-
8/4/2019 Finalizing HCV
1/15
P a g e | 2
Muhammad Ali Minhas HCV
Hepatitis C Virus
(HCV)
Introduction:Hepatitis is a disease characterized by
inflammation of the liver, usually producing
swelling and, in many cases, permanent damage to liver tissues.
A number of different agentscan cause hepatitis, including
infectious diseases, chemical poisons, drugs and alcohol.
Viralhepatitis refers to a set of at least six viruses that are
known to cause hepatitis: hepatitis A(HAV), hepatitis B (HBV),
hepatitis C (HCV), hepatitis D (HDV), hepatitis E (HEV),
andhepatitis G (HGV). Recent scientific evidence also suggests the
existence of other, as yetunidentified hepatitis viruses.
The most common types of viral hepatitis are hepatitis A, B, and
hepatitis C. Both hepatitis Band C can lead to serious, permanent
liver damage, and in many cases, death.
There are two primary types of viral hepatitis, food-borne and
blood-borne hepatitis. The former,which is spread through
contaminated food and water, does not cause chronic liver disease.
Bycontrast, blood borne viral hepatitis may lead to long-term,
persistent infections and chronic liverdisease that has lethal
consequences many years after infection.
The Hepatitis C Virus:Hepatitis C is an RNA virus - which means
that it mutates frequently. Once an infection
has begun, hepatitis C creates different genetic variations of
itself within the body of the host.The mutated forms are frequently
different enough from their ancestors that the immune systemcannot
recognize them. Thus, even if the immune system begins to succeed
against one variation,the mutant strains quickly take over and
become new, predominant strains. As a result, thedevelopment of
antibodies against HCV does not produce immunity against the
disease like itdoes with most other viruses. More than 80% of the
individuals infected with HCV will progressto a chronic form of the
disease.
There are six basic genotypes of HCV, with 15 recorded subtypes,
which vary inprevalence in different regions of the world. Each of
these major genotypes can differsignificantly in their biological
effects - in terms of replication, mutation rates, type and
severityof liver damage, and detection and treatment options.
However, these differences are not yetclearly understood.
The 21 current variations in genotype, complicated by the
constant mutation of the viruswithin infected individuals,
represents a major challenge for the development of treatments
and
-
8/4/2019 Finalizing HCV
2/15
P a g e | 3
Muhammad Ali Minhas HCV
vaccinesagainst HCV- and evenfor reliabledetection of
the virus.There is noguaranteethat atreatment,test,
orvaccineagainst onestrain will beeffectiveagainst all of
them.Moreover, individuals cured of one strain will be prone to
reinfection by any of the other strains.
Anatomy of the Hepatitis C Virus:The structure of the hepatitis
C virus is like that of most complex viruses - a core of
genetic material (RNA), surrounded by a protective shell of
protein, and further encased in alipid (fatty) envelope of celluar
material. However, the fact that the genetic information of
thevirus is stored in RNA, not DNA, has important consequences in
the life cycle of the virus, andgives hepatitis C its dangerous
ability to mutate.
All organisms, with the exception of the RNA viruses, store
their permanent informationin DNA, using RNA only as a temporary
messenger for information. DNA is quite a stablemolecule, not
particularly reactive with other molecules, and the processes which
reproduce itmake very few mistakes in the process of copying the
molecule (between one in 1 million and 1in 10 million). Most of
these mistakes are normally corrected even when they do occur.
Thismakes DNA an ideal format for the storage of information, for
mutations (errors) only rarelyoccur, and most are not
significant.
RNA, by contrast, is a quite reactive molecule, capable of
reacting even with itself underthe correct conditions. It also
makes frequent mistakes during copying - averaging one mistakeper
10,000 nucleotides each time it is copied. These properties make
RNA very poorly suited for
the storage of information.
