Embed Size (px)
Citation preview

Deep Vein Thrombosis
Unit 4 & 7Guide:
Dr. (Col.) S. V. PanchabhaiDr. B. D. Dhaigude
Problem Based LearningDept of General Surgery
29rd February, 2016
1

Learning Objectives
• To learn the protocols for diagnosis and treatment of deep vein thrombosis.
• To identify and discuss problems seen in diagnosis and treatment of deep vein thrombosis.
2

Cases
1) Provoked DVT : DVT where there is an identifiable risk factor that likely caused the DVT.
2) Unprovoked DVT : DVT where there is no identifiable risk factor that likely caused the DVT.
3) Proximal DVT [ileofemoral] with post-thrombotic syndrome
3

• It is important to distinguish between a provoked and unprovoked DVT because the guidelines for extended anticoagulation take these aspects into account.
4

Case 1
• A 40 yr old male patient had presented with ℅ painful swelling of his right lower limb since 4 days.– Sudden onset– Increasing gradually– Severe cramping pain in calf and thigh– Increases on walking and movement of the limb
• No C/O chest pain, breathlessness• No C/O pain in abdomen
5

• Patient underwent left sided nephrectomy 15 days back for left side renal cell carcinoma.– Operative time:– Inferior Vena Cava exploration was done with
thrombectomy.– Post operatively he received limb physiotherapy as
DVT prophylaxis but was not ambulatory for 7 days.
– Inj. Heparin was given post operatively 5000IU IV 12th hourly
• H/O chronic tobacco chewing. No any other addictions. 6

7
• P/H: Not a K/C/O thrombophilia, DM, HTN, IHD or any major illness
• F/H: No family history of VTE• G/E:
• Edema present over right lower limb from foot up to thigh• No Pallor, cyanosis, clubbing, icterus, lymphadenopathy• P: 82/min, regular rhythm• P: 130/80 mm Hg
• On inspection of right lower limb, swelling & redness present from foot to thigh. No dilated, engorged veins. Skin is stretched and shiny.

• Palpation:–Normal temp.–Tenderness present over calf and thigh–Pitting edema present till lower thigh–Homan Sign Positive–Moses Sign Positive.–Peripheral pulsations normal.–No cough impulse felt at SFJ–No palpable inguinal lymph nodes
• Left lower limb is normal• P/A:
–Scar of nephrectomy is seen over left lumbar region and normal. No guarding/rigidity.
–No palpable lump/organomegaly 8

• Wells score: 7 (high probability)• Duplex ultrasound:
–Common femoral, deep femoral, popliteal & posterior tibial vein show echogenic Thrombus & absent flow.
–GSV, SSV, ATV normal–SFJ competent–Subcutaneous oedema noted–Few inguinal LN enlarged.
9

Course in hospital • TPR/BP charting done• PT-INR done every alternate day• Limb elevation was given to patient• Magnesium sulphate dressing applied on
lower limbs.
10

•Pt. started on Inj. Unfractionated Heparin 5000 IU IV 6 HRLY for 5 days
•Inj. Dextran 40 mg 2-6 drops/min IV over 24hrs
•Inj. Tramadol 1 amp in 100 ml NS IV 12 hrly;•Inj. Emeset 4mg IV 12 hrly;•Inj. Pan 40 mg IV 12 hrly;•T. Warfarin 5 mg OD from 1st day of admission was started.
•On 5th INR was 2.3 so Inj. Heparin was stopped.
11

•T. Warfarin 5 mg OD•Pt. adviced to do PT INR weekly so as to see that INR is being maintained between 2-3
•Avoid sitting, standing, or lying down for long periods without moving your legs and feet.
• When traveling by car, make frequent stops to get out and move around.
• On long airplane, train, or bus rides, get up and move around when possible.
• If patient can’t get up, wiggle toes and tighten calves.
On discharge
12

Lifestyle Changes
•Patient was adviced simple activities such as walking.
•Maintain a healthy weight.•Total cessation of smoking, tobacco use & Alcohol intake
13

Preoperative VTE risk assessment
• American College of Chest Physicians (ACCP) guidelines for prevention of VTE in non-orthopedic surgical patients recommends:– Rogers score– Caprini score
14

15

16

Case 2
• A 33 yr old male patient came with ℅ painful swelling over his Lt. lower limb since 3 days• acute onset • gradually progressive• severe cramping pain in L.t lower limb.
• No h/o trauma, pain abdomen, breathlessness, chest pain
• No h/o recent immobilozation or surgery
17

