Embed Size (px)
Citation preview

June 1, 1985 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 55 1643
Flecainide-Induced Aggravation of Ventricular Arrhythmias
MICHAEL WEHR, MD BERND NOLL, MD
JOACHIM KRAPPE, MD
Flecainide acetate, a new antiarrhythmic agent, has a high rate of antiarrhythmic efficacy in animaI~.l~~ It has electrophysiologic properties similar to those of other class I antiarrhythmic agents such as quinidine, pro- cainamide and disopyramide.3 Flecainide can prolong the QT interval and give rise to ventricular tachy- arrhythmias. We herein report 2 patients who had syncope caused by flecainide-induced ventricular tachyarrhythmias associated with marked QT prolon- gation.
Patient 1, a 64-year-old woman with coronary heart dis- ease without a history of presyncope OF syncope, had recur- rent paroxsysmal palpitations. devious antiarrhythmic drug treatment included propafenone and disopyramide. A pretreatment Halter electFocaFdiogFam (ECG) was not performed. She had signs of New York Heart Association class II congestive heart failure. A l&lead ECG (Fig. 1) re- vealed sinus rhythm at a rate of 80 beatslmin, a normal axis, T-wave abnormalities in the precordial leads, and unifocal premature ventricular complexes (WCs). The intraatrial and intraventricular conduction times were normal, as was the uncorrected QT interval (0.38 second) and the corrected QTc interval (0.43 second). The cardiothoracic ratio was 0.6. The serum potassium, calcium and magnesium levels were normal. The patient was subsequently treated with fle- cainide, 400 mglday (200 mg twice daily). An electrophysi- ologic study before antiarrhythmic treatment was not done. Two weeks later, during a routine follow-up examination in the physician’s office, the patient collapsed and was resus- citated by direct-current shock (200 J) from pleomorphic ventricular tachycardia (VT) as seen on the scope. On ad- mission, the ECG (Fig. 2) showed an isorhythmic dissociation between a sinus rhythm and an atrioventricular nodal
From the Department of Cardiology, Center for internal Medicine, PhilippsUniversity Marburg, Safdinger Strasse, D 3550 Marburg, Federal Republic of Germany. Manuscript received December 17, 1984; revised IWNJSCriPt reCeiVed February 14, 1985, accepted February 18, 1985.
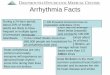
FfGURE 1. Twelve-lead ektmcard iogam of patient 1 before treatment with flecainide treatment was initiated.
rhythm, both at rates of 50 beatslmin. The QRS duration was normal (0.08 second), but the uncorrected QT interval (0.58 second) and the corrected QTc interval (0.53 second) were markedly prolonged. No electrolyte disturbance OF electro- cardiographic signs of myocardial infarction were detected. Blood levels of flecainide were not determined. Flecainide was immediately withdrawn, the QT interval normalized and the clinical follow-up of the patient during no antiarrhyth- mic treatment revealed no further complications.
Patient 2 was a 21-year-old woman with known dilated cardiomyopathy and PVCs who had been treated previously with quinidine and later with disopyramide, without satis- factory results. One week after flecainide treatment, 400 mglday (200 mg twice daily), was started (with successful suppression of PVCs), she collapsed during a routine check-up. The ECG (Fig. 3) showed a regular wide QRS
OVL V5 2 f ---L---
-J,------ f----- !
FIGURE 2. Twelve-lead electrocardiogram of patient 1 after cardio- version because of pofymorphic ventricular tachycardia 2 weeks after flecainide treatment (400 mgkfay) was initiated.
I
II
Ill
aVR
aVL
aVF
FIGURE 3. Twelve-lead electrocardiogram of patient 2 one week after flecainide treatment (400 mg/day) was initiated showing a regular ventricular tachycardia at a rate of 135 beatslmin.

