Embed Size (px)
Citation preview

ORAL MEDICINE MINOR CASE
FISSURED TONGUE
CHAPTER I
INTRODUCTION

1
Tongue disorders are characterized by changes in the texture and appearance of
the tongue's surface. People of all ages can experience several different types of tongues
disorders due to poor oral hygiene, infection, genetic tendencies and various underlying
medical conditions. Although some tongue disorders are symptomatic meanwhile some are
completely symptom free (John Hopkins, 2008).
Following is the description of the patient. He is a male aged 19 years old,
complained that his tongue has crack and groove on surface of his tongue. Patient said
that he never had any discomfort or pain but he finds it difficult to clean and sometime
there are white coatings on the tongue. The patient only brush his teeth as daily oral
hygiene and do not use any mouthwashes. Patient has no history of previous disease or
known systemic diseases. Patient also complaints of ulceration on right cheek. The ulcers
form around 3 days ago. The patient did not recall any bitting or traumatizing at the ulcer
location and not taking any medication for the ulcers.
Through clinical examination, the diagnosis for the tongue disease is fissured
tongue. The treatment for the ulcer is antibacterial mouthwash contains Chlorohexidine
0.2% and used twice daily with 30 to 60 seconds gargling. After 1 week, the lesions is
evaluated to get the best result from the treatment given.
CHAPTER II
PATIENT STATUS
2.1 Clinical Working Record

2
Name : Mr. R
Sex : Male
Age : 19 years old
Religion : Muslim
Occupation : Private
Marital Status : Single
2.2 Anamnesis
The patient complained that his tongue has crack and groove on surface of his
tongue. Patient said that he never had any discomfort or pain but he finds it difficult to
clean and sometime there are white coatings on the tongue. The patient only brush his
teeth as daily oral hygiene and do not use any mouthwashes. Patient has no history of
previous disease or known systemic diseases. Patient also complaints of ulceration on
right cheek. The ulcers form around 3 days ago. The patient did not recall any bitting or
traumatizing at the ulcer location and not taking any medication for the ulcers. He decided
to see a dentist to get the further treatment with the hope that the lesion can be reduced.
2.3 History of Systemic Disease
Heart disease : No
Hypertension : No
Diabetes Mellitus : No
Asthma/Allergy : No
Hepatitis : No
GIT disease : No
Blood Abnormalities : No

3
Others : No
2.4 History of Previous Disease: No
2.5 General Condition
General Condition : Good
Blood Pressure : 120/70 mmHg
Consciousness : Compos Mentis
Respiration : 18 x minute
Temperature : Normal
Pulse : 84 x minute
2.6 Extra Oral Examination
Lymph nodes:
Submandibular : Right: Non palpable
Left : Non palpable
Submental : Right: Non palpable
Left: Non palpable
Cervical : Right: Non palpable
Left: Non palpable
Others : -
Lip : Normal
Face : Symmetry
Circum oral : Normal

4
Others : Normal
2.7 Intra Oral Examination
Oral hygiene (based on Plaque Indice (PI) by O’Leary et al., 1972): Moderate
o Plaque : +
o Calculus : -
o Stain : -
Gingiva : Normal
Buccal Mucosa : Ulcer on buccal dextra reg 46 with diameter of
4mm with erythematous border and pseudomembranous layer base
Labial Mucosa : Normal
Palatal Dorum : Normal
Palatal Mole : Normal
Frenulum : Normal
Tongue : Fissured on the dorsm and lateral of tongue.
Floor of The Mouth : Normal
Teeth
Caries : 15
Missing : 36
Filling : -
Discoloration : -

5
Fissure on the lateral side of the tongue (1st visit)

6
Fissure on the dorsum surface of the tongue (1st visit)
Ulcer on right buccal at area 46 (1st visit)
2.8 Diagnosis
1. Fissured tongue
2. Traumatic ulcer
2.9 Treatment Planning and Management
Treatment planning involve communication and information about fissured tongue.
The patient should be informed about the benign nature and the progression of this lesion
with age. The patient was explained that this is normal. He is assured that good hygiene is
sufficient to manage fissured tongue. The patient is educated about the proper tooth
brushing method and advised to use tongue scraper to clean his tongue. The patient was
also prescribed chlorhexidine gargle to rinse the oral cavity 2x per day until the ulcer
subsides. Patient is then asked to come for control after 1 week.
2.10 Evaluation After 1 week
Patient came for control after 1 week. Based on patient’s memory, patient said that
the ulcer was reduced and eventually disappeared after rinsing with the antibacterial