•Past History: Not significant, no known risk factors for DVT
•O/E- –P- 82/min, regular rhythm –BP- 130/80 mm Hg. –No Pallor, cyanosis, clubbing, icterus, lymphadenopathy
–Edema present over left lower limb•On inspection of left lower limb
–Edema & redness present up to lower thigh.–no dilated/engorged veins.–Stretched and shiny skin.
18

•Palpation- –Temperature normal–Calf tenderness present–Pitting edema present up to lower thigh
•Femoral, Dorsalis pedis pulses normal•Left LL Venous Doppler show echogenic thrombus & absent flow in Popliteal & posterior tibial veins.
–GSV, SSV normal–SFJ competent–Subcutaneous oedema noted
•All blood investigations were within normal range 19

Impression: UNPROVOKED DVT
Cancer screening: • CECT abdomen and pelvis: normal study• CECT chest: normal study• Upper GI endoscopy: normal study
20

Treatment
Inj. Heparin 5000 IU IV 6th hourlyInj. Tramadol 1 amp in 100 ml NS IV 12 hrly;Inj. Emset 4mg IV 12 hrly;Inj. Pan 40 mg IV 12 hrly;T. Warfarin 5 mg OD from 1st day of admissionPT/INR achieved 2.5 on 4th day and Inj. Heparin
was stopped.No extension of thrombus on repeat ultrasound
on the 7th day.21

•On 10th day of admission, there was significant decrease in edema and pain.
•INR of 2.4•Hence, patient was discharged.
22

On discharge•T. Warfarin 5 mg OD for atleast 3 months •Pt. adviced to do PT INR weekly so as to see that INR is being maintained between 2-3
•DVT stockings•Avoid immobilization•Immediate follow up in case of bleeding/reappearance of symptoms
23

Lifestyle changes
•Patient was adviced simple activities such as walking.
•Maintain a healthy weight.•Cessation of tobacco, alcohol intake.•Plenty of fluid intake.
24

• Up to 10% of patients with an unprovoked venous thromboembolism (VTE) are diagnosed with cancer within a year following their event
• This observation causes some providers to order extensive cancer workups in patients with unprovoked venous thromboembolism. Whether this practice is prudent is a matter of debate. [6,7]
6. Incidence and risk factors for venous thromboembolism after laparoscopic surgery for colorectal cancer. Cecilia Becattini,1 Fabio Rondelli et al. Haematologica 2015 Jan; 100(1): e35–e38.
7. Screening for Occult Cancer in Unprovoked Venous Thromboembolism. Carrier M, Lazo-Langner A, Shivakumar S et al. N Engl J Med. 2015 Aug 20;373(8):697-704. 25

•The SOME study found no benefit of adding an abdominal and pelvic CT to standard screening in patients with unprovoked VTE. Standard testing in this study varied somewhat from current screening recommendations because it included PSA testing and did not include colon cancer screening.[7]
7. Screening for Occult Cancer in Unprovoked Venous Thromboembolism. Carrier M, Lazo-Langner A, Shivakumar S et al. N Engl J Med. 2015 Aug 20;373(8):697-704.
26

• It's unclear if an unprovoked VTE is a marker of increased cancer risk. In order to evaluate this, a group of patients with unprovoked VTE would have to be compared with a matched control group that underwent all the same testing.
• No such study has been performed. • The high incidence of cancer in patients diagnosed
with VTE may be a product of surveillance bias as opposed to an association of VTE with cancer risk.
• Some studies have found that the risk of cancer following VTE returns to normal after 6 months. This finding tends to argue against VTE being a marker of increased cancer risk. [7]
27

Case 3• A 42 years old female came with c/o ulcer
over her left foot since 1 month. – Patient had itching and she scratched the skin.– Painless. – No increase or decrease in size. – No pus discharge or bleeding from the ulcer.
• C/O swelling of left leg with dull aching pain in calf. Increases as the day progresses.
• No C/O dilated veins over lower limbs• No C/O chest pain, breathlessness
28

• Past history: Patient had DVT of left lower limb 2 years back. – Ultrasound: DVT of ileofemoral and popliteal
veins.– Patient had received unfractionated heparin for
initial treatment and had taken warfarin for 3 months.
– Patient again developed similar complaints and was diagnosed to have recurrent DVT on ultrasound. She again received a similar treatment.
• Patient gives no history of receiving thrombolysis
29

