Embed Size (px)
Citation preview

Filling in the gaps of clerkship with a comprehensiveclinical skills curriculum
Pamela Veale • Julie Carson • Sylvain Coderre • Wayne Woloschuk •
Bruce Wright • Kevin McLaughlin
Received: 2 August 2013 / Accepted: 3 February 2014� Springer Science+Business Media Dordrecht 2014
Abstract Although the clinical clerkship model is based upon sound pedagogy,
including theories of social learning and situated learning, studies evaluating clinical
performance of residents suggests that this model may not fully meet the learning needs
of students. Here our objective was to design a curriculum to bridge the learning gaps of
the existing clerkship model and then evaluate the impact of this on performance on
clerkship summative evaluations. We followed Kern’s framework to design our curric-
ulum and then compared performance on the clerkship objective structured clinical
examination (OSCE), all summative clerkship multiple choice question (MCQ) examin-
ations, and the Medical Council of Canada Qualifying Examination (MCCQE) Part 1
before and after the introduction of our curriculum. In the 2 years following the intro-
duction of our clinical skills curriculum the mean score on the clerkship OSCE was
significantly higher than in the 2 years prior to our curriculum [67.12 (5.3) vs. 62.44
(4.93), p \ 0.001, d = 0.91]. With the exception of the surgical clerkship MCQ, per-
formance on all clerkship summative MCQ examinations and MCCQE Part 1 was sig-
nificantly higher following the introduction of our curriculum. In this study we found a
significant improvement in the performance on clerks on summative evaluations of
knowledge and clinical skills following the introduction of our clinical skills curriculum.
Given the unpredictable nature of clinical rotations, the clerkship will always be a risk of
failing to deliver the intended curriculum—so medical schools should continue to explore
and evaluate ways of changing the delivery of clerkship training to improve learning
outcomes.
Keywords Clerkship � Clinical skills � Curriculum
P. Veale � J. Carson � S. Coderre � W. Woloschuk � B. Wright � K. McLaughlin (&)Office of Undergraduate Medical Education, Health Sciences Centre, University of Calgary,3330 Hospital Drive NW, Calgary, AB T2N 4N1, Canadae-mail: [email protected]
123
Adv in Health Sci EducDOI 10.1007/s10459-014-9496-6
Introduction
During their undergraduate training, medical students transition from preclinical learning
experiences—primarily didactic and small group learning—to the immersive experience of
clerkship where they transfer their knowledge to the clinical setting and hone their clinical
skills. The clinical clerkship model is based upon theories of social learning and situated
learning, and should therefore be the ideal preparation for further training in residency and
beyond (Brown et al. 1989; Miller and Dollard 1941; Tulving and Thomson 1973). Or at
least this is what we had assumed until data began to emerge highlighting significant
deficiencies in the clinical skills of residents (Fred 2005; Mangione and Nieman 1997;
Mangione and Nieman 1999; Mangione 2001). So why does our current clerkship model
fail to provide the type of learning experiences necessary to develop clinical skills?
Finding deficiencies in trainees’ clinical skills does not necessarily imply that the
objectives of clerkship are misguided and/or our clerkship teachers are unskilled (He-
idenreich et al. 2000; Irby 1995; Sutkin et al. 2008). A more likely explanation for this
problem is the inescapable truth that training opportunities during clerkship are unpre-
dictable and conditional. First, we need patients with appropriate clinical findings who are
willing to be examined for the benefit of students, and then we need preceptors who have
the time and motivation to create this learning opportunity. But, when rounding on in-
patients we don’t usually have a stable patient with a pleural rub or critical aortic stenosis,
and even when we do we rarely have the time to allow each of our learners to perform the
appropriate physical examination and then provide them with feedback on their perfor-
mance. Thus, all too often valuable learning experiences are compromised by the need to
deliver efficient clinical care (Irby et al. 2004; Neher et al. 1992).
Prompted by an accreditation review of our program by the Liaison Committee on
Medical Education (LCME) in 2009, we sought to address some of the deficiencies of our
clerkship model at the University of Calgary. Our objectives in this study were first to
design a curriculum to bridge the learning gaps of the existing clerkship model and,
second, to evaluate the impact of this on performance on clerkship summative evaluations.
