Embed Size (px)
DESCRIPTION
Fishing for a Diagnosis - “Nervous” infections. Neurology Grand Rounds 08 January 2009 Antony Thomas Consultant Neurologist UHCW & Alexandra hospital Redditch. Best Wishes for a Happy, successful, peaceful and prosperous New Year to all. RC. 23 years, Right handed, sheep farmer - PowerPoint PPT Presentation
Citation preview
Fishing for a Diagnosis -“Nervous” infections
Neurology Grand Rounds08 January 2009
Antony ThomasConsultant Neurologist
UHCW & Alexandra hospital Redditch
Best Wishes for a Happy, successful, peaceful and prosperous New Year to all.
RC
• 23 years, Right handed, sheep farmer• Well until 8/05/08
– Occipital headache: severe– Nausea, vomiting– Blurred vision, double vision– Dribbling– “behaves as drunk” slurred speech, dizziness
and unsteady – Weak right face with failure to close right eye
RC
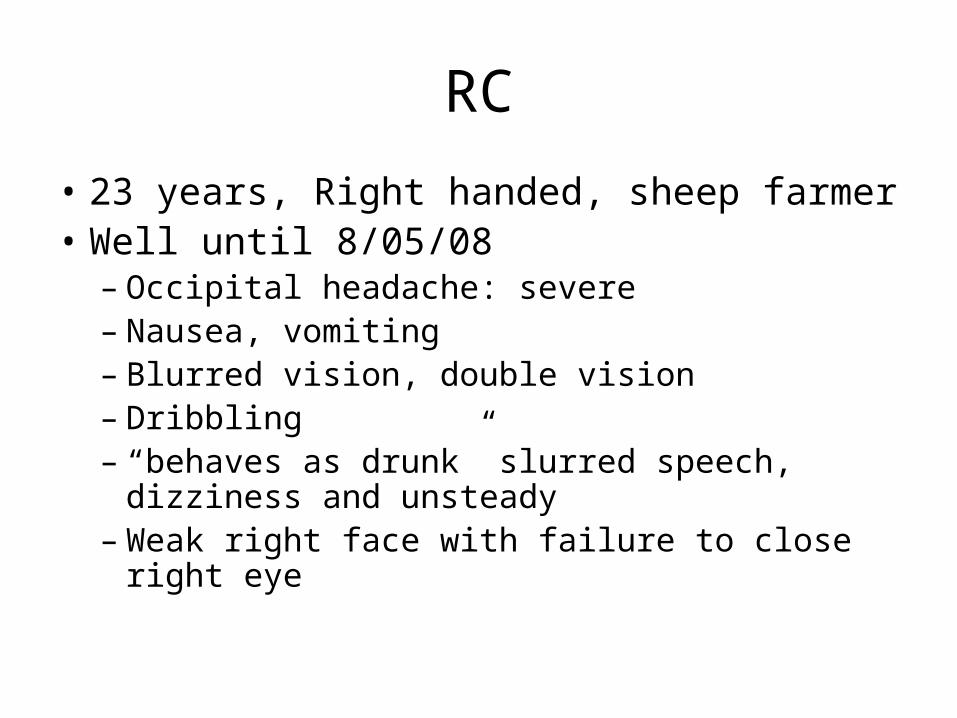
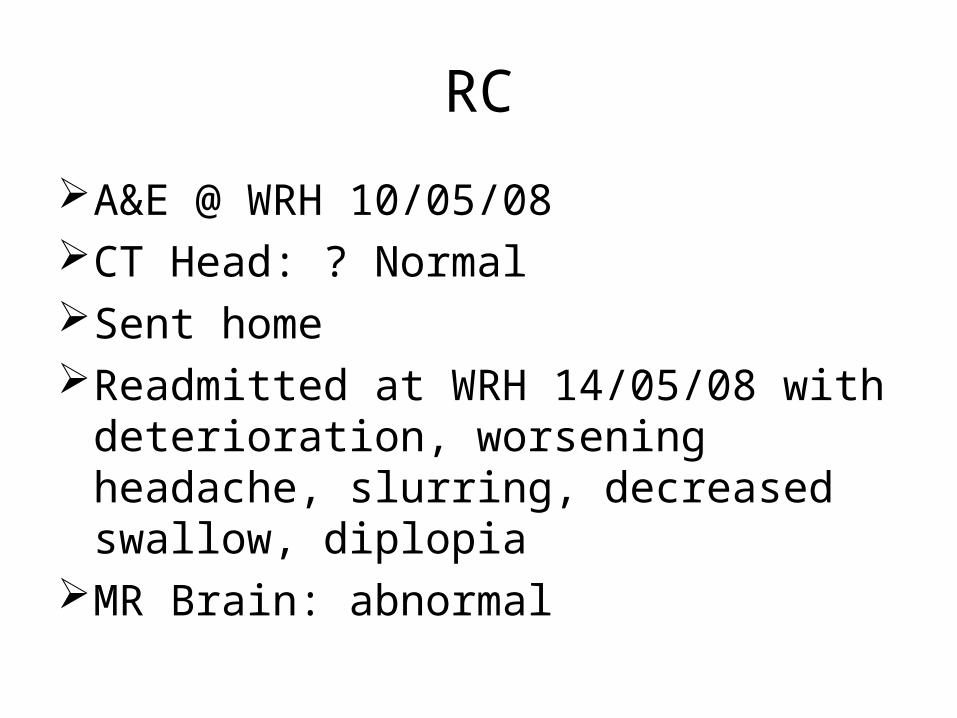
A&E @ WRH 10/05/08CT Head: ? NormalSent homeReadmitted at WRH 14/05/08 with
deterioration, worsening headache, slurring, decreased swallow, diplopia
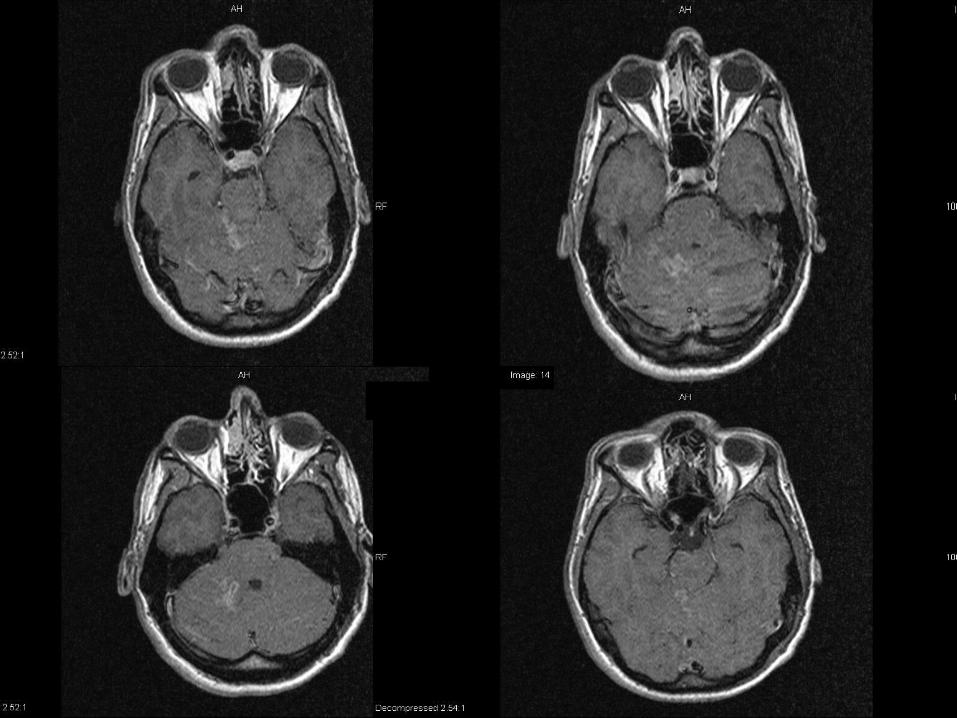
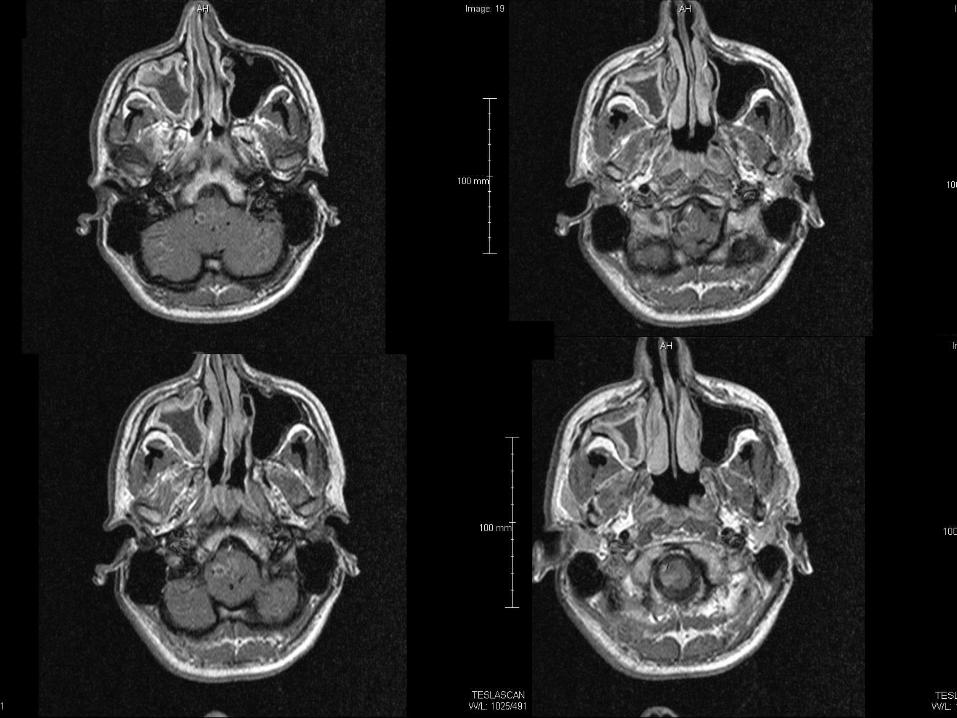