However, these very propeties make RNA ideal for the storage of
viral information. Oncethe immune system has learned to recognize
an infecting virus and create antibodies against it(developed an
immunity), it can quickly destroy it, so the virus can no longer
use that host forreproduction. In order to reinfect a host - it
must first change its nature enough that the immunesystem will no
longer recognize it - in other words, it must mutate.
-
8/4/2019 Finalizing HCV
3/15
P a g e | 4
Muhammad Ali Minhas HCV
Hepatitis C virus. Structure of the viral capsid is clearly
visible
The unstable nature of the RNA molecule provides this mutagenic
factor, allowing theHepatitis C virus to develop new genetic
variations of itself. As discussed earlier, the mutatedforms are
frequently different enough from their ancestors that the immune
system cannotrecognize them, so if the immune system begins to
succeed against one variation, the mutantstrains quickly take over
and become new, predominant strains. Because each surviving
virusreproduces itself thousands of times, mutations in the RNA
sequence occur frequently, allowingit to evolve faster than any
other type of living organism. This evolution is known as
antigenicdrift. Mutations occur randomly across the entire length
of the viral RNA, and so of course mostare not beneficial,
producing viruses which lack a needed protein or are otherwise
disadvantaged.However, because of the enormous number of offspring
produced by each virus, even a high rateof mutation does not
threaten the survival of the virus - and when advantageous
mutations dooccur, they are rapidly selected for and
reproduced.
Hepatitis C, as an RNA virus, has apowerful reproductive
strategy. Because itstores its information in a "sense" strand
ofRNA, the viral RNA itself can be directlyread by the host cell's
ribosomes,functioning like the normal mRNA presentin the cell. The
virus thus needs no specialabilities of its own - it uses the
cell's ownribosomes to produce everything it needsfor its takeover
of the cell's processes andreproduction. This means hepatitis C
requires only a small amount of RNA to encode its core
information, and thus has lots of room
-
8/4/2019 Finalizing HCV
4/15
P a g e | 5
Muhammad Ali Minhas HCV
for genetic variation within the non-essential portions of its
RNA. This also gives it fewercommon characteristics that can be
readily identified by the immune system - or, for that
matter,exploited by scientists working to create a treatment.
Genome of HCV:Hepatitis C virus has a positive sense
single-stranded RNA genome. The genome consists
of a single open reading frame that is 9600 nucleotide bases
long. This single open reading frameis translated to produce a
single protein product, which is then further processed to
producesmaller active proteins.
At the 5' and 3' ends of the RNA are the UTR, which are not
translated into proteins butare important to translation and
replication of the viral RNA. The 5' UTR has a ribosome bindingsite
(IRES - Internal ribosome entry site) that starts the translation
of a very long proteincontaining about 3,000 amino acids. This
large pre-protein is later cut by cellular and viral
proteases into the 10 smaller proteins that allow viral
replication within the host cell, or assembleinto the mature viral
particles.
-
8/4/2019 Finalizing HCV
5/15
P a g e | 6
Muhammad Ali Minhas HCV
Structural proteins made by the hepatitis C virus include Core
protein, E1 and E2; nonstructuralproteins include NS2, NS3, NS4,
NS4A, NS4B, NS5, NS5A, and NS5B.
The Life Cycle of Hepatitis C:1) The hepatitis C virus must
attach to and infect liver cells in order to carry out its life
cycle and reproduce - this is why it is associated with liver
disease. While little isknown about the exact natural processes of
hepatitis C, like other viruses, it mustcomplete eight key steps to
carry out its life cycle:
2) The virus locates and attaches itself to a liver cell.
Hepatitis C uses particular proteinspresent on its protective lipid
coat to attach to a receptor site (a recognizable structureon the
surface of the liver cell).
3) The virus's protein core penetrates the plasma membrane and
enters the cell. Toaccomplish this, hepatitis C utlilizes its
protective lipid (fatty) coat, merging its lipidcoat with the cells
outer membrane (the coat is in fact composed of a fragment
ofanother liver cell's plasma membrane). Once the lipid coat has
successfully fused tothe plasma membrane, the membrane engulfs the
virus - and the viral core is insidethe cell.
