Embed Size (px)
Citation preview

FIRM 1 GRANDROUND
ASEPTIC LOOSENING OF
THA
PRESENTER: ONDARI N.J
FACILITATOR: DR. MUSEVE
03-04-2014

Incidence of hip arthritis is 3-5% in >55yrs



A good prosthesis important


Biomechanics
THA components bears atleast 3X body weight
Abductor lever arm ~2.5X body lever arm
Abductor lever arm may be dec by OA or neck shortening
Lever arm ratios can increase to 4:1
Lenghts of lever can be surgically changed to approach 1:1
This theoretically reduces load hip by 30%

Lateral and distal reattachment of osteotomized GT
Medialization of acetabulum

Stress transfer to bone
Bone quality determines most appropriate implant
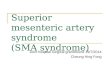
Dorr radiographic classification of proximal femur Type A femurs
Thick cortices Narrow distal canal – ‘champaigne flute’ appearance Found in young pts Permits good fixation
Type B femurs Exhibit bone loss, shape not compromised Implant fixation not a problem
Type C femurs Thin cortex, wide medullary canal – ‘stovepipe’ shape Occurs in older osteoporotic women Less favorable for implant fixation

Dorr classification of morphology of femur

Stress transfer to bone
Stress transfer to bone desirable
Measures to decrease stress shielding Decrease modulus of elasticity of stem
eg titanium alloy Smaller diameter stems Prosthetic collar Stem shape
Tapered geometries better

Complications of THA
Intraoperative Mortality, nerve injuries, vascular injuries
Early postoperative Thromboembolism, hemartoma
formation, infection, dislocation, limb length discrepancy
Late postoperative Heterotopic ossification Loosening
Most serious long term problem

Loosening of THA components
Most serious complication Commonly leads to revision
With Cemented THAs, the acetabulum is the first component to fail from loosening
With cementless hips, the femoral component loosens more often as a result of osteolysis
Can be septic or aseptic

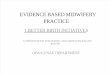
Zones of loosening
Femoral component Seven Gruen zones
Acetabular component Three Delee and Charnley zones

Gruen 7 zones of femur

Delee and Charnley acetabular zones

Cemented Femoral loosening; Radiographic features
Definite loosening Stem failure – fracture/deformation Cement mantle fracture esp zone 4 Radiolucency >1mm Changes in stem position- usually varus
position Pistoning effect
Probable loosening Continous radioluscent line at bone-cement
interface Endosteal cavitation-linear and focal osteolysis
Possible loosening Radioluscent lines at bone-cement interface 50-
100%

Are all radioluscent line due to loosening?
Radioluscent lines btn femoral cortex and cement can be produced by; Cancellous bone not completely removed during sx Normal age related expansion of femoral canal
assoc cortical thinning. Poss et al study;Medullay canal expands at 0.33mm/yrCortical thickness decrease by 0.14mm/yr
NB; these radioluscet lines do not typically have the surrounding sclerotic line noted on loose femoral stems
Medullary canal widening has not been implicated in the process of femoral loosening

Technical problems that contribute to stem loosening
Failure to remove adequate cancellous bone medially
Inadequate quantity of cement Thin column cracks easily Tip of stem should be supported by a plug of cement
Cements laminations Presence of voids in cement
Poor mixing, injecting technique, blood or fragments of bone
Failure to pressurize cement Failure to prevent stem motion while cement is
hardening Failure to position component in neutral or mildly
valgus position

Cementless femoral components

Cemented Acetabular loosening;radiographic features
Bone-cement lucency >2mm and/or progressive
Medial migration and protrusion of cement and cup
Change in inclination of cup >50
Eccentric PE wear of the cup
Fracture of cup and/or cement(rare)


Technical problems during sx leading to cup loosening
Inadequate support of the cup by bone & cement Insufficient bone stock Acetabullum not reamed deeply enough
Failure to remove all cartilage, loose bone fragments, fibous tissue and blood
Failure to make sufficient no of holes in acetabulum to secure good cement-bone bon
Failure to pressurize cement
Failure to distribute cement around entire outer surface of cup
Mvt of cup or cement mantle while cement is hardening
Malpositioning of cup – neck of femoral component impinges on margin of socket

Pathophysiology
Generation of particulate debris Wear corrosion
Mechanisms of wear Adhesion, abrasion, microfatigue and
3rd body wear Wear debris sources
PE, cement, metal particles PE bearing surfaces are the major
factor responsible for periprosthetic osteolysis

Pathophysiology cont.
Particle size important 0.5 – 10microm – pagocytosed <0.5microm – too small to activate a response
>10microm – stimulate a giant cell response
Irregularly shaped particles more active than spherical poarticles

Modes of wear
Is the mechanical condition under which prosthesis was working when wear occurred
Four modes Mode 1
Motion btn two bearing surfaces as intended by designer
Mode 2 10 bearing surface rubbing against 20 surface
Mode 3 Two 10 surfaces with interposed third-body particles
Mode 4 Two non-primary surfaces rubbing together


OSTEOLYSIS
Is the final pathway related to host cellular response to debris of all types
Mechanism Generation of wear particles Access of these particles to periprosthetic bone Cellular response to particulate debris
Debris dispensed through joint fluid by pressure gradient
Pattern of lysis depends on implant design

Osteolysis; cellular response MQs predominant cells
Surface interaction btn MQs and wear debris incite inflammatory response whether or not phagocytosis occurs
Multiple cytokines/chemokines produced
Osteoclasts activated, osteoblasts inhibited
Net result – bone resorption

osteoclast osteoblast interaction
cytokines/ chemokines
MACROPHAGESDEBRIS
phagocytosis
inhibit

Diagnosis History
Pain on wt bearing –groin, buttock or thigh Typically ‘start-up’ pain Pain relieved by rest, aggravated by hip
rotation Physical exam
Antalgic gait Limb length discrepancy
Investigations Laboratory
R/O infection Imaging
Progressive radiolucency Migration of implant

Treatment
Asymptomatic patient Radiographic loosening often appears be4 symptoms
More frequent follow-up Revision surgery if bone destruction is progressive
Symptomatic patient Revision surgery

Indications for surgery
Symptomatic patient
Loose implants
Large lytic lesions
Progressive osteolysis even if no symptoms

Revision Total Hip Arthroplasty cementless components are generally
preferred in revision settings. The bone sclerotic and does not provide
optimal conditions for cement interdigitation
only the loose components need to be revised
If implant remains stable despite osteolysis, bone grafting of the defects with retention of the implant is recommended