Embed Size (px)
Citation preview
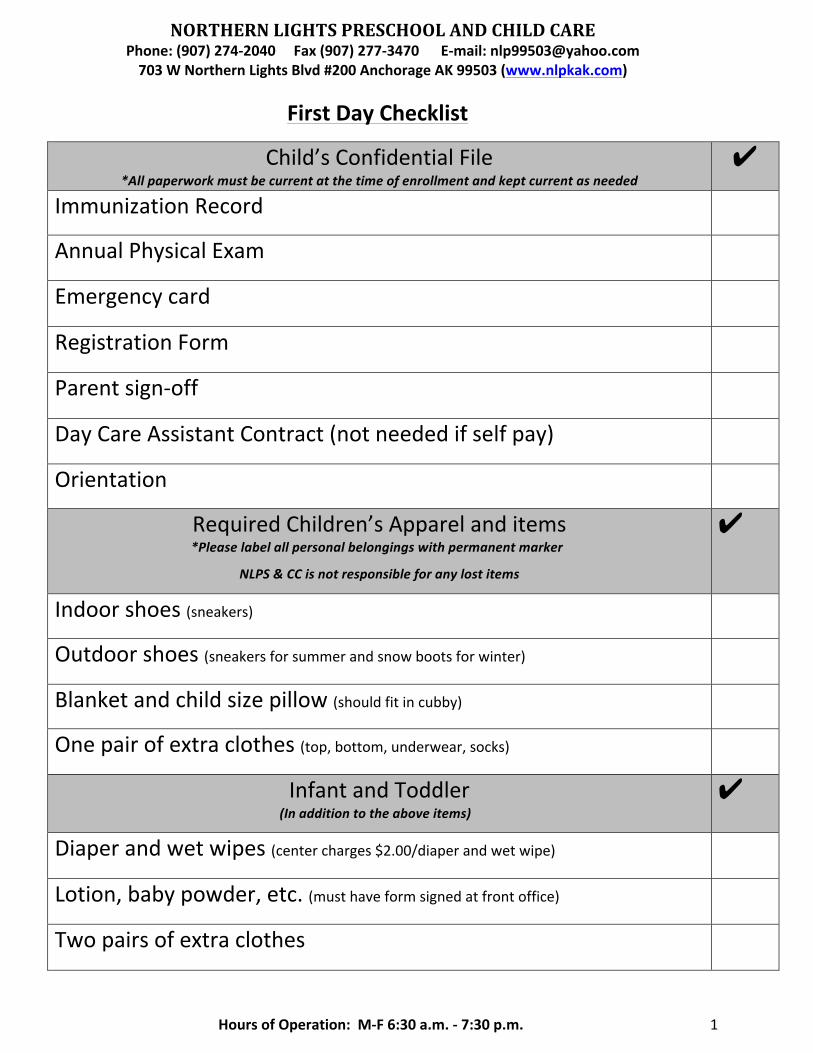
NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 1
FirstDayChecklist
Child’sConfidentialFile*Allpaperworkmustbecurrentatthetimeofenrollmentandkeptcurrentasneeded
✔
ImmunizationRecord
AnnualPhysicalExam
Emergencycard
RegistrationForm
Parentsign-off
DayCareAssistantContract(notneededifselfpay)
Orientation
RequiredChildren’sApparelanditems*Pleaselabelallpersonalbelongingswithpermanentmarker
NLPS&CCisnotresponsibleforanylostitems
✔
Indoorshoes(sneakers)
Outdoorshoes(sneakersforsummerandsnowbootsforwinter)
Blanketandchildsizepillow(shouldfitincubby)
Onepairofextraclothes(top,bottom,underwear,socks)
InfantandToddler(Inadditiontotheaboveitems)
✔
Diaperandwetwipes(centercharges$2.00/diaperandwetwipe)
Lotion,babypowder,etc.(musthaveformsignedatfrontoffice)
Twopairsofextraclothes

NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 2
RegistrationForm
StartDate://20
SectionI:Child’sInformation
Name(firstandlast): Age:
DOB: Placeofbirth: Gender:☐Male☐Female
Address: SS#:
City: State: Zip: Primary/2ndLanguage:
Phone#
PreviousChildcarefacility:
