Embed Size (px)
Citation preview

no reprints without permission 1
Treadmill protocols across ages and stages: A fresh look at dosageJulia Looper, PT, PhD
Associate Professor, Physical Therapy
University of Puget Sound, Tacoma, WA
Katrin Mattern‐Baxter, PT, DPT, PCS
Associate Professor, Physical Therapy
California State University, Sacramento
Noelle Moreau, PT, PhD
Associate Professor, Physical Therapy
Louisiana State University Health Sciences Center, New Orleans
Kristie F. Bjornson, PhD, PT, PCS
Associate Professor, Pediatrics
Seattle Children’s Research Institute, WA
Disclosure Information
The speakers have no financial relationships to disclose. The speakers declare no conflict of interest.
Objectives
1. Describe the theoretical and neuroplastic mechanisms behind infant treadmill protocols
2. Describe the available evidence on treadmill training in pre‐ambulatory children with CP and neuromotor impairment
3. Describe muscle performance impairments in children with CP and the implications for treadmill training
4. Describe implementation and outcomes of short‐burst interval treadmill training in ambulatory children with CP

no reprints without permission 2
Objective
1. Describe the theoretical and neuroplasticmechanisms behind infant treadmill protocols
Infant Stepping
• Infants are born with a stepping response
– Legs are alternating
– One leg has knee and hip extension
– Other leg has knee and hip flexion
• Usually “disappears” in the first 2 months of life
Manipulating the Stepping Response
• Thelen showed that the stepping response can be manipulated (1982)– In infants who still exhibit the stepping response, adding weight to their legs will make it disappear
– In infants who no longer exhibit the stepping response, submerging their legs in water will make it reappear
• Zelazo showed that if the stepping response is practiced is does not disappear AND children who practice stepping walk earlier (1972,1983)
no reprints without permission 3
Infant Stepping in Supine?
• Video of 5‐month old baby with typical development
• The stepping movement does not really disappear but takes the form of supine kicking. (Thelen and Fisher, 1982)
– Has less strength demands that upright stepping
• Typically Developing infants are practicing the stepping pattern well before they start to pull to stand
Practice leads to synaptic change
– A synapse changes in strength depending on its past activity
• Increased frequency of firing or strength of activation leads to Long‐Term Potentiation (more likely to fire again)
• Decreased frequency of firing or strength of activation leads to Long‐Term Depression (less likely to fire again)
– Long term potentiation is enhanced in the young brain (Crair and Malenka, 1995)
– Children have more synapses than adults (Huttenlocher& de Court, 1987)
• This provides more neurological options and greater plasticity
Variable Repetition
• Gait is an individual solution to the problem of how to get from point A to point B– So development of the pattern is individualized too
• Variable repetition allows for an adaptive pattern
no reprints without permission 4
How does this relate to the Treadmill?
• Children who are not typically developing do not develop supine kicking in the same way – So, they do not get the same amount of stepping practice
– Children with DS show less antigravity movement (Ulrich and Ulrich, 1995)
– Infants born preterm display decreased dissociation of their lower limbs when kicking (Jeng, Chen, & Yau, 2002)
• One way to help children with DD practice a stepping pattern is the treadmill
How does the treadmill help?
• It provides an environment that helps to facilitate stepping
• It provides the opportunity for multiple repetitions
• It provides the opportunity for variable practice
• It allows for a varied level of trunk control
Down Syndrome:An example of treadmill training in action
• 8 min./day, 5 days/week
• Support infant’s body weight through the trunk
• Allow the infant to actively explore the stepping pattern
• Infants seem to respond to the treadmill when they begin to sit independently
no reprints without permission 5
Down Syndrome:An example of treadmill training in action
• Leads to earlier walking onset (101 days on average) (Ulrich et al, 2001)
• Better gait parameters (Wu et al., 2007)
• Increased intensity led to improved gait parameters and ability to clear an object (Wu et al., 2007)
• Waiting until the children can pull to stand may be too late (Looper & Ulrich, 2010)
Objective
2. Describe the available evidence on treadmill training in pre‐ambulatory children with CP and neuromotor impairment

