Embed Size (px)
Citation preview

Findings of Extrathyroid LesionsEncountered With Thyroid Sonography
Jin Young Kwak, MD, Eun-Kyung Kim, MD, Sun Young Park, MD, Min Jung Kim, MD, Won-Jin Moon, MD, Seon Hyeong Choi, MD, Eun Ju Son, MD, Ki Keun Oh, MD, Ki Whang Kim, MD, Woo-Ick Yang, MD,Ju Yeon Pyo, MD
Objective. The purpose of this presentation is to illustrate the normal sonographic anatomy of theanterior neck region and the sonographic findings of various kinds of extrathyroid lesions. Methods.Cases of extrathyroid lesions were collected and reviewed retrospectively from our archives. All of thesonographic examinations were performed with high-frequency (5- to 15-MHz) linear array transducers.Results. The normal sonographic anatomy of the anterior neck region and various pathologic condi-tions of patients with extrathyroid lesions are discussed. Conclusions. Sonography is a useful imagingmethod for evaluating anterior neck anatomy and various pathologic conditions in patients withextrathyroid lesions. Key words: neck anatomy; sonography; thyroid glands.
Received July 9, 2007, from the Department ofDiagnostic Radiology (J.Y.K., E.-K.K., M.J.K., S.H.C.,E.J.S., K.K.O., K.W.K.), Research Institute ofRadiological Science (J.Y.K., E.-K.K., M.J.K., S.H.C.,E.J.S., K.K.O., K.W.K.), and Department ofPathology (W.-I.Y., J.Y.P.), Yonsei University Collegeof Medicine, Seoul, Korea; Gachon University GilMedical Center, Incheon, Korea (S.Y.P.); andKonkuk University, Seoul, Korea (W.-J.M.). Revisionrequested July 26, 2007. Revised manuscriptaccepted for publication September 6, 2007.
Address correspondence to Eun-Kyung Kim,MD, Department of Diagnostic Radiology, YonseiUniversity College of Medicine, 250 Seongsanno,134 Sinchon-dong, Seodaemun-gu, Seoul 120-752,Korea.
E-mail: [email protected]
AbbreviationsCT, computed tomography; H&E, hematoxylin-eosin;MRI, magnetic resonance imaging
ith the increased use of state-of-the-artsonography, many anterior neck lesions,including thyroid lesions, are being found.Sonography of the neck is extremely sensi-
tive in detecting thyroid and parathyroid lesions, cervi-cal lymph nodes, and other neck lesions,1 althoughsome parathyroid lesions with an ectopic location can bemissed by sonography. The high sensitivity of sonogra-phy is due to the superficial locations of most structureswithin the anterior neck and superior sonographic imag-ing provided by small parts transducers with frequenciesof 7.5 to 15 MHz.
This presentation discusses and illustrates manyextrathyroid lesions mimicking thyroidal lesions. Thesecase examples provide a framework for sharing interpre-tative pearls and pitfalls with practicing radiologists.Careful sonographic examination, along with knowledgeof the anatomy of the cervical region, is very helpful in thediagnosis and differentiation of extrathyroid lesions.
© 2007 by the American Institute of Ultrasound in Medicine • J Ultrasound Med 2007; 26:1747–1759 • 0278-4297/07/$3.50
W
Image Presentation

Materials and Methods
The teaching files of our institution weresearched. We retrospectively reviewed medi-cal records and their associated sonographicfeatures. All sonographic examinations wereperformed with a 7- to 15-MHz linear arraytransducer (HDI 5000; Philips Medical Systems,Bothell, WA), an 8- to 15-MHz linear array trans-ducer (Acuson Sequoia; Siemens MedicalSolutions USA, Inc, Mountain View, CA), or a 5- to 12-MHz linear array transducer (iU22;Philips Medical Systems). With the use of theHDI 5000 and iU22 machines, compound imag-ing was performed in all cases.