• P/H/O developing ulcer at the same site 3 months back. She was advised dressings and compression bandage.
• Patient has no history of any risk factors for developing DVT (unprovoked DVT)
• Not a K/C/O Diabetes Mellitus, hypertension, ischaemic heart.
• G/E: – Edema present over left lower limb up to tibial
tuberosity.– Vitally stable– No other abnormality 30

• L/E: Ulcer and left lower limb– Single, non-tender, 5×5 cm, circular ulcer present
over medial aspect of dorsum of left foot.– Healing edge, minimal slough seen over floor.– No discharge or bleeding.– Hyperpigmented skin present over foot and ankle.– Pitting edema present up to 10 cm below tibial
tuberosity over shin of tibia.– Dilated veins not visible over the limb.– No calf tenderness.
• Right lower limb is normal.31

• Wells score: 3 (high probability).• Duplex Ultrasound:
– Dilated GSV (>6mm) with SFJ incompetence in left lower limb.
– Subcutaneous edema below knee. – No DVT. Deep veins are patent – Right lower limb veins normal.
• Patient’s coagulation profile, CBC, LFTs, RFTs, blood sugar level, lipid profile and glycosylated haemoglobin were normal
IMPRESSION: Post-thrombotic syndrome32

Post Thrombotic Syndrome• The syndrome is marked by
– leg pain, – swelling, – leg heaviness, – skin changes (brownish pigmentation), – venous insufficiency with ulcers.
• It occurs in up to a third of patients after their first proximal DVT. It typically occurs within 2 years after the DVT.
33

34

• In most cases, symptoms are mild (small amount of leg swelling). Severe symptoms are rare (intense pain and leg ulcers).
• In one study, the cumulative incidence of severe symptoms after 5 years of follow-up was 8%. [2, 8]
• Can be reduced by wearing compression stockings2. Pulmonary embolism and deep vein thrombosis. Goldhaber SZ, Bounameaux H. Lancet 2012 May 12;379(9828):1835-46.8. Deep vein thrombosis. Kyrle PA, Eichinger S. Lancet 2005 Mar 26-Apr 1;365(9465):1163-74.
35

• The AHA recommends that patients with proximal DVT wear knee-high, graduated elastic compression stockings (30 - 40 mmHg at the ankle) daily for 2 years after their DVT to prevent post-thrombotic syndrome.
Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Jaff MR, McMurtry MS et al. Circulation. 2011 Apr 26;123(16):1788-830.
36

• The ACCP guidelines from 2015 do not recommend compression stockings.
• In practice, compression stockings can be uncomfortable and hot to wear, and compliance with this recommendation will likely be low in many patients.
• A randomized, controlled trial published in the Lancet in Dec 2013 found no benefit of compression stockings in preventing post-thrombotic syndrome. [10]10.Elastic compression stockings—is there any benefit? Arina J ten Cate-Hoek. The lancet. Volume 383, No. 9920, p851–853, 8 March 2014 37

• Compression stockings may also be used to treat post-thrombotic syndrome, although their efficacy in this situation remains unproven
• Patients with obstructive clots that are thought to be causing post-thrombotic syndrome may be treated with angioplasty and stenting of the lesion. [9]
9. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Jaff MR, McMurtry MS et al. Circulation. 2011 Apr 26;123(16):1788-830. 38

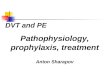
DVT
Symptoms of PTS
Conservative treatment
Improvement Conservative
treatment
No improvement
Ultrasound
Reflux
Superficial
Ablation
Perforator
Interruption
Obstruction
Deep
Phlebography
Stenting, Bypass, Endophlebectomy
Reflux + Obstruction
Deep
Phlebography
Stenting, Bypass, Valve repair, Valve transfer,
Endophlebectomy
No symptoms of PTS
Observe
39

Advice
•Patient was advised continuous use of compression stockings.
•Lifestyle modifications.•Ablation of superficial veins in case of reccurance of ulcer.
•Immediate follow up in case of sudden onset of pain and swelling.
40

Definition
• Deep venous thrombosis is the formation of a semisolid coagulum within flowing blood in any of the deep veins of the body, usually in the lower limb or pelvic veins.
41

VEINS OF LOWER LIMB•Classification:
–Superficial veins–Deep veins–Perforating veins
•Superficial veins:
–Includes great and small saphenous veins and their tributaries
–They drain into deep veins through perforating
veins42

Lower Limb veins
43

44
• GSV ends at SFJ roughly 2.5 cm below and lateral to pubic tubercle.
• The lesser saphenous vein terminates at a variable site in the popliteal fossa.