no reprints without permission 6
Updated Review
• 6 studies included (151 children)
• Accelerated onset of walking in children with Down syndrome
• Early use of orthotics might hinder progress in children with Down syndrome
• Emerging evidence for accelerated walking skills in children with CP
• Benefits on step quality in infants with moderate risk for delay
• Further investigation needed with larger sample size and to determine optimal dosage
Valentin‐Gudiol et al., 2011, 2015 update
Study Design
Pre‐intervention
6‐week post‐intervention
1‐month post‐intervention
4‐month post‐intervention
Control group: no treadmill trainingTreadmill group:treadmill training
5.5 monthsBoth groups receive regularly scheduled PT
no reprints without permission 7
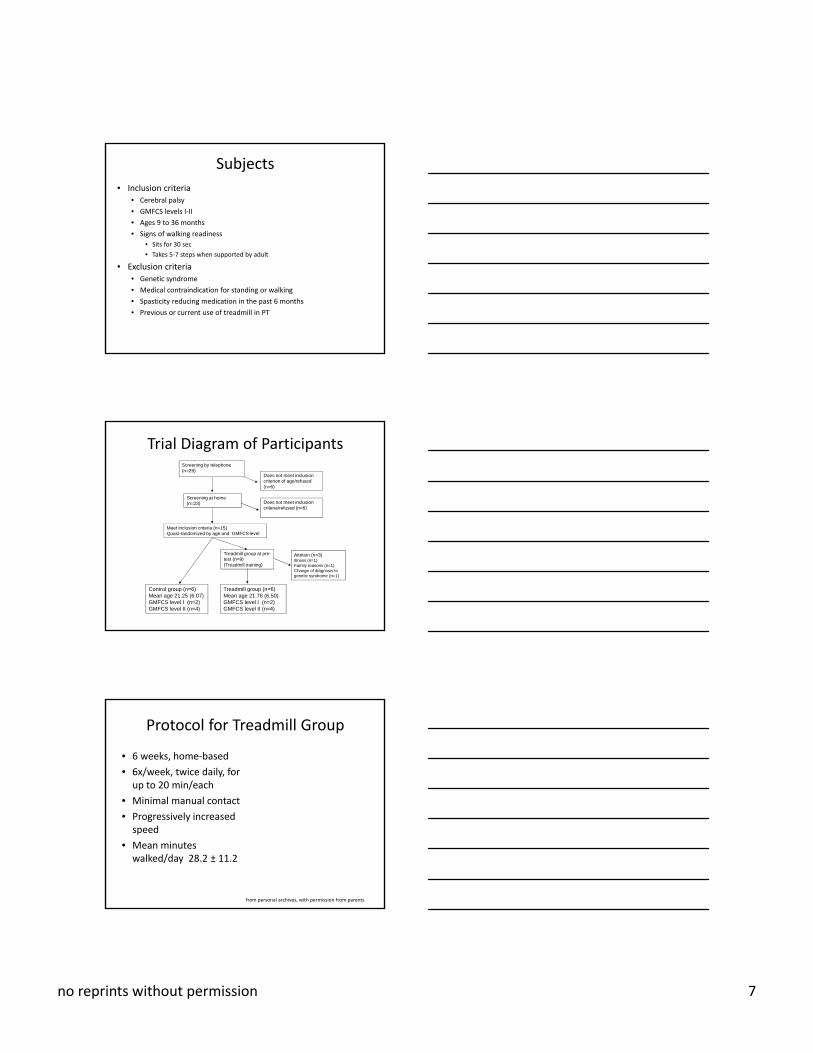
Subjects
• Inclusion criteria• Cerebral palsy
• GMFCS levels I‐II
• Ages 9 to 36 months
• Signs of walking readiness
• Sits for 30 sec
• Takes 5‐7 steps when supported by adult
• Exclusion criteria• Genetic syndrome
• Medical contraindication for standing or walking
• Spasticity reducing medication in the past 6 months
• Previous or current use of treadmill in PT
Screening by telephone (n=29)
Screening at home (n=23)
Control group (n=6)Mean age 21.25 (6.07)GMFCS level I (n=2)GMFCS level II (n=4)
Treadmill group at pre-test (n=9)(Treadmill training)
Meet inclusion criteria (n=15)Quasi-randomized by age and GMFCS level
Does not meet inclusion criteria/refused (n=8)
Does not meet inclusion criterion of age/refused (n=6)
Attrition (n=3)Illness (n=1)Family reasons (n=1)Change of diagnosis to genetic syndrome (n=1)
Treadmill group (n=6)Mean age 21.76 (6.50)GMFCS level I (n=2)GMFCS level II (n=4)
Trial Diagram of Participants
Protocol for Treadmill Group
• 6 weeks, home‐based
• 6x/week, twice daily, for up to 20 min/each
• Minimal manual contact
• Progressively increased speed
• Mean minutes walked/day 28.2 ± 11.2
from personal archives, with permission from parents

no reprints without permission 8
Outcome Measures
• Blinded• Gross Motor Function Measure‐66 (GMFM‐66) Dimension D and E
• Peabody Developmental Motor Scales‐2 (PDMS‐2) Locomotion Subscale
• Parent‐Reported• Pediatric Evaluation of Disability Inventory (PEDI) Mobility Scale
• Fast Timed 10‐meter walk test
• Functional Mobility Scale
GMFM Dimension D and E
*p=0.004
PDMS‐2 Locomotion Subtest
**p=0.01
p=0.009

no reprints without permission 9
PEDI Mobility
*
**
p=0.01
p=0.09
p=0.04
Walking Speed
0
50
100
150
200
250
Child 1
Child 2
Child 3
Child 4
Child 5
Child 6
0
50
100
150
200
250
Child 1
Child 2
Child 3
Child 4
Child 5
Child 6
Control Group
Treadmill Group
Unable to walk with or without assistive device
Unable to walk with or without assistive device
Significant Between‐Group Results
• GMFM‐D at post‐test
• PDMS‐2 at post‐test and 1 month follow‐up
• PEDI at post‐test, 1 month and 4‐month follow‐up
• FMS at the post‐test
• Moderate effect size (Cohen’s d=0.47) for walking speed

no reprints without permission 10
Pre‐intervention
4 ‐month postintervention
Post‐intervention
1‐month post intervention
● ●● ●
●
●●●●
● ●
Control Group
Treadmill Group
●●●
● ●
●
● ●● ●
Control Group
Control Group
Control Group
Treadmill Group
Treadmill Group
Treadmill Group
● ●
● ●●
●●
●●
● ●● ●
●●●●
●●● ●●
● ●●
Functional Ambulation
● ●
Research
Reality
Perceived Problem
from personal archives, with permission from parents/students
Collaboration of clinical and academic
setting
Translation of Clinical Research into Practice
+
=
Supported Treadmill Exercise Program at
Sacramento State‐ Easter Seals
STEPS

no reprints without permission 11
STEPS‐Overview• Free group‐based treadmill program
at University
• Twice weekly sessions during spring and fall semesters for 14 weeks
• Sessions individualized for each child
• 3‐5 DPT students/day, supervised by PT/faculty
• Additional over‐ground walking activities
• Consultation/collaboration on orthotics/equipment
• >50 children served since Spring 2013
from personal archives, with permission from parents/students
Personalized Training
pictures from personal archives, with permission from parents/students
Effects of a Group‐Based Treadmill
Program on Pre‐Ambulatory Children with Neurodevelopmental Impairment
Katrin Mattern‐Baxter

no reprints without permission 12
Subjects
• n=12
• n=4 Cerebral Palsy
• n=5 genetic syndrome
• n=3 other
• Mean age 30.4 (19‐47) months
• M:F ratio 7:5
from personal archives, with permission from parents/students
Program Admission
Child receives physical therapy
Child shows signs of walking-readiness• sit for 30 seconds• take 5-7 steps when supported
Does not have any exclusion criteria• Uncontrolled seizures• Prior orthopedic surgery/contraindications
for standing/walking
PT refers child to
STEPS
Child attends treadmill sessions in addition to ongoing PT until independent walking onset or age 5 years
Outcome Measures
• At program entry and at end‐of program
– Timed 10 meter walk test
– Gross Motor Function Measure, Dimensions D and E
– Pediatric Evaluation of Disability Inventory‐Mobility Caregiver Scale
– Functional Mobility Scale