7
mouthwash prescribed to the patient after 5 days from the first visit. Since that, patient
always takes precaution by maintaining good oral hygiene making sure his tongue is clean.
2.10.2 Extra Oral
Lymph nodes
Submandibular : Normal
Submental : Normal
Servikal :Normal
Lip : Normal
TMJ : Normal
Face : Symmetry
Oral Sirkum : Normal
2.10.3 Intra Oral
Oral Hygiene : Good
Staining : Negative
Gingiva : Pinkish red
Buccal Mucosa : Normal
Labial Mucosa : Normal
Palatum Durum : Normal
Palatum Mole : Normal
Frenulum : Normal
Palate : Normal
Tongue : Fissured on the dorsm and lateral of tongue
Floor of the mouth : Normal

8
Tonsils : Normal
Gingival : Normal
Fissure on Dorsum of tongue (Control 1 week)

9
Fissure on lateral side of tongue (Control 1 week)
CHAPTER III
LITERATURE REVIEW
Anatomy of tongue
The tongue
The tongue consists of a buccal and a pharyngeal portion separated by a V-
shaped groove on its dorsal surface, the sulcus terminalis. At the apex of this groove is a
shallow depression, the foramen caecum, marking thethe sulcus lie a row of large vallate
papilliae. The under aspect of the tongue bears the median frenulum linguae; the mucosa
is thin on this surface and the lingual veins can thus be seen on either side of the frenulum.
The lingual nerve and the lingual artery are medial to the vein but not visible. More laterally
can be seen a fringed fold of mucous membrane termed the plica fimbriata. On either side
of the base of the frenulum can be seen the orifice of the submandibular duct on its papilla.
Inspect this in a mirror and note the discharge of saliva when you press on your
submandibular gland just below the angle of the jaw. (Ellis, 2006)

10
Structure
The thick stratified squamous mucosa of the dorsum of the tongue bears papillae
over the anterior two-thirds back as far as the sulcus terminalis. These papillae (particularly
the vallate) bear the taste buds. The posterior one-third has no papillae but carries
numerous lymphoid nodules which, with the palatine tonsils and adenoids, make up the
lymphoid ring of Waldeyer. (Ellis, 2006)
Small glands are scattered throughout the submucosa of the dorsum; these are
predominantly serous anteriorly and mucous posteriorly.The tongue is divided by a median
vertical fibrous septum, as indicated on the dorsum by a shallow groove. On each side of
this septum are the intrinsic and extrinsic muscles of the tongue.The intrinsic muscles are
disposed in vertical, longitudinal and transverse bundles; they alter the shape of the
tongue. The extrinsic muscles move the tongue as a whole. They pass to the tongue from
the symphysis of the mandible, the hyoid, styloid process and the soft palate, respectively
the genioglossus, hyoglossus, styloglossus andpalatoglossus. The functions of the
individual extrinsic muscles can be deduced from their relative positions. Genioglossus

11
protrudes the tongue, styloglossus retracts it and hyoglossus depresses it. Palatoglossus
is, in fact, a palatal muscle and helps to narrow the oropharynx in swallowing. (Ellis, 2006)
The mucous membrane on the anterior part of the tongue is rough because of the
presence of numerous small lingual papillae (Moore & Dalley, 2006):
1. Vallate papillae: large and flat topped, they lie directly anterior to the terminal
sulcus and are arranged in a V-shaped row. They are surrounded by deep moat-
like trenches, the walls of which are studded with taste buds. The ducts of the
serous glands of the tongue open into the trenches.
2. Foliate papillae: small lateral folds of the lingual mucosa. They are poorly
developed in humans.
3. Filliform papillae: long and numerous, they contain afferent nerve endings that are
sensitive to touch. These scaly, conical projections are pinkish gray and are
arranged in V-shaped rows that are parallel to the terminal sulcus, except at the
apex, where they tend to be arranged transversely.
4. Fungiform papillae: mushroom shaped pink or red spots, they are scattered among
filliform papillae but are most numerous at the apex and margins of the tongue.

