Embed Size (px)
Citation preview

Filing at a Glance
Company: Capital District Physicians Health Plan Inc
Product Name: 2020 Individual Rate
State: New York
TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)
Sub-TOI: HOrg02I.005D Individual - HMO
Filing Type: 2020 Prior Approval ACA Rates
Date Submitted: 05/13/2019
SERFF Tr Num: CAPD-131909302
SERFF Status: Pending Industry Response
State Tr Num: 2019050149
State Status: CP-xx-CR
Co Tr Num: 2020 INDV RATE
ImplementationDate Requested:
01/01/2020
Disposition Date:
Disposition Status:
Implementation Date:
State Filing Description:
SERFF Tracking #: CAPD-131909302 State Tracking #: 2019050149 Company Tracking #: 2020 INDV RATE
State: New York Filing Company: Capital District Physicians Health Plan Inc
TOI/Sub-TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)/HOrg02I.005D Individual - HMO
Product Name: 2020 Individual Rate
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number CAPD-131909302 Generated 05/21/2019 09:06 AM

General Information
Company and Contact
Filing Fees
State Specific
Project Name: Status of Filing in Domicile:
Project Number: Date Approved in Domicile:
Requested Filing Mode: Review & Approval Domicile Status Comments:
Explanation for Combination/Other: Market Type: Individual
Submission Type: Individual Market Type: Individual, Non Employer Group -Individual
Overall Rate Impact: Filing Status Changed: 05/15/2019
State Status Changed: 05/15/2019
Deemer Date:
Corresponding Filing Tracking Number: CAPD-131893519
PPACA: Not PPACA-Related
PPACA Notes: null
Exchange Intentions: NY State Indiv Exchange
Filing Description:
2020 Indiv On & Off Rate Filing Form (CAPD-131919800), (CAPD-131919800)
Filing Contact Information
Filing Company InformationCapital District Physicians HealthPlan Inc
Patroon Creek Corporate Center
1223 Washington Avenue
Albany, NY 12206-1057
(518) 641-3000 ext. [Phone]
CoCode: 95491
Group Code: -99
Group Name:
FEIN Number: 14-1641028
State of Domicile: New York
Company Type:
State ID Number: 95491
Fee Required? No
Retaliatory? No
Fee Explanation:
1. Is a parallel filing being submitted for another issuing entity of the same parent organization? Yes/No (If Yes, enter nameof other entity, submission date, and SERFF Tracking Number of the parallel file.): No2. Does this filing contain a dental, vision or health insurance policy or contract that uses a network of health care providers?(If Yes, enter the PNDS Network ID number and name. If the network has not been filed in PNDS, it must be filed within 60
SERFF Tracking #: CAPD-131909302 State Tracking #: 2019050149 Company Tracking #: 2020 INDV RATE
State: New York Filing Company: Capital District Physicians Health Plan Inc
TOI/Sub-TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)/HOrg02I.005D Individual - HMO
Product Name: 2020 Individual Rate
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number CAPD-131909302 Generated 05/21/2019 09:06 AM

days of approval.): NYN002, CDPHP HMO3. : NA4. Type of filing? Enter Form and Rate, Form only, Rate only (Form only should be used ONLY when the filing only containsan application, advertisement, administrative form, or is a group prefiling notification, out-of-state, or a report filing. Formsubmissions with no proposed rate impact are considered form and rate filings and require an actuarial memorandum.): Rate5. Is this a Rate only filing? Yes/No [If Yes, enter one: Commission/Fee Schedule, DBL Loss Ratio Monitoring, ExperienceFiling Monitoring, Experience Rating Formula, Medicare Supplement Annual Filing (other than rate adjustment), RateAdjustment, or Other with brief explanation).]: Yes6. Does this submission contain a form subject to Regulation 123 (i.e., the certificate is deemed delivered in New York State)?Yes/No (If Yes, provide a full explanation in the Filing Description field.): No7. Did this insurer prefile group coverage for this group under Section 52.32 prior to this filing? Yes/No (If Yes, enter thestate tracking number assigned and the effective date of coverage.): 20190500378. Does this submission contain any form which is subject to review by the Life Bureau, the Property Bureau or both? Yes/No(If Yes, identify the forms, the Bureau, the date submitted, and the SERFF file number.): No9. Does this filing contain forms that replace any other previously approved forms? Yes/No (If Yes, identify the formnumbers, the file number, and the date of approval of the forms being replaced in the Filing Description field.): NA
SERFF Tracking #: CAPD-131909302 State Tracking #: 2019050149 Company Tracking #: 2020 INDV RATE
State: New York Filing Company: Capital District Physicians Health Plan Inc
TOI/Sub-TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)/HOrg02I.005D Individual - HMO
Product Name: 2020 Individual Rate
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number CAPD-131909302 Generated 05/21/2019 09:06 AM

Rate Information Rate data applies to filing.
Filing Method: 2020 Prior Approval ACA Rates
Rate Change Type: Increase
Overall Percentage of Last Rate Revision: 5.100%
Effective Date of Last Rate Revision: 01/01/2019
Filing Method of Last Filing: 2019 Prior Approval ACA Rates
SERFF Tracking Number of Last Filing: CAPD-131471166
Company Rate Information
Company
Name:
Company
Rate
Change:
Overall %
Indicated
Change:
Overall %
Rate
Impact:
Written
Premium
Change for
this Program:
Number of Policy
Holders Affected
for this Program:
Written
Premium for
this Program:
Maximum %
Change
(where req'd):
Minimum %
Change
(where req'd):
Capital DistrictPhysicians HealthPlan Inc
Increase 7.050% 7.050% $2,682,388 4,118 $40,732,266 8.960% -5.290%
SERFF Tracking #: CAPD-131909302 State Tracking #: 2019050149 Company Tracking #: 2020 INDV RATE
State: New York Filing Company: Capital District Physicians Health Plan Inc
TOI/Sub-TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)/HOrg02I.005D Individual - HMO
Product Name: 2020 Individual Rate
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number CAPD-131909302 Generated 05/21/2019 09:06 AM

Rate Review Detail
COMPANY:Company Name: Capital District Physicians Health Plan Inc
HHS Issuer Id: 94788
PRODUCTS:
Product Name HIOS Product ID HIOS Submission ID Number of Covered
LivesHMO 5812
Trend Factors:
FORMS:New Policy Forms: 01-0001-2020, 01-0002-2020
Affected Forms:
Other Affected Forms:
REQUESTED RATE CHANGE INFORMATION:Change Period: Annual
Member Months: 63,815
Benefit Change: Increase
Percent Change Requested: Min: -5.29 Max: 8.96 Avg: 7.05
PRIOR RATE:Total Earned Premium: 35,722,720.00
Total Incurred Claims: 32,118,297.00
Annual $: Min: 228.48 Max: 1,091.74 Avg: 545.56
REQUESTED RATE:Projected Earned Premium: 40,732,266.00
Projected Incurred Claims: 35,185,974.00
Annual $: Min: 233.72 Max: 1,195.37 Avg: 584.03
SERFF Tracking #: CAPD-131909302 State Tracking #: 2019050149 Company Tracking #: 2020 INDV RATE
State: New York Filing Company: Capital District Physicians Health Plan Inc
TOI/Sub-TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)/HOrg02I.005D Individual - HMO
Product Name: 2020 Individual Rate
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number CAPD-131909302 Generated 05/21/2019 09:06 AM
Rate/Rule Schedule
Item
No.
Schedule
Item
Status
Document Name
Affected Form Numbers
(Separated with commas) Rate Action Rate Action Information Attachments
1 Manual- New 2020 Rate Manual -Individual HMO OffExchange v2.pdf, 2020Rate Manual -Individual HMO OffExchange v2.xlsx,2020 Rate Manual -Individual HMO OnExchange v2.pdf, 2020Rate Manual -Individual HMO OnExchange v2.xlsx,
SERFF Tracking #: CAPD-131909302 State Tracking #: 2019050149 Company Tracking #: 2020 INDV RATE
State: New York Filing Company: Capital District Physicians Health Plan Inc
TOI/Sub-TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)/HOrg02I.005D Individual - HMO
Product Name: 2020 Individual Rate
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number CAPD-131909302 Generated 05/21/2019 09:06 AM

Capital District Physicians' Health Plan2020 Premium Rate Filing
Individual HMO Off Exchange
TABLE OF CONTENTS
Table of Contents 1
I. Rate Pages
Individual
Albany Region 2-4
Mid-Hudson Region 5-7
Syracuse Region 8-10
Utica/Watertown Region 11-13
II. Benefit Summary 14-21
III. Conversion Factor 22
IV. Region Factors 23
V. Tier Factors 24
VI. Rate Calculation 25
VIII. Expected Loss Ratio 26
IX. Commission Schedule 27
X. Factors for Base Plan Variations 28
1

Capital District Physicians' Health Plan
Albany Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Platinum HMO IHPF1053 IHPF1136
Single $853.03 $890.75 $37.72 4.42%
Double $1,706.06 $1,781.50 $75.44 4.42%
Emp/Child(ren) $1,450.15 $1,514.28 $64.13 4.42%
Family $2,431.14 $2,538.64 $107.50 4.42%
Platinum HMO IHPF1054 IHPF1137
Single $855.85 $895.09 $39.24 4.58%
Double $1,711.70 $1,790.18 $78.48 4.58%
Emp/Child(ren) $1,454.95 $1,521.65 $66.70 4.58%
Family $2,439.17 $2,551.01 $111.84 4.59%
Gold HMO IHGF2043 IHGF2135
Single $696.19 $758.54 $62.35 8.96%
Double $1,392.38 $1,517.08 $124.70 8.96%
Emp/Child(ren) $1,183.52 $1,289.52 $106.00 8.96%
Family $1,984.14 $2,161.84 $177.70 8.96%
Gold HMO IHGF2044 IHGF2136
Single $698.48 $762.23 $63.75 9.13%
Double $1,396.96 $1,524.46 $127.50 9.13%
Emp/Child(ren) $1,187.42 $1,295.79 $108.37 9.13%
Family $1,990.67 $2,172.36 $181.69 9.13%
Silver HMO IHSF3068 IHSF3280
Single $563.46 $588.53 $25.07 4.45%
Double $1,126.92 $1,177.06 $50.14 4.45%
Emp/Child(ren) $957.88 $1,000.50 $42.62 4.45%
Family $1,605.86 $1,677.31 $71.45 4.45%
Silver HMO IHSF3069 IHSF3281
Single $565.30 $591.37 $26.07 4.61%
Double $1,130.60 $1,182.74 $52.14 4.61%
Emp/Child(ren) $961.01 $1,005.33 $44.32 4.61%
Family $1,611.11 $1,685.40 $74.29 4.61%
Silver HMO IHSF3072 IHSF3288
Single $539.62 $569.86 $30.24 5.60%
Double $1,079.24 $1,139.72 $60.48 5.60%
Emp/Child(ren) $917.35 $968.76 $51.41 5.60%
Family $1,537.92 $1,624.10 $86.18 5.60%
Silver HMO IHSF3073 IHSF3289
Single $541.39 $572.62 $31.23 5.77%
Double $1,082.78 $1,145.24 $62.46 5.77%
Emp/Child(ren) $920.36 $973.45 $53.09 5.77%
Family $1,542.96 $1,631.97 $89.01 5.77%
Bronze HMO IHBF4061 IHBF4149
Single $405.74 $427.39 $21.65 5.34%
Double $811.48 $854.78 $43.30 5.34%
Emp/Child(ren) $689.76 $726.56 $36.80 5.34%
Family $1,156.36 $1,218.06 $61.70 5.34%
Bronze HMO IHBF4056 IHBF4150
Single $407.05 $429.44 $22.39 5.50%
Double $814.10 $858.88 $44.78 5.50%
Emp/Child(ren) $691.99 $730.05 $38.06 5.50%
Family $1,160.09 $1,223.90 $63.81 5.50%
Bronze HMO IHBF4057 IHBF4151
Single $400.11 $423.13 $23.02 5.75%
Double $800.22 $846.26 $46.04 5.75%
Emp/Child(ren) $680.19 $719.32 $39.13 5.75%
Family $1,140.31 $1,205.92 $65.61 5.75%
2020 Individual HMO Off Exchange Rate Manual Page 2

Capital District Physicians' Health Plan
Albany Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBF4058 IHBF4152
Single $401.41 $425.15 $23.74 5.91%
Double $802.82 $850.30 $47.48 5.91%
Emp/Child(ren) $682.40 $722.76 $40.36 5.91%
Family $1,144.02 $1,211.68 $67.66 5.91%
Platinum HMO New Plan IHPF5101
Single N/A $867.08 $0.00 0.00%
Double N/A $1,734.16 $0.00 0.00%
Emp/Child(ren) N/A $1,474.04 $0.00 0.00%
Family N/A $2,471.18 $0.00 0.00%
Platinum HMO New Plan IHPF5102
Single N/A $871.31 $0.00 0.00%
Double N/A $1,742.62 $0.00 0.00%
Emp/Child(ren) N/A $1,481.23 $0.00 0.00%
Family N/A $2,483.23 $0.00 0.00%
Silver HMO New Plan IHSF5101
Single N/A $566.62 $0.00 0.00%
Double N/A $1,133.24 $0.00 0.00%
Emp/Child(ren) N/A $963.25 $0.00 0.00%
Family N/A $1,614.87 $0.00 0.00%
Silver HMO New Plan IHSF5102
Single N/A $569.36 $0.00 0.00%
Double N/A $1,138.72 $0.00 0.00%
Emp/Child(ren) N/A $967.91 $0.00 0.00%
Family N/A $1,622.68 $0.00 0.00%
Platinum HMO IHPF1055 IHPF1057
Single $820.20 $891.04 $70.84 8.64%
Double $1,640.40 $1,782.08 $141.68 8.64%
Emp/Child(ren) $1,394.34 $1,514.77 $120.43 8.64%
Family $2,337.57 $2,539.46 $201.89 8.64%
Platinum HMO IHPF1056 IHPF1058
Single $822.91 $895.39 $72.48 8.81%
Double $1,645.82 $1,790.78 $144.96 8.81%
Emp/Child(ren) $1,398.95 $1,522.16 $123.21 8.81%
Family $2,345.29 $2,551.86 $206.57 8.81%
Gold HMO IHGF2045 IHGF2047
Single $713.80 $745.40 $31.60 4.43%
Double $1,427.60 $1,490.80 $63.20 4.43%
Emp/Child(ren) $1,213.46 $1,267.18 $53.72 4.43%
Family $2,034.33 $2,124.39 $90.06 4.43%
Gold HMO IHGF2046 IHGF2048
Single $716.15 $749.03 $32.88 4.59%
Double $1,432.30 $1,498.06 $65.76 4.59%
Emp/Child(ren) $1,217.46 $1,273.35 $55.89 4.59%
Family $2,041.03 $2,134.74 $93.71 4.59%
Silver HMO IHSF3074 IHSF3076
Single $577.19 $596.37 $19.18 3.32%
Double $1,154.38 $1,192.74 $38.36 3.32%
Emp/Child(ren) $981.22 $1,013.83 $32.61 3.32%
Family $1,644.99 $1,699.65 $54.66 3.32%
2020 Individual HMO Off Exchange Rate Manual Page 3

Capital District Physicians' Health Plan
Albany Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Silver HMO IHSF3075 IHSF3077
Single $579.08 $599.26 $20.18 3.48%
Double $1,158.16 $1,198.52 $40.36 3.48%
Emp/Child(ren) $984.44 $1,018.74 $34.30 3.48%
Family $1,650.38 $1,707.89 $57.51 3.48%
Bronze HMO IHBF4059 IHBF4062
Single $410.65 $432.93 $22.28 5.43%
Double $821.30 $865.86 $44.56 5.43%
Emp/Child(ren) $698.11 $735.98 $37.87 5.42%
Family $1,170.35 $1,233.85 $63.50 5.43%
Bronze HMO IHBF4060 IHBF4063
Single $411.98 $435.00 $23.02 5.59%
Double $823.96 $870.00 $46.04 5.59%
Emp/Child(ren) $700.37 $739.50 $39.13 5.59%
Family $1,174.14 $1,239.75 $65.61 5.59%
Platinum HMO IHPFC012 IHPFC016
Single $346.54 $367.11 $20.57 5.94%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Gold HMO IHGFC013 IHGFC017
Single $302.71 $307.11 $4.40 1.45%
Double N/A N/A $0.00 $0.00
Emp/Child(ren) N/A N/A $0.00 $0.00
Family N/A N/A $0.00 $0.00
Silver HMO IHSFC014 IHSFC018
Single $246.42 $245.71 ($0.71) -0.29%
Double N/A N/A $0.00 $0.00
Emp/Child(ren) N/A N/A $0.00 $0.00
Family N/A N/A $0.00 $0.00
Bronze HMO IHBFC015 IHBFC019
Single $177.81 $178.37 $0.56 0.31%
Double N/A N/A $0.00 $0.00
Emp/Child(ren) N/A N/A $0.00 $0.00
Family N/A N/A $0.00 $0.00
Catastrophic HMO IHCF5007 IHCF5008
Single $246.92 $238.33 ($8.59) -3.48%
Double $493.84 $476.66 ($17.18) -3.48%
Emp/Child(ren) $419.76 $405.16 ($14.60) -3.48%
Family $703.72 $679.24 ($24.48) -3.48%
2020 Individual HMO Off Exchange Rate Manual Page 4

Capital District Physicians' Health Plan
Mid-Hudson Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Platinum HMO IHPF1053 IHPF1136
Single $1,222.56 $1,273.03 $50.47 4.13%
Double $2,445.13 $2,546.06 $100.93 4.13%
Emp/Child(ren) $2,078.36 $2,164.15 $85.79 4.13%
Family $3,484.31 $3,628.13 $143.82 4.13%
Platinum HMO IHPF1054 IHPF1137
Single $1,226.61 $1,279.23 $52.62 4.29%
Double $2,453.21 $2,558.46 $105.25 4.29%
Emp/Child(ren) $2,085.23 $2,174.69 $89.46 4.29%
Family $3,495.83 $3,645.81 $149.98 4.29%
Gold HMO IHGF2043 IHGF2135
Single $997.78 $1,084.08 $86.30 8.65%
Double $1,995.56 $2,168.16 $172.60 8.65%
Emp/Child(ren) $1,696.23 $1,842.93 $146.70 8.65%
Family $2,843.68 $3,089.62 $245.94 8.65%
Gold HMO IHGF2044 IHGF2136
Single $1,001.06 $1,089.35 $88.29 8.82%
Double $2,002.13 $2,178.70 $176.57 8.82%
Emp/Child(ren) $1,701.81 $1,851.90 $150.09 8.82%
Family $2,853.03 $3,104.65 $251.62 8.82%
Silver HMO IHSF3068 IHSF3280
Single $807.55 $841.11 $33.56 4.16%
Double $1,615.10 $1,682.21 $67.11 4.16%
Emp/Child(ren) $1,372.84 $1,429.88 $57.04 4.15%
Family $2,301.52 $2,397.15 $95.63 4.16%
Silver HMO IHSF3069 IHSF3281
Single $810.19 $845.16 $34.97 4.32%
Double $1,620.38 $1,690.33 $69.95 4.32%
Emp/Child(ren) $1,377.32 $1,436.78 $59.46 4.32%
Family $2,309.04 $2,408.72 $99.68 4.32%
Silver HMO IHSF3072 IHSF3288
Single $773.38 $814.42 $41.04 5.31%
Double $1,546.77 $1,628.85 $82.08 5.31%
Emp/Child(ren) $1,314.75 $1,384.52 $69.77 5.31%
Family $2,204.15 $2,321.11 $116.96 5.31%
Silver HMO IHSF3073 IHSF3289
Single $775.92 $818.37 $42.45 5.47%
Double $1,551.84 $1,636.74 $84.90 5.47%
Emp/Child(ren) $1,319.07 $1,391.23 $72.16 5.47%
Family $2,211.38 $2,332.35 $120.97 5.47%
Bronze HMO IHBF4061 IHBF4149
Single $581.51 $610.81 $29.30 5.04%
Double $1,163.01 $1,221.62 $58.61 5.04%
Emp/Child(ren) $988.56 $1,038.38 $49.82 5.04%
Family $1,657.30 $1,740.81 $83.51 5.04%
Bronze HMO IHBF4056 IHBF4150
Single $583.39 $613.74 $30.35 5.20%
Double $1,166.77 $1,227.48 $60.71 5.20%
Emp/Child(ren) $991.75 $1,043.36 $51.61 5.20%
Family $1,662.65 $1,749.16 $86.51 5.20%
Bronze HMO IHBF4057 IHBF4151
Single $573.44 $604.72 $31.28 5.45%
Double $1,146.88 $1,209.44 $62.56 5.45%
Emp/Child(ren) $974.85 $1,028.03 $53.18 5.46%
Family $1,634.30 $1,723.46 $89.16 5.46%
2020 Individual HMO Off Exchange Rate Manual Page 5

Capital District Physicians' Health Plan
Mid-Hudson Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBF4058 IHBF4152
Single $575.30 $607.61 $32.31 5.62%
Double $1,150.60 $1,215.22 $64.62 5.62%
Emp/Child(ren) $978.01 $1,032.94 $54.93 5.62%
Family $1,639.61 $1,731.69 $92.08 5.62%
Platinum HMO New Plan IHPF5101
Single N/A $1,239.20 $0.00 0.00%
Double N/A $2,478.40 $0.00 0.00%
Emp/Child(ren) N/A $2,106.64 $0.00 0.00%
Family N/A $3,531.72 $0.00 0.00%
Platinum HMO New Plan IHPF5102
Single N/A $1,245.24 $0.00 0.00%
Double N/A $2,490.49 $0.00 0.00%
Emp/Child(ren) N/A $2,116.92 $0.00 0.00%
Family N/A $3,548.95 $0.00 0.00%
Silver HMO New Plan IHSF5101
Single N/A $809.79 $0.00 0.00%
Double N/A $1,619.59 $0.00 0.00%
Emp/Child(ren) N/A $1,376.65 $0.00 0.00%
Family N/A $2,307.91 $0.00 0.00%
Silver HMO New Plan IHSF5102
Single N/A $813.71 $0.00 0.00%
Double N/A $1,627.42 $0.00 0.00%
Emp/Child(ren) N/A $1,383.30 $0.00 0.00%
Family N/A $2,319.07 $0.00 0.00%
Platinum HMO IHPF1055 IHPF1057
Single $1,175.51 $1,273.44 $97.93 8.33%
Double $2,351.02 $2,546.88 $195.86 8.33%
Emp/Child(ren) $1,998.37 $2,164.85 $166.48 8.33%
Family $3,350.21 $3,629.31 $279.10 8.33%
Platinum HMO IHPF1056 IHPF1058
Single $1,179.40 $1,279.66 $100.26 8.50%
Double $2,358.79 $2,559.32 $200.53 8.50%
Emp/Child(ren) $2,004.97 $2,175.42 $170.45 8.50%
Family $3,361.28 $3,647.03 $285.75 8.50%
Gold HMO IHGF2045 IHGF2047
Single $1,023.02 $1,065.30 $42.28 4.13%
Double $2,046.04 $2,130.60 $84.56 4.13%
Emp/Child(ren) $1,739.13 $1,811.01 $71.88 4.13%
Family $2,915.61 $3,036.10 $120.49 4.13%
Gold HMO IHGF2046 IHGF2048
Single $1,026.39 $1,070.49 $44.10 4.30%
Double $2,052.78 $2,140.97 $88.19 4.30%
Emp/Child(ren) $1,744.86 $1,819.83 $74.97 4.30%
Family $2,925.21 $3,050.89 $125.68 4.30%
Silver HMO IHSF3074 IHSF3076
Single $827.23 $852.31 $25.08 3.03%
Double $1,654.46 $1,704.62 $50.16 3.03%
Emp/Child(ren) $1,406.29 $1,448.93 $42.64 3.03%
Family $2,357.61 $2,429.08 $71.47 3.03%
2020 Individual HMO Off Exchange Rate Manual Page 6

Capital District Physicians' Health Plan
Mid-Hudson Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Silver HMO IHSF3075 IHSF3077
Single $829.94 $856.44 $26.50 3.19%
Double $1,659.88 $1,712.88 $53.00 3.19%
Emp/Child(ren) $1,410.90 $1,455.95 $45.05 3.19%
Family $2,365.33 $2,440.86 $75.53 3.19%
Bronze HMO IHBF4059 IHBF4062
Single $588.54 $618.73 $30.19 5.13%
Double $1,177.09 $1,237.46 $60.37 5.13%
Emp/Child(ren) $1,000.53 $1,051.84 $51.31 5.13%
Family $1,677.35 $1,763.37 $86.02 5.13%
Bronze HMO IHBF4060 IHBF4063
Single $590.45 $621.69 $31.24 5.29%
Double $1,180.90 $1,243.37 $62.47 5.29%
Emp/Child(ren) $1,003.77 $1,056.87 $53.10 5.29%
Family $1,682.78 $1,771.81 $89.03 5.29%
Platinum HMO IHPFC012 IHPFC016
Single $496.66 $524.66 $28.00 5.64%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Gold HMO IHGFC013 IHGFC017
Single $433.84 $438.91 $5.07 1.17%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSFC014 IHSFC018
Single $353.17 $351.16 ($2.01) -0.57%
Double N/A N/A $0.00 $0.00
Emp/Child(ren) N/A N/A $0.00 $0.00
Family N/A N/A $0.00 $0.00
Bronze HMO IHBFC015 IHBFC019
Single $254.84 $254.92 $0.08 0.03%
Double N/A N/A $0.00 $0.00
Emp/Child(ren) N/A N/A $0.00 $0.00
Family N/A N/A $0.00 $0.00
Catastrophic HMO IHCF5007 IHCF5008
Single $353.89 $340.61 ($13.28) -3.75%
Double $707.77 $681.23 ($26.54) ($0.04)
Emp/Child(ren) $601.61 $579.04 ($22.57) ($0.04)
Family $1,008.58 $970.75 ($37.83) ($0.04)
2020 Individual HMO Off Exchange Rate Manual Page 7

Capital District Physicians' Health Plan
Syracuse Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Platinum HMO IHPF1053 IHPF1136
Single $1,022.50 $1,009.02 ($13.48) -1.32%
Double $2,044.99 $2,018.04 ($26.95) -1.32%
Emp/Child(ren) $1,738.24 $1,715.33 ($22.91) -1.32%
Family $2,914.12 $2,875.71 ($38.41) -1.32%
Platinum HMO IHPF1054 IHPF1137
Single $1,025.88 $1,013.94 ($11.94) -1.16%
Double $2,051.75 $2,027.87 ($23.88) -1.16%
Emp/Child(ren) $1,743.99 $1,723.69 ($20.30) -1.16%
Family $2,923.75 $2,889.72 ($34.03) -1.16%
Gold HMO IHGF2043 IHGF2135
Single $834.50 $859.26 $24.76 2.97%
Double $1,669.00 $1,718.51 $49.51 2.97%
Emp/Child(ren) $1,418.65 $1,460.74 $42.09 2.97%
Family $2,378.32 $2,448.88 $70.56 2.97%
Gold HMO IHGF2044 IHGF2136
Single $837.24 $863.44 $26.20 3.13%
Double $1,674.49 $1,726.87 $52.38 3.13%
Emp/Child(ren) $1,423.31 $1,467.84 $44.53 3.13%
Family $2,386.14 $2,460.79 $74.65 3.13%
Silver HMO IHSF3068 IHSF3280
Single $675.40 $666.67 ($8.73) -1.29%
Double $1,350.80 $1,333.35 ($17.45) -1.29%
Emp/Child(ren) $1,148.18 $1,133.34 ($14.84) -1.29%
Family $1,924.89 $1,900.02 ($24.87) -1.29%
Silver HMO IHSF3069 IHSF3281
Single $677.61 $669.89 ($7.72) -1.14%
Double $1,355.21 $1,339.78 ($15.43) -1.14%
Emp/Child(ren) $1,151.93 $1,138.81 ($13.12) -1.14%
Family $1,931.17 $1,909.19 ($21.98) -1.14%
Silver HMO IHSF3072 IHSF3288
Single $646.82 $645.52 ($1.30) -0.20%
Double $1,293.65 $1,291.05 ($2.60) -0.20%
Emp/Child(ren) $1,099.60 $1,097.39 ($2.21) -0.20%
Family $1,843.45 $1,839.74 ($3.71) -0.20%
Silver HMO IHSF3073 IHSF3289
Single $648.95 $648.65 ($0.30) -0.05%
Double $1,297.89 $1,297.30 ($0.59) -0.05%
Emp/Child(ren) $1,103.21 $1,102.71 ($0.50) -0.05%
Family $1,849.49 $1,848.65 ($0.84) -0.05%
Bronze HMO IHBF4061 IHBF4149
Single $486.35 $484.14 ($2.21) -0.45%
Double $972.69 $968.27 ($4.42) -0.45%
Emp/Child(ren) $826.79 $823.03 ($3.76) -0.45%
Family $1,386.09 $1,379.79 ($6.30) -0.45%
Bronze HMO IHBF4056 IHBF4150
Single $487.92 $486.46 ($1.46) -0.30%
Double $975.83 $972.92 ($2.91) -0.30%
Emp/Child(ren) $829.46 $826.98 ($2.48) -0.30%
Family $1,390.56 $1,386.41 ($4.15) -0.30%
Bronze HMO IHBF4057 IHBF4151
Single $479.60 $479.31 ($0.29) -0.06%
Double $959.20 $958.62 ($0.58) -0.06%
Emp/Child(ren) $815.32 $814.83 ($0.49) -0.06%
Family $1,366.85 $1,366.04 ($0.81) -0.06%
2020 Individual HMO Off Exchange Rate Manual Page 8

Capital District Physicians' Health Plan
Syracuse Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBF4058 IHBF4152
Single $481.16 $481.60 $0.44 0.09%
Double $962.31 $963.20 $0.89 0.09%
Emp/Child(ren) $817.97 $818.72 $0.75 0.09%
Family $1,371.29 $1,372.56 $1.27 0.09%
Platinum HMO New Plan IHPF5101
Single N/A $982.21 $0.00 0.00%
Double N/A $1,964.42 $0.00 0.00%
Emp/Child(ren) N/A $1,669.75 $0.00 0.00%
Family N/A $2,799.29 $0.00 0.00%
Platinum HMO New Plan IHPF5102
Single N/A $987.00 $0.00 0.00%
Double N/A $1,974.00 $0.00 0.00%
Emp/Child(ren) N/A $1,677.90 $0.00 0.00%
Family N/A $2,812.95 $0.00 0.00%
Silver HMO New Plan IHSF5101
Single N/A $641.85 $0.00 0.00%
Double N/A $1,283.71 $0.00 0.00%
Emp/Child(ren) N/A $1,091.15 $0.00 0.00%
Family N/A $1,829.28 $0.00 0.00%
Silver HMO New Plan IHSF5102
Single N/A $644.96 $0.00 0.00%
Double N/A $1,289.92 $0.00 0.00%
Emp/Child(ren) N/A $1,096.43 $0.00 0.00%
Family N/A $1,838.13 $0.00 0.00%
Platinum HMO IHPF1055 IHPF1057
Single $983.14 $1,009.35 $26.21 2.67%
Double $1,966.29 $2,018.70 $52.41 2.67%
Emp/Child(ren) $1,671.35 $1,715.89 $44.54 2.66%
Family $2,801.96 $2,876.64 $74.68 2.67%
Platinum HMO IHPF1056 IHPF1058
Single $986.39 $1,014.28 $27.89 2.83%
Double $1,972.79 $2,028.55 $55.76 2.83%
Emp/Child(ren) $1,676.87 $1,724.27 $47.40 2.83%
Family $2,811.22 $2,890.69 $79.47 2.83%
Gold HMO IHGF2045 IHGF2047
Single $855.61 $844.37 ($11.24) -1.31%
Double $1,711.21 $1,688.74 ($22.47) -1.31%
Emp/Child(ren) $1,454.53 $1,435.43 ($19.10) -1.31%
Family $2,438.48 $2,406.46 ($32.02) -1.31%
Gold HMO IHGF2046 IHGF2048
Single $858.42 $848.48 ($9.94) -1.16%
Double $1,716.85 $1,696.97 ($19.88) -1.16%
Emp/Child(ren) $1,459.32 $1,442.42 ($16.90) -1.16%
Family $2,446.51 $2,418.18 ($28.33) -1.16%
Silver HMO IHSF3074 IHSF3076
Single $691.86 $675.55 ($16.31) -2.36%
Double $1,383.71 $1,351.11 ($32.60) -2.36%
Emp/Child(ren) $1,176.16 $1,148.44 ($27.72) -2.36%
Family $1,971.79 $1,925.33 ($46.46) -2.36%
2020 Individual HMO Off Exchange Rate Manual Page 9

Capital District Physicians' Health Plan
Syracuse Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Silver HMO IHSF3075 IHSF3077
Single $694.12 $678.83 ($15.29) -2.20%
Double $1,388.25 $1,357.66 ($30.59) -2.20%
Emp/Child(ren) $1,180.01 $1,154.01 ($26.00) -2.20%
Family $1,978.25 $1,934.66 ($43.59) -2.20%
Bronze HMO IHBF4059 IHBF4062
Single $492.23 $490.41 ($1.82) -0.37%
Double $984.46 $980.83 ($3.63) -0.37%
Emp/Child(ren) $836.79 $833.70 ($3.09) -0.37%
Family $1,402.86 $1,397.68 ($5.18) -0.37%
Bronze HMO IHBF4060 IHBF4063
Single $493.83 $492.76 ($1.07) -0.22%
Double $987.65 $985.52 ($2.13) -0.22%
Emp/Child(ren) $839.50 $837.69 ($1.81) -0.22%
Family $1,407.40 $1,404.36 ($3.04) -0.22%
Platinum HMO IHPFC012 IHPFC016
Single $415.39 $415.85 $0.46 0.11%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Gold HMO IHGFC013 IHGFC017
Single $362.85 $347.89 ($14.96) -4.12%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSFC014 IHSFC018
Single $295.37 $278.33 ($17.04) -5.77%
Double N/A N/A $0.00 $0.00
Emp/Child(ren) N/A N/A $0.00 $0.00
Family N/A N/A $0.00 $0.00
Bronze HMO IHBFC015 IHBFC019
Single $213.13 $202.05 ($11.08) -5.20%
Double N/A N/A $0.00 $0.00
Emp/Child(ren) N/A N/A $0.00 $0.00
Family N/A N/A $0.00 $0.00
Catastrophic HMO IHCF5007 IHCF5008
Single $295.97 $269.97 ($26.00) -8.78%
Double $591.95 $539.95 ($52.00) ($0.09)
Emp/Child(ren) $503.16 $458.96 ($44.20) ($0.09)
Family $843.53 $769.43 ($74.10) ($0.09)
2020 Individual HMO Off Exchange Rate Manual Page 10

Capital District Physicians' Health Plan
UticaWatertown Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Platinum HMO IHPF1053 IHPF1136
Single $1,005.03 $996.81 ($8.22) -0.82%
Double $2,010.06 $1,993.62 ($16.44) -0.82%
Emp/Child(ren) $1,708.55 $1,694.58 ($13.97) -0.82%
Family $2,864.34 $2,840.91 ($23.43) -0.82%
Platinum HMO IHPF1054 IHPF1137
Single $1,008.35 $1,001.67 ($6.68) -0.66%
Double $2,016.71 $2,003.34 ($13.37) -0.66%
Emp/Child(ren) $1,714.20 $1,702.84 ($11.36) -0.66%
Family $2,873.81 $2,854.75 ($19.06) -0.66%
Gold HMO IHGF2043 IHGF2135
Single $820.24 $848.86 $28.62 3.49%
Double $1,640.49 $1,697.72 $57.23 3.49%
Emp/Child(ren) $1,394.42 $1,443.06 $48.64 3.49%
Family $2,337.70 $2,419.25 $81.55 3.49%
Gold HMO IHGF2044 IHGF2136
Single $822.94 $852.99 $30.05 3.65%
Double $1,645.88 $1,705.98 $60.10 3.65%
Emp/Child(ren) $1,399.00 $1,450.08 $51.08 3.65%
Family $2,345.39 $2,431.02 $85.63 3.65%
Silver HMO IHSF3068 IHSF3280
Single $663.86 $658.61 ($5.25) -0.79%
Double $1,327.73 $1,317.21 ($10.52) -0.79%
Emp/Child(ren) $1,128.57 $1,119.63 ($8.94) -0.79%
Family $1,892.01 $1,877.03 ($14.98) -0.79%
Silver HMO IHSF3069 IHSF3281
Single $666.03 $661.78 ($4.25) -0.64%
Double $1,332.06 $1,323.57 ($8.49) -0.64%
Emp/Child(ren) $1,132.25 $1,125.03 ($7.22) -0.64%
Family $1,898.19 $1,886.08 ($12.11) -0.64%
Silver HMO IHSF3072 IHSF3288
Single $635.78 $637.71 $1.93 0.30%
Double $1,271.55 $1,275.43 $3.88 0.31%
Emp/Child(ren) $1,080.82 $1,084.11 $3.29 0.30%
Family $1,811.96 $1,817.48 $5.52 0.30%
Silver HMO IHSF3073 IHSF3289
Single $637.86 $640.80 $2.94 0.46%
Double $1,275.72 $1,281.60 $5.88 0.46%
Emp/Child(ren) $1,084.36 $1,089.36 $5.00 0.46%
Family $1,817.90 $1,826.28 $8.38 0.46%
Bronze HMO IHBF4061 IHBF4149
Single $478.04 $478.28 $0.24 0.05%
Double $956.08 $956.56 $0.48 0.05%
Emp/Child(ren) $812.67 $813.07 $0.40 0.05%
Family $1,362.41 $1,363.10 $0.69 0.05%
Bronze HMO IHBF4056 IHBF4150
Single $479.58 $480.57 $0.99 0.21%
Double $959.16 $961.15 $1.99 0.21%
Emp/Child(ren) $815.29 $816.97 $1.68 0.21%
Family $1,366.81 $1,369.63 $2.82 0.21%
Bronze HMO IHBF4057 IHBF4151
Single $471.41 $473.51 $2.10 0.45%
Double $942.81 $947.02 $4.21 0.45%
Emp/Child(ren) $801.39 $804.97 $3.58 0.45%
Family $1,343.51 $1,349.51 $6.00 0.45%
2020 Individual HMO Off Exchange Rate Manual Page 11

Capital District Physicians' Health Plan
UticaWatertown Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBF4058 IHBF4152
Single $472.94 $475.77 $2.83 0.60%
Double $945.87 $951.54 $5.67 0.60%
Emp/Child(ren) $803.99 $808.81 $4.82 0.60%
Family $1,347.87 $1,355.95 $8.08 0.60%
Platinum HMO New Plan IHPF5101
Single N/A $970.32 $0.00 0.00%
Double N/A $1,940.65 $0.00 0.00%
Emp/Child(ren) N/A $1,649.55 $0.00 0.00%
Family N/A $2,765.42 $0.00 0.00%
Platinum HMO New Plan IHPF5102
Single N/A $975.06 $0.00 0.00%
Double N/A $1,950.11 $0.00 0.00%
Emp/Child(ren) N/A $1,657.60 $0.00 0.00%
Family N/A $2,778.91 $0.00 0.00%
Silver HMO New Plan IHSF5101
Single N/A $634.09 $0.00 0.00%
Double N/A $1,268.17 $0.00 0.00%
Emp/Child(ren) N/A $1,077.95 $0.00 0.00%
Family N/A $1,807.15 $0.00 0.00%
Silver HMO New Plan IHSF5102
Single N/A $637.15 $0.00 0.00%
Double N/A $1,274.31 $0.00 0.00%
Emp/Child(ren) N/A $1,083.16 $0.00 0.00%
Family N/A $1,815.89 $0.00 0.00%
Platinum HMO IHPF1055 IHPF1057
Single $966.35 $997.14 $30.79 3.19%
Double $1,932.70 $1,994.27 $61.57 3.19%
Emp/Child(ren) $1,642.80 $1,695.13 $52.33 3.19%
Family $2,754.10 $2,841.84 $87.74 3.19%
Platinum HMO IHPF1056 IHPF1058
Single $969.54 $1,002.00 $32.46 3.35%
Double $1,939.09 $2,004.01 $64.92 3.35%
Emp/Child(ren) $1,648.23 $1,703.41 $55.18 3.35%
Family $2,763.20 $2,855.71 $92.51 3.35%
Gold HMO IHGF2045 IHGF2047
Single $840.99 $834.15 ($6.84) -0.81%
Double $1,681.98 $1,668.31 ($13.67) -0.81%
Emp/Child(ren) $1,429.69 $1,418.06 ($11.63) -0.81%
Family $2,396.83 $2,377.34 ($19.49) -0.81%
Gold HMO IHGF2046 IHGF2048
Single $843.76 $838.22 ($5.54) -0.66%
Double $1,687.52 $1,676.43 ($11.09) -0.66%
Emp/Child(ren) $1,434.39 $1,424.97 ($9.42) -0.66%
Family $2,404.72 $2,388.92 ($15.80) -0.66%
Silver HMO IHSF3074 IHSF3076
Single $680.04 $667.38 ($12.66) -1.86%
Double $1,360.08 $1,334.76 ($25.32) -1.86%
Emp/Child(ren) $1,156.07 $1,134.55 ($21.52) -1.86%
Family $1,938.11 $1,902.03 ($36.08) -1.86%
2020 Individual HMO Off Exchange Rate Manual Page 12

