/s00167-006-0163-1
37. Itoi E, Hatakeyama Y, Urayama M, Pradhan RL, Kido T, Sato K. Position of immobilization after dislocation of the shoulder. A cadaveric study. J Bone Joint Surg Am. 1999;81:385-390.
38. Jaggi A, Malone AA, Cowan J, Lambert S, Bayley I, Cairns MC. Prospective blinded comparison of surface versus wire electromyographic analysis of muscle recruitment in shoulder instability. Physiother Res Int. 2009;14:17-29. http://dx.doi.org/10.1002/pri.407
39. Jobe FW, Giangarra CE, Kvitne RS, Glousman RE. Anterior capsulolabral reconstruction of the
forces and capsular ligaments in a cadaver model. J Shoulder Elbow Surg. 1992;1:140-150.
10. Boileau P, Villalba M, Hery JY, Balg F, Ahrens P, Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006;88:1755-1763. http://dx.doi.org/10.2106/JBJS.E.00817
11. Boissonnault WG, Badke MB, Wooden MJ, Eke-dahl S, Fly K. Patient outcome following rehabili-tation for rotator cuff repair surgery: the impact of selected medical comorbidities. J Orthop Sports Phys Ther. 2007;37:312-319.
12. Borsa PA, Dover GC, Wilk KE, Reinold MM. Glenohumeral range of motion and stiffness in professional baseball pitchers. Med Sci Sports Exerc. 2006;38:21-26.
13. Cain PR, Mutschler TA, Fu FH, Lee SK. Anterior stability of the glenohumeral joint. A dynamic model. Am J Sports Med. 1987;15:144-148.
14. Cleland J. On the actions of muscles pass-ing over more than one joint. J Anat Physiol. 1867;1:85-93.
15. Cole BJ, L’Insalata J, Irrgang J, Warner JJ. Com-parison of arthroscopic and open anterior shoul-der stabilization. A two to six-year follow-up study. J Bone Joint Surg Am. 2000;82-A:1108-1114.
16. Crawford SD, Sauers EL. Glenohumeral joint laxity and stiffness in the functional throwing position of high school baseball pitchers. J Athl Train. 2006;41:52-59.
17. Decker MJ, Hintermeister RA, Faber KJ, Hawkins RJ. Serratus anterior muscle activity during selected rehabilitation exercises. Am J Sports Med. 1999;27:784-791.
18. Decker MJ, Tokish JM, Ellis HB, Torry MR, Hawk-ins RJ. Subscapularis muscle activity during selected rehabilitation exercises. Am J Sports Med. 2003;31:126-134.
19. Delforge G. Musculoskeletal Trauma: Implica-tions for Sports Injury Management. Cham-paign, IL: Human Kinetics; 2002.
20. Dockery ML, Wright TW, LaStayo PC. Elec-tromyography of the shoulder: an analysis of passive modes of exercise. Orthopedics. 1998;21:1181-1184.
21. Doody SG, Freedman L, Waterland JC. Shoulder movements during abduction in the scapular plane. Arch Phys Med Rehabil. 1970;51:595-604.
22. Ekstrom RA, Donatelli RA, Soderberg GL. Sur-face electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther. 2003;33:247-258.
23. Fabbriciani C, Milano G, Demontis A, Fadda S, Ziranu F, Mulas PD. Arthroscopic versus open treatment of Bankart lesion of the shoulder: a prospective randomized study. Arthroscopy. 2004;20:456-462. http://dx.doi.org/10.1016/j.arthro.2004.03.001
24. Falsone SA, Gross MT, Guskiewicz KM, Sch-neider RA. One-arm hop test: reliability and effects of arm dominance. J Orthop Sports Phys Ther. 2002;32:98-103.
25. Flatow EL, Soslowsky LJ, Ticker JB, et al. Excur-sion of the rotator cuff under the acromion. Pat-terns of subacromial contact. Am J Sports Med.
habilitation status should be determined by the patient’s ability to complete his or her desired functional tasks without pain, limitation, or residual sensations of instability. Typically, patients are able to return to low-demand activities at 8 to16 weeks postoperative and return to very high-demand activities at 24 to 32 weeks. Periodic updates to this guideline will be necessary, as arthroscopic surgical tech-niques improve and our understanding of the implementation and effects of specific therapeutic interventions evolves. t
ACKNOWLEDGEMENTS: The authors would like to acknowledge the members of The Ameri-can Society of Shoulder and Elbow Thera-pists (www.asset-usa.org) for their expertise in the development this international consen-sus guideline. The authors would also like to acknowledge Carol Capers, MSMI, CMI, for creating the figures.
40-03 Gaunt.indd 164 2/17/10 2:53:17 PM
journal of orthopaedic & sports physical therapy | volume 40 | number 3 | march 2010 | 165
YH. Comparative evaluation of the measurement properties of various shoulder outcome instru-ments. Am J Sports Med. 2009;37:1161-1168.
70. Plancher KD, Lipnick SL. Analysis of evidence-based medicine for shoulder instability. Arthroscopy. 2009;25:897-908. http://dx.doi.org/10.1016/j.arthro.2009.03.017
71. Pollock RG, Wang VM, Bucchieri JS, et al. Effects of repetitive subfailure strains on the mechani-cal behavior of the inferior glenohumeral liga-ment. J Shoulder Elbow Surg. 2000;9:427-435. http://dx.doi.org/10.1067/mse.2000.108388
72. Reinold MM, Macrina LC, Wilk KE, et al. Electro-myographic analysis of the supraspinatus and deltoid muscles during 3 common rehabilitation exercises. J Athl Train. 2007;42:464-469.
73. Reinold MM, Wilk KE, Fleisig GS, et al. Elec-tromyographic analysis of the rotator cuff and deltoid musculature during common shoulder external rotation exercises. J Orthop Sports Phys Ther. 2004;34:385-394.
74. Reinold MM, Wilk KE, Reed J, Crenshaw K, An-drews JR. Interval sport programs: guidelines for baseball, tennis, and golf. J Orthop Sports Phys Ther. 2002;32:293-298.
75. Roth CA, Bartolozzi AR, Ciccotti MG, et al. Fail-ure properties of suture anchors in the glenoid and the effects of cortical thickness. Arthros-copy. 1998;14:186-191.
76. Schollmeier G, Uhthoff HK, Sarkar K, Fukuhara K. Effects of immobilization on the capsule of the canine glenohumeral joint. A structural func-tional study. Clin Orthop Relat Res. 1994;37-42.
77. Sethi PM, Tibone JE, Lee TQ. Quantitative assessment of glenohumeral translation in baseball players: a comparison of pitchers versus nonpitching athletes. Am J Sports Med. 2004;32:1711-1715.
78. Smith J, Dahm DL, Kotajarvi BR, et al. Elec-tromyographic activity in the immobilized shoulder girdle musculature during ipsilateral kinetic chain exercises. Arch Phys Med Rehabil. 2007;88:1377-1383. http://dx.doi.org/10.1016/j.apmr.2007.07.028
79. Smith J, Dietrich CT, Kotajarvi BR, Kaufman KR. The effect of scapular protraction on isometric shoulder rotation strength in normal subjects. J Shoulder Elbow Surg. 2006;15:339-343. http://dx.doi.org/10.1016/j.jse.2005.08.023
80. Speer KP. Anatomy and pathomechan-ics of shoulder instability. Clin Sports Med. 1995;14:751-760.
81. Terry GC, Hammon D, France P, Norwood LA. The stabilizing function of passive shoulder restraints. Am J Sports Med. 1991;19:26-34.
82. Thigpen CA, Padua DA, Morgan N, Kreps C, Karas SG. Scapular kinematics during supraspi-natus rehabilitation exercise: a comparison of full-can versus empty-can techniques. Am J Sports Med. 2006;34:644-652. http://dx.doi.org/10.1177/0363546505281797
83. Ticker JB, Warner JJ. Selective capsular shift technique for anterior and anterior-inferior glenohumeral instability. Clin Sports Med. 2000;19:1-17.
shoulder in athletes in overhand sports. Am J Sports Med. 1991;19:428-434.
40. Johnson LL. The shoulder joint. An arthrosco-pist’s perspective of anatomy and pathology. Clin Orthop Relat Res. 1987;113-125.
41. Johnston TB. The movements of the shoulder-joint: a plea for the use of the “plane of the scapula” as the plane of reference for move-ments occurring at the humero-scapular joint. British Journal of Surgery. 1937;25:252-260.
42. Karduna AR, Williams GR, Williams JL, Ian-notti JP. Kinematics of the glenohumeral joint: influences of muscle forces, ligamentous con-straints, and articular geometry. J Orthop Res. 1996;14:986-993. http://dx.doi.org/10.1002/jor.1100140620
43. Kibler WB, Chandler TJ, Shapiro R, Conuel M. Muscle activation in coupled scapulohumeral motions in the high performance tennis serve. Br J Sports Med. 2007;41:745-749. http://dx.doi.org/10.1136/bjsm.2007.037333
44. Kim SH, Ha KI. Bankart repair in trau-matic anterior shoulder instability: open versus arthroscopic technique. Arthroscopy. 2002;18:755-763.
45. Kim SH, Ha KI, Cho YB, Ryu BD, Oh I. Ar-throscopic anterior stabilization of the shoulder: two to six-year follow-up. J Bone Joint Surg Am. 2003;85-A:1511-1518.
46. Kim SH, Ha KI, Jung MW, Lim MS, Kim YM, Park JH. Accelerated rehabilitation after arthroscopic Bankart repair for selected cases: a prospec-tive randomized clinical study. Arthroscopy. 2003;19:722-731.
47. Kirkley A, Griffin S, McLintock H, Ng L. The de-velopment and evaluation of a disease-specific quality of life measurement tool for shoulder instability. The Western Ontario Shoulder Instability Index (WOSI). Am J Sports Med. 1998;26:764-772.
48. Kocher MS, Horan MP, Briggs KK, Richardson TR, O’Holleran J, Hawkins RJ. Reliability, validity, and responsiveness of the American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis. J Bone Joint Surg Am. 2005;87:2006-2011. http://dx.doi.org/10.2106/JBJS.C.01624
49. Labriola JE, Lee TQ, Debski RE, McMahon PJ. Stability and instability of the glenohumeral joint: the role of shoulder muscles. J Shoulder Elbow Surg. 2005;14:32S-38S. http://dx.doi.org/10.1016/j.jse.2004.09.014
50. LaPrade RF, Brown GA. Recurrent anterior instabil-ity: open surgical treatment. In: Warren RF, Craig EV, Altchek D, eds. The Unstable Shoulder. Phila-delphia, PA: Lippincott-Raven; 1999:205-223.
51. Lee SB, Kim KJ, O’Driscoll SW, Morrey BF, An KN. Dynamic glenohumeral stability provided by the rotator cuff muscles in the mid-range and end-range of motion The Journal of Bone and Joint Surgery. 2000;82:849-857.
52. Levine WN, Rieger K, McCluskey GM, 3rd. Arthroscopic treatment of anterior shoulder instability. Instr Course Lect. 2005;54:87-96.
53. Lin TW, Cardenas L, Soslowsky LJ. Biomechan-ics of tendon injury and repair. J Biomech. 2004;37:865-877. http://dx.doi.org/10.1016/j.jbiomech.2003.11.005
54. Lister JL, Del Rossi G, Ma F, et al. Scapular stabilizer activity during Bodyblade, cuff weights, and Thera-Band use. J Sport Rehabil. 2007;16:50-67.
55. Louie JK, Mote CD. Contribution of the muscu-lature to rotatory laxity and torsional stiffness at the knee. J Biomech. 1987;20:281-300.
56. Lucas DB. Biomechanics of the shoulder joint. Arch Surg. 1973;107:425-432.
57. Ludewig PM, Hoff MS, Osowski EE, Meschke SA, Rundquist PJ. Relative balance of serratus anterior and upper trapezius muscle activity during push-up exercises. Am J Sports Med. 2004;32:484-493.
58. Maenhout A, Van Praet K, Pizzi L, Van Herzeele M, Cools A. Electromyographic analysis of knee push up plus variations: what’s the influence of the kinetic chain on scapular muscle activity? Br J Sports Med. 2009;14 Sept: Epub.
59. Manske R, Davies GJ. Post-rehabilitation out-comes of muscle power (torque acceleration energy) in patients with selected shoulder con-ditions. J Sport Rehabil. 2003;12:181-198.
60. McClure P, Balaicuis J, Heiland D, Broersma ME, Thorndike CK, Wood A. A randomized controlled comparison of stretching procedures for pos-terior shoulder tightness. J Orthop Sports Phys Ther. 2007;37:108-114.
61. McDermott DM, Neumann L, Frostick SP, Wal-lace WA. Early results of Bankart repair with a patient-controlled rehabilitation program. J Shoulder Elbow Surg. 1999;8:146-150.
62. McEleney ET, Donovan MJ, Shea KP, Nowak MD. Initial failure strength of open and arthroscopic Bankart repairs. Arthroscopy. 1995;11:426-431.
63. Michener LA, McClure PW, Sennett BJ. Ameri-can Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: reliability, validity, and responsiveness. J Shoulder Elbow Surg. 2002;11:587-594. http://dx.doi.org/10.1067/mse.2002.127096
64. Mihata T, Lee Y, McGarry MH, Abe M, Lee TQ. Excessive humeral external rotation results in increased shoulder laxity. Am J Sports Med. 2004;32:1278-1285. http://dx.doi.org/10.1177/0363546503262188
65. Morgan CD, Bodenstab AB. Arthroscopic Ban-kart suture repair: technique and early results. Arthroscopy. 1987;3:111-122.
66. Moseley JB, Jr, Jobe FW, Pink M, Perry J, Tibone J. EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med. 1992;20:128-134.
67. Nelson BJ, Arciero RA. Arthroscopic manage-ment of glenohumeral instability. Am J Sports Med. 2000;28:602-614.
68. O’Connell PW, Nuber GW, Mileski RA, Lauten-schlager E. The contribution of the glenohumer-al ligaments to anterior stability of the shoulder joint. Am J Sports Med. 1990;18:579-584.
69. Oh JH, Jo KH, Kim WS, Gong HS, Han SG, Kim
40-03 Gaunt.indd 165 2/17/10 2:53:18 PM
166 | march 2010 | volume 40 | number 3 | journal of orthopaedic & sports physical therapy
[ clinical commentary ]
@ More inforMaTionWWW.jOSpT.OrG
84. Torchia ME, Caspari RB, Asselmeier MA, Beach WR, Gayari M. Arthroscopic transglenoid mul-tiple suture repair: 2 to 8 year results in 150 shoulders. Arthroscopy. 1997;13:609-619.
85. Townsend H, Jobe FW, Pink M, Perry J. Electro-myographic analysis of the glenohumeral mus-cles during a baseball rehabilitation program. Am J Sports Med. 1991;19:264-272.
86. Turkel SJ, Panio MW, Marshall JL, Girgis FG. Stabilizing mechanisms preventing anterior dis-location of the glenohumeral joint. J Bone Joint Surg Am. 1981;63:1208-1217.
87. Uhl TL, Carver TJ, Mattacola CG, Mair SD, Nitz AJ. Shoulder musculature activation during up-per extremity weight-bearing exercise. J Orthop Sports Phys Ther. 2003;33:109-117.
88. Warner JJ, Miller MD, Marks P. Arthroscopic Bankart repair with the Suretac device. Part II: Experimental observations. Arthroscopy. 1995;11:14-20.
89. Warner JJ, Miller MD, Marks P, Fu FH. Ar-throscopic Bankart repair with the Suretac de-vice. Part I: Clinical observations. Arthroscopy. 1995;11:2-13.
90. Warner JP. Anatomy, biomechanics, and pathophysiology of glenohumeral instability. In: Warren RF, Craig EV, Altchek D, eds. The Unsta-ble Shoulder. Philadelphia, PA: Lippincott-Raven; 1999:
91. Weiser WM, Lee TQ, McMaster WC, McMahon PJ. Effects of simulated scapular protraction on an-terior glenohumeral stability. Am J Sports Med. 1999;27:801-805.
92. Wetzler MJ, Bartolozzi AR, Gillespie MJ, et al. Fatigue properties of suture anchors in anterior shoulder reconstructions: Mitek GII. Arthros-copy. 1996;12:687-693.
93. Wilk KE. Rehabilitation after shoulder stabiliza-tion surgery. In: Warren RF, Craig EV, Altchek D, eds. The Unstable Shoulder. Philadelphia, PA:
Lippincott-Raven; 1999:367-402. 94. Wilk KE, Reinold MM, Arrigo A, Moser MW,
Dugas JR, Andrews JR. Current concepts in the recognition and treatment of superior labral (SLAP) lesions. J Orthop Sports Phys Ther. 2005;35:273-291. http://dx.doi.org/10.2519/jospt.2005.1701
95. Wilk KE, Reinold MM, Dugas JR, Andrews JR. Rehabilitation following thermal-assisted capsular shrinkage of the glenohumeral joint: current concepts. J Orthop Sports Phys Ther. 2002;32:268-292.