4) The protein coat dissolves to release the viral RNA in the
cell. This may beaccomplished during penetration of the cell
membrane (it is broken open when it isreleased into the cytoplasm),
or special enzymes present in liver cells may be used todissolve
the casing.
5) The viral RNA then coopts the cell's ribosomes, and begins
the production ofmaterials necessary for viral reproduction.
Because hepatitis C stores its informationin a "sense" strand of
RNA, the viral RNA itself can be directly read by the host
cell'sribosomes, functioning like the normal mRNA present in the
cell. As it beginsproducing the materials coded in its RNA, the
virus also probably shuts down most of
the normal functions of the cell, conserving its energy for the
production of viralmaterial,
6) although it occasionally appears that hepatitis C will
stimulate the cell to reproduce(presumably to create more cells
that can produce viruses), which is why hepatitis Cis often
associated with liver cancer. The viral RNA first synthesizes the
RNAtranscriptase it will need for reproduction.
7) Once there is adequate RNA transcriptase, the viral RNA
creates an antisense version(the paired opposite) of itself as a
template for the creation of new viral RNA. Theviral RNA is now
copied hundreds or thousands of times, making the genetic
materialfor new viruses. Some of this new RNA will contain
mutations.
8) Viral RNA then directs the production of protein-based
Capsomeres (the buildingblocks for the virus's protective protein
coat). Ribosomes create the proteins andrelease them for use.
9) The completed Capsomeres assemble around the new viral RNA
into new viralparticles. The Capsomeres are designed to attract
each other and fit together in acertain way. When enough Capsomeres
are brought together, they self-assemble toform a spherical shell,
called a capsid that fully encapsulates the virus's RNA.
Thecompleted particle is called a nucleocapsid.
-
8/4/2019 Finalizing HCV
6/15
P a g e | 7
Muhammad Ali Minhas HCV
10)The newly formed viruses travel to the inside portion of the
plasma membrane andattach to it, creating a bud. The plasma
membrane encircles the virus and thenreleases it - providing the
virus with its protective lipid coat, which it will later use
toattach to another liver cell. This process of budding and release
of new viruses
continues for hours at the cell surface until the cell dies from
exhaustion.
Each surviving virus - those which are not destroyed by the
immune system or otherenvironmental factors - can produce hundreds
or thousands of offspring. Over time, this endlesscycle of
reproduction results in significant damage to the liver, as
millions upon millions of cellsare destroyed by viral reproduction
or by the immune system's attacks on infected cells.
-
8/4/2019 Finalizing HCV
7/15
P a g e | 8
Muhammad Ali Minhas HCV
Cellular immune responses against hepatitis C virusHCV, like
other viruses,
induces multiple immuneeffector responses, but this
review focuses primarily on Tlymphocytes. There is goodevidence
that both CD4+ andCD8+ T lymphocytes play amajor role in
determiningoutcome after acute infectionand therefore in the long
term.This comes from the followingobservations.
Clearance of acute infection in both man and in chimpanzee
models is accompanied bystrong CD4+ and CD8+ T cellresponses
against numerous HCVderived antigens. The evidence wasobtained
first for CD4+ T cellresponses and initially some specificepitopes
were highlighted aspotentially protective. Although
these do appear to be targeted, this isnot exclusive and
responses to othergene products are also seen. The
strength of the CD8+
T cell responseagainst one epitope when measuredusing a
tetramer, may be up to 8% ofthe total CD8+ T cells, and can
includeresponses to at least 8 separateepitopes. By ELISpot
analysis, theCD4+ T cell responses appear to be ofa similar
magnitude.
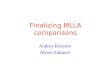
Figure: Interactions of HCV proteins withdifferent effectors of
the immune response.
The effects of HCV proteins on the
different components of the innate and
specific immunity are summarized.