Capital District Physicians' Health Plan
UticaWatertown Region
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Silver HMO IHSF3075 IHSF3077
Single $682.27 $670.61 ($11.66) -1.71%
Double $1,364.53 $1,341.23 ($23.30) -1.71%
Emp/Child(ren) $1,159.85 $1,140.04 ($19.81) -1.71%
Family $1,944.46 $1,911.25 ($33.21) -1.71%
Bronze HMO IHBF4059 IHBF4062
Single $483.82 $484.48 $0.66 0.14%
Double $967.65 $968.96 $1.31 0.14%
Emp/Child(ren) $822.50 $823.61 $1.11 0.13%
Family $1,378.90 $1,380.76 $1.86 0.13%
Bronze HMO IHBF4060 IHBF4063
Single $485.39 $486.80 $1.41 0.29%
Double $970.78 $973.59 $2.81 0.29%
Emp/Child(ren) $825.16 $827.55 $2.39 0.29%
Family $1,383.36 $1,387.37 $4.01 0.29%
Platinum HMO IHPFC012 IHPFC016
Single $408.29 $410.82 $2.53 0.62%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Gold HMO IHGFC013 IHGFC017
Single $356.65 $343.68 ($12.97) -3.64%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSFC014 IHSFC018
Single $290.33 $274.97 ($15.36) -5.29%
Double N/A N/A $0.00 $0.00
Emp/Child(ren) N/A N/A $0.00 $0.00
Family N/A N/A $0.00 $0.00
Bronze HMO IHBFC015 IHBFC019
Single $209.49 $199.61 ($9.88) -4.72%
Double N/A N/A $0.00 $0.00
Emp/Child(ren) N/A N/A $0.00 $0.00
Family N/A N/A $0.00 $0.00
Catastrophic HMO IHCF5007 IHCF5008
Single $290.92 $266.71 ($24.21) -8.32%
Double $581.84 $533.42 ($48.42) ($0.08)
Emp/Child(ren) $494.56 $453.40 ($41.16) ($0.08)
Family $829.12 $760.12 ($69.00) ($0.08)
2020 Individual HMO Off Exchange Rate Manual Page 13

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 J R S T V W X Y Z AA AB ac
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code
2020 Plan
Code Standard?AV OV SP INN HOSP OUT SURG ER AMB DME
URGENT
CAREDIABETIC PT/OT/ST
01-0002-2020 Ind HMO Platinum 94788NY0280129-00 IHPF1053 IHPF1136 Non-Standard 88.5% 15 20 10% 0.1 10% 10% 0.5 30 15 20
01-0002-2020 Ind HMO Platinum 94788NY0280130-00 IHPF1054 IHPF1137 Non-Standard 88.5% 15 20 10% 0.1 10% 10% 0.5 30 15 20
01-0002-2020 Ind HMO Gold 94788NY0280131-00 IHGF2043 IHGF2135 Non-Standard 82.0% 20 40 20% 20% 20% 20% 0.5 50 20 40
01-0002-2020 Ind HMO Gold 94788NY0280132-00 IHGF2044 IHGF2136 Non-Standard 82.0% 20 40 20% 20% 20% 20% 0.5 50 20 40
01-0002-2020 Ind HMO Silver 94788NY0280021-00 IHSF3068 IHSF3280 Non-Standard 71.9% 15% 15% 15% 15% 15% 15% 0.5 0.15 15% 15%
01-0002-2020 Ind HMO Silver 94788NY0280022-00 IHSF3069 IHSF3281 Non-Standard 71.9% 15% 15% 15% 15% 15% 15% 0.5 0.15 15% 15%
01-0002-2020 Ind HMO Silver 94788NY0280017-00 IHSF3072 IHSF3288 Non-Standard 71.7%
EPC
0%/Non
EPC 10%
10% 10% 10% 10% 10% 0.5 0.1 0.1 10%
01-0002-2020 Ind HMO Silver 94788NY0280018-00 IHSF3073 IHSF3289 Non-Standard 71.7%
EPC
0%/Non
EPC 10%
10% 10% 10% 10% 10% 0.5 0.1 0.1 10%
01-0002-2020 Ind HMO Bronze 94788NY0280029-00 IHBF4061 IHBF4149 Non-Standard 63.1% 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2
01-0002-2020 Ind HMO Bronze 94788NY0280030-00 IHBF4056 IHBF4150 Non-Standard 63.1% 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2
01-0002-2020 Ind HMO Bronze 94788NY0280145-00 IHBF4057 IHBF4151 Non-Standard 62.5% 0 0 0 0 0 0 0 0 0 0
01-0002-2020 Ind HMO Bronze 94788NY0280146-00 IHBF4058 IHBF4152 Non-Standard 62.5% 0 0 0 0 0 0 0 0 0 0
01-0001-2020 Ind HMO Platinum 94788NY0280147-00 New Plan IHPF5101 Non-Standard 87.7% 0 25 250 100 200 200 0.5 40 0 25
01-0001-2020 Ind HMO Platinum 94788NY0280148-00 New Plan IHPF5102 Non-Standard 87.7% 0 25 250 100 200 200 0.5 40 0 25
01-0001-2020 Ind HMO Silver 94788NY0280149-00 New Plan IHSF5101 Non-Standard 68.5% 25 50 1500 200 500 500 0.5 60 25 50
01-0001-2020 Ind HMO Silver 94788NY0280150-00 New Plan IHSF5102 Non-Standard 68.5% 25 50 1500 200 500 500 0.5 60 25 50
Page 142013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 J R S T V W X Y Z AA AB ac
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code
2020 Plan
Code Standard?AV OV SP INN HOSP OUT SURG ER AMB DME
URGENT
CAREDIABETIC PT/OT/ST
01-0002-2020 Ind HMO Platinum 94788NY0280053-00 IHPF1055 IHPF1057 Standard 88.7% 15 35 500 100 100 100 10% 55 15 25
01-0002-2020 Ind HMO Platinum 94788NY0280064-00 IHPF1056 IHPF1058 Standard 88.7% 15 35 500 100 100 100 10% 55 15 25
01-0002-2020 Ind HMO Gold 94788NY0280054-00 IHGF2045 IHGF2047 Standard 80.9% 25 40 1000 100 150 150 20% 60 25 30
01-0002-2020 Ind HMO Gold 94788NY0280065-00 IHGF2046 IHGF2048 Standard 80.9% 25 40 1000 100 150 150 20% 60 25 30
01-0002-2020 Ind HMO Silver 94788NY0280055-00 IHSF3074 IHSF3076 Standard 72.0% 30 50 1500 150 250 150 30% 70 30 30
01-0002-2020 Ind HMO Silver 94788NY0280066-00 IHSF3075 IHSF3077 Standard 72.0% 30 50 1500 150 250 150 30% 70 30 30
01-0002-2020 Ind HMO Bronze 94788NY0280059-00 IHBF4059 IHBF4062 Standard 63.4% 50% 50% 50% 50% 50% 50% 50% 0.5 50% 50%
01-0002-2020 Ind HMO Bronze 94788NY0280070-00 IHBF4060 IHBF4063 Standard 63.4% 50% 50% 50% 50% 50% 50% 50% 0.5 50% 50%
01-0017-2020 Ind HMO Platinum 94788NY0280081-00 IHPFC012 IHPFC016 Standard 88.7% 15 35 500 100 100 100 10% 55 15 25
01-0017-2020 Ind HMO Gold 94788NY0280080-00 IHGFC013 IHGFC017 Standard 80.9% 25 40 1000 100 150 150 20% 60 25 30
01-0017-2020 Ind HMO Silver 94788NY0280082-00 IHSFC014 IHSFC018 Standard 72.0% 30 50 1500 150 250 150 30% 70 30 30
01-0017-2020 Ind HMO Bronze 94788NY0280079-00 IHBFC015 IHBFC019 Standard 63.4% 50% 50% 50% 50% 50% 50% 50% 0.5 50% 50%
01-0007-2020 Ind HMO Catastrophic 94788NY0280047-00 IHCF5007 IHCF5008 Standard 61.1% 0 0 0 0 0 0 0 0 0 0
Page 152013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code
2020 Plan
Code Standard?
01-0002-2020 Ind HMO Platinum 94788NY0280129-00 IHPF1053 IHPF1136 Non-Standard
01-0002-2020 Ind HMO Platinum 94788NY0280130-00 IHPF1054 IHPF1137 Non-Standard
01-0002-2020 Ind HMO Gold 94788NY0280131-00 IHGF2043 IHGF2135 Non-Standard
01-0002-2020 Ind HMO Gold 94788NY0280132-00 IHGF2044 IHGF2136 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280021-00 IHSF3068 IHSF3280 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280022-00 IHSF3069 IHSF3281 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280017-00 IHSF3072 IHSF3288 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280018-00 IHSF3073 IHSF3289 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280029-00 IHBF4061 IHBF4149 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280030-00 IHBF4056 IHBF4150 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280145-00 IHBF4057 IHBF4151 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280146-00 IHBF4058 IHBF4152 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280147-00 New Plan IHPF5101 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280148-00 New Plan IHPF5102 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280149-00 New Plan IHSF5101 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280150-00 New Plan IHSF5102 Non-Standard
AG AH AI AJ AP AQ AR AS
COIN INN Ded Single INN Ded Family INN Max SingleOON Max
Family
Aggregate/
EmbeddedProduct Line Benefit Type
0.1 200 400 7350 N/A Embedded HMO Transitional
0.1 200 400 7350 N/A Embedded HMO Transitional
0.2 750 1500 6500 N/A Embedded HMO Transitional
0.2 750 1500 6500 N/A Embedded HMO Transitional
0.2 2500 5000 5500 N/A Aggregate HMO Transitional
0.2 2500 5000 5500 N/A Aggregate HMO Transitional
0.2 4000 8000 7900 N/A Embedded HMO Transitional
0.2 4000 8000 7900 N/A Embedded HMO Transitional
0.2 5500 11000 6750 N/A Aggregate HMO Transitional
0.2 5500 11000 6750 N/A Aggregate HMO Transitional
0.2 6750 13500 6750 N/A Embedded HMO Transitional
0.2 6750 13500 6750 N/A Embedded HMO Transitional
0 0 0 3000 N/A Embedded HMO Copayment
0 0 0 3000 N/A Embedded HMO Copayment
0 2200 4400 6750 N/A Aggregate HDHMOQualified High
Deductible
0 2200 4400 6750 N/A Aggregate HDHMOQualified High
Deductible
Page 162013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code
2020 Plan
Code Standard?
01-0002-2020 Ind HMO Platinum 94788NY0280053-00 IHPF1055 IHPF1057 Standard
01-0002-2020 Ind HMO Platinum 94788NY0280064-00 IHPF1056 IHPF1058 Standard
01-0002-2020 Ind HMO Gold 94788NY0280054-00 IHGF2045 IHGF2047 Standard
01-0002-2020 Ind HMO Gold 94788NY0280065-00 IHGF2046 IHGF2048 Standard
01-0002-2020 Ind HMO Silver 94788NY0280055-00 IHSF3074 IHSF3076 Standard
01-0002-2020 Ind HMO Silver 94788NY0280066-00 IHSF3075 IHSF3077 Standard
01-0002-2020 Ind HMO Bronze 94788NY0280059-00 IHBF4059 IHBF4062 Standard
01-0002-2020 Ind HMO Bronze 94788NY0280070-00 IHBF4060 IHBF4063 Standard
01-0017-2020 Ind HMO Platinum 94788NY0280081-00 IHPFC012 IHPFC016 Standard
01-0017-2020 Ind HMO Gold 94788NY0280080-00 IHGFC013 IHGFC017 Standard
01-0017-2020 Ind HMO Silver 94788NY0280082-00 IHSFC014 IHSFC018 Standard
01-0017-2020 Ind HMO Bronze 94788NY0280079-00 IHBFC015 IHBFC019 Standard
01-0007-2020 Ind HMO Catastrophic 94788NY0280047-00 IHCF5007 IHCF5008 Standard
AG AH AI AJ AP AQ AR AS
COIN INN Ded Single INN Ded Family INN Max SingleOON Max
Family
Aggregate/
EmbeddedProduct Line Benefit Type
0 0 0 2000 N/A Embedded HMO Copayment
0 0 0 2000 N/A Embedded HMO Copayment
0 600 1200 4000 N/A Embedded HMO Copayment
0 600 1200 4000 N/A Embedded HMO Copayment
0 1300 2600 7900 N/A Embedded HMO Copayment
0 1300 2600 7900 N/A Embedded HMO Copayment
0.5 5500 11000 6550 N/A Embedded HDHMOQualified High
Deductible
0.5 5500 11000 6550 N/A Embedded HDHMOQualified High
Deductible
0 0 0 2000 N/A Embedded HMO Copayment
0 600 1200 4000 N/A Embedded HMO Copayment
0 1300 2600 7900 N/A Embedded HMO Copayment
0.5 5500 11000 6550 N/A Embedded HDHMOQualified High
Deductible
0 8150 16300 8150 N/A Embedded HMONon Qualified High
Deductible
Page 172013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code
2020 Plan
Code Standard?
01-0002-2020 Ind HMO Platinum 94788NY0280129-00 IHPF1053 IHPF1136 Non-Standard
01-0002-2020 Ind HMO Platinum 94788NY0280130-00 IHPF1054 IHPF1137 Non-Standard
01-0002-2020 Ind HMO Gold 94788NY0280131-00 IHGF2043 IHGF2135 Non-Standard
01-0002-2020 Ind HMO Gold 94788NY0280132-00 IHGF2044 IHGF2136 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280021-00 IHSF3068 IHSF3280 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280022-00 IHSF3069 IHSF3281 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280017-00 IHSF3072 IHSF3288 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280018-00 IHSF3073 IHSF3289 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280029-00 IHBF4061 IHBF4149 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280030-00 IHBF4056 IHBF4150 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280145-00 IHBF4057 IHBF4151 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280146-00 IHBF4058 IHBF4152 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280147-00 New Plan IHPF5101 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280148-00 New Plan IHPF5102 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280149-00 New Plan IHSF5101 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280150-00 New Plan IHSF5102 Non-Standard
AT AU AV AW AX
Rx Benefit Riders Additional Benefits Additional Benefits Additional Benefits
$1/10%/40% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$1/10%/40% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$1/20%/50% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$1/20%/50% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$4/50%/50% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$4/50%/50% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$4/30%/50% (Tier 1 not subject to deductible) No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$4/30%/50% (Tier 1 not subject to deductible) Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
50%/50%/50% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
50%/50%/50% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$0/$0/$0 No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$0/$0/$0 Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$5/$15/$45 No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$5/$15/$45 Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$10/$50/$80 No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
$10/$50/$80 Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
Page 182013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code
2020 Plan
Code Standard?
01-0002-2020 Ind HMO Platinum 94788NY0280053-00 IHPF1055 IHPF1057 Standard
01-0002-2020 Ind HMO Platinum 94788NY0280064-00 IHPF1056 IHPF1058 Standard
01-0002-2020 Ind HMO Gold 94788NY0280054-00 IHGF2045 IHGF2047 Standard
01-0002-2020 Ind HMO Gold 94788NY0280065-00 IHGF2046 IHGF2048 Standard
01-0002-2020 Ind HMO Silver 94788NY0280055-00 IHSF3074 IHSF3076 Standard
01-0002-2020 Ind HMO Silver 94788NY0280066-00 IHSF3075 IHSF3077 Standard
01-0002-2020 Ind HMO Bronze 94788NY0280059-00 IHBF4059 IHBF4062 Standard
01-0002-2020 Ind HMO Bronze 94788NY0280070-00 IHBF4060 IHBF4063 Standard
01-0017-2020 Ind HMO Platinum 94788NY0280081-00 IHPFC012 IHPFC016 Standard
01-0017-2020 Ind HMO Gold 94788NY0280080-00 IHGFC013 IHGFC017 Standard
01-0017-2020 Ind HMO Silver 94788NY0280082-00 IHSFC014 IHSFC018 Standard
01-0017-2020 Ind HMO Bronze 94788NY0280079-00 IHBFC015 IHBFC019 Standard
01-0007-2020 Ind HMO Catastrophic 94788NY0280047-00 IHCF5007 IHCF5008 Standard
AT AU AV AW AX
Rx Benefit Riders Additional Benefits Additional Benefits Additional Benefits
$10/$30/$60 No Riders No Riders No Riders No Riders
$10/$30/$60 Age 29 No Riders No Riders No Riders
$10/$35/$70 No Riders No Riders No Riders No Riders
$10/$35/$70 Age 29 No Riders No Riders No Riders
$10/$35/$70 No Riders No Riders No Riders No Riders
$10/$35/$70 Age 29 No Riders No Riders No Riders
$10/$35/$70 No Riders No Riders No Riders No Riders
$10/$35/$70 Age 29 No Riders No Riders No Riders
$10/$30/$60 No Riders No Riders No Riders No Riders
$10/$35/$70 No Riders No Riders No Riders No Riders
$10/$35/$70 No Riders No Riders No Riders No Riders
$10/$35/$70 No Riders No Riders No Riders No Riders
$0/$0/$0 No Riders No Riders No Riders No Riders
Page 192013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code
2020 Plan
Code Standard?
01-0002-2020 Ind HMO Platinum 94788NY0280129-00 IHPF1053 IHPF1136 Non-Standard
01-0002-2020 Ind HMO Platinum 94788NY0280130-00 IHPF1054 IHPF1137 Non-Standard
01-0002-2020 Ind HMO Gold 94788NY0280131-00 IHGF2043 IHGF2135 Non-Standard
01-0002-2020 Ind HMO Gold 94788NY0280132-00 IHGF2044 IHGF2136 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280021-00 IHSF3068 IHSF3280 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280022-00 IHSF3069 IHSF3281 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280017-00 IHSF3072 IHSF3288 Non-Standard
01-0002-2020 Ind HMO Silver 94788NY0280018-00 IHSF3073 IHSF3289 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280029-00 IHBF4061 IHBF4149 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280030-00 IHBF4056 IHBF4150 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280145-00 IHBF4057 IHBF4151 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280146-00 IHBF4058 IHBF4152 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280147-00 New Plan IHPF5101 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280148-00 New Plan IHPF5102 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280149-00 New Plan IHSF5101 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280150-00 New Plan IHSF5102 Non-Standard
Ay
Additional non EHB Benefits Additional non EHB Benefits
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Lasik Surgery ($750 Max) Gym Membership
Page 202013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO Off Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code
2020 Plan
Code Standard?
01-0002-2020 Ind HMO Platinum 94788NY0280053-00 IHPF1055 IHPF1057 Standard
01-0002-2020 Ind HMO Platinum 94788NY0280064-00 IHPF1056 IHPF1058 Standard
01-0002-2020 Ind HMO Gold 94788NY0280054-00 IHGF2045 IHGF2047 Standard
01-0002-2020 Ind HMO Gold 94788NY0280065-00 IHGF2046 IHGF2048 Standard
01-0002-2020 Ind HMO Silver 94788NY0280055-00 IHSF3074 IHSF3076 Standard
01-0002-2020 Ind HMO Silver 94788NY0280066-00 IHSF3075 IHSF3077 Standard
01-0002-2020 Ind HMO Bronze 94788NY0280059-00 IHBF4059 IHBF4062 Standard
01-0002-2020 Ind HMO Bronze 94788NY0280070-00 IHBF4060 IHBF4063 Standard
01-0017-2020 Ind HMO Platinum 94788NY0280081-00 IHPFC012 IHPFC016 Standard
01-0017-2020 Ind HMO Gold 94788NY0280080-00 IHGFC013 IHGFC017 Standard
01-0017-2020 Ind HMO Silver 94788NY0280082-00 IHSFC014 IHSFC018 Standard
01-0017-2020 Ind HMO Bronze 94788NY0280079-00 IHBFC015 IHBFC019 Standard
01-0007-2020 Ind HMO Catastrophic 94788NY0280047-00 IHCF5007 IHCF5008 Standard
Ay
Additional non EHB Benefits Additional non EHB Benefits
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
Page 212013 UBI SG Base Medical

Exhibit C
Capital District Physicians' Health Plan
Individual
Conversion Factor Summary - 4-tier only
IV. Conversion Factor
Average Weighted Desired Weighted
Contract Contract Contract Loading Loading Conversion
Mix Size Size Factors Factors Factor
Four Tier Premiums
Single 68.6% 1.00 0.686 1.000 0.686
Double 21.8% 2.00 0.436 2.000 0.436
Emp/Child(ren) 2.9% 2.55 0.074 1.700 0.050
Family 6.7% 3.80 0.255 2.850 0.191
Total 4T 100.0% 1.451 1.362
1.065
2019 Filed 1.081
Page 22

V. Area Factors
2020 Rating Factors
Rating Region
Region 1
(Albany Area)
Region 3
(Mid-Hudson Area)
Region 6
(Syracuse Area)
Region 7
(Utica/Watertown
Area)
Regional Rating Factor 0.9686 1.3843 1.0972 1.0839
Normalized to Albany Area 1.0000 1.4292 1.1328 1.1191
Counties: Albany Delaware Broome Chenango
Columbia Dutchess Tioga Clinton
Fulton Orange Essex
Greene Ulster Franklin
Montgomery Hamilton
Rensselaer Herkimer
Saratoga Madison
Schenectady Oneida
Schoharie Otsego
Warren
Washington
Capital District Physicians' Health Plan
HMO Products
Regional Area Factors
EXEMPTION FROM FOIL REQUESTED
Page 23

VI. Tier Factors
2020 Rating Factors
Rating Method Contract Type Small Group
4-Tier Individual 1
Employee + Spouse 2.00
Employee + Child(ren) 1.70
Family 2.85
Capital District Physicians' Health Plan
HMO Product
Tier Factors
Page 24

VI. Rate Calculation
Plan Code Single Double Emp/Child(ren) Family
IHPF1136 $890.75 1,781.50$ 1,514.28$ 2,538.64$
Final Rates $890.75 $1,781.50 $1,514.28 $2,538.64
Capital District Physicians' Health Plan
Individual HMO Product
Sample Rate Calculation
Sample rate calculation for a individual on exchange benefit package in the Albany region
Page 25

Capital District Physicians' Health Plan
HMO Product
Expected Loss Ratio
All policy forms in all regions
VIII. Expected Loss Ratio
86.4%
Page 26

Capital District Physicians' Health Plan
Individual HMO Product
Broker Commissions
Page 27

Base Plan Base Plan Variation Adjustment
Characteristic Factor Characteristic FactorWithout Through Age 29 Coverage 1.000 With Through Age 29 Coverage 1.0050
With Family Planning Coverage 1.000 Without Family Planning Coverage 0.9924
With Domestic Partner Coverage 1.000 Without Domestic Partner Coverage 1.0000
Without Pediatric Dental Coverage 1.000 With Pediatric Dental Coverage N/A
Capital District Physicians' Health Plan
HMO Product
Factors for Base Plan Variations
Page 28

Capital District Physicians' Health Plan2020 Premium Rate Filing
Individual HMO On Exchange
TABLE OF CONTENTS
Table of Contents 1
I. Rate Pages
Individual
Albany Region 2-5
Mid-Hudson Region 6-9
Syracuse Region 10-13
Utica/Watertown Region 14-17
II. Benefit Summary 18-23
III. Conversion Factor 24
IV. Region Factors 25
V. Tier Factors 26
VI. Rate Calculation 27
VIII. Expected Loss Ratio 28
IX. Commission Schedule 29
X. Factors for Base Plan Variations 30
1

Capital District Physicians' Health Plan
Albany Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Platinum HMO IHPX1034 IHPX1136
Single $853.03 $890.75 $37.72 4.42%
Double $1,706.06 $1,781.50 $75.44 4.42%
Emp/Child(ren) $1,450.15 $1,514.28 $64.13 4.42%
Family $2,431.14 $2,538.64 $107.50 4.42%
Platinum HMO IHPX1035 IHPX1137
Single $855.85 $895.09 $39.24 4.58%
Double $1,711.70 $1,790.18 $78.48 4.58%
Emp/Child(ren) $1,454.95 $1,521.65 $66.70 4.58%
Family $2,439.17 $2,551.01 $111.84 4.59%
Gold HMO IHGX2035 IHGX2135
Single $696.19 $758.54 $62.35 8.96%
Double $1,392.38 $1,517.08 $124.70 8.96%
Emp/Child(ren) $1,183.52 $1,289.52 $106.00 8.96%
Family $1,984.14 $2,161.84 $177.70 8.96%
Gold HMO IHGX2036 IHGX2136
Single $698.48 $762.23 $63.75 9.13%
Double $1,396.96 $1,524.46 $127.50 9.13%
Emp/Child(ren) $1,187.42 $1,295.79 $108.37 9.13%
Family $1,990.67 $2,172.36 $181.69 9.13%
Silver HMO IHSX3180 IHSX3280
Single $563.46 $588.53 $25.07 4.45%
Double $1,126.92 $1,177.06 $50.14 4.45%
Emp/Child(ren) $957.88 $1,000.50 $42.62 4.45%
Family $1,605.86 $1,677.31 $71.45 4.45%
Silver HMO IHSX3181 IHSX3281
Single $565.30 $591.37 $26.07 4.61%
Double $1,130.60 $1,182.74 $52.14 4.61%
Emp/Child(ren) $961.01 $1,005.33 $44.32 4.61%
Family $1,611.11 $1,685.40 $74.29 4.61%
Silver HMO IHSX3182 IHSX3282
Single $563.46 $588.53 $25.07 4.45%
Double $1,126.92 $1,177.06 $50.14 4.45%
Emp/Child(ren) $957.88 $1,000.50 $42.62 4.45%
Family $1,605.86 $1,677.31 $71.45 4.45%
Silver HMO IHSX3183 IHSX3283
Single $565.30 $591.37 $26.07 4.61%
Double $1,130.60 $1,182.74 $52.14 4.61%
Emp/Child(ren) $961.01 $1,005.33 $44.32 4.61%
Family $1,611.11 $1,685.40 $74.29 4.61%
Silver HMO IHSX3188 IHSX3288
Single $539.62 $569.86 $30.24 5.60%
Double $1,079.24 $1,139.72 $60.48 5.60%
Emp/Child(ren) $917.35 $968.76 $51.41 5.60%
Family $1,537.92 $1,624.10 $86.18 5.60%
Silver HMO IHSX3189 IHSX3289
Single $541.39 $572.62 $31.23 5.77%
Double $1,082.78 $1,145.24 $62.46 5.77%
Emp/Child(ren) $920.36 $973.45 $53.09 5.77%
Family $1,542.96 $1,631.97 $89.01 5.77%
Silver HMO IHSX3186 IHSX3286
Single $539.62 $569.86 $30.24 5.60%
Double $1,079.24 $1,139.72 $60.48 5.60%
Emp/Child(ren) $917.35 $968.76 $51.41 5.60%
Family $1,537.92 $1,624.10 $86.18 5.60%
Silver HMO IHSX3187 IHSX3287
Single $541.39 $572.62 $31.23 5.77%
Double $1,082.78 $1,145.24 $62.46 5.77%
Emp/Child(ren) $920.36 $973.45 $53.09 5.77%
Family $1,542.96 $1,631.97 $89.01 5.77%
Bronze HMO IHBX4049 IHBX4149
Single $405.74 $427.39 $21.65 5.34%
Double $811.48 $854.78 $43.30 5.34%
Emp/Child(ren) $689.76 $726.56 $36.80 5.34%
Family $1,156.36 $1,218.06 $61.70 5.34%
Bronze HMO IHBX4050 IHBX4150
Single $407.05 $429.44 $22.39 5.50%
Double $814.10 $858.88 $44.78 5.50%
Emp/Child(ren) $691.99 $730.05 $38.06 5.50%
Family $1,160.09 $1,223.90 $63.81 5.50%
2020 Individual HMO On Exchange Rate Manual Page 2

Capital District Physicians' Health Plan
Albany Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBX4051 IHBX4151
Single $400.11 $423.13 $23.02 5.75%
Double $800.22 $846.26 $46.04 5.75%
Emp/Child(ren) $680.19 $719.32 $39.13 5.75%
Family $1,140.31 $1,205.92 $65.61 5.75%
Bronze HMO IHBX4052 IHBX4152
Single $401.41 $425.15 $23.74 5.91%
Double $802.82 $850.30 $47.48 5.91%
Emp/Child(ren) $682.40 $722.76 $40.36 5.91%
Family $1,144.02 $1,211.68 $67.66 5.91%
Platinum HMO New Plan IHPX5101
Single N/A $867.08 $0.00 0.00%
Double N/A $1,734.16 $0.00 0.00%
Emp/Child(ren) N/A $1,474.04 $0.00 0.00%
Family N/A $2,471.18 $0.00 0.00%
Platinum HMO New Plan IHPX5102
Single N/A $871.31 $0.00 0.00%
Double N/A $1,742.62 $0.00 0.00%
Emp/Child(ren) N/A $1,481.23 $0.00 0.00%
Family N/A $2,483.23 $0.00 0.00%
Silver HMO New Plan IHSX5101
Single N/A $566.62 $0.00 0.00%
Double N/A $1,133.24 $0.00 0.00%
Emp/Child(ren) N/A $963.25 $0.00 0.00%
Family N/A $1,614.87 $0.00 0.00%
Silver HMO New Plan IHSX5102
Single N/A $569.36 $0.00 0.00%
Double N/A $1,138.72 $0.00 0.00%
Emp/Child(ren) N/A $967.91 $0.00 0.00%
Family N/A $1,622.68 $0.00 0.00%
Silver HMO New Plan IHSX5103
Single N/A $591.38 $0.00 0.00%
Double N/A $1,182.76 $0.00 0.00%
Emp/Child(ren) N/A $1,005.35 $0.00 0.00%
Family N/A $1,685.43 $0.00 0.00%
Silver HMO New Plan IHSX5104
Single N/A $594.24 $0.00 0.00%
Double N/A $1,188.48 $0.00 0.00%
Emp/Child(ren) N/A $1,010.21 $0.00 0.00%
Family N/A $1,693.58 $0.00 0.00%
Platinum HMO IHPX1036 IHPX1038
Single $820.19 $891.04 $70.85 8.64%
Double $1,640.38 $1,782.08 $141.70 8.64%
Emp/Child(ren) $1,394.32 $1,514.77 $120.45 8.64%
Family $2,337.54 $2,539.46 $201.92 8.64%
Platinum HMO IHPX1037 IHPX1039
Single $822.90 $895.39 $72.49 8.81%
Double $1,645.80 $1,790.78 $144.98 8.81%
Emp/Child(ren) $1,398.93 $1,522.16 $123.23 8.81%
Family $2,345.27 $2,551.86 $206.59 8.81%
Gold HMO IHGX2037 IHGX2039
Single $713.79 $745.40 $31.61 4.43%
Double $1,427.58 $1,490.80 $63.22 4.43%
Emp/Child(ren) $1,213.44 $1,267.18 $53.74 4.43%
Family $2,034.30 $2,124.39 $90.09 4.43%
Gold HMO IHGX2038 IHGX2040
Single $716.14 $749.03 $32.89 4.59%
Double $1,432.28 $1,498.06 $65.78 4.59%
Emp/Child(ren) $1,217.44 $1,273.35 $55.91 4.59%
Family $2,041.00 $2,134.74 $93.74 4.59%
Silver HMO IHSX3190 IHSX3198
Single $577.18 $596.37 $19.19 3.32%
Double $1,154.36 $1,192.74 $38.38 3.32%
Emp/Child(ren) $981.21 $1,013.83 $32.62 3.32%
Family $1,644.96 $1,699.65 $54.69 3.32%
Silver HMO IHSX3191 IHSX3199
Single $577.18 $596.37 $19.19 3.32%
Double $1,154.36 $1,192.74 $38.38 3.32%
Emp/Child(ren) $981.21 $1,013.83 $32.62 3.32%
Family $1,644.96 $1,699.65 $54.69 3.32%
2020 Individual HMO On Exchange Rate Manual Page 3

Capital District Physicians' Health Plan
Albany Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Silver HMO IHSX3192 IHSX3200
Single $577.18 $596.37 $19.19 3.32%
Double $1,154.36 $1,192.74 $38.38 3.32%
Emp/Child(ren) $981.21 $1,013.83 $32.62 3.32%
Family $1,644.96 $1,699.65 $54.69 3.32%
Silver HMO IHSX3193 IHSX3201
Single $577.18 $596.37 $19.19 3.32%
Double $1,154.36 $1,192.74 $38.38 3.32%
Emp/Child(ren) $981.21 $1,013.83 $32.62 3.32%
Family $1,644.96 $1,699.65 $54.69 3.32%
Silver HMO IHSX3194 IHSX3202
Single $579.07 $599.26 $20.19 3.49%
Double $1,158.14 $1,198.52 $40.38 3.49%
Emp/Child(ren) $984.42 $1,018.74 $34.32 3.49%
Family $1,650.35 $1,707.89 $57.54 3.49%
Silver HMO IHSX3195 IHSX3203
Single $579.07 $599.26 $20.19 3.49%
Double $1,158.14 1,198.52$ 40.38$ 3.49%
Emp/Child(ren) $984.42 1,018.74$ 34.32$ 3.49%
Family $1,650.35 1,707.89$ 57.54$ 3.49%
Silver HMO IHSX3196 IHSX3204
Single $579.07 $599.26 $20.19 3.49%
Double $1,158.14 1,198.52$ 40.38$ 3.49%
Emp/Child(ren) $984.42 1,018.74$ 34.32$ 3.49%
Family $1,650.35 1,707.89$ 57.54$ 3.49%
Silver HMO IHSX3197 IHSX3205
Single $579.07 $599.26 $20.19 3.49%
Double $1,158.14 1,198.52$ 40.38$ 3.49%
Emp/Child(ren) $984.42 1,018.74$ 34.32$ 3.49%
Family $1,650.35 1,707.89$ 57.54$ 3.49%
Bronze HMO IHBX4053 IHBX4055
Single $410.64 $432.93 $22.29 5.43%
Double $821.28 865.86$ 44.58$ 5.43%
Emp/Child(ren) $698.09 735.98$ 37.89$ 5.43%
Family $1,170.32 1,233.85$ 63.53$ 5.43%
Bronze HMO IHBX4054 IHBX4056
Single $411.97 $435.00 $23.03 5.59%
Double $823.94 $870.00 $46.06 5.59%
Emp/Child(ren) $700.35 $739.50 $39.15 5.59%
Family $1,174.11 $1,239.75 $65.64 5.59%
Platinum HMO IHPXC022 IHPXC025
Single $346.54 $367.11 $20.57 5.94%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Gold HMO IHGXC024 IHGXC026
Single $302.70 $307.11 $4.41 1.46%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC036 IHSXC040
Single $246.42 $245.71 ($0.71) -0.29%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC037 IHSXC041
Single $246.42 $245.71 ($0.71) -0.29%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC038 IHSXC042
Single $246.42 $245.71 ($0.71) -0.29%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC039 IHSXC043
Single $246.42 $245.71 ($0.71) -0.29%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
2020 Individual HMO On Exchange Rate Manual Page 4

Capital District Physicians' Health Plan
Albany Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBXC025 IHBXC026
Single $177.80 $178.37 $0.57 0.32%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Catastrophic HMO IHCX5006 IHCX5008
Single $246.92 $238.33 ($8.59) -3.48%
Double $493.84 $476.66 ($17.18) -3.48%
Emp/Child(ren) $419.76 $405.16 ($14.60) -3.48%
Family $703.72 $679.24 ($24.48) -3.48%
2020 Individual HMO On Exchange Rate Manual Page 5

Capital District Physicians' Health Plan
Mid-Hudson Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Platinum HMO IHPX1034 IHPX1136
Single $1,222.56 $1,273.03 $50.47 4.13%
Double $2,445.13 $2,546.06 $100.93 4.13%
Emp/Child(ren) $2,078.36 $2,164.15 $85.79 4.13%
Family $3,484.31 $3,628.13 $143.82 4.13%
Platinum HMO IHPX1035 IHPX1137
Single $1,226.61 $1,279.23 $52.62 4.29%
Double $2,453.21 $2,558.46 $105.25 4.29%
Emp/Child(ren) $2,085.23 $2,174.69 $89.46 4.29%
Family $3,495.83 $3,645.81 $149.98 4.29%
Gold HMO IHGX2035 IHGX2135
Single $997.78 $1,084.08 $86.30 8.65%
Double $1,995.56 $2,168.16 $172.60 8.65%
Emp/Child(ren) $1,696.23 $1,842.93 $146.70 8.65%
Family $2,843.68 $3,089.62 $245.94 8.65%
Gold HMO IHGX2036 IHGX2136
Single $1,001.06 $1,089.35 $88.29 8.82%
Double $2,002.13 $2,178.70 $176.57 8.82%
Emp/Child(ren) $1,701.81 $1,851.90 $150.09 8.82%
Family $2,853.03 $3,104.65 $251.62 8.82%
Silver HMO IHSX3180 IHSX3280
Single $807.55 $841.11 $33.56 4.16%
Double $1,615.10 $1,682.21 $67.11 4.16%
Emp/Child(ren) $1,372.84 $1,429.88 $57.04 4.15%
Family $2,301.52 $2,397.15 $95.63 4.16%
Silver HMO IHSX3181 IHSX3281
Single $810.19 $845.16 $34.97 4.32%
Double $1,620.38 $1,690.33 $69.95 4.32%
Emp/Child(ren) $1,377.32 $1,436.78 $59.46 4.32%
Family $2,309.04 $2,408.72 $99.68 4.32%
Silver HMO IHSX3182 IHSX3282
Single $807.55 $841.11 $33.56 4.16%
Double $1,615.10 $1,682.21 $67.11 4.16%
Emp/Child(ren) $1,372.84 $1,429.88 $57.04 4.15%
Family $2,301.52 $2,397.15 $95.63 4.16%
Silver HMO IHSX3183 IHSX3283
Single $810.19 $845.16 $34.97 4.32%
Double $1,620.38 $1,690.33 $69.95 4.32%
Emp/Child(ren) $1,377.32 $1,436.78 $59.46 4.32%
Family $2,309.04 $2,408.72 $99.68 4.32%
Silver HMO IHSX3188 IHSX3288
Single $773.38 $814.42 $41.04 5.31%
Double $1,546.77 $1,628.85 $82.08 5.31%
Emp/Child(ren) $1,314.75 $1,384.52 $69.77 5.31%
Family $2,204.15 $2,321.11 $116.96 5.31%
Silver HMO IHSX3189 IHSX3289
Single $775.92 $818.37 $42.45 5.47%
Double $1,551.84 $1,636.74 $84.90 5.47%
Emp/Child(ren) $1,319.07 $1,391.23 $72.16 5.47%
Family $2,211.38 $2,332.35 $120.97 5.47%
Silver HMO IHSX3186 IHSX3286
Single $773.38 $814.42 $41.04 5.31%
Double $1,546.77 $1,628.85 $82.08 5.31%
Emp/Child(ren) $1,314.75 $1,384.52 $69.77 5.31%
Family $2,204.15 $2,321.11 $116.96 5.31%
Silver HMO IHSX3187 IHSX3287
Single $775.92 $818.37 $42.45 5.47%
Double $1,551.84 $1,636.74 $84.90 5.47%
Emp/Child(ren) $1,319.07 $1,391.23 $72.16 5.47%
Family $2,211.38 $2,332.35 $120.97 5.47%
Bronze HMO IHBX4049 IHBX4149
Single $581.51 $610.81 $29.30 5.04%
Double $1,163.01 $1,221.62 $58.61 5.04%
Emp/Child(ren) $988.56 $1,038.38 $49.82 5.04%
Family $1,657.30 $1,740.81 $83.51 5.04%
Bronze HMO IHBX4050 IHBX4150
Single $583.39 $613.74 $30.35 5.20%
Double $1,166.77 $1,227.48 $60.71 5.20%
Emp/Child(ren) $991.75 $1,043.36 $51.61 5.20%
Family $1,662.65 $1,749.16 $86.51 5.20%
2019 Individual HMO On Exchange Rate Manual Page 6