We followed Kern’s framework to create and implement a clinical skills curriculum that
runs alongside the clinical clerkship (Kern et al. 1998). Herein we describe how we
completed Kern’s six-step process for curricular design: problem identification and general
needs assessment; targeted needs assessment; goals and objectives; educational strategies;
implementation; and evaluation and feedback. Having designed our curriculum, we then
used a pre/post study design to compare performance on knowledge and clinical skills
evaluations for cohorts before and after the introduction of our clinical skills curriculum to
evaluate the impact of our new curriculum on learning outcomes.
Method
Participants
Our participants included medical students, recent graduates, and clerkship teachers at the
University of Calgary. We have a 3-year undergraduate curriculum, during which the first
2 years is a pre-clerkship Clinical Presentation Curriculum and the final year is the clinical
clerkship (Mandin et al. 1995). We have two clerkship streams: the rotation-based clerk-
ship where students rotate between seven mandatory rotations (Emergency Medicine,
Family Medicine, Internal Medicine, Obstetrics and Gynecology, Pediatrics, Psychiatry,
P. Veale et al.
123
and Surgery), and the Rural Integrated Community Clerkship, where students spend
9 months in a primary care setting covering the clinical presentation from each discipline,
and complete their clerkship with rotations in Internal Medicine and Pediatrics
(McLaughlin et al. 2011). In addition to clinical experiences, each of the clerkship rota-
tions also has a formal teaching curriculum, which is primarily in the form of didactic
teaching. Prior to initiation, our study was approved by the Conjoint Health Research
Ethics Board at the University of Calgary.
Participants who contributed to the needs assessment for our curriculum were clerkship
program directors, evaluation coordinators, clerks (from graduating class of 2010), and first
year residents who had graduated from the class of 2009. The participants who helped us
study the impact of our curriculum on learning outcomes were students from the two
graduating classes preceding the introduction of our curriculum (classes of 2009 and 2010,
n = 290) and the two classes following the introduction of the curriculum (classes of 2011
and 2012, n = 346).
Materials
The data used to guide our curriculum included the 2009 LCME Accreditation documents,
Graduate Questionnaire and student log books for the classes of 2007 and 2008, and
questionnaires and focus groups during which we asked participants to suggest changes to
the content and delivery of the clinical clerkship that would improve the quality of the
learning experience. As a measure of baseline academic performance we compared the
mean performance on all summative evaluations prior to clerkship for students from the
classes of 2009 and 2010 to that of students from classes 2011 and 2012. To assess the
impact of our curriculum on learning outcomes we used students’ scores on the summative
objective structured clinical examination (OSCE) and clerkship summative multiple choice
question (MCQ) examination for the classes of 2009–12, in addition to the Medical
Council of Canada Qualifying Examination (MCCQE) Part 1. During the 4 years of
observation there were no major changes in the content or minimum performance level of
the OSCE or local MCQ examinations.
Procedure
When creating our new curriculum we followed the six-step process for curricular design
described by Kern et al. (1998). For step 1 (problem identification and general needs
assessment) we used the accreditation report and supplemented this by results of student
log books and data from the Graduate Questionnaire. For step 2 (targeted needs assess-
ment) we used the detailed normative and perceived needs assessment from the key
stakeholders in undergraduate medical education program—including students, curriculum
planners, and teachers that formed part of the accreditation report—and supplemented
these data by administering questionnaires followed by focus groups interviews of clerk-
ship program directors, evaluation coordinators, clerks, and first year residents who had
recently graduated from our undergraduate program. The theme for our questionnaire and
focus group interviews was ways to improve the learning experience during clerkship. We
conducted two focus groups with clerkship directors and evaluation coordinators and two
focus groups with clerks and residents. In each case no new themes were identified in the
second focus group, from which we inferred saturation of themes.
Filling in the gaps of clerkship
123
To evaluate the impact of our new curriculum on learning outcomes we used a pre/post
study design to compare performance of cohorts from 2 years before and 2 years after the
introduction of our curriculum on all summative evaluations of knowledge during clerkship
in addition to the summative clerkship OSCE.