no reprints without permission 13
Results
17.4
37.30
29.7
0
5
10
15
20
25
30
35
40
week 1 week 7 week 13
minutes
Mean Minutes Walked/Week
0.18
0.25
0.29
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
week 1 week 7 week 13meters/second
Mean Treadmill Speed
77% attended
sessions
23%missed sessions
Program Utilization
Results
* **p=0.0005 p=0.001
p=0.001
Results
Pre‐Test Post‐Test
● ●● ●
● ●● ●
●● ●
● ●● ●
●●
● ●● ●
●●
●
Functional Mobility Scalep=0.039
Timed 10‐meter Walk Testp=0.06
no reprints without permission 14
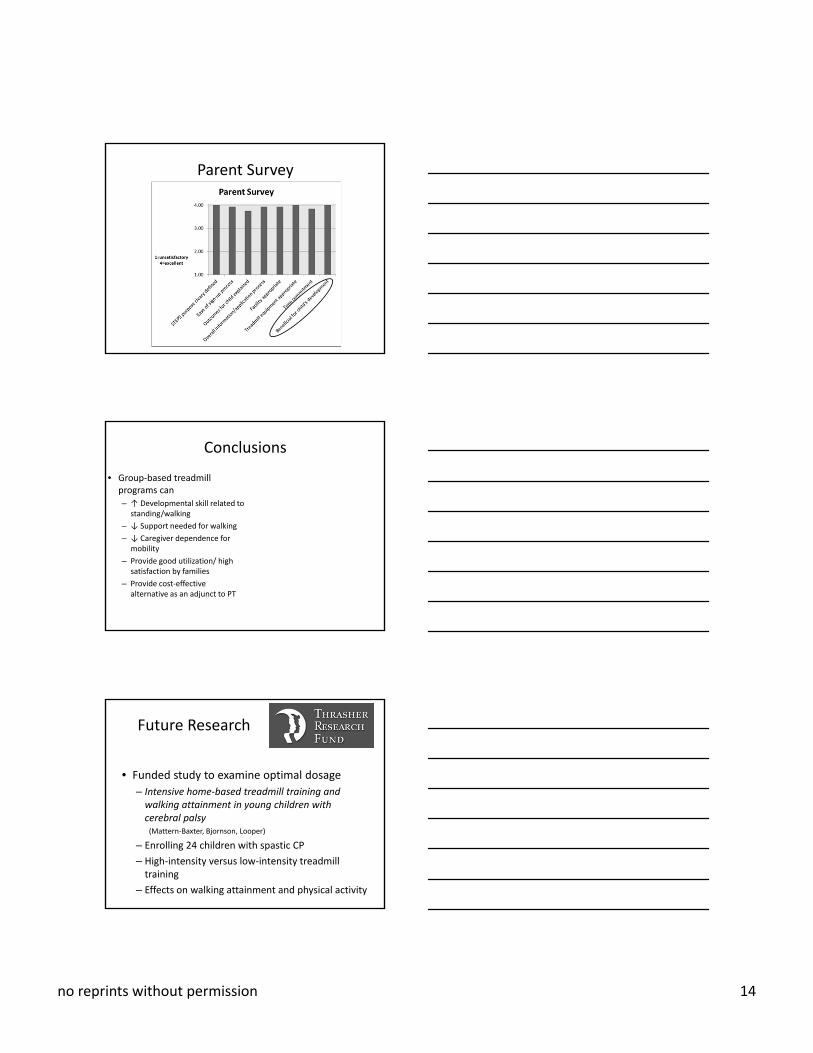
Parent Survey
Conclusions
• Group‐based treadmill programs can
– ↑ Developmental skill related to standing/walking
– ↓ Support needed for walking
– ↓ Caregiver dependence for mobility
– Provide good utilization/ high satisfaction by families
– Provide cost‐effective alternative as an adjunct to PT
Future Research
• Funded study to examine optimal dosage
– Intensive home‐based treadmill training and walking attainment in young children with cerebral palsy (Mattern‐Baxter, Bjornson, Looper)
– Enrolling 24 children with spastic CP
– High‐intensity versus low‐intensity treadmill training
– Effects on walking attainment and physical activity

no reprints without permission 15
Thank you
Thanks to all of the children and their families who participated and
all the DPT students who assisted during the studies
Objective
3. Describe muscle performance impairments in children with CP and the implications for treadmill training
Muscle Structure, Function, and Plasticity in CP: Implications for
Treadmill Training
Combined Sections Meeting2016
Noelle G. Moreau, PT, PhD

no reprints without permission 16
Theoretical Framework for Improving Walking
Task‐Specific
(Treadmill, BWSTT, robotic
devices)
Impairment‐based
(strength, power, ROM)
Do we need more practice?
Are we lacking the underlying
muscular resources?
International Classification of Function (ICF)
Activities
Gait
Cerebral Palsy
Body Structure
Muscle ArchitectureBody Functions
Muscle Function
Participation
Society
Theoretical Framework
Treatment & Dosing
Muscle Architecture
• Muscle architecture determines the force‐velocity properties of muscles!!