Capital District Physicians' Health Plan
Mid-Hudson Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBX4051 IHBX4151
Single $573.44 $604.72 $31.28 5.45%
Double $1,146.88 $1,209.44 $62.56 5.45%
Emp/Child(ren) $974.85 $1,028.03 $53.18 5.46%
Family $1,634.30 $1,723.46 $89.16 5.46%
Bronze HMO IHBX4052 IHBX4152
Single $575.30 $607.61 $32.31 5.62%
Double $1,150.60 $1,215.22 $64.62 5.62%
Emp/Child(ren) $978.01 $1,032.94 $54.93 5.62%
Family $1,639.61 $1,731.69 $92.08 5.62%
Platinum HMO New Plan IHPX5101
Single N/A $1,239.20 $0.00 0.00%
Double N/A $2,478.40 $0.00 0.00%
Emp/Child(ren) N/A $2,106.64 $0.00 0.00%
Family N/A $3,531.72 $0.00 0.00%
Platinum HMO New Plan IHPX5102
Single N/A $1,245.24 $0.00 0.00%
Double N/A $2,490.49 $0.00 0.00%
Emp/Child(ren) N/A $2,116.92 $0.00 0.00%
Family N/A $3,548.95 $0.00 0.00%
Silver HMO New Plan IHSX5101
Single N/A $809.79 $0.00 0.00%
Double N/A $1,619.59 $0.00 0.00%
Emp/Child(ren) N/A $1,376.65 $0.00 0.00%
Family N/A $2,307.91 $0.00 0.00%
Silver HMO New Plan IHSX5102
Single N/A $813.71 $0.00 0.00%
Double N/A $1,627.42 $0.00 0.00%
Emp/Child(ren) N/A $1,383.30 $0.00 0.00%
Family N/A $2,319.07 $0.00 0.00%
Silver HMO New Plan IHSX5103
Single N/A $845.18 $0.00 0.00%
Double N/A $1,690.36 $0.00 0.00%
Emp/Child(ren) N/A $1,436.80 $0.00 0.00%
Family N/A $2,408.76 $0.00 0.00%
Silver HMO New Plan IHSX5104
Single N/A $849.27 $0.00 0.00%
Double N/A $1,698.53 $0.00 0.00%
Emp/Child(ren) N/A $1,443.75 $0.00 0.00%
Family N/A $2,420.41 $0.00 0.00%
Platinum HMO IHPX1036 IHPX1038
Single $1,175.50 $1,273.44 $97.94 8.33%
Double $2,351.00 $2,546.88 $195.88 8.33%
Emp/Child(ren) $1,998.35 $2,164.85 $166.50 8.33%
Family $3,350.17 $3,629.31 $279.14 8.33%
Platinum HMO IHPX1037 IHPX1039
Single $1,179.38 $1,279.66 $100.28 8.50%
Double $2,358.76 $2,559.32 $200.56 8.50%
Emp/Child(ren) $2,004.95 $2,175.42 $170.47 8.50%
Family $3,361.24 $3,647.03 $285.79 8.50%
Gold HMO IHGX2037 IHGX2039
Single $1,023.01 $1,065.30 $42.29 4.13%
Double $2,046.01 $2,130.60 $84.59 4.13%
Emp/Child(ren) $1,739.11 $1,811.01 $71.90 4.13%
Family $2,915.57 $3,036.10 $120.53 4.13%
Gold HMO IHGX2038 IHGX2040
Single $1,026.37 $1,070.49 $44.12 4.30%
Double $2,052.75 $2,140.97 $88.22 4.30%
Emp/Child(ren) $1,744.83 $1,819.83 $75.00 4.30%
Family $2,925.16 $3,050.89 $125.73 4.30%
Silver HMO IHSX3190 IHSX3198
Single $827.22 $852.31 $25.09 3.03%
Double $1,654.43 $1,704.62 $50.19 3.03%
Emp/Child(ren) $1,406.27 $1,448.93 $42.66 3.03%
Family $2,357.56 $2,429.08 $71.52 3.03%
Silver HMO IHSX3191 IHSX3199
Single $827.22 $852.31 $25.09 3.03%
Double $1,654.43 $1,704.62 $50.19 3.03%
Emp/Child(ren) $1,406.27 $1,448.93 $42.66 3.03%
Family $2,357.56 $2,429.08 $71.52 3.03%
2019 Individual HMO On Exchange Rate Manual Page 7

Capital District Physicians' Health Plan
Mid-Hudson Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Silver HMO IHSX3192 IHSX3200
Single $827.22 $852.31 $25.09 3.03%
Double $1,654.43 $1,704.62 $50.19 3.03%
Emp/Child(ren) $1,406.27 $1,448.93 $42.66 3.03%
Family $2,357.56 $2,429.08 $71.52 3.03%
Silver HMO IHSX3193 IHSX3201
Single $827.22 $852.31 $25.09 3.03%
Double $1,654.43 $1,704.62 $50.19 3.03%
Emp/Child(ren) $1,406.27 $1,448.93 $42.66 3.03%
Family $2,357.56 $2,429.08 $71.52 3.03%
Silver HMO IHSX3194 IHSX3202
Single $829.92 $856.44 $26.52 3.20%
Double $1,659.85 $1,712.88 $53.03 3.19%
Emp/Child(ren) $1,410.87 $1,455.95 $45.08 3.20%
Family $2,365.28 $2,440.86 $75.58 3.20%
Silver HMO IHSX3195 IHSX3203
Single $829.92 $856.44 $26.52 3.20%
Double $1,659.85 $1,712.88 $53.03 3.19%
Emp/Child(ren) $1,410.87 $1,455.95 $45.08 3.20%
Family $2,365.28 $2,440.86 $75.58 3.20%
Silver HMO IHSX3196 IHSX3204
Single $829.92 $856.44 $26.52 3.20%
Double $1,659.85 1,712.88$ 53.03$ 3.19%
Emp/Child(ren) $1,410.87 1,455.95$ 45.08$ 3.20%
Family $2,365.28 2,440.86$ 75.58$ 3.20%
Silver HMO IHSX3197 IHSX3205
Single $829.92 $856.44 $26.52 3.20%
Double $1,659.85 1,712.88$ 53.03$ 3.19%
Emp/Child(ren) $1,410.87 1,455.95$ 45.08$ 3.20%
Family $2,365.28 2,440.86$ 75.58$ 3.20%
Bronze HMO IHBX4053 IHBX4055
Single $588.53 $618.73 $30.20 5.13%
Double $1,177.06 1,237.46$ 60.40$ 5.13%
Emp/Child(ren) $1,000.50 1,051.84$ 51.34$ 5.13%
Family $1,677.31 1,763.37$ 86.06$ 5.13%
Bronze HMO IHBX4054 IHBX4056
Single $590.44 $621.69 $31.25 5.29%
Double $1,180.87 1,243.37$ 62.50$ 5.29%
Emp/Child(ren) $1,003.74 1,056.87$ 53.13$ 5.29%
Family $1,682.74 1,771.81$ 89.07$ 5.29%
Platinum HMO IHPXC022 IHPXC025
Single $496.66 $524.66 $28.00 5.64%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Gold HMO IHGXC024 IHGXC026
Single $433.83 $438.91 $5.08 1.17%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC036 IHSXC040
Single $353.17 $351.16 ($2.01) -0.57%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC037 IHSXC041
Single $353.17 $351.16 ($2.01) -0.57%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC038 IHSXC042
Single $353.17 $351.16 ($2.01) -0.57%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC039 IHSXC043
Single $353.17 $351.16 ($2.01) -0.57%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
2019 Individual HMO On Exchange Rate Manual Page 8
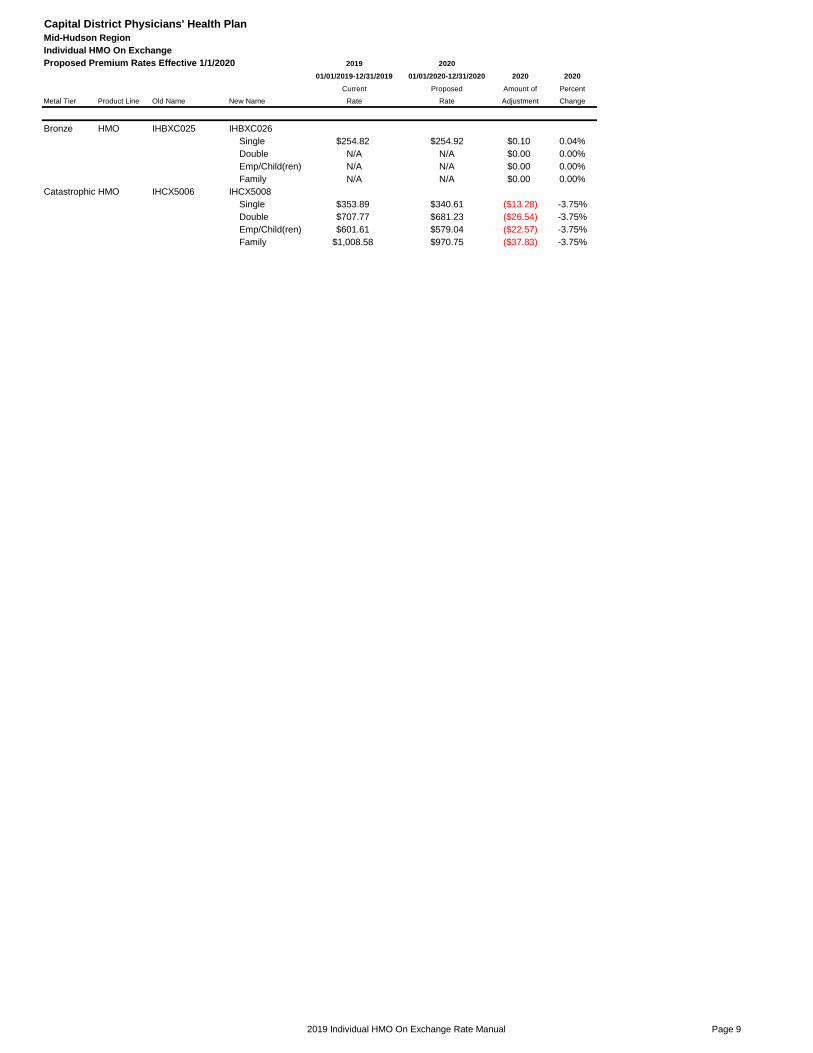
Capital District Physicians' Health Plan
Mid-Hudson Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBXC025 IHBXC026
Single $254.82 $254.92 $0.10 0.04%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Catastrophic HMO IHCX5006 IHCX5008
Single $353.89 $340.61 ($13.28) -3.75%
Double $707.77 $681.23 ($26.54) -3.75%
Emp/Child(ren) $601.61 $579.04 ($22.57) -3.75%
Family $1,008.58 $970.75 ($37.83) -3.75%
2019 Individual HMO On Exchange Rate Manual Page 9

Capital District Physicians' Health Plan
Syracuse Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Platinum HMO IHPX1034 IHPX1136
Single $1,022.50 $1,009.02 ($13.48) -1.32%
Double $2,044.99 $2,018.04 ($26.95) -1.32%
Emp/Child(ren) $1,738.24 $1,715.33 ($22.91) -1.32%
Family $2,914.12 $2,875.71 ($38.41) -1.32%
Platinum HMO IHPX1035 IHPX1137
Single $1,025.88 $1,013.94 ($11.94) -1.16%
Double $2,051.75 $2,027.87 ($23.88) -1.16%
Emp/Child(ren) $1,743.99 $1,723.69 ($20.30) -1.16%
Family $2,923.75 $2,889.72 ($34.03) -1.16%
Gold HMO IHGX2035 IHGX2135
Single $834.50 $859.26 $24.76 2.97%
Double $1,669.00 $1,718.51 $49.51 2.97%
Emp/Child(ren) $1,418.65 $1,460.74 $42.09 2.97%
Family $2,378.32 $2,448.88 $70.56 2.97%
Gold HMO IHGX2036 IHGX2136
Single $837.24 $863.44 $26.20 3.13%
Double $1,674.49 $1,726.87 $52.38 3.13%
Emp/Child(ren) $1,423.31 $1,467.84 $44.53 3.13%
Family $2,386.14 $2,460.79 $74.65 3.13%
Silver HMO IHSX3180 IHSX3280
Single $675.40 $666.67 ($8.73) -1.29%
Double $1,350.80 $1,333.35 ($17.45) -1.29%
Emp/Child(ren) $1,148.18 $1,133.34 ($14.84) -1.29%
Family $1,924.89 $1,900.02 ($24.87) -1.29%
Silver HMO IHSX3181 IHSX3281
Single $677.61 $669.89 ($7.72) -1.14%
Double $1,355.21 $1,339.78 ($15.43) -1.14%
Emp/Child(ren) $1,151.93 $1,138.81 ($13.12) -1.14%
Family $1,931.17 $1,909.19 ($21.98) -1.14%
Silver HMO IHSX3182 IHSX3282
Single $675.40 $666.67 ($8.73) -1.29%
Double $1,350.80 $1,333.35 ($17.45) -1.29%
Emp/Child(ren) $1,148.18 $1,133.34 ($14.84) -1.29%
Family $1,924.89 $1,900.02 ($24.87) -1.29%
Silver HMO IHSX3183 IHSX3283
Single $677.61 $669.89 ($7.72) -1.14%
Double $1,355.21 $1,339.78 ($15.43) -1.14%
Emp/Child(ren) $1,151.93 $1,138.81 ($13.12) -1.14%
Family $1,931.17 $1,909.19 ($21.98) -1.14%
Silver HMO IHSX3188 IHSX3288
Single $646.82 $645.52 ($1.30) -0.20%
Double $1,293.65 $1,291.05 ($2.60) -0.20%
Emp/Child(ren) $1,099.60 $1,097.39 ($2.21) -0.20%
Family $1,843.45 $1,839.74 ($3.71) -0.20%
Silver HMO IHSX3189 IHSX3289
Single $648.95 $648.65 ($0.30) -0.05%
Double $1,297.89 $1,297.30 ($0.59) -0.05%
Emp/Child(ren) $1,103.21 $1,102.71 ($0.50) -0.05%
Family $1,849.49 $1,848.65 ($0.84) -0.05%
Silver HMO IHSX3186 IHSX3286
Single $646.82 $645.52 ($1.30) -0.20%
Double $1,293.65 $1,291.05 ($2.60) -0.20%
Emp/Child(ren) $1,099.60 $1,097.39 ($2.21) -0.20%
Family $1,843.45 $1,839.74 ($3.71) -0.20%
Silver HMO IHSX3187 IHSX3287
Single $648.95 $648.65 ($0.30) -0.05%
Double $1,297.89 $1,297.30 ($0.59) -0.05%
Emp/Child(ren) $1,103.21 $1,102.71 ($0.50) -0.05%
Family $1,849.49 $1,848.65 ($0.84) -0.05%
Bronze HMO IHBX4049 IHBX4149
Single $486.35 $484.14 ($2.21) -0.45%
Double $972.69 $968.27 ($4.42) -0.45%
Emp/Child(ren) $826.79 $823.03 ($3.76) -0.45%
Family $1,386.09 $1,379.79 ($6.30) -0.45%
Bronze HMO IHBX4050 IHBX4150
Single $487.92 $486.46 ($1.46) -0.30%
Double $975.83 $972.92 ($2.91) -0.30%
Emp/Child(ren) $829.46 $826.98 ($2.48) -0.30%
Family $1,390.56 $1,386.41 ($4.15) -0.30%
2020 Individual HMO On Exchange Rate Manual Page 10
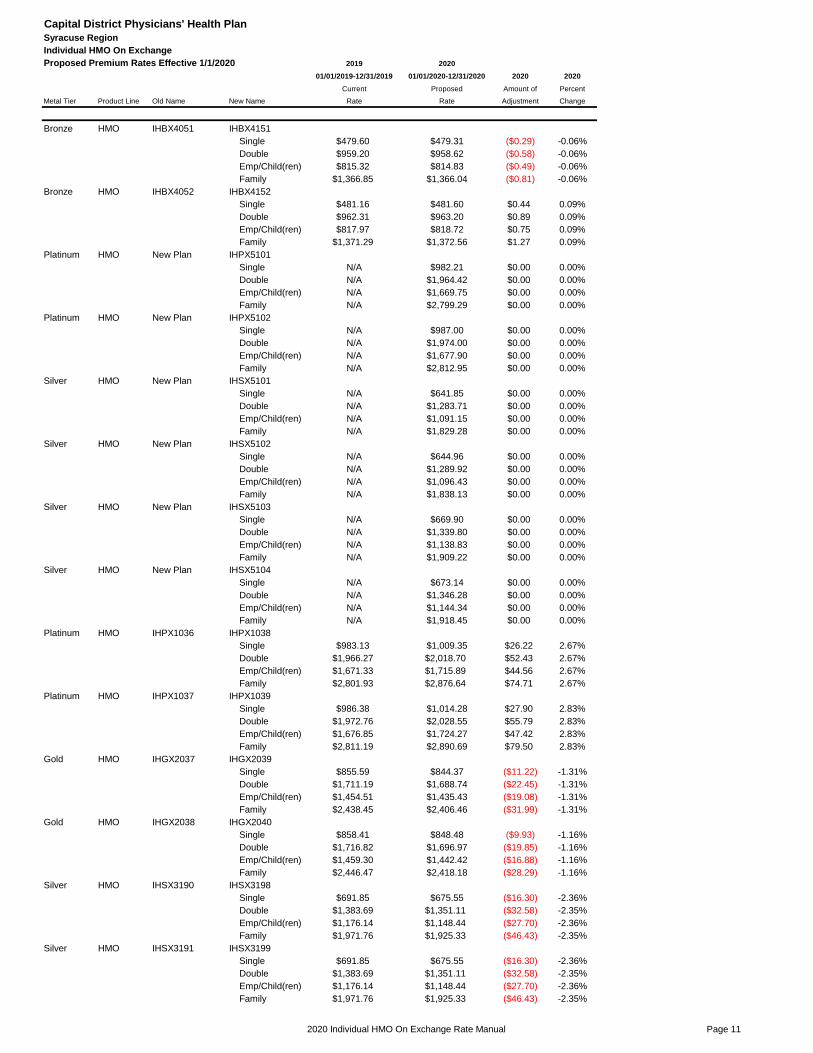
Capital District Physicians' Health Plan
Syracuse Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBX4051 IHBX4151
Single $479.60 $479.31 ($0.29) -0.06%
Double $959.20 $958.62 ($0.58) -0.06%
Emp/Child(ren) $815.32 $814.83 ($0.49) -0.06%
Family $1,366.85 $1,366.04 ($0.81) -0.06%
Bronze HMO IHBX4052 IHBX4152
Single $481.16 $481.60 $0.44 0.09%
Double $962.31 $963.20 $0.89 0.09%
Emp/Child(ren) $817.97 $818.72 $0.75 0.09%
Family $1,371.29 $1,372.56 $1.27 0.09%
Platinum HMO New Plan IHPX5101
Single N/A $982.21 $0.00 0.00%
Double N/A $1,964.42 $0.00 0.00%
Emp/Child(ren) N/A $1,669.75 $0.00 0.00%
Family N/A $2,799.29 $0.00 0.00%
Platinum HMO New Plan IHPX5102
Single N/A $987.00 $0.00 0.00%
Double N/A $1,974.00 $0.00 0.00%
Emp/Child(ren) N/A $1,677.90 $0.00 0.00%
Family N/A $2,812.95 $0.00 0.00%
Silver HMO New Plan IHSX5101
Single N/A $641.85 $0.00 0.00%
Double N/A $1,283.71 $0.00 0.00%
Emp/Child(ren) N/A $1,091.15 $0.00 0.00%
Family N/A $1,829.28 $0.00 0.00%
Silver HMO New Plan IHSX5102
Single N/A $644.96 $0.00 0.00%
Double N/A $1,289.92 $0.00 0.00%
Emp/Child(ren) N/A $1,096.43 $0.00 0.00%
Family N/A $1,838.13 $0.00 0.00%
Silver HMO New Plan IHSX5103
Single N/A $669.90 $0.00 0.00%
Double N/A $1,339.80 $0.00 0.00%
Emp/Child(ren) N/A $1,138.83 $0.00 0.00%
Family N/A $1,909.22 $0.00 0.00%
Silver HMO New Plan IHSX5104
Single N/A $673.14 $0.00 0.00%
Double N/A $1,346.28 $0.00 0.00%
Emp/Child(ren) N/A $1,144.34 $0.00 0.00%
Family N/A $1,918.45 $0.00 0.00%
Platinum HMO IHPX1036 IHPX1038
Single $983.13 $1,009.35 $26.22 2.67%
Double $1,966.27 $2,018.70 $52.43 2.67%
Emp/Child(ren) $1,671.33 $1,715.89 $44.56 2.67%
Family $2,801.93 $2,876.64 $74.71 2.67%
Platinum HMO IHPX1037 IHPX1039
Single $986.38 $1,014.28 $27.90 2.83%
Double $1,972.76 $2,028.55 $55.79 2.83%
Emp/Child(ren) $1,676.85 $1,724.27 $47.42 2.83%
Family $2,811.19 $2,890.69 $79.50 2.83%
Gold HMO IHGX2037 IHGX2039
Single $855.59 $844.37 ($11.22) -1.31%
Double $1,711.19 $1,688.74 ($22.45) -1.31%
Emp/Child(ren) $1,454.51 $1,435.43 ($19.08) -1.31%
Family $2,438.45 $2,406.46 ($31.99) -1.31%
Gold HMO IHGX2038 IHGX2040
Single $858.41 $848.48 ($9.93) -1.16%
Double $1,716.82 $1,696.97 ($19.85) -1.16%
Emp/Child(ren) $1,459.30 $1,442.42 ($16.88) -1.16%
Family $2,446.47 $2,418.18 ($28.29) -1.16%
Silver HMO IHSX3190 IHSX3198
Single $691.85 $675.55 ($16.30) -2.36%
Double $1,383.69 $1,351.11 ($32.58) -2.35%
Emp/Child(ren) $1,176.14 $1,148.44 ($27.70) -2.36%
Family $1,971.76 $1,925.33 ($46.43) -2.35%
Silver HMO IHSX3191 IHSX3199
Single $691.85 $675.55 ($16.30) -2.36%
Double $1,383.69 $1,351.11 ($32.58) -2.35%
Emp/Child(ren) $1,176.14 $1,148.44 ($27.70) -2.36%
Family $1,971.76 $1,925.33 ($46.43) -2.35%
2020 Individual HMO On Exchange Rate Manual Page 11

Capital District Physicians' Health Plan
Syracuse Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Silver HMO IHSX3192 IHSX3200
Single $691.85 $675.55 ($16.30) -2.36%
Double $1,383.69 $1,351.11 ($32.58) -2.35%
Emp/Child(ren) $1,176.14 $1,148.44 ($27.70) -2.36%
Family $1,971.76 $1,925.33 ($46.43) -2.35%
Silver HMO IHSX3193 IHSX3201
Single $691.85 $675.55 ($16.30) -2.36%
Double $1,383.69 $1,351.11 ($32.58) -2.35%
Emp/Child(ren) $1,176.14 $1,148.44 ($27.70) -2.36%
Family $1,971.76 $1,925.33 ($46.43) -2.35%
Silver HMO IHSX3194 IHSX3202
Single $694.11 $678.83 ($15.28) -2.20%
Double $1,388.22 $1,357.66 ($30.56) -2.20%
Emp/Child(ren) $1,179.99 $1,154.01 ($25.98) -2.20%
Family $1,978.22 $1,934.66 ($43.56) -2.20%
Silver HMO IHSX3195 IHSX3203
Single $694.11 $678.83 ($15.28) -2.20%
Double $1,388.22 $1,357.66 ($30.56) -2.20%
Emp/Child(ren) $1,179.99 $1,154.01 ($25.98) -2.20%
Family $1,978.22 $1,934.66 ($43.56) -2.20%
Silver HMO IHSX3196 IHSX3204
Single $694.11 $678.83 ($15.28) -2.20%
Double $1,388.22 1,357.66$ (30.56)$ -2.20%
Emp/Child(ren) $1,179.99 1,154.01$ (25.98)$ -2.20%
Family $1,978.22 1,934.66$ (43.56)$ -2.20%
Silver HMO IHSX3197 IHSX3205
Single $694.11 $678.83 ($15.28) -2.20%
Double $1,388.22 1,357.66$ (30.56)$ -2.20%
Emp/Child(ren) $1,179.99 1,154.01$ (25.98)$ -2.20%
Family $1,978.22 1,934.66$ (43.56)$ -2.20%
Bronze HMO IHBX4053 IHBX4055
Single $492.22 $490.41 ($1.81) -0.37%
Double $984.44 980.83$ (3.61)$ -0.37%
Emp/Child(ren) $836.77 833.70$ (3.07)$ -0.37%
Family $1,402.83 1,397.68$ (5.15)$ -0.37%
Bronze HMO IHBX4054 IHBX4056
Single $493.81 $492.76 ($1.05) -0.21%
Double $987.63 985.52$ (2.11)$ -0.21%
Emp/Child(ren) $839.48 837.69$ (1.79)$ -0.21%
Family $1,407.37 1,404.36$ (3.01)$ -0.21%
Platinum HMO IHPXC022 IHPXC025
Single $415.39 $415.85 $0.46 0.11%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Gold HMO IHGXC024 IHGXC026
Single $362.84 $347.89 ($14.95) -4.12%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC036 IHSXC040
Single $295.37 $278.33 ($17.04) -5.77%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC037 IHSXC041
Single $295.37 $278.33 ($17.04) -5.77%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC038 IHSXC042
Single $295.37 $278.33 ($17.04) -5.77%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC039 IHSXC043
Single $295.37 $278.33 ($17.04) -5.77%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
2020 Individual HMO On Exchange Rate Manual Page 12

Capital District Physicians' Health Plan
Syracuse Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBXC025 IHBXC026
Single $213.12 $202.05 ($11.07) -5.19%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Catastrophic HMO IHCX5006 IHCX5008
Single $295.97 $269.97 ($26.00) -8.78%
Double $591.95 $539.95 ($52.00) -8.78%
Emp/Child(ren) $503.16 $458.96 ($44.20) -8.78%
Family $843.53 $769.43 ($74.10) -8.78%
2020 Individual HMO On Exchange Rate Manual Page 13

Capital District Physicians' Health Plan
UticaWatertown Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Platinum HMO IHPX1034 IHPX1136
Single $1,005.03 $996.81 ($8.22) -0.82%
Double $2,010.06 $1,993.62 ($16.44) -0.82%
Emp/Child(ren) $1,708.55 $1,694.58 ($13.97) -0.82%
Family $2,864.34 $2,840.91 ($23.43) -0.82%
Platinum HMO IHPX1035 IHPX1137
Single $1,008.35 $1,001.67 ($6.68) -0.66%
Double $2,016.71 $2,003.34 ($13.37) -0.66%
Emp/Child(ren) $1,714.20 $1,702.84 ($11.36) -0.66%
Family $2,873.81 $2,854.75 ($19.06) -0.66%
Gold HMO IHGX2035 IHGX2135
Single $820.24 $848.86 $28.62 3.49%
Double $1,640.49 $1,697.72 $57.23 3.49%
Emp/Child(ren) $1,394.42 $1,443.06 $48.64 3.49%
Family $2,337.70 $2,419.25 $81.55 3.49%
Gold HMO IHGX2036 IHGX2136
Single $822.94 $852.99 $30.05 3.65%
Double $1,645.88 $1,705.98 $60.10 3.65%
Emp/Child(ren) $1,399.00 $1,450.08 $51.08 3.65%
Family $2,345.39 $2,431.02 $85.63 3.65%
Silver HMO IHSX3180 IHSX3280
Single $663.86 $658.61 ($5.25) -0.79%
Double $1,327.73 $1,317.21 ($10.52) -0.79%
Emp/Child(ren) $1,128.57 $1,119.63 ($8.94) -0.79%
Family $1,892.01 $1,877.03 ($14.98) -0.79%
Silver HMO IHSX3181 IHSX3281
Single $666.03 $661.78 ($4.25) -0.64%
Double $1,332.06 $1,323.57 ($8.49) -0.64%
Emp/Child(ren) $1,132.25 $1,125.03 ($7.22) -0.64%
Family $1,898.19 $1,886.08 ($12.11) -0.64%
Silver HMO IHSX3182 IHSX3282
Single $663.86 $658.61 ($5.25) -0.79%
Double $1,327.73 $1,317.21 ($10.52) -0.79%
Emp/Child(ren) $1,128.57 $1,119.63 ($8.94) -0.79%
Family $1,892.01 $1,877.03 ($14.98) -0.79%
Silver HMO IHSX3183 IHSX3283
Single $666.03 $661.78 ($4.25) -0.64%
Double $1,332.06 $1,323.57 ($8.49) -0.64%
Emp/Child(ren) $1,132.25 $1,125.03 ($7.22) -0.64%
Family $1,898.19 $1,886.08 ($12.11) -0.64%
Silver HMO IHSX3188 IHSX3288
Single $635.78 $637.71 $1.93 0.30%
Double $1,271.55 $1,275.43 $3.88 0.31%
Emp/Child(ren) $1,080.82 $1,084.11 $3.29 0.30%
Family $1,811.96 $1,817.48 $5.52 0.30%
Silver HMO IHSX3189 IHSX3289
Single $637.86 $640.80 $2.94 0.46%
Double $1,275.72 $1,281.60 $5.88 0.46%
Emp/Child(ren) $1,084.36 $1,089.36 $5.00 0.46%
Family $1,817.90 $1,826.28 $8.38 0.46%
Silver HMO IHSX3186 IHSX3286
Single $635.78 $637.71 $1.93 0.30%
Double $1,271.55 $1,275.43 $3.88 0.31%
Emp/Child(ren) $1,080.82 $1,084.11 $3.29 0.30%
Family $1,811.96 $1,817.48 $5.52 0.30%
Silver HMO IHSX3187 IHSX3287
Single $637.86 $640.80 $2.94 0.46%
Double $1,275.72 $1,281.60 $5.88 0.46%
Emp/Child(ren) $1,084.36 $1,089.36 $5.00 0.46%
Family $1,817.90 $1,826.28 $8.38 0.46%
Bronze HMO IHBX4049 IHBX4149
Single $478.04 $478.28 $0.24 0.05%
Double $956.08 $956.56 $0.48 0.05%
Emp/Child(ren) $812.67 $813.07 $0.40 0.05%
Family $1,362.41 $1,363.10 $0.69 0.05%
Bronze HMO IHBX4050 IHBX4150
Single $479.58 $480.57 $0.99 0.21%
Double $959.16 $961.15 $1.99 0.21%
Emp/Child(ren) $815.29 $816.97 $1.68 0.21%
Family $1,366.81 $1,369.63 $2.82 0.21%
2020 Individual HMO On Exchange Rate Manual Page 14

Capital District Physicians' Health Plan
UticaWatertown Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBX4051 IHBX4151
Single $471.41 $473.51 $2.10 0.45%
Double $942.81 $947.02 $4.21 0.45%
Emp/Child(ren) $801.39 $804.97 $3.58 0.45%
Family $1,343.51 $1,349.51 $6.00 0.45%
Bronze HMO IHBX4052 IHBX4152
Single $472.94 $475.77 $2.83 0.60%
Double $945.87 $951.54 $5.67 0.60%
Emp/Child(ren) $803.99 $808.81 $4.82 0.60%
Family $1,347.87 $1,355.95 $8.08 0.60%
Platinum HMO New Plan IHPX5101
Single N/A $970.32 $0.00 0.00%
Double N/A $1,940.65 $0.00 0.00%
Emp/Child(ren) N/A $1,649.55 $0.00 0.00%
Family N/A $2,765.42 $0.00 0.00%
Platinum HMO New Plan IHPX5102
Single N/A $975.06 $0.00 0.00%
Double N/A $1,950.11 $0.00 0.00%
Emp/Child(ren) N/A $1,657.60 $0.00 0.00%
Family N/A $2,778.91 $0.00 0.00%
Silver HMO New Plan IHSX5101
Single N/A $634.09 $0.00 0.00%
Double N/A $1,268.17 $0.00 0.00%
Emp/Child(ren) N/A $1,077.95 $0.00 0.00%
Family N/A $1,807.15 $0.00 0.00%
Silver HMO New Plan IHSX5102
Single N/A $637.15 $0.00 0.00%
Double N/A $1,274.31 $0.00 0.00%
Emp/Child(ren) N/A $1,083.16 $0.00 0.00%
Family N/A $1,815.89 $0.00 0.00%
Silver HMO New Plan IHSX5103
Single N/A $661.80 $0.00 0.00%
Double N/A $1,323.59 $0.00 0.00%
Emp/Child(ren) N/A $1,125.05 $0.00 0.00%
Family N/A $1,886.12 $0.00 0.00%
Silver HMO New Plan IHSX5104
Single N/A $665.00 $0.00 0.00%
Double N/A $1,329.99 $0.00 0.00%
Emp/Child(ren) N/A $1,130.49 $0.00 0.00%
Family N/A $1,895.24 $0.00 0.00%
Platinum HMO IHPX1036 IHPX1038
Single $966.34 $997.14 $30.80 3.19%
Double $1,932.68 $1,994.27 $61.59 3.19%
Emp/Child(ren) $1,642.78 $1,695.13 $52.35 3.19%
Family $2,754.07 $2,841.84 $87.77 3.19%
Platinum HMO IHPX1037 IHPX1039
Single $969.53 $1,002.00 $32.47 3.35%
Double $1,939.07 $2,004.01 $64.94 3.35%
Emp/Child(ren) $1,648.21 $1,703.41 $55.20 3.35%
Family $2,763.17 $2,855.71 $92.54 3.35%
Gold HMO IHGX2037 IHGX2039
Single $840.98 $834.15 ($6.83) -0.81%
Double $1,681.96 $1,668.31 ($13.65) -0.81%
Emp/Child(ren) $1,429.67 $1,418.06 ($11.61) -0.81%
Family $2,396.79 $2,377.34 ($19.45) -0.81%
Gold HMO IHGX2038 IHGX2040
Single $843.75 $838.22 ($5.53) -0.66%
Double $1,687.50 $1,676.43 ($11.07) -0.66%
Emp/Child(ren) $1,434.37 $1,424.97 ($9.40) -0.66%
Family $2,404.69 $2,388.92 ($15.77) -0.66%
Silver HMO IHSX3190 IHSX3198
Single $680.03 $667.38 ($12.65) -1.86%
Double $1,360.06 $1,334.76 ($25.30) -1.86%
Emp/Child(ren) $1,156.05 $1,134.55 ($21.50) -1.86%
Family $1,938.08 $1,902.03 ($36.05) -1.86%
Silver HMO IHSX3191 IHSX3199
Single $680.03 $667.38 ($12.65) -1.86%
Double $1,360.06 $1,334.76 ($25.30) -1.86%
Emp/Child(ren) $1,156.05 $1,134.55 ($21.50) -1.86%
Family $1,938.08 $1,902.03 ($36.05) -1.86%
2020 Individual HMO On Exchange Rate Manual Page 15

Capital District Physicians' Health Plan
UticaWatertown Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Silver HMO IHSX3192 IHSX3200
Single $680.03 $667.38 ($12.65) -1.86%
Double $1,360.06 $1,334.76 ($25.30) -1.86%
Emp/Child(ren) $1,156.05 $1,134.55 ($21.50) -1.86%
Family $1,938.08 $1,902.03 ($36.05) -1.86%
Silver HMO IHSX3193 IHSX3201
Single $680.03 $667.38 ($12.65) -1.86%
Double $1,360.06 $1,334.76 ($25.30) -1.86%
Emp/Child(ren) $1,156.05 $1,134.55 ($21.50) -1.86%
Family $1,938.08 $1,902.03 ($36.05) -1.86%
Silver HMO IHSX3194 IHSX3202
Single $682.25 $670.61 ($11.64) -1.71%
Double $1,364.51 $1,341.23 ($23.28) -1.71%
Emp/Child(ren) $1,159.83 $1,140.04 ($19.79) -1.71%
Family $1,944.43 $1,911.25 ($33.18) -1.71%
Silver HMO IHSX3195 IHSX3203
Single $682.25 $670.61 ($11.64) -1.71%
Double $1,364.51 $1,341.23 ($23.28) -1.71%
Emp/Child(ren) $1,159.83 $1,140.04 ($19.79) -1.71%
Family $1,944.43 $1,911.25 ($33.18) -1.71%
Silver HMO IHSX3196 IHSX3204
Single $682.25 $670.61 ($11.64) -1.71%
Double $1,364.51 $1,341.23 ($23.28) -1.71%
Emp/Child(ren) $1,159.83 $1,140.04 ($19.79) -1.71%
Family $1,944.43 $1,911.25 ($33.18) -1.71%
Silver HMO IHSX3197 IHSX3205
Single $682.25 $670.61 ($11.64) -1.71%
Double $1,364.51 $1,341.23 ($23.28) -1.71%
Emp/Child(ren) $1,159.83 $1,140.04 ($19.79) -1.71%
Family $1,944.43 $1,911.25 ($33.18) -1.71%
Bronze HMO IHBX4053 IHBX4055
Single $483.81 $484.48 $0.67 0.14%
Double $967.62 $968.96 $1.34 0.14%
Emp/Child(ren) $822.48 $823.61 $1.13 0.14%
Family $1,378.86 $1,380.76 $1.90 0.14%
Bronze HMO IHBX4054 IHBX4056
Single $485.38 $486.80 $1.42 0.29%
Double $970.76 $973.59 $2.83 0.29%
Emp/Child(ren) $825.14 $827.55 $2.41 0.29%
Family $1,383.33 $1,387.37 $4.04 0.29%
Platinum HMO IHPXC022 IHPXC025
Single $408.29 $410.82 $2.53 0.62%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Gold HMO IHGXC024 IHGXC026
Single $356.64 $343.68 ($12.96) -3.63%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC036 IHSXC040
Single $290.33 $274.97 ($15.36) -5.29%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC037 IHSXC041
Single $290.33 $274.97 ($15.36) -5.29%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC038 IHSXC042
Single $290.33 $274.97 ($15.36) -5.29%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Silver HMO IHSXC039 IHSXC043
Single $290.33 $274.97 ($15.36) -5.29%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
2020 Individual HMO On Exchange Rate Manual Page 16

Capital District Physicians' Health Plan
UticaWatertown Region
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 2019 2020
01/01/2019-12/31/2019 01/01/2020-12/31/2020 2020 2020
Current Proposed Amount of Percent
Metal Tier Product Line Old Name New Name Rate Rate Adjustment Change
Bronze HMO IHBXC025 IHBXC026
Single $209.48 $199.61 ($9.87) -4.71%
Double N/A N/A $0.00 0.00%
Emp/Child(ren) N/A N/A $0.00 0.00%
Family N/A N/A $0.00 0.00%
Catastrophic HMO IHCX5006 IHCX5008
Single $290.92 $266.71 ($24.21) -8.32%
Double $581.84 $533.42 ($48.42) -8.32%
Emp/Child(ren) $494.56 $453.40 ($41.16) -8.32%
Family $829.12 $760.12 ($69.00) -8.32%
2020 Individual HMO On Exchange Rate Manual Page 17