Statistical analyses
We performed thematic analysis of questionnaire data and the transcripts of our focus
groups to identify areas for improvement in clerkship. Two researchers (JC and KM)
extracted themes independently before reaching a consensus on the major themes and
categories. We used data from the questionnaires for data source triangulation of the focus
group data (Thurmond 2001). We used an independent sample t test with Cohen’s d as a
measure of effect size to compared scores for the two cohorts on pre-clerkship evaluations
and on clerkship evaluations before and after the introduction of our curriculum (Cohen
1988). We categorized effect sizes according to the thresholds suggested by Cohen (Cohen
1988): small (d = 0.20), medium (d = 0.5), and large (d = 0.8). We used STATA�
version 11.0 (StataCorp LP, College Station, TX) for our statistical analyses.
Results
Steps involved in creating a clinical skills curriculum in clerkship
Step 1: problem identification and general needs assessment
The LCME accreditation identified two clerkship-related concerns: ED-2, which states that
‘‘…faculty must monitor student experience and modify it as necessary to ensure that the
objectives of the clinical education program will be met’’; and ED-27 that requires
‘‘…ongoing assessment that assures students have acquired and can demonstrate on direct
observation the core clinical skills…’’ (http://www.lcme.org/functions.pdf, June 2008).
Reviewing the available data on our clerkship curriculum, we articulated the problem of
our existing model as inconsistent observation and teaching of clinical skills in important
clinical presentations.
Step 2: targeted needs assessment of learners
Qualitative analysis of our questionnaire and focus group interviews identified ten prob-
lems with our existing clerkship model that were grouped into the themes of content and
delivery. Content-related deficiencies included: inconsistent exposure to some clinical
presentations (Accreditation Standard ED-2), clinical skills training, procedural skills
training, teaching in diagnostic and therapeutics, teaching in basic science (including
microbiology), teaching in chronic disease management, and training in conflict resolution.
Delivery-related deficiencies included: limited direct observation of clinical skills
(Accreditation Standard ED-27), block learning rather than dispersed learning, and over-
reliance on didactic teaching.
P. Veale et al.
123

Step 3: goals and objectives
For each component of our curriculum we articulated specific learning objectives,
including the desired changes in knowledge, skills, and/or attitudes as a result of the
planned learning experiences. Consistent with the problem identified in step 1, however,
the a priori goal of our curriculum was that: following the introduction of the clinical skills
curriculum the rating of students’ knowledge and clinical skills will increase.
Step 4: educational strategies
When we considered ways of addressing the deficiencies of our existing clerkship model,
we opted for a curriculum to run alongside clerkship rather than to try and change each
clerkship rotation. This was because we considered that some of the problems identified
may not be remediable during busy clerkship rotations. For example, some conditions are
seasonal—so it is not possible to provide cases of croup for students who complete their
Pediatrics rotation during the summer months; in teaching hospitals residents typically
have priority in performing the limited number of procedural skills available, thus limiting
training opportunities for clerks; and a clerkship model based on rotation blocks is not
designed to create dispersed learning (Glenberg and Lehmann 1980; Sisti et al. 2007).
Based upon the needs assessment, we deciding that our curriculum must be compre-
hensive, should be dispersed, and that learning experiences should, where possible, adhere
to the principles of ‘‘deliberate practice’’ (Ericsson and Lehmann 1994; Glenberg and
Lehmann 1980; Kerfoot et al. 2007; Raman et al. 2010; Sisti et al. 2007). We began by
identifying all mandatory clinical presentations for clerkship, after which we created a
blueprint for our curriculum to ensure that each of these presentations would be encoun-
tered (Coderre et al. 2009). We then selected the most appropriate delivery format for each
presentation. For example, to cover emergency presentations—such as acute onset chest
pain and/or dyspnea—we selected training on a human patient simulator. For presentations
emphasizing either communication skills (e.g., depression, family violence) or physical
examination skills (e.g., hypertension, joint pain) we used standardized patients, whereas
we used computerized virtual patients for presentations dealing with abnormal laboratory
tests (e.g., hyperkalemia, anemia). Training on human patient simulators, task trainers (for
procedural skills), standardized patients, and virtual patients involved direct observation of
performance with feedback and the opportunity for practice for training (Ericsson and
Lehmann 1994). Learning experiences were primarily in a small group or team-based
learning format (Michaelsen et al. 2002). Table 1 shows the type of learning experience for
each content area. As clerks are on a variety of rotations at any point in their clerkship year,
the timing of our curricular content did not coincide with the clinical experiences of
clerkship and was thus dispersed (Kerfoot et al. 2007; Raman et al. 2010). With the
exception of conflict resolution, we also introduced formative evaluations for each section
to provide feedback and enhance learning (Roediger and Karpicke 2006).
