Embed Size (px)
Citation preview

Fleischner Society: Glossary ofTerms for Thoracic Imaging1
David M. Hansell, MD, FRCP, FRCRAlexander A. Bankier, MDHeber MacMahon, MB, BCh, BAOTheresa C. McLoud, MDNestor L. Muller, MD, PhDJacques Remy, MD
Members of the Fleischner Society compiled a glossary ofterms for thoracic imaging that replaces previous glossa-ries published in 1984 and 1996 for thoracic radiographyand computed tomography (CT), respectively. The need toupdate the previous versions came from the recognitionthat new words have emerged, others have become obso-lete, and the meaning of some terms has changed. Briefdescriptions of some diseases are included, and pictorialexamples (chest radiographs and CT scans) are providedfor the majority of terms.
� RSNA, 2008
1 From the Department of Radiology, Royal BromptonHospital, Sydney Street, London SW3 6NP, United King-dom (D.M.H.); Department of Radiology, Beth Israel Dea-coness Medical Center, Boston, Mass (A.A.B.); Depart-ment of Radiology, University of Chicago Hospital, Chi-cago, Ill (H.M.); Department of Radiology, MassachusettsGeneral Hospital, Boston, Mass (T.C.M.); Department ofRadiology, Vancouver General Hospital, Vancouver, BritishColumbia, Canada (N.L.M.); and Department of Radiology,CHRU de Lille, Hopital Calmette, Lille, France (J.R.). Re-ceived April 21, 2007; revision requested May 29; revi-sion received June 6; accepted August 7; final versionaccepted September 19. Address correspondence to:D.M.H. (e-mail: [email protected]).
� RSNA, 2008
REVIEWS
ANDCOM
MENTARY
�SPECIAL
REVIEW
Radiology: Volume 246: Number 3—March 2008 697
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.

The present glossary is the thirdprepared by members of the Fleis-chner Society and replaces the
glossaries of terms for thoracic radiol-ogy (1) and CT (2), respectively. Theimpetus to combine and update the pre-vious versions came from the recogni-tion that with the recent developmentsin imaging new words have arrived, oth-ers have become obsolete, and themeaning of some terms has changed.The intention of this latest glossary isnot to be exhaustive but to concentrateon those terms whose meaning may beproblematic. Terms and techniques notused exclusively in thoracic imaging arenot included.
Two new features are the inclusionof brief descriptions of the idiopathicinterstitial pneumonias (IIPs) and picto-rial examples (chest radiographs andcomputed tomographic [CT] scans) forthe majority of terms. The decision toinclude vignettes of the IIPs (but notother pathologic entities) was based onthe perception that, despite the recentscrutiny and reclassification, the IIPs re-main a confusing group of diseases. Wetrust that the illustrations enhance, butdo not distract from, the definitions. Inthis context, the figures should be re-garded as of less importance than thetext—they are merely examples andshould not be taken as representing thefull range of possible imaging appear-ances (which may be found in the refer-ences provided in this glossary or incomprehensive textbooks).
We hope that this glossary of termswill be helpful, and it is presented in thespirit of the sentiment of Edward J. Huththat “scientific writing calls for precisionas much in naming things and concepts asin presenting data” (3). It is right to re-peat the request with which the last Fleis-chner Society glossary closed: “[U]se ofwords is inherently controversial and weare pleased to invite readers to offer im-provements to our definitions” (2).
Glossary
acinusAnatomy.—The acinus is a structuralunit of the lung distal to a terminal bron-
chiole and is supplied by first-order re-spiratory bronchioles; it contains alveo-lar ducts and alveoli. It is the largest unitin which all airways participate in gasexchange and is approximately 6–10mm in diameter. One secondary pulmo-nary lobule contains between three and25 acini (4).
Radiographs and CT scans.—Indi-vidual normal acini are not visible, butacinar arteries can occasionally be iden-tified on thin-section CT scans. Accumu-lation of pathologic material in acinimay be seen as poorly defined nodularopacities on chest radiographs and thin-section CT images. (See also nodules.)
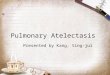
acute interstitial pneumonia, or AIPPathology.—The term acute interstitialpneumonia is reserved for diffuse alveo-lar damage of unknown cause. Theacute phase is characterized by edemaand hyaline membrane formation. Thelater phase is characterized by airspaceand/or interstitial organization (5). Thehistologic pattern is indistinguishablefrom that of acute respiratory distresssyndrome.
Radiographs and CT scans.—In theacute phase, patchy bilateral ground-glass opacities are seen (6), often withsome sparing of individual lobules, pro-
ducing a geographic appearance; denseopacification is seen in the dependentlung (Fig 1). In the organizing phase,architectural distortion, traction bron-chiectasis, cysts, and reticular opacitiesare seen (7).
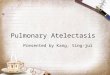
air bronchogramRadiographs and CT scans.—An airbronchogram is a pattern of air-filled(low-attenuation) bronchi on a back-ground of opaque (high-attenuation) air-less lung (Fig 2). The sign implies (a) pa-tency of proximal airways and (b) evacua-tion of alveolar air by means of absorption(atelectasis) or replacement (eg, pneu-monia) or a combination of these pro-cesses. In rare cases, the displacementof air is the result of marked interstitialexpansion (eg, lymphoma) (8).
Figure 1
Figure 1: Transverse CT scan in a patient withacute interstitial pneumonia.
Figure 2
Figure 2: Transverse CT scan shows air bron-chogram as air-filled bronchi (arrows) againstbackground of high-attenuation lung.
Published online before print10.1148/radiol.2462070712
Radiology 2008; 246:697–722
Authors stated no financial relationship to disclose.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
698 Radiology: Volume 246: Number 3—March 2008

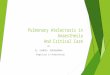
air crescentRadiographs and CT scans.—An aircrescent is a collection of air in a cres-centic shape that separates the wall of acavity from an inner mass (Fig 3). Theair crescent sign is often consideredcharacteristic of either Aspergillus colo-nization of preexisting cavities or re-traction of infarcted lung in angioinva-sive aspergillosis (9,10). However, theair crescent sign has also been reportedin other conditions, including tuberculo-sis, Wegener granulomatosis, intracavi-tary hemorrhage, and lung cancer. (Seealso mycetoma.)
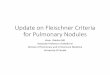
air trappingPathophysiology.—Air trapping is re-tention of air in the lung distal to anobstruction (usually partial).
CT scans.—Air trapping is seen onend-expiration CT scans as parenchy-mal areas with less than normal in-crease in attenuation and lack of volumereduction. Comparison between in-spiratory and expiratory CT scans canbe helpful when air trapping is subtle ordiffuse (11,12) (Fig 4). Differentiationfrom areas of decreased attenuation re-sulting from hypoperfusion as a conse-quence of an occlusive vascular disorder(eg, chronic thromboembolism) may beproblematic (13), but other findings ofairways versus vascular disease are usu-ally present. (See also mosaic attenua-tion pattern.)
airspaceAnatomy.—An airspace is the gas-con-taining part of the lung, including therespiratory bronchioles but excludingpurely conducting airways, such as ter-minal bronchioles.
Radiographs and CT scans.—Thisterm is used in conjunction with consol-idation, opacity, and nodules to desig-nate the filling of airspaces with theproducts of disease (14).
aortopulmonary windowAnatomy.—The aortopulmonary win-dow is the mediastinal region boundedanteriorly by the ascending aorta, pos-teriorly by the descending aorta, crani-ally by the aortic arch, inferiorly by theleft pulmonary artery, medially by theligamentum arteriosum, and laterally bythe pleura and left lung (15,16).
Radiographs and CT scans.—Focalconcavity in the left mediastinal borderbelow the aorta and above the left pul-monary artery can be seen on a frontalradiograph (Fig 5). Its appearance maybe modified by tortuosity of the aorta.The aortopulmonary window is a com-mon site of lymphadenopathy in a vari-ety of inflammatory and neoplastic dis-eases.
apical capPathology.—An apical cap is a caplikelesion at the lung apex, usually causedby intrapulmonary and pleural fibrosispulling down extrapleural fat (17) orpossibly by chronic ischemia resulting inhyaline plaque formation on the visceralpleura (18). The prevalence increaseswith age. It can also be seen in hema-toma resulting from aortic rupture or inother fluid collection associated with in-fection or tumor, either outside the pa-rietal pleura or loculated within thepleural space (19).
Radiographs and CT scans.—Theusual appearance is of homogeneoussoft-tissue attenuation capping the ex-
Figure 3
Figure 3: Magnified chest radiograph showsair crescent (arrows) adjacent to mycetoma.
Figure 4
Figure 4: Transverse CT scans at end inspira-tion and end expiration show air trapping.
Figure 5
Figure 5: Magnified chest radiograph showsaortopulmonary window.
Figure 6
Figure 6: Magnified chest radiograph showsapical cap (arrow).
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 699

treme lung apex (uni- or bilaterally),with a sharp or irregular lower border(Fig 6). Thickness is variable, rangingup to about 30 mm (17). An apical capoccasionally mimics apical consolidationon transverse CT scans.
architectural distortionPathology.—Architectural distortion ischaracterized by abnormal displace-ment of bronchi, vessels, fissures, orsepta caused by diffuse or localizedlung disease, particularly interstitialfibrosis.
CT scans.—Lung anatomy has a dis-torted appearance and is usually associ-ated with pulmonary fibrosis (Fig 7) andaccompanied by volume loss.
atelectasisPathophysiology.—Atelectasis is re-duced inflation of all or part of the lung(20). One of the commonest mechanismsis resorption of air distal to airway ob-struction (eg, an endobronchial neo-plasm) (21). The synonym collapse is of-ten used interchangeably with atelectasis,particularly when it is severe or accompa-nied by obvious increase in lung opacity.
Radiographs and CT scans.—Re-duced volume is seen, accompanied byincreased opacity (chest radiograph) orattenuation (CT scan) in the affectedpart of the lung (Fig 8). Atelectasis isoften associated with abnormal dis-placement of fissures, bronchi, vessels,diaphragm, heart, or mediastinum (22).The distribution can be lobar, segmen-tal, or subsegmental. Atelectasis is oftenqualified by descriptors such as linear,discoid, or platelike. (See also linearatelectasis, rounded atelectasis.)
azygoesophageal recessAnatomy.—The azygoesophageal re-cess is a right posterior mediastinal re-cess into which the edge of the rightlower lobe extends. It is limited superi-orly by the azygos arch, posteriorly bythe azygos vein and pleura anterior tothe vertebral column, and medially bythe esophagus and adjacent structures.
Radiographs and CT scans.—On afrontal chest radiograph, the recess isseen as a vertically oriented interfacebetween the right lower lobe and theadjacent mediastinum (the medial limitof the recess). Superiorly, the interfaceis seen as a smooth arc with convexityto the left. Disappearance or distortionof part of the interface suggests disease(eg, subcarinal lymphadenopathy). OnCT scans, the recess (Fig 9) merits at-tention because small lesions located inthe recess will often be invisible onchest radiographs (23).
azygos fissureSee fissure.
beaded septum signCT scans.—This sign consists of irregu-lar and nodular thickening of interlobu-lar septa reminiscent of a row of beads(Fig 10). It is frequently seen in lym-phangitic spread of cancer and less of-ten in sarcoidosis (24).
blebAnatomy.—A bleb is a small gas-con-taining space within the visceral pleuraor in the subpleural lung, not larger than1 cm in diameter (25).
CT scans.—A bleb appears as athin-walled cystic air space contiguouswith the pleura. Because the arbitrary(size) distinction between a bleb and
Figure 7
Figure 7: Transverse CT scan shows architec-tural distortion caused by pulmonary fibrosis.
Figure 8
Figure 8: Transverse CT scan shows atelecta-sis of right middle lobe as increased attenuation(arrows) adjacent to right border of heart.
Figure 9
Figure 9: Transverse CT scan shows azygo-esophageal recess (arrows).
Figure 10
Figure 10: Transverse CT scan shows beadedseptum sign (arrows).
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
700 Radiology: Volume 246: Number 3—March 2008