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 J R s t u v X Y Z AA AB AC AG AH AI AJ
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code 2020 Plan Code Standard?AV OV SP INN HOSP OUT SURG ER AMB DME
URGENT
CAREDIABETIC PT/OT/ST COIN INN Ded Single INN Ded Family INN Max Single
01-0001-2020 Ind HMO Platinum 94788NY0280129-01 IHPX1034 IHPX1136 Non-Standard 88.5% 15 20 10% 0.1 10% 10% 0.5 30 15 20 0.1 200 400 7350
01-0001-2020 Ind HMO Platinum 94788NY0280130-01 IHPX1035 IHPX1137 Non-Standard 88.5% 15 20 10% 0.1 10% 10% 0.5 30 15 20 0.1 200 400 7350
01-0001-2020 Ind HMO Gold 94788NY0280131-01 IHGX2035 IHGX2135 Non-Standard 82.0% 20 40 20% 20% 20% 20% 0.5 50 20 40 0.2 750 1500 6500
01-0001-2020 Ind HMO Gold 94788NY0280132-01 IHGX2036 IHGX2136 Non-Standard 82.0% 20 40 20% 20% 20% 20% 0.5 50 20 40 0.2 750 1500 6500
01-0001-2020 Ind HMO Silver 94788NY0280021-01 IHSX3180 IHSX3280 Non-Standard 71.9% 15% 15% 15% 15% 15% 15% 0.5 0.15 15% 15% 0.15 2500 5000 5500
01-0001-2020 Ind HMO Silver 94788NY0280022-01 IHSX3181 IHSX3281 Non-Standard 71.9% 15% 15% 15% 15% 15% 15% 0.5 0.15 15% 15% 0.15 2500 5000 5500
01-0001-2020 Ind HMO Silver 94788NY0280021-04 IHSX3182 IHSX3282 Non-Standard 73.9% 15% 15% 15% 15% 15% 15% 0.5 15% 15% 15% 0.15 2350 4700 5250
01-0001-2020 Ind HMO Silver 94788NY0280022-04 IHSX3183 IHSX3283 Non-Standard 73.9% 15% 15% 15% 15% 15% 15% 0.5 15% 15% 15% 0.15 2350 4700 5250
01-0001-2020 Ind HMO Silver 94788NY0280017-01 IHSX3188 IHSX3288 Non-Standard 71.7%
EPC
0%/Non
EPC 10%
10% 10% 10% 10% 10% 0.5 0.1 0.1 10% 0.1 4000 8000 7900
01-0001-2020 Ind HMO Silver 94788NY0280018-01 IHSX3189 IHSX3289 Non-Standard 71.7%
EPC
0%/Non
EPC 10%
10% 10% 10% 10% 10% 0.5 0.1 0.1 10% 0.1 4000 8000 7900
01-0001-2020 Ind HMO Silver 94788NY0280017-04 IHSX3186 IHSX3286 Non-Standard 74.0%
EPC
0%/Non
EPC 40%
0.4 0.4 0.4 0.4 0.4 0.5 0.4 0.4 0.4 0.4 2900 5800 6000
01-0001-2020 Ind HMO Silver 94788NY0280018-04 IHSX3187 IHSX3287 Non-Standard 74.0%
EPC
0%/Non
EPC 40%
0.4 0.4 0.4 0.4 0.4 0.5 0.4 0.4 0.4 0.4 2900 5800 4900
01-0001-2020 Ind HMO Bronze 94788NY0280029-01 IHBX4049 IHBX4149 Non-Standard 63.1% 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 5500 11000 6750
01-0001-2020 Ind HMO Bronze 94788NY0280030-01 IHBX4050 IHBX4150 Non-Standard 63.1% 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2 5500 11000 6750
01-0002-2020 Ind HMO Bronze 94788NY0280145-01 IHBX4051 IHBX4151 Non-Standard 62.5% 0 0 0 0 0 0 0 0 0 0 0 6750 13500 6750
01-0002-2020 Ind HMO Bronze 94788NY0280146-01 IHBX4052 IHBX4152 Non-Standard 62.5% 0 0 0 0 0 0 0 0 0 0 0 6750 13500 6750
01-0001-2020 Ind HMO Platinum 94788NY0280147-01 New Plan IHPX5101 Non-Standard 87.7% 0 25 250 100 200 200 0.5 40 0 25 0 0 0 3000
01-0001-2020 Ind HMO Platinum 94788NY0280148-01 New Plan IHPX5102 Non-Standard 87.7% 0 25 250 100 200 200 0.5 40 0 25 0 0 0 3000
01-0001-2020 Ind HMO Silver 94788NY0280149-01 New Plan IHSX5101 Non-Standard 70.0% 25 50 1500 200 500 500 0.5 60 25 50 0 1600 3200 6750
01-0001-2020 Ind HMO Silver 94788NY0280150-01 New Plan IHSX5102 Non-Standard 70.0% 25 50 1500 200 500 500 0.5 60 25 50 0 1600 3200 6750
01-0001-2020 Ind HMO Silver 94788NY0280149-04 New Plan IHSX5103 Non-Standard 72.8% 25 50 1000 150 250 250 0.5 60 25 50 0 1500 3000 5500
01-0001-2020 Ind HMO Silver 94788NY0280150-04 New Plan IHSX5104 Non-Standard 72.8% 25 50 1000 150 250 250 0.5 60 25 50 0 1500 3000 5500
01-0001-2020 Ind HMO Platinum 94788NY0280053-01 IHPX1036 IHPX1038 Standard 88.7% 15 35 500 100 100 100 10% 55 15 25 0 0 0 2000
01-0001-2020 Ind HMO Platinum 94788NY0280064-01 IHPX1037 IHPX1039 Standard 88.7% 15 35 500 100 100 100 10% 55 15 25 0 0 0 2000
01-0001-2020 Ind HMO Gold 94788NY0280054-01 IHGX2037 IHGX2039 Standard 80.9% 25 40 1000 100 150 150 20% 60 25 30 0 600 1200 4000
01-0001-2020 Ind HMO Gold 94788NY0280065-01 IHGX2038 IHGX2040 Standard 80.9% 25 40 1000 100 150 150 20% 60 25 30 0 600 1200 4000
01-0001-2020 Ind HMO Silver 94788NY0280055-01 IHSX3190 IHSX3198 Standard 72.0% 30 50 1500 150 250 150 30% 70 30 30 0 1300 2600 7900
Page 182013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 J R s t u v X Y Z AA AB AC AG AH AI AJ
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code 2020 Plan Code Standard?AV OV SP INN HOSP OUT SURG ER AMB DME
URGENT
CAREDIABETIC PT/OT/ST COIN INN Ded Single INN Ded Family INN Max Single
01-0001-2020 Ind HMO Silver 94788NY0280055-04 IHSX3191 IHSX3199 Silver CSR 74.0% 30 50 1500 150 250 150 0.25 70 30 30 0 1100 2200 6500
01-0001-2020 Ind HMO Silver 94788NY0280055-05 IHSX3192 IHSX3200 Silver CSR 87.6% 15 35 250 75 75 75 0.1 50 15 25 0 250 500 2100
01-0001-2020 Ind HMO Silver 94788NY0280055-06 IHSX3193 IHSX3201 Silver CSR 94.3% 10 20 100 25 50 50 0.05 30 10 15 0 0 0 1000
01-0001-2020 Ind HMO Silver 94788NY0280066-01 IHSX3194 IHSX3202 Standard 72.0% 30 50 1500 150 250 150 30% 70 30 30 0 1300 2600 7900
01-0001-2020 Ind HMO Silver 94788NY0280066-04 IHSX3195 IHSX3203 Silver CSR 74.0% 30 50 1500 150 250 150 0.25 70 30 30 0 1100 2200 6500
01-0001-2020 Ind HMO Silver 94788NY0280066-05 IHSX3196 IHSX3204 Silver CSR 86.9% 15 35 250 75 75 75 0.1 50 15 25 0 250 500 2100
01-0001-2020 Ind HMO Silver 94788NY0280066-06 IHSX3197 IHSX3205 Silver CSR 93.9% 10 20 100 25 50 50 0.05 30 10 15 0 0 0 1000
01-0001-2020 Ind HMO Bronze 94788NY0280059-01 IHBX4053 IHBX4055 Standard 63.4% 50% 50% 50% 50% 50% 50% 50% 0.5 50% 50% 0.5 5500 11000 6550
01-0001-2020 Ind HMO Bronze 94788NY0280070-01 IHBX4054 IHBX4056 Standard 63.4% 50% 50% 50% 50% 50% 50% 50% 0.5 50% 50% 0.5 5500 11000 6550
01-0004-2020 Ind HMO Platinum 94788NY0280081-01 IHPXC022 IHPXC025 Standard 88.7% 15 35 500 100 100 100 10% 55 15 25 0 0 0 2000
01-0004-2020 Ind HMO Gold 94788NY0280080-01 IHGXC024 IHGXC026 Standard 80.9% 25 40 1000 100 150 150 20% 60 25 30 0 600 1200 4000
01-0004-2020 Ind HMO Silver 94788NY0280082-01 IHSXC036 IHSXC040 Standard 72.0% 30 50 1500 150 250 150 30% 70 30 30 0 1300 2600 7900
01-0004-2020 Ind HMO Silver 94788NY0280082-04 IHSXC037 IHSXC041 Silver CSR Child 74.0% 30 50 1500 150 250 150 0.25 70 30 30 0 1100 2200 6500
01-0004-2020 Ind HMO Silver 94788NY0280082-05 IHSXC038 IHSXC042 Silver CSR Child 87.6% 15 35 250 75 75 75 0.1 50 15 25 0 250 500 2100
01-0004-2020 Ind HMO Silver 94788NY0280082-06 IHSXC039 IHSXC043 Silver CSR Child 94.3% 10 20 100 25 50 50 0.05 30 10 15 0 0 0 1000
01-0004-2020 Ind HMO Bronze 94788NY0280079-01 IHBXC025 IHBXC026 Standard 63.4% 50% 50% 50% 50% 50% 50% 50% 0.5 50% 50% 0.5 5500 11000 6550
01-0005-2020 Ind HMO Catastrophic 94788NY0280047-01 IHCX5006 IHCX5008 Standard 61.1% 0 0 0 0 0 0 0 0 0 0 0 8150 16300 8150
Page 192013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code 2020 Plan Code Standard?
01-0001-2020 Ind HMO Platinum 94788NY0280129-01 IHPX1034 IHPX1136 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280130-01 IHPX1035 IHPX1137 Non-Standard
01-0001-2020 Ind HMO Gold 94788NY0280131-01 IHGX2035 IHGX2135 Non-Standard
01-0001-2020 Ind HMO Gold 94788NY0280132-01 IHGX2036 IHGX2136 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280021-01 IHSX3180 IHSX3280 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280022-01 IHSX3181 IHSX3281 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280021-04 IHSX3182 IHSX3282 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280022-04 IHSX3183 IHSX3283 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280017-01 IHSX3188 IHSX3288 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280018-01 IHSX3189 IHSX3289 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280017-04 IHSX3186 IHSX3286 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280018-04 IHSX3187 IHSX3287 Non-Standard
01-0001-2020 Ind HMO Bronze 94788NY0280029-01 IHBX4049 IHBX4149 Non-Standard
01-0001-2020 Ind HMO Bronze 94788NY0280030-01 IHBX4050 IHBX4150 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280145-01 IHBX4051 IHBX4151 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280146-01 IHBX4052 IHBX4152 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280147-01 New Plan IHPX5101 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280148-01 New Plan IHPX5102 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280149-01 New Plan IHSX5101 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280150-01 New Plan IHSX5102 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280149-04 New Plan IHSX5103 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280150-04 New Plan IHSX5104 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280053-01 IHPX1036 IHPX1038 Standard
01-0001-2020 Ind HMO Platinum 94788NY0280064-01 IHPX1037 IHPX1039 Standard
01-0001-2020 Ind HMO Gold 94788NY0280054-01 IHGX2037 IHGX2039 Standard
01-0001-2020 Ind HMO Gold 94788NY0280065-01 IHGX2038 IHGX2040 Standard
01-0001-2020 Ind HMO Silver 94788NY0280055-01 IHSX3190 IHSX3198 Standard
AP AQ AR AS AT AU AV AW AX
OON Max
Family
Aggregate/
EmbeddedProduct Line Benefit Type Rx Benefit Riders Additional Benefits
Additional
BenefitsAdditional Benefits
N/A Embedded HMO Transitional $1/10%/40% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Transitional $1/10%/40% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Transitional $1/20%/50% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Transitional $1/20%/50% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible $4/50%/50% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible $4/50%/50% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible 10%/20%/30% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible 10%/20%/30% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Smart Deductible
$4/30%/50% (Tier 1
not subject to
deductible)
No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Smart Deductible
$4/30%/50% (Tier 1
not subject to
deductible)
Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Smart Deductible 40%/40%/40% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Smart Deductible 40%/40%/40% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible 50%/50%/50% No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible 50%/50%/50% Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HDHMO Qualified High Deductible $0/$0/$0 No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HDHMO Qualified High Deductible $0/$0/$0 Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Copayment $5/$15/$45 No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Copayment $5/$15/$45 Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible $10/$50/$80 No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible $10/$50/$80 Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible $10/$50/$80 No Riders Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Aggregate HDHMO Qualified High Deductible $10/$50/$80 Age 29 Adult Vision Exam/HWSNF - 200 to
365 daysAcupuncture
N/A Embedded HMO Copayment $10/$30/$60 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$30/$60 Age 29 No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$35/$70 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$35/$70 Age 29 No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$35/$70 No Riders No Riders No Riders No Riders
Page 202013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code 2020 Plan Code Standard?
01-0001-2020 Ind HMO Silver 94788NY0280055-04 IHSX3191 IHSX3199 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280055-05 IHSX3192 IHSX3200 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280055-06 IHSX3193 IHSX3201 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280066-01 IHSX3194 IHSX3202 Standard
01-0001-2020 Ind HMO Silver 94788NY0280066-04 IHSX3195 IHSX3203 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280066-05 IHSX3196 IHSX3204 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280066-06 IHSX3197 IHSX3205 Silver CSR
01-0001-2020 Ind HMO Bronze 94788NY0280059-01 IHBX4053 IHBX4055 Standard
01-0001-2020 Ind HMO Bronze 94788NY0280070-01 IHBX4054 IHBX4056 Standard
01-0004-2020 Ind HMO Platinum 94788NY0280081-01 IHPXC022 IHPXC025 Standard
01-0004-2020 Ind HMO Gold 94788NY0280080-01 IHGXC024 IHGXC026 Standard
01-0004-2020 Ind HMO Silver 94788NY0280082-01 IHSXC036 IHSXC040 Standard
01-0004-2020 Ind HMO Silver 94788NY0280082-04 IHSXC037 IHSXC041 Silver CSR Child
01-0004-2020 Ind HMO Silver 94788NY0280082-05 IHSXC038 IHSXC042 Silver CSR Child
01-0004-2020 Ind HMO Silver 94788NY0280082-06 IHSXC039 IHSXC043 Silver CSR Child
01-0004-2020 Ind HMO Bronze 94788NY0280079-01 IHBXC025 IHBXC026 Standard
01-0005-2020 Ind HMO Catastrophic 94788NY0280047-01 IHCX5006 IHCX5008 Standard
AP AQ AR AS AT AU AV AW AX
OON Max
Family
Aggregate/
EmbeddedProduct Line Benefit Type Rx Benefit Riders Additional Benefits
Additional
BenefitsAdditional Benefits
N/A Embedded HMO Copayment $10/$35/$70 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $9/$20/$40 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $6/$15/$30 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$35/$70 Age 29 No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$35/$70 Age 29 No Riders No Riders No Riders
N/A Embedded HMO Copayment $9/$20/$40 Age 29 No Riders No Riders No Riders
N/A Embedded HMO Copayment $6/$15/$30 Age 29 No Riders No Riders No Riders
N/A Embedded HDHMO Qualified High Deductible $10/$35/$70 No Riders No Riders No Riders No Riders
N/A Embedded HDHMO Qualified High Deductible $10/$35/$70 Age 29 No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$30/$60 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$35/$70 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$35/$70 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $10/$35/$70 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $9/$20/$40 No Riders No Riders No Riders No Riders
N/A Embedded HMO Copayment $6/$15/$30 No Riders No Riders No Riders No Riders
N/A Embedded HDHMO Qualified High Deductible $10/$35/$70 No Riders No Riders No Riders No Riders
N/A Aggregate HDHMONon Qualified High
Deductible$0/$0/$0 No Riders No Riders No Riders No Riders
Page 212013 UBI SG Base Medical

Capital District Physicians' Health Plan
Benefit Summary
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code 2020 Plan Code Standard?
01-0001-2020 Ind HMO Platinum 94788NY0280129-01 IHPX1034 IHPX1136 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280130-01 IHPX1035 IHPX1137 Non-Standard
01-0001-2020 Ind HMO Gold 94788NY0280131-01 IHGX2035 IHGX2135 Non-Standard
01-0001-2020 Ind HMO Gold 94788NY0280132-01 IHGX2036 IHGX2136 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280021-01 IHSX3180 IHSX3280 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280022-01 IHSX3181 IHSX3281 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280021-04 IHSX3182 IHSX3282 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280022-04 IHSX3183 IHSX3283 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280017-01 IHSX3188 IHSX3288 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280018-01 IHSX3189 IHSX3289 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280017-04 IHSX3186 IHSX3286 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280018-04 IHSX3187 IHSX3287 Non-Standard
01-0001-2020 Ind HMO Bronze 94788NY0280029-01 IHBX4049 IHBX4149 Non-Standard
01-0001-2020 Ind HMO Bronze 94788NY0280030-01 IHBX4050 IHBX4150 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280145-01 IHBX4051 IHBX4151 Non-Standard
01-0002-2020 Ind HMO Bronze 94788NY0280146-01 IHBX4052 IHBX4152 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280147-01 New Plan IHPX5101 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280148-01 New Plan IHPX5102 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280149-01 New Plan IHSX5101 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280150-01 New Plan IHSX5102 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280149-04 New Plan IHSX5103 Non-Standard
01-0001-2020 Ind HMO Silver 94788NY0280150-04 New Plan IHSX5104 Non-Standard
01-0001-2020 Ind HMO Platinum 94788NY0280053-01 IHPX1036 IHPX1038 Standard
01-0001-2020 Ind HMO Platinum 94788NY0280064-01 IHPX1037 IHPX1039 Standard
01-0001-2020 Ind HMO Gold 94788NY0280054-01 IHGX2037 IHGX2039 Standard
01-0001-2020 Ind HMO Gold 94788NY0280065-01 IHGX2038 IHGX2040 Standard
01-0001-2020 Ind HMO Silver 94788NY0280055-01 IHSX3190 IHSX3198 Standard
Ay
Additional non EHB BenefitsAdditional non
EHB Benefits
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
Lasik Surgery ($750 Max)Gym
Membership
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
Page 222013 UBI SG Base Medical
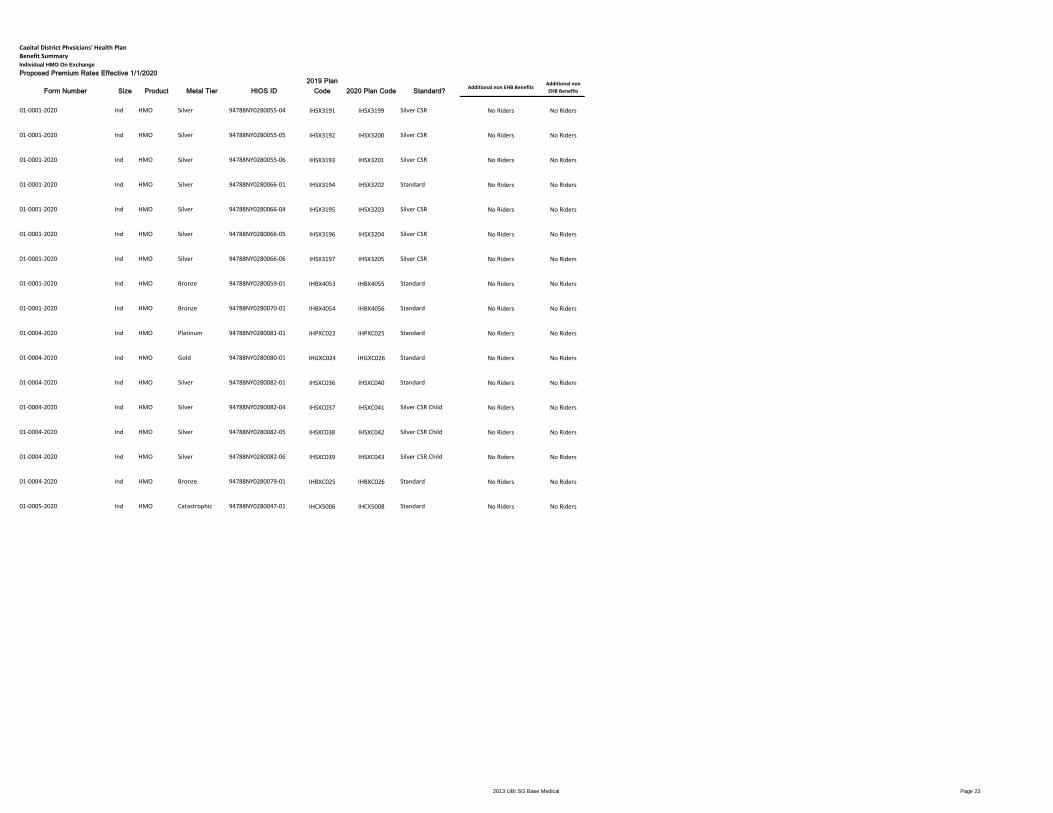
Capital District Physicians' Health Plan
Benefit Summary
Individual HMO On Exchange
Proposed Premium Rates Effective 1/1/2020 J
Form Number Size Product Metal Tier HIOS ID
2019 Plan
Code 2020 Plan Code Standard?
01-0001-2020 Ind HMO Silver 94788NY0280055-04 IHSX3191 IHSX3199 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280055-05 IHSX3192 IHSX3200 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280055-06 IHSX3193 IHSX3201 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280066-01 IHSX3194 IHSX3202 Standard
01-0001-2020 Ind HMO Silver 94788NY0280066-04 IHSX3195 IHSX3203 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280066-05 IHSX3196 IHSX3204 Silver CSR
01-0001-2020 Ind HMO Silver 94788NY0280066-06 IHSX3197 IHSX3205 Silver CSR
01-0001-2020 Ind HMO Bronze 94788NY0280059-01 IHBX4053 IHBX4055 Standard
01-0001-2020 Ind HMO Bronze 94788NY0280070-01 IHBX4054 IHBX4056 Standard
01-0004-2020 Ind HMO Platinum 94788NY0280081-01 IHPXC022 IHPXC025 Standard
01-0004-2020 Ind HMO Gold 94788NY0280080-01 IHGXC024 IHGXC026 Standard
01-0004-2020 Ind HMO Silver 94788NY0280082-01 IHSXC036 IHSXC040 Standard
01-0004-2020 Ind HMO Silver 94788NY0280082-04 IHSXC037 IHSXC041 Silver CSR Child
01-0004-2020 Ind HMO Silver 94788NY0280082-05 IHSXC038 IHSXC042 Silver CSR Child
01-0004-2020 Ind HMO Silver 94788NY0280082-06 IHSXC039 IHSXC043 Silver CSR Child
01-0004-2020 Ind HMO Bronze 94788NY0280079-01 IHBXC025 IHBXC026 Standard
01-0005-2020 Ind HMO Catastrophic 94788NY0280047-01 IHCX5006 IHCX5008 Standard
Ay
Additional non EHB BenefitsAdditional non
EHB Benefits
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
No Riders No Riders
Page 232013 UBI SG Base Medical

Exhibit C
Capital District Physicians' Health Plan
Individual
Conversion Factor Summary - 4-tier only
IV. Conversion Factor
Average Weighted Desired Weighted
Contract Contract Contract Loading Loading Conversion
Mix Size Size Factors Factors Factor
Four Tier Premiums
Single 68.6% 1.00 0.686 1.000 0.686
Double 21.8% 2.00 0.436 2.000 0.436
Emp/Child(ren) 2.9% 2.55 0.074 1.700 0.050
Family 6.7% 3.80 0.255 2.850 0.191
Total 4T 100.0% 1.451 1.362
1.065
2019 Filed 1.081
Page 24

V. Area Factors
2020 Rating Factors
Rating Region
Region 1
(Albany Area)
Region 3
(Mid-Hudson Area)
Region 6
(Syracuse Area)
Region 7
(Utica/Watertown
Area)
Regional Rating Factor 0.9686 1.3843 1.0972 1.0839
Normalized to Albany Area 1.0000 1.4292 1.1328 1.1191
Counties: Albany Delaware Broome Chenango
Columbia Dutchess Tioga Clinton
Fulton Orange Essex
Greene Ulster Franklin
Montgomery Hamilton
Rensselaer Herkimer
Saratoga Madison
Schenectady Oneida
Schoharie Otsego
Warren
Washington
Capital District Physicians' Health Plan
HMO Products
Regional Area Factors
EXEMPTION FROM FOIL REQUESTED
Page 25

VI. Tier Factors
22020 Rating Factors
Rating Method Contract Type Small Group
4-Tier Individual 1
Employee + Spouse 2.00
Employee + Child(ren) 1.70
Family 2.85
Capital District Physicians' Health Plan
HMO Product
Tier Factors
Page 26

VI. Rate Calculation
Plan Code Single Double Emp/Child(ren) Family
IHPX1136 $890.75 1,781.50$ 1,514.28$ 2,538.64$
Final Rates $890.75 $1,781.50 $1,514.28 $2,538.64
Capital District Physicians' Health Plan
Individual HMO Product
Sample Rate Calculation
Sample rate calculation for a individual on exchange benefit package in the Albany region
Page 27

Capital District Physicians' Health Plan
HMO Product
Expected Loss Ratio
All policy forms in all regions
VIII. Expected Loss Ratio
86.4%
Page 28

Capital District Physicians' Health Plan
Individual HMO Product
Broker Commissions
Page 29

Base Plan Base Plan Variation Adjustment
Characteristic Factor Characteristic FactorWithout Through Age 29 Coverage 1.000 With Through Age 29 Coverage 1.0050
With Family Planning Coverage 1.000 Without Family Planning Coverage 0.9924
With Domestic Partner Coverage 1.000 Without Domestic Partner Coverage 1.0000
Without Pediatric Dental Coverage 1.000 With Pediatric Dental Coverage N/A
Capital District Physicians' Health Plan
HMO Product
Factors for Base Plan Variations
Page 30

Supporting Document Schedules Satisfied - Item: Actuarial Value CalculationsComments:Attachment(s): AV Screenshots - INDV.pdfItem Status:Status Date:
Satisfied - Item: Exhibit 13a: Numerical Summary and Rate Indication CalculationComments:
Attachment(s): 2020_exh13A_04022019 INDV.pdf2020_exh13A_04022019 INDV.xlsm
Item Status:Status Date:
Satisfied - Item: Exhibit 13b: Narrative SummaryComments:Attachment(s): 2020_exh13B_04022019 INDV.pdfItem Status:Status Date:
Satisfied - Item: Exhibit 13c: Average Premium DetailsComments:
Attachment(s): 2020_exh13C_04022019 INDV.pdf2020_exh13C_04022019 INDV.xlsm
Item Status:Status Date:
Satisfied - Item: Exhibit 14: Summary of Requested Percentage ChangesComments:
Attachment(s): 2020_exh14_04022019 INDV.pdf2020_exh14_04022019 INDV.xlsm
Item Status:Status Date:
Bypassed - Item: Exhibit 15a: Product Discontinuance CertificationBypass Reason: Not DiscontinuingAttachment(s):
SERFF Tracking #: CAPD-131909302 State Tracking #: 2019050149 Company Tracking #: 2020 INDV RATE
State: New York Filing Company: Capital District Physicians Health Plan Inc
TOI/Sub-TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)/HOrg02I.005D Individual - HMO
Product Name: 2020 Individual Rate
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number CAPD-131909302 Generated 05/21/2019 09:06 AM

Item Status:Status Date:
Satisfied - Item: Exhibit 16: Summary of Policy Form & Product ChangesComments:
Attachment(s): 2020_exh16_04022019 INDV.pdf2020_exh16_04022019 INDV.xlsm
Item Status:Status Date:
Satisfied - Item: Exhibit 17: Claims ExperienceComments:
Attachment(s): 2020_exh17_04022019 INDV.pdf2020_exh17_04022019 INDV.xlsm
Item Status:Status Date:
Satisfied - Item: Exhibit 18: Index Rate/Plan-Design Level AdjustmentComments:
Attachment(s): 2020_exh18_04022019 INDV.pdf2020_exh18_04022019 INDV.xlsm
Item Status:Status Date:
Satisfied - Item: Exhibit 19: Summary of Average Claim Trend and Admin Expenses and Profit MarginComments:
Attachment(s): 2020_exh19_04022019 INDV.pdf2020_exh19_04022019 INDV.xlsm
Item Status:Status Date:
Satisfied - Item: Exhibit 23: Summary of Requested 2019 Premium RatesComments:
Attachment(s): 2020_exh23_04022019 INDV.pdf2020_exh23_04022019 INDV.xlsm
Item Status:Status Date:
Satisfied - Item: Final Notice of Proposed Rate Adjustment
SERFF Tracking #: CAPD-131909302 State Tracking #: 2019050149 Company Tracking #: 2020 INDV RATE
State: New York Filing Company: Capital District Physicians Health Plan Inc
TOI/Sub-TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)/HOrg02I.005D Individual - HMO
Product Name: 2020 Individual Rate
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number CAPD-131909302 Generated 05/21/2019 09:06 AM

Comments:
Attachment(s): Renewal_Ind_Off_NYSOH.pdfRenewal_Ind_On_NYSOH.pdf
Item Status:Status Date:
Satisfied - Item: Initial Notice of Proposed Rate AdjustmentComments:Attachment(s): 19-11324 2020 Initial Notice Individuals FINAL.pdfItem Status:Status Date:
Satisfied - Item: Redacted Documents for Web PostingComments:
Attachment(s):
1. 2020 Actuarial Memorandum - Individual_Redacted.pdf2020_checklist_filing_INDV_Redacted.pdf2020_exh11_04022019 INDV_Redacted.pdf2020_exh11_04022019 INDV_Redacted.xlsm2020_exh15B_MHPAEA_Cert_04022019_REDACTED.pdf
Item Status:Status Date:
Satisfied - Item: Unified Rate Review TemplateComments:
Attachment(s): 2020_URRT_INDV.pdf2020_URRT_INDV.xlsm
Item Status:Status Date:
SERFF Tracking #: CAPD-131909302 State Tracking #: 2019050149 Company Tracking #: 2020 INDV RATE
State: New York Filing Company: Capital District Physicians Health Plan Inc
TOI/Sub-TOI: HOrg02I Individual Health Organizations - Health Maintenance (HMO)/HOrg02I.005D Individual - HMO
Product Name: 2020 Individual Rate
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number CAPD-131909302 Generated 05/21/2019 09:06 AM












EXHIBIT 13a: NUMERICAL SUMMARY AND RATE INDICATION CALCULATION
NUMERICAL SUMMARY
CDPHP
95491
SERFF Tracking #: CAPD-131909302
Market Segment: Individual
1 Please complete the Numerical Summary below as well as the Narrative Summary (a separate attachment) for each market segment for which a rate filing is being submitted.
2 The Narrative Summary must be in plain English and should clearly and simply explain the reasons for the requested rate adjustment (This should be included in the provided blank template "2020 Exhibit 13b - Narrative Summary.docx")
3 The purpose of the Narrative Summary is to provide a written explanation to the company's policyholders to help them understand the reasons why a rate increase is needed.
4 The purpose of the Numerical Summary is to provide a clear and simple overview of the requested rate adjustment.
5 These Summaries (with the exception of the Rate Indication Calculation Section) will be public documents and will be posted on DFS’s website and furnished by DFS to the public upon request.
6 The company should submit these Summaries to DFS ten (10) days before submitting a rate adjustment filing.
7 A draft of these Summaries and of the Initial Notice must be included in a "Prior Approval Pre-filing" submitted to DFS via SERFF.
8 Once reviewed by DFS, these Summaries must be posted to a location on its website that is publicly available and accessible without the need for a user ID/password.
9 Links should be provided on key pages of the company's website so that the information may be easily located.
10 Any change(s) made to the Narrative Summary/Numerical Summary subsequent to the posting must be submitted to DFS with the specific change(s) identified.
11 Rate Change Adjustment calculations between Year 2019 and 2020 should be based on the DFS Membership Survey data as of 3/31/2019.
12 This exhibit must be submitted as an Excel file and as a PDF file.
A. Average 2019 and 2020 Premium Rates:
1 Weighted Average Monthly Base Premium Rates are as calculated in Row 32 of the appropriate columns in Exhibit 13c (Columns L-P for 2019 and Columns U-Y for 2020)
2 Premium Rates for 2020 should be Consistent with the Premium Rates reflected in Exhibit 23.
Average Individual Rate Average Individual Rate Average Individual Rate Average Individual Rate Average Individual Rate
Platinum Gold Silver Bronze Catastrophic
2019 Weighted Average Base Premium Rates $868.44 $736.79 $606.67 $442.95 $246.92
2020 Weighted Average Base Premium Rates $936.84 $779.41 $630.21 $465.61 $238.33
B. Weighted Average Annual Percentage Requested Adjustments:
2019 Weighted Average PMPM Rate 2020 Weighted Average PMPM Rate
2019 to 2020 All - Metals All - Metals
Requested Rate Adjustment 7.04966% $545.56 $584.03 From Cells Q-74 and Z-74 of Exhibit 13c
C. Weighted Average Annual Percentage Adjustments for each of the Past Two Years [If Applicable]*:
2017 to 2018 2018 to 2019
Average Rate Adjustment Requested 15.23021% 5.04629%
Average Rate Adjustment Approved 14.90000% -1.90454%
D. Average Medical Loss Ratios [MLR] for All Policies Impacted [Ratios of Incurred Claims to Earned Premiums] [If Applicable]*:
2016 2017 2018
MLR 99.5% 93.4% 81.3%
E. Claim Trend Rates and Average Ratios to Earned Premiums [Per Exhibit 19 for 2018-2020 and Comparable Exhibits for 2018] [If Applicable]*:
2018 2019 2020
Annual Claim Trend Rates 5.5% 5.5% 6.7%
Expense Ratios 9.1% 9.5% 12.6%
Pre Tax Profit Ratios 1.0% 1.0% 1.0%
* If no products were offered in a particular year, indicate "N/A" in the applicable box.
Company
NAIC Code:
Exhibit 13a Updated by DFS 3/14/2018 1

Exhibit 13b – Narrative Summary Last Updated: 4/3/2019
EXHIBIT 13b: NARRATIVE SUMMARY
Company Name: CDPHP
NAIC Code: 95491
SERFF Tracking #: CAPD-131909302
Market Segment: Individual
Capital District Physicians’ Health Plan, Inc. (CDPHP®) offers a health maintenance organization (HMO) product on a community-rated, direct-pay basis to individuals. CDPHP has filed a request for approval by the New York State Department of Financial Services for a change to the premium for this product effective January 1, 2020. Policyholders will receive rate adjustments upon their renewal in 2020. The weighted average single premium rate increase is 5.5%. 5,812 members and 4,118 policyholders are affected by this request. As a not-for-profit health plan, CDPHP takes seriously its responsibility to control rising health care costs and be a good steward of your premium dollars. However, we continue to battle the rising cost of care, driven primarily by state and federal regulations and taxes, specialty drugs, and provider consolidation. These factors have resulted in the need to increase insurance premiums. We are working hard to alleviate these cost increases in a variety of ways, such as:
The CDPHP Enhanced Primary Care (EPC) program, a nationally-recognized patient-centered medical home that encourages high-quality, cost-effective services at the primary care level.
Dedicating resources to improving the overall health of our membership.
Easier and more convenient access to care through our telemedicine (live video doctor visits) partner, Doctor On Demand.
CDPHP Price Check, a cost transparency tool that provides members estimated costs on a range of health care services.
Movement of services to more cost-effective outpatient settings, such as freestanding surgical centers.
Case management and medication therapy management services, available at no out-of-pocket cost.
Mental health and substance use programs, including access to a 24-hour crisis line. DFS’s view of these matters may differ. The 2020 expected change in medical and pharmacy costs due to trend is +6.7%. Federal Risk Adjustment is a program that requires insurance carriers with low-risk members to pay into a fund that covers high-risk members. As a result of an increase in the anticipated receivable from this program, the impact on the rates is -5.2%. Federal ACA fees were reinstated for 2020 and will have an unfavorable impact of 1.0%. CDPHP is required by New York state insurance law to meet a minimum Medical Loss Ratio (MLR) standard of 82%. This means that 82% of premiums must be used to cover health care costs. CDPHP will exceed this minimum requirement in 2020 with an MLR of 86.4%.

EXHIBIT 13C - AVERAGE PREMIUM DETAILS
Company Name: CDPHP
NAIC Code: 95491
SERFF Tracking #: CAPD-131909302
Market Segment: Individual
1 Please complete all of the shaded boxes in rows 24-47 below. The goal of this Exhibit is to calculate the rate change being requested in a consistent manner for all insurers.
2 The "Weighted Average Monthly Base Premiums" in cells C24-G31 should be calculated as a weighted average of the insurer's base premiums (i.e., single adult rates prior to application of tier factors, etc.) using the number of plan subscribers as the weights.
3 Cells L24 - P31, should be a recalculation of cells C24-G31 where any plans (and associated members enrolled in those plans as of 3/31/2019) that will no longer be offered in 2020 are removed.
The sum of cells C37-G44 should be equal to the Company's total membership for the relevant market as of 3/31/2019.
4 Cells L37-P44 should be equal to cells C37-G44 less any members that are enrolled in plans that will no longer be offered in 2020.
5 If the Company is not eliminating any plans in 2020, then cells C24-G31 and L24-P31 should be the same, as should cells C37-G44 and L37-P44.
6 The "Conversion Factors" should be the factors that were developed in pricing to convert the "Weighted Average Monthly Base Premiums" to "Weighted Average Monthly PMPM Premium Rates". These factors should be adjusted as necessary to reflect any changes that are not reflected in the Base Premiums.
7 The value in cell Q74 of this Exhibit should match cell D96 (Line 54) of Exhibit 18.
8 The value in cell Z74 of this Exhibit should match cell D102 (Line 56) of Exhibit 18.
2019 Weighted Average Monthly Base Premiums - CALCULATED BASED ON ACTUAL DISTRIBUTION AS OF 3/31/2019 (Weighted by number 2019 Weighted Average Monthly Base Premiums - RE-CALCULATED USING ONLY THE SUBSET OF 2019 PLANS THAT WILL STILL
of subscribers) BE AVAILABLE IN 2020 (weighted by subscribers in those specific plans)
Average Monthly Base Premium assuming 3/31/2019 membership Average Monthly Base Premium paid assuming 3/31/2019 membership and all policies are paid in full for the entire year)
Region Platinum Gold Silver Bronze Catastrophic All Metals Region Platinum Gold Silver Bronze Catastrophic All Metals
1 - Albany Area $819.43 $700.65 $559.61 $404.74 $246.92 555.71 1 - Albany Area $819.43 $700.65 $559.61 $404.74 $246.92 555.71
2 -Buffalo Area 2 -Buffalo Area
3- Mid-Hudson Area $1,179.84 $985.87 $805.98 $577.88 742.02 3- Mid-Hudson Area $1,179.84 $985.87 $805.98 $577.88 742.02
4- NYC Area 4- NYC Area
5- Rochester Area 5- Rochester Area
6- Syracuse Area $988.76 $848.56 $668.56 $483.89 645.72 6- Syracuse Area $988.76 $848.56 $668.56 $483.89 645.72
7- Utica/Watertown Area $971.87 $832.69 $643.48 $477.50 596.17 7- Utica/Watertown Area $971.87 $832.69 $643.48 $477.50 596.17
8- Long Island Area 8- Long Island Area
9 - All Regions 868.44 736.79 606.67 442.95 246.92 589.59 9 - All Regions 868.44 736.79 606.67 442.95 246.92 589.59 To Exhibit 13a (Section A)
2019 Members - as of 3/31/2019 - Actual Distribution (All members as of 3/31/2019 should be included) Members - as of 3/31/2019 - Only those members currently enrolled in plans that will continue to be offered in 2020
Region Platinum Gold Silver Bronze Catastrophic All Metals Region Platinum Gold Silver Bronze Catastrophic All Metals
1 - Albany Area 749 692 1,156 1,982 10 4,589 1 - Albany Area 749 692 1,156 1,982 10 4,589
2 -Buffalo Area 2 -Buffalo Area
3- Mid-Hudson Area 107 94 259 526 0 986 3- Mid-Hudson Area 107 94 259 526 - 986
4- NYC Area 4- NYC Area
5- Rochester Area 5- Rochester Area
6- Syracuse Area 11 4 26 32 0 73 6- Syracuse Area 11 4 26 32 - 73
7- Utica/Watertown Area 20 12 32 100 0 164 7- Utica/Watertown Area 20 12 32 100 - 164
8- Long Island Area 8- Long Island Area
9 - All Regions 887 802 1,473 2,640 10 5,812 9 - All Regions 887 802 1,473 2,640 10 5,812 Should equal Cell H-24 of Exhibit 14
2019 Conversion Factor - A 0.9253 Must be less than or equal to 1.000 2019 Conversion Factor - B 0.9253 Must be less than or equal to 1.000
2019 Estimated Aggregate Annualized Premium by Metal and Region - based on membership as of 3/31/2019 2019 Estimated Aggregate Annualized Premium by Metal and Region - based on membership as of 3/31/2019
Aggregate premium that would be collected assuming 3/31/2019 membership and all policies are paid in full for the entire year) Aggregate premium that would be collected assuming 3/31/2019 membership and all policies are paid in full for the entire year) - Adjusted for plan eliminations
Region Platinum Gold Silver Bronze Catastrophic All Metals Region Platinum Gold Silver Bronze Catastrophic All Metals
1 - Albany Area 6,815,055 5,383,709 7,183,189 8,907,508 27,418 28,316,879 1 - Albany Area 6,815,055 5,383,709 7,183,189 8,907,508 27,418 28,316,879
2 -Buffalo Area 2 -Buffalo Area
3- Mid-Hudson Area 1,401,789 1,029,025 2,317,929 3,375,199 8,123,943 3- Mid-Hudson Area 1,401,789 1,029,025 2,317,929 3,375,199 8,123,943
4- NYC Area 4- NYC Area
5- Rochester Area 5- Rochester Area
6- Syracuse Area 120,770 37,689 193,015 171,938 523,412 6- Syracuse Area 120,770 37,689 193,015 171,938 523,412
7- Utica/Watertown Area 215,832 110,953 228,644 530,217 1,085,645 7- Utica/Watertown Area 215,832 110,953 228,644 530,217 1,085,645
8- Long Island Area 8- Long Island Area
9 - All Regions 8,553,445 6,561,376 9,922,778 12,984,861 27,418 38,049,878 9 - All Regions 8,553,445 6,561,376 9,922,778 12,984,861 27,418 38,049,878 Should equal Cell G-24 of Exhibit 14
2019 Weighted Average Monthly PMPM Premium Rates 2019 Weighted Average Monthly PMPM Premium Rates - Reflecting adjustment for eliminated plans
Region Platinum Gold Silver Bronze Catastrophic All Metals Region Platinum Gold Silver Bronze Catastrophic All Metals
1 - Albany Area 758.24 648.33 517.82 374.52 228.48 514.22 1 - Albany Area 758.24 648.33 517.82 374.52 228.48 514.22
2 -Buffalo Area 2 -Buffalo Area
3- Mid-Hudson Area 1,091.74 912.26 745.79 534.73 686.61 3- Mid-Hudson Area 1,091.74 912.26 745.79 534.73 686.61
4- NYC Area 4- NYC Area
5- Rochester Area 5- Rochester Area
6- Syracuse Area 914.92 785.19 618.64 447.75 597.50 6- Syracuse Area 914.92 785.19 618.64 447.75 597.50
7- Utica/Watertown Area 899.30 770.51 595.43 441.85 551.65 7- Utica/Watertown Area 899.30 770.51 595.43 441.85 551.65
8- Long Island Area 8- Long Island Area
9 - All Regions 803.59 681.77 561.37 409.88 228.48 545.56 9 - All Regions 803.59 681.77 561.37 409.88 228.48 545.56 To Exhibit 13a (Section B)
Exhibit 13c Updated by DFS 3/14/2018 1