12
Blood supply
Blood is supplied from the lingual branch of the external carotid artery. (Ellis, 2006)
Lymph drainage
The drainage zones of the mucosa of the tongue can be grouped into three: (Ellis, 2006)
1 The tip drains to the submental nodes;
2 The anterior two-thirds drains to the submental and submandibular nodes and
thence to the lower nodes of the deep cervical chain along the carotid sheath;
3 The posterior one-third drains to the upper nodes of the deep cervical chain.
Nerve supply
The anterior two-thirds of the tongue receives its sensory supply from the lingual
branch of V which also transmits the gustatory fibres of the chorda tympani (VII). Common
sensation and taste to the posterior one-third, including the vallate papillae, are derived
from IX. Afew fibres of the superior laryngeal nerve (X) carry sensory fibres from the
posterior part of the tongue.All the muscles of the tongue except palatoglossus are
supplied by XII; palatoglossus, a muscle of the soft palate, is innervated by the pharyngeal
branch of X (Ellis, 2006)
Fissured tongue
Definition
Fissured tongue (FT), also termed lingua fissurata, lingua plicata, scrotal tongue
and grooved tongue is recognized clinically by an groove oriented anteroposteriorly, often
with multiple branch fissures extending laterally. The frequency of FT increases with age
and has been associated with psoriasis, acromegaly, and Sjo¨gren’s, Down’s and

13
Melkerson–Rosenthal syndromes (Zargari, 2005). The fissured tongue (FT) is a condition,
either inherited or acquired, that manifests variable degrees of grooves or fissures on the
tongue dorsum (Silverman et al, 2002). A tongue with fissures on the dorsum (Scully et al,
2010).
Prevalence
About 5% of population. Age mainly affected: More noticeable with increasing age.
Gender mainly affected: M = F (Scully et al, 2010). It is unclear whether FT occurs more
frequently in male or female patients. It has been reported in patients ranging in age from
15 to 84 years (Wood & Goaz, 1997).
Etiology
The etiology is uncertain, because the time when the fissures first appeared
cannot be documented with certainty. Whereas there has been some testimonial
association with nutritional and vitamin deficiencies, this has not been frequent or well-
confirmed (Silverman et al, 2002). For years median rhomboid glossitis (MRG) (central
papillary atrophy of the tongue) has been considered a developmental and congenital
defect causing a segment of the tuberculum impar to persist on the dorsal surface of the
tongue, instead of being buried in normal embryonic development. However, the paucity of
cases in children and some cases of remission has diminished support for this theory. It is
thought that a chronic candidal infection plays a leading etiologic role and smoking may
also act as a promoter. Conflicting reports concern a possible role by diabetes (Wood &
Goaz, 1997).
The etiology is unknown but hereditary plays a significant role. The condition may
be congenital, present at birth, or may become apparent during childhood or later in life.
Ajra examined clinical and genetic characteristics of histologically defined fissured tongue

14
in a familial study and reported that fissured tongue with smooth-surfaced papillae was
transmitted as a dominant characteristic with incomplete penetrance and was preceded by
geographic tongue. The severity of fissured tongue changed with increasing age. Tongue
fissuring with normal appearing filiform papillae was not familial and was not associated
with geographic tongue. Fissuring with normal-appearing structure should be considered
as variation of normal anatomy, whereas fissured tongue and geographical tongue are
clinical and etiological disease entity. Aging and local environmental factors may also
contribute to its development. Fissured tongue may present as an independent
manifestation or associated with certain underlying syndromes or familial
conditions. Conditions associated with fissured tongue include Melkersson-Rosenthal
syndrome, Down syndrome, acromegaly, Sjorgen’s syndrome, oro-facial granulomatosis,
psoriasis and geographic tongue (Rathee et al, 2010).
Clinical findings
Usually asymptomatic. However, it is often complicated by geographic tongue, or
the tongue becomes sore for no apparent reason. Multiple fissures on the dorsum of the
tongue. There is such a wide range of fissuring appearances that there is no standard
classification or adequate description (Scully et al, 2010). Occasionally, when a patient
notices a FT for the first time or feels that the fissures are increasing, there is concern over
the significance. In some patients, there are complaints of discomfort, or coincidental
tongue symptoms; these are eventually shown to be unrelated to the fissuring (Silverman
et al, 2002).
The lesion is located on the dorsal surface of the tongue in the midline and anterior
to the circumvallate papillae. The surface is dusky red, completely devoid of filiform
papillae, and usually smooth; however, nodular or fissured surfaces have been noted.