-
8/4/2019 Finalizing HCV
8/15
P a g e | 9
Muhammad Ali Minhas HCV
The timing of these responses appears to correlate with
resolution of viraemia in thosecases where virus is cleared. The
level of activation of HCV-specific T cell responses(assessed
byCD38expression)
correlates withthe degree ofliverinflammationanalysed byblood
ALTlevels.
There is anassociationbetweenpossession of
specific HLAgenes(DRB1*1101and/or DQ1*0301) and spontaneous
clearance of virus. This strongly suggests thatselection of
particular epitopes is associated with better initial control of
viraemia. Thosebearing HLA DQ1*0301 (which is in tight linkage
disequilibrium with DRB1*1101)were found to be more likely to
possess significant HCV-specific CD4+ T cell responses,further
evidence that the responses in these individuals are more
robust.
So much for successful responseswhich are in fact the exception.
The mechanism for viralpersistence, i.e. failure of Tcell responses
in the majorityof patients, is not yet clear.Studies of those who
go on todevelop persistent infectionhave highlighted the weakCD4+ T
cell responses,although it is not clear yetwhether persistence of
viruscauses attenuation of T cellresponses or vice versa.
Re-emergence of CD4+ T cellresponses upon clearance ofvirus with
interferon-alpha/ribavirin therapysuggests the latter ,
i.e.suppression of T cells byvirus may be important.
-
8/4/2019 Finalizing HCV
9/15
P a g e | 10
Muhammad Ali Minhas HCV
The picture with regards to CD8+ T cell responses is even less
clear. CD8+ T cell responseshave been observed in the acute phase
of infection in those who fail to clear virus at levels of 13% of
CD8+ lymphocytes against 12 separate T cell epitopes. Whether these
are the mainepitopes targeted in these individuals and how,
overall, the responses differ in magnitude
between clearers and nonclearers is not known. It appears that
failure to clear virus is not due tofailure to mount any CTL
response whatsoever, although, like CD4+ T cell responses, these
maybe poorly maintained in the face of ongoing viraemia. The
overall quality of the response maydiffer in terms of magnitude or
breadthor, importantly, peptide selection. It is this latter
issuethat forms the focus of this review.Clinical features of
HCV
After inoculation, unlike Hepatitis A and B, the acute illness
caused by HCV is not welldocumented. This is partly because it is
genuinely milder, and possibly it is poorly recognized
byphysicians, and also those in the current western risk groups may
not present to hospital. This isunfortunate, as it now appears that
early intervention is of benefit. When it has been documented,or in
animal models, the following features are apparent:
The peak of viraemia may take several weeks to arise. The liver
inflammation/liverenzyme level in the blood (usually measured as
ALT or AST) does not parallel the viralloadconsistent with the idea
that at this stage much of the liver damage is not causeddirectly
by the virus.
Resolution of the viraemia(accompanied by cellular
immuneresponses) is associated with liverinflammation and in some
but not allcases, clinical jaundice. The level ofALT may be 5002000
IU/l, compared
with HBV where it may be 5 or 10times higher. After this period,
viraemia either
persists or the individual, in about 15%of cases, becomes RNA
negative in theblood. There may be a state ofinstability where
virus may become
undetectable in blood temporarily andthen reappears.
If viraemia is established, the level ofviraemia does not
correlate with progression of disease, unlike HIV. Disease
progression
is measured by the development of liver inflammation, as
assessed by blood ALT andhistological indices of lymphocytic
infiltration and also by creeping fibrosis. The extentof these vary
widely between individuals, and apart from a few factors such as
alcoholand coinfection (for example with HIV), the basis of this
variation is not understood.
-
8/4/2019 Finalizing HCV
10/15
P a g e | 11
Muhammad Ali Minhas HCV
In those where disease has progressed, therapy (in the form of
interferon-alpha andribavirin) may lead to long-term clearance of
virus from blood, with accompanyingimprovement in liver histology.