Step 5: implementation
We introduced our curriculum beginning with the class of 2011. Since then, on alternate
Friday afternoon from 12 to 5 pm clerks leave their clerkship rotations to attend the clinical
skills curriculum. The schedule for each session is shown in ‘‘Appendix’’ section. With the
exception of clerkships giving up 5 % of their scheduled time to our curriculum, the format
of the clinical clerkship has not changed.
Filling in the gaps of clerkship
123
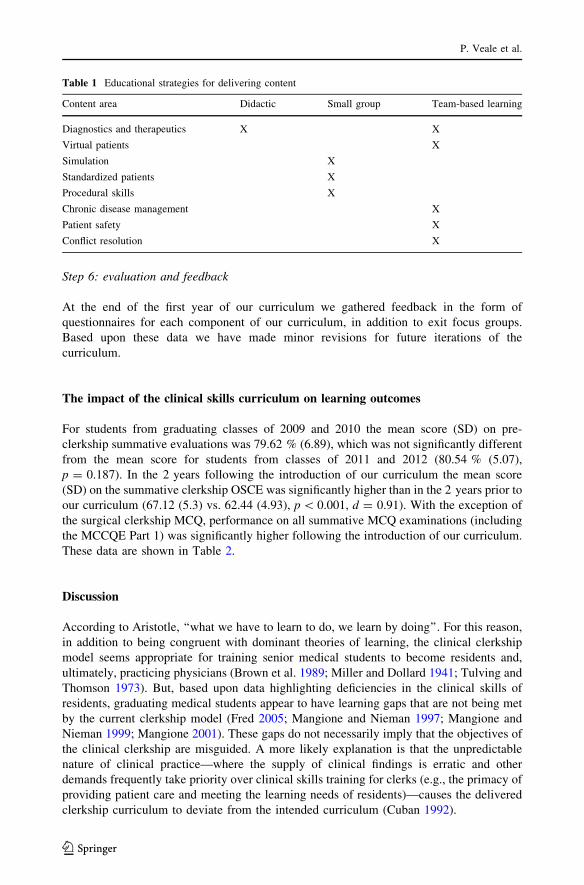
Step 6: evaluation and feedback
At the end of the first year of our curriculum we gathered feedback in the form of
questionnaires for each component of our curriculum, in addition to exit focus groups.
Based upon these data we have made minor revisions for future iterations of the
curriculum.
The impact of the clinical skills curriculum on learning outcomes
For students from graduating classes of 2009 and 2010 the mean score (SD) on pre-
clerkship summative evaluations was 79.62 % (6.89), which was not significantly different
from the mean score for students from classes of 2011 and 2012 (80.54 % (5.07),
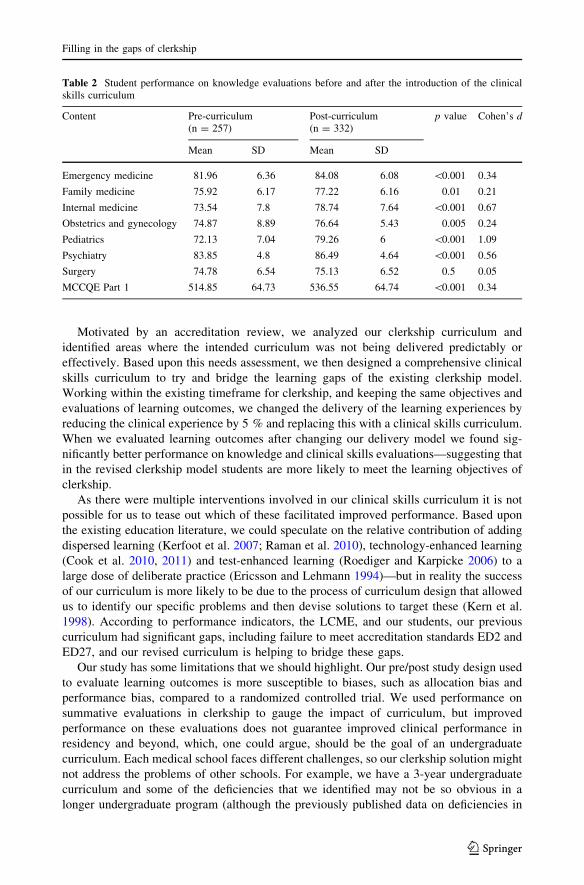
p = 0.187). In the 2 years following the introduction of our curriculum the mean score
(SD) on the summative clerkship OSCE was significantly higher than in the 2 years prior to
our curriculum (67.12 (5.3) vs. 62.44 (4.93), p \ 0.001, d = 0.91). With the exception of
the surgical clerkship MCQ, performance on all summative MCQ examinations (including
the MCCQE Part 1) was significantly higher following the introduction of our curriculum.
