Embed Size (px)
Citation preview

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 1/30
Journal of Biosocial Sciencehttp://journals.cambridge.org/JBS
Additional services for Journal of Biosocial Science:
Email alerts: Click here
Subscriptions: Click hereCommercial reprints: Click hereTerms of use : Click here
‘MAYBE IT WAS HER FATE AND MAYBE SHE RAN OUT OF BLOOD’: FINALCAREGIVERS' PERSPECTIVES ON ACCESS TO CARE IN OBSTETRICEMERGENCIES IN RURAL INDONESIA
LUCIA D'AMBRUOSO, PETER BYASS and SITI NURUL QOMARIYAH
Journal of Biosocial Science / Volume 42 / Issue 02 / March 2010, pp 213 - 241
DOI: 10.1017/S0021932009990496, Published online: 17 December 2009
Link to this article: http://journals.cambridge.org/abstract_S0021932009990496
How to cite this article:LUCIA D'AMBRUOSO, PETER BYASS and SITI NURUL QOMARIYAH (2010). ‘MAYBE IT WASHER FATE AND MAYBE SHE RAN OUT OF BLOOD’: FINAL CAREGIVERS' PERSPECTIVES ON ACCESS TO CARE IN OBSTETRIC EMERGENCIES IN RURAL INDONESIA. Journal of Biosocial
Science, 42, pp 213-241 doi:10.1017/S0021932009990496
Request Permissions : Click here
Downloaded from http://journals.cambridge.org/JBS, IP address: 12.183.71.67 on 04 Dec 2015

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 2/30
‘ MAYB E I T WAS H E R F AT E AN D MAYB E SH E
RAN OUT OF BLOOD’: FINAL CAREGIVERS’PERSPECTIVES ON ACCESS TO CARE INOBSTETRIC EMERGENCIES IN RURAL
INDONESIA
LUCIA D’AMBRUOSO*, PETER BYASS*† SITI NURUL QOMARIYAH‡
*Immpact, Population Health Section, University of Aberdeen, UK, †Umeå Centre
for Global Health Research, Epidemiology and Public Health Sciences, UmeåUniversity, Sweden and ‡Immpact, Center for Family Welfare, Faculty of Public
Health, University of Indonesia, Indonesia
Summary. Maternal mortality persists in low-income settings despite prevent-
ability with skilled birth attendance and emergency obstetric care. Poor access
limits the eff ectiveness of life-saving interventions and is typical of maternal
health care in low-income settings. This paper examines access to care in
obstetric emergencies from the perspectives of service users, using established
and contemporary theoretical frameworks of access and a routine healthsurveillance method. The implications for health planning are also consid-
ered. The final caregivers of 104 women who died during pregnancy or
childbirth were interviewed in two rural districts in Indonesia using an
adapted verbal autopsy. Qualitative analysis revealed social and economic
barriers to access and barriers that arose from the health system itself. Health
insurance for the poor was highly problematic. For providers, incomplete
reimbursements, and low public pay, acted as disincentives to treat the poor.
For users, the schemes were poorly socialized and understood, complicated to
use and led to lower quality care. Services, staff , transport, equipment and
supplies were also generally unavailable or unaff ordable. The multiple
barriers to access conferred a cumulative disadvantage that culminated in
exclusion. This was reflected in expressions of powerlessness and fatalism
regarding the deaths. The analysis suggests that conceiving of access as a
structurally determined, complex and dynamic process, and as a reciprocally
maintained phenomenon of disadvantaged groups, may provide useful
explanatory concepts for health planning. Health planning from this perspec-
tive may help to avoid perpetuating exclusion on social and economic
grounds, by health systems and services, and help foster a sense of control at
the micro-level, among peoples’ feelings and behaviours regarding their
health. Verbal autopsy surveys provide an opportunity to routinely collect
J. Biosoc. Sci., (2010) 42, 213–241, Cambridge University Press, 2009doi:10.1017/S0021932009990496 First published online 17 Dec 2009
213

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 3/30
information on the exclusory mechanisms of health systems, important
information for equitable health planning.
Background
Maternal mortality in developing countries
Maternal ill health is a serious public health problem in developing countries.
Over 99% of the 536,000 maternal deaths estimated worldwide in 2005 occurred in
less-developed countries (WHO et al ., 2007). In addition, over 30 million women
suff er illnesses and long-term disabilities from the complications of pregnancy and
childbirth (Filippi et al ., 2006). Maternal mortality has also proved to be an
intractable problem; globally, there has been no detectable change in levels of
maternal mortality in almost three decades (WHO & UNICEF, 1996; WHO et al .,
2001, 2004a, 2007a).Epidemiological studies have revealed that during the intrapartum period, and the
days directly after, the risk of mortality is significantly elevated (Ronsmans &
Graham, 2006), and that the direct complications of pregnancy and childbirth (i.e.
haemorrhage, hypertensive disorders, sepsis, abortion and obstructed labour) are
responsible for the majority of deaths (Khan et al ., 2006). This information has
provided the evidence base for a core strategy of intrapartum care in health centres
(Campbell & Graham, 2006).
Key interventions are: (1) skilled birth attendance, delivery attended by an
accredited health professional who functions within an enabling environment of
transport, drugs and supplies; and (2) emergency obstetric care (EmOC), a packageof medical interventions required to treat the main direct complications of pregnancy
and childbirth (noted above). With sufficient coverage and utilization of these
interventions, it is estimated that over 90% of maternal mortality could be prevented
(Kilpatrick et al ., 2002; Bartlett et al ., 2005; Campbell & Graham, 2006).
Provision and uptake of care are problematic due to the ‘massive deprivation in
access’ characterized by the ‘sheer scarcity of staff and the excessive costs of care to
mothers’ (Filippi et al., 2006). In an emergency, when care may be required suddenly
and/or at difficult times (e.g. at night), ensuring access is particularly difficult. Access
is also typically constrained for vulnerable or marginalized groups (Weiss &
Greenlick, 1970). A vast array of studies have demonstrated barriers to, or
inequalities in, access related to social, cultural and economic disadvantage (Ensor &
Cooper, 2004; Cham et al ., 2005; Richard et al ., 2008b), rurality and lack of transport
(McCaw-Binns et al ., 2001; Davis-Floyd, 2003), and as arising from health policy
(Mavalankar & Rosenfield, 2005), systems and services (McCaw-Binns, 2005).
This article is concerned with describing and explaining access to health care in
obstetric emergencies. Access is examined from the perspectives of the final caregivers
of women who died during pregnancy or childbirth in two rural districts in Indonesia.
Established and contemporary theoretical frameworks of access and a routine health
surveillance method are used to consider the implications for health research and
planning.
214 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 4/30
The concept of access
One of the most influential theoretical models of access to health care is the
Andersen Behavioural Model (ABM) (Andersen & Newman, 1973; Aday & Andersen,
1974; Andersen, 1995). It consists of determining factors related to individuals and
systems that influence health behaviour and service utilization (with the latter used asa proxy for access). Explanatory variables include: ‘predisposing factors’, e.g. age, sex
and education; ‘enabling factors’, e.g. wealth, organization of services; and ‘need’, e.g.
symptoms. The ABM, arguably the dominant concept of access, is used widely in
policy and research (Gold, 1998; Eden, 1998; Ricketts & Goldsmith, 2005).
Other models have focused on the interaction between users and services.
Penchansky & Thomas (1981) have considered the ‘fit’ between patients’ needs and
services’ ability to meet those needs. The Institute of Medicine has also conceived of
access as an interaction between personal characteristics and structural features giving
rise to service utilization and health outcomes (Millman, 1993).
Dixon-Woods and colleagues (2006) recently developed a framework that con-
ceives of access as a dynamic, multi-dimensional, contingent process. They argue that
utilization, conceptualized and measured relative to affluent groups, overlooks the
issues of vulnerable groups, for whom access is typically constrained. They propose
‘candidacy’, or eligibility of care, as an alternative.
Candidacy encompasses a series of negotiations related to how individuals come
to use or receive care. These are: ‘identification of candidacy’ (how disadvantaged
people identify need in regard to specific events or crises), ‘navigation’ (an awareness
of services and mobilization of resources), ‘permeability of services’ (how easily people
can use services), ‘appearances’ (the ability of an individual to present credibly and
articulately), ‘adjudications’ (providers’ judgements or decisions that allow, or
disallow, access), ‘off ers and resistance’ (acknowledging that some refuse care that hasbeen off ered) and ‘operating conditions of the local production of candidacy’
(perceived and actual availability of health care determined by local conditions and
revealed through repeated encounters of individuals and providers) (Dixon-Woods
et al., 2006).
Models and frameworks have traditionally been used for measurement to select
categorized variables and objectively evaluate trends and relationships between
determinants of utilization to empirically demonstrate inequities in access. Over time,
however, conceptualizations of access have come to reflect context-specific inter-
actions between individuals and services. Finally, the concept of barriers to access
(defined as individual and systemic social and economic factors that lead to reducedaccess (McCullock-Melnyk, 1988)) is said to be deficient in that it is derived from the
viewpoints of professionals and fails to take into account the ‘lived experiences’ of
service users (McCullock-Melnyk, 1990; Sword, 1999).
‘Three delays’ framework
The ‘three delays’ framework is a classic pathways-based conceptualization of
access to good quality EmOC (and thus maternal mortality prevention) rooted in the
perspective of the service user (Thaddeus & Maine, 1994). Developed in the 1990s as
Perspectives on access to emergency obstetric care in Indonesia 215

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 5/30
part of the Prevention of Maternal Mortality programme at Columbia University, the
framework is concerned with timely treatment of obstetric complications to prevent
deaths and focuses on the interval between onset of a complication and receipt of
care.
This framework sets out that delays may occur in an obstetric emergency in one
or more of three ‘phases’: (a) in the decision to seek care (phase 1); (b) in the journeyto care, once a decision to seek care has been made (phase 2); and/or (c) in receiving
good quality care when a facility has been reached (phase 3).
Delays that occur in phase 1 are related to distance, cost and (perceived) quality
of services, women’s autonomy, economic status, education, illness and cultural
factors. Despite cultural beliefs aff ecting preferences for care, Thaddeus & Maine
(1994) acknowledge the interplay of structural and individual factors: ‘a narrow focus
on “cultural barriers” obscures the role that institutional inadequacies and economic
considerations play in the decision to seek care’. Phase 2 delays refer to obstacles in
reaching health facilities, including the distribution of facilities, travel distances and
transport. Delays occur in phase 3 due to shortages of staff and equipment, and poororganization and management.
The framework has been used extensively in studies of maternal mortality in
developing countries. Its applications include: quantifying the incidence of delays for
service planning in Haiti and Nigeria (Okonofua et al ., 1992; Barnes-Josiah et al .,
1998); community-based investigations of maternal mortality in Zimbabwe (Fawcus
et al ., 1996); multivariate analysis into the determinants of delay in Bangladesh
(Killewo et al ., 2006); verbal autopsy in Afghanistan (Bartlett et al ., 2005) and
Pakistan (Bartlett et al ., 2002); and clinical audit in Tanzania (Mbaruku et al., 2009).