no reprints without permission 17
Muscle Architecture
• Muscle size is directly proportional to maximal force generation in healthy muscle
• Fiber length is proportional to the maximal shortening velocity of a muscle and excursion
• Fascicle or pennation angle ‐> allows more contractile material to
be packed in a given volume
“Muscles respond in a fairly stereotypical manner to the amount and type of
activity imposed upon them”Lieber et al, 2004
PositiveNegative• Bedrest• Immobilization• Spaceflight• Paralysis
• Resistance training• Exercise & Activity
Neurological Disorders‐Cerebral Palsy (CP)‐Stroke‐Traumatic Brain Injury

no reprints without permission 18
Muscle Structure – Function Relationships in CP
Muscle Performance
- Strength
- Power
Architectural Basis for Strength Deficits in CP
• Strength deficits ranging between 40% and 85% of normal have been reported for LE muscle groups (Eek & Beckung, DMCN, 2008; Ross &
Engsberg, DMCN, 2002; Wiley & Damiano, DMCN, 1998)
• Decreased muscle volume and cross‐sectional area of LE (14% to 50%) (Lampe et al,
Brain Dev, 2006; Oberhofer et al, Clin Biom, 2010; Moreau et al, DMCN, 2009; Elder et al., DMCN, 2003; Malaiya et al Electromyogr Kinesiol, 2007)
• Less sarcomeres working in parallel results in a decrease in force‐generating capacity
• Overlengthened sarcomeres (Lieber & Friden, Muscle Nerve, 2002; Smith et al, J Phys, 2011)
Activities
Gait
Cerebral Palsy
Body Structure
Muscle ArchitectureBody Functions
Muscle Function
Participation
Society
Strength Training??
Treatment & Dosing

no reprints without permission 19
Muscle Plasticity ‐ Strength
• Increase in plantarflexor muscle volume after 8 weeks of strength training (McNee et al, DMCN,
2009)
• Increase in quadriceps cross‐sectional area and muscle thickness after 8 weeks of knee extensor strength training (Moreau et al, NNR, 2013)
• No change in Walking or functional mobility!!
Evidence for muscle hypertrophy in response to strength training in CP but no change in walking!
Evidence: Strength Training in CP
• Despite moderate increases in strength, there is no higher level evidence that resistance training improves walking speed or other measures of functional walking capacity (Scianni et al, AJPT, 2009;
Verschuren et al, PTJ, 2011)
• Small but clinically insignificant effects on GMFM (Scianni et al, AJPT, 2009)
Muscle Power
• “the ability to exert a maximal force in as short a time as possible”
• “generating as much force as fast as possible”

no reprints without permission 20
Architectural Basis for Muscle Power Deficits
2 Important Components:
1. Muscle size 2. Fiber (fascicle) length
(Reproduced with permission: Lieber RL. Skeletal muscle structure, function, and plasticity: the physiological basis for rehabilitation. 3rd ed. Baltimore: Lippincott Williams & Wilkins; 2010).
Muscle Architectural Basis for Diminished Muscle Power
• Studies have shown decreases in rectus femoris and gastrocnemius cross‐sectional area and fascicle length in children with CP compared to TD children. (Moreau et al., 2009;
Malaiya et al, 2007; Mohagheghi et al, 2007; 2008)
Decreased Shortening Velocity
Decreased Force ProductionCSA
FascicleLength
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2771733/
Muscle Power ‐ CP
0
20
40
60
80
100
Peak Torque
Power
64%
18%
% of TD children
(Moreau et al, NNR, 2013)
Knee Extensors
↓ by 82%