96. Woo SL, Chan SS, Yamaji T. Biomechanics of knee ligament healing, repair and reconstruc-tion. J Biomech. 1997;30:431-439.
appenDiX
phase 1: poW 0 to poW 6
Goals• Maximallyprotectthesurgicalrepair(capsule,liga-
ments, labrum, sutures)• AchievestagedROMgoals.Donotsignificantlyexceed
them:- PFE: POW 3, 90°; POW 6, 135°- PER at 20° abd: POW 3, 10°-30°; POW 6, 35°-50°- PER at 90° abd: POW 3, contraindicated; POW 6, 45°- AFE: POW 3, NA; POW 6, 115°
• Patienteducationinpostoperativerestrictions• Minimizeshoulderpainandinflammatoryresponse• Ensureadequatescapularfunction
Interventions to Avoid• DonotalloworperformROM/stretchingsignificantly
beyond staged ROM goals, especially external rotation both by the side and in abduction
• Donotallowthepatienttousearmforheavyliftingorany use of the arm that requires ROM greater than the staged ROM goals
Specific InterventionsActivities of primary importance:• Patienteducationregardinglimitinguseofthearm
despite lack of pain or other symptoms• Protectionofrepair• AchievestagedROMgoalsthroughgentleROM
activities• MinimizeinflammationSupplementary activities:• Normalizescapularposition,mobility,anddynamic
stability• ROMofuninvolvedjoints• Beginrestorationofshoulderstrengththroughisomet-
ric exercisesImmobilization:• Viastandardsling• Absoluteimmobilization(noglenohumeralROM
exercises and constant sling use) for variable time of 0 up to 4 weeks, based on patient-specific factors and surgeon recommendation
• Relativeimmobilization(outofslingforROMexercises,sitting with the arm supported, and standing for short periods), starting after the period of absolute immo-bilization and continuing for the remainder of phase 1, followed by sling use for comfort
Patient education:• Explainnatureofthesurgery• Discussprecautionsspecifictothenatureofthesurgi-
cal repair
- Importance of not significantly exceeding staged ROM goals
- Importance of tissue healing- Proper sling use (assure sling provides upward sup-
port to the glenohumeral joint)- Limiting use of arm for ADLs
ROM:• Followingtheabsoluteimmobilizationperiodbegin:
- Pendulum exercises (unweighted)- Passive/active assisted forward elevation to achieve
staged ROM goals listed earlier. ROM should not be forceful
- Passive/active assisted external rotation with the shoulder in slight abduction to achieve staged ROM goals listed earlier. ROM should not be forceful
- Scapular clock exercises or alternately elevation, depression, protraction, retraction. Progress to scapular strengthening as patient tolerates78,79
• ActiveROMofuninvolvedjointsMiscellaneous:• Submaximalrotatorcuffisometricsastolerated• Posturalawareness/educationPain management:• Activityrestriction• Properfittingofslingtosupportarm• Electrophysicalagents
The aMerican SocieTy of ShoulDer anD elBoW TherapiSTS’ conSenSuS rehaBiliTaTion GuiDeline for arThroScopic anTerior capSulolaBral repair of The ShoulDer
40-03 Gaunt.indd 166 2/17/10 2:53:20 PM
journal of orthopaedic & sports physical therapy | volume 40 | number 3 | march 2010 | 167
appenDiX (conTinueD)
• Physicianprescribedorover-the-countermedications
Milestones (Testing Criteria) to Progress to Phase 2• Appropriatehealingofthesurgicalrepairbyadhering
to the precautions and immobilization guidelines.• StagedROMgoalsachievedbutnotsignificantly
exceeded• Minimaltonopain(NPRS,0-2/10)withROM
phase 2: poW 6 to poW 12
Goals• AchievestagedROMgoalstonormalizepassiveROM
and active ROM. Do not significantly exceed:- PFE: POW 9, 155°; POW 12, WNL- PER at 20° abd: POW 9, 50°-65°; POW 12, WNL- PER at 90° abd: POW 9, 75°; POW 12, WNL- AFE: POW 9, 145°; POW 12, WNL
• Minimizeshoulderpain• Begintoincreasestrengthandendurance• Increasefunctionalactivities
Interventions to Avoid• Donotperformstretchingsignificantlybeyondstaged
ROM goals• Donotperformanystretchtogainendrangeexternal
rotation or external rotation at 90º of abduction unless significant tightness is present
• Donotallowthepatienttousearmforheavyliftingor any activities that require ROM beyond the staged ROM goals
• Donotperformanystrengtheningexercisesthatplacea large load on the shoulder in the position of horizontal abduction or the combined position of abduction with external rotation (eg, no push-ups, bench press, pectoralis flys)
• Donotperformscapularplaneabductionwithinternalrotation (empty can) at any stage of rehabilitation due to the likelihood of impingement
Specific InterventionsActivities of primary importance• Continuedpatienteducation• Passive/activeassistedROMasneededtoachievebut
not significantly exceed staged ROM goals• Establishbasicrotatorcuffandscapularneuromuscu-
lar control within the allowed ROMSupplementary activities:• Introductionoffunctionalpatternsofmovement• ProgressiveenduranceexercisesPatient education:• Counselaboutusingtheupperextremityforappropri-
ate ADLs in the pain-free ROM (starting with waist-level activities and progressing to shoulder-level and finally to overhead activities over time)
• Continueeducationregardingavoidanceofheavyliftingor quick, sudden motions
• Educationtoavoidpositionsthatplacestressontheanterior inferior capsule during ADLs
ROM:• Passive/activeassistedROMasneededtoachieve
staged ROM goals in all planes. Many times only light stretching or no stretching is needed
• IfROMissignificantlylessthanstagedROMgoals,gentle joint mobilizations may be performed. However, they should be done only into the limited directions and only until staged ROM goals are achieved
• Addressscapulothoracicandtrunkmobilitylimitations.Ensure normal cervical spine ROM and thoracic spine extension to facilitate full upper extremity ROM
Neuromuscular re-education:• Addressabnormalscapularalignmentandmobility
PRN - Strengthen scapular retractors and upward rotators
- Increase pectoralis minor flexibility if limited- Biofeedback by auditory, visual, or tactile cues- Weight-bearing exercises with a fixed distal
segment. Examples: quadruped position while working to maintain proper position of the scapula, quadruped with scapula protraction, progressing from quadruped to tripod position, no push-ups87
• AddresscorestabilitydeficitsPRN• Activitiestoimproveneuromuscularcontrolofthe
rotator cuff and shoulder girdle such as use of unstable surfaces, Bodyblade, manual resistance exercises
Strength/endurance:• Scapulaandcorestrengthening• Balancedrotatorcuffstrengtheningtomaintainthe
humeral head centered within the glenoid fossa during progressively more challenging activities- Should be initially performed in a position of com-
fort with low stress to the glenohumeral joint, such as less than 45° elevation in the plane of the scapula (eg, elastic band or dumbbell external rotation, internal rotation, forward flexion)
- Exercises should be progressive in terms of shoulder elevation (eg, start with exercises performed at waist level progressing to shoulder level and finally overhead activities)
- Exercises should be progressive in terms of muscle demand. It is suggested to use activities that have muscle activity levels documented with EMG4,8,17,18,20,
22,33,36,38,43,54,57,58,66,72,73,85,87
- Elevation activities may progress from assistive exercises (eg, rope and pulley, wall walks) to active, to resistive upright exercises, then, finally, to prone exercises
- Nearly full active elevation in the plane of the scapula should be achieved before progressing to elevation in other planes
- Exercises should be progressive in terms of adding stress to the anterior capsule, gradually working towards a position of elevated external rotation in the coronal plane, the “90-90” position PRN
- Rehabilitation activities should be pain free and per-formed without substitutions or altered movement patterns
- Rehabilitation may include both weight-bearing and non–weight-bearing activities
- Rehabilitation may include both isolated and complex movement patterns
- Depending upon the goals of the exercise (control versus strengthening), rehabilitation activities may also be progressive in terms of speed once the patient demonstrates proficiency at slower speeds
- The rotator cuff and scapula stabilizer strengthen-ing program should emphasize high repetitions (typically 30-50 reps) and relatively low resistance (typically 1-2 kg)
- No heavy lifting or plyometrics should be performed during this stage
- Elbow flexion/extension strengthening with elbow by the side can begin in this phase
Pain management:• EnsureappropriateuseofarmduringADLs• Ensureappropriateleveloftherapeuticinterventions• Electrophysicalagentsasneeded
Milestones to Progress to Phase 3• StagedactiveROMgoalsachievedwithminimaltono
pain (NPRS, 0-2/10) and without substitution patterns• Appropriatescapularpostureatrestanddynamic
scapular control during ROM and strengthening exercises
• Strengtheningactivitiescompletedwithminimaltonopain (NPRS 0-2/10)
phase 3: poW 12 to poW 24
Goals• Normalizestrength,endurance,neuromuscularcontrol,
and power• Gradualandplannedbuild-upofstresstoanterior
capsulolabral tissues• GradualreturntofullADLs,work,andrecreational
activities
Interventions to Avoid• Donotincreasestresstotheshoulderinashortperiod
or in an uncontrolled manner• Donotperformadvancedrehabilitationexercises(such
as plyometrics or exercises requiring end range ROM) if the patient does not perform these activities during ADLs, work, or recreation
• Donotprogressintoactivity-specifictraininguntilpatient has nearly full ROM and strength
• Donotperformweightliftingactivitiesthatplaceex-cessive stress on the anterior capsule. For instance, latissimus pull-downs, and military press performed with the hands behind the head stress the anterior
40-03 Gaunt.indd 167 2/17/10 2:53:20 PM
168 | march 2010 | volume 40 | number 3 | journal of orthopaedic & sports physical therapy
[ clinical commentary ]
appenDiX (conTinueD)
capsule with no additional benefit in terms of muscle activity. Similarly, activities which encourage end range shoulder extension, such as dips, should also be avoided
Specific InterventionsActivities of primary importance:• Progressivestrengtheningandenduranceexercises• Progressiveneuromuscularcontrolexercises• Activity-specificprogression:sport,work,hobbiesSupplementary activities:• NormalizecoreandscapularstabilityPatient education:• Counselinimportanceofgraduallyincreasingstressto
the shoulder while returning to normal ADLs, work, and recreational activities, including heavy lifting, repetitive activities, and overhead sports
ROM:• PassiveROM,stretching,andjointmobilizationsas
needed to address any remaining deficitsNeuromuscular re-education:• Addressanyremainingdeficitsoftherotatorcuff,
scapula musculature, or trunk musculatureStrength/endurance/power:• Continueshoulder-strengtheningprogramasinitiated
in phase 2, with increasing emphasis on high-speed multiplanar activities that incorporate the entire kinetic chain
• Graduallyprogressrehabilitationactivitiestoreplicatedemanding ADL/work activities
• Progressivereturntoweight-liftingprogramemphasiz-ing the larger, primary mover upper extremity muscles (deltoid, latissimus dorsi, pectoralis major)- Start with relatively lightweight and high repetitions
(sets of 15-25 repetitions), and gradually decrease repetitions and increase weight after several months
- Suggested upper extremity exercises for early phase 3 • Bicepscurls,shoulderadducted(addedin
phase 2) • Tricepspress-downsorkick-backs,shoulder
adducted (added in phase 2) • Shouldershrugs • Rows(scapularretraction),shoulderadducted • Latissimusbarpull-downs,withhandsinfront
of the head • Dumbbelloverheadshoulderpresswith
hands starting in front of the shoulders (not in the abducted/externally rotated position)
• Push-upsaslongastheelbowsdonotflex past 90º
- Suggested upper extremity exercises to be added in intermediate phase 3• Isotonicpressingactivities(eg,flatorincline
presses using machines, barbells, or dumbbells)• Dumbbellshoulderraisesto90º• Rows(scapularretraction),shoulderselevated• Machineorbarbellshoulderpressesthatdonot
require end range abduction/external rotation- Suggested upper extremity exercises to be added in
late phase 3• Overheadpresseswithshouldersinabduction
with external rotation (military press)• Pectoralismajorflys• Deadlift• Powercleans
- Upper extremity exercises that are not advisable for this patient population• Dips• Latissimuspull-downsormilitarypresswiththe
bar behind headPlyometric program (as necessary):• Criteriatoinitiateplyometricprogram
- Goals of returning to overhead athletics or other work or recreational activities requiring large amounts of upper extremity power
- Adequate strength (4+/5) of entire shoulder girdle musculature
- Pain free with basic ADLs and current strengthening program
- At least 3 weeks of tolerance to high-speed multi-planar activities that progressively mimic functional demands
• Parameters- Due to the explosive nature of this type of exercise,
emphasis of plyometrics exercises should be on quality not quantity
- Perform a few times a week and utilize moderate repetitions (eg, 3-5 sets of 15-20 repetitions)
- Begin with unweighted balls and progress to lightly weighted balls (plyoballs)
Interval sport programs for activities such as throwing, swimming, and golf, once approved by physician (usually POW 16 or longer)
Milestones to Return to Work, Hobbies, Sport• Clearancefromphysician• Nocomplaintsofpainatrestandminimaltonopain
(NPRS 0-2/10) with activities• Noorminimalsensationofinstabilitywithactivities• RestorationofsufficientROMtoperformdesiredactivi-
ties• Adequatestrengthandenduranceofrotatorcuffand
scapular muscles to perform activities with minimal to no pain (NPRS 0-2/10) or difficulty
• Ifthepatientstruggleswithconfidenceorshoulderstability, a stabilizing brace may be considered for return to activity, but is most commonly used only for collision sports
Abbreviations: Abd, abduction; ADL, activities of daily living; AFE, active forward elevation; EMG, electromyography; NPRS, numeric pain rating scale; PER, passive external rotation; PFE, passive forward elevation; POW, postoperative week; ROM, range of motion; WNL, within normal limits.
DOWNLOAD PowerPoint Slides of JOSPT Figures & Tables
JOSPT offers PowerPoint slides of figures and tables to accompany selected articles on the Journal’s website (www.jospt.org). These slides can be downloaded and saved and include the article title, authors, and full citation. With each article where this feature is available, click “View Slides” and then right click on the link and select “Save Target As”.
40-03 Gaunt.indd 168 2/17/10 2:53:21 PM
38 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]KEVIN E. WILK, PT, DPT¹ MD² DPT³
MD4 MD4 MD5
Shoulder Injuries in the Overhead Athlete
1Vice President of Education, Physiotherapy Associates, Exton, PA; Associate Clinical Director, Champion Sports Medicine, A Physiotherapy Associates Clinic, Birmingham,AL; Director of Rehabilitation Research, American Sports Medicine Institute, Birmingham, AL; Rehabilitation Consultant, Tampa Bay Rays Baseball Organization, Tampa Bay,
FL. ² Orthopaedic Sports Medicine Fellow, Andrews Sports Medicine, Birmingham, AL. ³ Physical Therapy Fellow, Champion Sports Medicine, Birmingham, AL. 4OrthopaedicSurgeon, Andrews Sports Medicine Center, Birmingham, AL. 5Orthopaedic Surgeon, Andrews Sports Medicine Center, Birmingham, AL; Medical Director, Tampa Bay RaysBaseball Organization, Tampa Bay, FL. Address correspondence to Dr Kevin E. Wilk, Champion Sports Medicine, 805 St Vincent’s Drive, Suite C100, Birmingham, AL 35205.E-mail: [email protected]
The overhead throwing motion is a highly skilled movementperformed at extremely high velocity, which requiresflexibility, muscular strength, coordination, synchronicity,and neuromuscular control. The throwing motion generates
extraordinary demands on the shoulder joint. It is because of thesehigh forces, which are repetitively applied, that the shoulder is themost commonly injured joint in professional baseball pitchers.27
isometric contraction (MVIC).34 Lastly,the thrower’s shoulder often exhibitsexcessive motion and laxity. Wilk et al112
stated that the thrower’s shoulder mustbe “loose enough to throw but stableenough to prevent symptoms.” Whetherthe typical injury sustained to the throw-er’s shoulder is due to hyperlaxity orcapsular tightness is currently a contro-versial topic of discussion. Shoulder pa-thology can manifest as pain, diminishedperformance (velocity and accuracy), or adecrease in strength or range of motion.The challenge for medical practitionersis to determine the accurate differentialdiagnosis, the cause of the injury, and themost effective treatment plan based onthe identified pathology.
In this manuscript, we will discuss thephysical characteristic of the overheadathlete, common pathologies seen, andthe nonoperative, surgical, and postop-erative treatment.
It is important for the clinicianto realize and appreciate the “typical”physical characteristics of the over-
head thrower.