SectionII:FamilyInformation
Father/GuardianName:
Employer: SS#:
Position: Work#: DL#:
Mobile#: Home#:
Mother/GuardianName:
Employer: SS#:
Position: Work#: DL#:
Mobile#: Home#:
EmergencyContactName:
Phone#: Relationship:
NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 3
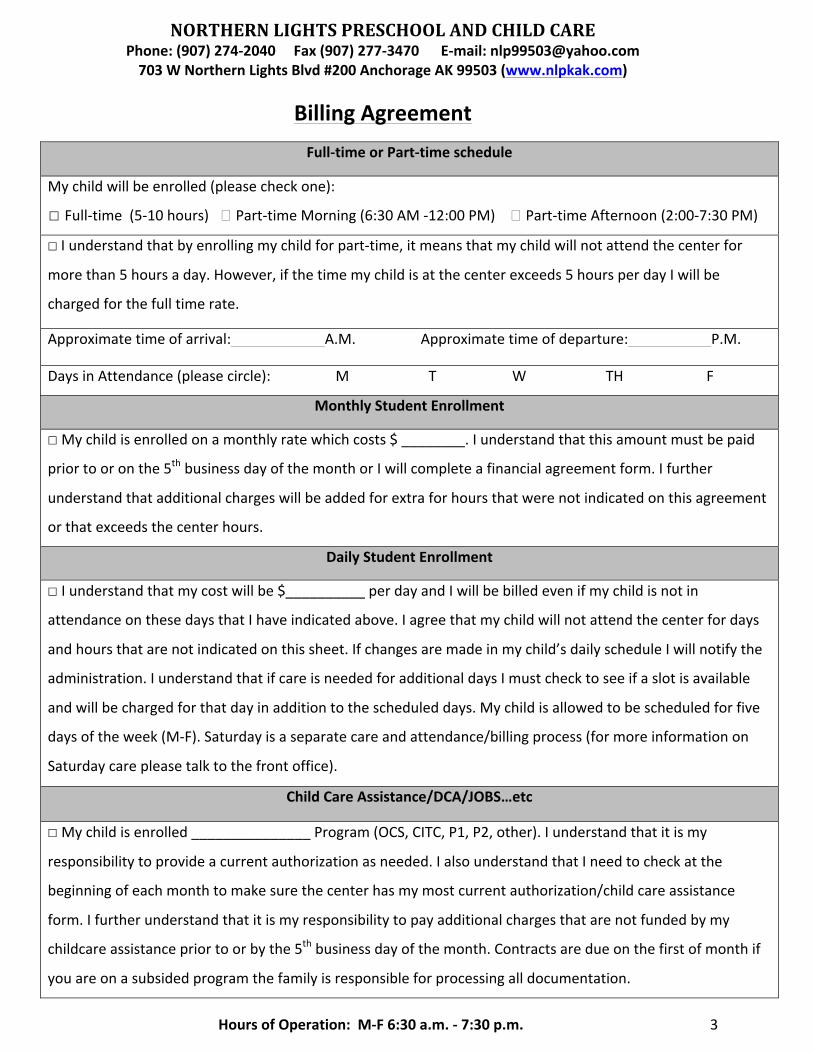
BillingAgreementFull-timeorPart-timeschedule
Mychildwillbeenrolled(pleasecheckone):
☐Full-time(5-10hours)�Part-timeMorning(6:30AM-12:00PM)�Part-timeAfternoon(2:00-7:30PM)
☐Iunderstandthatbyenrollingmychildforpart-time,itmeansthatmychildwillnotattendthecenterfor
morethan5hoursaday.However,ifthetimemychildisatthecenterexceeds5hoursperdayIwillbe
chargedforthefulltimerate.
Approximatetimeofarrival:A.M.Approximatetimeofdeparture:P.M.
DaysinAttendance(pleasecircle):MTWTHF
MonthlyStudentEnrollment
☐ Mychildisenrolledonamonthlyratewhichcosts$________.Iunderstandthatthisamountmustbepaid
priortooronthe5thbusinessdayofthemonthorIwillcompleteafinancialagreementform.Ifurther
understandthatadditionalchargeswillbeaddedforextraforhoursthatwerenotindicatedonthisagreement
orthatexceedsthecenterhours.