bulla is of little clinical importance, theuse of this term by radiologists is dis-couraged.
bronchiectasisPathology.—Bronchiectasis is irrevers-ible localized or diffuse bronchial dilata-tion, usually resulting from chronic in-fection, proximal airway obstruction, orcongenital bronchial abnormality (26).(See also traction bronchiectasis.)
Radiographs and CT scans.—Mor-phologic criteria on thin-section CTscans include bronchial dilatation withrespect to the accompanying pulmonaryartery (signet ring sign), lack of taperingof bronchi, and identification of bronchiwithin 1 cm of the pleural surface (27)(Fig 11). Bronchiectasis may be classi-fied as cylindric, varicose, or cystic, de-pending on the appearance of the af-fected bronchi. It is often accompaniedby bronchial wall thickening, mucoidimpaction, and small-airways abnormal-ities (27–29). (See also signet ring sign.)
bronchioleAnatomy.—Bronchioles are non–carti-lage-containing airways. Terminal bron-chioles are the most distal of the purelyconducting airways; they give rise to re-spiratory bronchioles, from which thealveoli arise and permit gas exchange.Respiratory bronchioles branch intomultiple alveolar ducts (30).
Radiographs and CT scans.—Bron-chioles are not identifiable in healthyindividuals, because the bronchiolarwalls are too thin (4). In inflammatorysmall-airways disease, however, thick-ened or plugged bronchioles may beseen as a nodular pattern on a chestradiograph or as a tree-in-bud patternon CT scans.
bronchiolectasisPathology.—Bronchiolectasis is definedas dilatation of bronchioles. It is causedby inflammatory airways disease (po-tentially reversible) or, more fre-quently, fibrosis.
CT scans.—When dilated bronchi-oles are filled with exudate and are thickwalled, they are visible as a tree-in-budpattern or as centrilobular nodules(31,32). In traction bronchiolectasis,the dilated bronchioles are seen assmall, cystic, tubular airspaces, associ-ated with CT findings of fibrosis (Fig12). (See also traction bronchiectasisand traction bronchiolectasis, tree-in-bud pattern.)
bronchiolitisPathology.—Bronchiolitis is bronchio-lar inflammation of various causes (33).
CT scans.—This direct sign of bron-chiolar inflammation (eg, infectiouscause) is most often seen as the tree-in-bud pattern, centrilobular nodules, andbronchiolar wall thickening on CT
scans. (See also small-airways disease,tree-in-bud pattern.)
bronchocelePathology.—A bronchocele is bronchialdilatation due to retained secretions(mucoid impaction) usually caused byproximal obstruction, either congenital(eg, bronchial atresia) or acquired (eg,obstructing cancer) (34).
Radiographs and CT scans.—Abronchocele is a tubular or branching Y-or V-shaped structure that may resem-ble a gloved finger (Fig 13). The CTattenuation of the mucus is generallythat of soft tissue but may be modifiedby its composition (eg, high-attenuationmaterial in allergic bronchopulmonaryaspergillosis). In the case of bronchialatresia, the surrounding lung may be ofdecreased attenuation because of re-duced ventilation and, thus, perfusion.
Figure 11
Figure 11: Transverse CT scan shows varicosebronchiectasis.
Figure 12
Figure 12: Transverse CT scan shows bronchi-olectasis within fibrotic lung (arrow).
Figure 13
Figure 13: Coronal CT scan shows bron-chocele (arrow).
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 701

bronchocentricCT scans.—This descriptor is applied todisease that is conspicuously centeredon macroscopic bronchovascular bun-dles (Fig 14). Examples of diseases witha bronchocentric distribution includesarcoidosis (35), Kaposi sarcoma (36),and organizing pneumonia (37).
broncholithPathology.—A broncholith, a calcifiedperibronchial lymph node that erodesinto an adjacent bronchus, is most oftenthe consequence of Histoplasma or tu-berculous infection.
Radiographs and CT scans.—Theimaging appearance is of a small calcificfocus in or immediately adjacent to anairway (Fig 15), most frequently theright middle lobe bronchus. Broncho-liths are readily identified on CT scans(38). Distal obstructive changes may in-clude atelectasis, mucoid impaction,and bronchiectasis.
bullaPathology.—An airspace measuringmore than 1 cm—usually several centi-meters—in diameter, sharply demar-cated by a thin wall that is no greaterthan 1 mm in thickness. A bulla is usu-ally accompanied by emphysematouschanges in the adjacent lung. (See alsobullous emphysema.)
Radiographs and CT scans.—A bullaappears as a rounded focal lucency orarea of decreased attenuation, 1 cm ormore in diameter, bounded by a thinwall (Fig 16). Multiple bullae are oftenpresent and are associated with othersigns of pulmonary emphysema (centri-lobular and paraseptal).
bullous emphysemaPathology.—Bullous emphysema is bul-lous destruction of the lung paren-chyma, usually on a background of para-septal or panacinar emphysema. (Seealso emphysema, bulla.)
cavityRadiographs and CT scans.—A cavity isa gas-filled space, seen as a lucency orlow-attenuation area, within pulmonaryconsolidation, a mass, or a nodule (Fig17). In the case of cavitating consolida-tion, the original consolidation may re-solve and leave only a thin wall. A cavityis usually produced by the expulsion ordrainage of a necrotic part of the lesionvia the bronchial tree. It sometimes con-tains a fluid level. Cavity is not a syn-onym for abscess.
centrilobularAnatomy.—Centrilobular describes theregion of the bronchiolovascular core ofa secondary pulmonary lobule (4,39,40).This term is also used by pathologists todescribe the location of lesions beyondthe terminal bronchiole that center onrespiratory bronchioles or even alveolarducts.
CT scans.–A small dotlike or linearopacity in the center of a normal sec-ondary pulmonary lobule, most obviouswithin 1 cm of a pleural surface, repre-sents the intralobular artery (approxi-mately 1 mm in diameter) (41). Centri-lobular abnormalities include (a) nod-ules, (b) a tree-in-bud pattern indicatingsmall-airways disease, (c) increased vis-
Figure 14
Figure 14: Transverse CT scan shows consoli-dation with bronchocentric distribution.
Figure 15
Figure 15: Transverse CT scan shows a bron-cholith (arrows).
Figure 16
Figure 16: Coronal CT scan shows large bullain left lower lung zone.
Figure 17
Figure 17: Transverse CT scan shows cavitat-ing mass in right upper lobe.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
702 Radiology: Volume 246: Number 3—March 2008

ibility of centrilobular structures due tothickening or infiltration of the adjacentinterstitium, or (d) abnormal areas oflow attenuation caused by centrilobularemphysema (4). (See also lobular corestructures.)
centrilobular emphysemaPathology.—Centrilobular emphysemais characterized by destroyed centri-lobular alveolar walls and enlargementof respiratory bronchioles and associ-ated alveoli (42,43). This is the com-monest form of emphysema in cigarettesmokers.
CT scans.—CT findings are centri-lobular areas of decreased attenuation,usually without visible walls, of nonuni-form distribution and predominantly lo-cated in upper lung zones (44) (Fig 18).The term centriacinar emphysema issynonymous. (See also emphysema.)
collapseSee atelectasis.
consolidationPathology.—Consolidation refers to anexudate or other product of disease thatreplaces alveolar air, rendering the lungsolid (as in infective pneumonia).
Radiographs and CT scans.—Con-solidation appears as a homogeneousincrease in pulmonary parenchymal at-tenuation that obscures the margins ofvessels and airway walls (45) (Fig 19).An air bronchogram may be present.The attenuation characteristics of con-solidated lung are only rarely helpfulin differential diagnosis (eg, decreasedattenuation in lipoid pneumonia [46]and increased in amiodarone toxicity[47]).
crazy-paving patternCT scans.—This pattern appears asthickened interlobular septa and in-tralobular lines superimposed on abackground of ground-glass opacity (Fig20), resembling irregularly shaped pav-ing stones. The crazy-paving pattern isoften sharply demarcated from morenormal lung and may have a geographicoutline. It was originally reported in pa-tients with alveolar proteinosis (48) andis also encountered in other diffuse lungdiseases (49) that affect both the inter-stitial and airspace compartments, suchas lipoid pneumonia (50).
cryptogenic organizing pneumonia, or COPSee organizing pneumonia.
cystPathology.—A cyst is any round circum-scribed space that is surrounded by anepithelial or fibrous wall of variablethickness (51).
Radiographs and CT scans.—A cystappears as a round parenchymal lu-cency or low-attenuating area with awell-defined interface with normal lung.Cysts have variable wall thickness butare usually thin-walled (�2 mm) andoccur without associated pulmonaryemphysema (Fig 21). Cysts in the lungusually contain air but occasionally con-tain fluid or solid material. The term isoften used to describe enlarged thin-walled airspaces in patients with lym-phangioleiomyomatosis (52) or Langer-hans cell histiocytosis (53); thicker-walled honeycomb cysts are seen inpatients with end-stage fibrosis (54).(See also bleb, bulla, honeycombing,pneumatocele.)
Figure 18
Figure 18: Transverse CT scan shows centri-lobular emphysema.
Figure 19
Figure 19: Transverse CT scan shows multifo-cal consolidation.
Figure 20
Figure 20: Transverse CT scan shows crazy-paving pattern.
Figure 21
Figure 21: Coronal CT scan shows a cyst.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 703

desquamative interstitial pneumonia, or DIPPathology.—Histologically, DIP is char-acterized by the widespread accumula-tion of an excess of macrophages in thedistal airspaces. The macrophages areuniformly distributed, unlike in respira-tory bronchiolitis–interstitial lung dis-ease, in which the disease is conspicu-ously bronchiolocentric. Interstitial in-volvement is minimal. Most cases of DIPare related to cigarette smoking, but afew are idiopathic or associated withrare inborn errors of metabolism (5).
Radiographs and CT scans.—Ground-glass opacity is the dominantabnormality and tends to have a basaland peripheral distribution (Fig 22). Mi-crocystic or honeycomb changes in thearea of ground-glass opacity are seen insome cases (55).
diffuse alveolar damage, or DADSee acute interstitial pneumonia.
emphysemaPathology.—Emphysema is character-ized by permanently enlarged airspacesdistal to the terminal bronchiole withdestruction of alveolar walls (42,43).Absence of “obvious fibrosis” was his-torically regarded as an additional crite-rion (42), but the validity of that crite-rion has been questioned because someinterstitial fibrosis may be present inemphysema secondary to cigarettesmoking (56,57). Emphysema is usuallyclassified in terms of the part of theacinus predominantly affected: proxi-mal (centriacinar, more commonlytermed centrilobular, emphysema), dis-
tal (paraseptal emphysema), or wholeacinus (panacinar or, less commonly,panlobular emphysema).
CT scans.—The CT appearance ofemphysema consists of focal areas orregions of low attenuation, usually with-out visible walls (58). In the case ofpanacinar emphysema, decreased at-tenuation is more diffuse. (See also bul-lous emphysema, centrilobular emphy-sema, panacinar emphysema, parasep-tal emphysema.)
fissureAnatomy.—A fissure is the infolding ofvisceral pleura that separates one lobeor part of a lobe from another; thus, theinterlobar fissures are produced by twolayers of visceral pleura. Supernumer-ary fissures usually separate segmentsrather than lobes. The azygos fissure,unlike the other fissures, is formed bytwo layers each of visceral and parietalpleura. All fissures (apart from the azy-gos fissure) may be incomplete.
Radiographs and CT scans.—Fis-sures appear as linear opacities, nor-mally 1 mm or less in thickness, thatcorrespond in position and extent to theanatomic fissural separation of pulmo-nary lobes or segments. Qualifiers in-clude minor, major, horizontal, oblique,accessory, anomalous, azygos, and infe-rior accessory.
folded lungSee rounded atelectasis.
fungus ballSee mycetoma.
gas trappingSee air trapping.
ground-glass noduleSee nodule.
ground-glass opacityRadiographs and CT scans.—On chestradiographs, ground-glass opacity ap-pears as an area of hazy increased lungopacity, usually extensive, within whichmargins of pulmonary vessels may beindistinct. On CT scans, it appears ashazy increased opacity of lung, withpreservation of bronchial and vascularmargins (Fig 23). It is caused by partialfilling of airspaces, interstitial thicken-ing (due to fluid, cells, and/or fibrosis),partial collapse of alveoli, increasedcapillary blood volume, or a combina-tion of these, the common factor beingthe partial displacement of air (59,60).Ground-glass opacity is less opaquethan consolidation, in which broncho-vascular margins are obscured. (Seealso consolidation.)
Figure 22
Figure 22: Transverse CT scan in a patient withdesquamative interstitial pneumonia.
Figure 23
Figure 23: Transverse CT scan shows ground-glass opacity.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
704 Radiology: Volume 246: Number 3—March 2008