Most throwers exhibit an obvious motiondisparity, whereby shoulder external ro-tation (ER) is excessive and internal rota-tion (IR) is limited when measured at 90°
During the throwing movement, tre-mendous forces are placed on the shoul-der joint at extremely high angularvelocities. The acceleration phaseof the pitch is the fastest move-ment recorded and reaches a peakangular velocity of 7250°/s.41,43 Ithas been estimated that the an-terior translation forces generatedwhen pitching are equal to one-half
body weight (BW) during the late cock-ing phase, and there is a distraction force
equal to BW during the decelerationphase.43 Consequently, throwingrequires a high level of muscleactivation, as indicated by theelectromyographic signal of the
shoulder musculature, which canexceed 80% to 100% of the signal
measured during a maximum voluntary
The overhead throwing motion is anextremely skillful and intricate movement. Whenpitching, the overhead throwing athlete placesextraordinary demands on the shoulder complexsubsequent to the tremendous forces that are gen-erated. The thrower’s shoulder must be lax enoughto allow excessive external rotation but stableenough to prevent symptomatic humeral headsubluxations, thus requiring a delicate balancebetween mobility and functional stability. We referto this as the “thrower’s paradox.” This balance isfrequently compromised and believed to lead tovarious types of injuries to the surrounding tissues.Frequently, injuries can be successfully treatedwith a well-structured and carefully implementednonoperative rehabilitation program. The key tosuccessful nonoperative treatment is a thorough
clinical examination and accurate diagnosis.Rehabilitation follows a structured, multiphaseapproach, with emphasis on controlling inflamma-tion, restoring muscles’ balance, improving softtissue flexibility, enhancing proprioception andneuromuscular control, and efficiently returningthe athlete to competitive throwing. Athletes oftenexhibit numerous adaptive changes that developfrom the repetitive microtraumatic stresses occur-ring during overhead throwing. Treatment shouldinclude the restoration of these adaptations.
Level 5. J OrthopSports Phys Ther 2009;39(2):38-54. doi:10.2519/jospt.2009.2929
baseball, glenohumeral joint,labral lesions, pitching, rotator cuff
SUPPLEMENTALVIDEO ONLINE
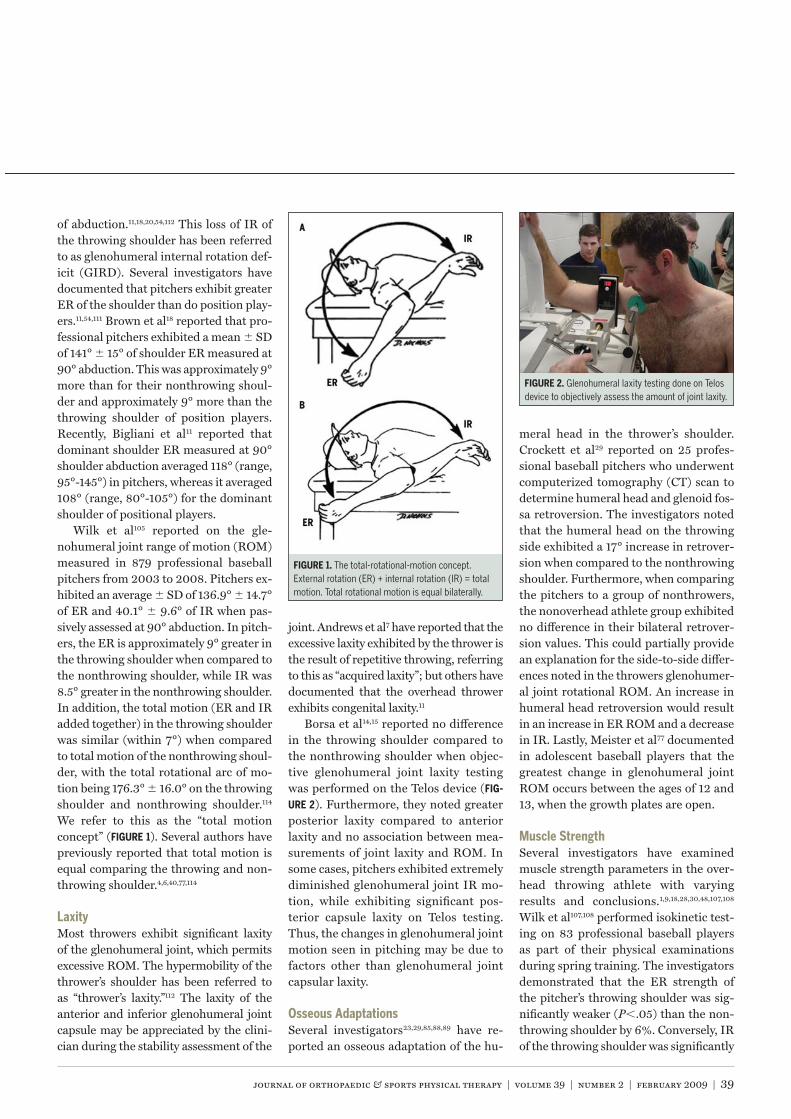
journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 39
of abduction.11,18,20,54,112 This loss of IR ofthe throwing shoulder has been referredto as glenohumeral internal rotation def-icit (GIRD). Several investigators havedocumented that pitchers exhibit greaterER of the shoulder than do position play-ers.11,54,111 Brown et al18 reported that pro-fessional pitchers exhibited a mean SDof 141° 15° of shoulder ER measured at90° abduction. This was approximately 9°more than for their nonthrowing shoul-der and approximately 9° more than thethrowing shoulder of position players.Recently, Bigliani et al11 reported thatdominant shoulder ER measured at 90°shoulder abduction averaged 118° (range,95°-145°) in pitchers, whereas it averaged108° (range, 80°-105°) for the dominantshoulder of positional players.
Wilk et al105 reported on the gle-nohumeral joint range of motion (ROM)measured in 879 professional baseballpitchers from 2003 to 2008. Pitchers ex-hibited an average SD of 136.9° 14.7°of ER and 40.1° 9.6° of IR when pas-sively assessed at 90° abduction. In pitch-ers, the ER is approximately 9° greater inthe throwing shoulder when compared tothe nonthrowing shoulder, while IR was8.5° greater in the nonthrowing shoulder.In addition, the total motion (ER and IRadded together) in the throwing shoulderwas similar (within 7°) when comparedto total motion of the nonthrowing shoul-der, with the total rotational arc of mo-tion being 176.3° 16.0° on the throwingshoulder and nonthrowing shoulder.114
We refer to this as the “total motionconcept” ( ). Several authors havepreviously reported that total motion isequal comparing the throwing and non-throwing shoulder.4,6,40,77,114
Most throwers exhibit significant laxityof the glenohumeral joint, which permitsexcessive ROM. The hypermobility of thethrower’s shoulder has been referred toas “thrower’s laxity.”112 The laxity of theanterior and inferior glenohumeral jointcapsule may be appreciated by the clini-cian during the stability assessment of the
joint. Andrews et al7 have reported that theexcessive laxity exhibited by the thrower isthe result of repetitive throwing, referringto this as “acquired laxity”; but others havedocumented that the overhead throwerexhibits congenital laxity.11
Borsa et al14,15 reported no differencein the throwing shoulder compared tothe nonthrowing shoulder when objec-tive glenohumeral joint laxity testingwas performed on the Telos device ( -
). Furthermore, they noted greaterposterior laxity compared to anteriorlaxity and no association between mea-surements of joint laxity and ROM. Insome cases, pitchers exhibited extremelydiminished glenohumeral joint IR mo-tion, while exhibiting significant pos-terior capsule laxity on Telos testing.Thus, the changes in glenohumeral jointmotion seen in pitching may be due tofactors other than glenohumeral jointcapsular laxity.
Several investigators23,29,85,88,89 have re-ported an osseous adaptation of the hu-
meral head in the thrower’s shoulder.Crockett et al29 reported on 25 profes-sional baseball pitchers who underwentcomputerized tomography (CT) scan todetermine humeral head and glenoid fos-sa retroversion. The investigators notedthat the humeral head on the throwingside exhibited a 17° increase in retrover-sion when compared to the nonthrowingshoulder. Furthermore, when comparingthe pitchers to a group of nonthrowers,the nonoverhead athlete group exhibitedno difference in their bilateral retrover-sion values. This could partially providean explanation for the side-to-side differ-ences noted in the throwers glenohumer-al joint rotational ROM. An increase inhumeral head retroversion would resultin an increase in ER ROM and a decreasein IR. Lastly, Meister et al77 documentedin adolescent baseball players that thegreatest change in glenohumeral jointROM occurs between the ages of 12 and13, when the growth plates are open.
Several investigators have examinedmuscle strength parameters in the over-head throwing athlete with varyingresults and conclusions.1,9,18,28,30,48,107,108
Wilk et al107,108 performed isokinetic test-ing on 83 professional baseball playersas part of their physical examinationsduring spring training. The investigatorsdemonstrated that the ER strength ofthe pitcher’s throwing shoulder was sig-nificantly weaker (P .05) than the non-throwing shoulder by 6%. Conversely, IRof the throwing shoulder was significantly
The total-rotational-motion concept.External rotation (ER) + internal rotation (IR) = totalmotion. Total rotational motion is equal bilaterally.
Glenohumeral laxity testing done on Telosdevice to objectively assess the amount of joint laxity.
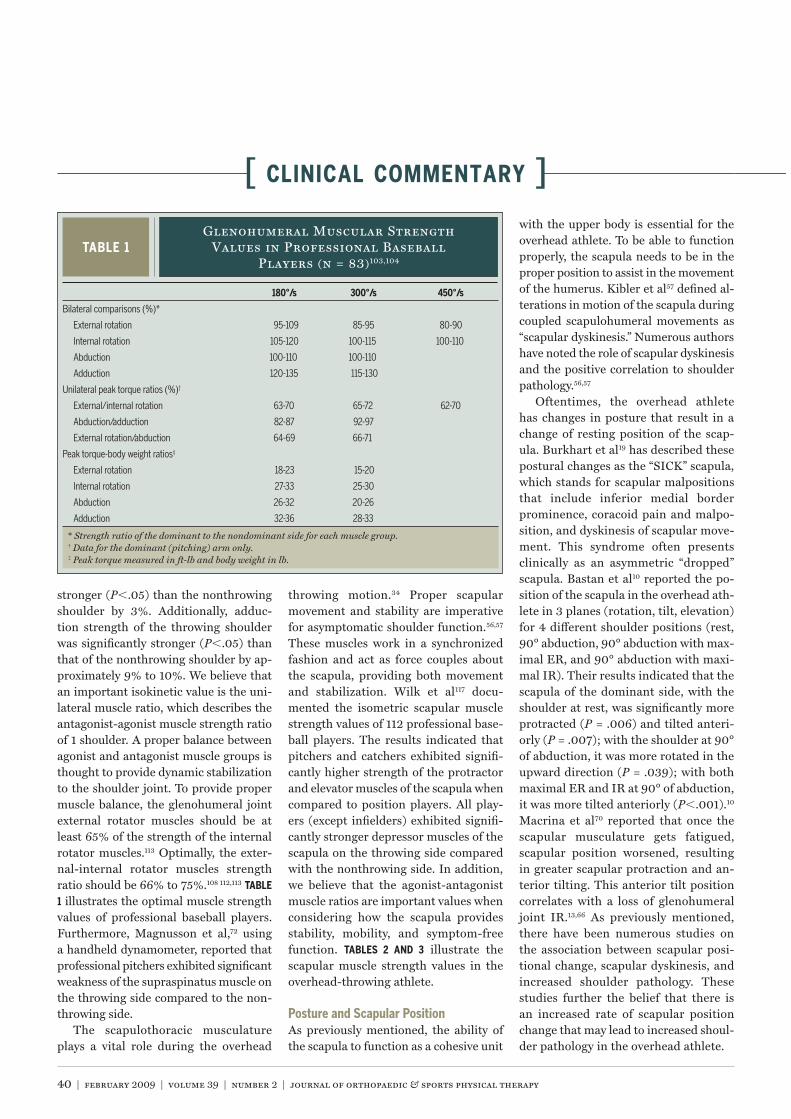
40 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
stronger (P .05) than the nonthrowingshoulder by 3%. Additionally, adduc-tion strength of the throwing shoulderwas significantly stronger (P .05) thanthat of the nonthrowing shoulder by ap-proximately 9% to 10%. We believe thatan important isokinetic value is the uni-lateral muscle ratio, which describes theantagonist-agonist muscle strength ratioof 1 shoulder. A proper balance betweenagonist and antagonist muscle groups isthought to provide dynamic stabilizationto the shoulder joint. To provide propermuscle balance, the glenohumeral jointexternal rotator muscles should be atleast 65% of the strength of the internalrotator muscles.113 Optimally, the exter-nal-internal rotator muscles strengthratio should be 66% to 75%.108 112,113
1 illustrates the optimal muscle strengthvalues of professional baseball players.Furthermore, Magnusson et al,72 usinga handheld dynamometer, reported thatprofessional pitchers exhibited significantweakness of the supraspinatus muscle onthe throwing side compared to the non-throwing side.
The scapulothoracic musculatureplays a vital role during the overhead
throwing motion.34 Proper scapularmovement and stability are imperativefor asymptomatic shoulder function.56,57
These muscles work in a synchronizedfashion and act as force couples aboutthe scapula, providing both movementand stabilization. Wilk et al117 docu-mented the isometric scapular musclestrength values of 112 professional base-ball players. The results indicated thatpitchers and catchers exhibited signifi-cantly higher strength of the protractorand elevator muscles of the scapula whencompared to position players. All play-ers (except infielders) exhibited signifi-cantly stronger depressor muscles of thescapula on the throwing side comparedwith the nonthrowing side. In addition,we believe that the agonist-antagonistmuscle ratios are important values whenconsidering how the scapula providesstability, mobility, and symptom-freefunction. illustrate thescapular muscle strength values in theoverhead-throwing athlete.
As previously mentioned, the ability ofthe scapula to function as a cohesive unit
with the upper body is essential for theoverhead athlete. To be able to functionproperly, the scapula needs to be in theproper position to assist in the movementof the humerus. Kibler et al57 defined al-terations in motion of the scapula duringcoupled scapulohumeral movements as“scapular dyskinesis.” Numerous authorshave noted the role of scapular dyskinesisand the positive correlation to shoulderpathology.56,57
Oftentimes, the overhead athletehas changes in posture that result in achange of resting position of the scap-ula. Burkhart et al19 has described thesepostural changes as the “SICK” scapula,which stands for scapular malpositionsthat include inferior medial borderprominence, coracoid pain and malpo-sition, and dyskinesis of scapular move-ment. This syndrome often presentsclinically as an asymmetric “dropped”scapula. Bastan et al10 reported the po-sition of the scapula in the overhead ath-lete in 3 planes (rotation, tilt, elevation)for 4 different shoulder positions (rest,90° abduction, 90° abduction with max-imal ER, and 90° abduction with maxi-mal IR). Their results indicated that thescapula of the dominant side, with theshoulder at rest, was significantly moreprotracted (P = .006) and tilted anteri-orly (P = .007); with the shoulder at 90°of abduction, it was more rotated in theupward direction (P = .039); with bothmaximal ER and IR at 90° of abduction,it was more tilted anteriorly (P .001).10
Macrina et al70 reported that once thescapular musculature gets fatigued,scapular position worsened, resultingin greater scapular protraction and an-terior tilting. This anterior tilt positioncorrelates with a loss of glenohumeraljoint IR.13,66 As previously mentioned,there have been numerous studies onthe association between scapular posi-tional change, scapular dyskinesis, andincreased shoulder pathology. Thesestudies further the belief that there isan increased rate of scapular positionchange that may lead to increased shoul-der pathology in the overhead athlete.
Glenohumeral Muscular StrengthValues in Professional Baseball
Players (n = 83)103,104
* Strength ratio of the dominant to the nondominant side for each muscle group.† Data for the dominant (pitching) arm only.‡ Peak torque measured in ft-lb and body weight in lb.