no reprints without permission 21
Muscle Power
• Take Home: youth with CP have difficulty producing torque at higher speeds of movement, which is often required during daily activities; therefore, muscle power should be considered for therapeutic interventions!
Activities
Gait
Cerebral Palsy
Body Structure
Muscle ArchitectureBody Functions
Muscle Function
Participation
Society
Power Training??
Treatment & Dosing
Muscle Plasticity ‐ Power
• Increase in rectus femoris cross‐sectional area and fascicle length after 8 weeks of velocity training for knee extensor muscle power! (Moreau et al, NNR, 2013)
• Accompanied by increases in walking speed and functional mobility!!
Muscle architectural changes specific to power/velocity training in CP and improved walking!
no reprints without permission 22
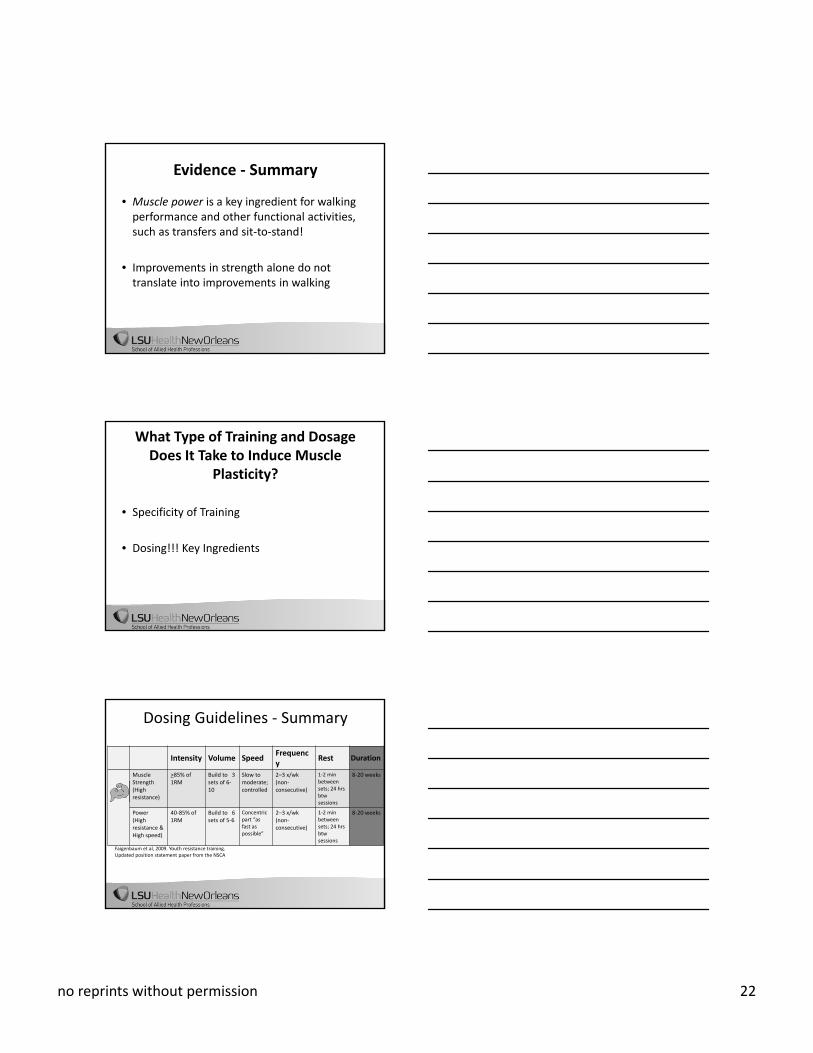
Evidence ‐ Summary
• Muscle power is a key ingredient for walking performance and other functional activities, such as transfers and sit‐to‐stand!
• Improvements in strength alone do not translate into improvements in walking
What Type of Training and Dosage Does It Take to Induce Muscle
Plasticity?
• Specificity of Training
• Dosing!!! Key Ingredients
Dosing Guidelines ‐ Summary
Intensity Volume SpeedFrequency
Rest Duration
Muscle Strength (High resistance)
>85% of 1RM
Build to 3 sets of 6‐10
Slow to moderate; controlled
2–3 x/wk (non‐consecutive)
1‐2 min between sets; 24 hrs btwsessions
8‐20 weeks
Power (High resistance & High speed)
40‐85% of 1RM
Build to 6 sets of 5‐6
Concentric part “as fast as possible”
2–3 x/wk (non‐consecutive)
1‐2 min between sets; 24 hrs btwsessions
8‐20 weeks
Faigenbaum et al, 2009. Youth resistance training. Updated position statement paper from the NSCA
no reprints without permission 23
Activities
Gait
Cerebral Palsy
Body Structure
Muscle ArchitectureBody Functions
Muscle Function
Participation
Society
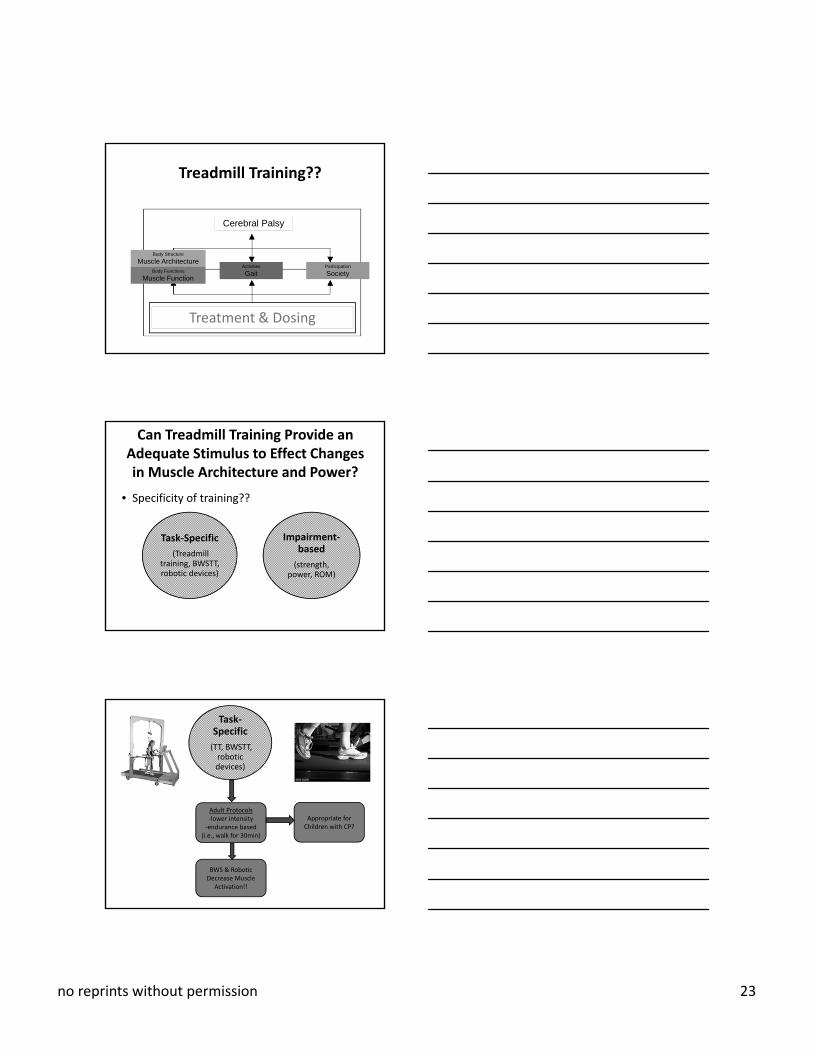
Treadmill Training??
Treatment & Dosing
Can Treadmill Training Provide an Adequate Stimulus to Effect Changes in Muscle Architecture and Power?
• Specificity of training??
Task‐Specific
(Treadmill training, BWSTT, robotic devices)
Impairment‐based
(strength, power, ROM)
Task‐Specific
(TT, BWSTT, robotic devices)
Adult Protocols‐lower intensity‐endurance based
(i.e., walk for 30min)
Appropriate for Children with CP?
BWS & Robotic Decrease Muscle
Activation!!
no reprints without permission 24
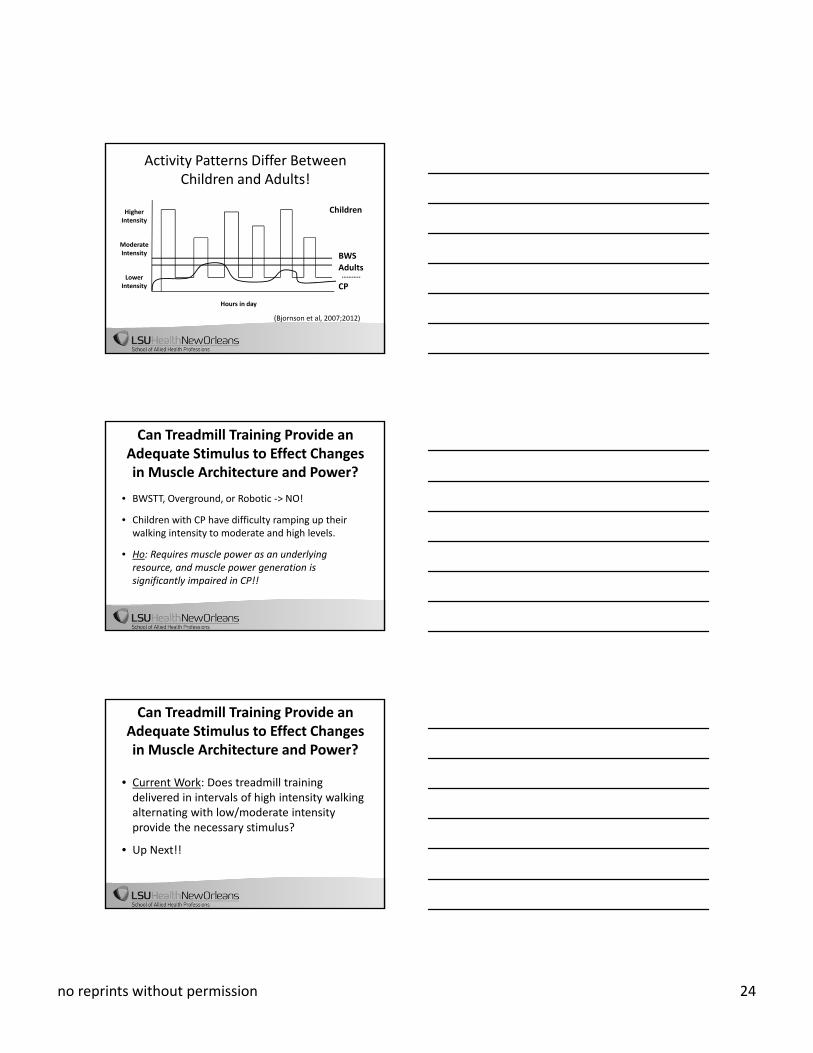
Activity Patterns Differ Between Children and Adults!
Higher Intensity
Hours in day
………..
Moderate Intensity
Lower Intensity CP
Adults
Children
BWS
(Bjornson et al, 2007;2012)
Can Treadmill Training Provide an Adequate Stimulus to Effect Changes in Muscle Architecture and Power?
• BWSTT, Overground, or Robotic ‐> NO!
• Children with CP have difficulty ramping up their walking intensity to moderate and high levels.
• Ho: Requires muscle power as an underlying resource, and muscle power generation is significantly impaired in CP!!
Can Treadmill Training Provide an Adequate Stimulus to Effect Changes in Muscle Architecture and Power?
• Current Work: Does treadmill training delivered in intervals of high intensity walking alternating with low/moderate intensity provide the necessary stimulus?
• Up Next!!