halo signCT scans.—The halo sign is a CT findingof ground-glass opacity surrounding anodule or mass (Fig 24). It was firstdescribed as a sign of hemorrhagearound foci of invasive aspergillosis(61). The halo sign is nonspecific andmay also be caused by hemorrhage as-sociated with other types of nodules(62) or by local pulmonary infiltrationby neoplasm (eg, adenocarcinoma).(See also reversed halo sign.)
hilumAnatomy.—Hilum is a generic term thatdescribes the indentation in the surfaceof an organ, where vessels and nervesconnect with the organ. It is the site onthe medial aspect of the lung where thevessels and bronchi enter and leave thelung.
Radiographs and CT scans.—A hi-lum appears as a composite opacity atthe root of each lung produced by bron-chi, arteries, veins, lymph nodes,nerves, and other tissue. The terms hi-lum (singular) and hila (plural) are pre-ferred to hilus and hili respectively; theadjectival form is hilar.
honeycombingPathology.—Honeycombing representsdestroyed and fibrotic lung tissue con-taining numerous cystic airspaces withthick fibrous walls, representing the latestage of various lung diseases, withcomplete loss of acinar architecture.The cysts range in size from a few milli-meters to several centimeters in diame-ter, have variable wall thickness, andare lined by metaplastic bronchiolar ep-ithelium (51).
Radiographs and CT scans.—Onchest radiographs, honeycombing ap-pears as closely approximated ringshadows, typically 3–10 mm in diameterwith walls 1–3 mm in thickness, thatresemble a honeycomb; the finding im-plies end-stage lung disease. On CTscans, the appearance is of clusteredcystic air spaces, typically of compara-ble diameters on the order of 3–10 mmbut occasionally as large as 2.5 cm (Fig25). Honeycombing is usually subpleu-ral and is characterized by well-definedwalls (54). It is a CT feature of estab-lished pulmonary fibrosis (5). Becausehoneycombing is often considered spe-cific for pulmonary fibrosis and is animportant criterion in the diagnosis ofusual interstitial pneumonia (63), theterm should be used with care, as it maydirectly impact patient care.
idiopathic pulmonary fibrosisPathology.—Idiopathic pulmonary fi-brosis is a specific form of chronic fibro-sing interstitial pneumonia of unknowncause and is characterized by a histo-logic pattern of usual interstitial pneu-monia (5,64).
Radiographs and CT scans.—Thetypical imaging findings are reticularopacities and honeycombing, with apredominantly peripheral and basal dis-tribution (Fig 26). Ground-glass opac-ity, if present, is less extensive than re-ticular and honeycombing patterns. Thetypical radiologic findings (65,66) arealso encountered in usual interstitialpneumonia secondary to specific causes,such as asbestos-induced pulmonary fi-brosis (asbestosis), and the diagnosis isusually one of exclusion. (See also usualinterstitial pneumonia.)
Figure 24
Figure 24: Transverse CT scan shows severalnodules exhibiting the halo sign (arrows).
Figure 25
Figure 25: Transverse CT scan showshoneycombing.
Figure 26
Figure 26: Coronal CT scan shows reticularopacities and honeycombing in the lower zones,typical of idiopathic pulmonary fibrosis.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 705

infarctionPathology.—Infarction is a process thatmay result in ischemic necrosis, usuallythe consequence of vascular compro-mise such as occlusion of a feeding pul-monary artery by an embolus (venousinfarction is rare but recognized). Ne-crosis is relatively uncommon becausetissue viability is maintained by thebronchial arterial blood supply. Pulmo-nary infarction may be secondary to avasculitis (eg, Wegener granulomato-sis).
Radiographs and CT scans.—A pul-monary infarct is typically triangular ordome-shaped, with the base abuttingthe pleura and the apex directed towardthe hilum (Fig 27). The opacity repre-sents local hemorrhage with or withoutcentral tissue necrosis (67,68).
infiltrateRadiographs and CT scans.—Formerlyused as a term to describe a region ofpulmonary opacification caused by air-space or interstitial disease seen on ra-diographs and CT scans. Infiltrate re-mains controversial because it meansdifferent things to different people (69).The term is no longer recommended,and has been largely replaced by otherdescriptors. The term opacity, with rel-evant qualifiers, is preferred.
interlobular septal thickeningRadiographs and CT scans.—This find-ing is seen on chest radiographs as thinlinear opacities at right angles to and incontact with the lateral pleural surfacesnear the lung bases (Kerley B lines); it isseen most frequently in lymphangiticspread of cancer or pulmonary edema.Kerley A lines are predominantly situ-ated in the upper lobes, are 2–6 cmlong, and can be seen as fine lines radi-ally oriented toward the hila. In recentyears, the anatomically descriptiveterms septal lines and septal thickeninghave gained favor over Kerley lines. OnCT scans, disease affecting one of thecomponents of the septa (see interlobu-lar septum) may be responsible forthickening and so render septa visible.On thin-section CT scans, septal thick-ening may be smooth or nodular (70)(Fig 28), which may help refine the dif-ferential diagnosis. (See also interlobu-lar septum, beaded septum.)
interlobular septumAnatomy.—Interlobular septa are sheet-like structures 10–20-mm long thatform the borders of lobules; they aremore or less perpendicular to the pleurain the periphery. Interlobular septa arecomposed of connective tissue and con-tain lymphatic vessels and pulmonaryvenules.
Radiographs and CT scans.—Inter-lobular septa appear as thin linear opac-ities between lobules (Fig 29); thesesepta are to be distinguished from cen-trilobular structures. They are not usu-ally seen in the healthy lung (normalsepta are approximately 0.1 mm thick)but are clearly visible when thickened(eg, by pulmonary edema). (See alsointerlobular septal thickening, lobule.)
Figure 27
Figure 27: Transverse CT scan shows pulmo-nary infarction.
Figure 28
Figure 28: Transverse CT scan shows interlob-ular septal thickening and pleural effusions.
Figure 29
Figure 29: Transverse CT scan shows interlob-ular septum (arrow) in a healthy individual.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
706 Radiology: Volume 246: Number 3—March 2008

interstitial emphysemaPathology.—Interstitial emphysema ischaracterized by air dissecting withinthe interstitium of the lung, typically inthe peribronchovascular sheaths, inter-lobular septa, and visceral pleura. It ismost commonly seen in neonates re-ceiving mechanical ventilation.
Radiographs and CT scans.—Inter-stitial emphysema is rarely recognizedradiographically in adults and is infre-quently seen on CT scans (Fig 30). Itappears as perivascular lucent or low-attenuating halos and small cysts(71,72).
interstitiumAnatomy.—The interstitium consists ofa continuum of connective tissuethroughout the lung comprising threesubdivisions: (a) the bronchovascular(axial) interstitium, surrounding andsupporting the bronchi, arteries, andveins from the hilum to the level of therespiratory bronchiole; (b) the paren-chymal (acinar) interstitium, situatedbetween alveolar and capillary base-ment membranes; and (c) the subpleu-ral connective tissue contiguous withthe interlobular septa (73).
intralobular linesCT scans.—Intralobular lines are visibleas fine linear opacities in a lobule whenthe intralobular interstitial tissue is ab-normally thickened (Fig 31). When nu-merous, they may appear as a fine retic-ular pattern. Intralobular lines may beseen in various conditions, including in-terstitial fibrosis and alveolar proteino-sis (41).
juxtaphrenic peakRadiographs and CT scans.—A juxta-phrenic peak is a small triangular opac-ity based at the apex of the dome of ahemidiaphragm, associated with upperlobe volume loss of any cause (eg, po-stirradiation fibrosis or upper lobec-tomy) (74). It is most readily appreci-ated on a frontal chest radiograph (Fig32). The peak is caused by upward re-traction of the inferior accessory fissure(75) or an intrapulmonary septum associ-ated with the pulmonary ligament (76).
linear atelectasisRadiographs and CT scans.—Linear at-electasis is a focal area of subsegmentalatelectasis with a linear configuration,almost always extending to the pleura(74). It is commonly horizontal butsometimes oblique or vertical. Thethickness of the atelectasis may rangefrom a few millimeters to more than 1cm (Fig 33). Linear atelectasis is alsoreferred to as discoid or platelike atel-ectasis. (See also atelectasis.)
lobeAnatomy.—The lobe is the principal di-vision of the lungs (normally, threelobes on the right and two on the left);each lobe is enveloped by visceral pleura,except at the lung root (hilum) and whenan interlobar fissure is incomplete.
Figure 30
Figure 30: Transverse CT scan shows intersti-tial emphysema (arrow).
Figure 31
Figure 31: Transverse CT scan shows ln-tralobular lines.
Figure 32
Figure 32: Chest radiograph shows juxta-phrenic peak of the right hemidiaphragm.
Figure 33
Figure 33: Chest radiograph shows basal lin-ear atelectasis.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 707

lobular core structuresAnatomy.—Lobular core structures arethe central structures in secondary pul-monary lobules and consist of a centri-lobular artery and bronchiole (40).
CT scans.—The pulmonary arteryand its immediate branches are visiblein the center of a secondary lobule onthin-section CT scans, particularly ifthickened (eg, by pulmonary edema)(Fig 34). These arteries measure ap-proximately 0.5–1.0 mm in diameter.However, the normal bronchiole in thecenter of the secondary pulmonary lob-ule cannot be seen on thin-section CTscans because of the thinness of its wall(approximately 0.15 mm) (4,41). (Seealso centrilobular, lobule.)
lobuleAnatomy.—The lobule is the smallestunit of lung surrounded by connective-tissue septa, as defined by Miller (78)and Heitzman et al (40). The lobule isalso referred to as the secondary pul-monary lobule; it contains a variablenumber of acini, is irregularly polyhe-dral in shape, and varies in size from 1.0to 2.5 cm in diameter. The centrilobularstructures, or core structures, includebronchioles and their accompanyingpulmonary arterioles and lymphatic ves-sels. The connective-tissue septa sur-rounding the pulmonary lobule—the in-terlobular septa, which contain veinsand lymphatic vessels—are best devel-oped in the periphery in the anterior,lateral, and juxtamediastinal regions ofthe upper and middle lobes.
CT scans.—On thin-section CTscans, the three basic components ofthe lobule—the interlobular septa andseptal structures, the central lobular re-gion (centrilobular structures), and thelobular parenchyma—can be identified,particularly in disease states. Peripherallobules are more uniform in appearanceand pyramidal in shape than are centrallobules (4) (Fig 35). (See also interlobu-lar septa, lobular core structures.)
lymphadenopathyPathology.—By common usage, theterm lymphadenopathy is usually re-stricted to enlargement, due to anycause, of the lymph nodes. Synonymsinclude lymph node enlargement (pre-ferred) and adenopathy.
CT scans.—There is a wide range inthe size of normal lymph nodes. Medias-tinal and hilar lymph nodes range in sizefrom sub-CT resolution to 12 mm.Somewhat arbitrary thresholds for theupper limit of normal of 1 cm in short-axis diameter for mediastinal nodes(79) and 3 mm for most hilar nodes (80)have been reported, but size criteria donot allow reliable differentiation be-tween healthy and diseased lymphnodes (Fig 36).
lymphoid interstitial pneumonia, or LIPPathology.—LIP is a rare disease char-acterized by diffuse pulmonary lym-phoid proliferation with predominantinterstitial involvement. It is included inthe spectrum of interstitial pneumoniasand is distinct from diffuse lymphomasof the lung. Features include diffuse hy-perplasia of bronchus-associated lym-phoid tissue and diffuse polyclonal lym-
Figure 34
Figure 34: Transverse CT scan shows lobularcore structure (arrow).
Figure 35
Figure 35: CT scan of resected lung showslobules.
Figure 36
Figure 36: Transverse CT scan shows lymph-adenopathy (enlarged mediastinal lymph nodes).
Figure 37
Figure 37: Transverse CT scan shows ground-glass opacities and perivascular cysts in a patientwith lymphoid interstitial pneumonia.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
708 Radiology: Volume 246: Number 3—March 2008