DailyStudentEnrollment
☐ Iunderstandthatmycostwillbe$__________perdayandIwillbebilledevenifmychildisnotin
attendanceonthesedaysthatIhaveindicatedabove.Iagreethatmychildwillnotattendthecenterfordays
andhoursthatarenotindicatedonthissheet.Ifchangesaremadeinmychild’sdailyscheduleIwillnotifythe
administration.IunderstandthatifcareisneededforadditionaldaysImustchecktoseeifaslotisavailable
andwillbechargedforthatdayinadditiontothescheduleddays.Mychildisallowedtobescheduledforfive
daysoftheweek(M-F).Saturdayisaseparatecareandattendance/billingprocess(formoreinformationon
Saturdaycarepleasetalktothefrontoffice).
ChildCareAssistance/DCA/JOBS…etc
☐ Mychildisenrolled_______________Program(OCS,CITC,P1,P2,other).Iunderstandthatitismy
responsibilitytoprovideacurrentauthorizationasneeded.IalsounderstandthatIneedtocheckatthe
beginningofeachmonthtomakesurethecenterhasmymostcurrentauthorization/childcareassistance
form.Ifurtherunderstandthatitismyresponsibilitytopayadditionalchargesthatarenotfundedbymy
childcareassistancepriortoorbythe5thbusinessdayofthemonth.Contractsaredueonthefirstofmonthif
youareonasubsidedprogramthefamilyisresponsibleforprocessingalldocumentation.

NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 4
BillingAgreementEffectiveJanuary1,2018
Infant/Toddler Full-time Part-time (FT/PT)DropIn
5Day 850 600 60/50
4Day 750 550 60/50
3Day 650 500 60/50
PreschoolAge Full-time Part-time (FT/PT)DropIn
5Day 700 560 50/40
4Day 600 500 50/40
3Day 500 450 50/40
SchoolAge Full-time Part-time(AM/PM) (FT/PT)DropIn
5Day 745 550summer/420/375a/400p 50/40
4Day 645 500summer/420/365a/375p 50/40
3Day 545 450summer/420/355a/365p 50/40
Toddler:15-35monthsPreschoolage:36mo.-4yearsSchoolage:5-12years
OtherFees
RegistrationFeeof$75.00/childannuallyisdueeverySeptember.LatePickupFeeis$2/minuteperchildoverthe10-hourlimit.Additional$200permonthifover10hourcareisnecessary.LateTuitionFee$50willbechargedafterthe5thdayandafterthe20tha$100latefeewillbeapplied.NSFFeeforreturnedchecksis$25andallNSFchecksandfeestobepaidincash.