It has also been used to design community-oriented strategies (Sibley & Armbruster,
1997), to examine the influence of women’s social positions on maternal mortality inNigeria (Wall, 1998) and to research health-seeking behaviours and perceptions of
quality in rural Haiti (White et al ., 2006), Malawi (Barber, 2003), Bolivia (Otis &
Brett, 2008) and Guatemala (Berry, 2008).
Rationale
Over a decade ago, a technical consultation marking ten years of the Safe
Motherhood Initiative set out improving access as a key action message (Starrs,
1997). Research and programmes implemented since then recognize the importance of
equitable access (ACCESS, 2009; Averting Maternal Death and Disability Program
(AMDD), 2009; Family Care International, 2009). Despite this, access to EmOC
remains poorly defined and difficult to ensure for poor and rural women in obstetric
emergencies. The rationale for this paper is to improve understandings of access to
EmOC and to inform research and policy to provide it.
Study setting
The study was conducted in January 2008 in the Serang and Pandeglang districts
of Banten province, Java, Indonesia. Indonesia has a population of over 220 million,
88% of which are Muslim (Badan Pusat Statistik-Statistics Indonesia (BPS) & ORC
216 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 6/30
Macro, 2003). Two-thirds of the population live in rural locations (BPS & ORC
Macro, 2003) and more than half on less than US$2 per day (World Bank, 2006).
With a population of over 123 million, Java, with Jakarta in the west, is the most
densely populated of all Indonesia’s 17,000 islands (BPS & ORC Macro, 2003).
The maternal mortality ratio for Indonesia is estimated between 307 (BPS & ORC
Macro, 2003) and 420 (WHO et al ., 2007) maternal deaths per 100,000 live births. Atsub-national level, ratios of 212 and 628 have been measured in urban Serang and
rural Pandeglang respectively (Ronsmans et al ., 2008) and extremely high levels of
2303 have been demonstrated among the poorest women in these districts (Ronsmans
et al ., 2009).
Home deliveries are common. Nationally, two in every three live deliveries occur
in the home (BPS & ORC Macro, 2003; Achadi et al ., 2007), over 80% in the study
districts (Ronsmans et al ., 2009). Uncertified Traditional Birth Attendants (TBAs or
dukun bayi ) attend two in every three deliveries for uneducated women and two of
every five in rural areas (BPS & ORC Macro, 2003).
Rural villages are served by the bidan di desa (village midwife) programme.Launched in 1989, it aims to post a qualified midwife in every rural village to live as
part of, and provide integrated maternal and child health (MCH) services to, the
community (Shankar et al ., 2008). Despite two decades of support, the coverage and
quality of services is compromised in remote and rural areas (Makowiecka et al .,
2008), with the poor obtaining unequal access to services (Ensor et al ., 2008),
particularly life-saving EmOC (Ronsmans et al ., 2001; Hatt et al ., 2007).
Indonesia has a decentralized governance system, of which villages (desa) are the
lowest level. Serang District has 373 desa, 80% of which are rural, and a population
of 1.7 million. There is one district referral hospital, two private hospitals, and 36
health centres ( puskesmas), ten with beds. Pandeglang is more remote with apopulation of 1.1 million and 335 desa, of which over 90% are rural. Pandeglang has
one public comprehensive EmOC facility and 30 puskesmas, five with beds (Izati et al .,
2005; Makowiecka et al., 2008). Villages are also served by posyandu, an integrated
health post used for primary preventative care. Unpaid volunteer health workers
(kader) provide basic care through posyandu. Five kader usually operate per posyandu.
Following the economic crisis in 1997, the government introduced health insurance
for the poor through a publically owned commercial insurance organization. Jaring
Pengaman Sosial (JPS), or social safety net schemes, use village authorities to identify
and exempt poor families from the costs of care. The schemes do not waive the costs
of incidentals, medication or transport (Sparrow, 2008). At the time of the study, an
insurance scheme called Asuransi Kesehatan untuk Keluarga Miskin (ASKESKIN), or
health insurance for the poor, was in operation.
Methods
Verbal autopsy
A routine health surveillance method called verbal autopsy was used. Verbal
autopsy is an established health surveillance technique used to generate cause-specific
mortality profiles in populations with significant numbers of deaths outside health
Perspectives on access to emergency obstetric care in Indonesia 217

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 7/30
facilities and/or poor routine certification (WHO, 2007). It is widely used in over 30
countries (Baiden et al ., 2007). In a verbal autopsy, final caregivers are interviewed on
the medical signs and symptoms of the deceased prior to death. The interview data
are then interpreted to establish a medical cause of death. Recently, verbal autopsy
has been used to collect additional information on non-medical causes, circumstances
and events surrounding deaths (WHO, 2004). In this study, verbal autopsy wasextended in this manner, to collect information on the interaction of women with
health services.
Identifying women and respondents
Women who had died during pregnancy, childbirth or within six weeks of
pregnancy ending, regardless of whether they had died in or been cared for in a
facility, were identified from a previous survey conducted in the study districts. The
previous study used village-based informants, volunteer health workers (kader) and
unpaid village officials (rukun tetangga), to collect information on maternal deathsthat had occurred between January 2004 and December 2005. This study identified
474 such deaths (Ronsmans et al ., 2009).
A total of 104 cases were purposively selected. The basis of the selection was
two-fold: first, it reflected the profile of causes from the original survey; and second,
based on geographical and resource feasibility, 104 cases represented a feasible
number of interviews to conduct. The cases were not selected randomly and the
selection did not seek to represent, nor make inferences for, the wider population.
District Health Office staff , consulted in the weeks prior to the survey, provided
valuable support in making contact with families of deceased women. Families were
approached for permission to conduct the interview through village leaders, commu-
nity health staff (including village midwives and kader) and others as possible and
necessary.
Ethical considerations
Informed consent was gained from all respondents. This included an explanation
of the study, a guarantee of anonymity and assurance that participation would not
have any bearing on the availability of health services to respondents or their families.
Participants were not obliged to answer questions, and could stop the interview at any
time and for any reason. Respondents were also given a gift at the end of the
interview as a gesture of goodwill and as compensation for time that may haveotherwise been spent generating income. The gift consisted of soap, shampoo, a
toothbrush and toothpaste.
Ethical approval for the study was granted from the Faculty of Public Health,
University of Indonesia and the College of Life Science and Medicine, University of
Aberdeen.
Interview
The interview contained two parts. Firstly, as in a traditional verbal autopsy, a
series of 75 checklist-style closed questions were used to collect information on
218 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 8/30
medical signs and symptoms, from which a medical cause of death was interpreted.
These were developed on the basis of standard verbal autopsy questions (WHO,
2007). Information was also collected on socioeconomic status through standard
questions on asset ownership.
In the second part, respondents were asked about the circumstances and events
surrounding the death in a semi-structured format with free dialogue. Respondentswere asked to recount the events between onset of the complication until death,
according to the ‘three delays’ framework (Thaddeus & Maine, 1994). At the end of
the interview, respondents were also asked their opinions on the preventability and
cause of death.
Descriptions of the general conduct of health professionals were invited, but
questions were not asked about their clinical actions due to the likelihood that
respondents were not in a position to be either exposed to or critique them in
anything more than general terms. As a result, technical aspects of care, particularly
those in facilities, cannot be examined in an equivalent manner.
Interviewers
Four public health graduates with general medical backgrounds (one nursing,
two midwifery and one public health), and who were also familiar with the local
context, were recruited and trained. In order not to impose a diagnostic line of
enquiry (implicit or explicit) onto the interview, doctors were purposely not recruited.
Although the majority of the work was conducted in Bahasa Indonesian, the
abilities of the interviewers to communicate in the indigenous languages of the
districts, Javanese and Sundanese, and in English, was also useful in maximizing
communication between interviewers, respondents and researchers.Three days of training were provided that adopted a role-playing format. Actions
and situations such as audio-recording, gaining informed consent and potentially
difficult or unwilling respondents were rehearsed to prepare the interviewers to
respond to the informants and their ability to describe the cases. The researchers
SNQ, PB and LD conducted the training and observed or participated in the
interviews. The interviews were conducted in Bahasa Indonesian, with some exchanges
in Sundanese and Javanese, and typically lasted 60–90 minutes. They were
audio-recorded for transcription and translation, with observations noted on paper.
Data analysis
Descriptive statistics were prepared on the characteristics of women and respond-
ents, and probable causes of death were interpreted from the data collected in the first
part of the interview (see Fottrell et al . (2007) for a description of the interpretation
method). The narratives gained in the second part of the interview were regarded as
representations of women’s lived experiences of health care and constituted the main
subject of the analysis.
The audio recordings were transcribed and translated into English and qualitative
analysis was performed. A combined inductive/deductive, iterative approach was
adopted whereby the ‘three delays’ framework and respondents’ opinions regarding
Perspectives on access to emergency obstetric care in Indonesia 219

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 9/30
the preventability and cause of death provided an initial coding frame (‘mega-
themes’). Through a detailed examination of the transcripts, further recurring
descriptive themes and sub-themes that emerged were used to supplement the initial
coding frame. Explanations of access to care were constructed by considering patterns
and relationships across the themes.
The researcher LD systematically searched and manually coded the data forrecurring themes until thematic saturation was reached (the point at which no new
categories, factors or explanations emerged). The results of the analysis are presented
with supporting verbatim quotes from the interviews. Where quotes are provided, the
relationship of the respondent to the deceased, the anonymized case reference number
and probable cause of death are also indicated.
Results and Discussion
Characteristics of the women and respondents
Over three-quarters of the women were aged 20–39 years at death; virtually all
were married and almost half were employed. The majority were literate, with
primary education. Husbands earned income mainly through labouring, informal
work and transport. Half of the women had 1–3 previous live deliveries, a quarter had
none and a quarter more than seven (Table 1). Just under half the women died at
home, a similar proportion in a facility and six died en route. The respondents were
mainly close relatives of the woman (parent, parent-in-law, spouse, sibling or child)
and most had lived in the same household. Respondents had an average age of 47 and
the majority were literate (data not shown).
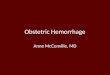
Causes and delays
The leading medical cause of death was sepsis, accounting for one-third of the
deaths. Haemorrhage and malaria together accounted for one-fifth and small
proportions were due to pregnancy-induced hypertension, unsafe abortion and
obstructed labour. Indirect causes (including conditions such as tuberculosis, human
immunodeficiency virus (HIV), diabetes and cardiovascular disease) accounted for
over a third of deaths (Table 2). Delays in the decision to seek care were reported by
nearly half the respondents. Delays in reaching care were reported by two-thirds, and
in receiving care in almost half of the cases (Table 3). These results are discussed in
greater depth elsewhere (D’Ambruoso et al ., 2009; Byass et al ., 2009).A thematic account of experiences of EmOC and perspectives on causation
and preventability is provided below. The thematic framework is presented in
Table 4.