2020 Weighted Average Monthly Proposed Base Premiums - THESE BASE PREMIUMS SHOULD BE CALCULATED USING THE SAME Change in Weighted Average Monthly Base Premiums
POPULATION OF SUBSCRIBERS THAT WAS USED TO CALCULATE CELLS L22 - P29)
Average Base Premium paid assuming 3/31/2019 membership and all policies are paid in full for the entire year) Average Base Premium paid assuming 3/31/2019 membership and all policies are paid in full for the entire year)
Region Platinum Gold Silver Bronze Catastrophic All Metals Region Platinum Gold Silver Bronze Catastrophic All Metals
1 - Albany Area $886.09 $742.44 $582.95 $426.96 $238.33 588.35 1 - Albany Area 8.14% 5.96% 4.17% 5.49% -3.48% 5.87%
2 -Buffalo Area 2 -Buffalo Area
3- Mid-Hudson Area $1,273.40 $1,040.82 $837.20 $607.74 781.54 3- Mid-Hudson Area 7.93% 5.57% 3.87% 5.17% 5.33%
4- NYC Area 4- NYC Area
5- Rochester Area 5- Rochester Area
6- Syracuse Area $1,009.30 $849.33 $660.57 $482.65 645.47 6- Syracuse Area 2.08% 0.09% -1.20% -0.26% -0.04%
7- Utica/Watertown Area $997.09 $840.03 $637.71 $478.53 599.28 7- Utica/Watertown Area 2.60% 0.88% -0.90% 0.22% 0.52%
8- Long Island Area 8- Long Island Area
9 - All Regions 936.84 779.41 630.21 465.61 238.33 622.15 To Exhibit 13a (Section A) 9 - All Regions 7.88% 5.78% 3.88% 5.11% -3.48% 5.52%
Members - as of 3/31/2019 - Only those members currently enrolled in plans that will continue to be offered in 2020 Change in Members - as of 3/31/2019 - Change due to current 2019 plans not being offered in 2020.
Region Platinum Gold Silver Bronze Catastrophic All Metals Region Platinum Gold Silver Bronze Catastrophic All Metals
1 - Albany Area 749 692 1,156 1,982 10 4,589 1 - Albany Area 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
2 -Buffalo Area 2 -Buffalo Area
3- Mid-Hudson Area 107 94 259 526 986 3- Mid-Hudson Area 0.00% 0.00% 0.00% 0.00% 0.00%
4- NYC Area 4- NYC Area
5- Rochester Area 5- Rochester Area
6- Syracuse Area 11 4 26 32 73 6- Syracuse Area 0.00% 0.00% 0.00% 0.00% 0.00%
7- Utica/Watertown Area 20 12 32 100 164 7- Utica/Watertown Area 0.00% 0.00% 0.00% 0.00% 0.00%
8- Long Island Area 8- Long Island Area
Should equal Cell H-24 of Exhibit 14 9 - All Regions 887 802 1,473 2,640 10 5,812 9 - All Regions 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
2020 Conversion Factor 0.9387 Must be less than or equal to 1.000 Change in Conversion Factor 1.44729%
2020 Estimated Aggregate Annualized Premium by Metal and Region - based on membership as of 3/31/2019 Change in Aggregate Annualized Premiums - based on membership as of 3/31/2019 (Ignoring any plan eliminations)
Aggregate premium that would be collected assuming 3/31/2019 membership and all policies are paid in full for the entire year) - Adjusted for plan eliminations
Region Platinum Gold Silver Bronze Catastrophic All Metals Region Platinum Gold Silver Bronze Catastrophic All Metals
1 - Albany Area 7,476,117 5,787,409 7,591,063 9,532,416 26,847 30,413,852 1 - Albany Area 9.70% 7.50% 5.68% 7.02% -2.08% 7.41%
2 -Buffalo Area 2 -Buffalo Area
3- Mid-Hudson Area 1,534,850 1,102,099 2,442,575 3,601,000 8,680,524 3- Mid-Hudson Area 9.49% 7.10% 5.38% 6.69% 6.85%
4- NYC Area 4- NYC Area
5- Rochester Area 5- Rochester Area
6- Syracuse Area 125,064 38,270 193,468 173,979 530,780 6- Syracuse Area 3.56% 1.54% 0.23% 1.19% 1.41%
7- Utica/Watertown Area 224,637 113,552 229,874 539,047 1,107,111 7- Utica/Watertown Area 4.08% 2.34% 0.54% 1.67% 1.98%
8- Long Island Area 8- Long Island Area
Should equal Cell G-24 of Exhibit 14 9 - All Regions 9,360,668 7,041,329 10,456,980 13,846,442 26,847 40,732,266 9 - All Regions 9.44% 7.31% 5.38% 6.64% -2.08% 7.05%
2020 Weighted Average Monthly PMPM Premium Rates -Reflecting adjustment for eliminated plans Change in Weighted Average PMPM Premiums
Region Platinum Gold Silver Bronze Catastrophic All Metals Region Platinum Gold Silver Bronze Catastrophic All Metals
1 - Albany Area 831.79 696.94 547.22 400.79 223.72 552.30 1 - Albany Area 9.70% 7.50% 5.68% 7.02% -2.08% 7.41%
2 -Buffalo Area 2 -Buffalo Area
3- Mid-Hudson Area 1,195.37 977.04 785.90 570.50 733.65 3- Mid-Hudson Area 9.49% 7.10% 5.38% 6.69% 6.85%
4- NYC Area 4- NYC Area
5- Rochester Area 5- Rochester Area
6- Syracuse Area 947.45 797.28 620.09 453.07 605.91 6- Syracuse Area 3.56% 1.54% 0.23% 1.19% 1.41%
7- Utica/Watertown Area 935.99 788.56 598.63 449.21 562.56 7- Utica/Watertown Area 4.08% 2.34% 0.54% 1.67% 1.98%
8- Long Island Area 8- Long Island Area
9 - All Regions 879.43 731.64 591.59 437.07 223.72 584.03 To Exhibit 13a (Section B) Total 9.44% 7.31% 5.38% 6.64% -2.08% 7.05%
Exhibit 13c Updated by DFS 3/14/2018 2

Company Name: CDPHP
NAIC Code: 95491 NOTE: THIS EXHIBIT SHOULD NOT INCLUDE MEMBERS THAT ARE CURRENTLY ENROLLED IN PLANS THAT WILL NOT BE AVAILABLE IN 2020
SERFF Tracking #: CAPD-131909302
Market Segment: Individual
1
2
3
4
5
6
7
8
9
10
11
12
13 The Total Annualized Premium in Cell G-24 of this Exhibit should equal the total in Cell Q-61 of Exhibit 13c.
14 The Total Number of Members in Cell H-24 of this Exhibit should equal the total in Cell Q-45 of Exhibit 13c (i.e., Only those members currently enrolled in plans that will continue to be offered in 2020)
Totals $38,131,513 5,812 4,118
Annualized Premiums
as of Total # of Members as of
Total # of Contracts
(Certificates for SG) as of
3/31/2019 3/31/2019 3/31/2019 Decrease No Change 0.1% - 4.9% 5.0% - 9.9% 10.0% - 14.9% 15.0% - 19.9% 20.0% - 24.9% 25.0% - 29.9% 30.0% - 39.9% 40.0% - 49.9% 50.0% or higher Lowest Highest Weighted Avg
Individual 01/01/20 Platinum 1 - Albany Area HMO HMO $6,823,965 749 523 0 0 76 673 0 0 0 0 0 0 0 4.42% 8.81% 8.19%
Individual 01/01/20 Gold 1 - Albany Area HMO HMO $5,404,068 692 465 0 0 464 228 0 0 0 0 0 0 0 1.46% 8.96% 5.89%
Individual 01/01/20 Silver 1 - Albany Area HMO HMO $5,773,599 928 654 10 0 588 330 0 0 0 0 0 0 0 -0.29% 5.60% 4.09%
Individual 01/01/20 Bronze 1 - Albany Area HMO HMO 0 0 0 0 0 0 0 0 0 0 0 0 0
Individual 01/01/20 Platinum 3 - Mid-Hudson Area HMO HMO $1,402,387 107 76 0 0 11 96 0 0 0 0 0 0 0 4.13% 8.33% 7.88%
Individual 01/01/20 Gold 3 - Mid-Hudson Area HMO HMO $1,040,859 94 61 0 0 67 27 0 0 0 0 0 0 0 1.17% 8.65% 5.40%
Individual 01/01/20 Silver 3 - Mid-Hudson Area HMO HMO $1,674,896 187 112 1 0 123 63 0 0 0 0 0 0 0 -0.57% 5.31% 3.76%
Individual 01/01/20 Bronze 3 - Mid-Hudson Area HMO HMO 0 0 0 0 0 0 0 0 0 0 0 0 0
Individual 01/01/20 Platinum 6 - Syracuse Area HMO HMO $120,520 11 7 1 0 10 0 0 0 0 0 0 0 0 -1.32% 2.67% 2.29%
Individual 01/01/20 Gold 6 - Syracuse Area HMO HMO $37,767 4 3 3 0 1 0 0 0 0 0 0 0 0 -1.31% 2.97% -0.26%
Individual 01/01/20 Silver 6 - Syracuse Area HMO HMO $140,963 19 14 19 0 0 0 0 0 0 0 0 0 0 -2.36% -0.20% -1.26%
Individual 01/01/20 Bronze 6 - Syracuse Area HMO HMO 0 0 0 0 0 0 0 0 0 0 0 0 0
Individual 01/01/20 Platinum 7 - Utica/Watertown Area HMO HMO $215,893 20 14 3 0 17 0 0 0 0 0 0 0 0 -0.82% 3.19% 2.57%
Individual 01/01/20 Gold 7 - Utica/Watertown Area HMO HMO $110,676 12 10 6 0 6 0 0 0 0 0 0 0 0 -0.81% 3.49% 1.31%
Individual 01/01/20 Silver 7 - Utica/Watertown Area HMO HMO $162,959 23 17 10 0 13 0 0 0 0 0 0 0 0 -5.29% 0.30% -0.71%
Individual 01/01/20 Bronze 7 - Utica/Watertown Area HMO HMO 0 0 0 0 0 0 0 0 0 0 0 0 0
Individual 01/01/20 Silver 1 - Albany Area HDHMO HDHMO $1,426,507 228 172 0 0 228 0 0 0 0 0 0 0 0 4.45% 4.45% 4.45%
Individual 01/01/20 Bronze 1 - Albany Area HDHMO HDHMO $8,916,193 1,982 1,478 0 0 7 1,975 0 0 0 0 0 0 0 0.32% 5.91% 5.49%
Individual 01/01/20 Silver 3 - Mid-Hudson Area HDHMO HDHMO $645,680 72 52 0 0 72 0 0 0 0 0 0 0 0 4.16% 4.32% 4.16%
Individual 01/01/20 Bronze 3 - Mid-Hudson Area HDHMO HDHMO $3,386,087 526 342 0 0 4 522 0 0 0 0 0 0 0 0.04% 5.45% 5.16%
Individual 01/01/20 Silver 6 - Syracuse Area HDHMO HDHMO $52,497 7 5 7 0 0 0 0 0 0 0 0 0 0 -1.29% -1.29% -1.29%
Individual 01/01/20 Bronze 6 - Syracuse Area HDHMO HDHMO $172,024 32 23 32 0 0 0 0 0 0 0 0 0 0 -0.45% -0.06% -0.27%
Individual 01/01/20 Silver 7 - Utica/Watertown Area HDHMO HDHMO $66,343 9 6 9 0 0 0 0 0 0 0 0 0 0 -0.79% -0.79% -0.79%
Individual 01/01/20 Bronze 7 - Utica/Watertown Area HDHMO HDHMO $530,212 100 74 0 0 100 0 0 0 0 0 0 0 0 0.05% 0.45% 0.22%
Individual 01/01/20 Catastrophic 1 - Albany Area HMO HMO $27,418 10 10 10 0 0 0 0 0 0 0 0 0 0 -3.48% -3.48% -3.48%
Individual 01/01/20 Catastrophic 3 - Mid-Hudson Area HMO HMO 0 0 0 0 0 0 0 0 0 0 0 0 0
Individual 01/01/20 Catastrophic 6 - Syracuse Area HMO HMO 0 0 0 0 0 0 0 0 0 0 0 0 0
Individual 01/01/20 Catastrophic 7 - Utica/Watertown Area HMO HMO 0 0 0 0 0 0 0 0 0 0 0 0 0
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Individual
Requested Percentage Rate Change
Percentage Rate Changes should be calculated using membership as of 3/31/2019.
This exhibit must be submitted as an Excel file and as a PDF file.
Market Segment Effective Date of New Rate
Metal Level
(or Catastrophic) Rating Region Product Name Product Street Name
DISTRIBUTION OF MEMBERS - Number of Members with Requested Percentage Rate Change at Renewal
The weighted average percentage should be developed based on annualized premium volume or membership for that metal level, and rating region, including any applicable riders.
EXHIBIT 14: SUMMARY OF REQUESTED PERCENTAGE CHANGES
Use this Exhibit for both Individual and Small Group Market Plans. A separate Exhibit should be provided for Individual and Small Group filings.
Market segment refers to Individual (which includes Catastrophic) or Small Group.
The requested percentage rate change reflects the expected change in premium rates that would apply to the contract holder (or member for Small Group business) on that contract holder's next rate change date for each contract holder within the indicated combination of metal level, rating region, and product name.
The "Product Street Name" is the product name as advertised to consumers (i.e., as consumers are likely to refer to this product/metal level when communicating with DFS). A separate row is to be used for each combination of metal level, rating region and product name.
If the percentage changes (lowest and highest and weighted average) are identical for all the rating regions, then separate rows by rating region need not be used, and "All Regions" can be shown in the Rating Region column. If the rate change range information differs by rating region, then separate rows need to be used for each rating region the
insurer uses. Rating region names used on this exhibit are to use the standard rating region names developed by DFS (e.g., Albany Area, Buffalo Area, etc.).
The "requested rate change" includes the impact of any riders (such as: age 29, domestic partner, family planning, pediatric dental, etc.).
"Lowest" should be the smallest percentage change that could affect any contract holder due to the submitted rate filing with that metal level and rating region, including any applicable riders.
"Highest" should be the largest percentage change that could affect any contract holder due to the submitted rate filing with that metal level and rating region, including any applicable riders.
The effective date is the earliest date that the proposed new rate would become effective if approved. The Effective Date for Individual is 1/1/2020. Effective Dates for Small Group are 1/1/2020, 4/1/2020, 7/1/2020 and 10/1/2020.
Exhibit 14 Updated by DFS 3/14/2018 1

Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment: Individual
Instructions:
1) This Exhibit summarizes all benefit/rate changes filed after the initial rate filing that impacts the rate tables in this current filing.
2)
3)
4) Extend the worksheet to add more rows as needed. Only use the first tab for data entry.
5)
Filing Status SERFF # NY State Tracking # Date of Submission Policy Form #
Product Name (including Street
Name)
Brief Description of Benefit/Rate
Change Approval Date
Pending CAPD-131919825 01-0002-2020
Pending CAPD-131919800 01-0001-2020
EXHIBIT 16: SUMMARY OF POLICY FORM AND PRODUCT CHANGES
The product street name is the product name as advertised to consumers (i.e., as consumers are likely to refer to this product/policy form when communicating with DFS).
Enter filing status (approved or pending) using the drop down list. For pending files leave the approval date blank.
This form must be submitted as an Excel file and as a PDF file.
List of rate filings that have been approved since the §3231(d) or §4308(b) initial rate filing, or are currently pending with DFS.
Exhibit 16 Updated by DFS 3/14/2018 1

EXHIBIT 17: HISTORICAL CLAIM DATA BY POLICY FORMS INCLUDED IN RATE ADJUSTMENT FILING
Company Name:
NAIC Code:
SERFF Number:
Market Segment:
1 Complete a separate ROW for each relevant policy form as indicated below.
• Information requested applies to New York State business only for each rating region and all regions combined.
• Include riders that may be available with that policy form in each policy form response. Discontinued policy forms and products are to be included in the Exhibit.
• Complete additional rows as needed to include all base medical policy forms that were offered in the applicable market segment.
2 This Exhibit must report the latest two years of experience for the following categories of business, broken out by rating region, and for all regions combined:
Market Description
Market Segment (Entry for
Exhibit 17, Column 4)
Group
Definition Counting Method Notes Standardized Premium Scale
Individual ACA Compliant Individual Plans Individual-ACA N/A N/A Issued on or after 1/1/2016 2019 Rates
Catastrophic ACA Compliant Catastrophic Plans Catastrophic N/A N/A Issued on or after 1/1/2016 2019 Rates
Small Group
Experience of ACA Compliant Small Group Plans
(Excluding Healthy New York plans) that were
written or renewed on or after 1/1/2016 SG-ACA-FTE 1-100
Current New York
(FTE)
All relevant experience in
the calendar year
4th Quarter 2019 for rolling;
2019 for non-rolling
Small Group - HNY
Experience of Small Group Healthy New York Plans
that were written or renewed on or after 1/1/2016 SG-ACA-HNY-FTE 1-50
Current New York
(FTE)
All relevant experience in
the calendar year
4th Quarter 2019 for rolling;
2019 for non-rolling
3 Product type is HMO, HMO based POS, POS-OON, EPO, PPO, Comprehensive Major Medical, Non-HMO based POS, and Consumer Health Plans. Indicate appropriate designation for policy form, etc.
4 The product street name is the product name as advertised to consumers (i.e., as consumers are likely to refer to this product/policy form when communicating with DFS.
5 Paid claims in Columns 14.6 - 14.7 and 15.6 - 15.7 are all claims paid during experience period that are attributed to the calendar year in question.
6 If members, covered lives or member months are not known, use reasonable estimates (note methodology used in the actuarial memorandum).
7 This exhibit must be submitted as an Excel file and as a PDF file. Only use the first tab for data entry.
8 These categories should be mutually exclusive (i.e., the sum of the values in a particular column should represent the total for the entire legal entity.
9 With regard to Small Group, the experience reported in this Exhibit should include only business that was considered "Small Group" according to the applicable rules at the time the underlying policies were in-force.
a. Any portion of a group's experience that was considered "Large" based on the rules that were applicable at that time, should not be included in this Exhibit.
CDPHP
95491
CAPD-131909302
Individual
Exhibit 17 - Instructions Last Updated 5/1/2017 1

1.a Company Name
1.b
NAIC
Code 1.c SERFF Number
1d.
Base medical
policy form
number
1e.
Product Name
(per Rate
Manual)
1f.
Product
Street Name
as indicated
to consumers
2.
Filing Type
3.
Effective date of
last rate change
(mm/dd/yy)
4.
Market Segment
5A.
Rating Region
5B.
Product Type (see "Instructions"
tab for examples)
6.
Is a rolling
rate
structure
used for this
base
medical
policy form?
(Yes or No)
7.
Is base medical
policy form open
(new sales
allowed) or closed
(no new sales)
8.
Number of
policyholders
affected by rate
change. (For
group business
this is number
of groups.)
9.
Number of
covered lives
affected by rate
change
CDPHP 95491 CAPD-131909302 01-0001-2020 HMO Individual HMO HMO 1/1/2019 Individual-ACA 1 - Albany Area HMO No New sales allowed 3,302 4,589
CDPHP 95491 CAPD-131909302 01-0001-2020 HMO Individual HMO HMO 1/1/2019 Individual-ACA 3 - Mid-Hudson Area HMO No New sales allowed 643 986
CDPHP 95491 CAPD-131909302 01-0001-2020 HMO Individual HMO HMO 1/1/2019 Individual-ACA 6 - Syracuse Area HMO No New sales allowed 52 73
CDPHP 95491 CAPD-131909302 01-0001-2020 HMO Individual HMO HMO 1/1/2019 Individual-ACA 7 - Utica/Watertown Area HMO No New sales allowed 121 164
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
CDPHP 95491 CAPD-131909302
Data Item for Specified Base Medical Policy Form
Exhibit 17 Updated by DFS 5/1/2017 2

14.1
Beginning Date
of the
experience
period
(mm/dd/y)
14.2
Ending Date of
the experience
period
(mm/dd/yy)
14.3
Member months for
experience period
14.4
Earned premiums for
experience period ($)
14.5
Standardized earned
premiums for experience
period ($)
14.6 Claims Paid
in calendar year 2018 on
claims incurred during
calendar year 2018 -
before any adjustment for
federal risk adjustment,
federal reinsurance, risk
corridors, state stop-loss
pools, or commercial
stop-loss payments ($)
14.6a Claims Paid in
calendar year 2019
(during the months of
January and February
only) on claims incurred
during calendar year
2018 - before any
adjustment for federal
risk adjustment, federal
reinsurance, risk
corridors, state stop-loss
pools, or commercial
stop-loss payments ($)
14.6b Estimated
claims remaining to be
paid in the future on
claims incurred during
2018 - before any
adjustment for federal
risk adjustment, federal
reinsurance, risk
corridors, state stop-loss
pools, or commercial
stop-loss payments ($)
14.6c Rx Rebates
associated with claims
reported in Columns 14.6
and 14.6a (enter as a
positive value) ($)
14.6d Estimated Rx
Rebates associated with
claims reported in
Column 14.6b or not
otherwise included in
14.6c (enter as a positive
value) ($)
14.7 Total
Incurred Claims for
calendar year 2018 Net of
Rx Rebates ($)
14.8
Adjustment to the
incurred claims for the
period due to receipts
from state or federal
reinsurance or stop loss
pools (enter receipts from
the pool as a negative
value) ($)
14.9
Adjustment to the
incurred claims for the
period due to receipts
from or payments to the
federal risk adjustment
pool (enter receipts as a
negative value and
payments to the pool as a
positive value) ($)
14.10
Administrative expenses
for experience period
(including commissions
and premium taxes, but
excluding federal and
state income taxes) ($)
15.1
Beginning date of the
experience period
(mm/dd/yy)
15.2
Ending Date of the
experience period
(mm/dd/yy)
1/1/2018 12/31/2018 50454.00 26,943,362 26,431,438 24,632,770 2,109,937 195,658 1,462,715 0 $ 25,475,649.73 $ - $ (4,312,194) $ 3,809,151 1/1/2017 12/31/2017
1/1/2018 12/31/2018 11335.00 8,173,298 8,018,005 5,803,964 476,563 36,182 328,751 0 $ 5,987,958.01 $ - $ (811,102) $ 856,121 1/1/2017 12/31/2017
1/1/2018 12/31/2018 650.00 429,374 421,216 661,506 41,219 3,129 18,852 0 $ 687,002.78 $ - $ (302,893) $ 49,094 1/1/2017 12/31/2017
1/1/2018 12/31/2018 1376.00 868,564 852,061 593,730 90,209 6,849 39,908 0 $ 650,879.79 $ - $ (51,623) $ 103,928 1/1/2017 12/31/2017
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
2018 Experience Period
(NY statewide experience, base medical policy form + associated riders)
2017 Experience Period
(NY statewide experience, base medical policy form + associated riders)
Exhibit 17 Updated by DFS 5/1/2017 3

15.3
Member months for
experience period
15.4
Earned premiums for
experience period ($)
15.5
Standardized earned
premiums for experience
period ($)
15.6 Claims Paid
in calendar year 2017 on
claims incurred during
calendar year 2017 -
before any adjustment for
federal risk adjustment,
federal reinsurance, risk
corridors, state stop-loss
pools, or commercial
stop-loss payments ($)
15.6a Claims Paid in
calendar year 2018
(during the months of
January and February
only) on claims incurred
during calendar year
2017 - before any
adjustment for federal
risk adjustment, federal
reinsurance, risk
corridors, state stop-loss
pools, or commercial
stop-loss payments ($)
15.6b All other claim
amounts associated with
claims incurred during
the 2017 calendar year
that are not included in
15.6 and 15.6a (i.e.,
Payments through
February of 2019 plus
any remaining IBNR
associated with claims
that were incurred during
2017) - before any
adjustment for federal
risk adjustment, federal
reinsurance, risk
corridors, state stop-loss
pools, or commercial
stop-loss payments ($)
15.6c Rx Rebates
associated with claims
reported in Columns 15.6
and 15.6a (enter as a
positive value) ($)
15.6d Estimated Rx
Rebates associated with
claims reported in
Column 15.6b or not
otherwise included in
15.6c (enter as a positive
value) ($)
15.7 Total
Incurred claims for
calendar year 2017 Net of
Rx Rebates ($)
15.8
Adjustment to the
incurred claims for the
period due to receipts
from state or federal
reinsurance or stop loss
pools (enter receipts from
the pool as a negative
value) ($)
15.9
Adjustment to the
incurred claims for the
period due to receipts
from or payments to the
federal risk adjustment
pool (enter receipts as a
negative value and
payments to the pool as a
positive value) ($)
15.10
Administrative expenses
for experience period
(including commissions
and premium taxes, but
excluding federal and
state income taxes) ($)
40,187 $ 21,200,478 $ 23,896,521 $ 24,418,653 $ 1,326,583 $ 79,116 $ 1,098,259 $ - $ 24,726,092.51 $ - $ (6,998,248) $ 2,631,444
14,026 $ 9,016,904 $ 10,163,575 $ 8,739,816 $ 400,791 $ 65,257 $ 383,313 $ - $ 8,822,551.39 $ - $ (1,297,881) $ 918,422
803 $ 477,625 $ 538,365 $ 494,873 $ 79,732 $ 2,221 $ 21,945 $ - $ 554,881.04 $ - $ (179,366) $ 52,580
1,916 $ 1,051,713 $ 1,185,459 $ 1,440,548 $ 51,693 $ 2,377 $ 52,362 $ - $ 1,442,255.66 $ - $ (306,829) $ 125,460
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
$ -
2017 Experience Period
(NY statewide experience, base medical policy form + associated riders)
Exhibit 17 Updated by DFS 5/1/2017 4

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only Plan 1 Plan 2 Plan 3
1 Product* XXXXXXX 94788NY 94788NY 94788NY
2 Product ID* XXXXXXX 94788NY028 94788NY028 94788NY028
3 Metal Level (or catastrophic)* XXXXXXX Silver Silver Silver
4 AV Metal Value (HHS Calculator)* XXXXXXX 0.71734 0.71734 0.71889
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX 0.71300 0.71300 0.73700
6 Plan Type* XXXXXXX HMO HMO HMO
7 Plan Name* XXXXXXX IHSX3288 IHSX3289 IHSX3280
8 HIOS Plan ID (14 Digits)* XXXXXXX 94788NY0280017 94788NY0280018 94788NY0280021
9 Exchange Plan?* XXXXXXX Both Both Both
9A 2020 Plan Status (as compared to 2019) XXXXXXX Uniform Mod Uniform Mod Uniform Mod
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Amounts should be consistent with appropriate categories in Column 14.3 of Exhibit 17
Experience Period Index Rate Plan 1 Plan 2 Plan 3
10 Earned Premiums for Latest Experience Period # 36,414,597.22 970,479.18 0.00 3,163,483.54
10A Incurred Claims for Latest Experience Period # 32,801,490.30 596,888.55 0.00 2,358,649.93
10B Member-Months for Latest Experience Period # 63,815.00 1,581.00 0.00 5,357.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909 377.53861 0.00000 440.29306
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909 616.53909 616.53909 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans Plan 1 Plan 2 Plan 3
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806 1.01806 1.01806 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans Plan 1 Plan 2 Plan 3
Exhibit 18 Updated by DFS 4/10/2018 1

29 Index Rate - After Marketwide Adjustments 627.6728 627.67279 627.67279 627.67279
30 Pricing actuarial value (without induced demand factor) # 0.7355 0.71300 0.71300 0.73700
31 Pricing actuarial value (only the induced demand factor) # 1.0415 1.03001 1.03001 1.03001
32 Impact of provider network characteristics ## 1.0000 1.00000 1.00000 1.00000
33 Impact of delivery system characteristics ## 1.0000 1.00000 1.00000 1.00000
34 Impact of utilization management practices ## 1.0000 1.00000 1.00000 1.00000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000 1.00000 1.00000 1.00000
36 Benefits in additional to EHB (greater than 1.00) 1.0018 1.00376 1.00376 1.00376
37 Impact of eligibility categories (catastrophic plans only) 0.9992 1.00000 1.00000 1.00000
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000 1.00000 1.00000 1.00000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000 1.00000 1.00000 1.00000
40 Impact of Age 26 / Age 29 1.0001 1.00000 1.00496 1.00000
41 Impact of Family Planning / No Family Planning 1.0000 1.00000 1.00000 1.00000
42 Impact of Dental vs No Dental 1.0000 1.00000 1.00000 1.00000
43 Premium Curve Adjustment 0.9828 1.01938 1.01938 1.01938
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018 1.00725 1.00725 1.00725
43b Rating Region Factor 1.0808 1.07214 1.00022 1.10228
44 Other 1 (specify) 1.0000 1.00000 1.00000 1.00000
45 Other 2 (specify) Child only 0.9693 1.00000 1.00000 1.00000
46 Base Benefit Changes 1.0008 1.00078 1.00078 1.00078
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224 0.81213 0.76141 0.86307
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans Plan 1 Plan 2 Plan 3
49 Plan Expected Costs 503.54 509.75 477.91 541.72
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460 13.20460 13.20460 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520% 10.520% 10.520% 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000% 1.000% 1.000% 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781% 13.754% 13.899% 13.625%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans Plan 1 Plan 2 Plan 3
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56 553.89 516.48 594.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00 416.00 0.00 314.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00 416.00 0.00 314.00
Calculation of Final 2020 Rates All Plans Plan 1 Plan 2 Plan 3
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03 591.04 555.06 627.18
57 Percent Change in Premium Rates (= L56 / L54) 7.05% 6.71% 7.47% 5.49%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans Weighted Average PMPM: 584.03
Difference From Line 56 Col D: 0.00
Overall Average Impact: 7.05% Percentage Difference: 0.0%
Exhibit 18 Updated by DFS 4/10/2018 2

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only
1 Product* XXXXXXX
2 Product ID* XXXXXXX
3 Metal Level (or catastrophic)* XXXXXXX
4 AV Metal Value (HHS Calculator)* XXXXXXX
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX
6 Plan Type* XXXXXXX
7 Plan Name* XXXXXXX
8 HIOS Plan ID (14 Digits)* XXXXXXX
9 Exchange Plan?* XXXXXXX
9A 2020 Plan Status (as compared to 2019) XXXXXXX
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Experience Period Index Rate
10 Earned Premiums for Latest Experience Period # 36,414,597.22
10A Incurred Claims for Latest Experience Period # 32,801,490.30
10B Member-Months for Latest Experience Period # 63,815.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans
Plan 4 Plan 5 Plan 6
94788NY 94788NY 94788NY
94788NY028 94788NY028 94788NY028
Silver Bronze Bronze
0.71889 0.63104 0.63104
0.73700 0.63750 0.63750
HMO HMO HMO
IHSX3281 IHBX4149 IHBX4150
94788NY0280022 94788NY0280029 94788NY0280030
Both Both Both
Uniform Mod Uniform Mod Uniform Mod
Amounts should be consistent with appropriate categories in Column 14.3 of Exhibit 17
Plan 4 Plan 5 Plan 6
34,549.30 4,455,759.06 58,508.62
1,538.93 1,538,755.67 10,919.40
66.00 10,041.00 114.00
23.31712 153.24725 95.78421
616.53909 616.53909 616.53909
Plan 4 Plan 5 Plan 6
1.01806 1.01806 1.01806
Plan 4 Plan 5 Plan 6
Exhibit 18 Updated by DFS 4/10/2018 3

29 Index Rate - After Marketwide Adjustments 627.6728
30 Pricing actuarial value (without induced demand factor) # 0.7355
31 Pricing actuarial value (only the induced demand factor) # 1.0415
32 Impact of provider network characteristics ## 1.0000
33 Impact of delivery system characteristics ## 1.0000
34 Impact of utilization management practices ## 1.0000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000
36 Benefits in additional to EHB (greater than 1.00) 1.0018
37 Impact of eligibility categories (catastrophic plans only) 0.9992
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000
40 Impact of Age 26 / Age 29 1.0001
41 Impact of Family Planning / No Family Planning 1.0000
42 Impact of Dental vs No Dental 1.0000
43 Premium Curve Adjustment 0.9828
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018
43b Rating Region Factor 1.0808
44 Other 1 (specify) 1.0000
45 Other 2 (specify) Child only 0.9693
46 Base Benefit Changes 1.0008
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans
49 Plan Expected Costs 503.54
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00
Calculation of Final 2020 Rates All Plans
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03
57 Percent Change in Premium Rates (= L56 / L54) 7.05%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans
Overall Average Impact: 7.05%
627.67279 627.67279 627.67279
0.73700 0.63750 0.63750
1.03001 1.00001 1.00001
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00376 1.00376 1.00376
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00496 1.00000 1.00496
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.01938 0.87889 0.87889
1.00725 1.00000 1.00000
1.42947 1.09966 1.42947
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00078 1.00078 1.00078
1.12480 0.61894 0.80857
Plan 4 Plan 5 Plan 6
706.01 388.49 507.51
13.20460 13.20460 13.20460
10.520% 10.520% 10.520%
1.000% 1.000% 1.000%
13.144% 14.428% 13.763%
Plan 4 Plan 5 Plan 6
772.91 427.10 556.54
2.00 877.00 9.00
2.00 877.00 9.00
Plan 4 Plan 5 Plan 6
812.85 453.99 588.51
5.17% 6.30% 5.74%
Exhibit 18 Updated by DFS 4/10/2018 4

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only
1 Product* XXXXXXX
2 Product ID* XXXXXXX
3 Metal Level (or catastrophic)* XXXXXXX
4 AV Metal Value (HHS Calculator)* XXXXXXX
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX
6 Plan Type* XXXXXXX
7 Plan Name* XXXXXXX
8 HIOS Plan ID (14 Digits)* XXXXXXX
9 Exchange Plan?* XXXXXXX
9A 2020 Plan Status (as compared to 2019) XXXXXXX
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Experience Period Index Rate
10 Earned Premiums for Latest Experience Period # 36,414,597.22
10A Incurred Claims for Latest Experience Period # 32,801,490.30
10B Member-Months for Latest Experience Period # 63,815.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans
Plan 7 Plan 8 Plan 9
94788NY 94788NY 94788NY
94788NY028 94788NY028 94788NY028
Catastrophic Platinum Gold
0.61074 0.88740 0.80850
0.55000 0.92478 0.83772
HMO HMO HMO
IHCX5008 IHPX1038 IHGX2039
94788NY0280047 94788NY0280053 94788NY0280054
Both Both Both
Uniform Mod Uniform Mod Uniform Mod
Plan 7 Plan 8 Plan 9
33,293.14 3,100,272.19 2,019,409.23
1,607.34 5,504,783.47 1,869,501.47
108.00 3,694.00 2,739.00
14.88278 1490.19585 682.54891
616.53909 616.53909 616.53909
Plan 7 Plan 8 Plan 9
1.01806 1.01806 1.01806
Plan 7 Plan 8 Plan 9
Exhibit 18 Updated by DFS 4/10/2018 5

29 Index Rate - After Marketwide Adjustments 627.6728
30 Pricing actuarial value (without induced demand factor) # 0.7355
31 Pricing actuarial value (only the induced demand factor) # 1.0415
32 Impact of provider network characteristics ## 1.0000
33 Impact of delivery system characteristics ## 1.0000
34 Impact of utilization management practices ## 1.0000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000
36 Benefits in additional to EHB (greater than 1.00) 1.0018
37 Impact of eligibility categories (catastrophic plans only) 0.9992
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000
40 Impact of Age 26 / Age 29 1.0001
41 Impact of Family Planning / No Family Planning 1.0000
42 Impact of Dental vs No Dental 1.0000
43 Premium Curve Adjustment 0.9828
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018
43b Rating Region Factor 1.0808
44 Other 1 (specify) 1.0000
45 Other 2 (specify) Child only 0.9693
46 Base Benefit Changes 1.0008
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans
49 Plan Expected Costs 503.54
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00
Calculation of Final 2020 Rates All Plans
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03
57 Percent Change in Premium Rates (= L56 / L54) 7.05%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans
Overall Average Impact: 7.05%
627.67279 627.67279 627.67279
0.55000 0.92478 0.83772
1.00001 1.15001 1.08001
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
0.55331 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.12395 1.10143
1.00000 1.00000 1.00000
1.00022 1.05885 1.05077
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00078 1.00078 1.00078
0.30463 1.26666 1.04793
Plan 7 Plan 8 Plan 9
191.20 795.05 657.76
13.20460 13.20460 13.20460
10.520% 10.520% 10.520%
1.000% 1.000% 1.000%
17.235% 12.965% 13.261%
Plan 7 Plan 8 Plan 9
235.56 830.43 716.42
10.00 760.00 265.00
10.00 760.00 265.00
Plan 7 Plan 8 Plan 9
231.02 913.48 758.32
-1.93% 10.00% 5.85%
Exhibit 18 Updated by DFS 4/10/2018 6

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only
1 Product* XXXXXXX
2 Product ID* XXXXXXX
3 Metal Level (or catastrophic)* XXXXXXX
4 AV Metal Value (HHS Calculator)* XXXXXXX
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX
6 Plan Type* XXXXXXX
7 Plan Name* XXXXXXX
8 HIOS Plan ID (14 Digits)* XXXXXXX
9 Exchange Plan?* XXXXXXX
9A 2020 Plan Status (as compared to 2019) XXXXXXX
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Experience Period Index Rate
10 Earned Premiums for Latest Experience Period # 36,414,597.22
10A Incurred Claims for Latest Experience Period # 32,801,490.30
10B Member-Months for Latest Experience Period # 63,815.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans
Plan 10 Plan 11 Plan 12
94788NY 94788NY 94788NY
94788NY028 94788NY028 94788NY028
Silver Bronze Platinum
0.71960 0.63390 0.88740
0.74990 0.64850 0.92478
HMO HMO HMO
IHSX3198 IHBX4055 IHPX1039
94788NY0280055 94788NY0280059 94788NY0280064
Both Both Both
Uniform Mod Uniform Mod Uniform Mod
Plan 10 Plan 11 Plan 12
2,604,297.60 6,506,538.99 8,459.58
1,970,241.32 2,644,522.00 2,737.52
4,003.00 15,702.00 12.00
492.19119 168.41944 228.12667
616.53909 616.53909 616.53909
Plan 10 Plan 11 Plan 12
1.01806 1.01806 1.01806
Plan 10 Plan 11 Plan 12
Exhibit 18 Updated by DFS 4/10/2018 7

29 Index Rate - After Marketwide Adjustments 627.6728
30 Pricing actuarial value (without induced demand factor) # 0.7355
31 Pricing actuarial value (only the induced demand factor) # 1.0415
32 Impact of provider network characteristics ## 1.0000
33 Impact of delivery system characteristics ## 1.0000
34 Impact of utilization management practices ## 1.0000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000
36 Benefits in additional to EHB (greater than 1.00) 1.0018
37 Impact of eligibility categories (catastrophic plans only) 0.9992
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000
40 Impact of Age 26 / Age 29 1.0001
41 Impact of Family Planning / No Family Planning 1.0000
42 Impact of Dental vs No Dental 1.0000
43 Premium Curve Adjustment 0.9828
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018
43b Rating Region Factor 1.0808
44 Other 1 (specify) 1.0000
45 Other 2 (specify) Child only 0.9693
46 Base Benefit Changes 1.0008
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans
49 Plan Expected Costs 503.54
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00
Calculation of Final 2020 Rates All Plans
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03
57 Percent Change in Premium Rates (= L56 / L54) 7.05%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans
Overall Average Impact: 7.05%
627.67279 627.67279 627.67279
0.74990 0.64850 0.92478
1.03001 1.00001 1.15001
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00496
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.01938 0.87889 1.12395
1.00725 1.00000 1.00000
1.07539 1.08986 1.00022
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00078 1.00078 1.00078
0.85353 0.62167 1.20245
Plan 10 Plan 11 Plan 12
535.74 390.21 754.75
13.20460 13.20460 13.20460
10.520% 10.520% 10.520%
1.000% 1.000% 1.000%
13.648% 14.416% 13.041%
Plan 10 Plan 11 Plan 12
593.25 428.05 785.03
704.00 963.00 31.00
704.00 963.00 31.00
Plan 10 Plan 11 Plan 12
620.41 455.93 867.93
4.58% 6.51% 10.56%
Exhibit 18 Updated by DFS 4/10/2018 8