Short Saphenous Vein
45

Deep Calf Veins
• Arise from three pairs of venae commitantes, which accompany the three crural arteries (anterior and posterior tibial and peroneal arteries)
• These six veins intercommunicate and join in the popliteal fossa to form the popliteal vein, which also receives the soleal and gastrocnemius veins.
46

Perforating Veins Of leg
• Perforating veins- connect superficial veins with deep veins.
• Perforators- –1-adductor canal perforator,–2-below knee peforator,–3-medial perforator,–4-lateral perforator
47

Deep Veins of Thigh• The popliteal vein passes up through the
adductor hiatus to enter the subsartorial canal as the femoral vein, which receives the deep (profunda) femoral vein (or veins) in the femoral triangle before passing behind the inguinal ligament to become the external iliac vein.
48

Pelvic Veins (MAJOR )
• The internal iliac vein joins with the external iliac vein in the pelvis to form the common iliac vein.
• The left common iliac vein passes behind the right common iliac artery to join the right common iliac vein on the right side of the abdominal aorta to form the inferior vena cava.
49

ETIOLOGY • DVT usually originates in the lower extremity
venous system, starting at the calf vein and progressing proximally to involve popliteal, femoral, or iliac system.
• 80 -90 % pulmonary emboli originates here
50

Virchow’s triad • More than 100 years ago, Virchow described a triad
of factors for the development of venous thrombosis-
• Venous stasis • Endothelial damage• Hypercoagulable state
51

Risk factors for VTE
Venous Stasis Hypercoagulability
Inherited
Acquired
Endothelial Injury
52

Venous stasis• Age: Incidence increases with advancing age• Obesity: >BMI > is DVT• Prolonged bed rest (4 days or more) • Lower limb fracture: A cast on the leg • Limb paralysis from stroke or spinal cord
injury • Extended travel (>6 hours)
53

Hypercoagulability• Acquired:
– Surgery and trauma are responsible for up to 40% of all thromboembolic disease
– Malignancy – Hormonal therapy: (due to a fall in protein ‘S)
Increased estrogen occurs during as in pregnancy and HRT, OCP Taking women.
– Pregnancy and puerperium– Nephrotic syndrome: loss of antithrombin III in urine– Antiphospholipid antibody syndrome
54

– Systemic Lupus Erythematosus(SLE)– Inflammatory Bowel Disease(IBD)
• Inherited:– Factor V leiden mutation– Prothrombin 20210 gene variant– Antithrombin deficiency– Protein C deficiency– Protein S deficiency– Factor XI elevation– Dysfibrongenemia/hyperfibrogenemia– Homocysteinemia
55

• Trauma• Surgery• Peripheral and Central venous lines
Iatrogenic causes of venous thrombosis are increasing due to the widespread use of central venous catheters, particularly subclavian and internal jugular lines. These lines are an important cause of upper extremity DVT, particularly in children. Femoral vein cannulation and Venesection for IV therapy (prolong duration) predispose for DVT
Endothelial Injury
56

Clinical Pathophysiology • An intimal defect often works
as a nidus for clot formation. • Initially a platelet aggregate,
develops.• Subsequently clotting factors
through intrinsic and extrinsic pathway fibrin and red cells form a mesh until the lumen clot occludes the vein wall.
57

• Coagulation cascade promotes clot to growth proximally.
• Thrombus extend from the superficial veins into the deepveins.
• After detachment passesthrough vena cava, through the right heartand from which it canembolize to one orboth the lungs via pulmonary arteries.
58

• TFPI: Tissue Factor Pathway Inhibitor59

60

• Opposing the coagulation cascade is the endogenous fibrinolytic system.
• After the clot organizes or dissolves, most veins will recanalize in several weeks.
• Residual clots retract as fibroblasts and capillary development lead to intimal thickening.
• Venous hypertension and residual clot may destroy valves, leading to the postphlebitic syndrome, which may develop within 2 years
61

An Organised Clot (c) Thrombus ( T)
62

Clinical Features of DVT• Many of the patients with DVT have no
symptoms.
• Signs and symptoms alone are not sufficiently Sensitive or Specific to make a diagnosis, but when considered in conjugation with known risk factors can help to determine the possibility of the DVT.
63

Clinical Features of DVT
1.Calf pain or tenderness or both
2.Swelling with pitting oedema
3.Increase in local temparature and fever
4.Redness or Discolouration
5.Dilatation of superficial veins
64

Less frequent manifestations of DVT includes –
• Phlegmasia cerulea dolens
• Phlegmasia alba dolens
• Venous gangrene
65

