Embed Size (px)
Citation preview

Filippi Syndrome: Report of Three Additional Cases
Marc S. Williams,1* Janet L. Williams,1 David S. Wargowski,2 Richard M. Pauli,2 andBeth A. Pletcher3
1Gundersen Lutheran Medical Center, La Crosse, Wisconsin2Department of Pediatrics, University of Wisconsin, Madison, Wisconsin3Department of Pediatrics, New Jersey Medical School, University of Medicine and Dentistry, Newark, New Jersey
Filippi syndrome is an autosomal recessivecondition characterized by variable soft tis-sue syndactyly of the fingers and toes, mi-crocephaly, pre- and postnatal growth re-tardation, mildly abnormal craniofacial ap-pearance, and mental retardation. Wereport on three unrelated individuals withFilippi syndrome. All have microcephaly,minor facial anomalies, variable syndactylyof digits, growth impairment, and develop-mental delay. One patient also has polydac-tyly, which has not been reported previ-ously in the Filippi syndrome. Am. J. Med.Genet. 87:128–133, 1999. © 1999 Wiley-Liss, Inc.
KEY WORDS: MCA/MR syndrome; syndac-tyly; microcephaly; growthfailure
INTRODUCTION
Filippi [1985] described an autosomal recessive syn-drome in three of eight sibs (two boys and one girl) bornto healthy, nonconsanguineous parents, comprisingsyndactyly of the 3rd and 4th fingers, syndactyly oftoes 2, 3, and 4, microcephaly, and severe physical andmental retardation. Five subsequent reports describednine affected patients. We report on new findings inthree unrelated patients with this disorder.
CLINICAL REPORTSCase 1
The patient is the second child born to healthy, non-consanguineous Caucasian parents. The pregnancywas uncomplicated. He was delivered vaginally andweighed 2.76 kg with an OFC of 35 cm. He had softtissue syndactyly of toes 2–5 bilaterally and a super-numerary soft tissue digit arising from the left 5th fin-ger that was ligated. He experienced feeding difficul-ties and failure to thrive and developed positional
plagiocephaly. Craniosynostosis was excluded by com-puted tomography scan of the skull. Development issignificantly delayed at age 26 months: gross and finemotor skills clustered at age 9–10 months, cognitiveskills at age 9–12 months, and social skills at age 12–18 months. He had frequent upper respiratory and si-nus infections until tonsillectomy and adenoidectomywere performed. Accommodative esotropia with pos-sible type 1 Duane syndrome is present, and the pa-tient wears glasses.
Exam at age 27 months showed the following: weight9.5 kg (< 3rd centile, weight average of age 10 months),length 81.5 cm (< 3rd centile, length average of age 17months), and OFC 45.4 cm (< 3rd centile, 50th centileat 8 months). Physical findings include brachycephalywith slight ridging of all sutures and frontal upsweep;bilateral mild ptosis, small, downward-slanting palpe-bral fissures (palpebral fissure length 20 mm, −4 SD),left lateral gaze palsy and relative telecanthus [innercanthal distance (ICD) 30 mm, 80th centile] (Fig. 1A,B); limited range of facial expression without truefacial palsy; small hands with proportionate brachy-dactyly (middle finger index (MFI) 0.44), tapered digitswith bilateral fifth finger clinodactyly, and indistinctpalmar creases (Fig. 3A); lateral deviation of the hal-luces and toe syndactyly as described above (Fig. 4A).Testes are descended. Karyotype is 46,XY.
Case 2
The patient is the second child born to healthy, non-consanguineous Egyptian parents. The pregnancy wasuncomplicated. She was delivered vaginally at termfrom a footling breech presentation. Birth weight was2.75 kg. She was breastfed and gained weight slowly.General health has been good. Development was de-layed as she first walked and talked at age 2 and 3years, respectively. Vision and hearing are normal. Atage 7, she attends a school for multiply handicappedchildren. She has 30–35 words and speaks in simplesentences.
Exam at age 7 years showed the following: weight18.2 kg (10th centile), height 108 cm (3rd centile), OFC47.6 cm (< 3rd centile). Physical findings include small,pinched nasal bridge with slight deviation of nasal sep-tum, and a pointed nasal tip; relative telecanthus with
*Correspondence to: Marc S. Williams, M.D., 1836 South Av-enue, La Crosse, WI 54601. E-mail: [email protected]
Received 4 February 1998; Accepted 14 July 1999
American Journal of Medical Genetics 87:128–133 (1999)
© 1999 Wiley-Liss, Inc.