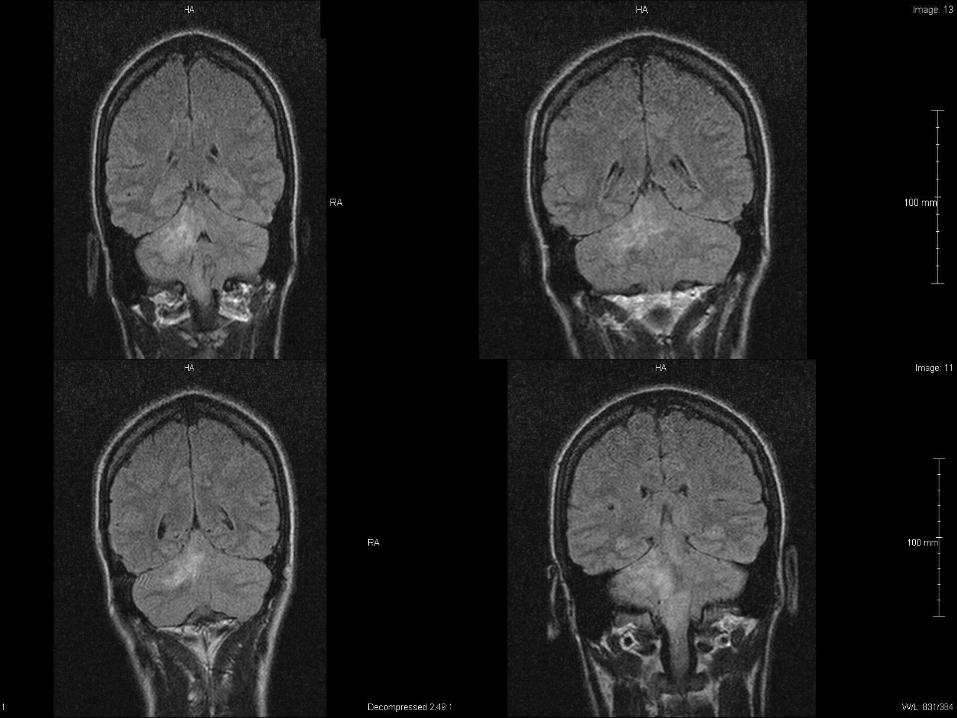
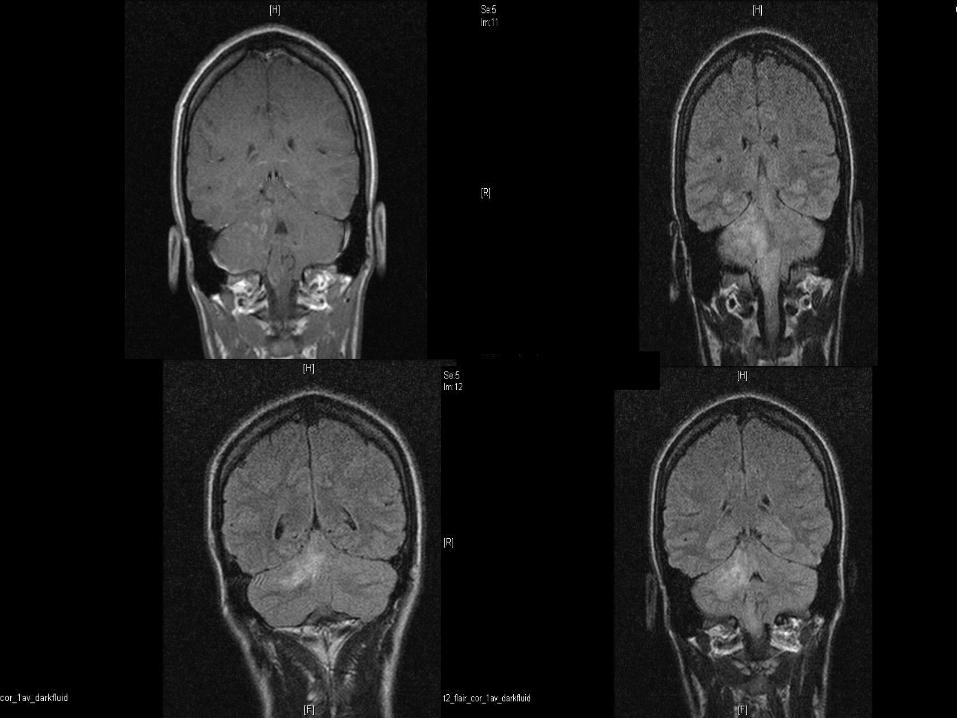
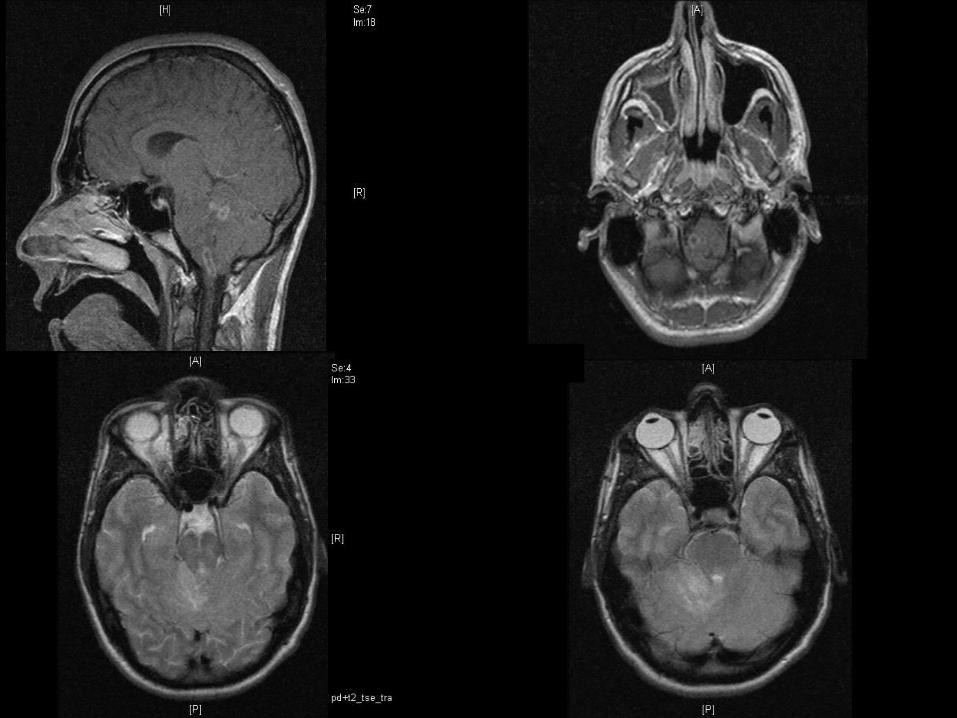
MR Brain: abnormal
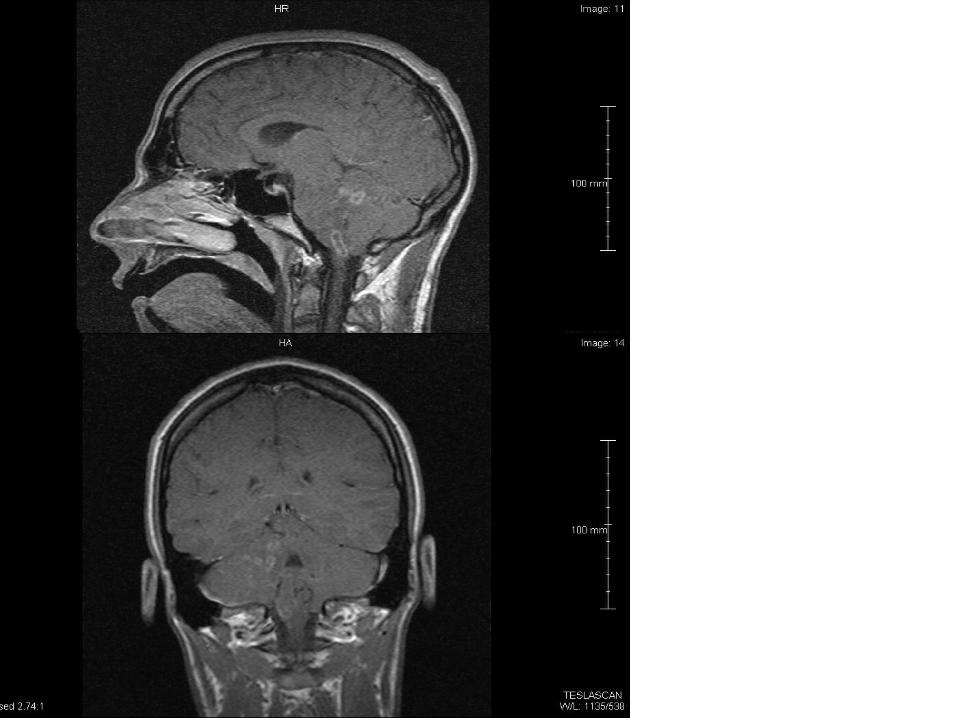
Transferred to Neurosurgery UHCW 16th
Pyrexial GCS 15, no papilledema Right V1 sensory impairement Right eye abduction weakness Bilateral nystagmus R>L Right Facial weakness LMN Bulbar paresis, dysarthria, right sided tongue weakness Mild right sided weakness and minimal sensory
impairement Right sided cerebellar signs Rest of the systemic examination unremarkable
Investigations