The effects of the drugs are not entirely understood, andit is
likely that in addition to antiviral activity they influence the
immune response, bothdirectly, and indirectly through lowering
viral load.
Diagnosis and TestingHow and when is HCV diagnosed?
HCV infection is not infrequently diagnosed as a complete
surprise and may causeconsiderable upset for patient and those
around the patient including doctor.
The disease can have a broad spectrum of presentations such
as:
Major symptoms (swelling of legs and abdomen, confusion)and
findings (abnormallaboratory tests (blood) or imagines (Ultrasound,
CT scan).
HCV can be diagnosed in a completely asymptomatic individual
during health or lifeinsurance check
focused test result after someone's history indicated risk
factor's (sometimes decadesago!)
Asymptomatic individual may becomes more symptomatic once
knowing that they carryHCV virus. This may due to prior denial of
symptoms or occur against the background ofincreased anxiety about
the diagnosis.
As part of work-up for a variety of symptoms and findings, often
- but not necessarily -including abnormal liver tests:
oFatigueo Jaundice (relatively rare)
o Fluid retention in abdomen or legso Skin and joint complaintso
Red blood cells in urineo Abnormal looking liver and/or spleen on
ultrasound or CTo Liver tumor on imagingo Mental status changes,
disturbance of sleeping pattern
Testing for HCV1)HCV antibodies:
All HIV-infected patients should be tested for HCV infection
with the HCV antibody test.Patients with risk factors for HCV
infection should be retested at regular intervals. In HIV-Infected
patients, the HCV antibody test result sometimes is falsely
negative; therefore, if HCVinfection is suspected (e.g., because of
a history of high-risk behavior, unexplained elevated
-
8/4/2019 Finalizing HCV
11/15
P a g e | 12
Muhammad Ali Minhas HCV
ALT, or evidence of cirrhosis), the HCV RNA should be tested
even if the HCV antibody testresult is negative. A false-negative
HCV RNA result is very unlikely in chronic infection.
2)HCV RNA:All patients who test positive for HCV antibody should
have HCV RNA testing performed.
As noted above, if patients have negative results on HCV
antibody tests but persistentlyabnormal transaminases or suspected
acute or chronic infection, HCV RNA testing should beperformed.
The definition of chronic HCV infection is the presence of HCV
RNA 6 months after theestimated time of infection. If a patient is
HCV antibody positive but HCV RNA negative, thepatient has cleared
the HCV and does not have chronic HCV infection.
There are quantitative RNA tests and qualitative RNA tests.
Although both types of RNAtests are highly sensitive and specific,
thequalitative tests can detect lower levels ofviremia than the
quantitative tests. Thechoice of RNA test can be important.
The quantitative RNA tests will bereported as a value, with a
measured numberof international units per milliliter
(IU/mL).Quantitative tests are useful for determiningthe prognosis
of HCV treatment and then
monitoring while on HCV treatment.Qualitative RNA tests will be
reported as apresent or absent value, but without anumerical value.
They are useful for serialtesting during suspected acute infection
andfor determining whether spontaneous viralclearance has occurred,
a sustainedvirological response has occurred during
treatment, or a relapse has occurred after treatment.
3)Genotyping:The HCV genotype is the strongest predictor of
response to HCV treatment and also is a
critical determinant of the dosage and duration of treatment.
HCV genotyping should beperformed once for all patients with
detectable HCV RNA; it does not need to be repeated.
-
8/4/2019 Finalizing HCV
12/15
P a g e | 13
Muhammad Ali Minhas HCV
4)Alanine aminotransferase:Monitoring of ALT can be useful to
assess acute infection, chronic liver inflammation, and
response to HCV treatment. However, ALT does not always
correlate with the degree of fibrosisand in addition, ALT can be
persistently normal in 25% of HCV patients, including patients
with
cirrhosis or advanced liver disease. Small fluctuations in ALT
usually are not clinicallysignificant in HCV, though trends can be
significant during or following HCV treatment.