Sonographic Findings
Normal Anatomy The anterior neck consists of a central visceralspace and surrounding vascular, nervous, andmuscular structures (Figure 1). The centralvisceral space includes the thyroid gland,parathyroid glands, cervical trachea or esoph-agus, recurrent laryngeal nerve, and paratra-cheal, prelaryngeal, and pretracheal lymph nodegroups.1 Various diseases originating from organsin the visceral space can make differentiation ofthyroid lesions difficult.
Parathyroid DiseasesThe location of the parathyroid glands is variable.Humans usually have 4 parathyroid glands. Thesuperior parathyroid glands are located at theposterior portion of thyroid gland at the level ofupper or mid pole of the thyroid gland.1,2 Thelocation of inferior parathyroid glands is more
variable. However, they are usually seen at theinferoposterior portion of the thyroid gland.1,2
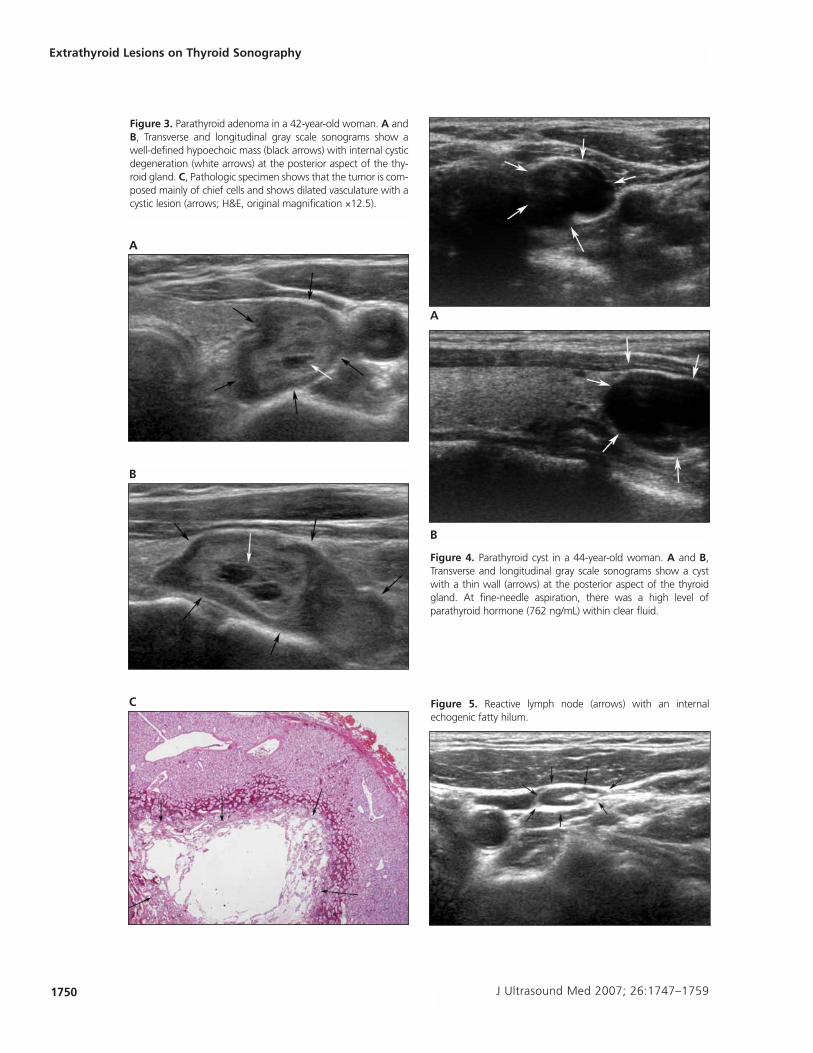
Normal parathyroid glands are not typicallyseen with sonography. However, pathologicparathyroid glands can be seen with sonography.Typically, parathyroid adenoma appears as a well-circumscribed round or oval hypoechoic nodule(Figure 2).2 Parathyroid adenoma is the most com-mon cause of primary hyperparathyroidism.Reeder et al3 reported the characteristic imagingfeatures and a systemic scanning approach forlocalization of parathyroid adenomas in patientswith primary hyperparathyroidism. They suggest-ed that several color Doppler features, includingperipheral and polar vascularity, an enlargingfeeding artery, and vascular asymmetry fromlocalized hyperemia, could be useful for identi-fying parathyroid adenoma.3 However, severalstructures such as lymph nodes, multinodulargoiters, and other tumors found within the vis-ceral space may mimic parathyroid adenoma.Infrequently, parathyroid adenoma may havecystic degeneration (Figure 3) and contain calci-fications.2 Parathyroid cysts are uncommon butwhen present are most commonly located belowthe inferior thyroid border. On sonography, aparathyroid cyst usually appears as a simple cystwith a prominent and thin wall (Figure 4). Withfine-needle aspiration, there is a high level ofparathyroid hormone within clear fluid.