Drop-in/Drop-offtimeinformation
Drop-instudentsmustcallpriortoarrival(preferablyminimum1daybefore-hand)tocheckforspaceavailability.Nochildrencanbedroppedoffbetween10AM–2PM
WithdrawalTwoweekswrittennoticeisrequiredforwithdrawalofyourchildfromourprogram.Fromthedateofreceivingsuchnotice,ourcenterwillchargetuitionfeesuptothedateofwithdrawal.Alltuitionsarenon-refundable.Ifchildhasbeenabsentoverfivedayswithoutnoticechildwillberemovedfromourattendancelist.Parent/GuardianSignature: Date:
NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 5
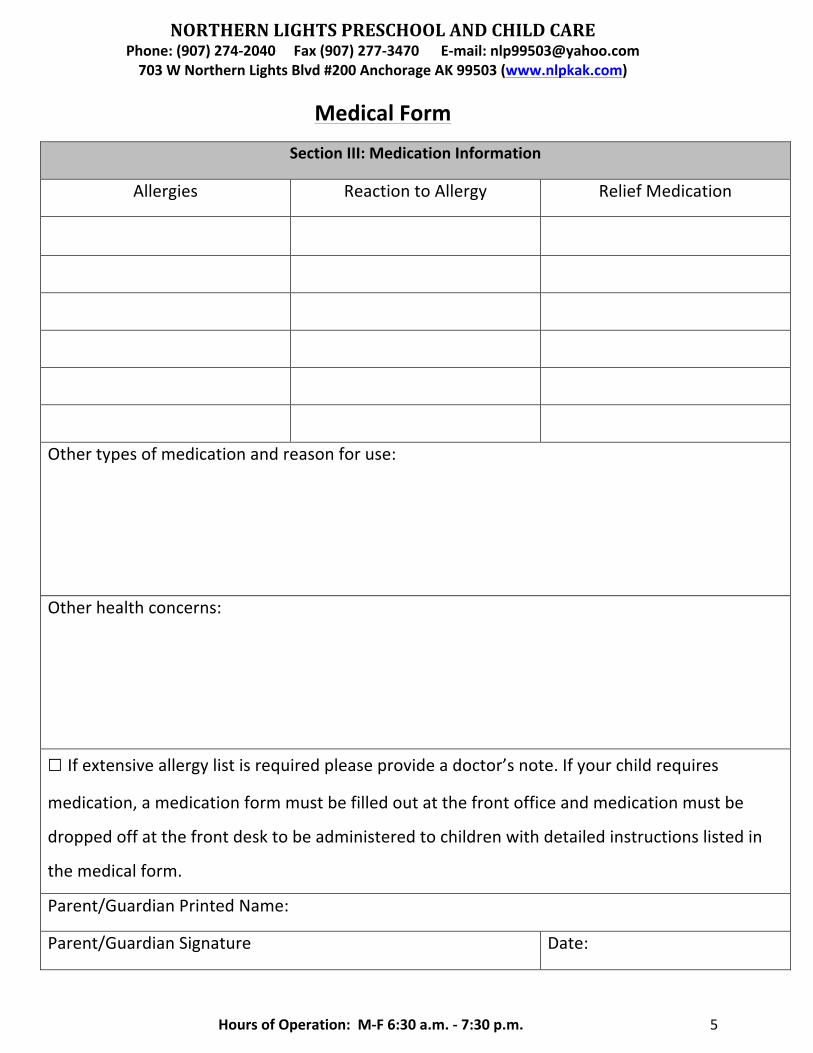
MedicalForm
SectionIII:MedicationInformation
Allergies ReactiontoAllergy ReliefMedication
Othertypesofmedicationandreasonforuse:
Otherhealthconcerns:
☐Ifextensiveallergylistisrequiredpleaseprovideadoctor’snote.Ifyourchildrequiresmedication,amedicationformmustbefilledoutatthefrontofficeandmedicationmustbe
droppedoffatthefrontdesktobeadministeredtochildrenwithdetailedinstructionslistedin
themedicalform.
Parent/GuardianPrintedName:
Parent/GuardianSignature Date:

NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 6
PermissionSlipforPictures
☐IgivepermissionforNorthernLightsPreschooltotakepicturesofmychildduringnormal
classroomsittings,formalpictureday,artworkpostedontheNLPSwebsiteandfor
yearbook(ifapplicable)
Child’sName:
Parent/GuardianPrintedName:
Parent/GuardianSignature: Date:
�IgivepermissionforNorthernLightsPreschooltotakepicturesofmychildduringformal
picturedayonly
Child’sName:
Parent/GuardianPrintedName:
Parent/GuardianSignature: Date:
☐Idonotwantmychild’spicturetakenorsharedonNLPS&CCwebsiteortakenduring
formalpicturedayevents
Child’sName:
Parent/GuardianPrintedName:
Parent/GuardianSignature: Date:
ChildPhysicalExaminationForm

NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 7
PhysicalExaminationrequiredbyMunicipalOrdinance16.55.090Children’sCareCenterStudentName: DOB:School:Parent/GuardianName:Address:Homephone#:Dateofphysicalexamination:// Parentpresentatexamination:�Y�N