no reprints without permission 25
Objective
4. Describe implementation and outcomes of short‐burst interval treadmill training in ambulatory children with CP
Short –Burst Interval Training: Walking Capacity &Performance-
Pilot study
Bjornson, Moreau, Bodkin, Rashid
Funding: SCRI CHBD Stimulus Fund 2013
K23 HD060764, UL1RR025014, NCT01217242
Background/Significance:
• Muscle power production and rapid force development are deficient in children with CP as compared to TD youth (Moreau, 2013 & 2012).
• Youth with CP have limitations in the ability to ramp up their walking activity into medium and/or high stride rates. (Bjornson, 2013, 2007)
• TD children engage in very short bursts of intense walking and physical activity interspersed with varying intervals of low and moderate intensity (Armstrong, 1990, Bailey, 1995).
• LTT protocols for children with CP have been based on adult walking activity patterns and do not approximate the high intensity short burst patterns of TD children (Dobkin, 2006 Duncan, 2011)

no reprints without permission 26
Short-burst Interval Locomotor Training
• will enhance muscle power production and subsequently
• walking performance and capacity
• through training patterns that are motivating
• and mirror the walking and physical activity patterns of TD youth
Pilot Study/Sample:
• Pre/Post Design
• N = 6, Spastic Diplegia
• GMFCS Levels• II = 4
• III = 2
• Average Age: 7.7 (5.1 to 10.9)
• 3 = female
• Independent walking primary mode of mobility
• No ortho/neurosurgery in last 12 months
• No injection therapy in last 3 months
• No serial casting in 30 days
• Uncontrolled seizure disorder
Short Burst Interval Training Protocol:
• 20 total sessions
• 5 days/week over 4 weeks
• 30 minutes total treadmill walking• 30 seconds – self selected speed – “slow”
• 30 seconds - fast walking speed- “fast”
• Wearing current clinically prescribed orthotics• Screen fail 2 subjects – in adequate orthotic support
• Training speeds based on 75-85% of baseline 10 meter walk tests
• Training speeds:• Average self-selected speed: 1.5 mph
• Average Fast speed: 2.6

no reprints without permission 27
Short-Burst Interval Treadmill training
Outcomes:
• Walking Capacity – clinic based measures
• 10 meter walk test (10MWT)- m/sec
• Self-selected walking speed
• Fast walking speed
• 1 Minute Walk Test (1MWT) – meters
Outcomes:
• Walking Performance- community walking activity
• StepWatch accelerometer
• Average Strides/day
• Peak Activity Index –average step rate/minute of the highest 30 minutes/day
• % of walking time :
• low, moderate and high activity*
*Bjornson, 2010 Ped Ex Sci, Bjornson 2010, 2014

no reprints without permission 28
Methods:
• Average of 5 days of StepWatch accelerometry data.
• Walking stride activity was defined as • Low 1-30 strides/min
• Moderate 31-60 strides/min
• High > 60 strides/min
*Bjornson, 2010 Ped Ex Sci, Bjornson 2010, 2014
Results: Walking Capacity – clinic measures
10 Meter Self – Selected walking speedAverage increase of .20 m/sec (MCID .1 m/sec)
MP
H

no reprints without permission 29
10 Meter Fast walking speedAverage increase of .17 m/sec (MCID .1 m/sec)
MP
H
One Minute Walk Test (meters)Average increase 11.4 meters
Me
ters
Results: Community Walking Performance