Central Lymph NodesLymphatic tissue is abundant in the neck. Withinthe visceral space, many level VI lymph nodesexist. Most reactive lymph nodes can be easilydifferentiated from other masses because of aninternal hyperechoic fatty hilum on sonography(Figure 5). However, pathologic central lymphnodes can be difficult to differentiate from othermasses such as parathyroid lesions. Various dis-eases such as metastasis, lymphoma, and otherbenign conditions can manifest as pathologiclymph nodes at the central area. Metastaticlymph nodes (Figure 6) from papillary thyroidcarcinoma can show cystic changes, hyperechoicpunctuations, and loss of the hilum.4 Reeder etal3 suggested that color Doppler imaging couldbe useful for distinguishing between parathyroidadenoma and pathologic lymph nodes becausethe polar vascularity seen with parathyroid ade-
1748 J Ultrasound Med 2007; 26:1747–1759
Extrathyroid Lesions on Thyroid Sonography
Figure 1. Normal anatomy of the anterior neck on a transverse scan.

noma differed from the typical central hilar flowpattern seen with lymph nodes.
Hypopharyngeal or Esophageal LesionsA pharyngoesophageal diverticulum is usuallyfound incidentally during esophagography.5
A pharyngoesophageal diverticulum occurs atsites of anatomic weakness in the hypopharynxor in the cervical esophagus near the cricopha-ryngeus muscle.6 With the increased use of high-frequency sonography in evaluation of the neck,a pharyngoesophageal diverticulum can be ini-tially detected on neck sonography. Because apharyngoesophageal diverticulum contains air,this lesion can be misdiagnosed as a thyroidnodule with calcifications. However, trapped air
within a pharyngoesophageal diverticulum canproduce echogenic foci with a comet or rever-beration artifact, which can help in differentiat-ing a pharyngoesophageal diverticulum from athyroid nodule with calcifciations.7 A fewreports have described several sonographic fea-tures for differentiating thyroid nodules frompharyngoesophageal diverticula.7,8 These fea-
J Ultrasound Med 2007; 26:1747–1759 1749
Kwak et al
Figure 2. Parathyroid adenoma in a 63-year-old woman. A andB, Transverse and longitudinal gray scale sonograms show a well-defined hypoechoic mass (arrows) at the posterior aspect of theright thyroid gland. C, Technetium Tc 99m methoxy isobutylisonitrile scan shows delayed wash-out (arrow) of the parathyroidadenoma. D, Pathologic specimen shows that the tumor is roundto oval with a thin capsule (arrows). It shows a trabecular growthpattern of a mixture of chief cells and oncocytic cells (hema-toxylin-eosin [H&E], original magnification ×12.5).
C
D
A
B
1750 J Ultrasound Med 2007; 26:1747–1759
Extrathyroid Lesions on Thyroid Sonography
C Figure 5. Reactive lymph node (arrows) with an internalechogenic fatty hilum.
B
B
A
A
Figure 3. Parathyroid adenoma in a 42-year-old woman. A andB, Transverse and longitudinal gray scale sonograms show awell-defined hypoechoic mass (black arrows) with internal cysticdegeneration (white arrows) at the posterior aspect of the thy-roid gland. C, Pathologic specimen shows that the tumor is com-posed mainly of chief cells and shows dilated vasculature with acystic lesion (arrows; H&E, original magnification ×12.5).