These data are shown in Table 2.
Discussion
According to Aristotle, ‘‘what we have to learn to do, we learn by doing’’. For this reason,
in addition to being congruent with dominant theories of learning, the clinical clerkship
model seems appropriate for training senior medical students to become residents and,
ultimately, practicing physicians (Brown et al. 1989; Miller and Dollard 1941; Tulving and
Thomson 1973). But, based upon data highlighting deficiencies in the clinical skills of
residents, graduating medical students appear to have learning gaps that are not being met
by the current clerkship model (Fred 2005; Mangione and Nieman 1997; Mangione and
Nieman 1999; Mangione 2001). These gaps do not necessarily imply that the objectives of
the clinical clerkship are misguided. A more likely explanation is that the unpredictable
nature of clinical practice—where the supply of clinical findings is erratic and other
demands frequently take priority over clinical skills training for clerks (e.g., the primacy of
providing patient care and meeting the learning needs of residents)—causes the delivered
clerkship curriculum to deviate from the intended curriculum (Cuban 1992).
Table 1 Educational strategies for delivering content
Content area Didactic Small group Team-based learning
Diagnostics and therapeutics X X
Virtual patients X
Simulation X
Standardized patients X
Procedural skills X
Chronic disease management X
Patient safety X
Conflict resolution X
P. Veale et al.
123
Motivated by an accreditation review, we analyzed our clerkship curriculum and
identified areas where the intended curriculum was not being delivered predictably or
effectively. Based upon this needs assessment, we then designed a comprehensive clinical
skills curriculum to try and bridge the learning gaps of the existing clerkship model.
Working within the existing timeframe for clerkship, and keeping the same objectives and
evaluations of learning outcomes, we changed the delivery of the learning experiences by
reducing the clinical experience by 5 % and replacing this with a clinical skills curriculum.
When we evaluated learning outcomes after changing our delivery model we found sig-
nificantly better performance on knowledge and clinical skills evaluations—suggesting that
in the revised clerkship model students are more likely to meet the learning objectives of
clerkship.
As there were multiple interventions involved in our clinical skills curriculum it is not
possible for us to tease out which of these facilitated improved performance. Based upon
the existing education literature, we could speculate on the relative contribution of adding
dispersed learning (Kerfoot et al. 2007; Raman et al. 2010), technology-enhanced learning
(Cook et al. 2010, 2011) and test-enhanced learning (Roediger and Karpicke 2006) to a
large dose of deliberate practice (Ericsson and Lehmann 1994)—but in reality the success
of our curriculum is more likely to be due to the process of curriculum design that allowed
us to identify our specific problems and then devise solutions to target these (Kern et al.
1998). According to performance indicators, the LCME, and our students, our previous
curriculum had significant gaps, including failure to meet accreditation standards ED2 and
ED27, and our revised curriculum is helping to bridge these gaps.