no reprints without permission 30
Walking Performance: Average Strides/day TDY and youth with CP
Bjornson, 2014 Dis & Rehab
SW: Average Strides/day
Mean difference GMFCS level I to II = 1284
Bjornson, 2014 Dis & Rehab
Average Strides/day Average increase 1441 strides/day(GMFCS level I to II = 1284 strides)
Bjornson, 2014 Dis & Rehab

no reprints without permission 31
Average strides/day
StepWatch: Peak Stride Activity Index
StepWatch: Peak Stride Activity IndexAverage increase 3.4 stride/min

no reprints without permission 32
StepWatch: Peak Stride Activity Index
Average % of Total Strides/day: Low, Medium & High Stride rates –TDY & Youth with CP
Bjornson, 2014 Dis & Rehab
Average % of Total Strides/day- Low, Medium & High: PRE Training
no reprints without permission 33
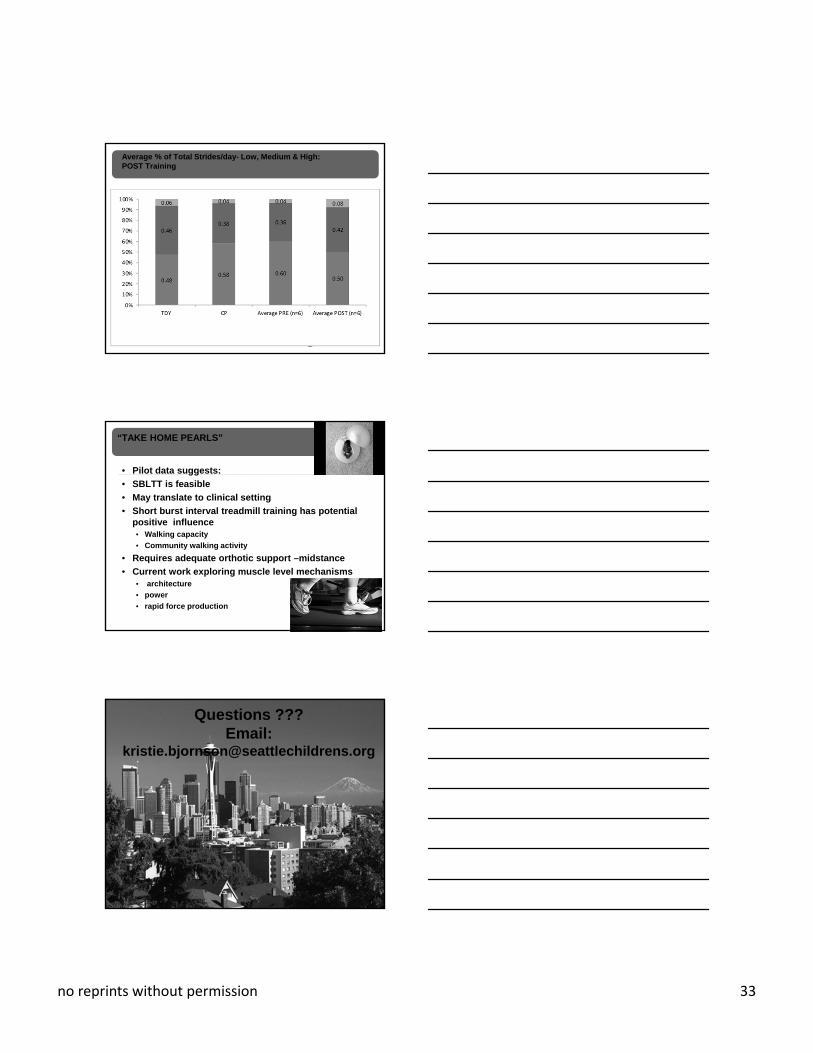
Average % of Total Strides/day- Low, Medium & High: POST Training
“TAKE HOME PEARLS”
• Pilot data suggests:
• SBLTT is feasible
• May translate to clinical setting
• Short burst interval treadmill training has potential positive influence • Walking capacity
• Community walking activity
• Requires adequate orthotic support –midstance
• Current work exploring muscle level mechanisms• architecture
• power
• rapid force production
Questions ???Email:
no reprints without permission 34
References• Crair MC, Malenka RC. A critical period for long‐term potentiation at
thalamocortical synapses. Nature. 1995; 375(6529):325‐8.
• Huttenlocher PR, de Court. The development of synapses in striate cortex of man. Hum Neurobiol. 1987; 6:1–9.
• Jeng SF, Chen LC, & Yau KIT. Kinematic analysis of kicking movements in preterm infants with very low birth weight and full‐term infants. Physical Therapy, 2002; 82(2): 148–159.
• Looper J, UlrichDA. Effects of various treadmill interventions on the development of joint kinematics in infants with Down syndrome. Phys Ther. 2010;90(9):1265‐76.
• Thelen E., Fischer DM. Newborn stepping: An explanation for a "disappearing" reflex. Developmental Psychology. 1982; 18(5): 760‐775.
• Ulrich BA, Ulrich DA. Spontaneous Leg Movements of Infants with Down Syndrome and Nondisabled Infants. Child Development. 1995; 66(6):1844–1855.
• Ulrich DA, Ulrich BD, Angulo‐Kinzler RM, Yun J. Treadmill training of infants with Down syndrome: evidence‐based developmental outcomes. Pediatrics. 2001;108(5):E84.
References• Wu et al., Exploring effects of different treadmill interventions on walking onset
and gait patterns in infants with Down syndrome. Dev Med Child Neurol. 2007; 49: 839–845.
• Zelazo PR, Zelazo NA, Kolb S. "Walking" in the newborn. Science. 1972; 176(4032):314‐5.
• Zelazo PR. The development of walking: new findings and old assumptions. J Mot Behav. 1983;15(2):99‐137.
• Valentin‐Gudiol M, Mattern‐Baxter K, Girabent‐Farrés M, Bagur‐Calafat C, Hadders‐Algra M, Angulo‐Barroso R. Treadmill interventions with partial body weight support in children under six years of age at risk of neuromotor delay. Cochrane Database Syst Rev; 2011; Art. No.: CD009242.
• Mattern‐Baxter K, McNeil S, Mansoor JK. Effects of Home‐Based Locomotor Treadmill Training on Gross Motor Function in Young Children With Cerebral Palsy: A Quasi‐Randomized Controlled Trial. Arch Phys Med Rehabil; 2013; 94:2061‐2067
• Mattern‐Baxter K. Effects of a Group‐Based Treadmill Program on Pre‐Ambulatory Children with Developmental Disability.2015; Ped Phys Ther (in press)
REFERENCES:
• Bjornson, K.F., et al., Ambulatory Physical Activity Performance in Youth With Cerebral Palsy and Youth Who Are Developing Typically. Physical Therapy, 2007. 87(3): p. 248‐257.
• Bjornson, K., Zhou, C., Stevenson, R.D., Christakis, D., Song, K., Walking activity patterns in youth with cerebral palsy and youth developing typically. Disability & Rehabilitation, 2014 36(15): p. 1279‐84.
• Armstrong, N., et al., Patterns of physical activity among 11 to 16 year old British children. BMJ, 1990. 301: p. 294‐5.
• Bailey, R.C., et al., The level and tempo of children's physical activities: an observational study. Medical Science Sport Exercise, 1995. 27(7): p. 1033‐1041.
• Dobkin B, A.D., Barbeau H, Basso M, Behrman A, Deforge D, Ditunno J, Dudley G, Elashoff R, Fugate L, Harkema S, Saulino M, Scott M; Spinal Cord Injury Locomotor Trial Group., Weight‐supported treadmill vs over‐ground training for walking after acute incomplete SCI. Neurology, 2006. 66(4): p. 484‐93.
• Duncan, P.W., et al., Body‐Weight–Supported Treadmill Rehabilitation after Stroke. New England Journal of Medicine, 2011. 364(21): p. 2026‐2036.
• Bjornson, K., et al., Measurement of walking activity throughout childhood: influence of leg length. Pediatric Exercise Science, 2010. 22(4): p. 581‐95.