downward slanting palpebral fissures (Fig. 1C);slightly high-arched palate; indistinct palmar creaseswith extremely tapered fingers and distal digital hypo-plasia with slight 3–4 syndactyly (Fig. 3B); broad greattoes and bilateral 2–5 toe syndactyly of the toes. Neu-rological examination was unremarkable with the ex-ception of the mental retardation. Karyotype is 46,XXand head magnetic resonance imaging was normal.
Case 3The patient is the first child of healthy nonconsan-
guineous parents. Prenatal history was unremarkable.Birth weight was 2,730 g and length was 45.7 cm.Weight, length, and head circumference remained be-low the third percentile. At age 2 4/12 years the follow-ing unusual anomalies were noted: apparent telecan-thus [ICD 3.0 cm, outer canthal distance (OCD) 7.7
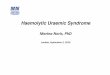
Fig. 1. Patient 1 (A and B) at age 27 months. Patient 2 (C) at age 7years. Note brachycephaly, relative telecanthus, ptosis, downward-slanting palpebral fissures, blepharophimosis, and unusual nose.
Filippi Syndrome 129

cm], epicanthic folds, small palpebral fissures (1.9 and2.1 cm right and left) that slant up, prominent glabella,broad, flat nasal base, broad nasal tip, moderate mi-crognathia, inability to open the mouth, mild overfold-ing of the helix, and mild skin redundancy of the neck(Fig. 2A,B). Limbs showed 2–3, 3–4, and mild 4–5 syn-
dactyly of the left hand. Proximal flexion creases of thethird fingers were displaced proximally, suggestingshortness of the proximal phalanges bilaterally. Thesecond and fifth fingers showed clinodactyly bilater-ally. There was a possible dislocation of the right pa-tella. Feet showed 2–3 and 3–4 syndactyly bilaterally,
Fig. 2. Patient 3 at ages 2 4/12 years and 17 years. Note brachycephaly, facial asymmetry, relative telecanthus, unusual nose, and small jaw.
130 Williams et al.

more prominent on the left. Neurological examinationwas remarkable for severe developmental delay, mildhypotonia, and sparse facial expression with no cra-nial nerve palsies.
The patient was subsequently examined at age 17years. She has significant mental retardation and un-usual behaviors that include inappropriate laughterwithout emotional content (sometimes lasting forhours), repetitive speech, and physical restlessness.Other episodes have been characterized as Tourette-like with explosive speech and profanity. She had sig-nificant scoliosis that required spinal fusion as well aspersistent leg length discrepancy treated with epiph-ysiodesis. Weight was 40 kg (< 5th centile), height139.7 cm (< 5th centile), span 135 cm, OFC 51.9 cm(−2 SD). Physical findings include marked brachy-cephaly with a prominent glabella; facial asymmetry(left side smaller than right); relative telecanthus(ICD 3.4 cm, 80th centile) with up-slanting palpebralfissures and bilateral epicanthic folds; broad nasal tipand columella with indistinct alae nasi and short phil-
trum (Fig. 2C,D; small mouth and chin with trismusand dysfunction of the left orbicularis anguli; smallright upper canine and absence of left upper canine;and a grade II/VI crescendo-decrescendo murmur. Bothhands were similar and unusual in form with long, thinpalms and short fingers (MFI 0.39, < 3rd centile).There is ulnar deviation of the second digits, radialdeviation of the fifth digits, shortness of the 4th middlephalanges, and cutaneous syndactyly of 2–3, 4–5, andto a milder degree 3–4 (Fig. 3C,D). Dermatographicpatterns are unremarkable. Feet show broad great toeswith marked 2–3 and moderate 3–4 syndactyly (Fig.4B,C). Neurological exam suggests cerebellar dysfunc-tion with truncal titubation, wide-based gait, and poorrecovery skills with no other findings besides mentalretardation.
DISCUSSION
This report brings the total number of patients withFilippi syndrome to 12. [Filippi, 1985; Meinecke, 1993;
Fig. 3. Hands of patients 1 (A), 2 (B), and 3 (C and D). Note tapering and varible brachydactyly and syndactyly.
Filippi Syndrome 131

Heron et al., 1995; Toriello and Higgins, 1995; Fryer,1996]. Common manifestations are presented in TableI. The only traits seen in every patient are postnatal,i.e., acquired microcephaly and growth retardation, toesyndactyly, characteristic facial appearance, and devel-opmental delay. The 3–4 syndactyly of the fingers maybe the single most distinctive finding in this condition,but is clearly not present in all patients even whenfrom the same family. This trait is shared with syndac-tyly type II [OMIM, 1996]. In contrast to Filippi syn-drome, 96% of these patients have 3–4 syndactyly ofthe fingers, whereas only 69.5% have syndactyly of thefeet [Sayli et al., 1995]. Polydactyly is also common inthis condition, whereas it has been seen in Filippi syn-drome only once [patient one, this report]. Mental re-tardation, growth retardation, and microcephaly have
not been reported in syndactyly type II. Syndactylytype II is known to be caused by mutations in theHOXD-13 gene [Akarsu et al., 1996] and is inherited inan autosomal dominant fashion. To our knowledge,this gene has not been analyzed in any patient withFilippi syndrome. Apparent tapering of the fingers isanother finding that seems to occur frequently in Fil-ippi syndrome. The face has a distinctive gestalt thatdoes not lend itself easily to objective delineation. Allthree of our patients had relative telecanthus. The pub-lished pictures of other affected individuals suggestthis may be a common anomaly, although measure-ments have not been published. The range of develop-mental delay/mental retardation is large, althoughmost showed moderate to severe dysfunction with theexception of the patients of Fryer [1996].
Fig. 4. Feet of patients 1 (A) and 3 (B and C).Note similarity of pattern of syndactyly.
132 Williams et al.