Figure 4. Parathyroid cyst in a 44-year-old woman. A and B,Transverse and longitudinal gray scale sonograms show a cystwith a thin wall (arrows) at the posterior aspect of the thyroidgland. At fine-needle aspiration, there was a high level ofparathyroid hormone (762 ng/mL) within clear fluid.

tures are as follows: first, there are changes in theshape and shadowing of the internal echoes thatare associated with content changes in the diver-ticulum during swallowing; second, there is a
connection to the esophagus (Figure 7); and last,there is a peripheral echogenic line or a boundaryhypoechoic zone that is suggestive of the stratalstructure of the digestive tract (Figure 7).5,7–11
J Ultrasound Med 2007; 26:1747–1759 1751
Kwak et al
C
B
A
Figure 6. Metastatic lymph node from papillary thyroid carcino-ma in a 48-year-old man. A and B, Transverse and longitudinalgray scale sonograms show an oval mass with internal microcal-cifications (black arrows) and cystic changes (white arrows) at theinferior aspect of the right thyroid gland. C, Pathologic specimenshows that the normal structure of the lymph node is distortedby tumor cells. Psammoma bodies are noted (arrows; H&E, orig-inal magnification ×40).
C
B
A
Figure 7. Pharyngoesophageal diverticulum in a 72-year-oldman. A, Transverse gray scale sonogram shows a hypoechoicmass with internal echogenic spots (arrows) at the posterioraspect of the thyroid gland. B, Longitudinal gray scale sonogramshows a hypoechoic mass with a peripheral hypoechoicboundary and a connection to the esophageal wall (arrows). C, Esophagography confirms a Zenker diverticulum projecting tothe left of the esophagus (arrow).

Esophageal carcinoma constitutes only about1% of all cancers and 7% of cancers in the gas-trointestinal tract.12 For detection of esophagealmalignancy, including early esophageal cancer,double-contrast esophagography has been wide-ly accepted as the best diagnostic technique.Sonographic examination of the hypopharyn-geal and cervical esophagus can be difficult.Therefore, sonograms are not routinely used toevaluate hypopharyngeal or esophageal cancer.Anatomically, the hypopharynx and esophagusare located near the posterior portion of the thy-roid gland. Therefore, a mass originating fromthe hypopharynx and esophagus can be misin-terpreted as a thyroid mass (Figure 8). Whenevaluating the neck node status for staging ofhypopharyngeal or esophageal malignancywithout the patient’s history, the possibility ofmisdiagnosing the malignancy as thyroid inorigin exists.
Tracheal LesionsThe extrathoracic trachea is encased anterolater-ally by the thyroid gland. Therefore, trachealmasses can be found on sonographic evaluationsof the neck. The most common tracheal tumor inadults is squamous cell carcinoma, followed byadenoid cystic carcinoma.13 Squamous cell carci-noma is seen as focal or circumferential irregularthickening of the tracheal wall with luminal nar-rowing. In contrast to this, adenoid cystic carci-noma is a low-grade malignancy that tends toinsidiously invade into the submucosal plane ofthe trachea. Adenoid cystic carcinoma is seen aseither a broad-based or pedunculated polypoidlesion. It may show smooth or nodular thicken-ing of the tracheal wall (Figure 9) with associatedluminal narrowing.
Paratracheal air cysts are rare lesions, which arehistologically lined by ciliated columnar epitheliaand communicate with the trachea.14–17 Most ofthem are located at the right posterolateralaspect of the trachea and are easily found bycomputed tomography (CT).14,15 When sonogra-phy of the neck is performed, a paratracheal aircyst can be misdiagnosed as a parathyroid orthyroid mass.18 The reported sonographic featureof a paratracheal air cyst is a masslike lesion con-taining hyperechoic foci at the right inferoposte-rior aspect of the thyroid gland and to the right of
the trachea (Figure 10).18 Internal hyperechoicfoci within a paratracheal air cyst on sonographywere due to air, which was proved by a phantommodel by Kim et al.18 Unlike pharyngoesophagealdiverticula, there are no chronologic changesduring swallowing.