Bilateral comparisons (%)*
External rotation 95-109 85-95 80-90
Internal rotation 105-120 100-115 100-110
Abduction 100-110 100-110
Adduction 120-135 115-130
Unilateral peak torque ratios (%)†
External/internal rotation 63-70 65-72 62-70
Abduction/adduction 82-87 92-97
External rotation/abduction 64-69 66-71
Peak torque-body weight ratios‡
External rotation 18-23 15-20
Internal rotation 27-33 25-30
Abduction 26-32 20-26
Adduction 32-36 28-33
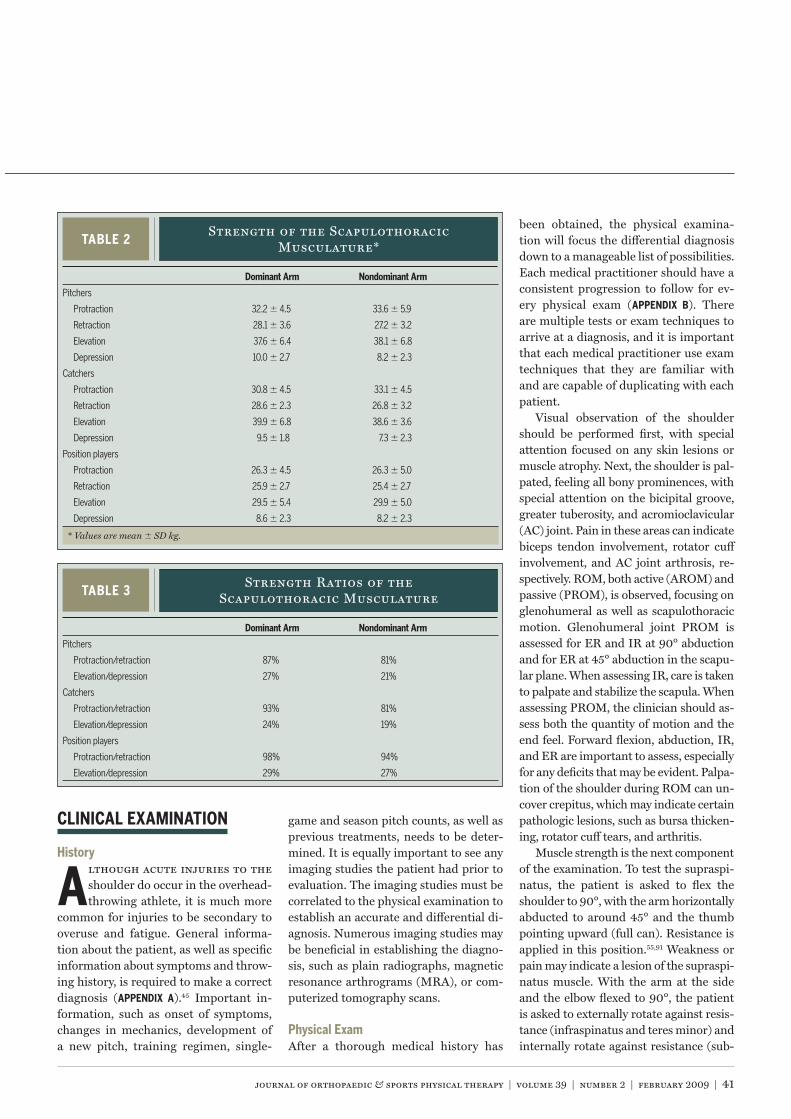
journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 41
game and season pitch counts, as well asprevious treatments, needs to be deter-mined. It is equally important to see anyimaging studies the patient had prior toevaluation. The imaging studies must becorrelated to the physical examination toestablish an accurate and differential di-agnosis. Numerous imaging studies maybe beneficial in establishing the diagno-sis, such as plain radiographs, magneticresonance arthrograms (MRA), or com-puterized tomography scans.
After a thorough medical history has
been obtained, the physical examina-tion will focus the differential diagnosisdown to a manageable list of possibilities.Each medical practitioner should have aconsistent progression to follow for ev-ery physical exam ( ). Thereare multiple tests or exam techniques toarrive at a diagnosis, and it is importantthat each medical practitioner use examtechniques that they are familiar withand are capable of duplicating with eachpatient.
Visual observation of the shouldershould be performed first, with specialattention focused on any skin lesions ormuscle atrophy. Next, the shoulder is pal-pated, feeling all bony prominences, withspecial attention on the bicipital groove,greater tuberosity, and acromioclavicular(AC) joint. Pain in these areas can indicatebiceps tendon involvement, rotator cuffinvolvement, and AC joint arthrosis, re-spectively. ROM, both active (AROM) andpassive (PROM), is observed, focusing onglenohumeral as well as scapulothoracicmotion. Glenohumeral joint PROM isassessed for ER and IR at 90° abductionand for ER at 45° abduction in the scapu-lar plane. When assessing IR, care is takento palpate and stabilize the scapula. Whenassessing PROM, the clinician should as-sess both the quantity of motion and theend feel. Forward flexion, abduction, IR,and ER are important to assess, especiallyfor any deficits that may be evident. Palpa-tion of the shoulder during ROM can un-cover crepitus, which may indicate certainpathologic lesions, such as bursa thicken-ing, rotator cuff tears, and arthritis.
Muscle strength is the next componentof the examination. To test the supraspi-natus, the patient is asked to flex theshoulder to 90°, with the arm horizontallyabducted to around 45° and the thumbpointing upward (full can). Resistance isapplied in this position.55,91 Weakness orpain may indicate a lesion of the supraspi-natus muscle. With the arm at the sideand the elbow flexed to 90°, the patientis asked to externally rotate against resis-tance (infraspinatus and teres minor) andinternally rotate against resistance (sub-
lthough acute injuries to theshoulder do occur in the overhead-throwing athlete, it is much more
common for injuries to be secondary tooveruse and fatigue. General informa-tion about the patient, as well as specificinformation about symptoms and throw-ing history, is required to make a correctdiagnosis ( ).45 Important in-formation, such as onset of symptoms,changes in mechanics, development ofa new pitch, training regimen, single-
Strength of the ScapulothoracicMusculature*
* Values are mean SD kg.
Pitchers
Protraction 32.2 4.5 33.6 5.9
Retraction 28.1 3.6 27.2 3.2
Elevation 37.6 6.4 38.1 6.8
Depression 10.0 2.7 8.2 2.3
Catchers
Protraction 30.8 4.5 33.1 4.5
Retraction 28.6 2.3 26.8 3.2
Elevation 39.9 6.8 38.6 3.6
Depression 9.5 1.8 7.3 2.3
Position players
Protraction 26.3 4.5 26.3 5.0
Retraction 25.9 2.7 25.4 2.7
Elevation 29.5 5.4 29.9 5.0
Depression 8.6 2.3 8.2 2.3
Strength Ratios of theScapulothoracic Musculature
Pitchers
Protraction/retraction 87% 81%
Elevation/depression 27% 21%
Catchers
Protraction/retraction 93% 81%
Elevation/depression 24% 19%
Position players
Protraction/retraction 98% 94%
Elevation/depression 29% 27%

42 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
scapularis). Again, weakness or pain mayindicate a lesion. Resisted ER and IR aresubsequently performed at 90° of abduc-tion and neutral rotation, which is a morefunctional position to assess the overheadathlete. It may be beneficial to assess ERand IR strength at 90° of abduction, withthe patients moving through an arc ofmotion concentrically and eccentricallyagainst resistance.
At this point, the examiner can per-form certain provocative maneuversto assess other possible pathology ( -
). A few selected common testsperformed in the clinic will be discussedbelow in more detail.
To assess subacromial impingement,the Hawkins-Kennedy test is often uti-lized. This subacromial impingementtest has been reported to have 66% to100% sensitivity and 25% to 66% speci-ficity for the diagnosis of impingement,rotator cuff tears, and bursitis.21,69,87 Thepatient’s shoulder joint is forward flexedto 90° and the shoulder is forcibly in-ternally rotated. This maneuver drivesthe greater tuberosity farther under thecoracoacromial ligament, producing im-pingement. Pain with this maneuver mayindicate subacromial impingement.98 Thetest is performed at 90° of abduction inthe scapular plane, sagittal plane, andwith horizontal adduction beyond thesagittal plane, with the more horizon-
tally adducted positions causing greaterimpingement and, therefore, being pos-sibly more provocative for pain.
There are a variety of tests describedto assess for a possible superior labrumanterior posterior (SLAP) tear.33 O’Brien’sactive compression test is frequentlyused.83 The examiner asks the patient toforward flex the affected arm 90°, withthe elbow in full extension. The patientthen adducts the arm 10° to 15° medially.The arm is internally rotated so that thethumb is pointing downward. The exam-iner then applies a uniform downwardforce to the arm. The exact same tech-nique is performed again, this time withthe patient placing the palm up towardthe ceiling. The test is considered positiveif pain (located within the subacromial orsuperior glenohumeral joint) is elicitedwith the first maneuver and is reducedor eliminated with the second maneu-ver.99 O’Brien et al83 have reported 100%sensitivity and 97% to 99% specificity forthis test in detecting glenoid labral or ACjoint abnormality. The tests we performto test the integrity of the glenoid labrumare the biceps load test, pronated bicepsload test,116 and resisted ER with supina-tion test.80 These tests, illustrated in -
( ), have beenshown to be highly sensitive for SLAPtears/lesions in the overhead athlete.80
There exist numerous joint stabilitytests. For a complete and thorough de-
scription of these tests the reader is en-couraged to review Wilk et al.113,116 Thosewe routinely perform are the anteriordrawer, fulcrum, relocation, and internalimpingement signs and tests. The mostimportant aspects of these tests are todetermine the extent of laxity present,end point, and, in particular, the tissueelasticity at end range. To assess endpoint elasticity, the fulcrum test is per-formed at 90° of abduction. The posteri-or impingement sign is performed in theplane of the scapula at 90° of abduction,with the examiner passively rotating thearm into maximum ER ( ). Apositive test is indicated by complaintsof pain in the deep posterior shoulder.Meister et al76 have reported 76% sensi-tivity and 85% specificity when perform-ing this test for posterior rotator cuffand/or labrum tears.
Imaging is the next important step in de-termining a diagnosis. Plain radiographswith multiple views of the involved gle-nohumeral joint are mandatory. Routineradiographic evaluation includes ante-rior-posterior (AP), Stryker notch, WestPoint, axillary, and acromial outlet views.These views allow visualization of the gle-nohumeral articulation as well as acromi-al morphology and the inferior glenoid.
Biceps load test performed to assessfor possible SLAP lesion. The patient abducts theshoulder to 90°, fully externally rotates the shoulder,flexes the elbow to 90°, and fully supinates theforearm. The patient is asked to actively flex theelbow against resistance. Pain is positive indicationfor a SLAP lesion.
Pronated biceps load test to assess forpossible SLAP lesion. The patient assumes the sameposition as the biceps load test but fully pronatesthe forearm. The patient is again asked to activelyflex the elbow against resistance. Pain located in thesuperior glenohumeral joint (deep) is indicative of aSLAP lesion.
Resisted external rotation with supinationperformed to assess integrity of the superior labrum.The patient is asked to abduct the arm to 90°,and flex the elbow to 90°, keeping the shoulder inneutral rotation. The examiner resists the patient,while active external rotation of the arm and forearmsupination is performed. Pain is considered a positivesign for a SLAP lesion.

journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 43
The imaging modality of choice to as-sess soft tissue pathology of the shoulderis magnetic resonance imaging (MRI)with intra-articular contrast (MRA). Thisallows the best view of the rotator cufftendons and muscles, glenoid labrum,biceps tendon, and other associated pa-thology, such as spinoglenoid cysts. Intra-articular contrast is especially useful todetermine if there is a full-thickness ver-sus partial-thickness tear of the rotatorcuff. Furthermore, the MRA techniqueallows the physician to evaluate the gle-noid labrum to determine if a detachedlabrum or frayed labrum exists. In thethrowing athlete the most common le-sions are partial-thickness rotator cufftears and glenoid labrum pathology.
There are numerous lesions thatmay occur in the overhead athlete( ).
Tendonitis, tendonosis, and bursitis are3 separate clinical entities for which thenames are often incorrectly used inter-changeably. Tendonitis is inflammationof the tendon. In many cases, it is actuallythe tendon sheath that is inflamed andnot the tendon itself. Bursitis is inflam-mation of the subacromial bursa. Ten-donosis implies intratendonous disease,such as intrasubstance degeneration ortearing.
The patient clinical presentation oftendonitis or tendonosis of the rotatorcuff are pain with overhead activity andweakness secondary to pain. The symp-toms in the thrower are pain during thelate cocking phase of throwing, when thearm is in maximal ER, or pain after ballrelease, as the muscles of the rotator cuffslow the arm during the decelerationphase.37 Weakness of the supraspinatusand infraspinatus are common findingsin throwers with shoulder pathology;but asymmetric muscle weakness in thedominant shoulder is often seen in the
healthy thrower. Differential diagnosisof tendonitis versus tendonosis is basedon MRI and duration and frequency ofsymptoms. On MRI, the patient withtendonitis will exhibit inflammation ofthe tendon sheath (the paratenon); con-versely, when tendonosis is present, thereexists intrasubstance wear (signal) of thetendon.
Tendonitis/tendonosis is most fre-quently an overuse injury in the overheadathlete and does not usually represent anacute injury process. The symptoms fre-quently occur early in the season, whenthe athlete’s arm is not conditioned prop-erly.114 These injuries may also occur at theend of the season, as the athlete begins tofatigue. If the athlete does not participatein an in-season strengthening program tocontinue proper muscular conditioning,tendonitis/tendonosis may also develop.Specific muscles (external rotator mus-cles and scapular muscles) may becomeweak and painful due to the stresses ofthrowing.114
Muscles of the rotator cuff are activeduring various phases of the throwingmotion.35,42,50 During the late cockingand early acceleration phases, the arm ismaximally externally rotated, potentiallyplacing the rotator cuff in position toimpinge between the humeral head andthe posterior-superior glenoid. Knownas “internal impingement” or “posteriorimpingement,” this may place the rota-tor cuff at risk for undersurface tearing(articular sided). Conversely, in the de-celeration phase of throwing, the rotatorcuff experiences extreme tensile loadsduring its eccentric action, which maylead to injury.36 Rotator cuff tears in theoverhead athlete may be of partial or fullthickness. The history of shoulder paineither at the top of the wind-up (accel-eration) or during the deceleration phaseof throwing should alert the examinerto a rotator cuff source of pain or loss offunction. Any history of trauma, changesin mechanics, loss of playing time, previ-ous treatments, voluntary time off from
throwing, and history of previous injuryshould be noted.
Rotator cuff tears may be caused byprimary tensile cuff disease (PTCD), pri-mary compressive cuff disease (PCCD),or internal impingement. PTCD resultsfrom the large, repetitive loads placed onthe rotator cuff as it acts to decelerate theshoulder during the deceleration phase ofthrowing in the stable shoulder. The in-jury is seen as a partial undersurface tearof the supraspinatus or infraspinatus.2,7
PCCD is found on the bursal surface ofthe rotator cuff in throwers with stableshoulders. This process occurs secondaryto the inability of the rotator cuff to pro-duce sufficient adduction torque and in-ferior force during the deceleration phaseof throwing. Processes that decrease thesubacromial space increase the risk forthis type of pathology.2 Partial-thicknessrotator cuff tears can also occur from in-ternal impingement.
Internal impingement was first describedin 1992 by Walch and associates in tennisplayers.104 They presented arthroscopicclinical evidence that partial, articular-sided rotator cuff tears were a direct con-sequence of what they termed “internalimpingement.” Internal impingement ischaracterized by contact of the articularsurface of the rotator cuff and the greatertuberosity with the posterior and superi-or glenoid rim and labrum in extremes ofcombined shoulder abduction and ER.49
In overhead throwing athletes, it ap-pears that excessive anterior translationof the humeral head, coupled with exces-sive glenohumeral joint ER, predisposesthe rotator cuff to impingement againstthe glenoid labrum.63 Repeated internalimpingement may be a cause of under-surface rotator cuff tearing and posteriorlabral tears. It is important that the un-derlying laxity of the glenohumeral jointbe addressed at the time of treatment foran internal impingement lesion to pre-vent recurrence of the lesion.7 Burkhartet al20 have proposed that restrictedposterior capsular mobility may result

44 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]in IR deficits and may cause pathologicincreases in internal rotator cuff contactand injury. The authors of this manu-script believe that the loss of IR is mostoften due to osseous adaptation29,89 andmuscular tightness, as opposed to capsu-lar tightness.
Patients with internal impingementusually describe an insidious onset of painin the shoulder.5 Pain tends to increaseas the season progresses. Symptoms mayhave been present over the past couple ofseasons, worsening in intensity with eachsuccessive year. Pain is usually dull andaching, and is located over the posterioraspect of the shoulder. Late cocking phaseseems to be most painful. Loss of controland velocity is often present secondary tothe inability to fully externally rotate thearm without pain.
On physical examination, pain maybe elicited over the infraspinatus muscleand tendon with palpation. Pain to palpa-tion is more often posterior, in contrastto rotator cuff tendonitis, which usuallyelicits pain to palpation over the greatertuberosity.5 With internal impingement,patients usually have full ROM. In boththe normal and pathologic thrower’sshoulder the dominant arm tends to have10° to 15° more ER and 10° to 15° less IRwith the arm abducted to 90°, comparedwith the nondominant arm.29 The mostcommon presentation is for the overheadathlete to have 1+ to 2+ anterior laxity and2+ posterior laxity. Inferior laxity is oftenpresent. Most provocative tests are nega-tive. The most frequent provocative examto elicit pain is the internal impingementsign,76 described earlier.
SLAP lesions are a complex of injuries tothe superior labrum and biceps anchor atthe glenoid attachment. Andrews and as-sociates4 were the first to describe this le-sion in 1985. They reported arthroscopicfindings in a group of throwing athleteswith shoulder dysfunction. Snyder andassociates94 later classified this injurycomplex as superior labrum anteriorand posterior lesions, and coined the
term SLAP lesion. The arthroscopic ap-pearances of the lesions were originallyclassified into 4 distinct lesion types,with 3 variations later being added.71 Thepathophysiology of SLAP lesions is de-bated frequently, but the essentials of thelesion are agreed upon.