15
Rarely, there may be some keratosis. The size and shape of the lesion are somewhat
variable, at times causing confusion as to the diagnosis. The lesions are generally
asymptomatic, but pain and ulceration have been reported (Wood & Goaz, 1997).
Fissured tongue is characterized by anteroposterior and multiple laterally fissures on the dorsal aspect of the tongue
Histology
Microscopic examination of fissured tongue reveals hyperplasia of the rete ridges
and loss of the keratin " hairs" on the surface of the filiform papillae. The papillae vary in
size and often arc separated by deepgrooves. Polymorphonuclear leukocytes can be seen
migrating into the epithelium. often forming microabscesses in the upper epithelial layers. A
mixed inflammatory cell in filtrate is present in the lamin a propria. (Neville et al, 2002)
Diagnosis
The diagnosis is made by clinical findings and history. If there are indications of a
systemic disease or condition based on signs and symptoms, then the appropriate referral

16
or laboratory tests should be carried out. By simply stretching the tongue with mild
pressure, the epithelial-lined fissures become obvious (Silverman et al, 2002).
Treatment
The prime treatment involves counseling the patient regarding the benign nature,
the common occurrence, and the lack of association with infections or other conditions or
diseases. Management is empirical, including optimal hygiene and mouthrinses. Rarely,
when a fissure is deep and associated with debris and exudate, débridement and closure
of the defect is in order (Silverman et al, 2002). No treatment is indicated or available.
(Scully et al, 2010)
Prognosis
Excellent. (Scully et al, 2010)
Differential Diagnosis : Geographic tongue
Definition
Geographic tongue (benign migratory glossitis) is an entity of unknown cause and
presents clinincally with loss of the filiform papillae on the dorsal and lateral surfaces of the
tongue sometimes accompanied by an advancing white border with or without erythema
(Rathee et al, 2010). GT, also known as benign migratory glossitis or glossitis areata
migrans, is an inflammatory disorder of unknown aetiology caused by the local loss of
filiform papillae. The condition usually presents as asymptomatic erythematous patches
with serpiginous borders. The patches are irregular and sharply demarcated, resembling a
map. These lesions characteristically have a migratory nature, and their colour and shape
change over time. GT is usually an isolated abnormality but has been associated with

17
psoriasis, atopic diathesis, diabetes mellitus, reactive bronchitis, anaemia, stress,
hormonal disturbances, Reiter’s and Down’s syndromes, and lithium therapy
(Zargari,2005).
Prevalence
Geographical tongue occurs in about 1% of general population, and 50% in
association with fissured tongue (Rathee et al, 2010). The reported prevalence is
approximately 1 per cent of the population and there is often a family history. The disorder
occurs over a wide age range and presents both in children and adults. (Soames &
Southam, 2005)
Etiology
The cause has not been clearly identified. It is considered to be an allergic or
hypersensitivity reaction to certain factors to which the tongue is exposed. This could be a
germ that usually lives in the mouth or a foodstuff. This reaction causes excessive
shedding of cells on the surface of the tongue (Scully et al, 2010).
Clinical findings
Irregular, partially depapillated, red areas on the anterior two-thirds of the dorsal
tongue surface and is associated with loss of the filiform papillae, the fungiform papillae
remaining as shiny, dark-red eminences. The margins of the lesions are often outlined by a
thin, white line or band and the disorder is frequently associated with fissured (scrotal)
tongue . The affected areas may begin as small lesions only a few millimetres in diameter
which, after gradually enlarging, heal and then reappear in another location. The condition

18
may regress for a period and then recur. It is usually symptomless but there may be some
irritation associated with acid and spicy foods. (Soames & Southam, 2005)
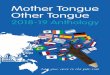
Geographical tongue. Note the atrophic red patches are sharply demarcated, resembling a map
Histology
Histological examination shows the epithelium at the edges of the lesions to be
acanthotic with a dense, neutrophil leucocyte infiltration throughout the epithelium and the
lamina propria. In the centres of the lesions, the loose desquamating cells on the surface
have been lost and there is underlying chronic inflammatory cell infiltration (Soames &
Southam, 2005)
Histologically, there is thinning of the epithelium in the centre of the lesion with
mild hyperplasia and hyperkeratosis at the periphery. There are chronic inflammatory cells
in the underlying connective tissue. The irregular areas of dekeratinized and desquamated
filliform papillae which is red in colour are surrounded by elevated whitish or yellow
margins due to acantholysis and hyperkeratosis. (Cawson & Odell, 2002)..