The decision to seek care (Phase 1)
Poor birth preparedness/emergency readiness. Most women sought traditional
therapies, including stomach massages and herbal medicines, from TBAs (dukun)
during pregnancy. Women also generally sought antenatal care on more than one
220 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 10/30
occasion with a village-based midwife. A common belief, recounted by respondents as
being perpetuated by both women and providers, was that if a pregnancy was
established as ‘normal’ by a midwife during antenatal care, then the delivery would
be presumed to be uncomplicated. Midwives were thought to be unnecessary for
‘normal’ deliveries and were only called when a complication arose.
Interviewer: Did the midwife recommend having the delivery with the midwife or at hospital?
Father: No, she was healthy. (Case 543215, Haemorrhage)
As a result, women generally planned to deliver with dukun, with little provision
for going to hospital in the event of a complication. If families failed to prepare
transport, finances and blood donors etc., then delays were incurred when unexpected
complications arose because the decision to seek care, and associated negotiations and
arrangements, still had to be made.
Interviewer: Did you call the midwife?
Sister: No . . . we did not call [the midwife].
Interviewer: And then who told you to bring her to hospital?Sister: Relatives, we discussed it.
Interview: You discussed it. It happened at 8 pm, and she was brought at . . .?
Sister: In the morning.
Interviewer: The event was at night, why did you bring her in the next morning? She had fainted;
she should be brought to hospital that night.
Sister: I do not know, maybe because we were shocked, and then . . . because we were far from
the main road, nobody had the chance to go there to seek the car.
Interviewer: During the night of the event until the next morning, what happened to [name]? Did
she faint or continue bleeding? What happened maam?
Sister: Yes . . . she had bleeding all night long.
Interviewer: From night until morning?
Sister: Yes. (Case 448106, Ectopic pregnancy)
Unmet need for community-based care in obstetric emergencies. Despite being
‘first-line’ delivery attendants, TBAs are not trained or equipped to manage
complications (Bailey et al ., 2002). When unexpected complications occurred,
traditional medicine was often administered before a midwife was called.
Interviewer: Did he [traditional healer] give some kind of water or something?
Mother-in-law: He gave water, but he didn’t say anything.
Interviewer: Did he ask to take her to hospital for instance?
Mother-in-law: Nope.
Interviewer: What did he do at that time?
Mother-in-law: He did nothing.Respondent 2: Only [cast] the spells . . . (Case 267305, Pregnancy-related sepsis)
When a midwife was called, further delays were usually introduced because of the
general shortage of health staff in villages.
Husband: The dukun pulled the placenta but it did not work. It was raining heavily, so when they
called the midwife it took longer for her to arrive. Because the rain was heavy, she could not be
saved by the time the midwife arrived. (Case 518105, Diabetes)
Respondent 2: There used to be a posyandu [integrated health post for rural areas], but only in
name . . . there was no function of it . . . Kind of, inactive.
Interviewer: How about the midwife around here?
Perspectives on access to emergency obstetric care in Indonesia 221

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 11/30
Respondent 1: There was no midwife. (Case 305302, Pregnancy-related sepsis)
Mother-in-law: When the midwife came she had already passed away. (Case 267305, Pregnancy-
related sepsis)
The poor availability of midwives can be attributed to their low public pay, which
necessitates their developing private practice. More than two-thirds of midwives’
salaries come from private practice and over 90% generate income this way (Ensor
et al ., 2008). As a result, midwives tend to prefer clients who can pay for services
immediately and they are discouraged from establishing practices in rural areas where
it is harder to make a private income.
Interviewer: What did midwife [name] say, why was the deceased brought to her house? Why
didn’t she help her to deliver at home?
Husband: She said that she had a lot of patients, she was busy. (Case 292101, Kidney disease)
Table 1. Characteristics of the 104 women who died
Characteristic n (%a)
Age <20 6 (6)
20–29 45 (43)30–39 34 (33)
40–49 19 (18)
R50 0 (0)
Education None 5 (5)
Primary 67 (64)
High school 31 (30)
Other 1 (1)
Literate 97 (93)
Worked for income 45 (43)
Married 103 (99)
Husband’s occupation Labourer/informal sector 67 (64)
Transport 20 (19)
Farmer 10 (10)
Government/formal sector 4 (4)
Unemployed 1 (1)
Not applicable (not married) 1 (1)
Gravidity 1–3 54 (52)
4–6 26 (25)
R7 24 (23)
Parity 0 17 (16)
1–3 48 (46)
4–6 23 (22)
R7 16 (15)Place of death Home 50 (48)
Facility (hospital/health centre) 48 (46)
En route 6 (6)
aTotals may be >100% due to rounding.
222 L. D’Ambruoso, P. Byass and S. N. Qomariyah
8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 12/30
In the cases where the midwife attended the woman in her household, and in time,
the situation had to be clinically assessed before a referral could be made. In several
cases, the midwife was also ill-equipped and/or had to convince the family of the need
for referral, introducing further delays.
Table 2. Mortality profile of the 104 women who died
Cause of death na (%b)
Abortion-related death 2 (2)
Anaemia 5 (5)Cancer 3 (3)
Cardiovascular disease 6 (6)
Diabetes 6 (6)
Ectopic pregnancy 4 (4)
Haemorrhage 13 (13)
HIV/AIDS-related death 2 (2)
Kidney disease 4 (4)
Liver disease 4 (4)
Malaria 8 (8)
Obstructed labour 2 (2)
Other maternal cause 4 (4)
Pregnancy-induced hypertension 4 (4)
Pregnancy-related sepsis 29 (28)
Ruptured uterus 1 (1)
Suicide 1 (0)
Tuberculosis (pulmonary) 5 (5)
Indeterminable 1 (1)
Total 104 (100)
aUp to three cause-of-death conclusions are generated by the Inter-
VAM model. These were weighted according to their likelihoods. For
example, if a case was concluded to be due to both haemorrhage (50%
likelihood) and sepsis (50% likelihood), then this case would count as0.5 of a case of haemorrhage and 0.5 of a case of sepsis.bTotals may be >100% due to rounding.
Table 3. Phases in which delays were reported
Phasea %b
Decision-making for care-seeking (Phase 1) 45
Reaching care (Phase 2) 66
Quality facility-based care (Phase 3) 44aAccording to the ‘three delays’ framework (Thaddeus & Maine,
1994).bAs a proportion of surviving women.
Perspectives on access to emergency obstetric care in Indonesia 223
8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 13/30
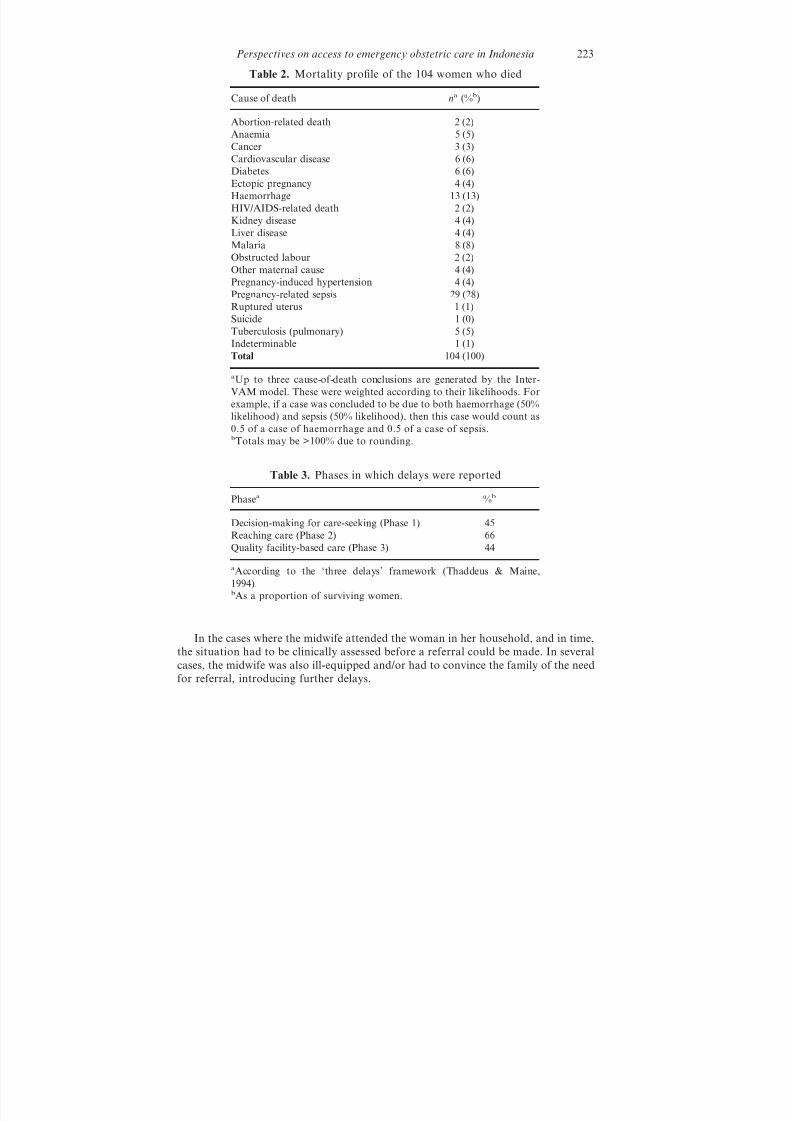
Fear of the hospital . Decisions to seek care were strongly influenced by concerns
over the costs of care. A dominant view was that delivery care would incur high costs,
Table 4. Thematic framework
Mega-themes Themes Sub-themes
The decision to seek
care (Phase 1)
Poor birth preparedness/
emergency readiness
Traditional therapies during pregnancy
Antenatal care visits with midwivesDelivery planned with midwife
Delivery planned with TBA
Pregnancy ‘normal’, uncomplicated delivery
assumed, and delivery planned with TBA
Poor preparation for complications
Unmet need for
community-based care in
obstetric emergencies
TBA-assisted complicated delivery
Traditional emergency therapies
Delays before calling midwife
Delays before midwife attended
Poor availability of midwife in emergency
Low acceptability of midwife in emergency
High cost of midwife in emergency
Midwife attended delivery after called by
TBA/family/both
Midwife assessment of complication
Poor quality of care from midwife in
emergency
Time taken before referral
Seeking care late
Death in the home
Fear of the hospital Fears/panic over costs of care
Time taken before making a decision
Death at homeReaching care
(Phase 2)
Difficulties arranging
health insurance for the
poor
No health insurance granted in
advance/previously
Arrangement of health insurance in
emergency
Complicated/time-consuming
health-insurance-arrangement process
Stigma of health insurance
Late and/or poor quality
referral
Women critical at referral
Poor quality referral
Lack of drugs, supplies
Midwife did not accompanyUnavailable, unaff ordable
and/or unsafe transport
Costs of transport
Availability of transport
Time taken to arrange transport
Modes of transport
Inappropriate/unsafe mode of transport
Death en route
224 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 14/30
of which respondents were fearful. In many cases, by the time a decision was made
to accept the costs and seek care, the women’s condition had become life-threatening.