Patients who have SLAP lesions fallinto 2 basic categories. The first consistsof overhead athletes, most commonlybaseball players, with a history of repeti-tive overhead activity and no history oftrauma. The second category involves pa-tients with a history of trauma.49
Burkhart et al20 have described thepeel-back lesion of the superior labrum,which frequently occurs in the overheadathlete ( ). Peel-back lesions areconsidered a type II SLAP lesion. Theathlete often presents to the practitio-ner with complaints of vague onset ofshoulder pain and possibly problemswith velocity, control, or other throwingcomplaints. The patient may complainof mechanical symptoms or pain in thelate cocking phase, often poorly localized.The diagnosis of SLAP lesions can be verydifficult, as symptoms can mimic rotatorcuff pathology and glenohumeral jointinstability. Definitive diagnosis can onlybe made by arthroscopy.49
Thrower’s exostosis is an extracapsularossification of the posteroinferior gle-noid rarely seen except in older longtimethrowers.75 This condition is a result ofsecondary ossification involving the pos-terior capsule, probably due to repeti-tive trauma.6 The osteophyte is thoughtto originate in the glenoid attachmentof the posterior band of the inferior gle-nohumeral ligament, possibly from trac-tion during deceleration. Patients oftenhave a tight posterior capsule, with cap-sular contracture and asymmetric shoul-der motion with an IR deficit.
This lesion can often mimic internalimpingement. Pain is often found inthe posterior part of the shoulder and isworse in late cocking. Patients often de-
scribe a pinching sensation during throw-ing. Pain usually is relieved by rest. Plainradiographs will assist in differentiatingthis lesion from internal impingement.
ubacromial impingement pa-thologies can frequently be treatednonoperatively with or without a
subacromial (extra-articular) injection,often consisting of a mixture of local an-esthetic and a corticosteroid. The anes-thetic and steroid are used to relieve painand inflammation, allowing the patient tomore effectively perform a therapy pro-gram. After the injection is performed,a period of rest and rehabilitation isused. It is common for the patient tobe re-evaluated after 2 to 3 weeks. If noimprovement is seen, a second injectionmay be indicated. If the patient fails thisnonoperative course, shoulder arthros-copy with rotator cuff debridement maybe indicated. At the time of surgery, theshoulder can be assessed for other lesionsand any identified pathology addressed.Often, instability and hyperlaxity are un-derlying causes for rotator cuff lesions.
Surgical intervention is only consideredwith a full-thickness rotator cuff tear orwith partial-thickness tears, after thepatient has failed at least 1, but usually2, courses of rehabilitation, followed byan interval throwing program. Prior tophysical therapy for partial-thickness ro-
Arthroscopic view of peel-back lesion ofthe superior labrum.

journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 45
tator cuff tears, either a subacromial cor-ticosteroid injection or a glenohumeralinjection is frequently performed. If thepatient fails this course of treatment, ar-throscopy is indicated.
The first step in the operative interven-tion is an examination under anesthesia.After the examination under anesthesiahas been performed, diagnostic arthros-copy of the shoulder begins by establish-ing a posterior viewing portal to visualizethe glenohumeral joint. Care is taken tolook at the labrum, with special attentionto the superior labrum, biceps anchor,and articular surface of the rotator cuff.The glenoid and humeral articular sur-faces are also visualized for lesions. Otherstructures visualized include the bicepstendon, superior border of the subscapu-laris tendon, the middle glenohumeralligament, rotator interval, and axillarypouch. An anterior working portal isthen created through the rotator interval.A probe is brought into the joint to as-sess integrity of the superior labrum andbiceps anchor, the rotator cuff, and anyother structures in question. The arthro-scope is then placed in the anterior portalto visualize the posterior structures.
Once any intra-articular pathologyhas been identified, a full-radius shaveris brought in through the anterior portal.Any fraying of the labrum or undersurfaceof the rotator cuff can be debrided backto a stable base. Undersurface rotator cufftears are evaluated for the percent thick-ness of the tendon that is torn. The nor-mal rotator cuff attaches to the articularmargin of the humerus, and the footprintspans approximately 14 mm from medialto lateral. Partial articular-sided tears canbe measured from the articular margin toassess the percentage of injury (7 mm ex-posed surface from the articular margin,50% tear). Tears of less than 50% thick-ness are debrided, while tears of greaterthan 50% thickness may also be debridedor repaired to the footprint.37 Significantpartial-thickness tears or full-thicknesstears may be repaired arthroscopically orthrough a standard mini-open technique.Arthroscopic repair involves placing the
arthroscope into the subacromial space(in most cases), performing a subacro-mial decompression, and repairing theinvolved rotator cuff tendon or tendonswith side-to-side repair or suture an-chors. More recently, double-row rota-tor cuff repairs have become increasinglypopular. The postoperative outcomes ofrotator cuff repairs in the overhead ath-lete have been reported to be less thanoptimal, with approximately less than15% of athletes returning to play.73
As mentioned earlier, internal impinge-ment is a common pathology seen in theoverhead athlete. The best treatment forthis lesion is a thorough and well-devel-oped nonoperative treatment program.If nonoperative measures fail, surgeryis indicated. As with other shoulder in-juries, an examination under anesthesia,followed by diagnostic arthroscopy, isperformed. Simple arthroscopic debri-dement of rotator cuff tears and labralfraying was originally described to treatinternal impingement.3 Results weremixed with simple debridement, andit became evident that some sort of an-terior stabilization was also required tohelp stabilize the shoulder. Therefore, inconjunction with debridement of the ro-tator cuff or labral lesions, capsulolabralreconstruction51 or thermal capsulo-raphy63 has been recommended. Gener-ally, subacromial decompression does nothave a role in the treatment of internalimpingement.
Once the diagnosis has been established,treatment options are considered. Thenonsurgical treatment of SLAP lesionsdepends upon the type of lesion. Most le-sions in the overhead athlete are type IIand may not respond well to nonsurgicalmanagement.
When pain and dysfunction persistafter a period of rest and rehabilitation,surgical intervention is indicated. As withother shoulder injuries, a physical exami-nation under anesthesia is done, followed
by diagnostic arthroscopy. All of the in-tra-articular structures are visualized andevaluated. Close attention to the superiorlabrum and biceps anchor is warranted.
If a true superior labral detachmentis noted, arthroscopic repair is the pro-cedure of choice. SLAP lesions occurringin the overhead athlete are almost alwaystype II.49 These tears must be repaired.Initially, the lesion must be identified andthe surgeon determines if there is a pri-marily posterior or anterior component.The location of the predominant patholo-gy dictates arthroscopic portal placementand repair techniques. Prior to repair ofthe lesion, a shaver must be used to deb-ride the glenoid neck and prepare a bonybed to which the labrum is reattached.Lesions with anterior extension may ormay not need an additional accessorylateral portal. Suture anchors are placedalong the glenoid rim, and the labrumand biceps complex are secured back tothe glenoid with arthroscopic knots. If thelesion is predominantly located posteriorto the biceps anchor, an accessory poste-rior portal will likely need to be created.Subacromial decompression is generallynot indicated after SLAP repair.
Treatment of athletes with this lesion iscontroversial. The senior author (J.R.A.)believes that the presence of posteriorglenoid exostosis is highly predictive ofan undersurface rotator cuff tear causedby internal impingement and injury tothe posterior labrum.6 Initially, thesepatients are treated with a period of ac-tive rest and supervised rehabilitation.Throwers with posterior glenoid exos-tosis can be conservatively managed forsome time; however, long-term successis limited and surgical intervention maybecome necessary.114
As with other shoulder lesions, whennonsurgical measures fail to relievesymptoms, operative intervention is un-dertaken. Initially, examination underanesthesia is performed, followed by di-agnostic arthroscopy. Any concurrent in-

46 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]tra-articular pathology is addressed at thetime of arthroscopy. A 70° arthroscope isplaced in the anterior portal to improvevisualization over the posterior glenoidrim. The posterior glenoid exostosis isuncovered through a small capsulotomyat the medial edge of the posteroinferiorcapsule by penetrating the capsule witha shaver just off the posterior labral at-tachment. A small round burr is thenemployed to debride the exostosis back tothe normal contour of the posterior gle-noid rim.7 Underlying glenohumeral jointinstability is also addressed during thesurgical procedure. The posterior capsuleis generally not repaired, resulting in aneffective posterior capsular release.
ost shoulder injuries in theoverhead thrower can be success-fully treated nonoperatively. The
rehabilitation program involves a multi-phased approach that is progressive andsequential, and is based on the physicalexamination, the specifically involvedstructures, and the primary cause. Thekey to successful rehabilitation is theidentification of the underlying factorsand structures causing the lesion. Thespecific goals of each of the 4 phases ofthe program are outlined in .Each phase represents a progression, theexercises becoming more aggressive anddemanding, and the stresses applied tothe shoulder joint gradually greater.
One of the goals, to diminish the athlete’spain and inflammation, is accomplishedthrough the use of local therapeuticmodalities such as ice, iontophoresis,nonsteroidal anti-inflammatory drugs(NSAIDs), and/or injections. We preferthe use of iontophoresis for soft tissueinflammation about the shoulder. In ad-dition, the athlete’s activities (such asthrowing and exercises) must be modi-fied to a pain-free level. The thrower isoften instructed to abstain from throwing
until advised by the physician or rehabili-tation specialist. Additionally, stretchingexercises have been shown to assist in re-ducing the athlete’s pain.81
Another essential goal during the firstphase of rehabilitation is to normalizeshoulder motion, particularly shoulder IRand horizontal adduction. It is commonfor the overhead thrower to exhibit loss ofIR of 20° or more, referred to as “GIRD.”This loss of IR has been suggested to be acause of specific shoulder injuries.19
We believe that the loss of IR is mostoften due to osseous adaptations of thehumerus and posterior muscle tight-ness.15 We do not believe that the loss ofIR is routinely due to posterior capsulartightness. It appears that most throwersexhibit significant posterior laxity whenevaluated.15 Thus, to improve IR motionand flexibility, we prefer the stretches il-lustrated in . These stretch-es include the sleeper’s stretch (
) and supine horizontal adductionwith IR. These stretches are performedto improve the flexibility of the poste-rior musculature, which may becometight because of the muscle contractionduring the deceleration phase of throw-ing. We do not recommend performingstretches for the posterior capsule unlessthe capsule has been shown on clinicalexamination to be excessively hypomo-bile. If the posterior glenohumeral jointcapsule is hypomobile, then a posterior-lateral joint mobilization glide techniqueis performed to effectively mobilize theposterior capsule.
The rehabilitation specialist, in ad-dition to helping restore glenohumeralmotion, should assess the resting positionand mobility of the scapula. Frequently,we see overhead throwers who exhibit aposture of rounded shoulders and a for-ward head. This posture appears associat-ed with muscle weakness of the scapularretractor muscles due to prolonged elon-gation or sustained stretches. In addition,the scapula may often appear protractedand anteriorly tilted. An anteriorly tiltedscapula has been shown to contribute toa loss of glenohumeral joint IR.13,70 Inoverhead throwers, it is our experiencethat this scapular position abnormalityis associated with pectoralis minor mus-cle tightness and lower trapezius muscleweakness, and a forward head posture.Tightness of the pectoralis minor muscle
Sleeper stretch performed to increaseinternal rotation. The patient is asked to lay on theinvolved side with arm flexed to 90°. The patientgrabs the wrist/forearm of the involved extremity andpushes the extremity into internal rotation. Care isgiven to assume the proper position to lock down thescapula. (B) Sleeper stretch with lift. The examinerlifts the patient’s scapula and repositions it laterally,stabilization of the scapula may be necessary.
Horizontal adduction with internal rotationstretch. The patient flexes the arm to 90°. Therehabilitation specialist applies a stabilizing forceto the lateral border of the scapula while the arm ishorizontally adducted and then applies a gentle forceinto internal rotation.

journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 47
can lead to axillary artery occlusion andneurovascular symptoms, such as armfatigue, pain, tenderness, and cyano-sis.8,82,93,95 The lower trapezius muscle isan important muscle in arm decelerationin that it controls scapular elevation andprotraction.34 Weakness of the lower tra-pezius muscle may result in improper me-chanics or shoulder symptoms. Thus, therehabilitation specialist should carefullyassess the position, mobility, and strengthof the overhead thrower’s scapula. Weroutinely have throwers stretch theirpectoralis minor muscle and strengthenthe lower trapezius muscle in addition tothe scapular retractors. Furthermore, ascapular brace may be utilized to assistin postural correction.
Additional primary goals of this firstphase are to restore muscle strength,re-establish baseline dynamic stability,and restore proprioception. In the earlyphase of rehabilitation, the goal is to re-establish muscle balance.112,113 Therefore,the focus is on improving the strength ofthe weak muscles such as the external ro-tator muscles, the scapular muscles, andthose of the lumbopelvic region and low-er extremities.112,113 If the injured athleteis extremely sore or in pain, submaximalisometric exercises should be employed;conversely, if the athlete exhibits minimalsoreness, then lightweight isotonic exer-cises may be safely initiated. Additionally,during this phase, we use rehabilitationexercise drills designed to restore theneurosensory properties of the shouldercapsule that has experienced microtrau-ma and to enhance the sensitivity of theafferent mechanoreceptors.60,62
Specific drills that restore neuromus-cular control during this initial phaseare rhythmic stabilization exercises forthe internal/external rotator muscles ofthe shoulders. Additionally, propriocep-tive neuromuscular facilitation patternsare used with rhythmic stabilizationand slow reversal hold to re-establishproprioception and dynamic stabiliza-tion.58,60,62,96,111,112 The purpose of these ex-ercises is to facilitate agonist/antagonistmuscle coactivation. Efficient coactiva-
tion assists in restoring the balance in theforce couples of the shoulder joint, thusenhancing joint congruency and com-pression.46 Padua et al84 used propriocep-tive neuromuscular facilitation patternsfor 5 weeks and significantly improvedtheir subjects’ shoulder function and en-hanced functional throwing performancetest scores. Uhl et al101 reported improvedproprioception after specific neuromus-cular training that challenged the gle-nohumeral musculature.
Other exercises commonly used dur-ing this first rehabilitation phase in-clude joint repositioning tasks60-62 andaxial loading exercises (upper extremityweight-bearing exercises). Active jointcompression stimulates the articular re-ceptors.26,59 Thus, axial loading exercises,such as weight shifts, weight shifting ona ball, wall push-ups, and quadruped po-sitioning drills, are beneficial in restoringproprioception.106,112,109
In phase 2 of the rehabilitation pro-gram, the primary goals are to progressthe strengthening program, continue toimprove flexibility, and facilitate neu-romuscular control. During this phase,the rehabilitation program is progressedto more aggressive isotonic strengthen-ing activities, with emphasis on restora-tion of muscle balance. Selective muscleactivation is also used to restore musclebalance and symmetry. In the overheadthrower, the shoulder external rotatormuscles and scapular retractor, protrac-tor and depressor muscles are frequentlyisolated because of weakness. We have es-tablished a fundamental exercise programfor the overhead thrower that specificallyaddresses the vital muscles involved inthe throwing motion.106,118 This exerciseprogram was developed based on thecollective12,31,47,53,64,74,78,86,91,100 informationderived from electromyographic researchof numerous investigators and is referredto as the “Thrower’s Ten” program.115 Fre-quently, the patient exhibits ER muscularweakness. The specific exercises we preferare side-lying ER ( ) and prone
rowing into ER. Both have been shown toelicit the highest amount of muscular ac-tivity of the posterior cuff muscles.91
The scapula provides proximal stabil-ity to the shoulder joint, enabling distalsegment mobility. Scapular stability isvital for normal asymptomatic arm func-tion. Several authors have emphasized theimportance of scapular muscle strengthand neuromuscular control in contribut-ing to normal shoulder function.31,56,57,85
Isotonic exercises are used to strengthenthe scapular muscles. Furthermore, Wilket al111 developed specific exercise drillsto enhance neuromuscular control of thescapulothoracic joint. These exercise drillsare designed to maximally challenge thescapulothoracic muscle force couples andto stimulate the proprioceptive and kin-esthetic awareness of the scapula. Thesescapular neuromuscular control drills areillustrated in ( ).
Another popular exercise used by ath-letes is the “empty can” exercise. With thisexercise movement, the arm is placed inthe scapular plane with the hand placedin full IR (thumb down). Originally Jobeand Moynes52 reported high levels ofactivation of the supraspinatus musclesduring this exercise. Recently, Reinoldet al90,91 reported that the best exercisefor supraspinatus muscle was insteadthe “full can” exercise. Blackburn et al12
noted that the position with the patientlying prone and with the arm abductedto 100° and full ER produced the highest
Scapular neuromuscular control drills. Theathlete lies on his side with the hand placed on thetable and the clinician applies manual resistance toresist scapular movements (such as protraction andretraction). The athlete is instructed to perform slowand controlled movements.

48 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
EMG signal in the supraspinatus musclescompared to the empty can position.
Also during this second rehabilitationphase, the overhead throwing athleteis instructed to perform strengtheningexercises for the lumbopelvic region,including the abdomen and lower backmusculature. Plus, the athlete shouldperform lower extremity strengtheningand participate in a running program,including jogging and sprinting. Upperextremity stretching exercises are con-tinued as needed to maintain soft tissueflexibility.