Additional tests:Check complete blood cell count with platelet
count, albumin, total bilirubin, and
prothrombin time.
Test all patients for hepatitis B (HBsAg, anti-HBsAb, and
anti-HBcAb). Patients with anegative HBsAg and negative anti-HBsAb
result should be vaccinated against HBV. Test for
hepatitis A virus (HAV) antibodies (total). All patients with a
negative HAV antibody resultshould be vaccinated against HAV.
5)ImagingUltrasonography can be performed to screen for
cirrhosis or focal hepatic masses. Computed
tomography (CT), magnetic resonance imaging (MRI), and
single-photon emission computedtomography (SPECT) are more
expensive and generally are reserved for further evaluation ofliver
masses detected by ultrasound.
6)Liver biopsyLiver biopsy is used to define the degree of
inflammation (the grade) and degree of fibrosis
(the stage) to determine the need for HCV treatment. Unless
there is clear evidence of cirrhosis,laboratory tests and radiology
studies are unable to quantitate the degree of fibrosis in the
liver.Liver biopsy carries some risk, primarily from bleeding (the
risk of significant bleeding orfatality is approximately 1/10,000).
Patients with severe thrombocytopenia or coagulopathyshould not
undergo liver biopsy. Fibrosis is scored from 0 to 4, with 0
indicating no fibrosis and4 indicating cirrhosis.
Biopsy can be useful in making management decisions for some HCV
patients, for example
when determining whether to treat a patient, particularly those
with genotype 1 virus (see below).If the biopsy reveals only
mild-to-moderate fibrosis, it may be preferable to defer treatment
andmonitor the patient. Conversely, if the biopsy reveals more
advanced fibrosis, treatment shouldbe considered more urgently.
With genotype 2 or 3 patients, some providers consider biopsy tobe
unnecessary because treatment outcomes are sufficiently high that
findings from a biopsywould not necessarily change the management
strategy. For HIV/HCV-coinfected patients, abiopsy may be
particularly useful in determining the stage of disease and in
planning whether orwhen to initiate HCV treatment, as the course of
liver disease may accelerate. Overall, deciding
-
8/4/2019 Finalizing HCV
13/15
P a g e | 14
Muhammad Ali Minhas HCV
whether to conduct a biopsy largely is a matter of individual
choice. It is not a requirement fortreatment of any patient, but
may be useful for helping the provider and patient make a
decisionabout whether or when to undergo treatment.
Test results to detect, diagnose, and monitor HCV include:
Anti-HCV HCV RIBA HCV RNA,Qualitative
HCV Infection
Negative No infection or, rarely,insufficient antibody
Positive Negative No infection; likely a falsepositive
Positive Need to do Negative Likely no infection, pastinfection,
or HCV viral loadlow
Positive Positive Negative Past infection or HCV viral load
lowPositive or Weak orIndeterminate
Not done orPositive
Positive Current infection
Indeterminate orPositive
Indeterminate Negative No infection, past infection, orHCV viral
load low
Basics of diagnostic tests1.HCV ELISA
An enzyme-linked immunosorbent assay (ELISA) was developed by
using a syntheticpolypeptide (SP) whose sequence was derived from
the structural region of hepatitis C virus(HCV). Since the
introduction in1990 of HCV antibody screening ofblood donations,
the incidence of thisinfection in transfusion recipients hasbeen
significantly reduced. The firstgeneration of HCV ELISAs showed
limited sensitivity and specificity andwas produced using
recombinantproteins complementary to the NS4region of the HCV
genome.
Second generation tests, whichincluded recombinant/synthetic
-
8/4/2019 Finalizing HCV
14/15
P a g e | 15
Muhammad Ali Minhas HCV
antigens from the Core and nonstructural regions NS3 and NS4
resulted in a remarkedimprovement in sensitivity and specificity.