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only
1 Product* XXXXXXX
2 Product ID* XXXXXXX
3 Metal Level (or catastrophic)* XXXXXXX
4 AV Metal Value (HHS Calculator)* XXXXXXX
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX
6 Plan Type* XXXXXXX
7 Plan Name* XXXXXXX
8 HIOS Plan ID (14 Digits)* XXXXXXX
9 Exchange Plan?* XXXXXXX
9A 2020 Plan Status (as compared to 2019) XXXXXXX
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Experience Period Index Rate
10 Earned Premiums for Latest Experience Period # 36,414,597.22
10A Incurred Claims for Latest Experience Period # 32,801,490.30
10B Member-Months for Latest Experience Period # 63,815.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans
Plan 13 Plan 14 Plan 15
94788NY 94788NY 94788NY
94788NY028 94788NY028 94788NY028
Gold Silver Bronze
0.80850 0.71960 0.63390
0.83772 0.74990 0.64850
HMO HMO HMO
IHGX2040 IHSX3202 IHBX4056
94788NY0280065 94788NY0280066 94788NY0280070
Both Both Both
Uniform Mod Uniform Mod Uniform Mod
Plan 13 Plan 14 Plan 15
3,093.61 0.00 21,773.40
489.85 0.00 2,591.52
4.00 0.00 60.00
122.46250 0.00000 43.19200
616.53909 616.53909 616.53909
Plan 13 Plan 14 Plan 15
1.01806 1.01806 1.01806
Plan 13 Plan 14 Plan 15
Exhibit 18 Updated by DFS 4/10/2018 9

29 Index Rate - After Marketwide Adjustments 627.6728
30 Pricing actuarial value (without induced demand factor) # 0.7355
31 Pricing actuarial value (only the induced demand factor) # 1.0415
32 Impact of provider network characteristics ## 1.0000
33 Impact of delivery system characteristics ## 1.0000
34 Impact of utilization management practices ## 1.0000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000
36 Benefits in additional to EHB (greater than 1.00) 1.0018
37 Impact of eligibility categories (catastrophic plans only) 0.9992
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000
40 Impact of Age 26 / Age 29 1.0001
41 Impact of Family Planning / No Family Planning 1.0000
42 Impact of Dental vs No Dental 1.0000
43 Premium Curve Adjustment 0.9828
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018
43b Rating Region Factor 1.0808
44 Other 1 (specify) 1.0000
45 Other 2 (specify) Child only 0.9693
46 Base Benefit Changes 1.0008
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans
49 Plan Expected Costs 503.54
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00
Calculation of Final 2020 Rates All Plans
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03
57 Percent Change in Premium Rates (= L56 / L54) 7.05%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans
Overall Average Impact: 7.05%
627.67279 627.67279 627.67279
0.83772 0.74990 0.64850
1.08001 1.03001 1.00001
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00496 1.00496 1.00496
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.10143 1.01938 0.87889
1.00000 1.00725 1.00000
1.13086 1.08607 1.12647
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00078 1.00078 1.00078
1.13340 0.86629 0.64574
Plan 13 Plan 14 Plan 15
711.40 543.75 405.31
13.20460 13.20460 13.20460
10.520% 10.520% 10.520%
1.000% 1.000% 1.000%
13.132% 13.617% 14.311%
Plan 13 Plan 14 Plan 15
773.26 600.28 443.09
0.00 25.00 17.00
0.00 25.00 17.00
Plan 13 Plan 14 Plan 15
818.95 629.46 473.01
5.91% 4.86% 6.75%
Exhibit 18 Updated by DFS 4/10/2018 10

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only
1 Product* XXXXXXX
2 Product ID* XXXXXXX
3 Metal Level (or catastrophic)* XXXXXXX
4 AV Metal Value (HHS Calculator)* XXXXXXX
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX
6 Plan Type* XXXXXXX
7 Plan Name* XXXXXXX
8 HIOS Plan ID (14 Digits)* XXXXXXX
9 Exchange Plan?* XXXXXXX
9A 2020 Plan Status (as compared to 2019) XXXXXXX
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Experience Period Index Rate
10 Earned Premiums for Latest Experience Period # 36,414,597.22
10A Incurred Claims for Latest Experience Period # 32,801,490.30
10B Member-Months for Latest Experience Period # 63,815.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans
Plan 16 Plan 17 Plan 18
94788NY 94788NY 94788NY
94788NY028 94788NY028 94788NY028
Bronze Gold Platinum
0.63390 0.80850 0.88740
0.64850 0.83772 0.92478
HMO HMO HMO
IHBXC026 IHGXC026 IHPXC025
94788NY0280079 94788NY0280080 94788NY0280081
Both Both Both
Uniform Mod Uniform Mod Uniform Mod
Plan 16 Plan 17 Plan 18
70,948.01 30,530.88 39,673.94
29,121.54 20,241.56 149,643.74
409.00 95.00 106.00
71.20181 213.06905 1411.73340
616.53909 616.53909 616.53909
Plan 16 Plan 17 Plan 18
1.01806 1.01806 1.01806
Plan 16 Plan 17 Plan 18
Exhibit 18 Updated by DFS 4/10/2018 11

29 Index Rate - After Marketwide Adjustments 627.6728
30 Pricing actuarial value (without induced demand factor) # 0.7355
31 Pricing actuarial value (only the induced demand factor) # 1.0415
32 Impact of provider network characteristics ## 1.0000
33 Impact of delivery system characteristics ## 1.0000
34 Impact of utilization management practices ## 1.0000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000
36 Benefits in additional to EHB (greater than 1.00) 1.0018
37 Impact of eligibility categories (catastrophic plans only) 0.9992
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000
40 Impact of Age 26 / Age 29 1.0001
41 Impact of Family Planning / No Family Planning 1.0000
42 Impact of Dental vs No Dental 1.0000
43 Premium Curve Adjustment 0.9828
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018
43b Rating Region Factor 1.0808
44 Other 1 (specify) 1.0000
45 Other 2 (specify) Child only 0.9693
46 Base Benefit Changes 1.0008
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans
49 Plan Expected Costs 503.54
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00
Calculation of Final 2020 Rates All Plans
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03
57 Percent Change in Premium Rates (= L56 / L54) 7.05%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans
Overall Average Impact: 7.05%
627.67279 627.67279 627.67279
0.64850 0.83772 0.92478
1.00001 1.08001 1.15001
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
0.87889 1.10143 1.12395
1.00000 1.00000 1.00000
1.15631 1.11729 1.00022
1.00000 1.00000 1.00000
0.41200 0.41200 0.41200
1.00078 1.00078 1.00078
0.27174 0.45908 0.49296
Plan 16 Plan 17 Plan 18
170.57 288.15 309.42
13.20460 13.20460 13.20460
10.520% 10.520% 10.520%
1.000% 1.000% 1.000%
17.877% 15.397% 15.141%
Plan 16 Plan 17 Plan 18
196.34 322.89 330.59
11.00 275.00 5.00
11.00 275.00 5.00
Plan 16 Plan 17 Plan 18
207.70 340.59 364.63
5.78% 5.48% 10.30%
Exhibit 18 Updated by DFS 4/10/2018 12

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only
1 Product* XXXXXXX
2 Product ID* XXXXXXX
3 Metal Level (or catastrophic)* XXXXXXX
4 AV Metal Value (HHS Calculator)* XXXXXXX
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX
6 Plan Type* XXXXXXX
7 Plan Name* XXXXXXX
8 HIOS Plan ID (14 Digits)* XXXXXXX
9 Exchange Plan?* XXXXXXX
9A 2020 Plan Status (as compared to 2019) XXXXXXX
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Experience Period Index Rate
10 Earned Premiums for Latest Experience Period # 36,414,597.22
10A Incurred Claims for Latest Experience Period # 32,801,490.30
10B Member-Months for Latest Experience Period # 63,815.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans
Plan 19 Plan 20 Plan 21
94788NY 94788NY 94788NY
94788NY028 94788NY028 94788NY028
Silver Platinum Platinum
0.71960 0.88537 0.88537
0.74990 0.92100 0.92100
HMO HMO HMO
IHSXC040 IHPX1136 IHPX1137
94788NY0280082 94788NY0280129 94788NY0280130
Both Both Both
Uniform Mod Uniform Mod Uniform Mod
Plan 19 Plan 20 Plan 21
16,917.84 940,713.82 19,875.27
2,222.68 1,490,740.60 10,470.44
62.00 1,134.00 40.00
35.84968 1314.58607 261.76100
616.53909 616.53909 616.53909
Plan 19 Plan 20 Plan 21
1.01806 1.01806 1.01806
Plan 19 Plan 20 Plan 21
Exhibit 18 Updated by DFS 4/10/2018 13

29 Index Rate - After Marketwide Adjustments 627.6728
30 Pricing actuarial value (without induced demand factor) # 0.7355
31 Pricing actuarial value (only the induced demand factor) # 1.0415
32 Impact of provider network characteristics ## 1.0000
33 Impact of delivery system characteristics ## 1.0000
34 Impact of utilization management practices ## 1.0000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000
36 Benefits in additional to EHB (greater than 1.00) 1.0018
37 Impact of eligibility categories (catastrophic plans only) 0.9992
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000
40 Impact of Age 26 / Age 29 1.0001
41 Impact of Family Planning / No Family Planning 1.0000
42 Impact of Dental vs No Dental 1.0000
43 Premium Curve Adjustment 0.9828
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018
43b Rating Region Factor 1.0808
44 Other 1 (specify) 1.0000
45 Other 2 (specify) Child only 0.9693
46 Base Benefit Changes 1.0008
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans
49 Plan Expected Costs 503.54
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00
Calculation of Final 2020 Rates All Plans
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03
57 Percent Change in Premium Rates (= L56 / L54) 7.05%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans
Overall Average Impact: 7.05%
627.67279 627.67279 627.67279
0.74990 0.92100 0.92100
1.03001 1.15001 1.15001
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00376 1.00376
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00496
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.01938 1.12395 1.12395
1.00725 1.00000 1.00000
1.04591 1.06153 1.00022
1.00000 1.00000 1.00000
0.41200 1.00000 1.00000
1.00078 1.00078 1.00078
0.34202 1.26944 1.20205
Plan 19 Plan 20 Plan 21
214.67 796.79 754.49
13.20460 13.20460 13.20460
10.520% 10.520% 10.520%
1.000% 1.000% 1.000%
16.647% 12.962% 13.041%
Plan 19 Plan 20 Plan 21
247.05 866.41 816.46
12.00 85.00 6.00
12.00 85.00 6.00
Plan 19 Plan 20 Plan 21
257.55 915.45 867.65
4.25% 5.66% 6.27%
Exhibit 18 Updated by DFS 4/10/2018 14

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only
1 Product* XXXXXXX
2 Product ID* XXXXXXX
3 Metal Level (or catastrophic)* XXXXXXX
4 AV Metal Value (HHS Calculator)* XXXXXXX
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX
6 Plan Type* XXXXXXX
7 Plan Name* XXXXXXX
8 HIOS Plan ID (14 Digits)* XXXXXXX
9 Exchange Plan?* XXXXXXX
9A 2020 Plan Status (as compared to 2019) XXXXXXX
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Experience Period Index Rate
10 Earned Premiums for Latest Experience Period # 36,414,597.22
10A Incurred Claims for Latest Experience Period # 32,801,490.30
10B Member-Months for Latest Experience Period # 63,815.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans
Plan 22 Plan 23 Plan 24
94788NY 94788NY 94788NY
94788NY028 94788NY028 94788NY028
Gold Gold Bronze
0.81997 0.81997 0.62453
0.84960 0.84960 0.63090
HMO HMO HMO
IHGX2135 IHGX2136 IHBX4151
94788NY0280131 94788NY0280132 94788NY0280145
Both Both Both
Uniform Mod Uniform Mod Uniform Mod
Plan 22 Plan 23 Plan 24
2,372,144.41 37,425.00 0.00
1,914,484.76 13,576.85 0.00
3,384.00 84.00 0.00
565.74609 161.62917 0.00000
616.53909 616.53909 616.53909
Plan 22 Plan 23 Plan 24
1.01806 1.01806 1.01806
Plan 22 Plan 23 Plan 24
Exhibit 18 Updated by DFS 4/10/2018 15

29 Index Rate - After Marketwide Adjustments 627.6728
30 Pricing actuarial value (without induced demand factor) # 0.7355
31 Pricing actuarial value (only the induced demand factor) # 1.0415
32 Impact of provider network characteristics ## 1.0000
33 Impact of delivery system characteristics ## 1.0000
34 Impact of utilization management practices ## 1.0000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000
36 Benefits in additional to EHB (greater than 1.00) 1.0018
37 Impact of eligibility categories (catastrophic plans only) 0.9992
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000
40 Impact of Age 26 / Age 29 1.0001
41 Impact of Family Planning / No Family Planning 1.0000
42 Impact of Dental vs No Dental 1.0000
43 Premium Curve Adjustment 0.9828
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018
43b Rating Region Factor 1.0808
44 Other 1 (specify) 1.0000
45 Other 2 (specify) Child only 0.9693
46 Base Benefit Changes 1.0008
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans
49 Plan Expected Costs 503.54
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00
Calculation of Final 2020 Rates All Plans
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03
57 Percent Change in Premium Rates (= L56 / L54) 7.05%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans
Overall Average Impact: 7.05%
627.67279 627.67279 627.67279
0.84960 0.84960 0.63090
1.08001 1.08001 1.00001
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00376 1.00376 1.00376
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00496 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.10143 1.10143 0.87889
1.00000 1.00000 1.00000
1.04769 1.00022 1.08088
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00078 1.00078 1.00078
1.06366 1.02051 0.60207
Plan 22 Plan 23 Plan 24
667.63 640.54 377.90
13.20460 13.20460 13.20460
10.520% 10.520% 10.520%
1.000% 1.000% 1.000%
13.236% 13.307% 14.507%
Plan 22 Plan 23 Plan 24
697.01 666.34 414.30
262.00 0.00 753.00
262.00 0.00 753.00
Plan 22 Plan 23 Plan 24
769.48 738.86 442.03
10.40% 10.88% 6.69%
Exhibit 18 Updated by DFS 4/10/2018 16

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only
1 Product* XXXXXXX
2 Product ID* XXXXXXX
3 Metal Level (or catastrophic)* XXXXXXX
4 AV Metal Value (HHS Calculator)* XXXXXXX
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX
6 Plan Type* XXXXXXX
7 Plan Name* XXXXXXX
8 HIOS Plan ID (14 Digits)* XXXXXXX
9 Exchange Plan?* XXXXXXX
9A 2020 Plan Status (as compared to 2019) XXXXXXX
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Experience Period Index Rate
10 Earned Premiums for Latest Experience Period # 36,414,597.22
10A Incurred Claims for Latest Experience Period # 32,801,490.30
10B Member-Months for Latest Experience Period # 63,815.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans
Plan 25 Plan 26 Plan 27
94788NY 94788NY 94788NY
94788NY028 94788NY028 94788NY028
Bronze Platinum Platinum
0.62453 0.87707 0.87707
0.63090 0.89610 0.89610
HMO HMO HMO
IHBX4152 IHPX5101 IHPX5102
94788NY0280146 94788NY0280147 94788NY0280148
Both Both Both
Uniform Mod New Plan New Plan
Plan 25 Plan 26 Plan 27
0.00 0.00 0.00
0.00 0.00 0.00
0.00 0.00 0.00
0.00000 0.00000 0.00000
616.53909 616.53909 616.53909
Plan 25 Plan 26 Plan 27
1.01806 1.01806 1.01806
Plan 25 Plan 26 Plan 27
Exhibit 18 Updated by DFS 4/10/2018 17

29 Index Rate - After Marketwide Adjustments 627.6728
30 Pricing actuarial value (without induced demand factor) # 0.7355
31 Pricing actuarial value (only the induced demand factor) # 1.0415
32 Impact of provider network characteristics ## 1.0000
33 Impact of delivery system characteristics ## 1.0000
34 Impact of utilization management practices ## 1.0000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000
36 Benefits in additional to EHB (greater than 1.00) 1.0018
37 Impact of eligibility categories (catastrophic plans only) 0.9992
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000
40 Impact of Age 26 / Age 29 1.0001
41 Impact of Family Planning / No Family Planning 1.0000
42 Impact of Dental vs No Dental 1.0000
43 Premium Curve Adjustment 0.9828
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018
43b Rating Region Factor 1.0808
44 Other 1 (specify) 1.0000
45 Other 2 (specify) Child only 0.9693
46 Base Benefit Changes 1.0008
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans
49 Plan Expected Costs 503.54
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00
Calculation of Final 2020 Rates All Plans
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03
57 Percent Change in Premium Rates (= L56 / L54) 7.05%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans
Overall Average Impact: 7.05%
627.67279 627.67279 627.67279
0.63090 0.89610 0.89610
1.00001 1.15001 1.15001
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00376 1.00376 1.00376
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00496 1.00000 1.00496
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
0.87889 1.12395 1.12395
1.00000 1.00000 1.00000
1.00022 1.00022 1.00022
1.00000 1.00000 1.00000
1.00000 1.00000 1.00000
1.00078 1.00078 1.00078
0.55990 1.16378 1.16955
Plan 25 Plan 26 Plan 27
351.44 730.47 734.10
13.20460 13.20460 13.20460
10.520% 10.520% 10.520%
1.000% 1.000% 1.000%
14.724% 13.091% 13.083%
Plan 25 Plan 26 Plan 27
382.94 0.00 0.00
10.00 0.00 0.00
10.00 0.00 0.00
Plan 25 Plan 26 Plan 27
412.11 840.50 844.60
7.62%
Exhibit 18 Updated by DFS 4/10/2018 18

Exhibit 18 - Index Rate/Plan-Design Level Adjustment Worksheet
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
A separate column must be used for each base plan design (i.e., for each separate and distinct 14 digit HIOS ID)
Line # General***
ACA Compliant Plans
Only
1 Product* XXXXXXX
2 Product ID* XXXXXXX
3 Metal Level (or catastrophic)* XXXXXXX
4 AV Metal Value (HHS Calculator)* XXXXXXX
5 AV Pricing Value (total, risk pool experience based)* XXXXXXX
6 Plan Type* XXXXXXX
7 Plan Name* XXXXXXX
8 HIOS Plan ID (14 Digits)* XXXXXXX
9 Exchange Plan?* XXXXXXX
9A 2020 Plan Status (as compared to 2019) XXXXXXX
* This field should be the same as used in the Unified Rate Review Template, Worksheet 2
Experience Period Index Rate
10 Earned Premiums for Latest Experience Period # 36,414,597.22
10A Incurred Claims for Latest Experience Period # 32,801,490.30
10B Member-Months for Latest Experience Period # 63,815.00
10C Average PMPM Incurred Claims [(10A)/(10B)] = (Initial Index PMPM) 514.00909
11 Average Pricing Actuarial Value reflected in experience period 0.83370
12 AV Adjusted Experience Period Index Rate PMPM = [(10C) / (11)] 616.53909
# Amounts should be prior to any adjustments for Federal Risk Adjustment and Healthy NY Stop-Loss Reimbursements, and should be consistent with the amounts reported in Column 14.7 of Exhibit 17 for the relevant market categories.
Market Wide Adjustments to the AV Adjusted Experience Period Index Rate All Plans
13 Impact of adjusting experience period data to EHB benefit level ** 0.99415
14 Market wide adjustment for changes in provider network ** 1.00000
15 Market wide adjustment for fee schedule changes ** 1.00000
16 Market wide adjustment for utilization management changes ** 1.00000
17 Market wide adjustment for impact on claim costs from quality improvement and cost containment initiatives ** 1.00000
18 Claim trend projection factor (midpoint of experience period to mid point of rate applicability period) 1.13785
19 Federal Risk Adjustment Program Impact (less than 1.00 to reflect a recovery, more than 1.00 to reflect a payment to the pool) ** 0.89108
20 Impact of adjustments due to experience period claim data not being sufficiently credible ** 1.00000
21 Adjustment for changes in distribution of risk pool membership by rating regions (i.e., standard rating regions) ** 1.00000
22 Change in morbidity not reflected in the experience data that is known and quantifiable at the time of the rate filing ** 1.00000
23 Impact of ACA Provision 9010 - Health Insurance Providers Fee ** 1.01000
23a Impact of changes in New York State Law that are not reflected in the experience data ** 1.00000
24 Other 1 (specify) 1.00000
25 Other 2 (specify) 1.00000
26 Other 3 (specify) 1.00000
27 Other 4 (specify) 1.00000
28 Impact of Market Wide Adjustments (= Product L13 through L27) 1.01806
** Not Included in Claim Trend Adjustment
Plan Level Adjustments Average - All Plans
Plan 28 Plan 29
94788NY 94788NY
94788NY028 94788NY028
Silver Silver
0.70019 0.70019
0.70883 0.70883
HMO HMO
IHSX5101 IHSX5102
94788NY0280149 94788NY0280150
Both Both
New Plan New Plan
Plan 28 Plan 29
0.00 0.00
0.00 0.00
0.00 0.00
0.00000 0.00000
616.53909 616.53909
Plan 28 Plan 29
1.01806 1.01806
Plan 28 Plan 29
Exhibit 18 Updated by DFS 4/10/2018 19

29 Index Rate - After Marketwide Adjustments 627.6728
30 Pricing actuarial value (without induced demand factor) # 0.7355
31 Pricing actuarial value (only the induced demand factor) # 1.0415
32 Impact of provider network characteristics ## 1.0000
33 Impact of delivery system characteristics ## 1.0000
34 Impact of utilization management practices ## 1.0000
35 Impact on claim costs from quality improvement and cost containment initiatives ## 1.0000
36 Benefits in additional to EHB (greater than 1.00) 1.0018
37 Impact of eligibility categories (catastrophic plans only) 0.9992
38 Addition of Out of Network Benefit Option (e.g., POS or PPO, if applicable) 1.0000
39 Impact of Adjustment for NYS Stop Loss reimbursements on SG HNY 1.0000
40 Impact of Age 26 / Age 29 1.0001
41 Impact of Family Planning / No Family Planning 1.0000
42 Impact of Dental vs No Dental 1.0000
43 Premium Curve Adjustment 0.9828
43a Impact of loss of CSR Funding (A common factor to be applied uniformly to all silver plans only - if applicable) 1.0018
43b Rating Region Factor 1.0808
44 Other 1 (specify) 1.0000
45 Other 2 (specify) Child only 0.9693
46 Base Benefit Changes 1.0008
47 Impact of Plan Wide Adjustments (= Weighted Average Factor using Line 55a) 0.80224
# Reflects changes that impact an entire standard population (e.g., cost sharing and other changes that are not based on health status, age, gender or occupation).
## Beyond what is reflected in Market Wide adjustments
48a Adjusted Incurred Claims (Excluding Admin Expense and Profit) 32,133,619.31
Expenses
Weighted Average - All
Plans
49 Plan Expected Costs 503.54
50 FIXED EXPENSE: Administrative Costs (excluding Exchange user fees and profits) - to be expressed as a PMPM Amount ### 13.20460
51 VARIABLE EXPENSE: Administrative costs (excluding Exchange user fees and profits) - to be expressed as a percentage ### 10.520%
52 VARIABLE EXPENSE: Profit/Contribution to surplus margins - to be expressed as a percentage ### 1.000%
53 Total Expense Load as a percentage of Premium (= [L50 + (L51 + L52) * L56] / L56) 13.781%
### The combined factors for Administrative Costs (Fixed and Variable) and Profit/Contribution to surplus margins cannot exceed 18% (equivalent to a factor of 1.2195 ( = 1.00 / 0.82) applied to Line 49).
The "FIXED EXPENSE" amount in Line 50 must be entered as a PMPM and "VARIABLE EXPENSE" amounts in Lines 51 and 52 must be entered as a percentage of premium.
2019 Premium Rates and Membership All Plans
54 2019 PMPM Rates (First Quarter 2019 rates for Small Group)*** 545.56
55 2019 Members as of 3/31/2019 (The total should tie to the 3/31/2019 Membership Survey Total) 5,812.00
55a 2019 Members as of 3/31/2019 - Only those enrolled in plans that will still be available in 2020 5,812.00
Calculation of Final 2020 Rates All Plans
56 TOTAL PROJECTED INDEX RATE PMPM (= [(L49 + L50) / (1 - L51 - L52)]) 584.03
57 Percent Change in Premium Rates (= L56 / L54) 7.05%
*** The information in the "General" Section above should also be completed for any 2019 plans that will no longer be available in 2020.
*** The Average PMPM rate for "All Plans" should be used for All Non-ACA Compliant Plans
Overall Average Impact: 7.05%
627.67279 627.67279
0.70883 0.70883
1.03001 1.03001
1.00000 1.00000
1.00000 1.00000
1.00000 1.00000
1.00000 1.00000
1.00376 1.00376
1.00000 1.00000
1.00000 1.00000
1.00000 1.00000
1.00000 1.00496
1.00000 1.00000
1.00000 1.00000
1.01938 1.01938
1.00725 1.00725
1.00022 1.00022
1.00000 1.00000
1.00000 1.00000
1.00078 1.00078
0.75322 0.75696
Plan 28 Plan 29
472.77 475.12
13.20460 13.20460
10.520% 10.520%
1.000% 1.000%
13.924% 13.912%
Plan 28 Plan 29
0.00 0.00
0.00 0.00
0.00 0.00
Plan 28 Plan 29
549.25 551.90
Exhibit 18 Updated by DFS 4/10/2018 20

Exhibit 18 Supplement
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment : Individual
Expense Data - Individual 2020 Expected 2019 Expected 2018 Expected 2017 Expected 2018 Actual 2017 Actual
Period assumed - beginning date 1/1/2020 1/1/2019 1/1/2018 1/1/2017 1/1/2018 1/1/2017
Period assumed - ending date 12/31/2020 12/31/2019 12/31/2018 12/31/2017 12/31/2018 12/31/2017
Average annual claim trend assumed 6.67% 5.46% 6.57% 7.11% 1.02% 0.44%
Regulatory authority licenses and fees, including New York State 206 assessment expenses - as a % of gross premium 0.85% 0.78% 1.74% 0.91% 0.88% 0.98%
Administrative expenses for activities that improve health care quality as defined in the NAIC Annual Statement Supplement Health Care Exhibit - as a % of gross premium 1.40% 1.89% 0.88% 1.03% 2.03% 1.60%
Commissions and broker fees - as a % of gross premium 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Premium Taxes - as a % of gross premium 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Other state and federal taxes and assessments (other than income taxes and covered lives assessment) - as a % of gross premium 1.07% 0.00% 0.00% 0.00% 1.29% 0.06%
Other administrative expenses - as a % of gross premium 9.30% 6.81% 6.47% 8.16% 9.31% 9.14%
Subtotal 12.616% 9.485% 9.091% 10.096% 13.521% 11.776%
After tax underwriting margin (profit/contribution to surplus) - as a % of gross premium 1.00% 1.00% 1.00% 1.00% 0.00% 0.00%
State income tax component - as a % of gross premium 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
State income tax rate assumed (e.g. 3%) 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Federal income tax component - as a % of gross premium 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Federal income tax rate assumed (e.g. 30%) 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Reduction for assumed net investment income - as a % of gross premium (enter as a negative value) 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Subtotal 1.000% 1.000% 1.000% 1.000% 0.000% 0.000%
Total 13.616% 10.485% 10.091% 11.096% 13.521% 11.776%
Exhibit 18 Supplement Last Updated - 4/10/2018 21

EXHIBIT 19 - SUMMARY OF AVERAGE CLAIM TREND AND ADMINISTRATIVE EXPENSES AND PROFIT MARGIN
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment: Individual
1 Complete a separate ROW for each Metal Level/Product for all ACA compliant business written or renewed on or after 1/1/2016 in the relevant market for which the Company
had business in-force during the applicable experience period.
• Information should be for all the benefits included in that plan design including any riders (medical, drugs, etc.).
• Enter in column 1 the Metal Tier level.
• Enter in column 2 the plan designation as to On/Off Plan and Std/Non Standard Plan.
• Enter in column 3 the Estimated Membership as of a recent date mm/dd/yyy; enter the date in column heading.
• Append additional rows to the end of the existing rows as needed. Only use the first tab for data entry.
2 The average claim trend is the average annualized claim trend that is used in the applicable rate adjustment
filing to project the source data forward to the applicable rating period (e.g. 10.0%).
3 Enter the required information for the new rate period included in this rate adjustment filing. This refers to the various expense
components and profit margin included in the requested rates and the average annual claim trend assumed.
4 Enter the corresponding information requested for the immediately prior rate and form filing. This refers to the various expense components in the requested rates submitted for
the immediately prior rate and form filing and the average claim trend assumed. If there is no immediately prior rate and form filing, enter the data from the initial
rate and form filing.
5 ACA Fees that may be applicable are to be entered in columns 6.1 and 16.1.
6 This exhibit must be submitted as an Excel file and as a PDF file.
Exhibit 19 - Instructions Updated by DFS 3/14/2018 1

A. Company Name B. NAIC Code C. SERFF Number D. Market
1.
Metal Level
2.
On/Off Exchange
Designation and
Standard/Non Std
3.
Estimated
Membership as of
03/31/2019
4.1
Period assumed -
beginning date
(mm/dd/yy)
4.2
Period assumed -
ending date
(mm/dd/yy)
5.
Average annual
claim trend
assumed
6.1
Regulatory authority
licenses and fees,
including New York
State 206
assessment
expenses - as a %
of gross premium
6.2
Administrative
expenses for
activities that
improve health care
quality as defined in
the NAIC Annual
Statement
Supplement Health
Care Exhibit - as a
% of gross premium
6.3
Commissions and
broker fees - as a %
of gross premium
6.4
Premium Taxes - as
a % of gross
premium
6.5
Other state and
federal taxes and
assessments (other
than income taxes
and covered lives
assessment) - as a
% of gross premium
6.6
Other administrative
expenses - as a %
of gross premium
6.7
Subtotal columns
6.1 through 6.6
7.
After tax
underwriting margin
(profit/contribution to
surplus) - as a % of
gross premium
8.
State income tax
component - as a %
of gross premium
8.1
State income tax
rate assumed (e.g.
3%)
9.
Federal income tax
component - as a %
of gross premium
9.1
Federal income tax
rate assumed (e.g.
30%)
10.
Reduction for
assumed net
investment income -
as a % of gross
premium (enter as a
negative value)
11.
Subtotal columns
6.7 + 7 + 8 + 9 + 10
CDPHP 95491 CAPD-131909302 Individual Platinum Standard on exchange 340.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Platinum Non Standard on exchange 44.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Platinum Standard off exchange 456.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Platinum Non Standard off exchange 47.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Gold Standard on exchange 253.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Gold Non Standard on exchange 198.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Gold Standard off exchange 287.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Gold Non Standard off exchange 64.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Silver Standard on exchange 447.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Silver Non Standard on exchange 640.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Silver Standard off exchange 294.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Silver Non Standard off exchange 92.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Bronze Standard on exchange 805.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Bronze Non Standard on exchange 1417.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Bronze Standard off exchange 186.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Bronze Non Standard off exchange 232.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Catastrophic Standard on exchange 10.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual Catastrophic Standard off exchange 0.00 1/1/2020 12/31/2020 6.67% 0.85% 1.40% 0.00% 0.00% 1.07% 9.30% 12.62% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 13.62%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
CDPHP 95491 CAPD-131909302 Individual 0.00% 0.00%
General Information For the rate period included in this rate adjustment filing
Exhibit 19 Updated by DFS 3/14/2018 2

14.1
Period assumed -
beginning date
(mm/dd/yy)
14.2
Period assumed -
ending date
(mm/dd/yy)
15.
Average annual
claim trend
assumed
16.1
Regulatory authority
licenses and fees,
including New York
State 206
assessment
expenses - as a %
of gross premium
16.2
Administrative
expenses for
activities that
improve health care
quality as defined in
the NAIC Annual
Statement
Supplement Health
Care Exhibit - as a
% of gross premium
16.3
Commissions and
broker fees - as a %
of gross premium
16.4
Premium Taxes - as
a % of gross
premium
16.5
Other state and
federal taxes and
assessments (other
than income taxes
and covered lives
assessment) - as a
% of gross premium
16.6
Other administrative
expenses - as a %
of gross premium
16.7
Subtotal columns
16.1 through 16.6
17
After tax
underwriting margin
(profit/contribution to
surplus) - as a % of
gross premium
18
State income tax
component - as a %
of gross premium
18.1
State income tax
rate assumed (e.g.
3%)
19
Federal income tax
component - as a %
of gross premium
19.1
Federal income tax
rate assumed (e.g.
30%)
20
Reduction for
assumed net
investment income -
as a % of gross
premium (enter as a
negative value)
21
Subtotal columns
16.7 + 17 + 18 + 19
+20
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
1/1/2019 12/31/2019 5.46% 0.78% 1.89% 0.00% 0.00% 0.00% 6.81% 9.49% 1.00% 0.00% 0.00% 0.00% 0.00% 0.00% 10.49%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
0.00% 0.00%
For the rate period included in the prior rate and form filing
Exhibit 19 Updated by DFS 3/14/2018 3

EXHIBIT 23: SUMMARY OF REQUESTED 2020 PREMIUM RATES
Company Name: CDPHP
NAIC Code: 95491
SERFF Number: CAPD-131909302
Market Segment: Individual
1 Purpose of this Exhibit is to provide the actual distribution of all base Premium Rates for all Metal Levels and Regions.
2 Premium rates and member months are required for Calendar Years 2017 - 2020 for Individual (Individual only) and First Quarter 2017 - 2020 for Small Group (Employee only).
3 Membership must be consistent with the applicable DFS survey as of 3/31 for each of the respective years.
4 Premium rates must be based on the subscriber (Individual) or employee (Small Group) rate and should not be a PMPM amount.
5 Premiums should be reported for all plan variations (e.g., if the Company has different rates when family planning, pediatric dental, domestic partner, or age 29 coverage are added, etc.).
6 Additional guidance is provided in the various headings of the Exhibit.
7 This exhibit must be submitted as an Excel and as a PDF file.
8 The "PNDS Identifier" represents the code used in the Department of Health's PNDS system to identify the specific provider network associated with a particular plan.
9 The "Company Network Identifier" represents the specific code used by the Company to identify each distinct provider network used by the Company.
Exhibit 23 - Instructions Updated by DFS 3/14/2018 1

1. Company
Name 2. NAIC Code
3. SERFF
Number 4. Market
5. Current HIOS
ID (14 Digits)
6. Previous HIOS
ID (14 Digits)
7. Metal Level or
Catastrophic
8. Exchange
["On"/"Off"]
9. Plan Type [Std
or Non Std]
CDPHP 95491 CAPD-131909302 Individual 94788NY0280029 Bronze EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280030 Bronze EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280145 Bronze EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280146 Bronze EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280059 Bronze EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280070 Bronze EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280079 Bronze EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280047 Catastrophic EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280131 Gold EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280132 Gold EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280054 Gold EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280065 Gold EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280080 Gold EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280129 Platinum EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280130 Platinum EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280053 Platinum EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280064 Platinum EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280081 Platinum EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280017 Silver EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280018 Silver EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280021 Silver EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280022 Silver EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280055 Silver EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280066 Silver EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280082 Silver EXCH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280029 Bronze NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280030 Bronze NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280145 Bronze NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280146 Bronze NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280059 94788NY0280142 Bronze NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280070 94788NY0280143 Bronze NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280079 94788NY0280144 Bronze NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280131 Gold NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280132 Gold NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280054 94788NY0280136 Gold NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280065 94788NY0280137 Gold NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280080 94788NY0280138 Gold NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280129 Platinum NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280130 Platinum NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280053 94788NY0280133 Platinum NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280064 94788NY0280134 Platinum NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280081 94788NY0280135 Platinum NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280017 Silver NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280021 Silver NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280055 94788NY0280139 Silver NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280066 94788NY0280140 Silver NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280082 94788NY0280141 Silver NEXH Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280022 Silver NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280147 Platinum EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280148 Platinum EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280149 Silver EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280150 Silver EXCH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280147 Platinum NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280148 Platinum NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280149 Silver NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280150 Silver NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280018 Silver NEXH Non-Standard
CDPHP 95491 CAPD-131909302 Individual 94788NY0280047 Catastrophic NEXH Standard
Exhibit 23 Updated by DFS 3/14/2018 1

10.
Limiting Child
Age?
(26 or 30)
11.
Domestic
Partner
Coverage
Included? (yes,
no)
12.
Family
Planning
Coverage?
(included,
excluded)
13.
Pediatric
Dental
Coverage
Included? (yes,
no)
14. Out of
Network
Benefits? (yes,
no)
15.
Includes
Benefits in
Addition to
EHB?
(yes, no)
16.
Healthy New
York
(yes, no)
17.
Child-Only
Plan (yes, no)
18.
Tiered Network
Plan (yes, no)
19.
HSA Plan (yes,
no)
20.
PNDS Identifier
21.
Company
Network
Identifier
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no yes no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no yes no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no yes no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no yes no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no yes no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no yes no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no yes no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no yes no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
29 Yes included no No yes no no no no 0147 NYN002
26 Yes included no No no no no no no 0147 NYN002
PLAN INFORMATION
Exhibit 23 Updated by DFS 3/14/2018 2

Region 1 - 2017
Rate (Albany)
Region 2 - 2017
Rate (Buffalo)
Region 3 - 2017
Rate (Mid-
Hudson)
Region 4 - 2017
Rate (New York)
Region 5 - 2017
Rate (Rochester)
Region 6 - 2017
Rate (Syracuse)
Region 7 - 2017
Rate (Utica)
Region 8 - 2017
Rate (Long
Island)
Region 1 - 2017
MMs (Albany)
Region 2 - 2017
MMs (Buffalo)
Region 3 - 2017
MMs (Mid-
Hudson)
Region 4 - 2017
MMs (New York)
Region 5 - 2017
MMs (Rochester)
405.71 542.20 478.46 457.48 2,547.00 1,773.00
406.32 543.02 479.18 458.17 24.00 9.00
0.00 0.00
0.00
405.07 541.35 477.70 456.76 2,061.00 1,342.00
405.69 542.17 478.43 457.46 34.00 34.00
166.89 223.04 196.81 188.19 126.00 43.00
243.21 325.03 286.82 274.25 151.00 1.00
598.06 799.26 705.29 674.38 1,643.00 738.00
598.98 800.49 706.38 675.42 36.00
616.61 824.05 727.17 695.30 2,943.00 537.00
617.55 825.31 728.28 696.36 311.00 12.00
254.04 339.51 299.59 286.46 84.00 11.00
684.78 915.16 807.56 772.17 1,009.00 99.00
685.83 916.56 808.80 773.35 0.00
698.56 933.57 823.82 787.70 3,653.00 901.00
699.63 935.00 825.08 788.91 340.00 72.00
287.81 384.64 339.42 324.54 68.00 19.00
509.95 681.51 601.39 575.03 901.00 494.00
510.73 682.55 602.31 575.90 9.00 0.00
495.36 662.01 584.18 558.57 3,840.00 1,405.00
496.11 663.01 585.06 559.42 0.00
513.74 686.57 605.86 579.30 3,541.00 2,093.00
514.53 687.63 606.79 580.19 240.00 35.00
211.66 282.87 249.61 238.67 61.00 28.00
405.71 542.20 478.46 457.48 874.00 614.00
406.32 543.02 479.18 458.17 12.00 48.00
0.00 0.00
0.00
405.08 541.36 477.71 456.77 347.00 384.00
405.70 542.19 478.44 457.47 0.00 15.00
166.89 223.04 196.81 188.19 0.00
598.06 799.26 705.29 674.38 627.00 67.00
598.98 800.49 706.38 675.42 0.00
616.62 824.07 727.18 695.31 3,620.00 529.00
617.56 825.32 728.29 696.37 476.00 94.00
254.05 339.52 299.60 286.47 4.00
684.79 915.17 807.58 772.18 786.00 108.00
685.83 916.56 808.80 773.35 40.00
698.58 933.60 823.84 787.73 6,087.00 1,048.00
699.65 935.03 825.10 788.93 280.00 36.00
287.81 384.64 339.42 324.54 2.00
509.95 681.51 601.39 575.03 103.00 50.00
495.36 662.01 584.18 558.57 889.00 198.00
513.75 686.59 605.87 579.31 2,189.00 1,089.00
514.54 687.64 606.80 580.20 160.00 100.00
211.66 282.87 249.61 238.67 24.00
496.11 663.01 585.06 559.42 0.00
2017 PREMIUM RATES 2017 MEMBER MONTHS
Exhibit 23 Updated by DFS 3/14/2018 3