The differential diagnosis of Filippi syndrome is welldiscussed by Toriello and Higgins [1995] and will notbe reiterated. The three patients most closely resembleFilippi syndrome, although they have several addi-tional anomalies not previously described in this disor-der. These include Duane syndrome, ptosis, blepharo-phimosis and polydactyly (patient 1), indistinct palmarcreases (patients 1 and 2), scoliosis, leg length discrep-ancy, and cerebellar dysfunction (patient 3).
Autosomal recessive inheritance is assumed. Thepathogenesis of this disorder is unknown. The currentinterest in genes expressed in the developing brain andlimb, such as sonic hedgehog, may yield candidates formutational analysis.
ACKNOWLEDGMENTS
We thank the assistance and review of Dr. FrankDesposito. Thanks also to Kathy Sandy who assisted inpreparation of the table and the Gundersen-Lutheranmedical media department who prepared the illustra-tions.
REFERENCESAkarsu AN, Stoilov I, Yilmaz E, Sayli BS, Sarfarazi M. 1996. Genomic
structure of HOXD13 gene: a nine polyalanine duplication causes syn-polydactyly in two unrelated families. Hum Mol Genet 5:945–952.
Filippi G. 1985. Unusual facial appearance, microcephaly, growth andmental retardation, and syndactyly: a new syndrome? Am J Med Genet22:821–824.
Fryer A. 1996. Filippi syndrome with mild learning difficulties. Clin Dys-morph 5:35–39.
Heron D, Billette de Villimeur T, Munnich A, Lyonnet S. 1995. Filippisyndrome: a new case with skeletal abnormalities. J Med Genet 32:659–661.
Meinecke P. 1993. Short stature, microcephaly, characteristic face, syndac-tyly and mental retardation: the Filippi syndrome: report on a secondfamily. Genet Couns 4:147–151.
Online Mendelian Inheritance in Man, OMIM (TM). 1996. Center for Medi-cal Genetics, Johns Hopkins University (Baltimore, MD) and NationalCenter for Biotechnology Information, National Library of Medicine(Bethesda, MD).
Sayli BS, Akarsu AN, Sayli U, Akhan O, Ceylaner S, Sarfarazi M. 1995. Alarge Turkish kindred with syndactyly type II (synpolydactyly): 1. Fieldinvestigation, clinical and pedigree data. J Med Genet 32:421–434.
Toriello HV, Higgins JV. 1995. Craniodigital syndromes: report of a childwith Filippi syndrome and discussion of differential diagnosis. Am JMed Genet 55:200–204.
TABLE I. Filippi Syndrome
ParametersFillipi,1985
Meinecke,1993
Heronet al.,1995
Torielloand Higgins,
1995Fryer,1996
Thisreport Total (%)
Case 1 2 3 1 2 1 2 1 2 3Sex M M F M F F M M M M F F 7M, 5FBirthweight <2.5 kg − − + + + + + + − − + + 8/12 (75)Short stature + + + + + − + + + + + + 11/12 (92)Microcephaly + + + + + + + + + + + + 12/12 (100)Facial
High frontal hairline/forehead + + + − − + + + + + + − 9/12 (75)Palpebral fissures slant (up or down) − − − ? − + + + ? + + + 6/10 (60)Broad nasal bridge/relative telecanthus + + + + + + + + + + + + 12/12 (100)Thin alae nasi + + + + + + + + ? − − + 9/11 (82)Micrognathia − − − − − − + − − + − + 3/12 (25)
HandsTapered fingers − − − − − + + + ? + + − 5/11 (45)Clinodactyly + + + − + + + − − + + + 9/12 (75)Syndactyly + + − + + − + + − − + + 8/12 (67)
Abnormal palmar crease − − + + + + + ? ? + + − 7/10 (70)Feet
Syndactyly + + + + + + + + + + + + 12/12 (100)Mental retardation/developmental delay + + + + + + + + + + + + 12/12 (100)
Filippi Syndrome 133