19
Pathophysiology
Red patches develop and then over a few days coalesce to form rather large areas
of raw-looking patches (Murtagh, 2010). In this condition, localized areas of filliform
papillae are rapidly lost and replaced by uneven areas of smooth dorsal surface lingual
mucosa that is often erythematous because of hyperemia (Sonis et al., 1995). The cause
of lost papillae is still unknown.
The fungiform papillae are exaggerated (Sonis et al., 1995). The papillae on the
tongue surface rapidly regrow and the affected area returns to normal. The process moves
around to other parts of the tongue with a major change occurring every three weeks. The
process may then subside and go into remission that may be complete or partial. However,
it may return at a later time (Murtagh, 2010).
Diagnosis
The diagnosis is based upon clinical appearance and history. When there is
clinical confusion because of a rather bizarre manifestation, or deep concern on the part of
the patient, a biopsy can be performed. (Scully et al, 2010).
Treatment
Most important, patients must be reassured that although this is a chronic or cyclic
condition, GT does not represent a neoplastic, infectious, or contagious disease. Biopsy is
elective. If a patient has generalized complaints or findings, then a physical examination
should be suggested to rule out a coincidental systemic problem. When a patient is
asymptomatic, no further treatment is necessary. Since some patients may be
uncomfortable or experience considerable pain, identifiable irritants (mainly food types)
should be avoided. Symptoms are treated empirically. Trials can include placebos

20
(vitamins), mouthrinses, antianxiety medications, and anti-inflammatory drugs. The latter
can include nonsteroidal anti-inflammatory drugs (NSAIDs) and topical or systemic
corticosteroids. Analgesic agents are sometimes needed. There is no specific treatment,
drug or process that makes it disappear. However, palliation in the form of sprays,
ointments or rinses may be helpful in symptomatic cases (Sonis et al, 1995 ; Scully et al,
2010).
Prognosis
There are no complications. Spontaneous resolution of the lesion in one area is not
uncommon, but usually another lesion appears in another location. (Scully et al, 2010)
Ulcer
Definition and Terminology
Ulcerative lesions are a group of common oral mucosal disorders. The most
common causes of these lesions are mechanical and reactive factors, infectious diseases,
and neoplasms, as well as autoimmune and hematological disorders. The main clinical
feature in all these conditions is an ulcer, which is defined as loss of all epithelial layers. In
addition, the term “erosion” is used to defined a superficial loss of epithelium. However, at
the clinical level, the terms “ulcer” and “erosion” are usually used interchangeably. In this
chapter, only primary ulcerative lesions are discussed, and not lesions that arise
secondarily fromrupture d bullae.(Laskaris, 2006)
Ulceration is a breach in the oral epithelium, which typically exposes nerve
endings in the underlying lamina propria, resulting in pain or soreness, especially when
eating spicy foods or citrus fruits. Patients vary enormously in the degree to which they
suffer and complain of soreness in relation to oral ulceration. It is always important to

21
exclude serious disorders such as oral cancer or other serious disease, but not all patients
who complain of soreness have discernible organic disease. Conversely, some with
serious disease have no pain. Even in those with detectable lesions, the level of complaint
can vary enormously. Some patients with large ulcers complain little; others with minimal
ulceration complain bitterly of discomfort. Sometimes there is a psychogenic influence.
(Scully, 2005)
Erosion which is the term used for superficial breaches of the epithelium. These
often have a red appearance initially as there is little damage to the underlying
lamina propria, but they typically become covered by a fibrinous exudate which
has a yellowish appearance (Scully, 2005).
Ulcer which is the term usually used where there is damage both to epithelium
and lamina propria. An inflammatory halo, if present, also highlights the ulcer with
a red halo around the yellow or grey ulcer (Scully, 2005).
Etiology
(Scully, 2005)
Trauma
Recurrent aphthous stomatitis (RAS)
Microbial infections
Mucocutaneous diseases
Systemic disorders
Drug therapy
Squamous cell carcinoma
Clinical features