phoid cell infiltrates surrounding theairways and expanding the lung intersti-tium. LIP is usually associated with au-toimmune diseases or human immuno-deficiency virus infection (5,81).
CT scans.—Ground-glass opacity isthe dominant abnormality, and thin-walled perivascular cysts may bepresent (Fig 37). Lung nodules, a retic-ular pattern, interlobular septal andbronchovascular thickening, and wide-spread consolidation may also occur(82,83).
massRadiographs and CT scans.—A mass isany pulmonary, pleural, or mediastinallesion seen on chest radiographs as anopacity greater than 3 cm in diameter(without regard to contour, border, ordensity characteristics). Mass usuallyimplies a solid or partly solid opacity.CT allows more exact evaluation of size,location, attenuation, and other fea-tures. (See also nodule.)
mediastinal compartmentsAnatomy.—Nominal anatomic com-partments of the mediastinum includethe anterior, middle, posterior, and (insome schemes) superior compart-ments. The anterior compartment isbounded anteriorly by the sternum andposteriorly by the anterior surface ofthe pericardium, the ascending aorta,and the brachiocephalic vessels. Themiddle compartment is bounded by theposterior margin of the anterior divisionand the anterior margin of the posteriordivision. The posterior compartment isbounded anteriorly by the posteriormargins of the pericardium and greatvessels and posteriorly by the thoracicvertebral bodies. In the four-compart-ment model, the superior compartmentis defined as the compartment abovethe plane between the sternal angle tothe T4-5 intervertebral disk or, moresimply, above the aortic arch (84,85).Exact anatomic boundaries between thecompartments do not exist, and thereare no barriers (other than the pericar-dium) to prevent the spread of diseasebetween compartments. Other classifi-cations exist, but the three- and four-
compartment models are the most com-monly used.
micronoduleCT scans.—A micronodule is a discrete,small, round, focal opacity. A variety ofdiameters have been used in the past todefine a micronodule; for example, adiameter of no greater than 7 mm (86).Use of the term is most often limited tonodules with a diameter of less than 5mm (87) or less than 3 mm (88). It isrecommended that the term be re-served for opacities less than 3 mm indiameter. (See also nodule, miliary pat-tern.)
miliary patternRadiographs and CT scans.—On chestradiographs, the miliary pattern con-sists of profuse tiny, discrete, roundedpulmonary opacities (�3 mm in diame-ter) that are generally uniform in sizeand diffusely distributed throughout thelungs (Fig 38). This pattern is a manifes-tation of hematogenous spread of tuber-culosis and metastatic disease. Thin-section CT scans show widespread, ran-domly distributed micronodules.
mosaic attenuation patternCT scans.—This pattern appears aspatchwork of regions of differing atten-uation that may represent (a) patchyinterstitial disease, (b) obliterative small-airways disease (Fig 39), or (c) occlu-sive vascular disease (89). Mosaic at-tenuation pattern is a more inclusiveterm than the original terms mosaic oli-gemia and perfusion (90). Air trappingsecondary to bronchial or bronchiolarobstruction may produce focal zones ofdecreased attenuation, an appearancethat can be enhanced by using expira-tory CT (91,92). The mosaic attenua-tion pattern can also be produced byinterstitial lung disease characterized byground-glass opacity; in this situation,areas of higher attenuation representthe interstitial process and areas oflower attenuation represent the normallung.
mosaic oligemia, perfusionSee mosaic attenuation pattern.
Figure 38
Figure 38: Magnified chest radiograph showsmiliary pattern.
Figure 39
Figure 39: Transverse CT scan shows mosaicattenuation pattern caused by obliterative small-airways disease.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 709

mycetomaPathology.—A mycetoma is a discretemass of intertwined hyphae, usually ofan Aspergillus species, matted togetherby mucus, fibrin, and cellular debris col-onizing a cavity, usually from prior fi-brocavitary disease (eg, tuberculosis orsarcoidosis).
Radiographs and CT scans.—A my-cetoma may move to a dependent loca-tion when the patient changes positionand may show an air crescent sign (Fig40). CT scans may show a spongelikepattern and foci of calcification in themycetoma (93). A synonym is fungusball. (See also air crescent.)
nodular patternRadiographs and CT scans.—A nodularpattern is characterized on chest radio-graphs by the presence of innumerablesmall rounded opacities that are dis-crete and range in diameter from 2 to10 mm (Fig 41). The distribution iswidespread but not necessarily uni-form. On CT scans, the pattern may beclassified as one of three anatomic dis-tributions: centrilobular, lymphatic, orrandom. (See also nodule.)
noduleRadiographs and CT scans.—The chestradiographic appearance of a nodule isa rounded opacity, well or poorly de-fined, measuring up to 3 cm in diame-ter. (a) Acinar nodules are round orovoid poorly defined pulmonary opaci-ties approximately 5–8 mm in diame-ter, presumed to represent an anatomicacinus rendered opaque by consolida-tion. This classification is used only inthe presence of numerous such opaci-ties. (b) A pseudonodule mimics a pul-monary nodule; it represents, for exam-ple, a rib fracture, a skin lesion, a deviceon the surface of the patient, anatomicvariants, or composite areas of in-creased opacity (94).
On CT scans, a nodule appears as arounded or irregular opacity, well orpoorly defined, measuring up to 3 cm indiameter (Fig 42). (a) Centrilobularnodules appear separated by severalmillimeters from the pleural surfaces,fissures, and interlobular septa. Theymay be of soft-tissue or ground-glassattenuation. Ranging in size from a fewmillimeters to a centimeter, centrilobu-lar nodules are usually ill-defined (4).(b) A micronodule is less than 3 mm indiameter (see also micronodule). (c) Aground-glass nodule (synonym, non-solid nodule) manifests as hazy in-creased attenuation in the lung thatdoes not obliterate the bronchial andvascular margins. (d) A solid nodule hashomogenous soft-tissue attenuation.(e) A part-solid nodule (synonym, semi-solid nodule) consists of both ground-glass and solid soft-tissue attenuationcomponents. (See also mass.)
nonspecific interstitial pneumonia, or NSIPPathology.—NSIP is characterized by ahistologic pattern of uniform interstitialinvolvement by varying degrees ofchronic inflammation or fibrosis. NSIPmay be idiopathic or seen in other set-tings, including collagen vascular dis-ease, hypersensitivity pneumonitis,drug-induced lung disease, infection,and immunodeficiency (including hu-man immunodeficiency virus infection)(5).
CT scans.—NSIP has variable thin-
Figure 40
Figure 40: Coronal CT scan shows mycetomasin both lungs.
Figure 41
Figure 41: Magnified chest radiograph showsa nodular pattern.
Figure 42
Figure 42: Transverse CT scan shows irregularnodule in left lower lobe.
Figure 43
Figure 43: Transverse CT scan shows nonspe-cific interstitial pneumonia.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
710 Radiology: Volume 246: Number 3—March 2008

section CT appearances: The most fre-quent is ground-glass opacities with re-ticulation, traction bronchiectasis orbronchiolectasis, and little or no honey-combing (Fig 43). The distribution isusually basal and subpleural (95).
oligemiaPathophysiology.—Oligemia is a reduc-tion in pulmonary blood volume. Mostfrequently, this reduction is regional,but occasionally it is generalized. Re-gional oligemia is usually associated withreduced blood flow in the oligemic area.
Radiographs and CT scans.—Olige-mia appears as a regional or widespreaddecrease in the size and number of identi-fiable pulmonary vessels (Fig 44), whichis indicative of less than normal bloodflow. (See also mosaic attenuation pattern,pulmonary blood flow redistribution.)
opacityRadiographs and CT scans.—Opacityrefers to any area that preferentially at-tenuates the x-ray beam and thereforeappears more opaque than the sur-rounding area. It is a nonspecific termthat does not indicate the size or patho-logic nature of the abnormality. (Seealso parenchymal opacification, ground-glass opacity.)
organizing pneumoniaPathology.—Organizing pneumonia man-ifests as a histologic pattern characterizedby loose plugs of connective tissue in theairspaces and distal airways. Interstitialinflammation and fibrosis are minimal orabsent. Cryptogenic organizing pneumo-nia, or COP, is a distinctive clinical disor-der among the idiopathic interstitialpneumonias (5), but the histologic pat-tern of organizing pneumonia is encoun-tered in many different situations, includ-ing pulmonary infection, hypersensitivitypneumonitis, and collagen vascular dis-eases.
Radiographs and CT scans.—Air-space consolidation is the cardinal fea-ture of organizing pneumonia on chestradiographs and CT scans. In COP, thedistribution is typically subpleural andbasal (Fig 45) and sometimes bron-chocentric (96). Other manifestations oforganizing pneumonia include ground-glass opacity, tree-in-bud pattern, andnodular opacities (37).
panacinar emphysemaPathology.—Panacinar emphysema in-volves all portions of the acinus and sec-ondary pulmonary lobule more or lessuniformly (42). It predominates in thelower lobes and is the form of emphy-sema associated with �1-antitrypsin de-ficiency.
CT scans.—Panacinar emphysemamanifests as a generalized decrease of thelung parenchyma with a decrease in thecaliber of blood vessels in the affectedlung (97,98) (Fig 46). Severe panacinaremphysema may coexist and merge withsevere centrilobular emphysema. The ap-pearance of featureless decreased attenu-ation may be indistinguishable from se-vere constrictive obliterative bronchiolitis(99). The term panlobular emphysema issynonymous. (See also emphysema.)
Figure 44
Figure 44: Transverse CT scan shows oligemia(arrows) in left lung.
Figure 45
Figure 45: Transverse CT scan shows crypto-genic organizing pneumonia with subpleural andbasal distribution.
Figure 46
Figure 46: Transverse CT scan shows panaci-nar emphysema.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 711