AssessmentEyes: Height:Ears: Weight:Noseandthroat: Vision:Mouth: Medication:Teeth:Lymphnode:Heart:Lungs:Abdomen:Genitals:Orthopedic:Nervoussystem:Skin:Nutrition:Endocrine:Other/positivefindings:
Abletoparticipateinusualgroupactivities?�Y�NProvider’sSignature Date:
*Physician’sOfficestamp(required)
Parent/GuardianSignOff
NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 8
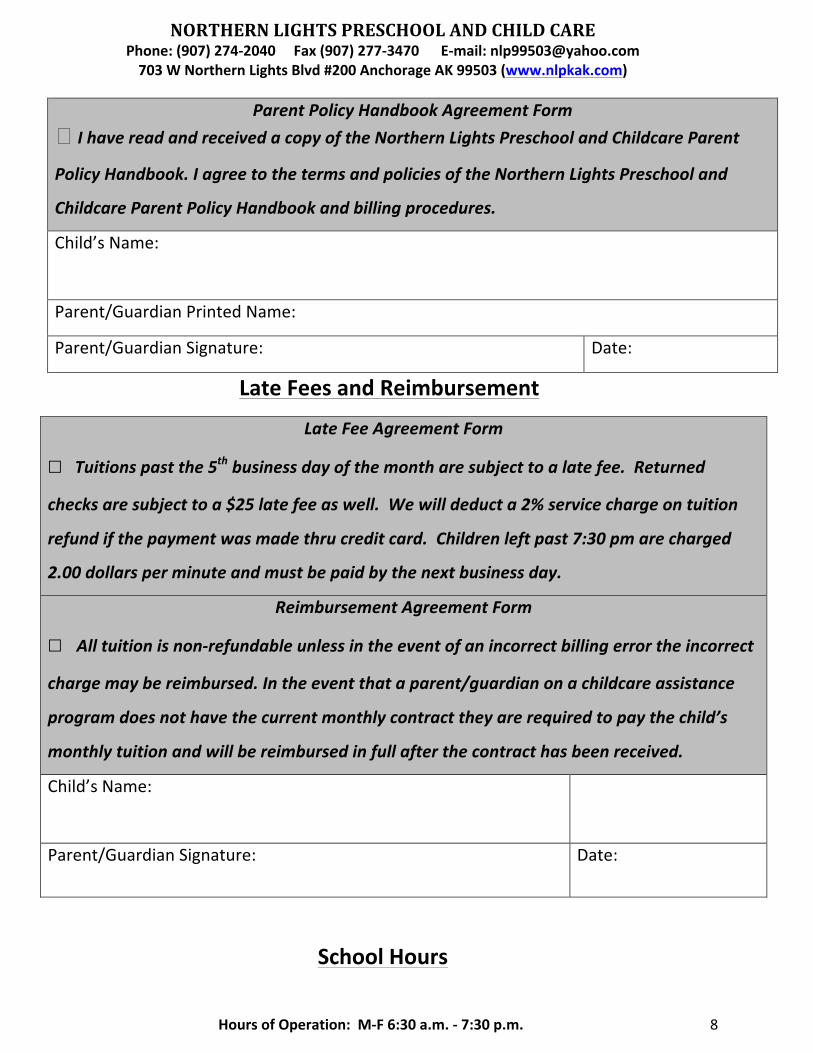
ParentPolicyHandbookAgreementForm�IhavereadandreceivedacopyoftheNorthernLightsPreschoolandChildcareParent
PolicyHandbook.IagreetothetermsandpoliciesoftheNorthernLightsPreschooland
ChildcareParentPolicyHandbookandbillingprocedures.
Child’sName:
Parent/GuardianPrintedName:
Parent/GuardianSignature: Date:
LateFeesandReimbursement
LateFeeAgreementForm
☐Tuitionspastthe5thbusinessdayofthemontharesubjecttoalatefee.Returned
checksaresubjecttoa$25latefeeaswell.Wewilldeducta2%servicechargeontuition
refundifthepaymentwasmadethrucreditcard.Childrenleftpast7:30pmarecharged
2.00dollarsperminuteandmustbepaidbythenextbusinessday.
ReimbursementAgreementForm
☐ Alltuitionisnon-refundableunlessintheeventofanincorrectbillingerrortheincorrectchargemaybereimbursed.Intheeventthataparent/guardianonachildcareassistance
programdoesnothavethecurrentmonthlycontracttheyarerequiredtopaythechild’s
monthlytuitionandwillbereimbursedinfullafterthecontracthasbeenreceived.
Child’sName:
Parent/GuardianSignature: Date:
SchoolHours

NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 9
Ourschoolisopenfrom6:30am-7:30pmMondaythroughFriday.Ifyoupickyour
child/childrenupafter7:30pmyouwillbecharged$2perminuteperchildeveryminuteyou
arelate.Similarfeesapplytochildrenexceedinga10-hourlimitfortheday.Ifyouneed
extrahoursa$200feeappliesamonth
Evenifyouhavearrangedforsomeoneelsetopickupyourchildandtheyarelate,youas
theparent/guardianareresponsibletopayforthislatefee.Thelatefeemustbepaidin
cashbyorbeforethecloseofthenextday,andifnot,yourchildwillnotbeabletoattend
untilthebalanceisfullypaid.