Mediastinal Lesions Many kinds of masses can arise in the prevascu-lar space of the anterior mediastinum. Theseinclude thymic masses, germ cell tumors, lym-phoma, thyroid masses, parathyroid masses, andother growths. Occasionally, a mediastinal masscan initially present as a cervical mass.19–21
A mass originating from the superior medi-astinum may extend superiorly into the thyroidspace (Figures 11 and 12), just as a thyroid masssuch as a goiter may extend inferiorly throughthe thoracic inlet into the superior mediastinum.On sonography, differentiation of these twolesions can be difficult, therefore needing addi-tional imaging studies such as CT or magneticresonance imaging (MRI). Among various medi-astinal masses, teratoma can be easily diagnosedon CT or MRI when the mass has a fat compo-nent.22 Therefore, the possibility of a mediastinalmass should be considered when the inferiormargin of a cervical mass cannot be evaluated byreal-time sonography.
Other Extrathyroid Lesions Originating FromSurrounding StructuresSoft tissue fibromatosis can be divided intosuperficial and deep lesions. Desmoid tumors(deep fibromatosis) arise from musculoaponeu-rotic structures of the limb, neck, trunk, abdomi-nal wall, and mesentery.23 Desmoid tumorsinvade contiguous tissues and are most commonbetween 25 and 35 years but can occur at anyage.23 The lesion is typically firm or hard and usu-ally painless. Most neck desmoids are found inthe upper neck (Figure 13). The tumor may bedifficult to manage because of involvement ofthe great vessels, trachea, and brachial plexus.Surgery is the treatment of choice.
Peripheral nerve sheath tumors in the neck arerelatively rare. The most common types areschwannoma and neurofibroma, which can beseen as a hypoechoic mass with distal acousticenhancement on sonography (Figure 14).24
1752 J Ultrasound Med 2007; 26:1747–1759
Extrathyroid Lesions on Thyroid Sonography

J Ultrasound Med 2007; 26:1747–1759 1753
Kwak et al
E
B
C
Figure 8. Hypopharyngeal squamous cell carcinoma in a 69-year-old man. A, Transverse gray scale sonogram shows a relativelywell-defined hypoechoic mass (arrows) at the upper pole of thethyroid gland. B, Fat suppressed T2-weighted MRI shows a poor-ly defined hyperintense mass (arrows) at the upper pole of theright thyroid gland. C, Fat suppressed T2-weighted MRI shows apoorly defined hyperintense mass (arrows) at the right hypophar-ynx involving the right pyriform sinus. D, Gross specimen at theposterior aspect shows a lobulating mass (black arrows) arisingfrom the right pyriform sinus (blue arrows indicate thyroid carti-lage; and green arrows, false vocal fold). E, Pathologic specimenshows that the squamous cancer cells have invaded the cartilage(arrows; H&E, original magnification ×40).