Phlegmasia cerulea dolens
• Extensive DVT of the major axial deep venous channels of the lower extremity with relative sparing of collateral veins causes a condition called phlegmasia cerulea dolens
• The leg becomes blue in colour, swollen and painful
• Which may result in venous gangrene.
66

67

Phlegmasia alba dolens• When the thrombosis extends to the
collateral veins, massive fluid sequestration and more significant edema ensue, resulting in a condition known as phlegmasia alba dolens.
• Also known as Milk leg or White leg.• The leg is pale and cold, secondary to arterial
insufficiency from dramatically elevated below lower knee compartment pressures
• Extremely tender• May result in venous gangrene.
68

69

Diagnosis of DVT• A good clinical assessment along with the proper
examinations of the patient supported with use of the imaging devices (such as ultrasound, MRI etc.) can make out the proper diagnosis of the DVT.
70

• Careful inspection of the affected limb.
• Palpation of peripheral pulses and evaluation of capillary refill is important to assess limb perfusion.
• Evaluation of joint pathology and neurological defect is also important.
71

• Homans sign ––Pain in the calf region or knee with forced dorsiflexion of the foot.
• Moses sign ––Gentle squeezing of the lower part of the calf from side to side causes severe pain.
72

• Neuhofs sign ––Thickening and deep tenderness elicited while palpating deep in calf muscles.
• Lintons sign ––After applying torniquet at SFJ, patient made to walk, then limb is elevated in supine position, prominent superficial veins will observed.
73

• Search for the stigmata of PE such as ––Tachycardia–Tachypnea–Chest discomfert
• Rule out the other underlying predisposing factors.
• The most studied clinical prediction rule to help in diagnosing the condition is Wells score or criteria.
74

Diagnostic AlgorithmSTEP 1 - Use Wells scoring to determine patient's risk of DVT
STEP 2 - Determine probability of DVT
High probability• Perform duplex ultrasound
Moderate or low probability• Order D-dimer• If D-dimer is elevated, order duplex ultrasound• If D-dimer is normal, DVT unlikely
75

76
Finding/History PointsActive cancer (treatment ongoing, administered within previous 6 months or palliative) +1
Paralysis or recent immobilization of the lower extremity +1
Recently bedridden for ≥ 3 days, or major surgery within previous 12 weeks +1
Localized tenderness along distribution of deep vein system +1
Swelling of entire leg +1Calf swelling ≥ 3 cm larger than that of the unaffected leg (measured 10 cm below the tibial tuberosity) +1
Pitting edema confined to affected leg +1Dilated superficial veins on affected leg (nonvaricose) +1Previously documented DVT +1Alternative diagnosis atleast as probable as DVT -2
Wells scoring

Wells Score DVT probability≤ 0 Low probability
1 - 2 Moderate probability
≥ 3 High probability
77

Diagnostic Studies
• Clinical examination alone is able to confirm only 20-30% cases of DVT.
• Blood Tests:–D-dimer test–Coagulation profile–Routine hematological investigate
• Imaging Studies• ECG and 2D echo
78

• D-Dimer:– The algorithm for diagnosing DVT includes
the D-dimer blood test– D-dimer is a degradation product of fibrin
cross-linking.– An elevated D-dimer level can occur when
blood clots are being formed. It can also be elevated in other conditions unrelated to DVT (ex. advanced age, cancer, pregnancy, recent surgery).
– The D-dimer test has high sensitivity and low specificity.
– The cutoff value for a normal D-dimer is ≤ 500 mcg/L
79

Imaging Studies
• Non Invasive ––Duplex Ultrasound–Plethysmography–MRI techniques
• Invasive ––Venography–Radiolabeled fibrinogen
80

• Imaging tests of the veins are used in the diagnosis of DVT, most commonly either proximal compression ultrasound or whole-leg ultrasound.
• Each technique has drawbacks: a single proximal scan may miss a distal DVT, while whole-leg scanning can lead to distal DVT overtreatment.
• CT scan venography, MRI venography, or MRI of the thrombus are also possibilities.
81

• The gold standard for judging imaging methods is contrast venography, which involves injecting a peripheral vein of the affected limb with a contrast agent and taking X-rays, to reveal whether the venous supply has been obstructed.
• Because of its cost, invasiveness, availability, and other limitations this test is rarely performed
82

83

84

85

Differntial Diagnosis of DVT
• Cellulitis• Thrombophebitis• Acute arthritis• Hematoma• Tumours• Venous or Arterial aneurysms• Connective tissue disorders
86