Other relative: . . . she was not hospitalized . . . because of her fear of hospital. You have to
understand our perception about being hospitalized, even if we get serious illnesses; we take care
of it ourselves.
Interviewer: Oh . . . I see . . . fear of what?
Other relative: Here, there is no social safety net – we don’t have the money. (Case 305302,Pregnancy-related sepsis)
Reaching care (Phase 2)
Di fficulties arranging health insurance for the poor. A further dominant theme was
the failure of the health insurance scheme for the poor to mediate these fears and
enable access when a decision to seek care had been made. In the majority of cases,
families had not been identified and issued with the green JPS health insurance card
and had to arrange insurance in the emergency. In these cases, a Surat Keterangan
Tidak Mampu (SKTM) letter, or poverty certificate, had to be issued from village
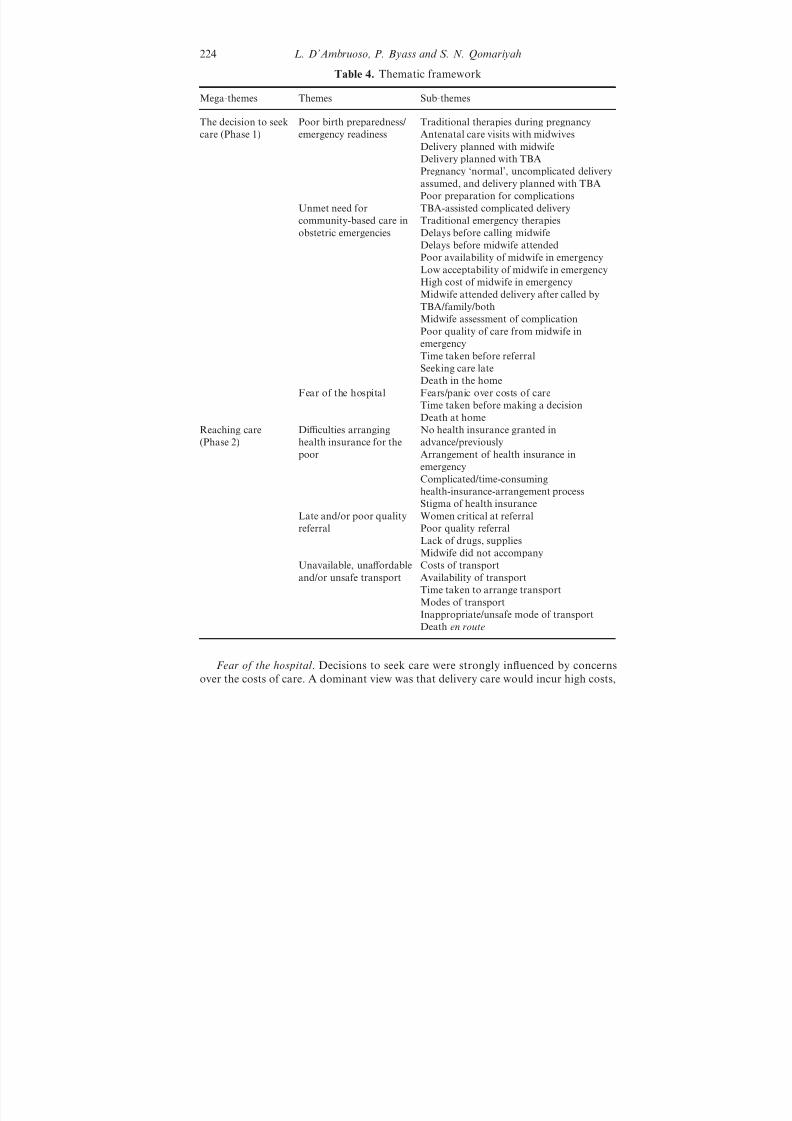
Table 4. Continued
Mega-themes Themes Sub-themes
Receiving good
quality EmOC in
hospitals (Phase 3)
Admissions of women
with health insurance
No health insurance/partially arranged
health insurance
Complicated admission
Time-consuming admission
Discrimination on basis of health insurance
use
Stigma of health
insurance
Discrimination on basis of health insurance
use
No communication to family on conditions
or treatments
No death certificate/information on cause of
death
No ‘right’ to ask questions if poor
Poor quality facility-basedcare
Lack of staff and/or equipmentAdditional cost considerations
Additional journeys for drugs, blood, care
Death in hospital
Second referrals Poorly staff ed and equipped facilities
Unavailable or poorly equipped ambulances
Death en route
Prevention and
cause
Fatalism and passivity Death was unavoidable
Sufficient eff ort/everything possible was
done: nyreat
Fate, destiny, God’s will
Dual recognition of fate and healthsystems/health care
Perspectives on access to emergency obstetric care in Indonesia 225
8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 15/30
authorities. The SKTM letter is an interim statement of eligibility for health insurance
in lieu of a JPS/ASKESKIN card. The SKTM has to be used within a short time
span, and covers a brief episode of care. In many cases, arranging the letter
introduced or exacerbated delays. Respondents described bureaucratic processes
whereby numerous forms of paperwork (cards, letters and certificates) required issue,
authorization and/or signature from various village officials and health workers.
Sister: The family discussed and planned to take her to hospital ‘X’, but because they didn’t have
money, they needed to manage the statement letter for poor people first [SKTM letter]. The time
to process the letter was so long, a day wasn’t enough, finally she didn’t have the chance to go
to the hospital, she died immediately. (Case 128101, Tuberculosis (pulmonary))
Mother: We had to arrange the administration [health insurance] first because we are poor. We
had to go to the bidan [midwife] first, then to the head of sub-district and to the head of the
village to arrange the [SKTM] letter, so it took a long time. We should not have to arrange the
administration [health insurance] first because it can be arranged later . . . I wanted her to be cared
for immediately. (Case 131103, Pregnancy-related sepsis)
In many cases, health insurance was only partially arranged before the women’scondition necessitated presenting at a facility. Even when successfully arranged and
used, families still had to meet the costs of drugs, transport and other incidentals.
Late and poor quality referral . By the time they were referred, many women were
in critical health states. Referral was also often of poor quality; the narratives
indicated that, when they did attend, many health staff did not follow standard
referral procedures on accompaniment, essential drugs, supplies, vehicles, referral
letters, communication and monitoring. Inadequate birth preparedness/emergency
readiness on the part of women and families coupled with inadequate community-
based services had negative synergistic eff ects resulting in women not being attendedor referred in time in the emergency situations.
Daughter: She died when there was no-one . . . When she died she cried for help like someone who
was strangled. (Case 635106, Pregnancy-induced hypertension)
Unavailable, una ff ordable and unsafe transport. When referral journeys were
embarked upon, the cost of transport (usually public) was often problematic. At
difficult times such as late at night, it was also usually unavailable. Even during the
day and in good weather, transport could take hours to arrange. Modes of transport
used in emergencies included: angkot, a public minibus, unlikely to be aseptic or
equipped; and ojek, a rented motorcycle, highly inappropriate and dangerous.Father: Her body was yellow, she was pale and weak with stomach ache and vomited
continuously . . . I was bringing her to the hospital but [after] three junctions I had to go back
because I couldn’t stand for her to be transported by motorcycle. (Case 487101, Anaemia)
Receiving good quality EmOC in hospitals (Phase 3)
Admissions of women with health insurance. The difficulties of using health insurance
extended into facilities. The bureaucratic, complicated and time-consuming admis-
sions of poor women with health insurance, partially arranged health insurance, or no
health insurance and no ability to pay for care, were recurrent themes. Some
226 L. D’Ambruoso, P. Byass and S. N. Qomariyah
8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 16/30
respondents felt that delays in receiving care arose because of using health insurance
and would not have occurred otherwise.
Husband: [The admission] was quite difficult at first; they made it difficult . . . because the letters
from ASKESKIN [health insurance for the poor] were not complete. And then I was told to
arrange it. (Case 635107, Pregnancy-related sepsis)
The stigma of health insurance. The stigma of health insurance and its negative
eff ect on quality of care were repeatedly recounted. In several cases, respondents
indicated that the quality of care received in hospitals was lower than it may have
been otherwise by virtue of the women’s low economic status, revealed by their use
of health insurance.
Mother: . . . the hospital staff don’t really take care, she was not really cured, the doctor
sometimes checked, but most of the time they don’t really care for poor people, especially if we
use the ASKESKIN [health insurance for the poor] card. (Case 540208, Abortion-related death)
Some respondents did not feel that there was a problem with bad quality care
because they were poor. Others felt discriminated against.
Sister-in-law: At the hospital, sometimes poor people are neglected, especially when there is no
referral from the bidan [midwife], they just ignored us . . . Just don’t treat us diff erently. Even if
we are poor people and use ASKESKIN, they neglect or ignore us. We are lacking in ways to
go to the bidan or doctor. (Case 281102, Cancer)
There were repeated accounts of how hospital staff failed to explain procedures or
conditions to family members, unless there was a direct implication for action (e.g.
buying blood or medication). Over 80% of families were not informed of the cause
of death or given death certificates. Many respondents expressed the opinion that they
did not have authority to ask questions about their health care because they were
poor.
Mother: . . . if you are poor, you can’t ask this or that. If you have money you can. (Case 547303,
Tuberculosis (pulmonary))
This context or culture of care is linked to how care is financed. Research on
public funding for delivery care has shown that professionals are not fully reimbursed
for care they provide through the ASKESKIN scheme (Ensor et al ., 2008). In
addition to low public pay, incomplete reimbursements from ASKESKIN serve as a
further disincentive to provide emergency care to poor women.
Poor quality facility-based care. Many respondents described facilities that were not
adequately staff ed or equipped, often lacking in crucial supplies, such as bloodproducts. As a result, many families had to embark on additional journeys, and pay
associated transport costs, to locate and purchase medicines and/or blood. This
presented particular difficulties for poor families who had to balance the likelihood
that their relative would survive with the cost implications of their death.
Interviewer: What about the cost?
Sister: Yes, it was difficult to find money to pay for the cost.
Interviewer: Was it expensive?
Sister: It was expensive. Where should we get the money from, from whom should we borrow
money? [We] should have to sell land for that [costs of care]. (Case 401101, Pregnancy-related
sepsis).
Perspectives on access to emergency obstetric care in Indonesia 227

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 17/30
In several cases, by the time the necessary resources to obtain medications or
blood products had been mobilized, the woman was too weak to have them
administered, or had passed away.