A
D
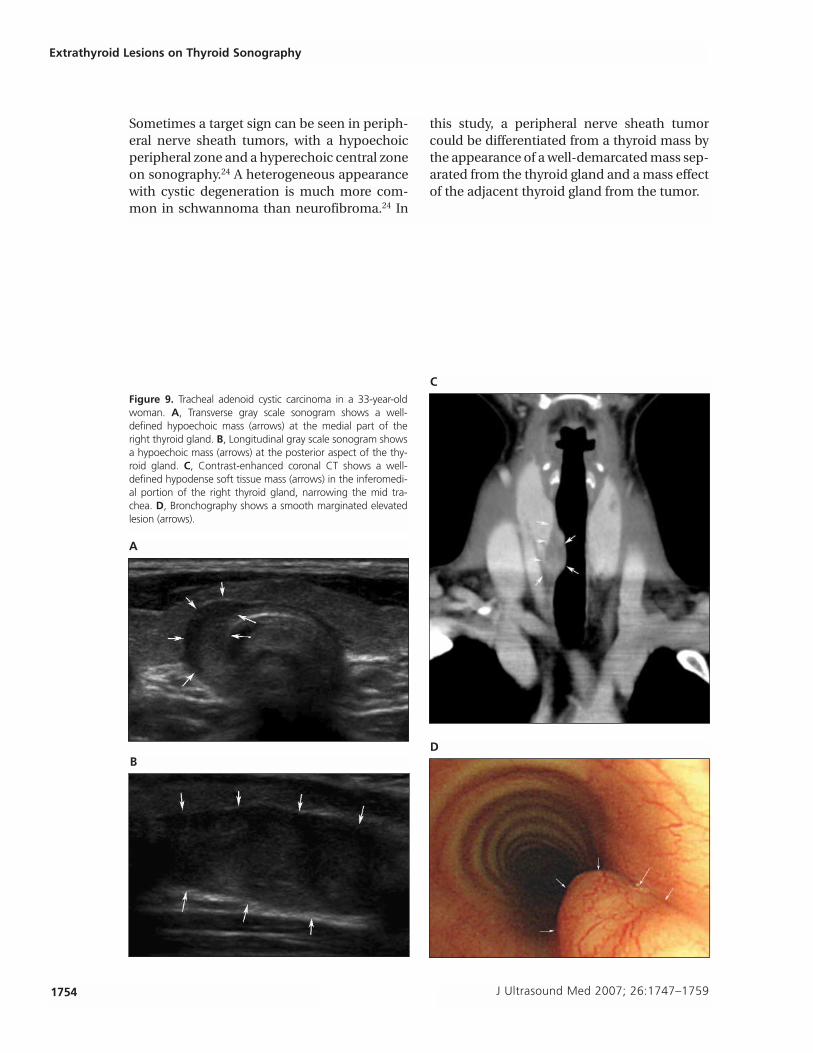
Sometimes a target sign can be seen in periph-eral nerve sheath tumors, with a hypoechoicperipheral zone and a hyperechoic central zoneon sonography.24 A heterogeneous appearancewith cystic degeneration is much more com-mon in schwannoma than neurofibroma.24 In
this study, a peripheral nerve sheath tumorcould be differentiated from a thyroid mass bythe appearance of a well-demarcated mass sep-arated from the thyroid gland and a mass effectof the adjacent thyroid gland from the tumor.
1754 J Ultrasound Med 2007; 26:1747–1759
Extrathyroid Lesions on Thyroid Sonography
Figure 9. Tracheal adenoid cystic carcinoma in a 33-year-oldwoman. A, Transverse gray scale sonogram shows a well-defined hypoechoic mass (arrows) at the medial part of theright thyroid gland. B, Longitudinal gray scale sonogram showsa hypoechoic mass (arrows) at the posterior aspect of the thy-roid gland. C, Contrast-enhanced coronal CT shows a well-defined hypodense soft tissue mass (arrows) in the inferomedi-al portion of the right thyroid gland, narrowing the mid tra-chea. D, Bronchography shows a smooth marginated elevatedlesion (arrows).
C
D
A
B

J Ultrasound Med 2007; 26:1747–1759 1755
Kwak et al
Figure 11. Mediastinal teratoma in a 23-year-old woman. A, Transverse gray scale sonogram shows a huge nearly cystic mass(arrows) at the left thyroid gland. B, Contrast-enhanced axial CT shows a well-defined hypodense mass (arrows) at the left thyroidgland (continued).
A
Figure 10. Paratracheal air cyst in a 40-year-old woman. A, Transverse gray scale sonogram shows a well-defined hypoechoic masswith multiple hyperechoic dots (arrows) at the inferoposterior aspect of the right thyroid gland. B, Axial CT shows communication(arrow) between the trachea and the air cyst.
A B
B
Conclusions
Radiologists should be aware of the various con-ditions that can affect the anterior neck sur-rounding the thyroid glands. To diagnose anteriorneck lesions, sonography is the cornerstone forlocalizing, differentiating, and guiding biopsy.Although some of these disease processes maypresent as extrathyroid lesions on sonography,
knowledge of the sonographic features ofextrathyroidal lesions, a clinical history includinglaboratory findings, and aspiration or biopsy maybe helpful in evaluation of some extrathyroid diseases by allowing for differentiation betweenthyroid and extrathyroid lesions. Therefore, anawareness of a wide range of extrathyroid lesionsis important to avoid misdiagnosis and to helpwith further diagnostic evaluations.