paraseptal emphysemaPathology.—Paraseptal emphysema ischaracterized by predominant involve-ment of the distal alveoli and their ductsand sacs. It is characteristically boundedby any pleural surface and the interlobu-lar septa (42,43).
CT scans.—This emphysema ischaracterized by subpleural and peri-bronchovascular regions of low attenua-tion separated by intact interlobularsepta (Fig 47), sometimes associatedwith bullae. The term distal acinar em-physema is synonymous. (See also em-physema.)
parenchymaAnatomy.—Parenchyma refers to thegas-exchanging part of the lung, consist-ing of the alveoli and their capillaries.
Radiographs and CT scans.—Theportion of the lung exclusive of visiblepulmonary vessels and airways.
parenchymal bandRadiographs and CT scans.—A paren-chymal band is a linear opacity, usually1–3 mm thick and up to 5 cm long thatusually extends to the visceral pleura(which is often thickened and may beretracted at the site of contact) (Fig 48).It reflects pleuroparenchymal fibrosisand is usually associated with distortionof the lung architecture. Parenchymalbands are most frequently encounteredin individuals who have been exposed toasbestos (100,101).
parenchymal opacificationRadiographs and CT scans.—Parenchy-mal opacification of the lungs may ormay not obscure the margins of vesselsand airway walls (45). Consolidation in-dicates that definition of these margins(excepting air bronchograms) is lostwithin the dense opacification, whereasground-glass opacity indicates a smallerincrease in attenuation, in which thedefinition of underlying structures ispreserved (59). The more specificterms consolidation and ground-glassopacity are preferred. (See also consol-idation, ground-glass opacity.)
peribronchovascular interstitiumAnatomy.—The peribronchovascular in-terstitium is a connective-tissue sheaththat encloses the bronchi, pulmonaryarteries, and lymphatic vessels. It ex-tends from the hila to the lung periph-ery.
perilobular distributionAnatomy.—The perilobular region com-prises the structures bordering the pe-riphery of the secondary pulmonary lob-ule.
CT scans.—This pattern is charac-terized by distribution along the struc-tures that border the pulmonary lobules(ie, interlobular septa, visceral pleura,and vessels) (102). The term is mostfrequently used in the context of dis-eases (eg, perilobular organizing pneu-monia) that are distributed mainlyaround the inner surface of the second-ary pulmonary lobule (103) (Fig 49).This may resemble indistinct thickeningof the interlobular septa.
Figure 47
Figure 47: Transverse CT scan shows para-septal emphysema.
Figure 48
Figure 48: Transverse CT scan shows paren-chymal bands (arrows).
Figure 49
Figure 49: Transverse CT scan shows organiz-ing pneumonia in a perilobular distribution(arrows).
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
712 Radiology: Volume 246: Number 3—March 2008

perilymphatic distributionAnatomy.—This pattern is character-ized by distribution along or adjacent tothe lymphatic vessels in the lung. Theroutes of lymphatics are found alongbronchovascular bundles, in the inter-lobular septa, around larger pulmonaryveins, and in the pleura; alveoli do nothave lymphatics.
CT scans.—Abnormalities along thepathway of the pulmonary lymphatics—that is, in the perihilar, peribronchovas-cular, and centrilobular interstitium, aswell as in the interlobular septa and sub-pleural locations—have a perilymphaticdistribution (104). A perilymphatic dis-tribution typically seen in sarcoidosis(Fig 50) and lymphangitic spread of can-cer.
platelike atelectasisSee linear atelectasis.
pleural plaquePathology.—A pleural plaque is a fibro-hyaline, relatively acellular lesion aris-ing predominantly on the parietal pleu-ral surface, particularly on the dia-phragm and underneath ribs (105).Pleural plaques are almost invariablythe consequence of previous (at least 15years earlier) asbestos exposure.
Radiographs and CT scans.—Pleu-ral plaques are well-demarcated areasof pleural thickening, seen as elevatedflat or nodular lesions that often containcalcification (Fig 51). Plaques are ofvariable thickness, range from less than1 to approximately 5 cm in diameter,and are more easily identified on CTscans than on chest radiographs (106).An en face plaque may simulate a pul-monary nodule on chest radiographs.(See also pseudoplaque.)
pneumatocelePathology.—A pneumatocele is a thin-walled, gas-filled space in the lung. It ismost frequently caused by acute pneu-monia, trauma, or aspiration of hydro-carbon fluid and is usually transient.The mechanism is believed to be a com-bination of parenchymal necrosis andcheck-valve airway obstruction (107).
Radiographs and CT scans.—Apneumatocele appears as an approxi-mately round, thin-walled airspace inthe lung (Fig 52).
pneumomediastinumPathology.—Pneumomediastinum is thepresence of gas in mediastinal tissueoutside the esophagus and tracheo-bronchial tree. It may be caused by
Figure 50
Figure 50: Transverse CT scan shows sarcoid-osis with a perilymphatic distribution.
Figure 51
Figure 51: Transverse CT scan shows pleuralplaque (arrow) anteriorly in right hemithorax.
Figure 52
Figure 52: Chest radiograph shows a pneu-matocele (arrows).
Figure 53
Figure 53: Magnified chest radiograph showspneumomediastinum.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 713

spontaneous alveolar rupture, with sub-sequent tracking of air along the bron-chovascular interstitium into the medi-astinum. Pneumomediastinum is partic-ularly associated with a history ofasthma, severe coughing, or assistedventilation.
Radiographs and CT scans.— Pneu-momediastinum appears as lucentstreaks on chest radiographs, mostlyvertically oriented (Fig 53). Some ofthese streaks may outline vessels andmain bronchi. (See also pneumoperi-cardium.)
pneumoniaPathology.—Pneumonia is inflamma-tion of the airspaces and/or interstitium(eg, due to infection, as in bacterialpneumonia). Infective pneumonia ischaracterized by exudate resulting inconsolidation. The term is also used torefer to a number of noninfectious dis-orders of the lung parenchyma charac-terized by varying degrees of inflamma-tion and fibrosis (eg, idiopathic intersti-tial pneumonias) (5).
pneumopericardiumPathology.—Pneumopericardium is thepresence of gas in the pericardial space.It usually has an iatrogenic, often surgi-cal, origin in adults.
Radiographs and CT scans.—Pneu-mopericardium is usually distinguish-
able from pneumomediastinum becausethe lucency (low attenuation) caused byair does not extend outside the pericar-dial sac (Fig 54). (See also pneumome-diastinum.)
pneumothorax and tension pneumothorax
Pathophysiology.—Pneumothorax re-fers to the presence of gas in the pleuralspace. Qualifiers include spontaneous,traumatic, diagnostic, and tension. Ten-sion pneumothorax is the accumulationof intrapleural gas under pressure. Inthis situation, the ipsilateral lung will, ifnormal, collapse completely; however,a less than normally compliant lung mayremain partially inflated.
Radiographs and CT scans.—Onchest radiographs, a visceral pleuraledge is visible (Fig 55) unless the pneu-mothorax is very small or the pleuraledge is not tangential to the x-ray beam.Tension pneumothorax may be associ-ated with considerable shift of the me-diastinum and/or depression of thehemidiaphragm. Some shift can occurwithout tension because the pleuralpressure in the presence of pneumo-thorax becomes atmospheric, whilethe pleural pressure in the contralat-eral hemithorax remains negative.
progressive massive fibrosisPathology.—This condition is caused byslow-growing conglomeration of dustparticles and collagen deposition in indi-viduals (mostly coal workers) heavilyexposed to inorganic dust (108).
Radiographs and CT scans.—Pro-gressive massive fibrosis manifests asmasslike lesions, usually bilateral and inthe upper lobes (Fig 56). Backgroundnodular opacities reflect accompanyingpneumoconiosis, with or without em-physematous destruction adjacent tothe massive fibrosis (109). Lesions similarto progressive massive fibrosis some-times occur in other conditions, such assarcoidosis and talcosis (109,110).
Figure 54
Figure 54: Chest radiograph showspneumopericardium.
Figure 55
Figure 55: Chest radiograph showspneumothorax.
Figure 56
Figure 56: Chest radiograph shows bilateralprogressive massive fibrosis.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
714 Radiology: Volume 246: Number 3—March 2008

pseudocavityCT scans.—A pseudocavity appears asan oval or round area of low attenuationin lung nodules, masses, or areas of con-solidation that represent spared paren-chyma, normal or ectatic bronchi, orfocal emphysema rather than cavita-tion. These pseudocavities usually mea-sure less than 1 cm in diameter. Theyhave been described in patients withadenocarcinoma (Fig 57), bronchioloal-veolar carcinoma (111), and benignconditions such as infectious pneumo-nia.
pseudoplaqueCT scans.—A pseudoplaque is a pulmo-nary opacity contiguous with the vis-ceral pleura formed by coalescent smallnodules. It simulates the appearance ofa pleural plaque. This entity is encoun-tered most commonly in sarcoidosis(Fig 58), silicosis, and coal-worker’spneumoconiosis (86).
pulmonary blood flow redistributionPathophysiology.—Pulmonary blood flowredistribution refers to any departurefrom the normal distribution of blood flowin the lungs that is caused by an increasein pulmonary vascular resistance else-where in the pulmonary vascular bed.
Radiographs and CT scans.—Pul-monary blood flow redistribution is indi-cated by a decrease in the size and/ornumber of visible pulmonary vessels inone or more lung regions (Fig 59), witha corresponding increase in numberand/or size of pulmonary vessels inother parts of the lung. Upper lobeblood diversion in patients with mitralvalve disease is the archetypal exampleof redistribution (112,113).
respiratory bronchiolitis–interstitial lungdisease, or RB-ILDPathology.—RB-ILD is a smoking-re-lated disease characterized by inflam-mation (predominantly by macro-phages) of the respiratory bronchiolesand peribronchiolar alveoli (5), some-times with elements of or overlap withnonspecific and desquamative intersti-tial pneumonias (114).
CT scans.—RB-ILD typically mani-fests as extensive centrilobular micronod-ules and patchy ground-glass opacity cor-responding to macrophage-rich alveolitis(Fig 60), with or without fine fibrosis(115,116). It is often accompanied bybronchial wall thickening and minor cen-trilobular emphysema. Areas of air trap-ping reflect a bronchiolitic component.
Figure 57
Figure 57: Transverse CT scan shows pseudo-cavitation in an adenocarcinoma.
Figure 58
Figure 58: Transverse CT scan shows pseudo-plaques (arrows) in a patient with sarcoidosis.
Figure 59
Figure 59: Chest radiograph shows redistribu-tion of blood flow to upper lung zones.
Figure 60
Figure 60: Transverse CT scan shows centri-lobular micronodules and patchy ground-glassopacity typical of respiratory bronchiolitis–inter-stitial lung disease.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 715

reticular pattern
Radiographs and CT scans.—On chestradiographs, a reticular pattern is a col-lection of innumerable small linearopacities that, by summation, producean appearance resembling a net (syn-onym: reticulation) (Fig 61). This find-ing usually represents interstitial lungdisease. The constituents of a reticularpattern are more clearly seen at thin-section CT, whether they are interlobu-lar septal thickening, intralobular lines,or the cyst walls of honeycombing. (Re-ticular pattern and honeycombingshould not be considered synonymous.See also honeycombing.)
reticulonodular patternRadiographs and CT scans.—A com-bined reticular and nodular pattern, thereticulonodular pattern is usually the re-sult of the summation of points of inter-section of innumerable lines, creatingthe effect on chest radiographs of super-imposed micronodules (Fig 62). The di-mension of the nodules depends on thesize and number of linear or curvilinearelements. (See also reticular pattern.)On CT scans, the pattern appears as aconcurrence of reticular and mi-cronodular patterns. The micronodulescan be situated in the center of the retic-ular elements (eg, centrilobular mi-cronodules) or superimposed on the lin-ear opacities (eg, septal micronodules).
reversed halo signCT scans.—The reversed halo sign is afocal rounded area of ground-glassopacity surrounded by a more or lesscomplete ring of consolidation (Fig 63).A rare sign, it was initially reported tobe specific for cryptogenic organizingpneumonia (117,118) but was subse-quently described in patients with para-coccidioidomycosis (119). Similar to thehalo sign, this sign will probably lose itsspecificity as it is recognized in otherconditions. (See also halo sign.)
right paratracheal stripeAnatomy and radiographs.—The rightparatracheal stripe is a vertical, linear,soft-tissue opacity less than 4 mm wide.It corresponds to the right tracheal wall,contiguous mediastinal tissues, and ad-jacent pleura (Fig 64). The stripe is 3–4cm in height and extends from approxi-mately the level of the medial ends ofthe clavicles to the right tracheobron-chial angle on a frontal chest radiograph(120). It is seen in up to 94% of adultsbut is widened or absent in individualswith abundant mediastinal fat. The com-monest pathologic cause of widening, de-formity, or obliteration of this stripe isparatracheal lymph node enlargement.
Figure 61
Figure 61: Chest radiograph shows reticularpattern.
Figure 62
Figure 62: Chest radiograph shows reticu-lonodular pattern.
Figure 63
Figure 63: Transverse CT scan shows reversedhalo sign (arrow).
Figure 64
Figure 64: Magnified chest radiograph showsparatracheal stripe (arrows).
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
716 Radiology: Volume 246: Number 3—March 2008