Other relative: We brought her on Saturday at 6 o’clock in the morning. Then on Sunday, the
blood was supposed to be transfused to her body. But we could not get it. We got it at 7 o’clock
at night. So it was kind of late to do a blood transfusion. We were looking for the blood in the
city. We couldn’t get it there. (Case 295105, Pregnancy-related sepsis)
Husband: [We] bought the blood for 750,000 rupiahs (~80US$), 3 bags . . . only one and a half
bags were used . . . then she died. (Case 302108 Haemorrhage)
Second referrals. Despite the physical presence of health facilities, shortages in
personnel, equipment and supplies often led to a second referral. Second referrals may
also have been made due to reluctance to treat poor patients (see D’Ambruoso
et al . (2008) for a detailed example). Ambulances provided for second referrals
were frequently un-staff ed and ill-equipped. Several women died en route between
hospitals.Mother: I do not know for sure whether the hospital was full or not. If you have the money, you
will immediately get the services. She did not have money. We had money, but now it is gone.
(Case 401101, Pregnancy-related sepsis)
Mother: The doctor said, ‘there’s no option, there’s no equipment here.’ She went by ambulance.
No health staff accompanied on the journey. (Case 300119, Malaria)
Opinions on preventability and cause. In more than half the cases, respondents felt
that the deaths could not have been avoided and attributed them to destiny, fate or
God’s will, particularly when they felt that everything possible had been done. The
extent of ‘everything possible’ varied, but generally referred to the eff orts, albeitunsuccessful, of various individuals (the woman, family, TBAs, health workers, village
leaders etc.). Sufficient eff ort to avoid death from disease or other conditions, by
traditional or medical means, beyond which it was permissible to attribute the death
to destiny, had a specific name: nyreat. When opinions of nyreat were explored, some
respondents did acknowledge the contribution of unavailable or ineff ective health
systems, services and/or personnel. However, there was often an equivalent and
ambiguous sense of submitting to or accepting destiny, fate or God’s will.
Brother-in-law: Maybe it was her fate . . . and maybe she ran out of blood. (Case 478102,
Haemorrhage)
Interviewer: After she was cut [episiotomy] by midwife [Y], she bled. According to you, was thata problem?
Husband: No . . . no problem. I let go of that, I am not disappointed. If I did not remember fate,
I would consider it a problem. It is just that, I remember fate. (Case 292101, Haemorrhage)
Sister: If you think that [the death was avoidable] it is difficult, heart breaking. Let’s think the
way I have been thinking. It’s her destiny, from the Almighty, I prefer it that way. (Case 548305,
Cancer)
The expressions of destiny and fate may represent coping mechanisms to mediate
grief, sorrow and/or culpability. They may also simply be a common turn of phrase.
Contextualizing this theme, however, provides an additional explanation. In West
228 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 18/30
Java, an elaborate and nuanced order of courtesy and politeness, related to social
standing, exists. As observed by Iskandar and colleagues (1996) ‘When a woman dies
it is God’s will, when she survives, it is the doctor’s skill’. The passivity and fatalism
over the deaths may therefore reflect feelings of powerlessness to question the medical
staff and systems associated with authority. In addition, the multiple barriers
described above conferred a cumulative disadvantage that culminated in exclusionfrom access. It is likely that the passivity and fatalism may have also reflected feelings
of powerlessness in the face of such marked exclusion.
Social exclusion
Theoretical frameworks of exclusion set out that participation in social systems
(including health care) is dictated by social and moral values that are expressed
through repeated interactions of individuals with systems (Gilson, 2003; Freedman,
2005; Popay et al ., 2008). As set out earlier, access to health care can be described
as a highly dynamic, relational process between personal characteristics and structuralfeatures. If access and exclusion are sufficiently similar, and if exclusion is a
phenomenon of the marginalized, then it follows that access might also usefully be
considered as a phenomenon of disadvantaged groups.
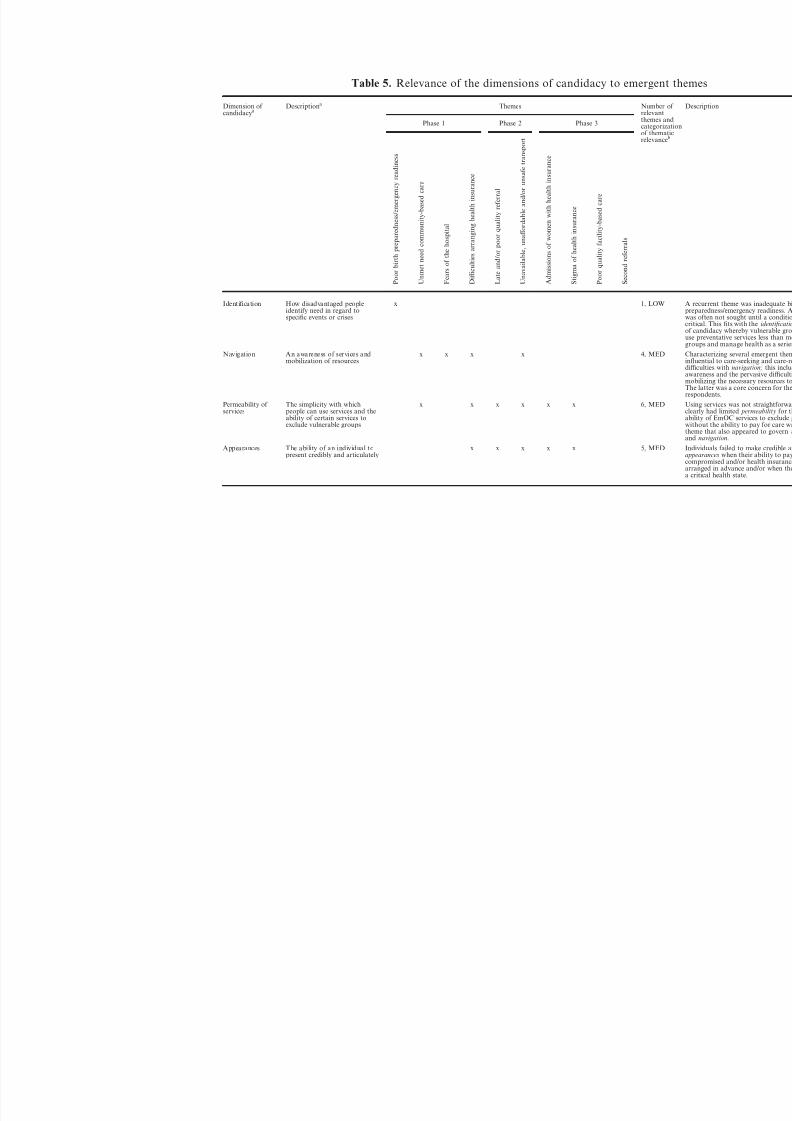
This supports the Dixon-Woods framework of access (2006). To examine its
relevance in more depth, the core element of candidacy was examined in terms of the
emergent themes (Table 5). This revealed a hierarchical arrangement of the relevance
of the dimensions of candidacy. For example, an awareness of available care and an
ability to mobilize resources (navigation) governed how people identified need and
whether care was ‘refused’ (identification, o ff ers and resistance), not the reverse.
Similarly, the ease with which people use services ( permeability) determined how theymust mobilize resources (navigation). The judgements of providers regarding people’s
eligibility for care (adjudications) governed whether people presented for care
convincingly (appearances). And the local conditions of systems and services
(operating conditions) determined the ease with which they were used and providers’
judgements allowed or disallowed access ( permeability and adjudications).
From this, it can be inferred that the organization of health systems dictates
service provision, provider and user behaviours; i.e. the locus of control over
candidacy, or eligibility for access to EmOC, lies within the macro-level operating
conditions. A reciprocal eff ect can also be seen whereby the behaviours and attitudes
of service users (expressed in terms of powerlessness and passivity) feed back into the
operating conditions, maintaining the social and cultural norms that shape the health
system, and exclusion from access (Fig. 1).
Social and cultural norms
These relationships are typical of the structuralist perspective, which sets out that
deep social structures are produced and maintained in human actions and interactions
(Riessman, 1974, 1984; Rappaport, 1995). Rural Indonesian society is governed by a
decentralized, yet staunchly hierarchical and bureaucratic system without a great deal
of eff ective social welfare or protection and with widespread abuse of power and
Perspectives on access to emergency obstetric care in Indonesia 229
8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 19/30
Table 5. Relevance of the dimensions of candidacy to emergent t
Dimension of candidacya
Descriptiona Themes Number ofrelevantthemes andcategorizatiof thematicrelevanceb
Phase 1 Phase 2 Phase 3
P o o
r b i r t h p r e p a r e d n e s s / e m e r g e n c y r e a d i n e s s
U n m
e t n e e d c o m m u n i t y - b a s e d c a r e
F e a r s o f t h e h o s p i t a l
D i ffi
c u l t i e s a r r a n g i n g h e a l t h i n s u r a n c e
L a t e a n d / o r p o o r q u a l i t y r e f e r r a l
U n a
v a i l a b l e , u n a ff o r d a b l e a n d / o r u n s a f e t r a n s p o r t
A d m
i s s i o n s o f w o m e n w i t h h e a l t h i n s u r a n c e
S t i g
m a o f h e a l t h i n s u r a n c e
P o o
r q u a l i t y f a c i l i t y - b a s e d c a r e
S e c o n d r e f e r r a l s
Identification How disadvantaged peopleidentify need in regard tospecific events or crises
x 1, LOW
Navigation An awareness of services andmobilization of resources
x x x x 4, MED
Permeability of
services
The simplicity with which
people can use services and theability of certain services toexclude vulnerable groups
x x x x x x 6, MED
Appearances The ability of an individual topresent credibly and articulately
x x x x x 5, MED
8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 20/30
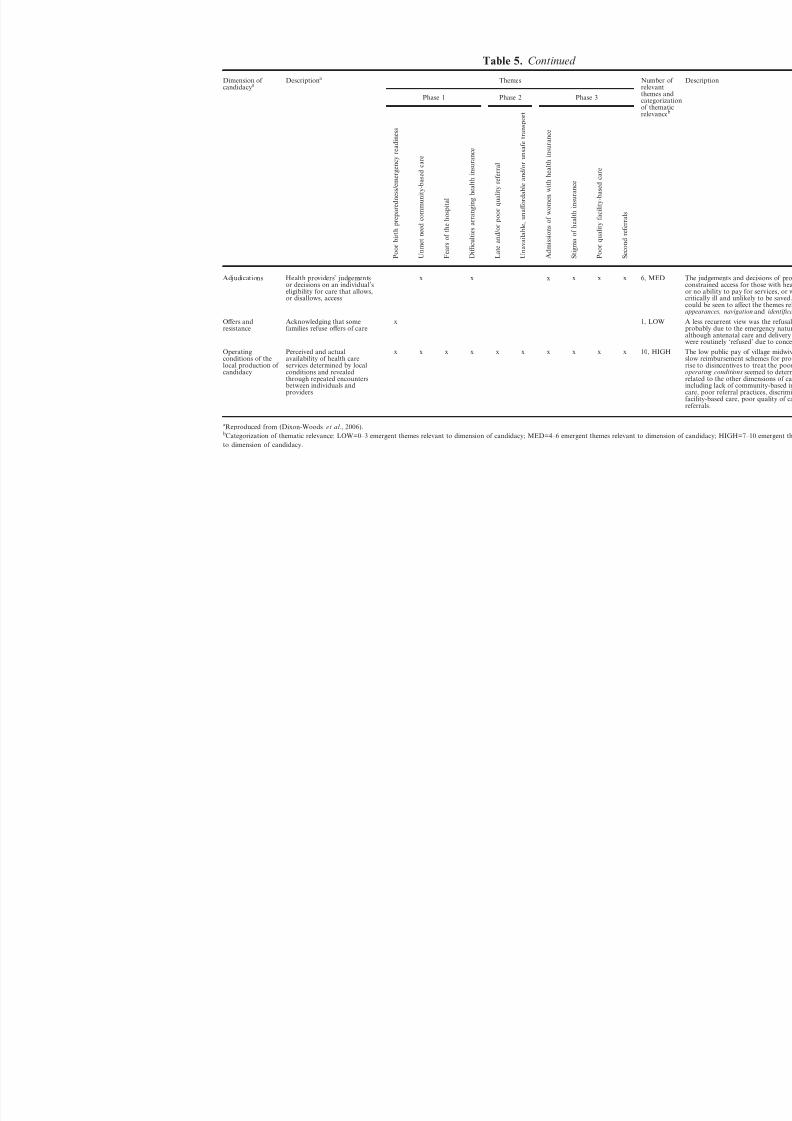
Table 5. Continued
Dimension of candidacya
Descriptiona Themes Number ofrelevantthemes andcategorizatiof thematicrelevanceb
Phase 1 Phase 2 Phase 3
P o o r b i r t h p r e p a r e d n e s s / e m e r g e n c y r e a d i n e s s
U n m e t n e e d c o m m u n i t y - b a s e d c a r e
F e a r s o f t h e h o s p i t a l
D i ffi c u l t i e s a r r a n g i n g h e a l t h i n s u r a n c e
L a t e a n d / o r p o o r q u a l i t y r e f e r r a l
U n a v a i l a b l e , u n a ff o r d a b l e a n d / o r u n s a f e t r a n s p o r t
A d m i s s i o n s o f w o m e n w i t h h e a l t h i n s u r a n
c e
S t i g m a o f h e a l t h i n s u r a n c e
P o o r q u a l i t y f a c i l i t y - b a s e d c a r e
S e c o n d r e f e r r a l s
Adjudications Health providers’ judgementsor decisions on an individual’seligibility for care that allows,or disallows, access
x x x x x x 6, MED
Off ers andresistance
Acknowledging that somefamilies refuse off ers of care
x 1, LOW
Operatingconditions of thelocal production of candidacy
Perceived and actualavailability of health careservices determined by localconditions and revealedthrough repeated encountersbetween individuals andproviders
x x x x x x x x x x 10, HIGH
aReproduced from (Dixon-Woods et al ., 2006).bCategorization of thematic relevance: LOW=0–3 emergent themes relevant to dimension of candidacy; MED=4–6 emergent themes relevant to dimension
to dimension of candidacy.