TreatmentAcute phase (usually around 5 days) - treatment with injectable, quick-acting anticoagulants (e.g. heparin, enoxaparin) until warfarin levels are therapeutic.Thrombolysis in indicated cases.
Intermediate phase (3 - 6 months) - treatment with warfarin (target INR of 2-3)
Extended phase (indefinite) - extended anticoagulation to prevent reoccurrence in appropriate patients
87

AIMS • Improve short- and long-term patient outcome. • The key to making sound treatment decisions
is recognizing that all venous thromboses are not the same.
88

• Some patients do well with anticoagulation alone (e.g., isolated calf vein thrombosis), whereas patient with extensive iliofemoral DVT often benefit from a strategy of thrombus removal followed by effective anticoagulation.
• The treatment strategies outlined are based on the level and extent of venous thrombosis, the known natural history of acute DVT, and the recognized benefits of therapy.
89

Anticoagulation
• The goal of immediate anticoagulation with heparin is to interrupt ongoing thrombosis while long-term oral anticoagulation with warfarin attempts to prevent recurrent DVT.
90

• Current guidelines–Favors low-molecular-weight heparin (LMWH) over unfractionated heparin (UFH) in the initial period –advise that heparin overlap Vit K Antagonists for a minimum of 5 days to ensure therapeutic anticoagulation.
91

Mechanism of action• Heparin:
–Binds to antithrombin via a specific 8-saccharide sequence and increases antithrombin activity over 1000-fold–Antithrombin inhibits activation of prothrombin and factor X.
92

•Vit k Antagonists:–Inhibits the γ-carboxylation of vitamin K-dependent procoagulants (factors II, VII, IX, and X) and anticoagulants (proteins C and S), resulting in formation of less functional proteins.
93

94

• Warfarin therapy is monitored by measuring the INR, calculated using the following equation:
• INR = (patient prothrombin time/laboratory control prothrombin time)ISI
ISI: International Sensitivity Index
95

Fondaparinux•It is a synthetic pentasaccharide that has been approved by the FDA for the initial treatment of DVT and PE.
•Its five-polysaccharide sequence binds and activates antithrombin, causing specific inhibition of factor Xa.
•The drug is administered SC once daily with a weight-based dosing protocol: 5 mg, 7.5 mg, or 10 mg for patients weighing <50 kg, 50 to 100 kg, or >100 kg, respectively.

Direct Thrombin Inhibitors(DTIs)• These antithrombotic agents bind to
thrombin, inhibiting the conversion of fibrinogen to fibrin as well as thrombin-induced platelet activation for example, hirudin, argatroban, and bivalirudin.
• These actions are independent of antithrombin. The DTIs should be reserved for
–patients in whom there is a high clinical suspicion or confirmation of Heparin induced thrombocytopenia (HIT)–patients who have a history of HIT or test positive for heparin-associated antibodies.
97

•In patients with established HIT, DTIs should be administered for at least 7 days, or until the platelet count normalizes. •Warfarin may then be introduced slowly, overlapping therapy with a DTI for at least 5 days.
98

Newer drugs• Direct inhibitors of factor Xa (rivaroxaban,
apixaban) are effective and safe in the management of patients with venous thromboembolic disease.
• Advantages:–They are rapidly absorbed–Require no monitoring–have fewer drug and food interactions than Vitamin K antagonists (VKAs)
–do not require parenteral heparin.
99

•The enhanced safety profile and ease of use associated with the new oral agents may ultimately shift the risk-benefit analysis in favor of prolonged anticoagulation to prevent DVT recurrence.
100

101

102

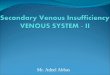
provoked vs unprovoked
Proximal vs distal
First episode vs second Bleeding risk
Extended anticoagulation recommended
provoked proximal and distal not specified any no
unprovoked
proximal
firstlow or moderate yes
high no
secondlow or moderate yes
high no
distal
first any no
secondlow or moderate yes
high no
Active cancer - ACCP recommends extended anticoagulation in all patients with active cancer
ACCP guidelines for extended coagulation
103

Calf Vein Thrombosis• They have the lowest thrombotic burden and
the best overall prognosis, they still carry a risk of thrombus extension or thromboembolic sequelae.
• Current guidelines recommend 3 months of anticoagulation for symptomatic calf DVT.
• For asymptomatic calf DVT, 2 weeks of serial ultrasound Doppler examinations should be performed and anticoagulation should be initiated if thrombus extension occurs.
104