Ifyouhavequestionspleasefeelfreetoaskatthefrontoffice.
� Iunderstandthatitismydutytopickupmychild/childrenontime.Alllatefeesaremy
responsibilitytopay.
Parent/GuardianSignature: Date:
NLPCCDATESOFCLOSURE:

NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 10
HolidayClosures
Date Holiday
01/01 NewYearsDay
01/15 MartinLutherKingJr.Day
02/19 President’sDay
03/30 GoodFriday
05/28 MemorialDay
07/04 IndependenceDay
09/03 LaborDay
11/11 Veteran’sDay
11/22 ThanksgivingDay
11/23 FridayAfterThanksgivingDay
12/24 ChristmasEve
12/25 ChristmasDay
12/31 NewYearsEve

NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 11
USDA Nondiscrimination Statement
In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its Agencies, offices, and employees, and institutions participating in or administering USDA programs are prohibited from discriminating based on race, color, national origin, sex, disability, age, or reprisal or retaliation for prior civil rights activity in any program or activity conducted or funded by USDA. Persons with disabilities who require alternative means of communication for program information (e.g. Braille, large print, audiotape, American Sign Language, etc.), should contact the Agency (State or local) where they applied for benefits. Individuals who are deaf, hard of hearing or have speech disabilities may contact USDA through the Federal Relay Service at (800) 877-8339. Additionally, program information may be made available in languages other than English. To file a program complaint of discrimination, complete the USDA Program Discrimination Complaint Form, (AD-3027) found online at: http://www.ascr.usda.gov/complaint_filing_cust.html, and at any USDA office, or write a letter addressed to USDA and provide in the letter all of the information requested in the form. To request a copy of the complaint form, call (866) 632-9992. Submit your completed form or letter to USDA by: (1) mail: U.S. Department of Agriculture Office of the Assistant Secretary for Civil Rights 1400 Independence Avenue, SW Washington, D.C. 20250-9410; (2) fax: (202) 690-7442; or (3) email: [email protected]. This institution is an equal opportunity provider.
NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 12
NORTHERNLIGHTSPRESCHOOLANDCHILDCAREPhone:(907)274-2040Fax(907)277-3470E-mail:[email protected]#200AnchorageAK99503(www.nlpkak.com)
HoursofOperation:M-F6:30a.m.-7:30p.m. 13
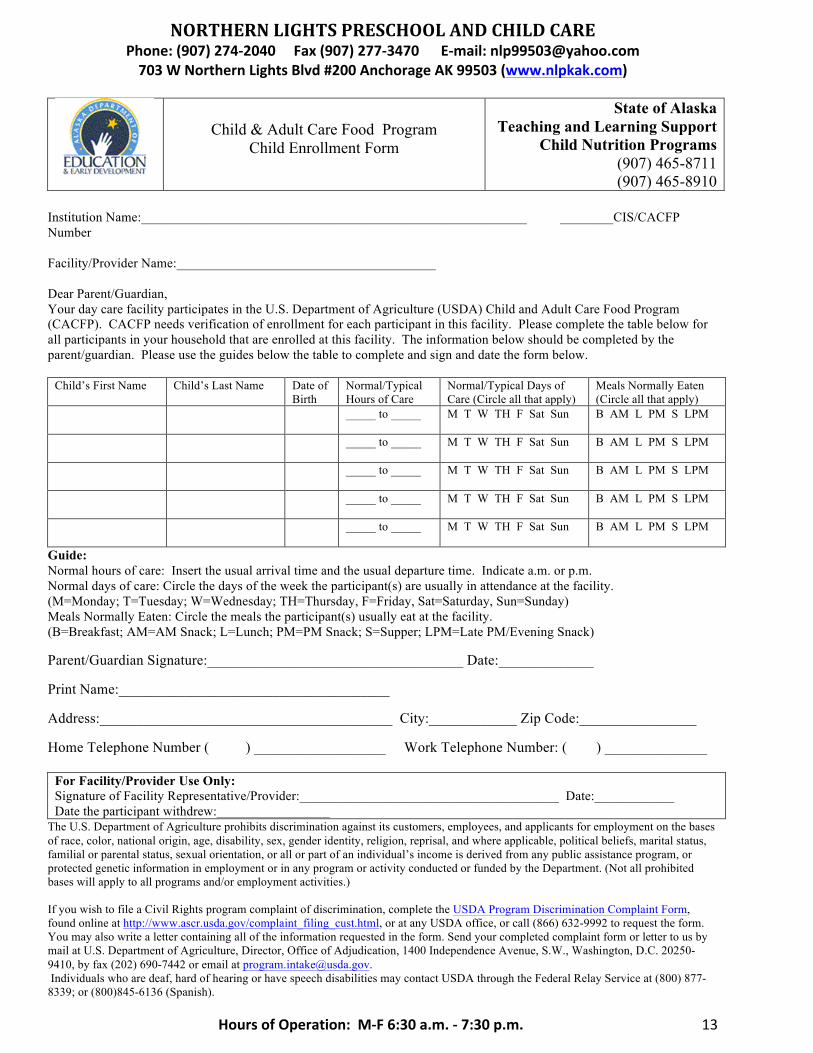
Child & Adult Care Food Program
Child Enrollment Form
State of Alaska Teaching and Learning Support
Child Nutrition Programs (907) 465-8711 (907) 465-8910
Institution Name:__________________________________________________________ ________CIS/CACFP Number Facility/Provider Name:_______________________________________ Dear Parent/Guardian, Your day care facility participates in the U.S. Department of Agriculture (USDA) Child and Adult Care Food Program (CACFP). CACFP needs verification of enrollment for each participant in this facility. Please complete the table below for all participants in your household that are enrolled at this facility. The information below should be completed by the parent/guardian. Please use the guides below the table to complete and sign and date the form below.