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 21/30
corruption (Friend, 2003; Utomo, 2005). Village governance systems have been
described as chaotic – ‘at the village level, most representatives (officials) scarcely
understand their roles’ (Bebbington et al ., 2006) – and village-level health care hasbeen characterized as being ‘without transparency and accountability’ and ‘increas-
ingly privatized’ (Kristiansen & Santoso, 2006). Society is also conservative and
restrictive towards women, and by extension, their reproductive health needs (Beegle
et al ., 2001). Norms of discrimination, elitism and a market ideology were clearly
reflected in the accounts of interactions and negotiations that took place when women
attempted to access EmOC.
Implications for health planning
A focus on the macro-level organization and the culture and context of care is
central to the structuralist reform agenda. Key approaches are well known. These
include increasing the roles of lower cadre providers to encompass responsibilities
traditionally within the realm of higher cadres, usually physicians (Riessman, 1984).
In the rural villages on Java, bidan, kader and other health staff represent viable entry
points for such reform. Increased investment, training and support with concomitant
improvements in local-level health infrastructure such as posyandu could maximize
their documented potential (Berman et al ., 1987; Leimena, 1989; Kristiansen &
Santoso, 2006).
Health insurance for the poor is highly problematic. For providers, incomplete
reimbursements, and low public pay, act as disincentives to treat the poor. For users,
Fig. 1. Elements of eligibility for access to health care (candidacy) arranged according
to thematic relevance reveals a structuralist and reciprocal hierarchy.
232 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 22/30
the schemes are poorly socialized and understood, highly bureaucratic and compli-
cated, and they lead to lower quality and discriminatory care. Informing and issuing
families with health insurance could also be achieved via kader and posyandu as part
of birth preparedness/emergency readiness during the antenatal period.
When they have not been arranged in advance, poverty certificates (SKTM letters)
need to be more quickly and easily attainable in emergencies. The SKTM letters couldbe placed within the authority and management of kader, to reduce bureaucracy and
dependence on busy village officials, puskesmas heads etc. The health insurance system
should also ensure rapid and full reimbursements to midwives in villages and hospitals
to encourage their services to be made available to the poor. Finally, health staff
should also receive training to improve their acceptance of women with health
insurance in obstetric emergencies.
More progressive structuralist health policies challenge the biomedical model of
health and health care by increasing mutual participation in care, reducing the
passivity of the patient, sharing medical knowledge, increasing kinship and so on,
allowing health and illness to be thought of as ‘inextricably linked to broader socialarrangements’ (Reissman, 1984). Health planning from a more holistic perspective has
the potential to develop robust solutions to complex problems. It could also help
foster a sense of control at the micro-level, influencing people’s feelings and
behaviours regarding their health, lives and futures, and conferring a sense of
self-worth and control that appear to be lacking in this setting.
Finally, the multitude of delays often resulted in admission of women to hospitals
in a critical or moribund condition. As well as being avoidable, this may negatively
distort clinical audits of quality of care that often do not take account of factors that
occur outside a facility (Adisasmita et al ., 2008).
Methodological reflections
By virtue of its focus on deaths outside hospitals, verbal autopsy provides an
opportunity to collect information on the very individuals excluded from (and by)
health care systems. Extending verbal autopsy to capture information on the
dynamics of access maximizes the potential of a widely used, routine and action-
oriented health planning method. Benefits and limitations of the approach are
described below.
Interviewers and interviews
The verbal autopsy interview is typically a brief, one-off discussion, without
feedback, conducted by a medical practitioner who may represent the structures of
‘medical authority’, so interpersonal power dynamics may be reproduced. The
interview also deals with a sensitive topic. On a number of occasions observed by the
authors and recounted by the interviewers, the interviewee struggled with or stopped
the interview due to its upsetting nature. In most of these cases, the respondent
decided to continue and complete the interview; only a small number did not wish to
carry on (in these cases, the gift was still given). As a result, careful recruitment and
training, continuous support for interviewers, appropriate conduct and carefully
Perspectives on access to emergency obstetric care in Indonesia 233

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 23/30
worded informed consent for respondents are critical to gain meaningful accounts of
the cases. Sufficient time is also required. The extended verbal autopsy interview was
20–30 minutes longer than a standard verbal autopsy, an increase that may be
significant in larger surveys.
Respondents
Although verbal autopsy collects subjective accounts of care, by virtue of the
emergency situation, an atypical chain of events occurs that is likely to be recalled in
detail – that is, ‘narrative reconstructions’ of ‘actual practices’ are likely to be
obtained rather than ‘normative statements’ (Lambert & McKevitt, 2002). In
addition, in the interviews in this study, several people (family members, friends and
neighbours) in addition to the primary respondent were present at various points
during the interview and information was often provided by more than one
respondent. This was not challenged by the interviewers; they did not insist on a
privately conducted one-to-one interview and attempted to gain consent from, and
record descriptive information for, all who gave significant or substantial information.
This approach allowed for cross-verification of information and ‘gap-filling’, which
was useful if the respondent(s) had not been with the woman continuously from the
onset of the complication until she died. Drawbacks were that confidentiality may
have been compromised and attributing all the information provided to the primary
respondent may have been inaccurate. The convention of verbal autopsy interviews
being privately conducted, confidential interviews may not always be necessary nor
appropriate. An interview under these conditions should be off ered to respondents,
rather than enforced.
Analysis
Verbal autopsy aims to detect the magnitude of medical disorders and identify,
associate and quantify risk factors at aggregate level. Qualitative enquiry off ers an
alternative, complementary, analytical perspective, to describe and explain why such
trends occur. Despite being time- and resource-intensive, the narrative approach is
particularly appropriate to examine issues of access. Individual explanations of
health-seeking behaviours ‘perform social functions rather than being neutral reflec-
tions’ (de Kok & Widdicombe, 2008) and allow for an examination of social contexts
on people’s behaviours, and vice versa.
It is also important to consider for whom the results of verbal autopsy are useful.
National and international organizations use standardized verbal autopsy data tomonitor disease burdens between populations and over time (Byass, 2007). Tradi-
tional verbal autopsy also considers cause of death in narrow biomedical terms of
disease classification and organ failure. Broadening the cause of death concept to
consider the impact of failures of health and social systems may provide more
complete information, relevant for local-level planning.
Implications for future research
Verbal autopsy can be used as a means, or an element, of clinical audit to examine
the social and structural constraints on access to quality care. Allied methods include
234 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 24/30
near-miss audit (Filippi et al ., 2004, 2009; Béhague et al ., 2007), community- and
facility-based maternal death reviews (Manandahar et al ., 2004; Richard et al ., 2008a)
and confidential enquiries (Pattinson & Hall, 2003; South Africa Every Death Counts
Writing Group, 2008). When conducted appropriately, these methods have the
potential to generate critical evaluations of access to (and quality of) health care using
the insights of service users and providers operating in the local contexts.Other more conventional qualitative approaches exist to describe and explain
phenomena such as access. Their visibility, and hence utility, for local-level health
planning is, however, limited. The analyses of the data collected, presented here and
elsewhere (D’Ambruoso et al ., 2009; Byass et al ., 2009), demonstrate that qualitative
enquiry can be combined with the wide application of verbal autopsy for a robust and
routine interpretation of the social and structural dimensions of health, as well as to
quantify the incidence of complications that are unpredictable and swift to kill in the
absence of good quality care.
Conclusion
The narratives reveal a multitude of social and economic barriers to access that
women encountered during obstetric emergencies in this setting. The manner in which
the barriers arose demonstrated the structural construction of access to health care for
disadvantaged groups, and that, in this setting, a diff erent standard of care seems to
be reserved for, and accepted by, the poor.
Although EmOC and skilled birth attendance require that women have access to
professional delivery care, access itself remains poorly understood. Conceiving of
access as dynamic and relational, and as a phenomenon of disadvantaged groups,
may provide a useful point of departure for re-positioning health planning and basicdistributive commitments that are appropriate for the social and economic, and
emergency, contexts in which these services are provided.