• Leukocytosis, Neutrophilia, Monocytosis
• Impaired LFT
• Deteriorating Renal functions
• CRP normal 85 172
• Autoantibodies: negative
• HIV: Negative
• Serum ACE: normal
Microbiology @ Worcester
Telephone call
Blood culture (14/05 sample): grown Listeria
Started on antibiotics after repeating cultures
Amoxicillin 2G Q4HGentamicin
Progress
• Respiratory distress
• Poor cough, inadequate gag
• Throat suction: thick yellowish secretions
• Hypoxic, hypercapneic
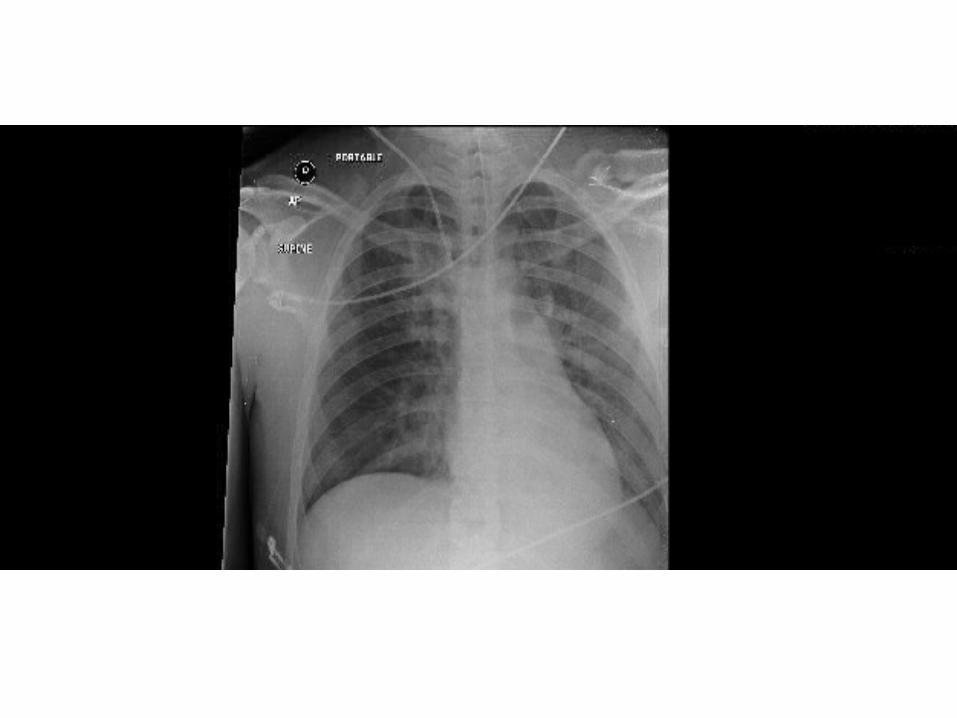
• Chest crackles more on right lower base
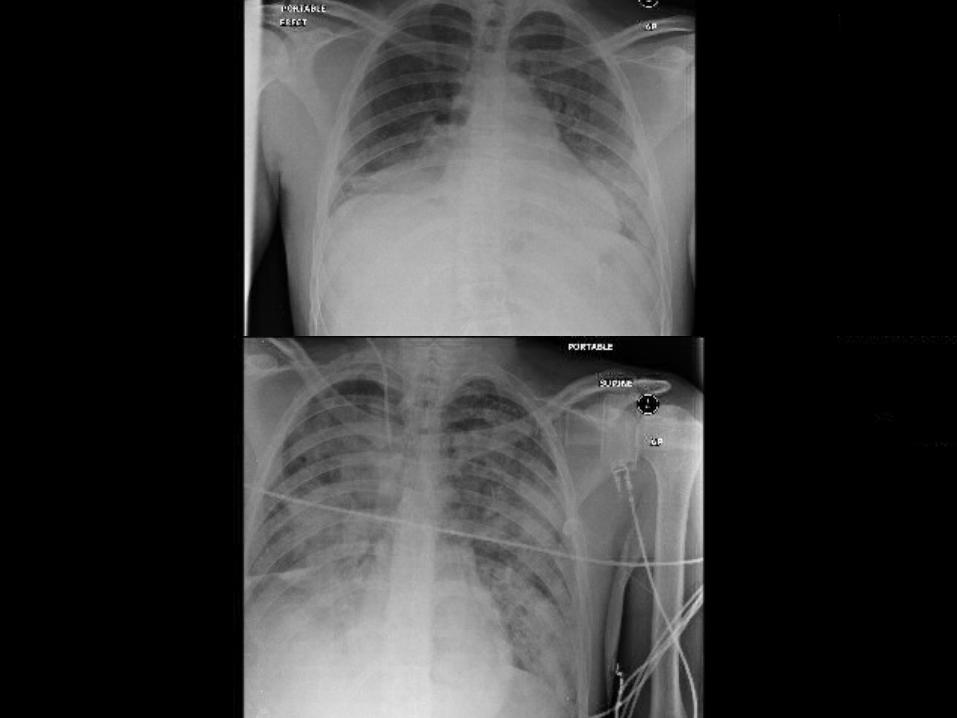