In phase 3, the advanced strengtheningphase, the goals are to initiate aggressivestrengthening drills, enhance power andendurance, perform functional drills,and gradually initiate throwing activities.During this phase, the athlete performsthe Thrower’s Ten exercise program,continues manual resistance stabiliza-
tion drills, and initiates plyometric drills.Dynamic stabilization drills are alsoperformed to enhance proprioceptionand neuromuscular control. These drillsinclude specific stabilization techniquesthat employ the concept of perturbationsand range stability. These drills includerhythmic stabilization exercise drills bythrowing a ball against the wall (10), push-ups onto a ball, and tubing ERwith end range manual resistance (
). Many of the stabilizationexercises may be performed on a physiob-all. The authors believe that performingthese exercises improves dynamic stabili-zation and increases muscular demands( ). Plyometric trainingmay be used to enhance dynamic stabili-ty, enhance proprioception, and graduallyincrease the functional stresses placed onthe shoulder joint.
Plyometric exercises employ 3 phas-es, all intended to use the elastic reac-tive properties of muscle to generatemaximal force production.16,22,25 The firstphase is the eccentric phase, where arapid prestretch is applied to the muscu-lotendinous unit, stimulating the musclespindle. The second phase is the amorti-zation phase, representing the time be-tween eccentric and concentric phases.This time should be as short as possibleso that the beneficial neurologic effects ofprestretch are not lost. The final phase isthe resultant concentric action. Wilk etal111-112,114 established a plyometric exer-cise program for the overhead thrower.The initial plyometric program consistsof 2-handed exercise drills such as chestpasses, overhead soccer throws, side-to-side throws, and side-throws. The goal ofthe plyometric drills is to transfer energyfrom the lower extremities and trunk tothe upper extremity. Once these 2-handedexercise drills are mastered, the athlete isprogressed to 1-handed drills. These drillsinclude standing 1-handed throws in afunctional throwing position, wall drib-bling, and plyometric step-and-throws.Swanik et al97 reported that a 6-weekplyometric training program resulted inenhanced joint position sense, enhanced
kinesthesia, and decreased time to peaktorque generation during isokinetic test-ing. Fortun et al44 noted improved shoul-der IR power and throwing distancesafter 8 weeks of plyometric training incomparison with conventional isotonictraining.
Additionally, muscular enduranceexercises should be emphasized for theoverhead thrower. Lyman et al68 docu-mented that the overhead athlete is atgreater risk for shoulder or elbow injurieswhen pitching when fatigued. Recently,Murray et al79 documented the effects offatigue on the entire body during pitch-ing using kinematic and kinetic motionanalysis. Once the thrower was fatigued,shoulder ER decreased and ball velocitydiminished, as did lead lower extrem-ity knee flexion and shoulder adductiontorque. Voight et al103 documented a re-lationship between muscle fatigue anddiminished proprioception. Chen et al24
demonstrated that once the rotator cuff
Ball throw into wall. The patient throwsa 2-pound (0.9 kg) Plyoball (Functional IntegratedTechnologies, Watsonville, CA) against the wall at endrange of external rotation (late cocking).
Seated external rotation on a physioballwith single-leg support. Resisted external rotationis performed with exercise tubing. To enhance thedemands on the shoulder stabilizers, a rhythmicstabilization technique may be performed.
Neuromuscular dynamic stabilizationexercise: exercise tubing resisting shoulder externalrotation with manual resistance at end range.
Scapular horizontal abduction performedon a physioball. This exercise is performed toenhance scapular muscle activity and core stability.

journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 49
muscles are fatigued, the humeral headmigrates superiorly when arm elevationis initiated. Furthermore, Lyman et al67
reported that the predisposing factorthat correlated to the highest percent-age of shoulder injuries in Little Leaguepitchers was complaints of muscle fatiguewhile pitching. Thus the endurance drillsdescribed here appear critical for theoverhead thrower.
Specific endurance exercise drills weuse include wall dribbling with a Plyoball(Functional Integrated Technologies, Wat-sonville, CA), wall arm circles, upper bodycycle, or isotonic exercises using lowerweights with higher repetitions. Othertechniques that may be beneficial to en-hance endurance include throwing an un-derweighted or overweighted ball (that is, aball that is either less than or more than theweight of an official baseball).17,25,32,39,65,102
These techniques are designed to enhancetraining, coordination, and the transfer ofkinetic energy. Fortun et al44 noted an in-crease in shoulder IR strength and powerafter an 8-week plyometric training pro-gram using a weighted ball. Most com-monly, the underweighted ball is used toimprove the transfer of energy and angularmomentum.32,39,102 Conversely, the over-weighted ball is generally used to enhanceshoulder strength and power.32,39,102
During this third rehabilitation phase,an interval throwing program may be ini-tiated. Before initiating such a program,we occasionally suggest that the athleteperform “shadow” or mirror throwing,which is the action of mimicking throw-ing mechanics into a mirror, but not ac-tively throwing. This is designed to allowthe athlete to work on proper throwingmechanics before throwing a baseball.The interval throwing program92 is ini-tiated once the athlete can fulfill thesespecific criteria: (1) satisfactory clinicalexamination, (2) nonpainful ROM, (3)satisfactory isokinetic test results, and (4)appropriate rehabilitation progress. Theinterval throwing program is designed togradually increase the quantity, distance,intensity, and type of throws needed to fa-cilitate the gradual restoration of normal
biomechanics.Interval throwing is organized into 2
phases: phase 1 is a long-toss program(45-180 ft [15-60 m]) and phase 2 isan off-the-mound program for pitchers.During this third rehabilitation phase,we usually initiate phase 1 of the inter-val throwing program at 45 ft (15 m) andprogress to throwing from 60 ft (20 m).The athlete is instructed to use a crow-hop type of throwing mechanism and lobthe ball with an arc for the prescribed dis-tance. Flat-ground, long-toss throwing isused before throwing off the mound to al-low the athlete to gradually increase theapplied loads to the shoulder while usingproper throwing mechanics. In addition,during this phase of rehabilitation, weroutinely allow the position player to ini-tiate a progressive batting program thatprogresses the athlete from swinging alight bat, to hitting a ball off a tee, to soft-toss hitting, to batting practice.
Phase 4 of the rehabilitation program,the return-to-throwing phase, usuallyinvolves the progression of the intervalthrowing program. For pitchers, we prog-ress the long-toss program to 120 ft (40m), whereas position players would prog-ress to throwing from 180 ft (60 m). Oncethe pitcher has successfully completedthrowing from 120 ft, the athlete is in-structed to throw 60 ft from the windupon level ground. Once this step is suc-cessfully completed, phase II (throwingfrom the mound) is performed.92 Positionplayers continue to progress the long-tossprogram to 180 ft, then perform fieldingdrills from their specific position. Whilethe athlete is performing the intervalthrowing program, the clinician shouldcarefully monitor the thrower’s mechan-ics and throwing intensity. In a studyconducted at our biomechanics labora-tory, we objectively measured the throw-ing intensity of healthy pitchers. Whenpitchers were asked to throw at 50%effort, radar gun analysis indicated thatactual effort was approximately 83% oftheir maximum speed. When asked to
throw at 75% effort, they threw at 90% oftheir maximum effort. This indicates thatthese athletes threw at greater intensitiesthan were suggested, which may implydifficulty of controlling velocity at lowerthrowing intensities.
In addition, during this fourth phase,the thrower is instructed to continue allthe exercises previously described to im-prove upper extremity strength, power,and endurance. The athlete is also in-structed to continue the Thrower’s Tenprogram, stretching program, core stabi-lization exercise training, and lower ex-tremity strengthening activities. Lastly,the athlete is counseled on a year-roundconditioning program based on the prin-ciples of periodization.38 Thus, the athleteis instructed when to begin such things asstrength training and throwing.112 To pre-vent the effects of overtraining or throw-ing when poorly conditioned, it is criticalto instruct the athlete specifically on whatto do through specific exercises through-out the year. This is especially critical inpreparing the athlete for the followingseason. Wooden et al119 demonstratedthat performing a dynamic variable re-sistance exercise program significantlyincreased throwing velocity.
verhead-throwing athletestypically present with a uniquemusculoskeletal profile. The over-
head thrower exhibits ROM, postural,and strength changes, which appearto be from adaptations from imposeddemands. This unique client exhibitsunique lesions, and the recognition andtreatment of these lesions may presenta significant challenge to the clinician.Based on the accurate recognition ofthe lesion and underlying cause of thepathology, a successful nonoperative orin some cases operative treatment plancan be implemented. In this manuscript,we have attempted to provide the readerwith information regarding the evalu-ation and treatment of the overheadthrowing athlete.
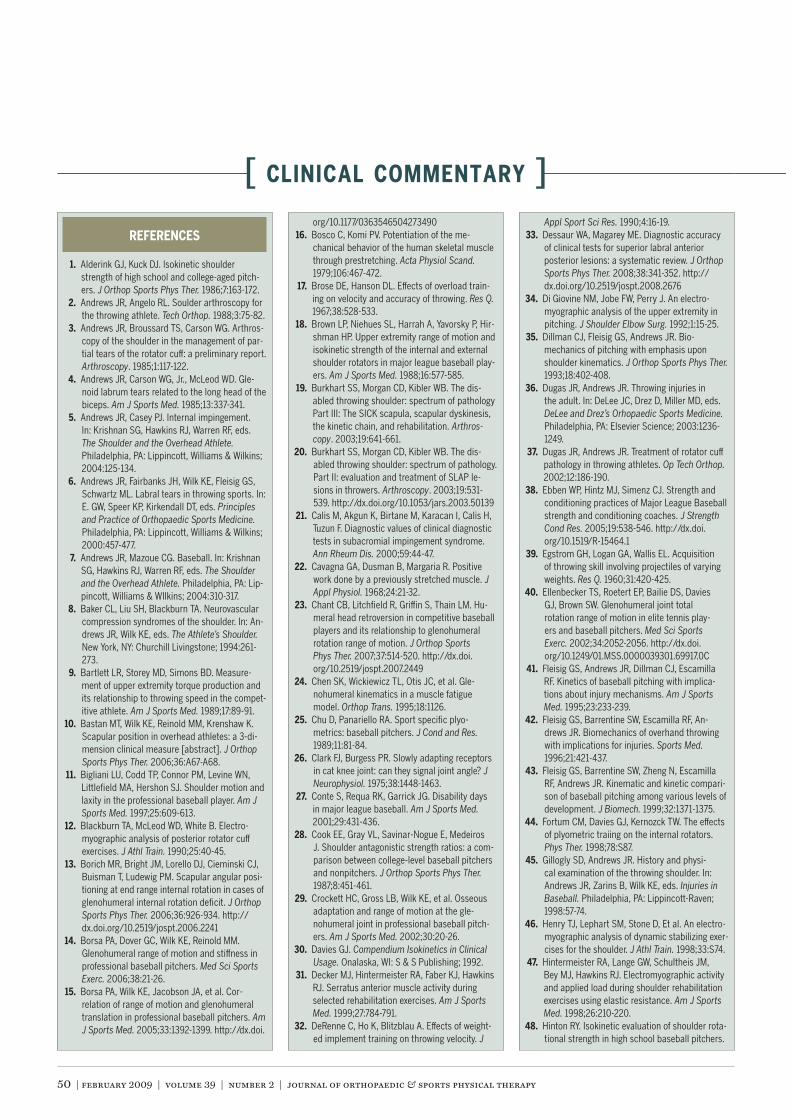
50 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
1. Alderink GJ, Kuck DJ. lsokinetic shoulderstrength of high school and college-aged pitch-ers. J Orthop Sports Phys Ther. 1986;7:163-172.Andrews JR, Angelo RL. Soulder arthroscopy forthe throwing athlete. Tech Orthop. 1988;3:75-82.Andrews JR, Broussard TS, Carson WG. Arthros-copy of the shoulder in the management of par-tial tears of the rotator cuff: a preliminary report.Arthroscopy. 1985;1:117-122.
4. Andrews JR, Carson WG, Jr., McLeod WD. Gle-noid labrum tears related to the long head of thebiceps. Am J Sports Med. 1985;13:337-341.
5. Andrews JR, Casey PJ. Internal impingement.In: Krishnan SG, Hawkins RJ, Warren RF, eds.The Shoulder and the Overhead Athlete.Philadelphia, PA: Lippincott, Williams & Wilkins;2004:125-134.Andrews JR, Fairbanks JH, Wilk KE, Fleisig GS,Schwartz ML. Labral tears in throwing sports. In:E. GW, Speer KP, Kirkendall DT, eds. Principlesand Practice of Orthopaedic Sports Medicine.Philadelphia, PA: Lippincott, Williams & Wilkins;2000:457-477.Andrews JR, Mazoue CG. Baseball. In: KrishnanSG, Hawkins RJ, Warren RF, eds. The Shoulderand the Overhead Athlete. Philadelphia, PA: Lip-pincott, Williams & WIlkins; 2004:310-317.
8. Baker CL, Liu SH, Blackburn TA. Neurovascularcompression syndromes of the shoulder. In: An-drews JR, Wilk KE, eds. The Athlete’s Shoulder.New York, NY: Churchill Livingstone; 1994:261-273.Bartlett LR, Storey MD, Simons BD. Measure-ment of upper extremity torque production andits relationship to throwing speed in the compet-itive athlete. Am J Sports Med. 1989;17:89-91.
10. Bastan MT, Wilk KE, Reinold MM, Krenshaw K.Scapular position in overhead athletes: a 3-di-mension clinical measure [abstract]. J OrthopSports Phys Ther. 2006;36:A67-A68.
11. Bigliani LU, Codd TP, Connor PM, Levine WN,Littlefield MA, Hershon SJ. Shoulder motion andlaxity in the professional baseball player. Am JSports Med. 1997;25:609-613.Blackburn TA, McLeod WD, White B. Electro-myographic analysis of posterior rotator cuffexercises. J Athl Train. 1990;25:40-45.Borich MR, Bright JM, Lorello DJ, Cieminski CJ,Buisman T, Ludewig PM. Scapular angular posi-tioning at end range internal rotation in cases ofglenohumeral internal rotation deficit. J OrthopSports Phys Ther. 2006;36:926-934. http://dx.doi.org/10.2519/jospt.2006.2241
14. Borsa PA, Dover GC, Wilk KE, Reinold MM.Glenohumeral range of motion and stiffness inprofessional baseball pitchers. Med Sci SportsExerc. 2006;38:21-26.
15. Borsa PA, Wilk KE, Jacobson JA, et al. Cor-relation of range of motion and glenohumeraltranslation in professional baseball pitchers. AmJ Sports Med. 2005;33:1392-1399. http://dx.doi.
org/10.1177/0363546504273490Bosco C, Komi PV. Potentiation of the me-chanical behavior of the human skeletal musclethrough prestretching. Acta Physiol Scand.1979;106:467-472.Brose DE, Hanson DL. Effects of overload train-ing on velocity and accuracy of throwing. Res Q.1967;38:528-533.