Incorporating qualitative data collection and analysis into traditional biomedical
and epidemiological approaches to health surveillance is a route to gaining cross-
disciplinary insights into complex problems. This approach has the potential to
inform more robust, eff ective and culturally relevant strategies to address the
cumulative disadvantage and restricted access to essential, life-saving care for
pregnant women in low-income settings.
Acknowledgments
This work was undertaken as part of the Initiative for Maternal Mortality
Programme Assessment (Immpact), funded by the Bill & Melinda Gates Foundation,
the UK Department for International Development, the European Commission and
US Agency for International Development (USAID). Immpact is an international
research programme which also provides technical assistance through its affiliate
organization, Ipact. The funders have no responsibility for the information provided
or views expressed in this paper. The views expressed herein are solely those of the
authors. The authors would also like to acknowledge the contributions of: Dr Linda
Barlett, for sharing the verbal autopsy interview schedule applied in a study in
Perspectives on access to emergency obstetric care in Indonesia 235

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 25/30
Afghanistan in 2002 (UNICEF and Centres for Disease Control, CDC, Atlanta),
upon which the interview guide in this study was based; Dr Endang Acahdi and her
team at the Centre for Family Welfare, University of Indonesia, including Kamalud-
din Latief for co-ordinating the fieldwork and to Trisari Anggondowati and Eko
Pambudi; the interviewers Lupthi Tri Utari, Sri Rahmi, Kray S. Asa and Agus
Khomeini; and the District Health Offices in Serang and Pandeglang for the valuablesupport in making contact with the families of the deceased women. The authors are
grateful to the respondents in Banten province who gave up their time to participate
in the interviews. Finally, acknowledgements go to Dr Alice Kiger, Ms Suzanne Cross
and Mr Alec Cumming at the University of Aberdeen, Dr Linda Bartlett at Johns
Hopkins School of Public Health and Dr Susan Murray at Kings College London
who gave useful comments on earlier versions of the manuscript.
References
ACCESS (2009) ACCESS Program: Access to Clinical and Community Maternal, Neonatal and
Women’s Health Services. US Agency for International Development, Baltimore (available at:
http://www.accesstohealth.org/program/overview.htm).
Achadi, E., Scott, S., Pambudi, E. S., Makowiecka, K., Marshall, T., Adisasmita, A., Deviany,
P. E. & Ronsmans, C. (2007) Midwifery provision and uptake of maternity care in Indonesia.
Tropical Medicine & International Health 12, 1490–1497.
Aday, L. A. & Andersen, R. (1974) A framework for the study of access to medical care. Health
Services Research 9, 208–220.
Adisasmita, A., Deviany, P. E., Nandiaty, F., Stanton, C. & Ronsmans, C. (2008) Obstetric near
miss and deaths in public and private hospitals in Indonesia. BMC Pregnancy and Childbirth
8, 10 (available at: http://www.biomedcentral.com/1471-2393/8/10/abstract).Andersen, R. & Newman, J. F. (1973) Societal and individual determinants of medical care
utilization in the United States. The Milbank Memorial Fund Quarterly Health and Society
51, 95–124.
Andersen, R. M. (1995) Revisiting the behavioural model and access to medical care: does it
matter? Journal of Health and Social Behavior 36, 1–10.
Averting Maternal Death and Disability Program (AMDD) (2009) Averting Maternal Death and
Disability Program. Columbia University, New York (available at: http://www.amddprogram.
org/).
Badan Pusat Statistik-Statistics Indonesia (BPS) & ORC Marco (2003) Indonesia Demographic
and Health Survey 2002–2003. Calverton, MD (available at: http://www.measuredhs.com/
pubs/pub_details.cfm?ID=439&ctry_id=17&SrchTp=psummary#dfiles)Baiden, F., Bawah, A., Biai, S., Binka, F., Boerma, T., Byass, P. et al. (2007) Setting
international standards for verbal autopsy. Bulletin of the World Health Organization 85, 570.
Bailey, P. E., Szaszdi, J. A. & Glover, L. (2002) Obstetric complications: does training
traditional birth attendants make a diff erence? Pan American Journal of Public Health 11,
15–23.
Barber, G. (2003) ‘To tell or not to tell’: ethics and secrecy in anthropology and childbearing
in rural Malawi. In Caplan, P. (ed.) The Ethics of Anthropology: Debates and Dilemmas.
Routledge, London and New York, pp. 133–154.
Barnes-Josiah, D., Myntti, C. & Augustin, A. (1998) The “three delays” as a framework for
examining maternal mortality in Haiti. Social Science & Medicine 46, 981–993.
236 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 26/30
Bartlett, L. A., Jamieson, D. J., Kahn, T., Sultana, M., Wilson, H. G. & Duerr, A. (2002)
Maternal mortality among Afghan refugees in Pakistan, 1999–2000. Lancet 359, 643–649.
Bartlett, L. A., Mawji, S., Whitehead, S., Crouse, C., Dalil, S., Ionete, D. & Salama, P. (2005)
Where giving birth is a forecast of death: maternal mortality in four districts of Afghanistan,
1999–2002. Lancet 365, 864–870.
Bebbington, A., Dharmawan, L., Fahmi, E. & Guggenheim, S. (2006) Local capacity, villagegovernance, and the political economy of rural development in Indonesia. World Develop-
ment 34, 1958–1976.
Beegle, K., Frankenberg, E. & Thomas, D. (2001) Bargaining power within couples and use of
prenatal and delivery care in Indonesia. Studies in Family Planning 32, 130–146.
Béhague, D. P., Kanhonou, L. G., Filippi, V., Lègonou, S. & Ronsmans, C. (2008) Pierre
Bourdieu and transformative agency: a study of how patients in Benin negotiate blame and
accountability in the context of severe obstetric events. Sociology of Health and Illness 30,
489–510.
Berman, P. A., Gwatkin, D. R. & Burger, S. E. (1987) Community-based health workers: head
start or false start towards health for all? Social Science & Medicine 25, 443–459.
Berry, N. S. (2008) Who’s judging the quality of care? Indigenous Maya and the problem of “not being attended”. Medical Anthropology: Cross-Cultural Studies in Health and Illness 27,
164–189.
Byass, P. (2007) Who needs cause-of-death data? PloS Medicine 4, e333 (available at:
http://www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.0040333).
Byass, P., D’Ambruoso, L., Ouédraogo, M. & Qomariyah, S. N. (2009) Assessing the repeat-
ability of verbal autopsy for determining cause of death in Burkina Faso and Indonesia.
Population Health Metrics 7, 6 (available at: http://www.pophealthmetrics.com/content/7/1/6).
Campbell, O. M. & Graham, W. J. (2006) Strategies for reducing maternal mortality: getting
on with what works. Lancet 368, 1284–1299.
Cham, M., Sundby, J. & Vangen, S. (2005) Maternal mortality in the rural Gambia, a
qualitative study on access to emergency obstetric care. Reproductive Health 2, 3 (available
at: http://www.reproductive-health-journal.com/content/2/1/3).
D’Ambruoso, L., Byass, P. & Qomariyah, S. N. (2008) Can the right to health inform public
health planning in developing counties? A case study for maternal healthcare from Indonesia.
Global Health Action 1 (available at: http://journals.sfu.ca/coaction/index.php/gha/article/
view/1828).
D’Ambruoso, L., Byass, P., Qomariyah, S. N. & Ouedraogo, M. (2009) A lost cause?
Investigating social and medical causes of maternal death with verbal autopsy: a method and
implications for health planning. Paper presented at: Loss in Childbearing in Sub-Saharan
Africa and South Asia Workshop, Department of Social and Political Studies, University of
Edinburgh, Edinburgh.
Davis-Floyd, R. (2003) Home-birth emergencies in the US and Mexico: the trouble with
transport. Social Science & Medicine 56, 1911–1931.De Kok, B. C. & Widdicombe, S. (2008) ‘I really tried’: Management of normative issues in
accounts of responses to infertility. Social Science & Medicine 67, 1083–1093.
Dixon-Woods, M., Cavers, D., Agarwal, S., Annandale, E., Arthur, A., Harvey, J. et al. (2006)
Conducting a critical interpretive synthesis of the literature on access to healthcare by
vulnerable groups. BMC Medical Research Methodology 6, 35 (available at: http://
www.biomedcentral.com/1471-2288/6/35).
Eden, J. (1998) Measuring access to care through population-based surveys: where are we now?
Health Services Research 33, 685–708.
Ensor, T. & Cooper, S. (2004) Overcoming barriers to health service access: influencing the
demand side. Health Policy and Planning 19, 69–79.
Perspectives on access to emergency obstetric care in Indonesia 237

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 27/30
Ensor, T., Nadjib, M., Quayyum, Z. & Megraini, A. (2008) Public funding for community-based
skilled delivery care in Indonesia: to what extent are the poor benefiting? European Journal
of Health Economics. DOI: 10.1007/s10198-007-0094-x.
Family Care International (FCI) (2009) The Skilled Care Initiative. Family Care International,
New York (available at: http://familycareintl.org/en/issues/35).
Fawcus, S., Mbizvo, M., Lindmark, G. & Nystrom, L. (1996) A community-based investigation of avoidable factors for maternal mortality in Zimbabwe. Studies in Family Planning 27, 319–327.
Filippi, V., Brugha, R., Browne, E., Gohou, V., Bacci, A., de Brouwere, V. et al. (2004) Obstetric
audit in resource-poor settings: lessons from a multi-country project auditing ‘near miss’
obstetrical emergencies. Health Policy and Planning 19, 57–66.
Filippi, V., Richard, F., Lange, I. & Ouattara, F. (2009) Identifying barriers from home to the
appropriate hospital through near-miss audits in developing countries. Best Practice &
Research: Clinical Obstetrics & Gynaecology 23, 389–400.
Filippi, V., Ronsmans, C., Campbell, O. M., Graham, W. J., Mills, A., Borghi, J. et al. (2006)
Maternal health in poor countries: the broader context and a call for action. Lancet 368,
1535–1541.
Fottrrel, E., Byass, P., Ouedraogo, T. W., Tamini, C., Gbangou, A., Sombie, I. et al.
(2007)Revealing the burden of maternal mortality: a probabilistic model for determining
pregnancy-related causes of death from verbal autopsies. Population Health Metrics 5
(available at: http://www.pophealthmetrics.com/content/5/1/1).
Freedman, L. (2005) Achieving the MDGs: health systems as core social institutions.
Development 48, 19–24.
Friend, T. (2003) Indonesia Destinies. Harvard University Press, United States.
Gilson, L. (2003) Trust and the development of health care as a social institution. Social Science
& Medicine 56, 1453–1468.
Gold, M. (1998) Beyond coverage and supply: measuring access to healthcare in today’s market.
Health Services Research 33, 625–652.
Hatt, L., Stanton, C., Makowiecka, K., Adisasmita, A., Achadi, E. & Ronsmans, C. (2007) Did
the strategy of skilled attendance at birth reach the poor in Indonesia? Bulletin of the World
Health Organization 85, 774–782 (available at http://www.who.int/bulletin/volumes/85/10/
06.033472/en/index.html).