rounded atelectasisPathology.—Rounded atelectasis isrounded collapsed lung associated withinvaginated fibrotic pleura and thick-ened and fibrotic interlobular septa.Most frequently, it is the consequenceof an asbestos-induced exudative pleu-ral effusion with resultant pleural scar-ring (121), but it may occur with anycause of pleural fibrosis.
Radiographs and CT scans.—Onchest radiographs, rounded atelectasisappears as a mass abutting a pleuralsurface, usually in the posterior part ofa lower lobe. Distorted vessels have acurvilinear disposition as they convergeon the mass (the comet tail sign). Thedegree of lobar retraction depends onthe volume of atelectatic lung. It is al-most invariably associated with othersigns of pleural fibrosis (eg, blunting ofcostophrenic angle). CT is more sensi-tive for the detection and display of thecharacteristic features of rounded atel-ectasis (122,123) (Fig 65). An addi-tional sign is homogeneous uptake ofcontrast medium in the atelectatic lung.Synonyms include folded lung syndrome,helical atelectasis, Blesovsky syndrome,pleural pseudotumor, and pleuroma.
secondary pulmonary lobuleSee lobule.
segmentAnatomy.—A segment is the unit of alobe ventilated by a segmental bron-chus, perfused by a segmental pulmo-nary artery, and drained by an interseg-mental pulmonary vein. There are twoto five segments per lobe.
Radiographs and CT scans.—Indi-vidual segments cannot be precisely de-lineated on chest radiographs and CTscans, and their identification is madeinferentially on the basis of the positionof the supplying segmental bronchusand artery. When occasionally present,intersegmental fissures help to identifysegments.
septal lineSee interlobular septum.
septal thickeningSee interlobular septal thickening.
signet ring signCT scans.—This finding is composed ofa ring-shaped opacity representing a di-lated bronchus in cross section and asmaller adjacent opacity representingits pulmonary artery, with the combina-tion resembling a signet (or pearl) ring(124) (Fig 66). It is the basic CT sign ofbronchiectasis (27,125). The signet ringsign can also be seen in diseases charac-
terized by abnormal reduced pulmonaryarterial flow (eg, proximal interruptionof pulmonary artery [126] or chronicthromboembolism [127]). Occasionally,the tiny vascular opacity abutting abronchus is a bronchial, rather than apulmonary, artery.
silhouette signRadiographs.—The silhouette sign isthe absence of depiction of an anatomicsoft-tissue border. It is caused by con-solidation and/or atelectasis of the adja-cent lung (Fig 67), by a large mass, or bycontiguous pleural fluid (128,129). Thesilhouette sign results from the juxtapo-sition of structures of similar radio-graphic attenuation. The sign actuallyrefers to the absence of a silhouette. It isnot always indicative of disease (eg, un-explained absence of right border ofheart is seen in association with pectusexcavatum and sometimes in healthy in-dividuals).
small-airways diseasePathology.—This phrase is an arbitraryterm used more frequently in thin-sec-tion CT descriptions than in the patho-physiology literature, where it was firstcoined (130). Small-airways diseasenow generally refers to any conditionaffecting the bronchioles, whereas
Figure 65
Figure 65: Sagittal CT scan shows roundedatelectasis in left lower lobe.
Figure 66
Figure 66: Transverse CT scan shows signetring sign (arrow).
Figure 67
Figure 67: Chest radiograph shows silhouettesign, with obscuration of right border of heart(arrows).
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 717

bronchiolitis more specifically describesinflammation of the bronchioles (131).
CT scans.—Small airways are consid-ered to be those with an internal diametersmaller than or equal to 2 mm and a nor-mal wall thickness of less than 0.5 mm(32). Small-airways disease is manifest onCT scans as one or more of the followingpatterns: mosaic attenuation, air trap-ping, centrilobular micronodules, tree-in-bud pattern, or bronchiolectasis.
subpleural curvilinear line
CT scans.—This finding is a thin curvi-linear opacity, 1–3 mm in thickness, ly-ing less than 1 cm from and parallel tothe pleural surface (Fig 68). It corre-sponds to atelectasis of normal lung ifseen in the dependent posteroinferiorportion of lung of a patient in the supineposition and is subsequently shown todisappear on CT sections acquired withthe patient prone. It may also be en-countered in patients with pulmonaryedema (132) or fibrosis (other signs areusually present). Though described inthe context of asbestosis, this finding isnot specific for asbestosis.
traction bronchiectasis and tractionbronchiolectasisCT scans.—Traction bronchiectasis andtraction bronchiolectasis respectivelyrepresent irregular bronchial and bron-chiolar dilatation caused by surroundingretractile pulmonary fibrosis (130). Di-lated airways are usually identifiable assuch (Fig 69) but may be seen as cysts(bronchi) or microcysts (bronchioles inthe lung periphery). The juxtapositionof numerous cystic airways may makethe distinction from “pure” fibrotic hon-eycombing difficult.
tree-in-bud patternCT scans.—The tree-in-bud pattern rep-resents centrilobular branching struc-tures that resemble a budding tree. Thepattern reflects a spectrum of endo- andperibronchiolar disorders, including mu-coid impaction, inflammation, and/or fi-brosis (134,135) (Fig 70). This pattern ismost pronounced in the lung peripheryand is usually associated with abnormali-ties of the larger airways. It is particularlycommon in diffuse panbronchiolitis (136),endobronchial spread of mycobacterialinfection (137), and cystic fibrosis. A sim-ilar pattern is a rare manifestation of arte-riolar (microangiopathic) disease (138).
Figure 68
Figure 68: Transverse CT scan shows a sub-pleural curvilinear line.
Figure 69
Figure 69: Transverse CT scan shows tractionbronchiectasis (arrows) cased by retractile pulmo-nary fibrosis.
Figure 70
Figure 70: Transverse CT scan shows tree-in-bud pattern (arrows).
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
718 Radiology: Volume 246: Number 3—March 2008

usual interstitial pneumonia, or UIPPathology.—UIP is a histologic patternof pulmonary fibrosis characterized bytemporal and spatial heterogeneity,with established fibrosis and honey-combing interspersed among normallung. Fibroblastic foci with fibrotic de-struction of lung architecture, oftenwith honeycombing, are the key findings(5). The fibrosis is initially concentratedin the lung periphery. UIP is the patternseen in idiopathic pulmonary fibrosis,but can be encountered in diseases ofknown cause (eg, some cases of chronichypersensitivity pneumonitis).
Radiographs and CT scans.—Honey-combing with a basal and subpleuraldistribution (Fig 71) is regarded as pa-thognomonic (63,65), but not all casesof biopsy-proved UIP have this distinc-tive CT pattern.
Acknowledgments: The authors thank PeterArmstrong, MD, David A. Lynch, MD, Tom V.Colby, MD, and Tomas Franquet, MD, for theirearly critical review and members of the Fleis-chner Society, particularly Eric Milne, MD, andPaul Friedman, MD, for their helpful comments.Hannah Rouse, MD, assisted with the collectionof illustrations. Anthony V. Proto, MD, placedarrows on the illustrations.
References1. Tuddenham WJ. Glossary of terms for tho-
racic radiology: recommendations of theNomenclature Committee of the FleischnerSociety. AJR Am J Roentgenol 1984;143:509–517.
2. Austin JH, Muller NL, Friedman PJ, et al.
Glossary of terms for CT of the lungs: rec-ommendations of the Nomenclature Com-mittee of the Fleischner Society. Radiology1996;200:327–331.
3. Huth EJ. Medical style and format: an inter-national manual for authors, editors, andpublishers. Philadelphia, Pa: ISI, 1987;126.Cited by:Skryd PJ. Radiologic nomencla-ture and abbreviations. Radiology 2001;218(1)10–11.
4. Webb WR. Thin-section CT of the second-ary pulmonary lobule: anatomy and the im-age—the 2004 Fleischner lecture. Radiology2006;239(2):322–338.
5. American Thoracic Society/European Re-spiratory Society International Multidisci-plinary Consensus Classification of the Idio-pathic Interstitial Pneumonias. This jointstatement of the American Thoracic Soci-ety (ATS), and the European RespiratorySociety (ERS) was adopted by the ATSboard of directors, June 2001 and by theERS executive committee, June 2001. Am JRespir Crit Care Med 2002;165:277–304.[Published correction appears in Am J Re-spir Crit Care Med 2002;166(3):426.]
6. Johkoh T, Muller NL, Taniguchi H, et al.Acute interstitial pneumonia: thin-sectionCT findings in 36 patients. Radiology 1999;211:859–863.
7. Lynch DA, Travis WD, Muller NL, et al.Idiopathic interstitial pneumonias: CT fea-tures. Radiology 2005;236(1):10–21.
8. Reed JC, Madewell JE. The air bronchogramin interstitial disease of the lungs: a radio-logical-pathological correlation. Radiology1975;116:1–9.
9. Buckingham SJ, Hansell DM. Aspergillus inthe lung: diverse and coincident forms. EurRadiol 2003;13:1786–1800.
10. Abramson S. The air crescent sign. Radiol-ogy 2001;218(1):230–232.
11. Arakawa H, Webb WR. Air trapping onexpiratory high-resolution CT scans in theabsence of inspiratory scan abnormalities:correlation with pulmonary function testsand differential diagnosis. AJR Am J Roent-genol 1998;170:1349–1353.
12. Bankier AA, Van Muylem A, Scillia P, DeMaertelaer V, Estenne M, Gevenois PA.Air trapping in heart-lung transplantrecipients: variability of anatomic distri-bution and extent at sequential expiratorythin-section CT. Radiology 2003;229:737–742.
13. Arakawa H, Kurihara Y, Sasaka K, Naka-jima Y, Webb WR. Air trapping on CT ofpatients with pulmonary embolism. AJRAm J Roentgenol 2002;178:1201–1207.
14. Murata K, Khan A, Herman PG. Pulmonaryparenchymal disease: evaluation with high-resolution CT. Radiology 1989;170:629–635.
15. Heitzman ER. The infraaortic area. In: Themediastinum: radiologic correlations withanatomy and pathology. Berlin, Germany:Springer-Verlag, 1988;151:–168.
16. Blank N, Castellino RA. Patterns of pleuralreflections of the left superior mediastinum:normal anatomy and distortions produced byadenopathy. Radiology 1972;102:585–589.
17. Im JG, Webb WR, Han MC, Park JH. Api-cal opacity associated with pulmonarytuberculosis: high-resolution CT findings.Radiology 1991;178:727–731.
18. Yousem SA. Pulmonary apical cap: a dis-tinctive but poorly recognized lesion in pul-monary surgical pathology. Am J SurgPathol 2001;25:679–683.
19. Dail DH. Pulmonary apical cap. Am J SurgPathol 2001;25:1344.
20. Woodring JH, Reed JC. Types and mecha-nisms of pulmonary atelectasis. J ThoracImaging 1996;11:92–108.
21. Molina PL, Hiken JN, Glazer HS. Imagingevaluation of obstructive atelectasis. J Tho-rac Imaging 1996;11:176–186.
22. Woodring JH, Reed JC. Radiographic man-ifestations of lobar atelectasis. J Thorac Im-aging 1996;11:109–144.
23. Heitzman ER. The azygoesophageal recess.In: The mediastinum: radiologic correla-tions with anatomy and pathology. Berlin,Germany: Springer-Verlag, 1988;276:–286.
24. Ren H, Hruban RH, Kuhlman JE, et al.Computed tomography of inflation-fixedlungs: the beaded septum sign of pulmo-nary metastases. J Comput Assist Tomogr1989;13:411–416.
25. Ryu JH, Swensen SJ. Cystic and cavitarylung diseases: focal and diffuse. Mayo ClinProc 2003;78:744–752.
26. Kang EY, Miller RR, Muller NL.Bronchiectasis: comparison of preopera-tive thin-section CT and pathologic findingsin resected specimens. Radiology 1995;195:649–654.
27. Naidich DP, McCauley DI, Khouri NF, Sti-tik FP, Siegelman SS. Computed tomogra-phy of bronchiectasis. J Comput Assist To-mogr 1982;6:437–444.
28. Grenier P, Maurice F, Musset D, Menu Y,Nahum H. Bronchiectasis: assessment bythin-section CT. Radiology 1986;161:95–99.
Figure 71
Figure 71: Transverse CT scan shows basaland subpleural honeycombing, indicative of usualinterstitial pneumonia.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 719