22
Acute reactive ulcers of oral mucous membranes exhibit the clinical signs and
symptoms of acute inflammation, including variable degrees of pain, redness, and swelling
The ulcers are covered by a yellow-white fibrinous exudate and are surrounded by an
erythematous halo. Chronic reactive ulcers may cause little or no pain. They are covered
by a yellow membrane and are surrounded by elevated margins that may show
hyperkeratosis. Induration, often associated with these lesions, is due to star formation and
chronic inflammatory cell infiltration (Regezi, 2003).
Oral ulcer at right buccal
Histology
Acute ulcers show a loss of surface epithelium that is replaced by a fibrin network
containing predominantly neutrophils. The ulcer base contains dilated capillaries and, with
time, granulation tissue. Regeneration of the epithelium begins at the ulcer margins, with
proliferating cells moving over the granulation tissue base and under the fibrin clot. Chronic
ulcers have a granulation tissue base, with scar found deeper in the tissue. A mixed
inflammatory cell infiltrate is seen throughout. Epithelial regeneration occasionally may not
occur because of continued trauma or because of unfavorable local tissue factors. It has
been speculated (hat these factors are related to inappropriate adhesion molecule
expression (integrins) and/or inadequate extracellular matrix receptors for the keratinocyte
integrins. In traumatic granulomas, tissue injury and inflammation extend into subjacent
skeletal muscle. The term granuloma as used here reflects the large numbers of

23
macrophages that dominate the infiltrate, but this is not a typical granuloma as seen in an
infectious process, such as tuberculosis. (Regezi et al,2003)
Histological examination shows an ulcer covered by a thick layer of fibrinous
exudate with a dense, chronic inflammatory cell infiltrate in its base involving underlying
damaged muscle. The deeper parts of the lesion are characterized by an infiltrate rich in
histiocytes and eosinophils (Soames, 2005).
Treatment
Management involves the elimination of the suspected cause and use of an
antiseptic mouthwash (for example, 0.2 per cent chlorhexidine) or a simple covering agent
such as Orabase). Ulcers of local cause usually heal spontaneously within 7–14 days if the
cause is removed. Maintenance of good oral hygiene and the use of hot saline mouthbaths
and 0.2% aqueous chlorhexidine gluconate mouthwash aid healing. Occasionally,
particularly in self-induced trauma, mechanical protection with a plastic guard may help.
Patients should be reviewed within three weeks to ensure healing has occurred. Any
patient with a single ulcer lasting more than 2–3 weeks should be regarded with suspicion
and investigated further; biopsy may be indicated. Most reactive ulcers of oral mucous
membranes arc simply observed. If pain is considerable, topical treatment may be of
benefit. This could be in the form of a topical corticosteroid (Regezi,2003; Scully, 2010 )

24
CHAPTER IV
DISCUSSION
The patient complained that his tongue has crack and groove on surface of his
tongue. Patient said that he never had any discomfort or pain but he finds it difficult to
clean and sometime there are white coatings on the tongue. Patient also complaints of
ulceration on right cheek. The ulcers form around 3 days ago. The patient did not recall
any bitting or traumatizing at the ulcer location and not taking any medication for the ulcers.
Extraoral examination and anemnesis showed no underlying systemic disease of
the patient that may manifest in the oral cavity. After intraoral examination, it is found that
there are fissuring on the dorsum and lateral side of the tongue. According to the patient,
the lesion never caused him any pain or discomfort but sometimes making cleaning the
tongue hard. This is consistent with statement from Silverman et al (2001), Scully et al
(2010), Wood & Goaz (1997) and Neville et al (2002) which state that fissure tongue are
usually asymptomatic. The patient also revealed ulcerations on the buccal right. The ulcer