Calf Vein Thrombosis cont..
• It is recommnded treating isolated calf DVT with anticoagulation and compression stockings unless the patient is at high risk for bleeding.
• Inpatients with a high bleeding risk, compression and ambulation with serial ultrasound surveillance is recommended.
105

106

Femoral Vein Thrombosis• Treated with anticoagulation alone due to
collateral venous drainage from the popliteal and profunda femoral veins to the common femoral vein.
• Often,functional valves exist above and below the vein segment involved with thrombus.
• Recanalization of the thrombus does not play a critical role as long as the popliteal and common femoral veins remain free of obstructive thrombus.
107

Popliteal Vein Thrombosis• Patients with occlusive femoropopliteal vein
thrombosis extending into the popliteal vein “trifurcation” frequently have severe acute symptoms.
• Occlusion of the axial venous drainage of the calf causes distal venous hypertension and significant post thrombotic morbidity.
• Patients with symptomatic femoropopliteal DVT are candidates for catheter-directed thrombolysis followed by compression and 3–6 months of anticoagulation. 108

Iliofemoral Thrombosis
• Iliofemoral DVT poses the threat of debilitating Post Thrombotic Syndrome(PTS) symptoms especially when patients are treated with anticoagulation alone.
• Anatomically, the common femoral, external iliac, and common iliac veins make up the single outflow venous channel for the entire lower extremity.
109

• Thrombotic obliteration of this lone outflow channel therefore results in the highest venous pressures and the most severe post-thrombotic morbidity
110

111

Systemic and Catheter Directed Thrombolysis
• Patients with extensive proximal, iliofemoral DVT may benefit from systemic thrombolysis or catheter-directed thrombolysis (CDT)
• CDT appears to be more effective and potentially reduces acute congestive lower extremity symptoms more rapidly than anticoagulation alone and decreases the development of PTS.
112

• Several thrombolytic agents are available, including streptokinase, urokinase, alteplase (recombinant tissue plasminogen activator), reteplase, and tenecteplase.
• All share the ability to convert plasminogen to plasmin, which leads to the degradation of fibrin.
• They differ with regard to their half-lives, their potential for inducing fibrinogenolysis (generalized lytic state), their potential for antigenicity, and their FDA-approved indications for use
113

• Streptokinase is purified from β-hemolytic Streptococcus.
• Approved for the treatment of acute myocardial infarction,PE, DVT, arterial thromboembolism, and occluded central lines and arteriovenous shunts.
• It is not specific for fibrin-bound plasminogen, however, and its use is limited by its significant rates of antigenicity.
• Fevers and shivering occur in 1% to 4% of patients.
114

• Urokinase is derived from human neonatal kidney cells grown in tissue culture. Currently, it is only approved for lysis of massive PE or PE associated with unstable hemodynamics.
• Alteplase, reteplase, and tenecteplase all are recombinant variants of tissue plasminogen activator(rtPA).
• Alteplase is indicated for the treatment of acute myocardial infarction, acute ischemic stroke, and acute massive PE.
• Often used for CDT of DVT. • Reteplase and tenecteplase are indicated
only for the treatment of acute myocardial infarction. 115

• Catheter-directed therapy: Venous access may be achieved through percutaneous catheterization of the ipsilateral popliteal vein, retrograde catheterization through the contralateral femoral vein, or retrograde cannulation from the internal jugular vein.
• Multi-side-hole infusion catheters, with or without infusion wires, are used to deliver the lytic agent directly into the thrombus.
• Lytic agents may be administered alone or, now more commonly, in combination with catheter-based methods to physically break up the clot—so-called pharmacomechanical thrombolysis.
116

117

• Surgical therapy is generally reserved for patients who worsen with anticoagulation therapy and those with phlegmasia cerulea dolens and impending venous gangrene.
• If the patient has phlegmasia cerulea dolens, a fasciotomy of the calf compartments is first performed.
• In iliofemoral DVT, a longitudinal venotomy is made in the common femoral vein and a venous balloon embolectomy catheter is passed through the thrombus into the IVC and pulled back several times until no further thrombus can be extracted.
Surgicial Thrombolectomy
118

• The distal thrombus in the leg is removed by manual pressure beginning in the foot.
• This is accomplished by application of a tight rubber elastic wrap beginning at the foot and extending to the thigh.
• If the thrombus in the femoral vein is old and cannot be extracted, the vein may be ligated.
119