18. Brown LP, Niehues SL, Harrah A, Yavorsky P, Hir-shman HP. Upper extremity range of motion andisokinetic strength of the internal and externalshoulder rotators in major league baseball play-ers. Am J Sports Med. 1988;16:577-585.Burkhart SS, Morgan CD, Kibler WB. The dis-abled throwing shoulder: spectrum of pathologyPart III: The SICK scapula, scapular dyskinesis,the kinetic chain, and rehabilitation. Arthros-copy. 2003;19:641-661.Burkhart SS, Morgan CD, Kibler WB. The dis-abled throwing shoulder: spectrum of pathology.Part II: evaluation and treatment of SLAP le-sions in throwers. Arthroscopy. 2003;19:531-539. http://dx.doi.org/10.1053/jars.2003.50139Calis M, Akgun K, Birtane M, Karacan I, Calis H,Tuzun F. Diagnostic values of clinical diagnostictests in subacromial impingement syndrome.Ann Rheum Dis. 2000;59:44-47.Cavagna GA, Dusman B, Margaria R. Positivework done by a previously stretched muscle. JAppl Physiol. 1968;24:21-32.Chant CB, Litchfield R, Griffin S, Thain LM. Hu-meral head retroversion in competitive baseballplayers and its relationship to glenohumeralrotation range of motion. J Orthop SportsPhys Ther. 2007;37:514-520. http://dx.doi.org/10.2519/jospt.2007.2449Chen SK, Wickiewicz TL, Otis JC, et al. Gle-nohumeral kinematics in a muscle fatiguemodel. Orthop Trans. 1995;18:1126.Chu D, Panariello RA. Sport specific plyo-metrics: baseball pitchers. J Cond and Res.1989;11:81-84.Clark FJ, Burgess PR. Slowly adapting receptorsin cat knee joint: can they signal joint angle? JNeurophysiol. 1975;38:1448-1463.Conte S, Requa RK, Garrick JG. Disability daysin major league baseball. Am J Sports Med.2001;29:431-436.Cook EE, Gray VL, Savinar-Nogue E, MedeirosJ. Shoulder antagonistic strength ratios: a com-parison between college-level baseball pitchersand nonpitchers. J Orthop Sports Phys Ther.1987;8:451-461.Crockett HC, Gross LB, Wilk KE, et al. Osseousadaptation and range of motion at the gle-nohumeral joint in professional baseball pitch-ers. Am J Sports Med. 2002;30:20-26.Davies GJ. Compendium Isokinetics in ClinicalUsage. Onalaska, WI: S & S Publishing; 1992.Decker MJ, Hintermeister RA, Faber KJ, HawkinsRJ. Serratus anterior muscle activity duringselected rehabilitation exercises. Am J SportsMed. 1999;27:784-791.DeRenne C, Ho K, Blitzblau A. Effects of weight-ed implement training on throwing velocity. J
Appl Sport Sci Res. 1990;4:16-19.Dessaur WA, Magarey ME. Diagnostic accuracyof clinical tests for superior labral anteriorposterior lesions: a systematic review. J OrthopSports Phys Ther. 2008;38:341-352. http://dx.doi.org/10.2519/jospt.2008.2676Di Giovine NM, Jobe FW, Perry J. An electro-myographic analysis of the upper extremity inpitching. J Shoulder Elbow Surg. 1992;1:15-25.Dillman CJ, Fleisig GS, Andrews JR. Bio-mechanics of pitching with emphasis uponshoulder kinematics. J Orthop Sports Phys Ther.1993;18:402-408.Dugas JR, Andrews JR. Throwing injuries inthe adult. In: DeLee JC, Drez D, Miller MD, eds.DeLee and Drez’s Orhopaedic Sports Medicine.Philadelphia, PA: Elsevier Science; 2003:1236-1249.Dugas JR, Andrews JR. Treatment of rotator cuffpathology in throwing athletes. Op Tech Orthop.2002;12:186-190.Ebben WP, Hintz MJ, Simenz CJ. Strength andconditioning practices of Major League Baseballstrength and conditioning coaches. J StrengthCond Res. 2005;19:538-546. http://dx.doi.org/10.1519/R-15464.1Egstrom GH, Logan GA, Wallis EL. Acquisitionof throwing skill involving projectiles of varyingweights. Res Q. 1960;31:420-425.
40. Ellenbecker TS, Roetert EP, Bailie DS, DaviesGJ, Brown SW. Glenohumeral joint totalrotation range of motion in elite tennis play-ers and baseball pitchers. Med Sci SportsExerc. 2002;34:2052-2056. http://dx.doi.org/10.1249/01.MSS.0000039301.69917.0C
41. Fleisig GS, Andrews JR, Dillman CJ, EscamillaRF. Kinetics of baseball pitching with implica-tions about injury mechanisms. Am J SportsMed. 1995;23:233-239.Fleisig GS, Barrentine SW, Escamilla RF, An-drews JR. Biomechanics of overhand throwingwith implications for injuries. Sports Med.1996;21:421-437.Fleisig GS, Barrentine SW, Zheng N, EscamillaRF, Andrews JR. Kinematic and kinetic compari-son of baseball pitching among various levels ofdevelopment. J Biomech. 1999;32:1371-1375.
44. Fortum CM, Davies GJ, Kernozck TW. The effectsof plyometric traiing on the internal rotators.Phys Ther. 1998;78:S87.
45. Gillogly SD, Andrews JR. History and physi-cal examination of the throwing shoulder. In:Andrews JR, Zarins B, Wilk KE, eds. Injuries inBaseball. Philadelphia, PA: Lippincott-Raven;1998:57-74.Henry TJ, Lephart SM, Stone D, Et al. An electro-myographic analysis of dynamic stabilizing exer-cises for the shoulder. J Athl Train. 1998;33:S74.Hintermeister RA, Lange GW, Schultheis JM,Bey MJ, Hawkins RJ. Electromyographic activityand applied load during shoulder rehabilitationexercises using elastic resistance. Am J SportsMed. 1998;26:210-220.
48. Hinton RY. Isokinetic evaluation of shoulder rota-tional strength in high school baseball pitchers.
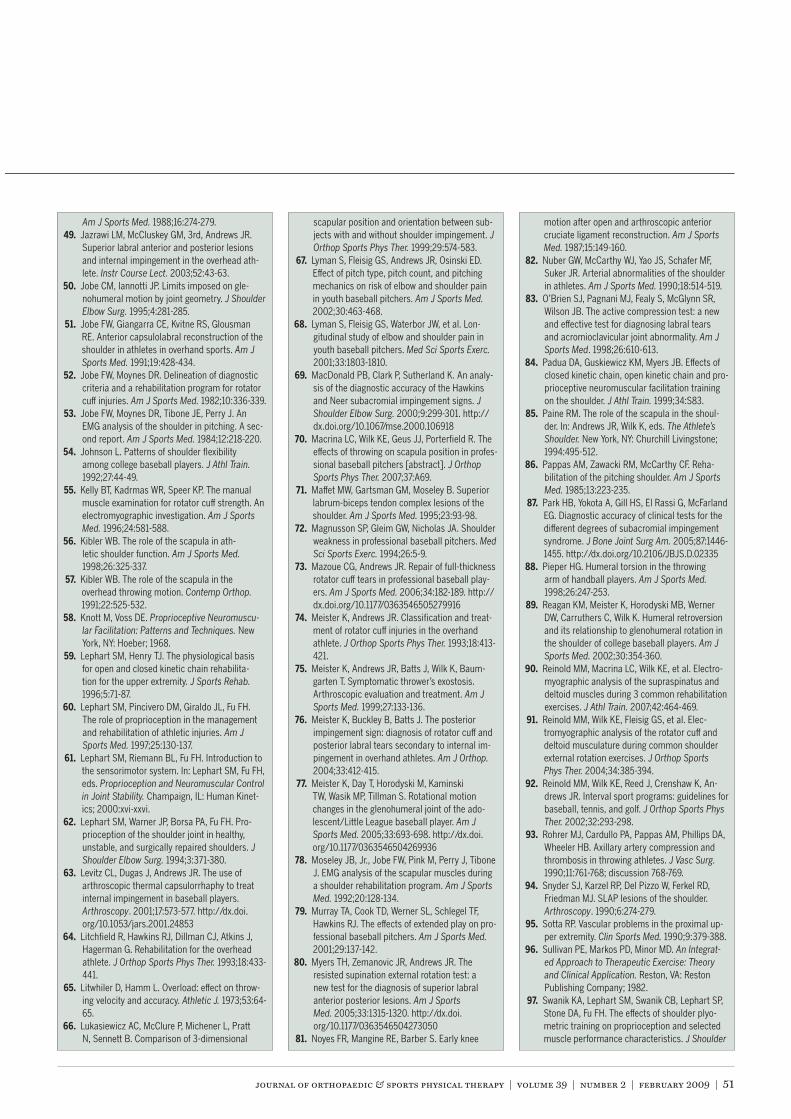
journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 51
Am J Sports Med. 1988;16:274-279.Jazrawi LM, McCluskey GM, 3rd, Andrews JR.Superior labral anterior and posterior lesionsand internal impingement in the overhead ath-lete. Instr Course Lect. 2003;52:43-63.
50. Jobe CM, Iannotti JP. Limits imposed on gle-nohumeral motion by joint geometry. J ShoulderElbow Surg. 1995;4:281-285.
51. Jobe FW, Giangarra CE, Kvitne RS, GlousmanRE. Anterior capsulolabral reconstruction of theshoulder in athletes in overhand sports. Am JSports Med. 1991;19:428-434.Jobe FW, Moynes DR. Delineation of diagnosticcriteria and a rehabilitation program for rotatorcuff injuries. Am J Sports Med. 1982;10:336-339.Jobe FW, Moynes DR, Tibone JE, Perry J. AnEMG analysis of the shoulder in pitching. A sec-ond report. Am J Sports Med. 1984;12:218-220.
54. Johnson L. Patterns of shoulder flexibilityamong college baseball players. J Athl Train.1992;27:44-49.
55. Kelly BT, Kadrmas WR, Speer KP. The manualmuscle examination for rotator cuff strength. Anelectromyographic investigation. Am J SportsMed. 1996;24:581-588.Kibler WB. The role of the scapula in ath-letic shoulder function. Am J Sports Med.1998;26:325-337.Kibler WB. The role of the scapula in theoverhead throwing motion. Contemp Orthop.1991;22:525-532.
58. Knott M, Voss DE. Proprioceptive Neuromuscu-lar Facilitation: Patterns and Techniques. NewYork, NY: Hoeber; 1968.Lephart SM, Henry TJ. The physiological basisfor open and closed kinetic chain rehabilita-tion for the upper extremity. J Sports Rehab.1996;5:71-87.Lephart SM, Pincivero DM, Giraldo JL, Fu FH.The role of proprioception in the managementand rehabilitation of athletic injuries. Am JSports Med. 1997;25:130-137.Lephart SM, Riemann BL, Fu FH. Introduction tothe sensorimotor system. In: Lephart SM, Fu FH,eds. Proprioception and Neuromuscular Controlin Joint Stability. Champaign, IL: Human Kinet-ics; 2000:xvi-xxvi.Lephart SM, Warner JP, Borsa PA, Fu FH. Pro-prioception of the shoulder joint in healthy,unstable, and surgically repaired shoulders. JShoulder Elbow Surg. 1994;3:371-380.Levitz CL, Dugas J, Andrews JR. The use ofarthroscopic thermal capsulorrhaphy to treatinternal impingement in baseball players.Arthroscopy. 2001;17:573-577. http://dx.doi.org/10.1053/jars.2001.24853Litchfield R, Hawkins RJ, Dillman CJ, Atkins J,Hagerman G. Rehabilitation for the overheadathlete. J Orthop Sports Phys Ther. 1993;18:433-441.Litwhiler D, Hamm L. Overload: effect on throw-ing velocity and accuracy. Athletic J. 1973;53:64-65.Lukasiewicz AC, McClure P, Michener L, PrattN, Sennett B. Comparison of 3-dimensional
scapular position and orientation between sub-jects with and without shoulder impingement. JOrthop Sports Phys Ther. 1999;29:574-583.Lyman S, Fleisig GS, Andrews JR, Osinski ED.Effect of pitch type, pitch count, and pitchingmechanics on risk of elbow and shoulder painin youth baseball pitchers. Am J Sports Med.2002;30:463-468.Lyman S, Fleisig GS, Waterbor JW, et al. Lon-gitudinal study of elbow and shoulder pain inyouth baseball pitchers. Med Sci Sports Exerc.2001;33:1803-1810.MacDonald PB, Clark P, Sutherland K. An analy-sis of the diagnostic accuracy of the Hawkinsand Neer subacromial impingement signs. JShoulder Elbow Surg. 2000;9:299-301. http://dx.doi.org/10.1067/mse.2000.106918Macrina LC, Wilk KE, Geus JJ, Porterfield R. Theeffects of throwing on scapula position in profes-sional baseball pitchers [abstract]. J OrthopSports Phys Ther. 2007;37:A69.Maffet MW, Gartsman GM, Moseley B. Superiorlabrum-biceps tendon complex lesions of theshoulder. Am J Sports Med. 1995;23:93-98.Magnusson SP, Gleim GW, Nicholas JA. Shoulderweakness in professional baseball pitchers. MedSci Sports Exerc. 1994;26:5-9.Mazoue CG, Andrews JR. Repair of full-thicknessrotator cuff tears in professional baseball play-ers. Am J Sports Med. 2006;34:182-189. http://dx.doi.org/10.1177/0363546505279916Meister K, Andrews JR. Classification and treat-ment of rotator cuff injuries in the overhandathlete. J Orthop Sports Phys Ther. 1993;18:413-421.Meister K, Andrews JR, Batts J, Wilk K, Baum-garten T. Symptomatic thrower’s exostosis.Arthroscopic evaluation and treatment. Am JSports Med. 1999;27:133-136.Meister K, Buckley B, Batts J. The posteriorimpingement sign: diagnosis of rotator cuff andposterior labral tears secondary to internal im-pingement in overhand athletes. Am J Orthop.2004;33:412-415.Meister K, Day T, Horodyski M, KaminskiTW, Wasik MP, Tillman S. Rotational motionchanges in the glenohumeral joint of the ado-lescent/Little League baseball player. Am JSports Med. 2005;33:693-698. http://dx.doi.org/10.1177/0363546504269936Moseley JB, Jr., Jobe FW, Pink M, Perry J, TiboneJ. EMG analysis of the scapular muscles duringa shoulder rehabilitation program. Am J SportsMed. 1992;20:128-134.Murray TA, Cook TD, Werner SL, Schlegel TF,Hawkins RJ. The effects of extended play on pro-fessional baseball pitchers. Am J Sports Med.2001;29:137-142.
80. Myers TH, Zemanovic JR, Andrews JR. Theresisted supination external rotation test: anew test for the diagnosis of superior labralanterior posterior lesions. Am J SportsMed. 2005;33:1315-1320. http://dx.doi.org/10.1177/0363546504273050
81. Noyes FR, Mangine RE, Barber S. Early knee
motion after open and arthroscopic anteriorcruciate ligament reconstruction. Am J SportsMed. 1987;15:149-160.Nuber GW, McCarthy WJ, Yao JS, Schafer MF,Suker JR. Arterial abnormalities of the shoulderin athletes. Am J Sports Med. 1990;18:514-519.O’Brien SJ, Pagnani MJ, Fealy S, McGlynn SR,Wilson JB. The active compression test: a newand effective test for diagnosing labral tearsand acromioclavicular joint abnormality. Am JSports Med. 1998;26:610-613.
84. Padua DA, Guskiewicz KM, Myers JB. Effects ofclosed kinetic chain, open kinetic chain and pro-prioceptive neuromuscular facilitation trainingon the shoulder. J Athl Train. 1999;34:S83.
85. Paine RM. The role of the scapula in the shoul-der. In: Andrews JR, Wilk K, eds. The Athlete’sShoulder. New York, NY: Churchill Livingstone;1994:495-512.Pappas AM, Zawacki RM, McCarthy CF. Reha-bilitation of the pitching shoulder. Am J SportsMed. 1985;13:223-235.Park HB, Yokota A, Gill HS, El Rassi G, McFarlandEG. Diagnostic accuracy of clinical tests for thedifferent degrees of subacromial impingementsyndrome. J Bone Joint Surg Am. 2005;87:1446-1455. http://dx.doi.org/10.2106/JBJS.D.02335
88. Pieper HG. Humeral torsion in the throwingarm of handball players. Am J Sports Med.1998;26:247-253.Reagan KM, Meister K, Horodyski MB, WernerDW, Carruthers C, Wilk K. Humeral retroversionand its relationship to glenohumeral rotation inthe shoulder of college baseball players. Am JSports Med. 2002;30:354-360.Reinold MM, Macrina LC, Wilk KE, et al. Electro-myographic analysis of the supraspinatus anddeltoid muscles during 3 common rehabilitationexercises. J Athl Train. 2007;42:464-469.Reinold MM, Wilk KE, Fleisig GS, et al. Elec-tromyographic analysis of the rotator cuff anddeltoid musculature during common shoulderexternal rotation exercises. J Orthop SportsPhys Ther. 2004;34:385-394.Reinold MM, Wilk KE, Reed J, Crenshaw K, An-drews JR. Interval sport programs: guidelines forbaseball, tennis, and golf. J Orthop Sports PhysTher. 2002;32:293-298.Rohrer MJ, Cardullo PA, Pappas AM, Phillips DA,Wheeler HB. Axillary artery compression andthrombosis in throwing athletes. J Vasc Surg.1990;11:761-768; discussion 768-769.Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD,Friedman MJ. SLAP lesions of the shoulder.Arthroscopy. 1990;6:274-279.Sotta RP. Vascular problems in the proximal up-per extremity. Clin Sports Med. 1990;9:379-388.Sullivan PE, Markos PD, Minor MD. An Integrat-ed Approach to Therapeutic Exercise: Theoryand Clinical Application. Reston, VA: RestonPublishing Company; 1982.Swanik KA, Lephart SM, Swanik CB, Lephart SP,Stone DA, Fu FH. The effects of shoulder plyo-metric training on proprioception and selectedmuscle performance characteristics. J Shoulder
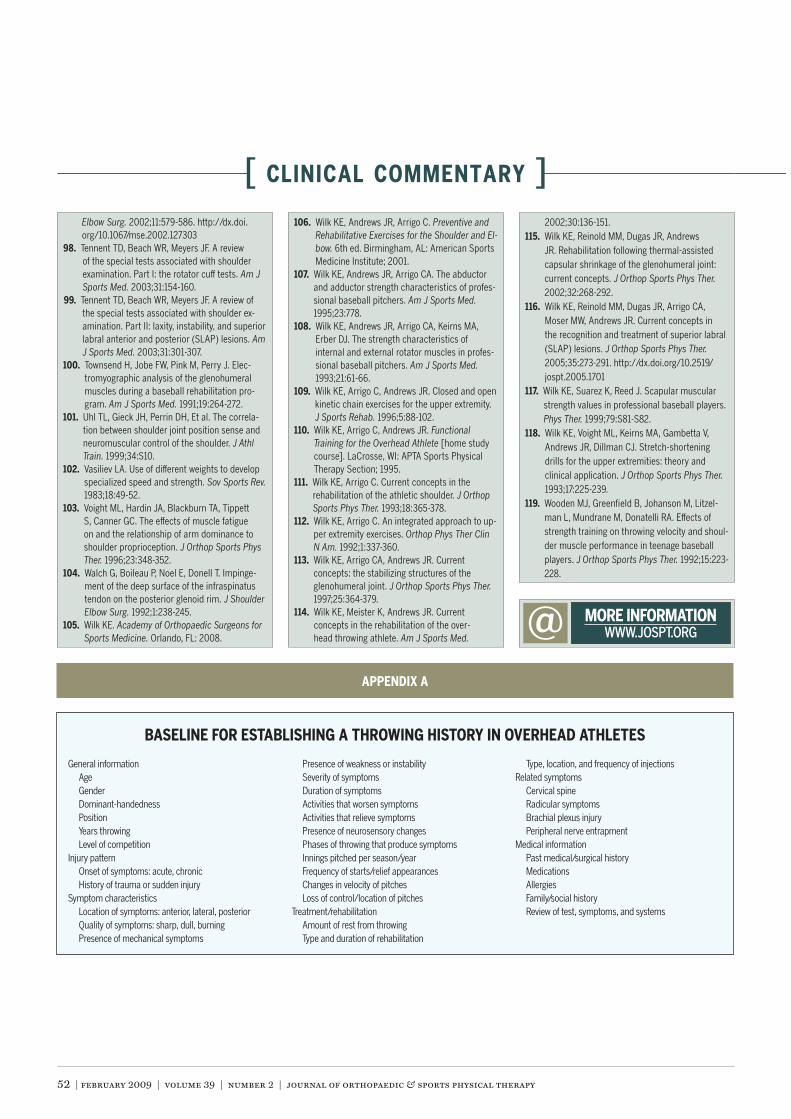
52 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
@ WWW.JOSPT.ORG
Elbow Surg. 2002;11:579-586. http://dx.doi.org/10.1067/mse.2002.127303Tennent TD, Beach WR, Meyers JF. A reviewof the special tests associated with shoulderexamination. Part I: the rotator cuff tests. Am JSports Med. 2003;31:154-160.Tennent TD, Beach WR, Meyers JF. A review ofthe special tests associated with shoulder ex-amination. Part II: laxity, instability, and superiorlabral anterior and posterior (SLAP) lesions. AmJ Sports Med. 2003;31:301-307.