• CXR: Right lower lobe opacity
Transfer to ITU
Intubated and ventilated
ARDS: on oscillator
Hydrocortisone
Co-trimoxazole added
Repeat MR Brain: similar findings
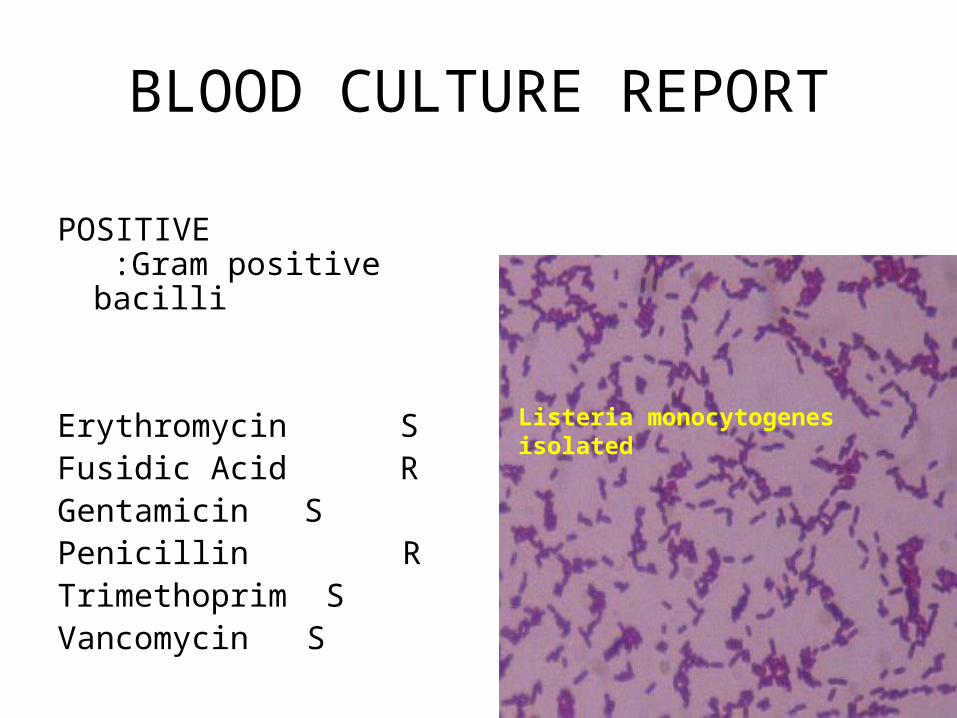
BLOOD CULTURE REPORT
POSITIVE :Gram positive bacilli
Erythromycin S Fusidic Acid R Gentamicin S Penicillin R Trimethoprim S Vancomycin S
Listeria monocytogenes isolated
Progress
Cardiorespiratory arrest x 2
Succesful CPR
Amiodarone
Gradually improved
CXR got better
Progress
• Unfortunately…………………
• Desaturating
• More ventilatory requirements