1756 J Ultrasound Med 2007; 26:1747–1759
Extrathyroid Lesions on Thyroid Sonography
D
E
C
Figure 11. (continued) C, Contrast-enhanced axial CT shows awell-defined hypodense mass (white arrows) with an internal fatcomponent (black arrow), suggesting teratoma in the anteriormediastinum. D, T1-weighted MRI shows a mediastinal mass(arrows) extending into the left neck. E, Pathologic specimenshows that the tumor is composed of mature cutaneous adnexa,cartilage (left, arrows; H&E, original magnification ×40), andpancreatic tissue (right; H&E, original magnification ×100).
Figure 12. Mediastinal lymphoma in a 23-year-old woman. A and B, Transverse gray scale sonograms show multiple conglomerat-ed hypoechoic masses (arrows) at the inferoposterior aspect of the thyroid gland (continued).
A B

J Ultrasound Med 2007; 26:1747–1759 1757
Kwak et al
DC
Figure 12. (continued). C–E, Contrast-enhanced axial CT shows multiple conglomerated hypodense masses (arrows) in the supero-posterior mediastinum, extending to the posterior aspect of the thyroid gland. F, Pathologic specimen shows that the lymph nodearchitecture is effaced by various numbers of mononuclear Hodgkin cells and multinucleated Reed-Sternberg cells (arrows; H&E, orig-inal magnification ×400).
Figure 13. Desmoid tumor in a 36-year-old woman. A, Transverse gray scale sonogram shows a well-defined hypoechoic mass(arrows) at the posterior aspect of the left thyroid gland. B, Longitudinal gray scale sonogram shows a well-defined hypoechoic mass(arrows) at the inferior aspect of the right thyroid gland (continued).
A B
E F

1758 J Ultrasound Med 2007; 26:1747–1759
Extrathyroid Lesions on Thyroid Sonography
Figure 13. (continued). C, Fat-suppressed T2-weighted MRI shows a well-defined hyperintense mass with an internal hypodense areaat the posterior aspect of the left thyroid gland (arrows). D, Pathologic specimen shows that the tumor is composed of palelyeosinophlic fibroblasts and myofibroblasts with variably tapering or plump vesicular nuclei (left; H&E, original magnification ×200).The cellularity is variable within tumor (right, white arrows) and shows focal hyalinization (right, black arrows; H&E, original magnifi-cation ×200). At the advancing edge of the tumor, degenerated skeletal muscle cells are present.
C D
Figure 14. Schwannoma in a 65-year-old woman. A and B, Transverse and longitudinal gray scale sonograms show a well-definedheterogeneous hypoechoic mass (arrows), compared with the adjacent thyroid tissue, between the left thyroid gland and the com-mon carotid artery. C, Contrast-enhanced axial CT shows a well-defined hypodense mass (arrows) at the posterior aspect of the leftthyroid gland. D, Pathologic specimen shows that the smear has several clusters of spindly cells (arrows) with variable cellularity andelongated wavy nuclei with a pale and fibrillar cytoplasm (H&E, original magnification ×400).
C D
A B
References
1. Akerström G, Malmaeus J, Bergström R. Surgical anatomyof human parathyroid glands. Surgery 1984; 95:14–21.
2. Kamaya A, Quon A, Jeffrey RB. Sonography of the abnor-mal parathyroid gland. Ultrasound Q 2006; 22:253–262.
3. Reeder SB, Desser TS, Weigel RJ, Jeffrey RB. Sonography inprimary hyperparathyroidism: review with emphasis onscanning technique. J Ultrasound Med 2002; 21:539–552.
4. Rosario PW, de Faria S, Bicalho L, et al. Ultrasonographicdifferentiation between metastatic and benign lymphnodes in patients with papillary thyroid carcinoma. J Ultrasound Med 2005; 24:1385–1389.