100. Townsend H, Jobe FW, Pink M, Perry J. Elec-tromyographic analysis of the glenohumeralmuscles during a baseball rehabilitation pro-gram. Am J Sports Med. 1991;19:264-272.
101. Uhl TL, Gieck JH, Perrin DH, Et al. The correla-tion between shoulder joint position sense andneuromuscular control of the shoulder. J AthlTrain. 1999;34:S10.Vasiliev LA. Use of different weights to developspecialized speed and strength. Sov Sports Rev.1983;18:49-52.Voight ML, Hardin JA, Blackburn TA, TippettS, Canner GC. The effects of muscle fatigueon and the relationship of arm dominance toshoulder proprioception. J Orthop Sports PhysTher. 1996;23:348-352.
104. Walch G, Boileau P, Noel E, Donell T. Impinge-ment of the deep surface of the infraspinatustendon on the posterior glenoid rim. J ShoulderElbow Surg. 1992;1:238-245.
105. Wilk KE. Academy of Orthopaedic Surgeons forSports Medicine. Orlando, FL: 2008.
Wilk KE, Andrews JR, Arrigo C. Preventive andRehabilitative Exercises for the Shoulder and El-bow. 6th ed. Birmingham, AL: American SportsMedicine Institute; 2001.Wilk KE, Andrews JR, Arrigo CA. The abductorand adductor strength characteristics of profes-sional baseball pitchers. Am J Sports Med.1995;23:778.
108. Wilk KE, Andrews JR, Arrigo CA, Keirns MA,Erber DJ. The strength characteristics ofinternal and external rotator muscles in profes-sional baseball pitchers. Am J Sports Med.1993;21:61-66.Wilk KE, Arrigo C, Andrews JR. Closed and openkinetic chain exercises for the upper extremity.J Sports Rehab. 1996;5:88-102.
110. Wilk KE, Arrigo C, Andrews JR. FunctionalTraining for the Overhead Athlete [home studycourse]. LaCrosse, WI: APTA Sports PhysicalTherapy Section; 1995.
111. Wilk KE, Arrigo C. Current concepts in therehabilitation of the athletic shoulder. J OrthopSports Phys Ther. 1993;18:365-378.Wilk KE, Arrigo C. An integrated approach to up-per extremity exercises. Orthop Phys Ther ClinN Am. 1992;1:337-360.Wilk KE, Arrigo CA, Andrews JR. Currentconcepts: the stabilizing structures of theglenohumeral joint. J Orthop Sports Phys Ther.1997;25:364-379.
114. Wilk KE, Meister K, Andrews JR. Currentconcepts in the rehabilitation of the over-head throwing athlete. Am J Sports Med.
2002;30:136-151.115. Wilk KE, Reinold MM, Dugas JR, Andrews
JR. Rehabilitation following thermal-assistedcapsular shrinkage of the glenohumeral joint:current concepts. J Orthop Sports Phys Ther.2002;32:268-292.Wilk KE, Reinold MM, Dugas JR, Arrigo CA,Moser MW, Andrews JR. Current concepts inthe recognition and treatment of superior labral(SLAP) lesions. J Orthop Sports Phys Ther.2005;35:273-291. http://dx.doi.org/10.2519/jospt.2005.1701Wilk KE, Suarez K, Reed J. Scapular muscularstrength values in professional baseball players.Phys Ther. 1999;79:S81-S82.
118. Wilk KE, Voight ML, Keirns MA, Gambetta V,Andrews JR, Dillman CJ. Stretch-shorteningdrills for the upper extremities: theory andclinical application. J Orthop Sports Phys Ther.1993;17:225-239.Wooden MJ, Greenfield B, Johanson M, Litzel-man L, Mundrane M, Donatelli RA. Effects ofstrength training on throwing velocity and shoul-der muscle performance in teenage baseballplayers. J Orthop Sports Phys Ther. 1992;15:223-228.
General informationAgeGenderDominant-handednessPositionYears throwingLevel of competition
Injury patternOnset of symptoms: acute, chronicHistory of trauma or sudden injury
Symptom characteristicsLocation of symptoms: anterior, lateral, posteriorQuality of symptoms: sharp, dull, burningPresence of mechanical symptoms
Presence of weakness or instabilitySeverity of symptomsDuration of symptomsActivities that worsen symptomsActivities that relieve symptomsPresence of neurosensory changesPhases of throwing that produce symptomsInnings pitched per season/yearFrequency of starts/relief appearancesChanges in velocity of pitchesLoss of control/location of pitches
Treatment/rehabilitationAmount of rest from throwingType and duration of rehabilitation
Type, location, and frequency of injectionsRelated symptoms
Cervical spineRadicular symptomsBrachial plexus injuryPeripheral nerve entrapment
Medical informationPast medical/surgical historyMedicationsAllergiesFamily/social historyReview of test, symptoms, and systems
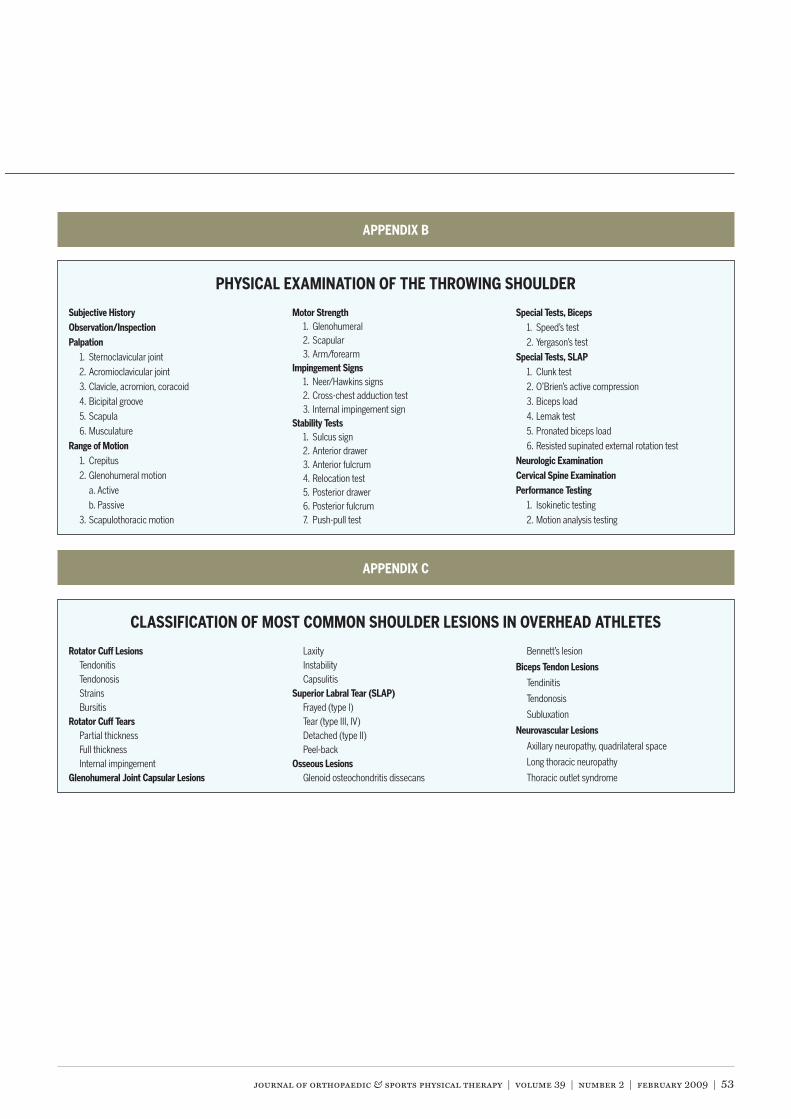
journal of orthopaedic & sports physical therapy | volume 39 | number 2 | february 2009 | 53
APPENDIX B
Subjective HistoryObservation/InspectionPalpation
1. Sternoclavicular joint
2. Acromioclavicular joint
3. Clavicle, acromion, coracoid
4. Bicipital groove
5. Scapula
6. Musculature
Range of Motion1. Crepitus
2. Glenohumeral motion
a. Active
b. Passive
3. Scapulothoracic motion
Motor Strength1. Glenohumeral2. Scapular3. Arm/forearm
Impingement Signs1. Neer/Hawkins signs2. Cross-chest adduction test3. Internal impingement sign
Stability Tests1. Sulcus sign2. Anterior drawer3. Anterior fulcrum4. Relocation test5. Posterior drawer6. Posterior fulcrum7. Push-pull test
Special Tests, Biceps1. Speed’s test
2. Yergason’s test
Special Tests, SLAP1. Clunk test
2. O’Brien’s active compression
3. Biceps load
4. Lemak test
5. Pronated biceps load
6. Resisted supinated external rotation test
Neurologic ExaminationCervical Spine ExaminationPerformance Testing
1. Isokinetic testing
2. Motion analysis testing
PHYSICAL EXAMINATION OF THE THROWING SHOULDER
APPENDIX C
Rotator Cuff LesionsTendonitisTendonosisStrainsBursitis
Rotator Cuff TearsPartial thicknessFull thicknessInternal impingement
Glenohumeral Joint Capsular Lesions
LaxityInstabilityCapsulitis
Superior Labral Tear (SLAP)Frayed (type I)Tear (type III, IV)Detached (type II)Peel-back
Osseous LesionsGlenoid osteochondritis dissecans
Bennett’s lesion
Biceps Tendon Lesions
Tendinitis
Tendonosis
Subluxation
Neurovascular Lesions
Axillary neuropathy, quadrilateral space
Long thoracic neuropathy
Thoracic outlet syndrome
CLASSIFICATION OF MOST COMMON SHOULDER LESIONS IN OVERHEAD ATHLETES
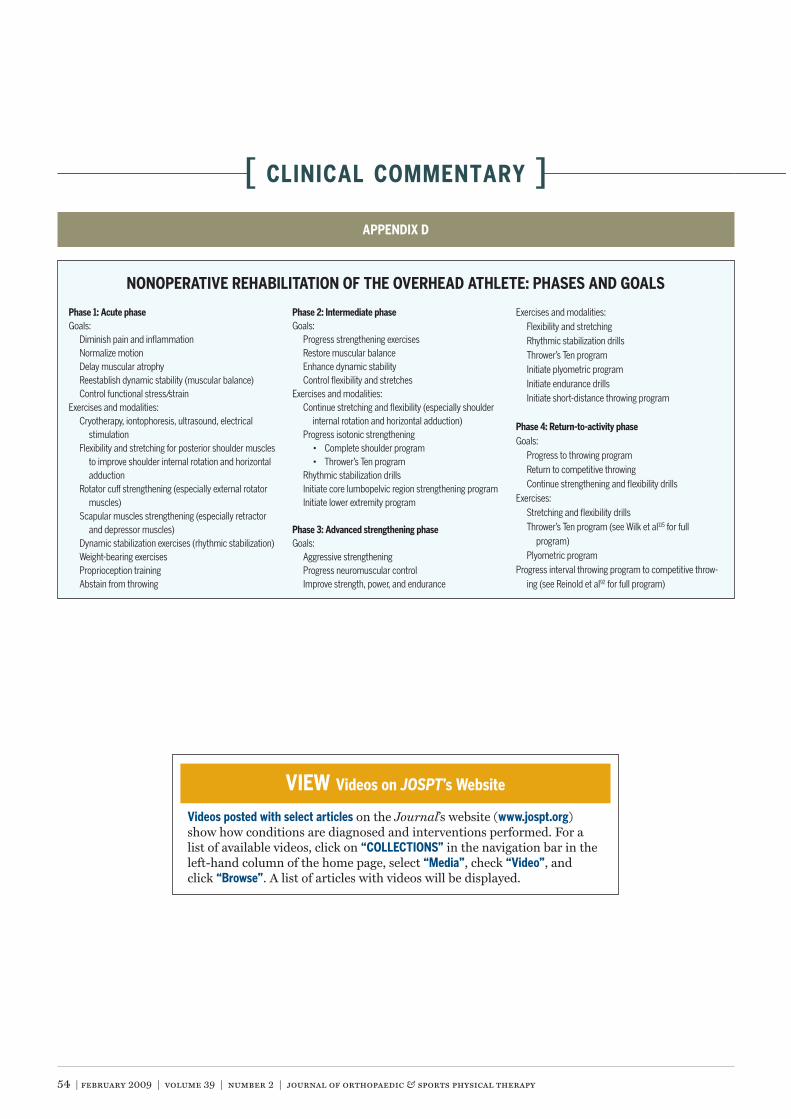
54 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
APPENDIX D
Phase 1: Acute phaseGoals:
Diminish pain and inflammationNormalize motionDelay muscular atrophyReestablish dynamic stability (muscular balance)Control functional stress/strain
Exercises and modalities:Cryotherapy, iontophoresis, ultrasound, electrical
stimulationFlexibility and stretching for posterior shoulder muscles
to improve shoulder internal rotation and horizontaladduction
Rotator cuff strengthening (especially external rotatormuscles)
Scapular muscles strengthening (especially retractorand depressor muscles)
Dynamic stabilization exercises (rhythmic stabilization)Weight-bearing exercisesProprioception trainingAbstain from throwing
Phase 2: Intermediate phaseGoals:
Progress strengthening exercisesRestore muscular balanceEnhance dynamic stabilityControl flexibility and stretches
Exercises and modalities:Continue stretching and flexibility (especially shoulder
internal rotation and horizontal adduction)Progress isotonic strengthening
Rhythmic stabilization drillsInitiate core lumbopelvic region strengthening programInitiate lower extremity program
Phase 3: Advanced strengthening phaseGoals:
Aggressive strengtheningProgress neuromuscular controlImprove strength, power, and endurance
Exercises and modalities:Flexibility and stretchingRhythmic stabilization drills
Initiate plyometric programInitiate endurance drillsInitiate short-distance throwing program
Phase 4: Return-to-activity phaseGoals:
Progress to throwing programReturn to competitive throwingContinue strengthening and flexibility drills
Exercises:Stretching and flexibility drills
115 for fullprogram)
Plyometric programProgress interval throwing program to competitive throw-
ing (see Reinold et al92 for full program)
NONOPERATIVE REHABILITATION OF THE OVERHEAD ATHLETE: PHASES AND GOALS
VIEW Videos on JOSPT’s Website
Videos posted with select articles on the Journal’s website (www.jospt.org)show how conditions are diagnosed and interventions performed. For alist of available videos, click on “COLLECTIONS” in the navigation bar in theleft-hand column of the home page, select “Media”, check “Video”, andclick “Browse”. A list of articles with videos will be displayed.