• Worsening respiratory, liver and renal functions
• Pupil unequal and dialated
• R.I.P
Listeria Monocytogenes
• Meningo-encephalitis: common
• Immunocompromised & debilitated individuals
• In new born, well known and often fatal
• CSF – pleocytosis (initially polymorphonuclear)
• Rarely normal CSF
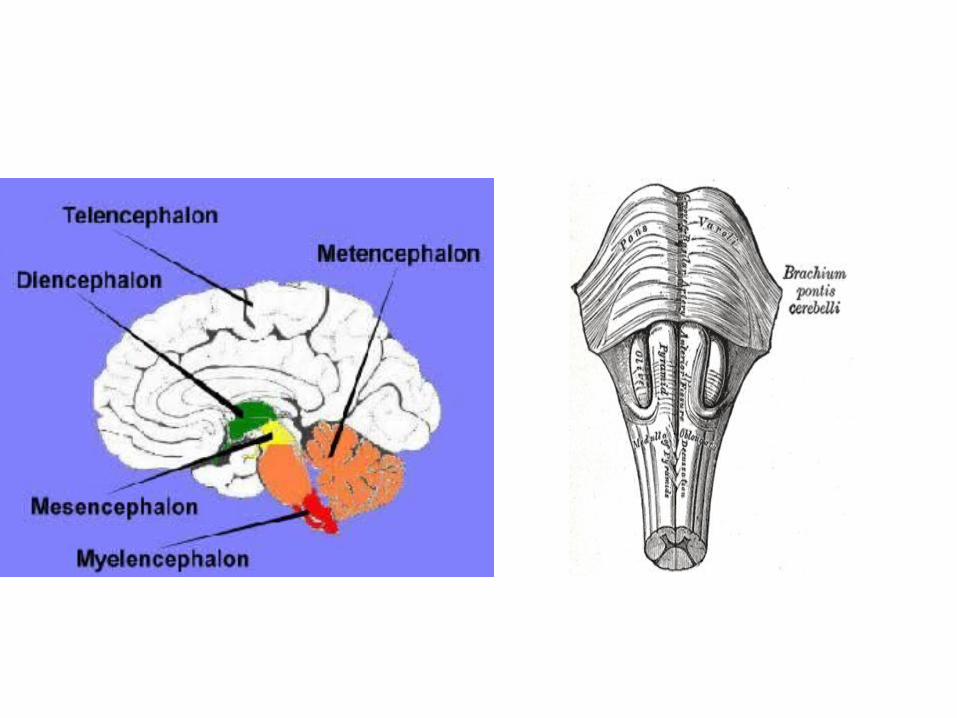
• Rhombencephalitis
Listeria
• Early CT scan normal
• Multiple abscesses in the brain
• Monocytosis
CNS Infections
• Meninges and subarachnoid space can be infected by viruses, bacteria, spirochaetes and fungi
• Virus and bacteria: seasonal variation