Our study has some limitations that we should highlight. Our pre/post study design used
to evaluate learning outcomes is more susceptible to biases, such as allocation bias and
performance bias, compared to a randomized controlled trial. We used performance on
summative evaluations in clerkship to gauge the impact of curriculum, but improved
performance on these evaluations does not guarantee improved clinical performance in
residency and beyond, which, one could argue, should be the goal of an undergraduate
curriculum. Each medical school faces different challenges, so our clerkship solution might
not address the problems of other schools. For example, we have a 3-year undergraduate
curriculum and some of the deficiencies that we identified may not be so obvious in a
longer undergraduate program (although the previously published data on deficiencies in
Table 2 Student performance on knowledge evaluations before and after the introduction of the clinicalskills curriculum
Content Pre-curriculum(n = 257)
Post-curriculum(n = 332)
p value Cohen’s d
Mean SD Mean SD
Emergency medicine 81.96 6.36 84.08 6.08 \0.001 0.34
Family medicine 75.92 6.17 77.22 6.16 0.01 0.21
Internal medicine 73.54 7.8 78.74 7.64 \0.001 0.67
Obstetrics and gynecology 74.87 8.89 76.64 5.43 0.005 0.24
Pediatrics 72.13 7.04 79.26 6 \0.001 1.09
Psychiatry 83.85 4.8 86.49 4.64 \0.001 0.56
Surgery 74.78 6.54 75.13 6.52 0.5 0.05
MCCQE Part 1 514.85 64.73 536.55 64.74 \0.001 0.34
Filling in the gaps of clerkship
123

clinical skills were not restricted to three-year curricula) (Mangione and Nieman 1997,
1999; Mangione 2001). Similarly, we cannot claim that our curriculum is the optimum way
to improve clinical skills training in our medical school as there are many questions that
our study does not address. For example, what is the ideal balance of clinical experience
and clinical skills training? What is the best learning experience in which to learn different
clinical skills—e.g., is training on a virtual patient with chest pain as effective as a high
fidelity simulator or standardized patient? Clearly there is still a long way to go before we
can describe the optimum clinical skills curriculum to complement the clinical training of
clerkship.
Implications for medical education
Real clinical experiences are, and should be, the core learning experience in clerkship. Yet,
the traditional clerkship model appears to fall short of meeting the learning needs of
students. It is unlikely that our medical school is alone in having struggled with meeting
accreditation standards and providing students with the types of learning experiences
during clerkship that allow them to develop their clinical skills. The supply of teaching
resources, such as available clinical teachers with willing patients who have good clinical
findings, is unpredictable in all clinical rotations—so the clinical clerkship will always be a
risk of failing to deliver the intended clerkship curriculum. As such, each medical school
should consider and evaluate ways of changing the delivery of clerkship training to
improve learning outcomes. In this study we have described how we designed a clinical
skills curriculum to run alongside the clinical rotations and how performance on clerkship
evaluations improved following the introduction of this curriculum. Our curriculum is
clearly not a panacea, but we hope that the description of how we devised this might help
others struggling to deliver their clerkship curriculum.
Appendix
See Table 3.
Table 3 Schedule for curricular content
Time Topic
12.00–12.45 Diagnostics and therapeutics (n = 160)
13.00–14.45 Virtual patients (n = 80) Simulation (n = 10)
Standardized patients (n = 20)
Procedural skills (n = 10)
Diagnostics and therapeutics OR
Chronic disease management OR
Patient safety OR
Conflict resolution OR
Back to basic science OR
Formative evaluations (n = 40)
15.00–16.45 Groups switch Groups switch
P. Veale et al.
123
References
Brown, J. S., Collins, A., & Duguid, P. (1989). Situated cognition and the culture of learning. EducationalResearcher, 18, 32–42.
Coderre, S., Woloschuk, W., & McLaughlin, K. (2009). Twelve tips for blueprinting. Medical Teacher, 31,322–324.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: LawrenceEarlbaum Associates.
Cook, D. A., Erwin, P. J., & Triola, M. M. (2010). Computerized virtual patients in health professionseducation: A systematic review and meta-analysis. Academic Medicine, 85, 1589–1602.
Cook, D. A., Hatala, R., Brydges, R., Zendejas, B., Szostek, J. H., Wang, A. T., et al. (2011). Technology-enhanced simulation for health professions education: A systematic review and meta-analysis. Journalof the American Medical Association, 306, 978–988.
Cuban, L. (1992). Curriculum stability and change. In P. W. Jackson (Ed.), Handbook of research oncurriculum. New York: Macmillan.