29. Dodd JD, Souza CA, Muller NL. Conven-tional high-resolution CT versus helicalhigh-resolution MDCT in the detection ofbronchiectasis. AJR Am J Roentgenol 2006;187:414–420.
30. Hansen JE, Ampaya PE, Bryant GH, NavinJJ. Branching pattern of airways and air-spaces of single human terminal bronchi-ole. J Appl Physiol 1975;38:983–989.
31. Buckley CE, Tucker DH, Thorne NA,Sieker HO. Bronchiolectasis: the clinicalsyndrome and its relationship to chroniclung disease. Am J Med 1965;38:190–198.
32. Hansell DM. Small airways diseases: detec-tion and insights with computed tomogra-phy. Eur Respir J 2001;17:1294–1313.
33. Myers JL, Colby TV. Pathologic manifesta-tions of bronchiolitis, constrictive bronchi-olitis, cryptogenic organizing pneumonia,and diffuse panbronchiolitis. Clin ChestMed 1993;14:611–622.
34. Woodring JH. Unusual radiographic mani-festations of lung cancer. Radiol Clin NorthAm 1990;28:599–618.
35. Muller NL, Kullnig P, Miller RR. The CTfindings of pulmonary sarcoidosis: analysisof 25 patients. AJR Am J Roentgenol 1989;152:1179–1182.
36. Huang L, Schnapp LM, Gruden JF,Hopewell PC, Stansell JD. Presentation ofAIDS-related pulmonary Kaposi’s sarcomadiagnosed by bronchoscopy. Am J RespirCrit Care Med 1996;153:1385–1390.
37. Oikonomou A, Hansell DM. Organizingpneumonia: the many morphological faces.Eur Radiol 2002;12:1486–1496.
38. Seo JB, Song KS, Lee JS, et al.Broncholithiasis: review of the causes withradiologic-pathologic correlation. Radio-Graphics 2002;22(Spec Issue):S199–S213.
39. Murata K, Itoh H, Todo G, et al. Centri-lobular lesions of the lung: demonstrationby high-resolution CT and pathologic corre-lation. Radiology 1986;161:641–645.
40. Heitzman ER, Markarian B, Berger I, Dai-ley E. The secondary pulmonary lobule: apractical concept for interpretation of chestradiographs. I. Roentgen anatomy of thenormal secondary pulmonary lobule. Radi-ology 1969;93:507–512.
41. Webb WR, Stein MG, Finkbeiner WE, ImJG, Lynch D, Gamsu G. Normal and dis-eased isolated lungs: high-resolution CT.Radiology 1988;166:81–87.
42. The definition of emphysema. Report of aNational Heart, Lung, and Blood Institute,Division of Lung Diseases workshop. AmRev Respir Dis 1985;132:182–185.
43. Thurlbeck WM, Muller NL. Emphysema:definition, imaging, and quantification. AJRAm J Roentgenol 1994;163:1017–1025.
44. Foster WL Jr, Pratt PC, Roggli VL, GodwinJD, Halvorsen RA Jr, Putman CE. Centri-lobular emphysema: CT-pathologic correla-tion. Radiology 1986;159:27–32.
45. Leung AN, Miller RR, Muller NL. Parenchy-mal opacification in chronic infiltrative lungdiseases: CT-pathologic correlation. Radi-ology 1993;188:209–214.
46. Laurent F, Philippe JC, Vergier B, et al.Exogenous lipoid pneumonia: HRCT, MR,and pathologic findings. Eur Radiol 1999;9:1190–1196.
47. Kuhlman JE, Scatarige JC, Fishman EK,Zerhouni EA, Siegelman SS. CT demonstra-tion of high attenuation pleural-parenchy-mal lesions due to amiodarone therapy.J Comput Assist Tomogr 1987;11:160–162.
48. Murch CR, Carr DH. Computed tomogra-phy appearances of pulmonary alveolarproteinosis. Clin Radiol 1989;40:240–243.
49. Rossi SE, Erasmus JJ, Volpacchio M, Fran-quet T, Castiglioni T, McAdams HP.“Crazy-paving” pattern at thin-section CTof the lungs: radiologic-pathologic over-view. RadioGraphics 2003;23:1509–1519.
50. Franquet T, Gimenez A, Bordes R, Rodri-guez-Arias JM, Castella J. The crazy-pavingpattern in exogenous lipoid pneumonia:CT-pathologic correlation. AJR Am JRoentgenol 1998;170:315–317.
51. Genereux GP. The end-stage lung: patho-genesis, pathology, and radiology. Radiol-ogy 1975;116:279–289.
52. Aberle DR, Hansell DM, Brown K, TashkinDP. Lymphangiomyomatosis: CT, chest ra-diographic, and functional correlations. Ra-diology 1990;176:381–387.
53. Moore AD, Godwin JD, Muller NL, et al.Pulmonary histiocytosis X: comparison ofradiographic and CT findings. Radiology1989;172:249–254.
54. Primack SL, Hartman TE, Hansell DM,Muller NL. End-stage lung disease: CT find-ings in 61 patients. Radiology 1993;189:681–686.
55. Hartman TE, Primack SL, Swensen SJ,Hansell D, McGuinness G, Muller NL. Des-quamative interstitial pneumonia: thin-sec-tion CT findings in 22 patients. Radiology1993;187:787–790.
56. Lang MR, Fiaux GW, Gillooly M, StewartJA, Hulmes DJ, Lamb D. Collagen contentof alveolar wall tissue in emphysematous
and non-emphysematous lungs. Thorax1994;49:319–326.
57. Cardoso WV, Sekhon HS, Hyde DM, Thurl-beck WM. Collagen and elastin in humanpulmonary emphysema. Am Rev Respir Dis1993;147:975–981.
58. Foster WL Jr, Gimenez EI, Roubidoux MA,et al. The emphysemas: radiologic-patho-logic correlations. RadioGraphics 1993;13:311–328.
59. Remy-Jardin M, Remy J, Giraud F,Wattinne L, Gosselin B. Computed tomog-raphy (CT) assessment of ground-glassopacity: semiology and significance. J Tho-rac Imaging 1993;8:249–264.
60. Remy-Jardin M, Giraud F, Remy J, CopinMC, Gosselin B, Duhamel A. Importance ofground-glass attenuation in chronic diffuseinfiltrative lung disease: pathologic-CT cor-relation. Radiology 1993;189:693–698.
61. Kuhlman JE, Fishman EK, Siegelman SS.Invasive pulmonary aspergillosis in acuteleukemia: characteristic findings on CT, theCT halo sign, and the role of CT in earlydiagnosis. Radiology 1985;157:611–614.
62. Primack SL, Hartman TE, Lee KS, MullerNL. Pulmonary nodules and the CT halosign. Radiology 1994;190:513–515.
63. Lynch DA, David GJ, Safrin S, et al. High-resolution computed tomography in idio-pathic pulmonary fibrosis: diagnosis andprognosis. Am J Respir Crit Care Med2005;172:488–493.
64. American Thoracic Society. Idiopathic pul-monary fibrosis: diagnosis and treatment:international consensus statement—Ameri-can Thoracic Society (ATS), and the Euro-pean Respiratory Society (ERS). Am JRespir Crit Care Med 2000;161(2 pt 1):646–664.
65. Hunninghake GW, Lynch DA, Galvin JR, etal. Radiologic findings are strongly associ-ated with a pathologic diagnosis of usualinterstitial pneumonia. Chest 2003;124:1215–1223.
66. Misumi S, Lynch DA. Idiopathic pulmonaryfibrosis/usual interstitial pneumonia: imag-ing diagnosis, spectrum of abnormalities,and temporal progression. Proc Am ThoracSoc 2006;3:307–314.
67. Dalen JE, Haffajee CI, Alpert JS III, HoweJP, Ockene IS, Paraskos JA. Pulmonaryembolism, pulmonary hemorrhage and pul-monary infarction. N Engl J Med 1977;296:1431–1435.
68. Ren H, Kuhlman JE, Hruban RH, FishmanEK, Wheeler PS, Hutchins GM. CT of infla-tion-fixed lungs: wedge-shaped density and
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
720 Radiology: Volume 246: Number 3—March 2008