25
healed 5 days after the first visit. According to Regezi and Scully,ulceration in oral mucosa
usually heal spontaneously within 7-14 days.
The patient was explained about his condition and the nature of fissure tongue.
According to Scully, fissured tongue progress with age. The patient was informed about
this progression of fissured tongue and was advised to not concern himself as long as the
patient does not feel any discomfort or pain and practices good oral hygiene. The patient
was reassure that good oral hygiene is a sufficient way to manage his treatment. The
patient is instructed to maintain a good oral hygiene. In addition to daily brushing, the
patient was instructed to scrape the tongue to ensure torough cleaning of the oral cavity.
This is to make sure that food debris and microorgannism will not accumulate and reside
between the groves and fissure. The treatment prescribed is antiseptic Chlorhexidine
gluconate 0.2% mouthrinse as it has antimicrobial properties to fight against germs and
bacteria. Antiseptic is a solution used to disinfect skin or other living tissue (Burton &
Engelkirk, 1996). Antimicrobial agent is defined as an agent that can kill or inhibit microbial
growth (Prescott, Harley & Klein, 2002). Chlorhexidine is used twice daily with 30 to 60
seconds gargling until the ulcer subsides.. This is also to make sure that there are no
secondary infection at the ulcers. Chlorhexidine gluconate is only advised to be used for 7-
14 days. It is known that prolonged usage or chlorhexidine can cause staining of tongue
and change of oral microflora (Yagiela, Dowd & Neidle, 2007).
Then, the lesion is examined again after 1 week. The ulcer on the buccal right
already healed. The patient has no complaints and has been using tongue scraper to helps
with the cleansing of the tongue surface. There is no specific management and treatment
for fissured tongue. The patient need optimal hygiene and mouthrinses in order to prevent
any progress or occurance of infection (Silverman et al, 2002; Scully et al, 2010).

26
CHAPTER V
CONCLUSSION
Based on the anamnesis and clinical examination, all the patient’s symptoms and the
clinical features of the lesion fulfill the criteria of diagnosing fissure tongue. According to
literature, no specific treatment was stated, the patient was instructed to maintaine good
oral hygine and encourage to scrape his tongue for a better removal of food debris. After a
week the patient is called back for control and the patient didn’t have any complaints.

27
REFERENCES
Better Health Channel, 2010. Tongue. P. 1-4. Available online at www.betterhealth.vic.gov.au.
Burton R and Engelkirk R;1996 Microbiology for the Health Sciences. 5 th ed. Lippincott. p. 125-126
Cawson, R.A. & Odell, E.W., 2006. Essential Pathology and Oral Medicine. 7th edition. Churchill Livingstone.
Ellis H. 2006.Clinical anatomy: applied anatomy for students and junior doctors .Wiley-Blackwell.
John Hopkins, 2008. Symptoms and Remedies: The Complete Home Medical References. Remedy Health Media, LLC.Available online at http://www.johnshopkinshealthalerts.com
Laskaris G, 2006, Pocket Atlas of Oral Diseases. Thieme
Moore & Dalley, 2006. Clinically Oriented Anatomy. 5th edition. Lippincott Williams & Wilkins
Neville B.W. Douglas D. Damm. Terry A Day .2002. Oral and maxillofacial pathology. Saunders/Elsevier
Prescott LM, Harley JP & Klein DA, 2002. Microbiology 5th Ed. Boston Mc Graw-Hill Higher Education. p. 806-812
Rathee M, A. Hooda & A. Kumar. 2010.Fissured Tongue: A Case Report and Review of Literature. The Internet Journal of Nutrition and Wellness. 10(1)
Regezi, Sciubba, Jordan.2003.Oral Pathology: Clinical Pathologic Correlations 4th ed. Saunders
Scully C. Oslei Paes de Almeida, Jose Bagan, Pedro Diz Dios, Adalberto Mosqueda Taylor. 2010. Oral Medicine and Pathology at a Glance .John Wiley and Sons.
Scully C. Felix DH. 2005.Oral medicine — Update for the dental practitioner Aphthous and other common ulcers, British Dental Journal ; 199:259–264

28
Silverman S, Lewis R.E, Edmond L.T, 2002,Essentials of oral medicine. PMPH-USA
Soames JV, Southam JC .2005.Oral Pathology - 4th Ed.
Sonis, Fazio & Fang 1995, Principles and Practices of Oral Medicine, 2nd ed. W.B. Saunders Company.
Wood NK, Goaz PW. 1997.Differential diagnosis of oral lesions. 5th ed. St. Louis: Mosby,
Yagiela JA,Frank J. Dowd,Bart Johnson,Angelo Mariotti,and Enid A. Neidle,2007. Pharmacology and Therapeutics for Dentistry, 4th Edition
Zargari O.2006. The prevalence and significance of fissured tongue and geographical tongue in psoriatic patients.Clinical and Experimental Dermatology, 31, 192–195