Child’s First Name Child’s Last Name Date of Birth
Normal/Typical Hours of Care
Normal/Typical Days of Care (Circle all that apply)
Meals Normally Eaten (Circle all that apply)
_____ to _____ M T W TH F Sat Sun B AM L PM S LPM
_____ to _____ M T W TH F Sat Sun B AM L PM S LPM
_____ to _____ M T W TH F Sat Sun B AM L PM S LPM
_____ to _____ M T W TH F Sat Sun B AM L PM S LPM
_____ to _____ M T W TH F Sat Sun B AM L PM S LPM
Guide: Normal hours of care: Insert the usual arrival time and the usual departure time. Indicate a.m. or p.m. Normal days of care: Circle the days of the week the participant(s) are usually in attendance at the facility. (M=Monday; T=Tuesday; W=Wednesday; TH=Thursday, F=Friday, Sat=Saturday, Sun=Sunday) Meals Normally Eaten: Circle the meals the participant(s) usually eat at the facility. (B=Breakfast; AM=AM Snack; L=Lunch; PM=PM Snack; S=Supper; LPM=Late PM/Evening Snack) Parent/Guardian Signature:___________________________________ Date:_____________ Print Name:_____________________________________ Address:________________________________________ City:____________ Zip Code:________________ Home Telephone Number ( ) __________________ Work Telephone Number: ( ) ______________
For Facility/Provider Use Only: Signature of Facility Representative/Provider:_______________________________________ Date:____________ Date the participant withdrew:_________________
The U.S. Department of Agriculture prohibits discrimination against its customers, employees, and applicants for employment on the bases of race, color, national origin, age, disability, sex, gender identity, religion, reprisal, and where applicable, political beliefs, marital status, familial or parental status, sexual orientation, or all or part of an individual’s income is derived from any public assistance program, or protected genetic information in employment or in any program or activity conducted or funded by the Department. (Not all prohibited bases will apply to all programs and/or employment activities.) If you wish to file a Civil Rights program complaint of discrimination, complete the USDA Program Discrimination Complaint Form, found online at http://www.ascr.usda.gov/complaint_filing_cust.html, or at any USDA office, or call (866) 632-9992 to request the form. You may also write a letter containing all of the information requested in the form. Send your completed complaint form or letter to us by mail at U.S. Department of Agriculture, Director, Office of Adjudication, 1400 Independence Avenue, S.W., Washington, D.C. 20250-9410, by fax (202) 690-7442 or email at [email protected]. Individuals who are deaf, hard of hearing or have speech disabilities may contact USDA through the Federal Relay Service at (800) 877-8339; or (800)845-6136 (Spanish).