• For a thrombus that extends into the IVC, the IVC is exposed transperitoneally and controlled below the renal veins.
• The IVC is opened and the thrombus is removed by gentle massage.
• An intraoperative completion venogram determines if any residual thrombus or stenosis is present. If a residual iliac vein.
• Ifstenosis is present, intraoperative angioplasty and stenting can be performed.
120

• In most cases, an arteriovenous fistula is then created by anastomosing the great saphenous vein (GSV) end to side with the superficial femoral artery in an effort to maintain patency of the thrombectomized iliofemoral venous segment.
• Heparin is administered postoperatively for several days. Warfarin anticoagulation is maintained for at least 6 months after thrombectomy.
• Complications of iliofemoral thrombectomy include PE in up to 20% of patients and death in <1% of patients.
121

IVC Filters
• They prevent pulmonary emboli, while allowing continuation of venous blood flow through the IVC.
• Early filters were placed surgically through the femoral vein.
• Currently, less invasive techniques allow percutaneous filter placement through femoral vein, internal jugular vein, or small peripheral vein under fluoroscopic or ultrasound guidance.
122

I
123

Complications
• ACUTE– Thrombosis – Bleeding at the insertion site – Misplacement of the filter
• CHRONIC– Thrombosis of the IVC, DVT, breaking, migration, or
erosion of the filter through the IVC.– The rate of fatal complications is <0.12%
124

125

DVT Prophylaxis• Patients who undergo major general surgical,
gynecologic, urologic, and neurosurgical procedures without thromboprophylaxis have a significant incidence of perioperative DVT.
• An estimated one third of the 150,000 to 200,000 VTE-related deaths per year in the United States occur following surgery.
• The goal of prophylaxis is to reduce the mortality and morbidity associated with VTE.
126

• Effective methods of VTE prophylaxis involve the use of one or more pharmacologic or mechanical modalities.
• Currently available pharmacologic agents include low-dose UFH, LMWH, synthetic pentasaccharides, and vitamin K Antagonists.
• Mechanical methods include intermittent pneumatic compression (IPC) and graduated compression stockings.
127

DVT complications
128

Conclusion
1. Prevention is better than cure.2. Stress on DVT prophylaxis in surgical patients
especially oncosurgery and elderly.3. Cancer screening in unprovoked DVT
especially young patients4. Thrombolysis for extensive DVT to avoid PTS.5. IVC filters should be reserved only for very
selective group.
129

References 1. Does this patient have deep vein thrombosis? Wells PS1,
Owen C et al. JAMA 2006 Jan 11;295(2):199-2072. Pulmonary embolism and deep vein thrombosis.
Goldhaber SZ1, Bounameaux H. Lancet 2012 May 12;379(9828):1835-46. doi: 10.1016/S0140-6736(11)61904-1.
3. Factors that predict thrombosis in relatives of patients with venous thromboembolism. Couturaud F1, Leroyer C2 et al Blood 2014 Sep 25;124(13):2124-30. doi: 10.1182/blood-2014-03-559757.
4. Risk of venous thromboembolism associated with peripherally inserted central catheters: a systematic review and meta-analysis. Chopra V1, Anand S et al. Lancet 2013 Jul 7;382(9889):311-25. doi: 10.1016/S0140-6736(13)60592-9.
130

5. Risk of venous and arterial thrombotic events in patients diagnosed with superficial vein thrombosis: a nationwide cohort study. Cannegieter SC1, Horváth-Puhó E et al. Blood 2015 Jan 8;125(2):229-35. doi: 10.1182/blood-2014-06-577783
6. Incidence and risk factors for venous thromboembolism after laparoscopic surgery for colorectal cancer. Cecilia Becattini,1 Fabio Rondelli et al. Haematologica 2015 Jan; 100(1): e35–e38.
7. Screening for Occult Cancer in Unprovoked Venous Thromboembolism. Carrier M1, Lazo-Langner A, Shivakumar S et al. N Engl J Med. 2015 Aug 20;373(8):697-704.
131

8. Deep vein thrombosis. Kyrle PA1, Eichinger S. Lancet 2005 Mar 26-Apr 1;365(9465):1163-74.
9.Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Jaff MR, McMurtry MS et al. Circulation. 2011 Apr 26;123(16):1788-830.
10.Elastic compression stockings—is there any benefit? Arina J ten Cate-Hoek. The lancet. Volume 383, No. 9920, p851–853, 8 March 2014
132

Thank you
133



















![Image Enhancement [DVT final project]](https://img.pdfslide.us/doc/110x75/568163bc550346895dd4d545/image-enhancement-dvt-final-project.jpg)