5. Kumar A, Aggarwal S, Pham DH. Pharyngoesophageal(Zenker’s) diverticulum mimicking thyroid nodule on ultra-sonography: report of two cases. J Ultrasound Med 1994;13:319–322.
6. Ekberg O, Nylander G. Lateral diverticula from the pharyn-go-esophageal junction area. Radiology 1983; 146:117–122.
7. Kim J, Kim YJ, Kim EK, Park CS. Incidentally found pharyn-goesophageal diverticulum on ultrasonography. YonseiMed J 2002; 43:271–273.
8. Kwak JY, Kim EK. Sonographic findings of Zenker divertic-ula. J Ultrasound Med 2006; 25:639–642.
9. Biggi E, Derchi LE, Cicio GR, Neumaier CE. Sonographicfindings of Zenker’s diverticulum. J Clin Ultrasound 1982;10:395–396.
10. Komatsu M, Komatsu T, Inove K. Ultrasonography ofZenker’s diverticulum: special reference to differential diag-nosis from thyroid nodules. Eur J Ultrasound 2000; 11:123–125.
11. DeFriend DE, Dubbins PA. Sonographic demonstration of apharyngoesophageal diverticulum. J Clin Ultrasound 2000;28:485–487.
12. Livstone EM, Skinner DB. Tumors of the esophagus. In:Berk JE (ed). Gastroenterology. Philadelphia, PA: WBSaunders Co; 1985:818–850.
13. Som PM, Curtin HD. Trachea: anatomy and pathology. In:Sasson JP, Abdelrahman NG, Aquino S, Lev MH (eds). Headand Neck Imaging. 4th ed. St Louis, MO: CV Mosby Co;2003:1700–1726.
14. Tanaka H, Mori Y, Kurokawa K, Abe S. Paratracheal aircysts communicating with the trachea: CT findings. J Thorac Imaging 1997; 12:38–40.
15. Goo JM, Im JG, Ahn JM, et al. Right paratracheal air cystsin the thoracic inlet: clinical and radiologic significance. AJRAm J Roentgenol 1999; 173:65–70.
16. Infante M, Mattavelli F, Valente M, Alloisio M, Preda F,Ravasi G. Tracheal diverticulum: a rare cause and conse-quence of chronic cough. Eur J Surg 1994; 160:315–316.
17. Tanaka H, Igarashi T, Teramoto S, Yoshida U, Abe S.Lymphoepithelial cysts in the mediastinum with an open-ing to the trachea. Respiration 1995; 62:110–113.
18. Kim YJ, Kim EK, Kim J, Park CS. Paratracheal air cysts:sonographic findings in two cases. Korean J Radiol 2003;4:136–139.
19. Mountzios G, Pavlakis G, Terpos E, et al. Concurrent devel-opment of testicular seminoma and choriocarcinoma ofthe superior mediastinum, presented as cervical mass: acase report and implications about pathogenesis of germ-cell tumours. BMC Clin Pathol 2006; 6:8–14.
20. Alvarez ZC, Riveros SP, Miranda TR, Yarur VO. Mediastinalhydatid cyst: case report and review. Rev Chilena Infectol2007; 24:149–152.
21. Tomà PL, Rossi UG. Paediatric ultrasound, II: other applica-tions. Eur Radiol 2001; 11:2369–2398.
22. Gaerte SC, Meyer CA, Winer-Muram HT, Tarver RD,Conces DJ. Fat-containing lesions of the chest.Radiographics 2002; 22(special issue):S61–S78.
23. Dinauer PA, Brixey CJ, Moncur JT, Fanburg-Smith JC,Murphey MD. Pathologic and MR imaging features ofbenign fibrous soft-tissue tumors in adults. Radiographics2007; 27:173–187.
24. Lin J, Martel W. Cross-sectional imaging of peripheralnerve sheath tumors: characteristic signs on CT, MR imag-ing, and sonography. AJR Am J Roentgenol 2001; 176:75–82.
J Ultrasound Med 2007; 26:1747–1759 1759
Kwak et al





