Region 6 - 2017
MMs (Syracuse)
Region 7 - 2017
MMs (Utica)
Region 8 - 2017
MMs (Long
Island)
Region 1 - 2018
Rate (Albany)
Region 2 - 2018
Rate (Buffalo)
Region 3 - 2018
Rate (Mid-
Hudson)
Region 4 - 2018
Rate (New York)
Region 5 - 2018
Rate (Rochester)
Region 6 - 2018
Rate (Syracuse)
Region 7 - 2018
Rate (Utica)
Region 8 - 2018
Rate (Long
Island)
Region 1 - 2018
MMs (Albany)
64.00 188.00 425.59 609.96 510.14 501.43 5,629.00
84.00 426.66 611.49 511.42 502.69 0.00
0.00 0.00 0.00
0.00
55.00 113.00 397.78 570.10 476.80 468.66 12,848.00
7.00 398.78 571.53 478.00 469.84 60.00
0.00 163.89 234.89 196.45 193.09 345.00
7.00 298.90 428.38 358.28 352.16 89.00
73.00 43.00 683.73 979.92 819.56 805.56 2,032.00
685.44 982.37 821.61 807.58 36.00
58.00 105.00 720.87 1,033.15 864.08 849.32 2,309.00
12.00 722.67 1,035.73 866.24 851.44 4.00
297.00 425.66 356.00 349.92 77.00
23.00 77.00 822.64 1,179.01 986.07 969.23 477.00
824.70 1,181.96 988.54 971.65 0.00
44.00 224.00 827.30 1,185.69 991.66 974.72 3,039.00
11.00 829.37 1,188.65 994.14 977.16 12.00
1.00 340.85 488.51 408.56 401.59 82.00
65.00 85.00 574.70 823.66 688.87 677.11 828.00
576.14 825.73 690.60 678.80 0.00
185.00 201.00 568.82 815.23 681.82 670.18 3,500.00
570.24 817.27 683.53 671.85 42.00
120.00 287.00 611.06 875.77 732.46 719.94 3,067.00
1.00 612.59 877.97 734.29 721.75 0.00
10.00 11.00 251.76 360.82 301.78 296.62 50.00
12.00 58.00 425.59 609.96 510.14 501.43 1,621.00
426.66 611.49 511.42 502.69 8.00
0.00
0.00
0.00 17.00 397.79 570.11 476.82 468.67 1,309.00
0.00 398.79 571.55 478.02 469.85 70.00
163.89 234.89 196.45 193.09 1.00
0.00 6.00 683.73 979.92 819.56 805.56 679.00
685.44 982.37 821.61 807.58 48.00
22.00 45.00 720.87 1,033.15 864.08 849.32 3,120.00
722.67 1,035.73 866.24 851.44 319.00
297.00 425.66 356.00 349.92 0.00
12.00 822.64 1,179.01 986.07 969.23 464.00
824.70 1,181.96 988.54 971.65 40.00
29.00 141.00 827.30 1,185.69 991.66 974.72 4,790.00
36.00 829.37 1,188.65 994.14 977.16 336.00
340.85 488.51 408.56 401.59 0.00
0.00 12.00 574.70 823.66 688.87 677.11 147.00
72.00 568.82 815.23 681.82 670.18 659.00
7.00 96.00 611.06 875.77 732.46 719.94 2,080.00
612.60 877.98 734.30 721.76 192.00
251.76 360.82 301.78 296.62 24.00
570.24 817.27 683.53 671.85
2018 PREMIUM RATES
Exhibit 23 Updated by DFS 3/14/2018 4

Region 2 - 2018
MMs (Buffalo)
Region 3 - 2018
MMs (Mid-
Hudson)
Region 4 - 2018
MMs (New York)
Region 5 - 2018
MMs (Rochester)
Region 6 - 2018
MMs (Syracuse)
Region 7 - 2018
MMs (Utica)
Region 8 - 2018
MMs (Long
Island)
Region 1 - 2019
Rate (Albany)
Region 2 - 2019
Rate (Buffalo)
Region 3 - 2019
Rate (Mid-
Hudson)
Region 4 - 2019
Rate (New York)
1,746.00 157.00 260.00 405.74 581.51
36.00 0.00 407.05 583.39
0.00 0.00 0.00 400.11 573.44
401.41 575.30
2,436.00 76.00 338.00 410.64 588.53
0.00 0.00 411.97 590.44
49.00 15.00 177.80 254.82
0.00 19.00 246.92 353.89
495.00 10.00 36.00 696.19 997.78
698.48 1,001.06
314.00 48.00 67.00 713.79 1,023.01
0.00 0.00 716.14 1,026.37
18.00 302.70 433.83
27.00 14.00 57.00 853.03 1,222.56
855.85 1,226.61
491.00 62.00 101.00 820.19 1,175.50
0.00 0.00 822.90 1,179.38
24.00 0.00 346.54 496.66
462.00 29.00 48.00 539.62 773.38
0.00 541.39 775.92
892.00 70.00 96.00 563.46 807.55
565.30 810.19
848.00 60.00 26.00 577.18 827.22
0.00 0.00 579.07 829.92
12.00 0.00 0.00 246.42 353.17
559.00 12.00 52.00 405.74 581.51
70.00 407.05 583.39
0.00 400.11 573.44
401.41 575.30
520.00 0.00 26.00 410.65 588.54
36.00 45.00 411.98 590.45
177.81 254.84
96.00 11.00 24.00 696.19 997.78
698.48 1,001.06
338.00 12.00 24.00 713.80 1,023.02
87.00 716.15 1,026.39
302.71 433.84
83.00 12.00 853.03 1,222.56
855.85 1,226.61
642.00 32.00 104.00 820.20 1,175.51
0.00 0.00 822.91 1,179.40
346.54 496.66
66.00 0.00 0.00 539.62 773.38
126.00 12.00 563.46 807.55
838.00 12.00 59.00 577.19 827.23
0.00 579.08 829.94
246.42 353.17
24.00 565.30 810.19
2018 MEMBER MONTHS 2019 PREMIUM RATES
Exhibit 23 Updated by DFS 3/14/2018 5

Region 5 - 2019
Rate (Rochester)
Region 6 - 2019
Rate (Syracuse)
Region 7 - 2019
Rate (Utica)
Region 8 - 2019
Rate (Long
Island)
Region 1 - 2019
Members as of
3/31/2019
(Albany)
Region 2 - 2019
Members as of
3/31/2019
(Buffalo)
Region 3 - 2019
Members as of
3/31/2019 (Mid-
Hudson)
Region 4 - 2019
Members as of
3/31/2019 (New
York)
Region 5 - 2019
Members as of
3/31/2019
(Rochester)
Region 6 - 2019
Members as of
3/31/2019
(Syracuse)
486.35 478.04 498.00 142.00 13.00
487.92 479.58 0.00 3.00
479.60 471.41 551.00 123.00 14.00
481.16 472.94 9.00
492.22 483.81 604.00 152.00 2.00
493.81 485.38 6.00 0.00
213.12 209.48 7.00 4.00
295.97 290.92 10.00 0.00
834.50 820.24 177.00 16.00 1.00
837.24 822.94 0.00
855.59 840.98 199.00 36.00 3.00
858.41 843.75 0.00 0.00
362.84 356.64 8.00 3.00
1,022.50 1,005.03 33.00 5.00 1.00
1,025.88 1,008.35 2.00
983.13 966.34 272.00 47.00 6.00
986.38 969.53 0.00 0.00
415.39 408.29 5.00 0.00
646.82 635.78 301.00 57.00 9.00
648.95 637.86 0.00 0.00
675.40 663.86 188.00 59.00 7.00
677.61 666.03 0.00
691.85 680.03 364.00 61.00 8.00
694.11 682.25 0.00 0.00
295.37 290.33 8.00 1.00 0.00
486.35 478.04 143.00 48.00 1.00
487.92 479.58 0.00 6.00
479.60 471.41 25.00 4.00
481.16 472.94 1.00
492.23 483.82 132.00 39.00 2.00
493.83 485.39 6.00 5.00 0.00
213.13 209.49 0.00
834.50 820.24 51.00 11.00 0.00
837.24 822.94 0.00
855.61 840.99 241.00 21.00 0.00
858.42 843.76 16.00 7.00
362.85 356.65 0.00
1,022.50 1,005.03 37.00 6.00
1,025.88 1,008.35 4.00
983.14 966.35 365.00 49.00 4.00
986.39 969.54 31.00 0.00 0.00
415.39 408.29 0.00
646.82 635.78 29.00 6.00 1.00
675.40 663.86 40.00 11.00
691.86 680.04 204.00 57.00 1.00
694.12 682.27 20.00 5.00
295.37 290.33 2.00
677.61 666.03 2.00
2019 MEMBERS (per DFS Membership Survey)2019 PREMIUM RATES
Exhibit 23 Updated by DFS 3/14/2018 6

Region 7 - 2019
Members as of
3/31/2019 (Utica)
Region 8 - 2019
Members as of
3/31/2019 (Long
Island)
Region 1 - 2020
Rate (Albany)
Region 2 - 2020
Rate (Buffalo)
Region 3 - 2020
Rate (Mid-
Hudson)
Region 4 - 2020
Rate (New York)
Region 5 - 2020
Rate (Rochester)
Region 6 - 2020
Rate (Syracuse)
Region 7 - 2020
Rate (Utica)
Region 8 - 2020
Rate (Long
Island)
Region 1 - 2019
Members as of
3/31/2019
(Albany)
Region 2 - 2019
Members as of
3/31/2019
(Buffalo)
Region 3 - 2019
Members as of
3/31/2019 (Mid-
Hudson)
28.00 427.39 610.81 484.14 478.28 498.00 142.00
0.00 429.44 613.74 486.46 480.57 0.00 3.00
36.00 423.13 604.72 479.31 473.51 551.00 123.00
425.15 607.61 481.60 475.77 9.00
30.00 432.93 618.73 490.41 484.48 604.00 152.00
0.00 435.00 621.69 492.76 486.80 6.00 0.00
0.00 178.37 254.92 202.05 199.61 7.00 4.00
0.00 238.33 340.61 269.97 266.71 10.00 0.00
4.00 758.54 1,084.08 859.26 848.86 177.00 16.00
762.23 1,089.35 863.44 852.99 0.00
4.00 745.40 1,065.30 844.37 834.15 199.00 36.00
0.00 749.03 1,070.49 848.48 838.22 0.00 0.00
307.11 438.91 347.89 343.68 8.00 3.00
3.00 890.75 1,273.03 1,009.02 996.81 33.00 5.00
895.09 1,279.23 1,013.94 1,001.67 2.00
10.00 891.04 1,273.44 1,009.35 997.14 272.00 47.00
0.00 895.39 1,279.66 1,014.28 1,002.00 0.00 0.00
0.00 367.11 524.66 415.85 410.82 5.00 0.00
11.00 569.86 814.42 645.52 637.71 301.00 57.00
572.62 818.37 648.65 640.80 0.00 0.00
8.00 588.53 841.11 666.67 658.61 188.00 59.00
591.37 845.16 669.89 661.78 0.00
4.00 596.37 852.31 675.55 667.38 364.00 61.00
0.00 599.26 856.44 678.83 670.61 0.00 0.00
1.00 245.71 351.16 278.33 274.97 8.00 1.00
4.00 427.39 610.81 484.14 478.28 143.00 48.00
429.44 613.74 486.46 480.57 0.00 6.00
423.13 604.72 479.31 473.51 25.00 4.00
425.15 607.61 481.60 475.77 1.00
2.00 432.93 618.73 490.41 484.48 132.00 39.00
435.00 621.69 492.76 486.80 6.00 5.00
178.37 254.92 202.05 199.61 0.00
2.00 758.54 1,084.08 859.26 848.86 51.00 11.00
762.23 1,089.35 863.44 852.99 0.00
2.00 745.40 1,065.30 844.37 834.15 241.00 21.00
749.03 1,070.49 848.48 838.22 16.00 7.00
307.11 438.91 347.89 343.68 0.00
0.00 890.75 1,273.03 1,009.02 996.81 37.00 6.00
895.09 1,279.23 1,013.94 1,001.67 4.00
7.00 891.04 1,273.44 1,009.35 997.14 365.00 49.00
895.39 1,279.66 1,014.28 1,002.00 31.00 0.00
367.11 524.66 415.85 410.82 0.00
2.00 569.86 814.42 645.52 637.71 29.00 6.00
1.00 588.53 841.11 666.67 658.61 40.00 11.00
5.00 596.37 852.31 675.55 667.38 204.00 57.00
599.26 856.44 678.83 670.61 20.00 5.00
245.71 351.16 278.33 274.97 2.00
591.37 845.16 669.89 661.78 2.00
867.08 1,239.20 982.21 970.32
871.31 1,245.24 987.00 975.06
566.62 809.79 641.85 634.09
569.36 813.71 644.96 637.15
867.08 1,239.20 982.21 970.32
871.31 1,245.24 987.00 975.06
566.62 809.79 641.85 634.09
569.36 813.71 644.96 637.15
572.62 818.37 648.65 640.80
238.33 340.61 269.97 266.71
2020 PREMIUM RATES
2019 MEMBERS (Should be consistent with DFS Membership Survey) - Only those members currently enrolled in 2019 plans that will continue to be
offered in 2020
Exhibit 23 Updated by DFS 3/14/2018 7

Region 4 - 2019
Members as of
3/31/2019 (New
York)
Region 5 - 2019
Members as of
3/31/2019
(Rochester)
Region 6 - 2019
Members as of
3/31/2019
(Syracuse)
Region 7 - 2019
Members as of
3/31/2019 (Utica)
Region 8 - 2019
Members as of
3/31/2019 (Long
Island)
Region 1 - 2019
Members as of
3/31/2019
(Albany)
Region 2 - 2019
Members as of
3/31/2019
(Buffalo)
Region 3 - 2019
Members as of
3/31/2019 (Mid-
Hudson)
Region 4 - 2019
Members as of
3/31/2019 (New
York)
Region 5 - 2019
Members as of
3/31/2019
(Rochester)
Region 6 - 2019
Members as of
3/31/2019
(Syracuse)
Region 7 - 2019
Members as of
3/31/2019 (Utica)
Region 8 - 2019
Members as of
3/31/2019 (Long
Island)
13.00 28.00
0.00
14.00 36.00
2.00 30.00
0.00
0.00
0.00
1.00 4.00
3.00 4.00
0.00
1.00 3.00
6.00 10.00
0.00
0.00
9.00 11.00
7.00 8.00
8.00 4.00
0.00
0.00 1.00
1.00 4.00
2.00 2.00
0.00
0.00 2.00
0.00 2.00
0.00
4.00 7.00
0.00
1.00 2.00
1.00
1.00 5.00
2019 MEMBERS (Should be consistent with DFS Membership Survey) - Only those members currently enrolled in 2019 plans that will continue to be 2019 MEMBERS - Only those members currently enrolled in 2019 plans Including plans that will be discontinued in 2020 ***** Columns CH - CO
apply to SMALL GROUP ONLY *****
Exhibit 23 Updated by DFS 3/14/2018 8

[Date] Member ID:
«Subscriber_First_Name» «Subscriber_Last_Name»
«Subscriber_Home_Address__1»
«Subscriber_Home_Address__1»
«Subscriber_Home__Address_City», «Subscriber_Home_Address__State»
«Subscriber_Home_Address_Postal_Code»
Dear Subscriber,
Your health insurance coverage is coming up for renewal. Your current coverage will be
automatically renewed on January 1, 2020, as long as you continue to be eligible, unless
you choose another policy. Included are changes we’ll be making to your policy, the new
premium for this policy, and some information about options if you wish to change
policies.
Premium rate change:
The premium rate for your health insurance policy is changing. The new rate will take
effect on January 1, 2020. The new rate below has been approved by the New York State
Department of Financial Services (DFS).
2020 Proposed Benefit Package Current 2019 Benefit Package
Medical Plan:
Office Visit Copay:
Specialist Visit Copay:
In-Network
Deductible:
Deductible Type:
Out-of-Network
Deductible:
In-Network
Coinsurance:
Out-of-Network Coinsurance:
In-Network
Maximum:
Out-of-Network
Maximum:
Inpatient Hospital:
Outpatient Surgery:
Emergency Room:
Ambulance:
Urgent Care:
NOTICE OF RENEWAL AND 2020 PREMIUM RATES

Durable Medical
Equipment:
Physical/Occupational/
Speech Therapy:
Rx:
Other Options:
New 2020 Monthly Premium Current 2019 Monthly Premium
Monthly Premium:
You may visit the DFS website at www.dfs.ny.gov for more information regarding this
rate change. You may also contact CDPHP® by calling member services at the number on
your member ID card or via our website at www.cdphp.com for further information about
this rate change.
Other changes to your current health insurance policy:
The name of your new policy is [2020 Plan name]. The benefit changes for your plan for
2019 are as follows:
[List Benefit changes]
Change in metal level:
Plans are separated into four categories known as “metal levels” (Bronze, Silver, Gold or
Platinum). The metal level is based on a plan’s actuarial value. Actuarial value is the
average percentage of the cost of all essential health benefits the plan pays. The metal
level of the plan you choose affects the total amount you will likely spend on out of
pocket costs for your benefits during the year (not including premiums). For instance, if
you choose a Bronze plan, you will likely pay more out-of-pocket for deductibles, co-
pays and other cost sharing than if you choose a Platinum plan. Please note that actuarial
value is an estimate of your expenses for the whole year, unlike coinsurance, in which
you pay a specific percentage of the cost of a particular service. The actuarial values for
each metal level are:
Bronze 60%
Silver 70%
Gold 80%
Platinum 90%
In order to maintain the required actuarial value for your plan’s existing metal level in
2019, we are required to make changes to the cost-sharing provisions of the plan. The
new cost-sharing is described above. You also have the option to choose another plan
with lower cost-sharing. See “Coverage options” below.

Coverage options:
If you do not want your current policy to automatically renew, you have the option of
choosing a different policy either from CDPHP® or from another insurer. You may
purchase a new policy directly from the insurer, or with the help of a broker or agent.
You may also purchase a new policy through the New York State of Health, New York’s
Official Health Plan Marketplace (the “Marketplace”). The Marketplace offers a variety
of coverage options from a number of insurers including CDPHP®. If you are eligible for
premium tax credits or assistance reducing deductibles, co-pays and other cost-sharing,
your monthly premium may be reduced when you purchase a policy through the
Marketplace. You or your family may also qualify for Medicaid, the Children’s Health
Insurance Program (CHIP), or the Essential Plan through the Marketplace. If you qualify
for lower monthly premiums or lower out-of-pocket costs, you can get those savings only
if you enroll in a policy through the Marketplace.
Before you decide to change policies:
Call the insurer or visit the insurer’s website to check which doctors, other healthcare
providers and prescription medications are covered by your current policy and the new
policy you are considering. This is an important step in selecting a policy that best meets
the needs of you and your family. If you are considering a new policy from us, our
website address is www.cdphp.com.
When you need to decide:
If you want to keep your present policy, you don’t need to do anything except pay the
new premium.
If you want to enroll in a different policy, the Open Enrollment period for 2020 plans
runs from November 1, 2019 to January 31, 2020. If you do not enroll during this Open
Enrollment period, you will not be eligible to change policies until the next annual Open
Enrollment Period, unless you have a qualifying event (for example, get married or have
a baby). To avoid gaps in coverage, and to be covered on January 1, 2020, you must
enroll in a policy by December 15, 2019 and the premium for the new policy must be
received by the insurance company before January 1, 2020.
If you have questions:
• Call CDPHP member services at the number on your member ID card between 8 a.m.
and 6 p.m., Monday through Friday, or visit our website at www.cdphp.com.
• To learn more about the New York State of Health Marketplace, visit
www.nystateofhealth.ny.gov, or call the Marketplace customer service at 1-855-355-
5777.

Getting help in other languages:
Para obtener asistencia en Español, llame al 1-800-777-2273.
Sincerely,
Patricia Lushkevich
Senior Vice President, Internal Operations
Capital District Physicians’ Health Plan, Inc.
[Date]
«Subscriber_First_Name» «Subscriber_Last_Name»
«Subscriber_Address_Line_1»
«Subscriber_Address_Line_2»
«Subscriber_Address_City», «Subscriber_Address_State_Code»
«Subscriber_Address_Postal_Code»
Dear Subscriber,
Your health insurance coverage is coming up for renewal. You may have already
received a renewal notice from the New York State of Health, New York’s Official
Health Plan Marketplace (“Marketplace”) with information about your 2020 coverage. If
you have not received your renewal notice by November 1, 2019, please contact the
Marketplace at 1-855-355-5777. You also have the option of selecting another individual
policy.
Below are changes we’ll be making to your current health insurance policy. The name of your new policy is (Plan Name)
2020 Proposed Benefit Package Current 2019 Benefit Package
Medical Plan:
Office Visit
Copay:
Specialist Visit
Copay:
In-Network
Deductible:
Deductible Type:
Out-of-Network
Deductible:
In-Network
Coinsurance:
Out-of-Network
Coinsurance:
In-Network
Maximum:
Out-of-Network
Maximum:
Inpatient Hospital:
Outpatient Surgery:
Emergency Room:
Ambulance:
NOTICE OF BENEFIT CHANGES AND
HEALTH INSURANCE COVERAGE OPTIONS FOR 2020

Urgent Care:
Durable Medical
Equipment:
Physical/Occupational/
Speech Therapy:
Rx:
Other Options:
New 2020 Monthly Premium Current 2019 Monthly Premium
Premium:
Change in metal level:
Plans are separated into four categories known as “metal levels” (Bronze, Silver, Gold or
Platinum). The metal level is based on a plan’s actuarial value. Actuarial value is the
average percentage of the cost of all essential health benefits the plan pays. The metal
level of the plan you choose affects the total amount you will likely spend for on out of
pocket costs for your benefits during the year (not including premiums). For instance, if
you choose a Bronze plan, you will likely pay more out-of-pocket for deductibles, co-
pays and other cost sharing than if you choose a Platinum plan. Please note that actuarial
value is an estimate of your expenses for the whole year, unlike coinsurance, in which
you pay a specific percentage of the cost of a particular service. The actuarial values for
each metal level are:
Bronze 60%
Silver 70%
Gold 80%
Platinum 90%
In order to maintain the required actuarial value for your plan’s existing metal level in
2019, we are required to make changes to the cost-sharing provisions of the plan. The
new cost-sharing is described above. You also have the option to choose another plan
with lower cost-sharing. See “Coverage options” below.
Coverage options:
If your current policy will automatically renew, but you would like to enroll in a different
policy, you may purchase a different policy through the Marketplace. The Marketplace
offers a variety of coverage options from a number of insurers including CDPHP®. You or
your family may also qualify for Medicaid, the Children’s Health Insurance Program
(CHIP), or the Essential Plan through the Marketplace. You may utilize the services of a
broker or agent for all Marketplace plans.
You may also purchase a new policy outside the Marketplace directly from an insurer or
with the help of a broker or agent. However, if you are eligible for premium tax credits or

assistance reducing deductibles, co-pays and other cost-sharing, your monthly premium
will be reduced only when you purchase a policy through the Marketplace.
Before you decide:
Call the insurer or visit the insurer’s website to check which doctors, other healthcare
providers and prescription medications are covered by your current policy and the new
policy you are considering. This is an important step in selecting a policy that best meets
the needs of you and your family. If you are considering a new policy from us, our
website address is www.cdphp.com.
When you need to decide:
If your policy has been automatically renewed, and you want to keep your current policy,
you don’t need to do anything more. You will receive information from the Marketplace
in December confirming your plan selection. This will include information about your
new premium, as well as tax credit and premium assistance eligibility. Your new
premium will start on January 1, 2020.
If your policy has not been automatically renewed, or you want to enroll in a different
policy, the 2020 Open Enrollment period runs from November 1, 2019 to January 31,
2020. After this Open Enrollment period you will not be eligible to change policies until
the next annual Open Enrollment Period unless you have a qualifying event (for example,
get married or have a baby). To avoid gaps in coverage, and to be covered on January 1,
2020, you must enroll in a policy by December 15, 2019, and your premium for the new
policy must be received by the insurance company before January 1, 2020.
If you have questions:
Call CDPHP member services at the number on your member ID card between 8 a.m.
and 6 p.m., Monday through Friday, or visit our website at www.cdphp.com.
• To learn more about the New York State of Health Marketplace, visit
www.nystateofhealth.ny.gov, or call the Marketplace customer service at 1-855-355-
5777.
Getting help in other languages:
Para obtener asistencia en Español, llame al 1-800-777-2273.
Sincerely,
Patricia Lushkevich
Senior Vice President, Internal Operations
Capital District Physicians’ Health Plan, Inc.

[Date]
Member ID: [Member Identifier] [Contact Name] [Address] [City State Zip] Notice of Proposed Premium Rate Change [Plan Name and Health Insurance Oversight System (HIOS) Plan ID number] Dear [Name]: Capital District Physicians’ Health Plan, Inc. (CDPHP®) is filing a request with the New York State Department of Financial Services (DFS) to approve a change to your premium rates for 2020. New York Insurance Law requires that we provide a notice to you when we submit requests for premium rate changes to DFS. DFS is required by law to review our requested rate change. DFS may approve, modify or disapprove the requested rate change. Proposed Premium Rate Change Please note that while we try to provide you with the most accurate information possible, the final approved rate may differ based on the benefit plan design and other features you select on renewal. Also, the final approved rate may differ because DFS may modify the proposed rate. If approved, the percentage change to your premium is [rate change]%. If you enrolled through the NY State of Health, the state’s health plan marketplace, and you qualified for financial assistance called an Advanced Premium Tax Credit (APTC), your current premium is less than the amount shown above. Your 2020 premium will also be less than shown above if you qualify for the APTC again next year. NY State of Health will calculate your eligibility for financial assistance each year. Why We Are Requesting a Rate Change As a not-for-profit health plan, CDPHP takes seriously its responsibility to control rising health care costs and be a good steward of your premium dollars. However, we continue to battle the rising cost of care, driven primarily by state and federal regulations and taxes, specialty drugs, and provider consolidation. These factors have resulted in the need to increase insurance premiums. We are working hard to alleviate these cost increases in a variety of ways, such as:
The CDPHP Enhanced Primary Care (EPC) program, a nationally-recognized patient-centered medical home that encourages high-quality, cost-effective services at the primary care level.
Dedicating resources to improving the overall health of our membership.

Easier and more convenient access to care through our telemedicine (live video doctor visits) partner, Doctor On Demand.
CDPHP Price Check, a cost transparency tool that provides members estimated costs on a range of health care services.
Movement of services to more cost-effective outpatient settings, such as freestanding surgical centers.
Case management and medication therapy management services, available at no out-of-pocket cost.
Mental health and substance use programs, including access to a 24-hour crisis line. DFS’s view of these matters may differ. 30-day Comment Period You can contact us or DFS to ask for more information or submit comments to DFS about the proposed rate change. The comments must be made within 30 days from the date of this notice. You can contact CDPHP for additional information at:
CDPHP 500 Patroon Creek Blvd. Albany, NY 12206 1-800-777-2273 www.cdphp.com
Comments or requests for more information on the proposed rate change may be submitted to DFS by visiting the DFS Website or via standard mail as follows: DFS Website: https://www.dfs.ny.gov/consumers/health_insurance/health_insurance_premiums United States Postal Service:
NYS Department of Financial Services Health Bureau – Premium Rate Adjustments One Commerce Plaza Albany, NY 12257
If you choose to submit comments to DFS, please include the following information:
1. The name of your insurer 2. The name of your plan 3. Whether you have individual or group coverage 4. Your HIOS Plan ID number, which is [Insert the HIOS Plan ID #]
Written comments submitted to DFS will be posted on the DFS website without your personal information.

Plain English Summary of Rate Change We have prepared a plain-English summary that provides a more detailed explanation of the reasons why a premium rate change is being requested. You can find this information at the following websites:
CDPHP website: www.cdphp.com DFS website: https://myportal.dfs.ny.gov/web/prior-approval/rate-applications-by-company
Notice of Approved Premium Rate After DFS approves the final premium rate, which may differ from the requested rates noted above, you will receive final rate information at least 60 days before your 2020 renewal date. Sincerely, Patricia Lushkevich Senior Vice President, Internal Operations Capital District Physicians’ Health Plan, Inc. Enclosure

Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
ACTUARIAL MEMORANDUM
Individual
On and Off Exchange
2020 Individual Plan Filing
General Information
Company Legal Name: Capital District Physicians’ Health Plan
State: New York
HIOS Issuer ID: 94788
QHP Template SERFF #: CAPD-131909302
Market: Individual
Effective Date: January through December 2020
Primary Contact Name:
Primary Contact Telephone Number:
Primary Contact Email Address:
Overview
This document contains the Actuarial Memorandum for Capital District Physicians’ Health Plan (“CDPHP”) Individual
comprehensive medical block of business, effective January 1, 2020. These individual rates are guaranteed 12 months
after the subscriber’s effective date. This actuarial memorandum is submitted in conjunction with the Part I Unified
Rate Review Template.
The purpose of the actuarial memorandum is to provide certain information related to the submission of premium rate
filings, including support for the values entered in the Part I Unified Rate Review Template. This memorandum may not
be appropriate for other purposes.
Identification
I, , am a Member of the American Academy of Actuaries. I meet the Academy qualification standards
for rendering an opinion in the area of health insurance.
This filing meets all Affordable Care Act (“ACA”) requirements for Essential Health Benefits (“EHB”), risk pooling,
actuarial value (“AV”), induced demand, metal level requirements, standardized rating regions, and standardized census
tier factors as further described below.
Proposed Rates
CDPHP is filing individual rates with effective dates beginning January 1, 2020 for plans to be marketed on and off the
NYHBE. The plan designs included in this filing are compliant with the EHB in accordance with the ACA. The
projected plan claim costs have been derived from the combined base claims experience for CDPHP’s existing Individual
pool. Plan design pricing considered assumptions for Induced Demand and AV as specified in the HHS Notice of
Benefit and Payment Parameters for 2020. Federal Risk Adjustment payments have been incorporated into the premium
rate development as further described below. The overall weighted-average premium change being requested is 5.5% as
indicated on Exhibit 13c.

Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
Experience Period Premium and Claims
The base period data used in the development of the medical expenses is the Individual incurred claims and membership
for all in-force plans, for the 12 months ending December 2018, paid through February 2019.
Worksheet 1 HHS Unified Rate Review Template
Earned Premiums are reported for the base period in-force membership in the individual pool. Premiums were obtained
from CDPHP’s data warehouse eligibility and premium tables. Earned premiums shown on Worksheet 1 were not
impacted by Federal MLR rebates as there were no rebates expected during the experience period.
Incurred claims and allowed claims presented on Worksheet 1 come directly from CDPHP’s claim payment records in the
data warehouse combined with capitated expenses and NYS HCRA surcharges from the accounting general ledger for the
base period.
Estimates for incurred but not reported (“IBNR”) claims are included and were derived using a standard industry lag
methodology. The standard lag methodology used combines large group, small group and individual historical lag
triangles separated for Inpatient, Outpatient, Professional, and Pharmacy type of services. The blocks are combined to
ensure the credibility of each lag cell. Final estimated reserve levels at the group size level are allocated based upon paid
claims by group size during the period. The base period claims include 2 months of paid run-out and therefore, IBNR is
0.7% of the base period starting claim cost.
Benefit Categories
The benefit categories are defined using standard industry definitions for Inpatient, Outpatient, Professional and Pharmacy
claims. Each claim, as it is adjudicated in the claims system and then loaded in the data warehouse, is mapped to the
appropriate category using one or more criteria including facility Bill Type, DRG code, Revenue Code, Procedure code,
CPT/HCPCS code, or NDC code. These categorizations are applied consistently across all financial related reporting. The
“Other” medical category includes case management, incentives, HCRA, home health, DME and orthotics.
General Overview of Proposed Rate Development
The general methodology used to develop the premium rates applies factors to the Index Rate for each component of the
rate buildup. Each component was compared to the starting net trended per member per month (“PMPM”) claims cost to
develop the applicable factor. The rates for the corresponding plan designs were developed by taking the product of the
following:
- Base Period Index Rate
- Impact of Essential Health Benefits
- Federal Risk Adjustment
- Claim Trend Projection - Pricing Actuarial Value without induced demand
- Pricing Actuarial Value – Induced Demand
- Benefits in addition to the Essential Health Benefits
- Additional Plan Factors
- Premium Curve Adjustment
- Impact of Loss of CSR (Silver Plans only)
- Child only factor, where applicable
- Administrative Expense and Profit were split between variable and fixed expenses to correspond to the changes made to
Exhibit 18.

Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
The resulting PMPM is then multiplied by the conversion factor, and regional factor to obtain the single rate for each
corresponding region.
Index Rate
The starting point claims PMPM for in-force plans, the Base Period Index Rate, was developed from the claims
experience as described above using the average AV for all in-force plans included in the base experience period.
Base Period In-force plan Index Rate Development
Average Incurred Claims PMPM $514.01 A
Average AV Pricing Value 0.8337 B
Individual Index Rate (Exhibit 18, line 12) $616.54 C = A / B
Membership Projections
The projected membership for 2020 is based on the current distribution for the plans in the experience period. This
projection is indicated on Worksheet 2 of the Unified Rate Review Template (URRT).
Impact of Market Wide Adjustments
Impact of compliance with Essential Health benefits
The impact of the additional costs associated with benefits in excess of the Essential Health benefits in the base period
experience as noted below are derived on Exhibit A and applied on Exhibit 18, Line 13 consistently for all plans in each
metal tier. This adjustment to the base claim experience was applied only for the proportion of membership in the base
that currently include these benefits.
Skilled Nursing Facility – Increase days from 200 to 365
Adult Vision Exam and Hardware
Acupuncture
Lasik Surgery
Impact of changes in the provider network, fee schedules levels, utilization management, and Quality Improvements that
apply to the entire market-wide risk pool not included in the claim trend
There are no changes planned for the composition of the provider network, fee schedules levels, utilization management,
or quality improvements in the projection period compared to the base period.
Impact on risk pool in expected covered membership risk characteristics
No adjustment has been made for expected changes due to membership risk characteristics.
Impact of anticipated changes in the distribution of the membership in the risk pool by the standard rating regions
There has been no adjustment to the membership in the risk pool by the standard rating regions

Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
Federal Risk Adjustment Program
CDPHP relied on final risk adjustment results from 2016 and 2017, along with our latest internal results from 2018, to
project anticipated payment transfer results in the final CMS report to be issued on June 30, 2019. To estimate 2019, we
adjusted our factors to reflect the enrollment shift recognized in early 2019. We anticipate this shift will continue throughout
the 2019 benefit year.
MM
2019 RA Transfer (Payment)/Refund
Estimate
2019 RA Transfer (Payment)/Refund
Estimate PMPM
Individual HMO 63,794 $5,635,384 $88.34 2019 Federal Reduction - 14% ($788,954) ($12.37)
$4,846,430 $75.97
The resulting PMPM was converted to a factor based upon overall average Projected Index rate PMPM for all metal tier
plans on and off the Exchange. This factor, 0.8911, was applied consistently across plans in each metal tier.
Exhibit RA has been provided to determine the impact to the proposed rates, in the event of a change in risk adjustment.
Credibility Adjustment:
The experience period used in the development of the 2020 premium rates is fully credible based on the member months
covered in the underlying claims experience and stability of the underlying benefit plan mix covered during the period.
Claim Trend Projection: Cost and Utilization Trend Factors
The average annual trend factor applied is 6.7%. The effective trend based on 24 months from the midpoint of the base
period to the midpoint of the rate period is 13.8%.
The allowed trend factors developed by type of service are shown in Exhibit B. The basis for development of trends is
CDPHP/CDPHP UBI’s commercial pool historical experience data, actual and projected contract provider reimbursement
rates, and input from CDPHP’s medical utilization management team and the following assumptions.
Service Mix Intensity: No additional adjustment has been made
Case Mix: No additional adjustment has been made
Adverse Selection: No additional adjustment for adverse selection has been incorporated in the annual trend
assumptions.
Deductible Leveraging: No explicit additional adjustments have been applied
Inpatient: Medical management programs will hold trend below the industry trend. Programs include Care
Management, Diabetic Management, and Readmission Avoidance.

Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
Outpatient: More procedures are moving to ambulatory surgery centers. CDPHP’s patient centered medical
home program (EPC) enhances access to primary care services for members thereby decreasing the number
of ER visits. Admission review of all requested inpatient stays has resulted in higher trends in observation
room care and decreased inpatient stays.
Professional: Continued movement of services to the more appropriate setting will result in more
outpatient/office/telephonic services. Emphasis on primary care services and management of specialty care
through value based programs.
Other Medical: An increase in homecare is expected as more palliative care services are provided. Number of
genetic tests available continues to expand. Continued focus on educating participating providers on evidence
based use of high tech imaging.
Pharmacy: Utilization and cost trends are based on the projected trends from CDPHP’s Pharmacy Benefit
Manager, Caremark, as well as input from CDPHP’s Pharmacy Management. Number and cost of Specialty Rx
continues to increase.
Annual rate trends are shown in the following table:
Projected Paid Trend Factor 2019 7.1%
Projected Paid Trend Factor 2020 7.4%
Plan Level Adjustments
AV Metal Values
The HHS Actuarial Value Calculator was used to determine the Metal Level for each plan design.
AV Pricing Values
The AV Pricing Value for each plan design was determined using CDPHP’s in house pricing tool. The pricing tool applies
factors for each applicable cost share corresponding to each plan design. The pricing AV is determined by applying the cost
share factor for each benefit, and dividing the expected paid claims by the starting allowed claims for each plan. The Induced
Demand factors included in the final pricing are consistent with the factors included in the HHS Notice of Benefits and
Payment Parameters for 2020.
Induced Demand
Platinum 1.1500
Gold 1.0800
Silver 1.0300
Bronze 1.0000

Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
New Plan Designs
CDPHP is adding one new Platinum and one new Silver plan for 2020. CDPHP will be offering all plan designs both On
and Off Exchange. HIOS IDs:
94788NY0280147
94788NY0280148
94788NY0280149
94788NY0280150
Impact of changes in characteristics for provider network, delivery systems, and claim cost for quality improvements
There are no changes planned for the characteristics of the provider network, delivery system, or claim costs for quality
improvements in the projection period compared to the base period. No adjustments were applied outside the claim trend
development.
Impact of changes utilization management
CDPHP’s Enhanced Primary Care (EPC) program has transitioned primary care doctors from a historic fee-for-service
(FFS) payment model, to a risk-adjusted global payment.
Benefit in addition to the Essential Health benefits
Unique plan designs have been created to incorporate the following additional benefits (Exhibit C):
Mandatory Make Available Benefits
Dependent coverage extended from age 26 to 29
Domestic Partner
Family Planning
Additional Benefits Available on all Non-Standard Products
Adult Vision Exam - available once per year
Skilled Nursing Facility – extends coverage from 200 days to 365 days
Acupuncture – maximum of 10 visits per year
Lasik Surgery – maximum reimbursement of $750
Additional Benefits Available on all plans (Exhibit A)
Gym Membership - $200/$100 for Subscriber/Spouse every six (6) months with documentation of fifty (50) visits.
DME subject to deductible
Cicotti Center (Next Step & Kids on the Move) – Reimbursement of $50 enrollment fee upon completion of the program
Child Birthing classes – reimbursement up to $75
Telenutrition – Nutritional counseling has been added as part of the Telemedicine benefit
Fertility Preservation – NYS Mandate

Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
Exhibit 23 -Change of HIOS IDs
In 2019 the Standard Off Exchange plans included an additional benefit to extend Skilled Nursing Facility (SNF) coverage
from 200 days to 365 days. This benefit has been changed to allow 200 days for SNF coverage in order to match the
Standard On exchange benefit and HIOS ID.
5. Current HIOS ID (14 Digits) 6. Previous HIOS ID (14 Digits)
94788NY0280059 94788NY0280142
94788NY0280070 94788NY0280143
94788NY0280079 94788NY0280144
94788NY0280054 94788NY0280136
94788NY0280065 94788NY0280137
94788NY0280080 94788NY0280138
94788NY0280053 94788NY0280133
94788NY0280064 94788NY0280134
94788NY0280081 94788NY0280135
94788NY0280055 94788NY0280139
94788NY0280066 94788NY0280140
94788NY0280082 94788NY0280141
Administrative Expense Load
The administrative expense load is based on actual 2018 administrative expense, along with 2019 budgeted expense in the
current individual market.
Taxes and Fees
PCORI: PCORI has not been included since PCORI will not be assessed for plan years ending after September 30th, 2019. Source: NYS DFS Instructions for the filing of 2020 Premium Rates
Risk Adjustment Fee: $0.18 pmpm has been included Source: NYS DFS Instructions for the filing of 2020 Premium Rates
NYS Regulatory Authority license and fees: Based on a percent of premium using prior year actuals
The total load for Administrative Expense and Contribution to Surplus compared to prior year actual is shown in the
following table. Non-benefit expense load is applied consistently for all plans across all metal tiers.

Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
On/Off Exchange – Individual 2020 % of
Premium Projected
% of Premium based on
2018 Actuals
2019 Filing % of
Premium Projected
General Administrative Expense 9.30% 9.31% 6.81%
Broker Commissions 0.00% 0.00% 0.00%
Quality Improvement 1.40% 2.03% 1.89%
Community Benefits 0.00% 0.00% 0.00%
Subtotal – Excluding ACA Taxes and Fees 10.69% 11.34% 8.71%
NYS Regulatory Authority license and fees 0.85% 0.88% 0.75%
ACA Insurers tax 1.00% 0.00% 0.00%
Risk Adjustment 0.07% 1.29% 0.03%
Total Administrative Expense Including ACA 12.62% 13.52% 9.49%
Profit and contribution to Surplus 1.00% 0.00% 1.00%
Total Retention including Profit 13.62% 13.52% 10.49%
Additional Factors applied to Premium rate build up
Child only plans
The child only rates were developed by multiplying the single rate by 0.412 as outlined by the Department of Financial
Services.
Catastrophic Plan Design
The development of the single rate for the catastrophic plan design includes a factor of 0.5533. This factor was calculated by
taking the ratio of the average costs, per member per month, for members under the age of thirty, to the average costs of
all members for the experience period. The purpose of this factor is to account for the eligibility guidelines, as outlined by
HHS, pertaining to this specific plan design.
Premium Curve Adjustment
CDPHP has calculated a premium slope adjustment based on the “Instructions for the Filing of 2020 Premium Rates”.
The calculation includes all Individual plan designs except Catastrophic.
The corresponding factors have been added to line 43, Exhibit 18.
All Region Single 3/31/19 Members
1. Avg Rel of Single Premium
2a. Ratio of step 1 to silver plan rel
2b. Ratio of factor in table to 2a
3. Impact of applying step 2
4. Factor to apply to eliminate rate impact of step 2
5. Factor for line 43 Check Slope
Platinum $836.83 887 1.3786 1.3786 1.1026 $922.68 1.0194 1.1239 $940.56 1.520 Gold $702.25 802 1.1569 1.1569 1.0805 $758.78 1.0194 1.1014 $773.48 1.250 Silver $607.03 1473 1.0000 1.0000 1.0000 $607.03 1.0194 1.0194 $618.79 1.000 Bronze $521.00 2638 0.8583 0.8583 0.8622 $449.20 1.0194 0.8789 $457.90 0.740 Catastrophic 1.0000 Total $616.21 5800 1.0151 0.9641 $604.50 1.0194 0.9828 $616.21

Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
Each HIOS ID has been tested against the comparable Silver Metal plan to ensure all plans fall within range.
HIOS ID Metal Tier Slope
94788NY0280053 Platinum 1.56
94788NY0280064 Platinum 1.56
94788NY0280081 Platinum 1.49
94788NY0280129 Platinum 1.56
94788NY0280130 Platinum 1.56
94788NY0280054 Gold 1.25
94788NY0280065 Gold 1.25
94788NY0280080 Gold 1.25
94788NY0280131 Gold 1.27
94788NY0280132 Gold 1.27
94788NY0280055 Silver 1.00
94788NY0280066 Silver 1.00
94788NY0280082 Silver 1.00
94788NY0280021 Silver 1.00
94788NY0280022 Silver 1.00
94788NY0280017 Silver 1.00
94788NY0280018 Silver 1.00
94788NY0280059 Bronze 0.74
94788NY0280070 Bronze 0.74
94788NY0280079 Bronze 0.73
94788NY0280029 Bronze 0.73
94788NY0280030 Bronze 0.73
94788NY0280145 Bronze 0.72
94788NY0280146 Bronze 0.72
94788NY0280047 Catastrophic Catastrophic
Impact of loss of CSR Funding
Based on claims paid for calendar year 2018 as of March 31, 2018, the impact is 1.00725, spread over all Silver plans.
Conversion Factor
The single conversion factor was calculated using subscribers and members enrolled in Individual HMO for calendar
year 2018. See Exhibit G.
Regional Factors
The regional factors have been updated for 2020. Due to the lack of credibility, regions 1, 6, and 7 have been combined. In
addition, the factors have been weighted to smooth out large swings from year to year split 33%/67% to the 2019 factors
and most recent 3 years of experience respectively. The overall impact of this change is 0%. See Exhibit H.
Capital District Physicians’ Health Plan
Premium Rate Filing FORMS # 01-0001-2020; 01-0002-2020; 01-0004-2020; 01-0005-2020; 01-0007-2020; 01-0017-2020
Exhibit Differences
Exhibit 18 vs Exhibit 19: The Total Expense Load as a percentage of Premium calculated on exhibit 18 (Cell D91) is
different from the percentage listed on Exhibit 19. The admin percentage on exhibit 19 is the correct amount used, however
since Exhibit 18 multiplies the regional factor before the admin, the overall admin is slightly off.
Exhibit 13c vs Exhibit 14: As indicated above, Exhibit 13c weights the single rate by subscribers. Exhibit 14 weights the
PMPM by membership. As a result the annual premium and average increases are slightly off.
Dental
CDPHP has entered into a partnership with Delta Dental to provide pediatric dental benefits. These benefits are in
compliance with the EHB in accordance with the ACA. CDPHP will assume the marketing, enrollment, billing and
renewal responsibilities, while Delta Dental will assume the underwriting risk and administration of the benefits as a
standalone contract.
Advance Primary Care (APC) Initiatives
An adjustment for funding the Advanced Primary Care (APC) initiatives in 2020 has not been included in the 2020 MLR
calculation. Since CDPHP has been involved in these types of programs with its provider community for the past several
years, it has already made significant investment of resources in the transformation of participating primary care practices.
CDPHP’s Enhanced Primary Care (EPC) program has transitioned primary care doctors from a historic fee-for-service (FFS)
payment model, to a risk-adjusted global payment with the addition of a Triple Aim performance bonus. The base payment
model is a risk-adjusted comprehensive global payment that pays providers above the traditional model (FFS/Care
Coordination/PIPs). Throughout the last 10+ years, CDPHP has given a significant amount of funding and resources to
support the transition to value-based care for participating providers. As new practices seek to transform to the APC model
CDPHP will provide them additional transformation assistance.
Historical Claim Data by Policy Form (Exhibit 17)
For each experience period represented in this exhibit, incurred claims and membership for all in-force plans, for each 12
month period, includes paid claims and revised estimates for remaining reserves as of March 2018. Exhibit 17 includes data
for all rating regions.
Standardized premium factors were developed in (Exhibit M) and was based on the scale required by the NYS Department
of Financial Services.
Projected Loss Ratio
The projected loss ratio based on the New York State definition is 86.4%.

NEW YORK STATE DEPARTMENT OF FINANCIAL SERVICES Checklist for the Filing of 2020 Individual Premium Rates
For On-Exchange Plans and Off-Exchange Plans
1. Under which Section of the New York State Insurance Law is this filing being made? (3231(e)(1), 4308(c), 3231(d), or 4308(b)) 4308(c) 2. For filings made pursuant to 3231(e)(1) and 4308(c):
a. Did the Company submit a combined filing for “On” and “Off” Exchange rates per the instructions along witha separate form filing that both contain cross references to each other?
b. For Individual filings, do the Exhibits only contain Individual plan/experience data per the instructions? c. For Small Group filings, do the Exhibits only contain Small Group plan/experience data per the instructions?
3. Does this filing introduce any new plans (i.e., new 14-digit HIOS IDs)? 4. Has the Company provided two versions (i.e., PDF and Excel) of all rate filing Exhibits and Rate Manual?5. Do the values in Line 10 of Exhibit 18 match the totals in column 14.4 of Exhibit 17 for the applicable Market Segments? 6. Do the values in Line 10A of Exhibit 18 match the totals in column 14.7 of Exhibit 17 for the applicable Market Segments? 7. Do the values in Line 10B of Exhibit 18 match the totals in column 14.3 of Exhibit 17 for the applicable Market Segments? 8. Confirm that the 2020 version (updated in 2019) of the rate filing Exhibits were utilized (Yes/No: Respond “Yes” to confirm). 9. With regard to the “Rate Review Detail” screen in SERFF:
a. Was it completed in a manner consistent with 2019 premium rate filings? b. Do the “Average” percentages look reasonable (e.g., do they fall between “Minimum” and “Maximum” percentages? c. Do the “Minimum” and “Maximum” values appear reasonable in light of changes that are being proposed? d. Are the “Minimum”, “Maximum” and “Average” values stated on an Annualized PMPM basis (as opposed to annual
premium)?e. Are all items that are not applicable left blank (i.e., Items that are not applicable should be left blank)? f. Have the “Requested Rate Period” data fields been populated with non-zero values?
10. Is the information presented in Exhibit 18 provided at the HIOS SCID level (i.e., are there 14 digits in the HIOS ID?) 11. Does Exhibit 23 contain rates for every distinct 14-digit HIOS ID as opposed to only the “Base” plan rates? 12. Does the Company’s claim experience for 2018 include two months of run-out? 13. Is the rate manual provided in both PDF and Excel format per our instructions? 14. Were adequate details (as well as a spreadsheet) included with the Actuarial Memorandum regarding how DFS should modify
the Company’s 2020 assumption for risk adjustment to the extent actual 2018 results are different from expected? 15. Does the PMPM value in Cell Q-74 of Exhibit 13C equal the value in Cell D-96 (Line 54 Column D) of Exhibit 18? 16. Does the PMPM value in Cell Z-74 of Exhibit 13C equal the value in Cell D-102 (Line 56 Column D) of Exhibit 18? 17. Does the overall rate change calculated in Exhibit 13c accurately represent the Company’s expectation of the rate change?
a. If not, did the Company’s Actuary reach out to DFS and resolve the issue? (Note that any such issues should be resolved prior to submission of the filing by contacting Frank Horn via e-mail at [email protected] or by phone at (518) 473- 5454).
Name of the Chief Actuary responsible for this filing: Signature: Date: E-mail Address: Phone Number:
Rate Filing Checklist – Last updated: 4/18/2019
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
May 13, 2019
YesYes
Yes
Yes
Yes

Company Name: CDPHP
NAIC Code: 95491
SERFF Tracking #: CAPD-131909302
Market Segment: Individual
A. Insurer Information: HMO - 44 Not-for-Profit 95491Company submitting the rate filing request Company Type Org. Type Company NAIC Code
B. Contact Person: Rate filing contact person name, title Contact phone number Contact Email address
C. Actuarial Contact (If different from above): Actuary name, title Actuary phone number Actuary Email address
D. New Rate Information: CAPD-131909302New rate applicability period New rate effective date SERFF Tracking Number
E.
F. Provide responses for the following questions:
1.
2.
3.
4.
5.
6
Notes:(1)
(2)
EXHIBIT 11: GENERAL INFORMATION
CDPHP
500 Patroon Creek Blvd, Albany NY 12206
Company mailing address
Confirm that initial notices have not been sent to any impacted policyholders and will not be sent until the Company
has received confirmation that all relevant 2020 rate applications have been posted on the Department's website. See
note (2).
Yes
January 1, 2020 - December 31, 2020 1/1/2020
Market segment included in filing (e.g., Small Group (including Healthy NY Small Group), Individual - only one market
segment per rate adjustment filing): Individual
Response
Does this filing include any revision to contract language that is not yet approved? See note (1). If yes, provide a brief
description of the contract language changes included in this filing.
Yes 2020 Model language
Are there any rate filings submitted and not yet approved that if approved would affect the rate tables included in this
rate filing? If yes, mention these filings on Exhibit 16.
No
As mentioned in the checklist, this combined non-grandfathered product rate adjustment and form/rate filing can only include minor contract revisions, such as due to changes in the model language, changes to the catastrophic
plan due to change in out of pocket maximum, changes to the standard plan designs. Substantial changes need to be submitted as a separate rate and form filing (e.g., a new plan design not replacing an existing plan design,
contract language changes not just due to changes in the model language).
For purposes of complying with §3231(e)(1)(A) and §4308(c)(2) of the New York Insurance Law, rate applications will be considered to have been submitted after all of the relevant rate applications have been posted on the
Department's website. Once the rate applications have been posted, the Department will send a blast email instructing insurers to send their initial rate notices to policy/certificate holders. Notices should not be sent prior to
having received the blast email from the Department. Note that the 60 (or 80) day review period will begin on the day in which DFS designates as the filing due date and the 30 day consumer comment period will begin on the
date DFS sends the blast email to insurers.
Have all the required exhibits been submitted with this rate filing? If any exhibit is not applicable, has an explanation
been provided why such exhibit is not applicable?
Yes
Did the company submit a "Prior Approval Pre-filing" containing a draft of the initial notice and a draft of the narrative
summary and numerical summary associated with this rate filing? Indicate Yes or No, and if Yes, please provide the
SERFF number of the pre-filing.
Yes CAPD-131893519
45 CFR 154.215 requires companies to submit rate filings via SERFF and HIOS simultaneously. Did the company
submit this rate filing in HIOS? If yes, please provide the HIOS submission tracking number.
Yes 94788-1482892079297991685
Exhibit 11 Updated by DFS 3/14/2018 1

Exhibit 15b MHPAEA Compliance Certification
I, _________________________________, certify that the mental health and substance use disorder [name of Company Officer]
(MH/SUD) benefits applicable to this filing by ________________________ comply with the Mental [name of health insurer]
Health Parity and Addiction Equity Act and any regulations promulgated thereunder (MHPAEA). The
medical/surgical and MH/SUD benefits applicable to this filing have been tested for compliance with
MHPAEA’s financial requirements and quantitative treatment limitations rules, including the
Substantially All and Predominant tests. This compliance certification pertains to the medical and
behavioral benefit designs provided by ________________________ and does not opine on the [name of health insurer]
compliance of any wellness or incentive programs that ________________________ may choose to offer. [name of health insurer]
To measure compliance, we created an actuarial cost model of the medical/surgical benefits that included
mapping the underlying experience data allowed healthcare costs for the plans included in this filing
into the six benefit classifications (or sub-classifications allowed for outpatient benefits) that MHPAEA
permits. We tested the financial requirements and quantitative treatment limitations imposed on the
MH/SUD benefits related to this filing and determined that they are no more restrictive than the
predominant financial requirements or treatment limitations applied to substantially all medical or
surgical benefits related to this filing.
I am an officer of ___________________________ with knowledge of the issuer’s comprehensive [name of health insurer]
medical expense products and the laws and regulations applicable to those products. To the best of my
knowledge and belief the above information is true, accurate and complete.
Signature: ___________________________________________________________________________ Printed name and title: _________________________________________________________________ Date: ______________________ Phone: ___________________________________________________ Email Address: _______________________________________________________________________
CDPHP
CDPHP
CDPHP
CDPHP

If
mUnified Rate Review v5.0 To add a product to Worksheet 2 - Plan Product Info, select the Add Product button or Ctrl + Shift + P.
To add a plan to Worksheet 2 - Plan Product Info, select the Add Plan button or Ctrl + Shift + L.
Company Legal Name: Capital District Physicians' Health Plan State: NY To validate, select the Validate button or Ctrl + Shift + I.
HIOS Issuer ID: 94788 Market: Individual To finalize, select the Finalize button or Ctrl + Shift + F.
Effective Date of Rate Change(s): 1/1/2020
Section I: Experience Period Data
Experience Period: 1/1/2018 to 12/31/2018
Total PMPM
$39,344,442.24 $616.54
$0.00 $0.00
$32,801,490.30 $514.01
-$4,847,716.34 -$75.97
$36,414,597.22 $570.63
63,815
Section II: Projections
Cost Utilization Cost Utilization
Inpatient Hospital $123.41 1.092 1.006 1.092 1.006 $148.93
Outpatient Hospital $129.90 1.043 1.038 1.046 1.038 $152.69
Professional $174.37 1.026 1.016 1.027 1.017 $189.85
Other Medical $44.26 1.062 1.003 1.065 1.003 $50.36
Capitation $14.67 1.020 1.000 1.020 1.000 $15.26
Prescription Drug $129.93 1.030 1.020 1.036 1.020 $144.25
Total $616.54 $701.34
1.000
1.000
0.994
1.000
1/1/2020 $697.14
$0.00
100.00%
Projected Period Totals
1/1/2020 $697.14 $44,487,989.10
$0.00 $0.00
$75.97 $4,848,025.55
1.00% $400,403.67
$627.44 $40,040,367.22
63,815
Other
Adjusted Trended EHB Allowed Claims PMPM for
Morbidity Adjustment
Information Not Releasable to the Public Unless Authorized by Law: This information has not been publically disclosed and may be privileged and confidential. It is for internal government use only and must not be disseminated, distributed, or copied to persons not authorized to receive the information. Unauthorized disclosure may result in prosecution to the full
extent of the law.
Projected Member Months
Projected Index Rate for
Reinsurance
Risk Adjustment Payment/Charge
Exchange User Fees
Market Adjusted Index Rate
Applied Credibility %
Manual EHB Allowed Claims PMPM
Demographic Shift
Plan Design Changes
Market Level Calculations (Same for all Plans)
Trended EHB Allowed Claims
PMPM
Year 1 Trend Year 2 Trend
Allowed Claims
Reinsurance
Incurred Claims in Experience Period
Risk Adjustment
Experience Period Premium
Experience Period Member Months
Benefit Category
Experience Period Index
Rate PMPM
1 of 10

If macros are disabled, press and hold the ALT key and press the F, then I, and then N key. After that, select the Enable All Content option by pressing enter. (note that you can also press the C key to select "Enable All Content") Instructions can be found in cells P1 through P4.Product-Plan Data Collection
Company Legal Name: Capital District Physicians' Health Plan
HIOS Issuer ID: 94788
Effective Date of Rate Change(s): 1/1/2020
Field # Section I: General Product and Plan Information
1.1 Product Name
1.2 Product ID
1.3 Plan Name IHSX3288 IHSX3289 IHSX3280 IHSX3281 IHBX4149 IHBX4150 IHCX5008
1.4 Plan ID (Standard Component ID) 94788NY0280017 94788NY0280018 94788NY0280021 94788NY0280022 94788NY0280029 94788NY0280030 94788NY0280047
1.5 Metal Silver Silver Silver Silver Bronze Bronze Catastrophic
1.6 AV Metal Value 0.717 0.717 0.719 0.719 0.631 0.631 0.611
1.7 Plan Category Renewing Renewing Renewing Renewing Renewing Renewing Renewing
1.8 Plan Type HMO HMO HMO HMO HMO HMO HMO
1.9 Exchange Plan? Yes Yes Yes Yes Yes Yes Yes
1.10 Effective Date of Proposed Rates 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020
1.11 Cumulative Rate Change % (over 12 mos prior) 5.10% 5.80% 3.90% 4.30% 4.80% 5.20% -3.50%
1.12 Product Rate Increase %
1.13 Submission Level Rate Increase %
Worksheet 1 Totals Section II: Experience Period and Current Plan Level Information
2.1 Plan ID (Standard Component ID) Total 94788NY0280017 94788NY0280018 94788NY0280021 94788NY0280022 94788NY0280029 94788NY0280030 94788NY0280047
$39,344,442 2.2 Allowed Claims $39,344,442 $797,125 $0 $3,080,983 $8,253 $2,634,395 $38,187 $3,818
$0 2.3 Reinsurance $0 $0 $0 $0 $0 $0 $0 $0
2.4 Member Cost Sharing $6,542,952 $200,236 $0 $722,333 $6,715 $1,095,639 $27,268 $2,210
2.5 Cost Sharing Reduction $0 $0 $0 $0 $0 $0 $0 $0
$32,801,490 2.6 Incurred Claims $32,801,490 $596,889 $0 $2,358,650 $1,539 $1,538,756 $10,919 $1,607
-$4,847,716 2.7 Risk Adjustment Transfer Amount -$4,847,716 -$120,101 $0 -$406,945 -$5,014 -$762,766 -$8,660 -$8,204
$36,414,597 2.8 Premium $36,414,597 $970,479 $0 $3,163,484 $34,549 $4,455,759 $58,509 $33,293
63,815 2.9 Experience Period Member Months 63,815 1,581 0 5,357 66 10,041 114 108
2.10 Current Enrollment 5,812 416 0 314 2 877 9 10
2.11 Current Premium PMPM $571.88 $580.60 $0.00 $623.25 $810.19 $447.71 $583.38 $246.92
2.12 Loss Ratio 103.91% 70.19% #DIV/0! 85.57% 5.21% 41.67% 21.91% 6.41%
Per Member Per Month
2.13 Allowed Claims $616.54 $504.19 #DIV/0! $575.13 $125.05 $262.36 $334.97 $35.35
2.14 Reinsurance $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
2.15 Member Cost Sharing $102.53 $126.65 #DIV/0! $134.84 $101.74 $109.12 $239.19 $20.47
2.16 Cost Sharing Reduction $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
2.17 Incurred Claims $514.01 $377.54 #DIV/0! $440.29 $23.32 $153.25 $95.78 $14.88
2.18 Risk Adjustment Transfer Amount -$75.97 -$75.97 #DIV/0! -$75.97 -$75.97 -$75.97 -$75.97 -$75.97
2.19 Premium $570.63 $613.84 #DIV/0! $590.53 $523.47 $443.76 $513.23 $308.27
Section III: Plan Adjustment Factors
3.1 Plan ID (Standard Component ID) 94788NY0280017 94788NY0280018 94788NY0280021 94788NY0280022 94788NY0280029 94788NY0280030 94788NY0280047
3.2 Market Adjusted Index Rate
3.3 AV and Cost Sharing Design of Plan 0.7090 0.7090 0.7330 0.7330 0.6340 0.6340 0.5470
3.4 Provider Network Adjustment 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000
3.5 Benefits in Addition to EHB 1.0040 1.0040 1.0040 1.0040 1.0040 1.0040 1.0000
Administrative Costs
3.6 Administrative Expense 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70%
3.7 Taxes and Fees 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90%
3.8 Profit & Risk Load 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00%
3.9 Catastrophic Adjustment 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000
Product/Plan Level Calculations
$627.44
HMO
94788NY028
5.46%
5.46%

3.10 Plan Adjusted Index Rate $516.94 $516.94 $534.44 $534.44 $462.26 $462.26 $397.24
3.11 Age Calibration Factor 1.0000
3.12 Geographic Calibration Factor 1.0000
3.13 Tobacco Calibration Factor 1.0000
3.14 Calibrated Plan Adjusted Index Rate $516.94 $516.94 $534.44 $534.44 $462.26 $462.26 $397.24
Section IV: Projected Plan Level Information
4.1 Plan ID (Standard Component ID) Total 94788NY0280017 94788NY0280018 94788NY0280021 94788NY0280022 94788NY0280029 94788NY0280030 94788NY0280047
4.2 Allowed Claims $45,287,830 $917,539 $0 $3,546,398 $9,500 $3,032,348 $43,956 $4,394
4.3 Reinsurance $0 $0 $0 $0 $0 $0 $0 $0
4.4 Member Cost Sharing $7,011,615 $214,579 $0 $774,073 $7,195 $1,174,119 $29,221 $2,369
4.5 Cost Sharing Reduction $0 $0 $0 $0 $0 $0 $0 $0
4.6 Incurred Claims $38,276,215 $702,960 $0 $2,772,325 $2,305 $1,858,229 $14,735 $2,026
4.7 Risk Adjustment Transfer Amount $0 $0 $0 $0 $0 $0 $0 $0
4.8 Premium $27,283,896 $815,061 $0 $3,209,638 $2,654 $2,171,543 $17,086 $2,448
4.9 Projected Member Months 63,815 1,581 0 5,357 66 10,041 114 108
4.10 Loss Ratio 140.29% 86.25% #DIV/0! 86.37% 86.86% 85.57% 86.24% 82.76%
Per Member Per Month
4.11 Allowed Claims $709.67 $580.35 #DIV/0! $662.01 $143.94 $302.00 $385.58 $40.69
4.12 Reinsurance $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
4.13 Member Cost Sharing $109.87 $135.72 #DIV/0! $144.50 $109.02 $116.93 $256.32 $21.93
4.14 Cost Sharing Reduction $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
4.15 Incurred Claims $599.80 $444.63 #DIV/0! $517.51 $34.92 $185.06 $129.25 $18.76
4.16 Risk Adjustment Transfer Amount $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
4.17 Premium $427.55 $515.54 #DIV/0! $599.15 $40.21 $216.27 $149.88 $22.66
1.0000
1.0000
1.0000

To add a product to Worksheet 2 - Plan Product Info, select the Add Product button or Ctrl + Shift + P.
To add a plan to Worksheet 2 - Plan Product Info, select the Add Plan button or Ctrl + Shift + L.
State: NY To validate, select the Validate button or Ctrl + Shift + I.
Market: Individual To finalize, select the Finalize button or Ctrl + Shift + F.
IHPX1038 IHGX2039 IHSX3198 IHBX4055 IHPX1039 IHGX2040 IHSX3202 IHBX4056 IHBXC026 IHGXC026 IHPXC025 IHSXC040
94788NY0280053 94788NY0280054 94788NY0280055 94788NY0280059 94788NY0280064 94788NY0280065 94788NY0280066 94788NY0280070 94788NY0280079 94788NY0280080 94788NY0280081 94788NY0280082
Platinum Gold Silver Bronze Platinum Gold Silver Bronze Bronze Gold Platinum Silver
0.887 0.809 0.720 0.634 0.887 0.809 0.720 0.634 0.634 0.809 0.887 0.720
Renewing Renewing Renewing Renewing Renewing Renewing Renewing Renewing Renewing Renewing Renewing Renewing
HMO HMO HMO HMO HMO HMO HMO HMO HMO HMO HMO HMO
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020
8.40% 4.30% 3.20% 5.10% 8.80% 5.10% 3.60% 6.00% 1.60% 1.80% 5.90% -0.90%
94788NY0280053 94788NY0280054 94788NY0280055 94788NY0280059 94788NY0280064 94788NY0280065 94788NY0280066 94788NY0280070 94788NY0280079 94788NY0280080 94788NY0280081 94788NY0280082
$5,779,277 $2,160,574 $2,450,507 $4,244,827 $3,049 $555 $0 $7,841 $75,912 $28,805 $155,200 $5,926
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$274,493 $291,073 $480,266 $1,600,305 $312 $66 $0 $5,250 $46,790 $8,563 $5,556 $3,704
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$5,504,783 $1,869,501 $1,970,241 $2,644,522 $2,738 $490 $0 $2,592 $29,122 $20,242 $149,644 $2,223
-$280,615 -$208,069 -$304,089 -$1,192,805 -$912 -$304 $0 -$4,558 -$31,070 -$7,217 -$8,052 -$4,710
$3,100,272 $2,019,409 $2,604,298 $6,506,539 $8,460 $3,094 $0 $21,773 $70,948 $30,531 $39,674 $16,918
3,694 2,739 4,003 15,702 12 4 0 60 409 95 106 62
760 265 704 963 31 0 25 17 11 275 5 12
$870.48 $750.97 $621.87 $448.69 $822.90 $810.56 $629.24 $464.46 $205.81 $338.46 $346.54 $258.98
195.23% 103.21% 85.65% 49.77% 36.27% 17.56% #DIV/0! 15.05% 73.03% 86.82% 473.23% 18.21%
$1,564.50 $788.82 $612.17 $270.34 $254.10 $138.86 #DIV/0! $130.69 $185.60 $303.21 $1,464.15 $95.59
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
$74.31 $106.27 $119.98 $101.92 $25.98 $16.40 #DIV/0! $87.50 $114.40 $90.14 $52.42 $59.74
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
$1,490.20 $682.55 $492.19 $168.42 $228.13 $122.46 #DIV/0! $43.19 $71.20 $213.07 $1,411.73 $35.85
-$75.97 -$75.97 -$75.97 -$75.97 -$75.97 -$75.97 #DIV/0! -$75.97 -$75.97 -$75.97 -$75.97 -$75.97
$839.27 $737.28 $650.59 $414.38 $704.97 $773.40 #DIV/0! $362.89 $173.47 $321.38 $374.28 $272.87
94788NY0280053 94788NY0280054 94788NY0280055 94788NY0280059 94788NY0280064 94788NY0280065 94788NY0280066 94788NY0280070 94788NY0280079 94788NY0280080 94788NY0280081 94788NY0280082
0.9200 0.8330 0.7460 0.6450 0.9200 0.8330 0.7460 0.6450 0.6450 0.8330 0.9200 0.7460
1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000
1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000
10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70%
1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90%
1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00%
1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000
Product/Plan Level Calculations
$627.44
HMO
94788NY028
5.46%
5.46%

$668.11 $604.93 $541.75 $468.40 $668.11 $604.93 $541.75 $468.40 $468.40 $604.93 $668.11 $541.75
$668.11 $604.93 $541.75 $468.40 $668.11 $604.93 $541.75 $468.40 $468.40 $604.93 $668.11 $541.75
94788NY0280053 94788NY0280054 94788NY0280055 94788NY0280059 94788NY0280064 94788NY0280065 94788NY0280066 94788NY0280070 94788NY0280079 94788NY0280080 94788NY0280081 94788NY0280082
$6,652,297 $2,486,951 $2,820,682 $4,886,052 $3,510 $639 $0 $9,026 $87,379 $33,156 $178,645 $6,822
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$294,155 $311,922 $514,667 $1,714,932 $334 $70 $0 $5,626 $50,142 $9,177 $5,954 $3,969
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$6,358,142 $2,175,030 $2,306,015 $3,171,119 $3,176 $569 $0 $3,400 $37,237 $23,979 $172,690 $2,853
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$7,305,281 $2,507,554 $2,670,482 $3,705,262 $3,652 $655 $0 $3,968 $45,343 $28,343 $203,503 $3,422
3,694 2,739 4,003 15,702 12 4 0 60 409 95 106 62
87.03% 86.74% 86.35% 85.58% 86.96% 86.87% #DIV/0! 85.69% 82.12% 84.60% 84.86% 83.35%
$1,800.84 $907.98 $704.64 $311.17 $292.49 $159.83 #DIV/0! $150.43 $213.64 $349.01 $1,685.33 $110.02
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
$79.63 $113.88 $128.57 $109.22 $27.84 $17.57 #DIV/0! $93.77 $122.60 $96.60 $56.17 $64.01
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
$1,721.21 $794.10 $576.07 $201.96 $264.65 $142.26 #DIV/0! $56.67 $91.04 $252.42 $1,629.15 $46.01
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00
$1,977.61 $915.50 $667.12 $235.97 $304.34 $163.77 #DIV/0! $66.13 $110.86 $298.35 $1,919.84 $55.20
1.0000
1.0000
1.0000

IHPX1136 IHPX1137 IHGX2135 IHGX2136 IHBX4151 IHBX4152 IHPX5101 IHPX5102 IHSX5101 IHSX5102 IHPF1055 IHPF1056
94788NY0280129 94788NY0280130 94788NY0280131 94788NY0280132 94788NY0280145 94788NY0280146 94788NY0280147 94788NY0280148 94788NY0280149 94788NY0280150 94788NY0280133 94788NY0280134
Platinum Platinum Gold Gold Bronze Bronze Platinum Platinum Silver Silver Platinum Platinum
0.885 0.885 0.820 0.820 0.625 0.625 0.877 0.877 0.700 0.700 0.880 0.880
Renewing Renewing Renewing Renewing Renewing Renewing New New New New Terminated Terminated
HMO HMO HMO HMO HMO HMO HMO HMO HMO HMO HMO HMO
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No No
1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020
4.10% 4.60% 8.80% 9.10% 5.20% 5.90% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
94788NY0280129 94788NY0280130 94788NY0280131 94788NY0280132 94788NY0280145 94788NY0280146 94788NY0280147 94788NY0280148 94788NY0280149 94788NY0280150 94788NY0280133 94788NY0280134
$1,630,865 $11,701 $2,259,750 $16,587 $0 $0 $0 $0 $0 $0 $8,446,194 $191,907
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$140,125 $1,230 $345,266 $3,010 $0 $0 $0 $0 $0 $0 $362,040 $10,394
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$1,490,741 $10,470 $1,914,485 $13,577 $0 $0 $0 $0 $0 $0 $8,084,153 $181,513
-$86,144 -$3,039 -$257,066 -$6,381 $0 $0 $0 $0 $0 $0 -$423,202 -$25,524
$940,714 $19,875 $2,372,144 $37,425 $0 $0 $0 $0 $0 $0 $4,511,995 $155,382
1,134 40 3,384 84 0 0 0 0 0 0 5,571 336
85 6 262 0 753 10 0 0 0 0 0 0
$908.21 $855.85 $730.64 $0.00 $434.28 $401.41 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
174.44% 62.19% 90.52% 43.73% #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! 197.71% 139.78%
$1,438.15 $292.52 $667.77 $197.47 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $1,516.10 $571.15
$0.00 $0.00 $0.00 $0.00 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $0.00 $0.00
$123.57 $30.76 $102.03 $35.84 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $64.99 $30.93
$0.00 $0.00 $0.00 $0.00 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $0.00 $0.00
$1,314.59 $261.76 $565.75 $161.63 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $1,451.11 $540.22
-$75.97 -$75.97 -$75.97 -$75.97 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! -$75.97 -$75.97
$829.55 $496.88 $700.99 $445.54 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $809.91 $462.45
94788NY0280129 94788NY0280130 94788NY0280131 94788NY0280132 94788NY0280145 94788NY0280146 94788NY0280147 94788NY0280148 94788NY0280149 94788NY0280150 94788NY0280133 94788NY0280134
0.9160 0.9160 0.8450 0.8450 0.6280 0.6280 0.8920 0.8920 0.7050 0.7050 0.0000 0.0000
1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000
1.0040 1.0040 1.0040 1.0040 1.0040 1.0040 1.0040 1.0040 1.0040 1.0040 0.0000 0.0000
10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70%
1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90%
1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00%
1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000
$627.44
HMO
94788NY028
5.46%
5.46%

$667.87 $667.87 $616.10 $616.10 $457.88 $457.88 $650.37 $650.37 $514.03 $514.03 $0.00 $0.00
$667.87 $667.87 $616.10 $616.10 $457.88 $457.88 $650.37 $650.37 $514.03 $514.03 $0.00 $0.00
94788NY0280129 94788NY0280130 94788NY0280131 94788NY0280132 94788NY0280145 94788NY0280146 94788NY0280147 94788NY0280148 94788NY0280149 94788NY0280150 94788NY0280133 94788NY0280134
$1,877,224 $13,468 $2,601,109 $19,093 $0 $0 $0 $0 $0 $0 $9,722,079 $220,896
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$150,162 $1,318 $369,997 $3,226 $0 $0 $0 $0 $0 $0 $387,973 $11,138
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$1,727,063 $12,150 $2,231,113 $15,867 $0 $0 $0 $0 $0 $0 $9,334,107 $209,758
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$1,984,263 $13,972 $2,571,463 $18,302 $0 $0 $0 $0 $0 $0 $0 $0
1,134 40 3,384 84 0 0 0 0 0 0 5,571 336
87.04% 86.96% 86.76% 86.69% #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0!
$1,655.40 $336.71 $768.65 $227.30 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $1,745.12 $657.43
$0.00 $0.00 $0.00 $0.00 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $0.00 $0.00
$132.42 $32.96 $109.34 $38.41 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $69.64 $33.15
$0.00 $0.00 $0.00 $0.00 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $0.00 $0.00
$1,522.98 $303.75 $659.31 $188.89 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $1,675.48 $624.28
$0.00 $0.00 $0.00 $0.00 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $0.00 $0.00
$1,749.79 $349.30 $759.89 $217.89 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! $0.00 $0.00
1.0000
1.0000
1.0000

IHPFC012 IHGF2045 IHGF2046 IHGFC013 IHSF3074 IHSF3075 IHSFC014 IHBF4059 IHBF4060 IHBFC015
94788NY0280135 94788NY0280136 94788NY0280137 94788NY0280138 94788NY0280139 94788NY0280140 94788NY0280141 94788NY0280142 94788NY0280143 94788NY0280144
Platinum Gold Gold Gold Silver Silver Silver Bronze Bronze Bronze
0.880 0.798 0.798 0.798 0.720 0.720 0.720 0.621 0.621 0.621
Terminated Terminated Terminated Terminated Terminated Terminated Terminated Terminated Terminated Terminated
HMO HMO HMO HMO HMO HMO HMO HMO HMO HMO
No No No No No No No No No No
1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020 1/1/2020
0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
94788NY0280135 94788NY0280136 94788NY0280137 94788NY0280138 94788NY0280139 94788NY0280140 94788NY0280141 94788NY0280142 94788NY0280143 94788NY0280144
$0 $2,140,208 $222,061 $0 $2,348,349 $33,530 $1,414 $555,061 $11,580 $0
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$0 $305,401 $26,052 $0 $352,045 $9,816 $1,171 $210,387 $5,236 $0
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$0 $1,834,806 $196,009 $0 $1,996,304 $23,714 $243 $344,674 $6,343 $0
$0 -$265,346 -$30,842 $0 -$227,136 -$14,585 -$1,823 -$140,991 -$11,471 -$76
$0 $2,346,212 $212,673 $0 $1,822,117 $70,755 $6,042 $731,409 $49,702 $164
0 3,493 406 0 2,990 192 24 1,856 151 1
0 0 0 0 0 0 0 0 0 0
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
#DIV/0! 88.18% 107.80% #DIV/0! 125.16% 42.22% 5.77% 58.38% 16.59% 0.00%
#DIV/0! $612.71 $546.95 #DIV/0! $785.40 $174.64 $58.92 $299.06 $76.69 $0.00
#DIV/0! $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
#DIV/0! $87.43 $64.17 #DIV/0! $117.74 $51.12 $48.78 $113.35 $34.68 $0.00
#DIV/0! $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
#DIV/0! $525.28 $482.78 #DIV/0! $667.66 $123.51 $10.14 $185.71 $42.01 $0.00
#DIV/0! -$75.97 -$75.97 #DIV/0! -$75.97 -$75.97 -$75.97 -$75.97 -$75.97 -$75.97
#DIV/0! $671.69 $523.82 #DIV/0! $609.40 $368.52 $251.76 $394.08 $329.15 $163.89
94788NY0280135 94788NY0280136 94788NY0280137 94788NY0280138 94788NY0280139 94788NY0280140 94788NY0280141 94788NY0280142 94788NY0280143 94788NY0280144
0.0000 0.0000 0.0000 0.0000 0.0000 0.0000 0.0000 0.0000 0.0000 0.0000
1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000
0.0000 0.0000 0.0000 0.0000 0.0000 0.0000 0.0000 0.0000 0.0000 0.0000
10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70% 10.70%
1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90% 1.90%
1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00%
1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000 1.0000
$627.44
HMO
94788NY028
5.46%
5.46%

$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
94788NY0280135 94788NY0280136 94788NY0280137 94788NY0280138 94788NY0280139 94788NY0280140 94788NY0280141 94788NY0280142 94788NY0280143 94788NY0280144
$0 $2,463,508 $255,605 $0 $2,703,091 $38,595 $1,628 $638,909 $13,329 $0
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$0 $327,277 $27,918 $0 $377,262 $10,519 $1,255 $225,457 $5,611 $0
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$0 $2,136,232 $227,687 $0 $2,325,830 $28,076 $373 $413,452 $7,717 $0
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0
$0 $0 $0 $0 $0 $0 $0 $0 $0 $0
0 3,493 406 0 2,990 192 24 1,856 151 1
#DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0!
#DIV/0! $705.27 $629.57 #DIV/0! $904.04 $201.02 $67.82 $344.24 $88.27 $0.00
#DIV/0! $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
#DIV/0! $93.70 $68.76 #DIV/0! $126.17 $54.79 $52.27 $121.47 $37.16 $0.00
#DIV/0! $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
#DIV/0! $611.58 $560.81 #DIV/0! $777.87 $146.23 $15.55 $222.77 $51.11 $0.00
#DIV/0! $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
#DIV/0! $0.00 $0.00 #DIV/0! $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
1.0000
1.0000
1.0000

Rating Area Data Collection Specify the total number of Rating Areas in your State by selecting the Create Rating Areas button or Ctrl + Shift + R.
If macros are disabled, press and hold the ALT key and press the F, then I, and then N key. After that, select the Enable All Content option by pressing enter. (note that you can also press the C key to select "Enable All Content") Instructions can be found in cells C1 through C4.Select only the Rating Areas you are offering plans within and add a factor for each area.
To validate, select the Validate button or Ctrl + Shift + I.
To finalize, select the Finalize button or Ctrl + Shift + F.
Rating Area Rating Factor
Rating Area 1 1.0000
Rating Area 3 1.4292
Rating Area 6 1.1328
Rating Area 7 1.1191













![2021 Vermont Individual and Small Group Rate Filing (SERFF ... Solvency... · State of Vermont For consumer assistance: Department of Financial Regulation [Banking] 888-568-4547 89](https://img.pdfslide.us/doc/110x75/5f3b65394652165b403a28b0/2021-vermont-individual-and-small-group-rate-filing-serff-solvency-state.jpg)