Ericsson, K. A., & Lehmann, A. C. (1994). Expert performance: Its structure and acquisition. AmericanPsychologist, 49, 725–747.
Fred, H. L. (2005). Hyposkillia: Deficiency of clinical skills. Texas Heart Institute Journal, 32, 255–257.Glenberg, A. M., & Lehmann, T. S. (1980). Spacing repetitions over 1 week. Memory & Cognition, 8,
528–538.Heidenreich, C., Lye, P., Simpson, D., & Lourich, M. (2000). The search for effective and efficient
ambulatory teaching methods through the literature. Pediatrics, 105, 231–237.Irby, D. M. (1995). Teaching and learning in ambulatory care settings: A thematic review of the literature.
Academic Medicine, 70, 898–931.Irby, D. M., Aagaard, E., & Teherani, A. (2004). Teaching points identified by preceptors observing one-
minute preceptor and traditional preceptor encounters. Academic Medicine, 79, 50–55.Kerfoot, B., DeWolf, W., Masser, B., Church, P. A., & Federman, D. D. (2007). Spaced education improves
the retention of clinical knowledge by medical students: A randomized controlled trial. MedicalEducation, 41, 23–31.
Kern, D. E., Thomas, P. A., Howard, D. M., & Bass, E. B. (1998). Curriculum development for medicaleducation: A six-step approach. Baltimore, MD: Johns Hopkins University Press.
LCME. http://www.lcme.org/functions.pdf (June 2008).Mandin, H., Harasym, P., Eagle, C., & Watanabe, M. (1995). Developing a ‘‘clinical presentation’’ cur-
riculum at the University of Calgary. Academic Medicine, 70, 186–193.Mangione, S. (2001). Cardiac auscultatory skills of physicians-in-training: A comparison of three English-
speaking countries. American Journal of Medicine, 110, 210–216.Mangione, S., & Nieman, L. Z. (1997). Cardiac auscultatory skills of internal medicine and family practice trainees:
A comparison of diagnostic proficiency. Journal of the American Medical Association, 278, 717–722.Mangione, S., & Nieman, L. Z. (1999). Pulmonary auscultatory skills during training in internal medicine
and family practice. American Journal of Respiratory and Critical Care Medicine, 159, 1–6.McLaughlin, K., Bates, J., Konkin, J., Woloschuk, W., Suddards, C. A., & Regehr, G. (2011). A comparison
of performance evaluations of students on longitudinal integrated clerkships and rotation-basedclerkships. Academic Medicine, 86(10 Suppl), S25–S29.
Michaelsen, L. K., Knight, A. B., & Fink, D. L. (2002). Team-based learning: A transformative use of smallgroups. Westport, CT: Praeger Publishers.
Miller, N. E., & Dollard, J. C. (1941). Social learning and imitation. New Haven, CT: Yale University Press.Neher, J. O., Gordon, K. C., Meyer, B., & Stevens, N. (1992). A five-step ‘‘microskills’’ model of clinical
teaching. Journal of the American Board of Family Practice, 5, 419–424.Raman, M., McLaughlin, K., Violato, C., Rostom, A., Allard, J. P., & Coderre, S. (2010). Teaching in small
portions dispersed over time enhances long-term knowledge retention. Medical Teacher, 32, 250–255.Roediger, H. L., & Karpicke, J. D. (2006). Test-enhanced learning: Taking memory tests improves long-
term retention. Psychological Science, 17, 249–255.Sisti, H. M., Glass, A. L., & Shors, T. J. (2007). Neurogenesis and the spacing effect: Learning over time
enhances memory and the survival of new neurons. Learning & Memory, 14, 368–375.Sutkin, G., Wagner, E., Harris, I., & Schiffer, R. (2008). What makes a good clinical teacher in medicine? A
review of the literature. Academic Medicine, 83, 452–466.Thurmond, V. A. (2001). The point of triangulation. Journal of Nursing Scholarship, 33, 253–258.Tulving, E., & Thomson, D. M. (1973). Encoding specificity and retrieval processes in episodic memory.
Psychological Review, 80, 352–373.
Filling in the gaps of clerkship
123





