no reprints without permission 35
References• Damiano, D. L., Martellotta, T. L., Sullivan, D. J., Granata, K. P., & Abel, M. F. (2000).
Muscle force production and functional performance in spastic cerebral palsy: Relationship of cocontraction.
• Eek MN, Beckung E. Walking ability is related to muscle strength in children with cerebral palsy. Gait Posture 2008;28(3):366‐371.
• Elder GC, Kirk J, Stewart G et al. Contributing factors to muscle weakness in children with cerebral palsy. Dev Med Child Neurol 2003;45(8):542‐550.
• Faigenbaum, A. D., Kraemer, W. J., Blimkie, C. J., Jeffreys, I., Micheli, L. J., Nitka, M., et al. (2009). Youth resistance training: Updated position statement paper from the national strength and conditioning association. Journal of Strength and Conditioning Research / National Strength & Conditioning Association, 23(5 Suppl), S60‐79.
• Lampe R, Grassl S, Mitternacht J, Gerdesmeyer L, Gradinger R. MRT‐measurements of muscle volumes of the lower extremities of youths with spastic hemiplegia caused by cerebral palsy. Brain Dev 2006;28(8):500‐506.
• Lieber RL, Friden J. Spasticity causes a fundamental rearrangement of muscle‐joint interaction. Muscle Nerve. 2002;25(0148‐639; 2):265‐270.
References• Lieber RL, Steinman S, Barash IA, Chambers H. Structural and functional changes in
spastic skeletal muscle. Muscle Nerve 2004;29(5):615‐627.
• Malaiya R, McNee AE, Fry NR, Eve LC, Gough M, Shortland AP. The morphology of the medial gastrocnemius in typically developing children and children with spastic hemiplegic cerebral palsy. J Electromyogr Kinesiol 2007;17(6):657‐663.
• Moreau NG, Teefey SA, Damiano DL. In vivo muscle architecture and size of the rectus femoris and vastus lateralis in children and adolescents with cerebral palsy. Dev Med Child Neurol 2009;51(10):800‐806.
• Moreau NG, Simpson KN, Teefey SA, Damiano DL. Muscle architecture predicts maximum strength and is related to activity levels in cerebral palsy. Phys Ther2010;90(11):1619‐1630.
• Moreau NG, Falvo MJ, Damiano DL. Rapid force generation is impaired in cerebral palsy and is related to decreased muscle size and functional mobility. Gait Posture2012;35(1):154‐158.
• Moreau, N. G., & Holthaus, K. (2011). Motor severity negatively affects muscle architecture in CP: a comparison between GMFCS levels, hemiplegia, and typically developing children. Dev.Med.Child Neurol., 53(s5), 78
References• Moreau NG, Holthaus K, Marlow N. Differential Adaptations of Muscle
Architecture to High‐Velocity Versus Traditional Strength Training in Cerebral Palsy. Neurorehabil Neural Repair 2013,27(4): 325‐34
• Oberhofer K, Stott NS, Mithraratne K, Anderson IA. Subject‐specific modelling of lower limb muscles in children with cerebral palsy. Clin Biomech (Bristol , Avon )2010;25(1):88‐94.
• Perry, J., & Burnfield, J. M. (2010). Gait analysis: Normal and pathological function. Thorofare, NJ: SLACK, Inc.
• Rose J, McGill KC. Neuromuscular activation and motor‐unit firing characteristics in cerebral palsy. Dev Med Child Neurol 2005;47(5):329‐336.
• Ross SA, Engsberg JR. Relation between spasticity and strength in individuals with spastic diplegic cerebral palsy. Dev Med Child Neurol 2002;44(3):148‐157.
• Smith LR, Lee KS, Ward SR, Chambers HG, Lieber RL. Hamstring contractures in children with spastic cerebral palsy result from a stiffer extracellular matrix and increased in vivo sarcomere length. J Physiol (Lond ). 2011;589(1469‐7793; 0022‐3751):2625‐2639.
• Wiley ME, Damiano DL. Lower‐extremity strength profiles in spastic cerebral palsy. Dev Med Child Neurol 1998;40(2):100‐107.