vascular sign in the diagnosis of infarction.J Comput Assist Tomogr 1990;14:82–86.
69. Patterson HS, Sponaugle DN. Is infiltrate auseful term in the interpretation of chestradiographs? physician survey results. Ra-diology 2005;235(1):5–8.
70. Kang EY, Grenier P, Laurent F, Muller NL.Interlobular septal thickening: patterns athigh-resolution computed tomography.J Thorac Imaging 1996;11:260–264.
71. Kemper AC, Steinberg KP, Stern EJ. Pul-monary interstitial emphysema: CT find-ings. AJR Am J Roentgenol 1999;172:1642.
72. Donnelly LF, Lucaya J, Ozelame V, et al. CTfindings and temporal course of persistentpulmonary interstitial emphysema inneonates: a multiinstitutional study. AJRAm J Roentgenol 2003;180:1129–1133.
73. Weibel ER. Looking into the lung: what canit tell us? AJR Am J Roentgenol 1979;133:1021–1031.
74. Kattan KR, Eyler WR, Felson B. The juxta-phrenic peak in upper lobe collapse. Radiol-ogy 1980;134:763–765.
75. Cameron DC. The juxtaphrenic peak (Kat-ten’s sign) is produced by rotation of aninferior accessory fissure. Australas Radiol1993;37:332–335.
76. Davis SD, Yankelevitz DF, Wand A,Chiarella DA. Juxtaphrenic peak in upperand middle lobe volume loss: assessmentwith CT. Radiology 1996;198:143–149.
77. Westcott JL, Cole S. Plate atelectasis. Radi-ology 1985;155:1–9.
78. Miller WS. The lung. 2nd ed. Springfield,Ill: Thomas, 1947;203:–205.
79. Glazer GM, Gross BH, Quint LE, FrancisIR, Bookstein FL, Orringer MB. Normalmediastinal lymph nodes: number and sizeaccording to American Thoracic Societymapping. AJR Am J Roentgenol 1985;144:261–265.
80. Remy-Jardin M, Duyck P, Remy J, et al.Hilar lymph nodes: identification with spiralCT and histologic correlation. Radiology1995;196:387–394.
81. Swigris JJ, Berry GJ, Raffin TA, KuschnerWG. Lymphoid interstitial pneumonia: anarrative review. Chest 2002;122:2150–2164.
82. Johkoh T, Muller NL, Pickford HA, et al.Lymphocytic interstitial pneumonia: thin-section CT findings in 22 patients. Radiol-ogy 1999;212:567–572.
83. Ichikawa Y, Kinoshita M, Koga T, OizumiK, Fujimoto K, Hayabuchi N. Lung cyst for-mation in lymphocytic interstitial
pneumonia: CT features. J Comput AssistTomogr 1994;18:745–748.
84. Heitzman ER. The mediastinum: radiologiccorrelations with anatomy and pathology.Berlin, Germany: Springer-Verlag, 1988;7:–309.
85. Fraser RS, Muller NL, Colman N, Pare PD.The mediastinum: diagnosis of diseases ofthe chest. 4th ed. Philadelphia, Pa: Saun-ders, 1999;205:–211.
86. Remy-Jardin M, Beuscart R, Sault MC,Marquette CH, Remy J. Subpleural mi-cronodules in diffuse infiltrative lungdiseases: evaluation with thin-section CTscans. Radiology 1990;177:133–139.
87. Remy-Jardin M, Remy J, Wallaert B, Mul-ler NL. Subacute and chronic bird breederhypersensitivity pneumonitis: sequentialevaluation with CT and correlation withlung function tests and bronchoalveolar la-vage. Radiology 1993;189:111–118.
88. Brauner MW, Lenoir S, Grenier P, CluzelP, Battesti JP, Valeyre D. Pulmonarysarcoidosis: CT assessment of lesion re-versibility. Radiology 1992;182:349–354.
89. Worthy SA, Muller NL, Hartman TE,Swensen SJ, Padley SP, Hansell DM. Mo-saic attenuation pattern on thin-section CTscans of the lung: differentiation among in-filtrative lung, airway, and vascular dis-eases as a cause. Radiology 1997;205:465–470.
90. Martin KW, Sagel SS, Siegel BA. Mosaicoligemia simulating pulmonary infiltrateson CT. AJR Am J Roentgenol 1986;147:670–673.
91. Arakawa H, Webb WR, McCowin M, Kat-sou G, Lee KN, Seitz RF. Inhomogeneouslung attenuation at thin-section CT: diag-nostic value of expiratory scans. Radiology1998;206:89–94.
92. Hansell DM, Wells AU, Rubens MB, ColePJ. Bronchiectasis: functional significanceof areas of decreased attenuation at expira-tory CT. Radiology 1994;193:369–374.
93. Roberts CM, Citron KM, Strickland B. In-trathoracic aspergilloma: role of CT in diag-nosis and treatment. Radiology 1987;165:123–128.
94. Erasmus JJ, Connolly JE, McAdams HP,Roggli VL. Solitary pulmonary nodules. I.Morphologic evaluation for differentiationof benign and malignant lesions. Radio-Graphics 2000;20:43–58.
95. MacDonald SL, Rubens MB, Hansell DM, etal. Nonspecific interstitial pneumonia andusual interstitial pneumonia: comparativeappearances at and diagnostic accuracy of
thin-section CT. Radiology 2001;221:600–605.
96. Lee KS, Kullnig P, Hartman TE, Muller NL.Cryptogenic organizing pneumonia: CTfindings in 43 patients. AJR Am J Roentge-nol 1994;162:543–546.
97. Guest PJ, Hansell DM. High resolutioncomputed tomography in emphysema asso-ciated with alpha-1-antitrypsin deficiency.Clin Radiol 1992;45:260–266.
98. Spouge D, Mayo JR, Cardoso W, MullerNL. Panacinar emphysema: CT and patho-logic findings. J Comput Assist Tomogr1993;17:710–713.
99. Copley SJ, Wells AU, Muller NL, et al.Thin-section CT in obstructive pulmonarydisease: discriminatory value. Radiology2002;223:812–819.
100. Akira M, Yamamoto S, Yokoyama K, et al.Asbestosis: high-resolution CT—pathologiccorrelation. Radiology 1990;176:389–394.
101. Akira M, Yamamoto S, Inoue Y, SakataniM. High-resolution CT of asbestosis and id-iopathic pulmonary fibrosis. AJR Am JRoentgenol 2003;181:163–169.
102. Johkoh T, Muller NL, Ichikado K, Naka-mura H, Itoh H, Nagareda T. Perilobularpulmonary opacities: high-resolution CTfindings and pathologic correlation. J Tho-rac Imaging 1999;14:172–177.
103. Ujita M, Renzoni EA, Veeraraghavan S,Wells AU, Hansell DM. Organizingpneumonia: perilobular pattern at thin-sec-tion CT. Radiology 2004;232:757–761.
104. Colby TV, Swensen SJ. Anatomic distribu-tion and histopathologic patterns in diffuselung disease: correlation with HRCT. J Tho-rac Imaging 1996;11:1–26.
105. Roberts GH. The pathology of parietal pleu-ral plaques. J Clin Pathol 1971;24:348–353.
106. Lynch DA, Gamsu G, Aberle DR. Conven-tional and high-resolution computed tomog-raphy in the diagnosis of asbestos-relateddiseases. RadioGraphics 1989;9:523–551.
107. Quigley MJ, Fraser RS. Pulmonarypneumatocele: pathology and pathogenesis.AJR Am J Roentgenol 1988;150:1275–1277.
108. Wagner JC, Wusteman FS, Edwards JH,Hill RJ. The composition of massive lesionsin coal miners. Thorax 1975;30:382–388.
109. Chong S, Lee KS, Chung MJ, Han J, KwonOJ, Kim TS. Pneumoconiosis: comparisonof imaging and pathologic findings. Radio-Graphics 2006;26:59–77.
110. Ward S, Heyneman LE, Reittner P, Kaze-
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
Radiology: Volume 246: Number 3—March 2008 721

rooni EA, Godwin JD, Muller NL. Talcosisassociated with IV abuse of oralmedications: CT findings. AJR Am J Roent-genol 2000;174:789–793.
111. Weisbrod GL, Chamberlain D, Herman SJ.Cystic change (pseudocavitation) associ-ated with bronchioloavleolar carcinoma: areport of four patients. J Thorac Imaging1995;10:106–111.
112. Simon M. The pulmonary veins in mitralstenosis. J Fac Radiol 1958;9:25–32.
113. Milne EN. Physiological interpretation ofthe plain radiograph in mitral stenosis, in-cluding a review of criteria for the radiolog-ical estimation of pulmonary arterial andvenous pressures. Br J Radiol 1963;36:902–913.
114. Fraig M, Shreesha U, Savici D, KatzensteinAL. Respiratory bronchiolitis: a clinico-pathologic study in current smokers, ex-smokers, and never-smokers. Am J SurgPathol 2002;26:647–653.
115. Heyneman LE, Ward S, Lynch DA, Remy-Jardin M, Johkoh T, Muller NL. Respira-tory bronchiolitis, respiratory bronchioli-tis-associated interstitial lung disease, anddesquamative interstitial pneumonia: dif-ferent entities or part of the spectrum ofthe same disease process? AJR Am JRoentgenol 1999;173:1617–1622.
116. Hansell DM, Nicholson AG. Smoking-re-lated diffuse parenchymal lung disease:HRCT-pathologic correlation. Semin RespirCrit Care Med 2003;24:377–392.
117. Zompatori M, Poletti V, Battista G, DiegoliM. Bronchiolitis obliterans with organizingpneumonia (BOOP), presenting as a ring-shaped opacity at HRCT (the atoll sign): acase report. Radiol Med (Torino) 1999;97:308–310.
118. Kim SJ, Lee KS, Ryu YH, et al. Reversedhalo sign on high-resolution CT of crypto-
genic organizing pneumonia: diagnostic im-plications. AJR Am J Roentgenol 2003;180:1251–1254.
119. Gasparetto EL, Escuissato DL, Davaus T, etal. Reversed halo sign in pulmonary para-coccidioidomycosis. AJR Am J Roentgenol2005;184:1932–1934.
120. Savoca CJ, Austin JH, Goldberg HI. Theright paratracheal stripe. Radiology 1977;122:295–301.
121. Cohen AM, Crass JR, Chung-Park M, To-mashefski JF Jr. Rounded atelectasis andfibrotic pleural disease: the pathologic con-tinuum. J Thorac Imaging 1993;8:309–312.
122. Lynch DA, Gamsu G, Ray CS, Aberle DR.Asbestos-related focal lung masses: mani-festations on conventional and high-resolu-tion CT scans. Radiology 1988;169:603–607.
123. O’Donovan PB, Schenk M, Lim K, Obu-chowski N, Stoller JK. Evaluation of thereliability of computed tomographic criteriaused in the diagnosis of round atelectasis.J Thorac Imaging 1997;12:54–58.
124. Ouellette H. The signet ring sign. Radiology1999;212:67–68.
125. McGuinness G, Naidich DP, Leitman BS,McCauley DI. Bronchiectasis: CT evalua-tion. AJR Am J Roentgenol 1993;160:253–259.
126. Ryu DS, Spirn PW, Trotman-Dickenson B,et al. HRCT findings of proximal interrup-tion of the right pulmonary artery. J ThoracImaging 2004;19:171–175.
127. Remy-Jardin M, Remy J, Louvegny S, Ar-taud D, Deschildre F, Duhamel A. Airwaychanges in chronic pulmonary embolism:CT findings in 33 patients. Radiology 1997;203:355–360.
128. Felson B, Felson H. Localisation of intratho-racic lesions by means of the postero-ante-
rior roentgenogram: the silhouette sign.Radiology 1950;55:363–374.
129. Marshall GB, Farnquist BA, MacGregor JH,Burrowes PW. Signs in thoracic imaging.J Thorac Imaging 2006;21:76–90.
130. Hogg JC, Macklem PT, Thurlbeck WM. Siteand nature of airway obstruction in chronicobstructive lung disease. N Engl J Med1968;278:1355–1360.
131. Muller NL, Miller RR. Diseases of thebronchioles: CT and histopathologic find-ings. Radiology 1995;196:3–12.
132. Arai K, Takashima T, Matsui O, Kadoya M,Kamimura R. Transient subpleural curvilin-ear shadow caused by pulmonary conges-tion. J Comput Assist Tomogr 1990;14:87–88.
133. Desai SR, Wells AU, Rubens MB, Du BoisRM, Hansell DM. Traction bronchiectasisin cryptogenic fibrosing alveolitis: associ-ated computed tomographic features andphysiological significance. Eur Radiol 2003;13:1801–1808.
134. Aquino SL, Gamsu G, Webb WR, Kee ST.Tree-in-bud pattern: frequency and signifi-cance on thin section CT. J Comput AssistTomogr 1996;20:594–599.
135. Eisenhuber E. The tree-in-bud sign. Radiol-ogy 2002;222:771–772.
136. Akira M, Kitatani F, Yong-Sik L, et al. Dif-fuse panbronchiolitis: evaluation with high-resolution CT. Radiology 1988;168:433–438.
137. Im JG, Itoh H, Shim YS, et al. Pulmonarytuberculosis: CT findings—early active dis-ease and sequential change with antituber-culous therapy. Radiology 1993;186:653–660.
138. Franquet T, Gimenez A, Prats R, Rodrigu-ez-Arias JM, Rodriguez C. Thrombotic mi-croangiopathy of pulmonary tumors: a vas-cular cause of tree-in-bud pattern on CT.AJR Am J Roentgenol 2002;179:897–899.
SPECIAL REVIEW: Glossary of Terms for Thoracic Imaging Hansell et al
722 Radiology: Volume 246: Number 3—March 2008