• Classic case unmistakable
• But subtle presentations can lead to fatal delay in diagnosis
Typical acute meningitis
• Pyrexia
• Severe headache
• Phtophobia
• Rapid development of neck stiffness
• Kernig’s sign, Brudzinski sign
• If untreated vomiting, drowsiness and eventually coma
Viral causes
• Meningitis– Entero ((Echo,polio,
coxsackie)– HSV2– Lymphocytic
choriomeningitis– VZ– Mumps– HIV
• Encephalitis– HSV– VZ– CMV– EBV– HIV– Mumps– Measles– Rabies– Arbo
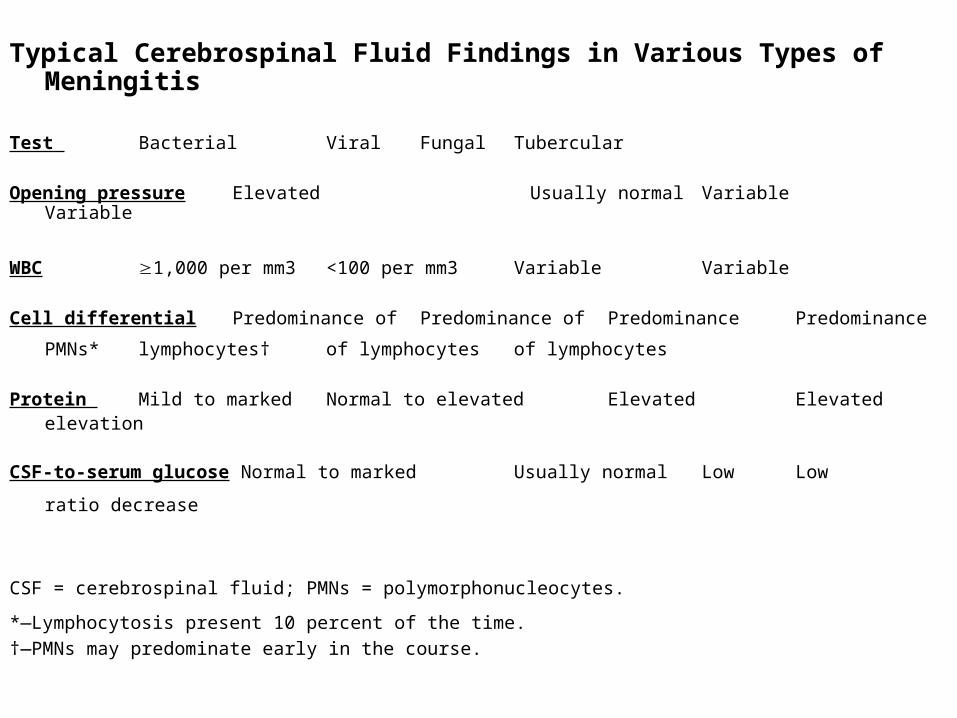
Typical Cerebrospinal Fluid Findings in Various Types of Meningitis
Test Bacterial Viral Fungal Tubercular
Opening pressure Elevated Usually normal Variable Variable
WBC ≥1,000 per mm3 <100 per mm3 Variable Variable
Cell differential Predominance of Predominance of Predominance Predominance
PMNs* lymphocytes† of lymphocytes of lymphocytes
Protein Mild to marked Normal to elevated Elevated Elevated elevation
CSF-to-serum glucose Normal to marked Usually normal Low Low
ratio decrease
CSF = cerebrospinal fluid; PMNs = polymorphonucleocytes. *—Lymphocytosis present 10 percent of the time. †—PMNs may predominate early in the course.