Iskandar, M. B., Utomo, B., Hull, T., Dharmaputra, N. G. & Anwar, Y. (1996) Unravelling the
Mysteries of Maternal Death in West Java: Re-examining the Witnesses. University of
Indonesia, Jakarta.
Izati, Y., Pambudi, E. & D’Ambruoso, L. (2005) A Descriptive Analysis of Dho and Bps Data
on Coverage and Profile of Midwifery Services in Serang and Pandeglang Districts . University
of Indonesia, Jakarta.
Khan, K. S., Wojdyla, D., Say, L., Gulmezoglu, A. M. & Van Look, P. F. (2006) WHO analysis
of causes of maternal death: a systematic review. Lancet 367, 1066–1074.
Kilpatrick, S. J., Crabtree, K. E., Kemp, A. & Geller, S. (2002) Preventability of maternaldeaths: comparison between Zambian and American referral hospitals. Obstetrics &
Gynecology 100, 321–326.
Killewo, J., Anwar, I., Bashir, I., Yunus, M. & Chakraborty, J. (2006) Perceived delay in
healthcare-seeking for episodes of serious illness and its implications for safe motherhood
interventions in rural Bangladesh. Journal of Health Population and Nutrition 24, 403–412
(available at: http://www.icddrb.org:8080/images/jhpn24_4_Perceived-Delay.pdf).
Kristiansen, S. & Santoso, P. (2006) Surviving decentralisation? Impacts of regional autonomy
on health service provision in Indonesia. Health Policy 77, 247–259.
Lambert, H. & McKevitt, C. (2002) Anthropology in health research: from qualitative methods
to multidisciplinarity. British Medical Journal 325, 210–213.
238 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 28/30
Leimena, S. L. (1989) Posyandu: a community based vehicle to improve child survival and
development. Asia Pacific Journal of Public Health 3, 264–267.
McCaw-Binns, A. (2005) Safe motherhood in Jamaica: from slavery to self-determination.
Paediatric and Perinatal Epidemiology 19, 254–261.
McCaw-Binns, A., Standard-Goldson, A., Ashley, D., Walker, G. & MacGillivray, I. (2001)
Access to care and maternal mortality in Jamaican hospitals: 1993–1995. International Journal of Epidemiology 30, 796–801.
McCullock-Melnyk, K. A. (1988) Barriers: a critical review of recent literature. Nursing
Research 37, 196–201.
McCullock-Melnyk, K. A. (1990) Barriers to care: operationalizing the variable. Nursing
Research 39, 108–112.
Makowiecka, K., Achadi, E., Izati, Y. & Ronsmans, C. (2008) Midwifery provision in
two districts in Indonesia: how well are rural areas served? Health Policy and Planning 23,
67–75.
Manandhar, D. S., Osrin, D., Shrestha, B. P., Mesko, N., Morrison, J., Tumbahangphe, K. M.
et al. (2004) Eff ect of a participatory intervention with women’s groups on birth outcomes
in Nepal: cluster-randomised controlled trial. Lancet
364, 970–979.Mavalankar, D. V. & Rosenfield, A. (2005) Maternal mortality in resource-poor settings: policy
barriers to care. American Journal of Public Health 95, 200–203.
Mbaruku, G., van Roosmalen, J., Kimondo, I., Bilango, F. & Bergström, S. (2009) Perinatal
audit using the 3-delays model in western Tanzania. International Journal of Gynecology &
Obstetrics 106, 85–88.
Millman, M. (ed.) (1993) Access to Health Care in America. Institute of Medicine (IOM),
Washington DC.
Okonofua, F. E., Abejide, A. & Makanjuola, R. A. (1992) Maternal mortality in Ile-Ife, Nigeria:
a study of risk factors. Studies in Family Planning 23, 319–324.
Otis, K. E. & Brett, J. A. (2008) Barriers to hospital births: why do many Bolivian women give
birth at home? Revista Panamericana de Salud Pública 24, 46–53.
Pattinson, R. C. & Hall, M. (2003) Near misses: a useful adjunct to maternal death enquiries.
British Medical Bulletin 67, 231–243.
Penchansky, R. & Thomas, J. W. (1981) The concept of access: definition and relationship to
consumer satisfaction. Medical Care 19, 127–140.
Popay, J., Escorel, S. H. M. , Johnston, H., Mathieson, J., Rispel, L. & On behalf of the WHO
Social Exclusion Knowledge Network (2008) Understanding and Tackling Social Exclusion:
Final Report to the WHO Commission on Social Determinants of Health From the Social
Exclusion Knowledge Network . World Health Organization, Geneva (available at:
http://www.who.int/entity/social_determinants/knowledge_networks/final_reports/sekn_final%
20report_042008.pdf).
Rappaport, J. (1995) Empowerment meets narrative: listening to stories and creating settings.
American Journal of Community Psychology 23, 795–807.Richard, F., Ouédraogo, C., Zongo, V., Ouattara, F., Zongo, S., Gruénais, M. E. et al. (2008a)
The difficulty of questioning clinical practice: experience of facility-based case reviews in
Ouagadougou, Burkina Faso. British Journal of Obstetrics and Gynaecology 116, 38–44.
Richard, F., Witter, S. & De Brouwere, V. (2008b) Reducing financial barriers to obstetric care
in low-income countries. Studies in Health Service Organisation and Policy 24.
Ricketts, T. C. & Goldsmith, L. J. (2005) Access in health services research: the battle of the
frameworks. Nursing Outlook 53, 274–280.
Riessman, C. K. (1974) The use of health services by the poor. Social Policy 5, 41–49.
Riessman, C. K. (1984) The use of health services by the poor: are there any promising models?
Social Policy 14, 30–40.
Perspectives on access to emergency obstetric care in Indonesia 239

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 29/30
Ronsmans, C., Endang, A., Gunawan, S., Zazri, A., McDermott, J., Koblinsky, M. & Marshall,
T. (2001) Evaluation of a comprehensive home-based midwifery programme in South
Kalimantan, Indonesia. Tropical Medicine and International Health 6, 799–810.
Ronsmans, C. & Graham, W. J. (2006) Maternal mortality: who, when, where, and why. Lancet
368, 1189–1200.
Ronsmans, C., Scott, S., Adisasmita, A., Deviany, P. & Nandiaty, F. (2008) Estimation of population-based incidence of pregnancy-related illness and mortality (PRIAM) in two
districts in West Java, Indonesia. British Journal of Obstetrics and Gynaecology 116, 82–90.
Ronsmans, C., Scott, S., Qomariyah, S. N., Achadi, E., Braunholtz, D., Marshall, T. et al. (2009)
Professional assistance during birth and maternal mortality in two Indonesian districts.
Bulletin of the World Health Organization 87, 416–423.
Shankar, A., Sebayang, S., Guarenti, L., Utomo, B., Islam, M., Fauveau, V. & Jalal, F. (2008)
The village-based midwife programme in Indonesia. Lancet 371, 1226–1229.
Sibley, L. & Armbruster, D. (1997) Obstetric first aid in the community – partners in safe
motherhood a strategy for reducing maternal mortality. Journal of Nurse-Midwifery 42,
117–121.
South Africa Every Death Counts Writing Group. (2008) Every death counts: use of mortalityaudit data for decision making to save the lives of mothers, babies, and children in South
Africa. Lancet 371, 1294–1304.
Sparrow, R. (2008) Targeting the poor in times of crisis: the Indonesian health card. Health
Policy and Planning 23, 188–199.
Starrs, A. (1997) The Safe Motherhood Action Agenda: Priorities for the Next Decade . Family
Care International, New York (available at: http://www.familycareintl.org/en/resources/
publications/51).
Sword, W. (1999) A socio-ecological approach to understanding barriers to prenatal care for
women of low income. Journal of Advanced Nursing 29, 1170–1177.
Thaddeus, S. & Maine, D. (1994) Too far to walk: maternal mortality in context. Social Science
& Medicine 38, 1091–1110.Utomo, B. (2005) Challenges in addressing safe motherhood issues in Indonesia. In United
Nations Economic and Social Commission for Asia and the Pacific: Health and Mortality in
the Asian and Pacific Region. Asian Population Studies Series, vol. 163, pp. 109–125
(available at: http://www.unescap.org/esid/psis/population/popseries/apss163/apss163.pdf
#page=116).
Wall, L. L. (1998) Dead mothers and injured wives: the social context of maternal morbidity
and mortality among the Hausa of northern Nigeria. Studies in Family Planning 29, 341–359.
Weiss, J. E. & Greenlick, M. R. (1970) Determinants of medical care utilization: the eff ect of
social class and distance on contacts with the medical care system. Medical Care 8, 456–462.
White, K., Small, M., Frederic, R., Joseph, G., Bateau, R. & Kershaw, T. (2006) Health seeking
behaviour among pregnant women in rural Haiti. Health Care for Women International 27,
822–838.
World Bank (2006) Making the New Indonesia Work for the Poor. World Bank, Jakarta/
Washington (available at: http://siteresources.worldbank.org/INTINDONESIA/Resources/
Publication/280016-1152870963030/2753486-1165385030085/Overview_standalone_en.pdf,).
World Health Organization (2004) Beyond the Numbers: Reviewing Maternal Deaths and
Complications to make Pregnancy Safer. WHO, Geneva. (available at http://www.who.int/
making_pregnancy_safer/documents/9241591838/en/index.html).
World Health Organization (2007) Verbal Autopsy Standards: Ascertaining and Attributing
Causes of Death. WHO, Geneva (available at: http://www.who.int/whosis/mort/
verbalautopsystandards/en/).
240 L. D’Ambruoso, P. Byass and S. N. Qomariyah

8/18/2019 Final Caregiver Perspective Obstetric Emergency Care Indonesia
http://slidepdf.com/reader/full/final-caregiver-perspective-obstetric-emergency-care-indonesia 30/30
World Health Organization & UNICEF (1996) Revised 1990 Estimates of Maternal Mortality:
A New Approach by WHO and UNICEF . WHO/FRH/MSM/96.11, Geneva (available at:
http://whqlibdoc.who.int/hq/1996/WHO_FRH_MSM_96.11.pdf,).
World Health Organization, UNICEF & UNFPA (2001) Maternal Mortality in 1995: Estimates
Developed by WHO, UNICEF, UNFPA. WHO/RHR/01.9, Geneva (available at: http://
www.who.int/reproductive-health/publications/rhr_01_9_maternal_mortality_1995/index.html).
World Health Organization, UNICEF & UNFPA (2004) Maternal Mortality in 2000: Estimates
Developed by WHO, UNICEF and UNFPA. WHO, Geneva (available at: http://www.who.int/
reproductive-health/publications/maternal_mortality_2000/index.html).
World Health Organization, UNICEF, UNFPA & World Bank (2007) Maternal Mortality in
2005: Estimates Developed by WHO, UNICEF and UNFPA. Geneva (available at: http://
www.who.int/reproductive-health/publications/maternal_mortality_2005/index.html).
Perspectives on access to emergency obstetric care in Indonesia 241