1644 BRIEF REPORTS
. -
FIGURE 4. Twelve-lead electrocardiogram of patient 2 after direct- ctrrent shodc because of hemodynamic deterioration during ventricular tachycardia (Fig. 3). The QT interval is prolonged (0.56 second).
tachycardia at a rate of 135 beatslmin and a left bundle branch block morphologic pattern with an extreme axis. Because of hemodynamic deterioration, cardioversion (200 Japplied once) became necessary. The ECG (Fig. 4) on ad- mission in our hospital showed a sinus rhythm at a rate of 80 beatslmin and left-axis deviation. The intraatrial conduction was prolonged (0.12 second), as was the QT interval (0.43 second) and the corrected QTc interval (0.49 second). The electrolyte levels were within normal limits. There were no electrocardiographic signs of an acute myocardial infarction. Blood levels of flecainide were not available. Flecainide therapy was withdrawn and during hospitalization of the patient, the QTc interval shortened to 0.44 second. The pa- tient was discharged with amiodarone therapy, 200 mglday, without significant QTc prolongation or adverse sequelae.
The most dangerous side effect of an antiarrhythmic therapy is the provocation of VT, torsades de pointes or ventricular fibrillation. Our patients show that fle- cainide can cause QTc prolongation and subsequent VT despite doses (400 mg/day) considered nontoxic. Toxic
doses of class I antiarrhythmic drugs (quinidine, pro- cainamide, disopyramide) uniformly cause marked in- creases of both QRS duration and the QT interval.4 However, in instances of quinidine- and disopyra- mide-induced VT without toxic serum levels, there may be marked QTc prolongation even in the absence of QRS widening and such unusual marked QTc prolon- gation occurred unexpectedly without prodromal signs suggesting an idosyncratic drug reaction.4ps Lui et al6 reported a patient who had VT caused by QT prolon- gation despite therapeutic levels of flecainide. Both our patients had marked QTc prolongation in the absence of significant QRS widening and electrolyte distur- bances. Most patients reported to have disopyramide- induced ventricular tachyarrhythmias were women with organic heart disease in whom a QTc prolongation without QRS widening were noted.5 The causal relation between the observed VT and flecainide is clear, since flecainide has been given for a short period in the ab- sence of other cardioactive drugs. For both patients it was the first episode of syncope despite previous treatment with other class I antiarrhythmic drugs. After withdrawal of flecainide therapy, QTc intervals short- ened in both patients and further arrhythmias were not observed. This observation excludes cardioversion as the only mechanism of QTc prolongation; however, an additional effect to the antiarrhythmic effect of fle- cainide on the QTc interval and the observed brady- cardia in the first patient cannot be excluded. Both patients collapsed during a routine examination in their physician’s office. An increased sympathomimetic re- action in the presence of QTc prolongation could be an important factor. Thus, flecainide as well as other class I antiarrhythmic drugs should not be given to patients with preexisting QTc prolongation. In all patients treated with flecainide or other type I drugs, a careful monitoring of the QTc interval may be advisable.
References 1. Bchmtdttfl,BeabeckBD,Hen+CL,BenlttE~.6cm
Tactions ;;; new compound, R 618 In dcgs and mice. Fed Proc 1 75,341.775-
2. And&eon IL, Steward IR, Perry BA, van Hamereveld DD, Johneon TA, Conrad GJ, Chang SF, Kvam DC, Pltt 6. Oral flecainide acetate for the treatment of ventricular arrhythmias. N Engl J Med 1981;305:473-476.
3. Hodeee AB, Follanebee WP? 6pear IF, Moore EN. Electrophysiological ef- fects of a new antiirrhythmlc agent, flecainide on the intact canine heart. J Cardlovasc Ft~macol 1979;1:427-431.
4. Koeter RW, Wellens HJJ. QMdinsinduced ventricular flutter and AtMation
5. without digitalis therapy. Am J Cardiol 1978;38:519-520. 6reltMclt G,6eipel t., Haerten K. Paradcxe Reaktion nach Disopyramid wl Chinidin. 2 Kardiol 1980;69:556-580.
6. Lul HK, Lee G, Dlelrlch P, Low RI, Masen DT. Flecainide-induced QT pre longation and ventricular tachycardia. Am Heart J 1982;103:567-589.