Clinical studies show that significant amount of HCVinfected
individuals develop antibodies to NS5 non-structural protein of the
virus. For this, thethird generation tests include antigens from
the NS5 region of the viral genome in addition toNS3, NS4 and the
Core. The third generation tests have improved sensitivity and have
shorten
the antibody detection window period to 70 days.
Principle:This anti-HCV employs solid phase, indirect ELISA
method for detection of antibodies
to HCV in two step incubation procedure. Polystyrene microwell
strips are pre-coated withrecombinant, highly immunoreactive
antigens corresponding to the core and the non-structuralregions of
HCV (third generation HCV ELISA). During the first incubation step,
anti-HCVspecific antibodies, if present, will be bound to the solid
phase pre-coated HCV antigens. Thewells are washed to remove
unbound serum proteins, and rabbit anti-human IgG antibodies
(anti-
IgG) conjugated to the enzyme horseradish peroxidase
(HRP-Conjugate) are added. During thesecond incubation step, these
HRP-conjugated antibodies will be bound to any
antigen-antibody(IgG) complexes previously formed and the unbound
HRP-conjugate is then removed bywashing. Chromogen solutions
containing Tetramethylbenzidine (TMB) and urea peroxide areadded to
the wells and in presence of the antigen-antibody-anti-IgG (HRP)
immunocomplex, thecolorless Chromogens are hydrolyzed by the bound
HRP conjugate to a blue-colored product.The blue color turns yellow
after stopping the reaction with sulfuric acid. The amount of
colorintensity can be measured and it is proportional to the amount
of antibody captured in the wells,and to the amount of antibody in
the sample respectively. Wells containing samples negative
foranti-HCV remain colorless.
Ag(p) + Ab(s) [Ag(p)Ab(s) + ENZ] [Ag(p)Ab(s)ENZ] blue yellow ( +
)
Ag(p)+ [Ag(p) +ENZ] [Ag(p) ] no color ( - )
Incubation1 Incubation 2 Immobilized Complex Coloring
results
30min 30min 15min
Ag(p)pre-coated HCV antigens(core, NS3/4,NS5);
Ab(s)HCV antibodies in sample (IgG);
ENZHRP conjugated rabbit anti-human IgG.
-
8/4/2019 Finalizing HCV
15/15
P a g e | 16
Muhammad Ali Minhas HCV
2.HCV PCRHCV RNA is first separated from the sample. There are
different methods available for doing
so. When viral RNA is separated, its cDNA is formed by a process
called Reverse Transcription(RT) by a reverse transcriptase enzyme.
Then this DNA fragment is amplified by PCR.
The reverse transcription (RT) and polymerase chain reaction
(PCR) amplification stepsare performed sequentially in a single
tube. First, genomic HCV RNA is reverse transcribed
intocomplementary DNA (cDNA) using HCV-specific primers. Next, the
mixture is heated to
activate the DNApolymerase forthe PCRamplification step
and
simultaneouslyinactivate the
reversetranscriptase.
Portions of the 5'UTR and coreregions of theHCV genome are
co-amplifiedfrom the cDNA
using two pairs of biotinylated primers to produce two distinct
biotinylated DNA fragments of
240 and 270 base pairs, representing the 5' UTR and core HCV
regions respectively. Thenucleotide sequence of the primers has
been optimized to yield comparable amplification of sixHCV
genotypes. PCR can be used for qualitative as well as quantitative
study of HCV.
The Future HCV will continue to put a tremendous burden on
future health care expenditures. Many patient have already often
irreversible damage. An enormous number of infected patients, many
of them as yet unidentified and who
contracted blood through blood products or past iv drug abuse
are at risk of developing
cirrhosis with all its complications including hepatocelluar
carcinoma. Once advanced cirrhosis with complications, viral
eradication (still) very difficult, often
impossible or associated with detrimental complications.
Continued contamination / infection through needle transmission
& illicit drug use. A fraction of all patients will be eligible
for liver transplantation: this is beyond the reach
of most worldwide and if available: the organ shortage is
tremendous.
********************