Embed Size (px)
Citation preview

number of spirals on a file than on a reamer of acorresponding size (Figure 3A and B).
The second and newer manufacturing method is togrind the spirals into the tapered wire rather thantwist the wire to produce the cutting blades. Grindingis usually necessary for nickel–titanium instruments.Because of their superelasticity, they cannot betwisted.
Originally, the cross-section of the K-file wassquare and the reamer triangular. However, manufac-
turers have started using many configurations toachieve better cutting and/or flexibility. Cross-sectionis now the prerogative of individual companies.
K-Style ModificationK-style endodontic instruments came into a series ofmodifications beginning in the 1980s. Not whollysatisfied with the characteristics of their K-styleinstrument, the Kerr Manufacturing Company in
A B
C D
E F
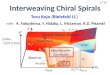
Figure 2 Comparisons of the condition of unused instruments from different manufacturers. A, New No. 30 K-file with consistently sharp blades andpoint. B, New No. 35 K-file, different brand, exhibiting dull blades. C, Cross-sectional profile of triangular No. 20 file showing consistency in angles. D,Cross-section of competing No. 20 file with dull, rounded angles of cutting blades. E, No. 15 file showing lack of consistency in the blade, reflecting poorquality control. F, New No. 08 file with no cutting blades at all.
Chapter 26 / Endodontics Instruments and Armamentarium / 815

1982 introduced a new instrument design that theytermed the K-Flex File (Sybron-Endo/Kerr, Orange,CA), a departure from the square and triangular con-figurations (Figure 3C).
The cross-section of the K-Flex is rhombus or dia-mond shaped. The spirals or flutes are produced bythe same twisting procedure used to produce thecutting edge of the standard K-type files; however,this new cross-section presents significant changes ininstrument flexibility and cutting characteristics. Thecutting edges of the high flutes are formed by the two
acute angles of the rhombus and present increasedsharpness and cutting efficiency. The alternating lowflutes formed by the obtuse angles of the rhombus aremeant to act as an auger, providing more area forincreased debris removal. The decreased contact bythe instrument with the canal walls provides a spacereservoir that, with proper irrigation, further reducesthe danger of compacting dentinal filings in the canal.Schafer16 found that the cross-sectional design andthe number of flutes will influence canal shape inseverely curved canals when employing the sameinstrumentation technique.
Testing five brands of K-type files for stiffness, Rothet al.17 found K-Flex files to be the most flexible.Moreover, not a single K-Flex fractured in torquetesting, even when twisted twice the recommendedlevel in the ADA specification.
REAMERSThe clinician should understand the importance ofdifferentiating endodontic files and reamers from burs.Burs are used for boring holes in solid materials such asgold, enamel, and dentin. Files, by definition, are usedby rasping. Reamers, on the other hand, are instrumentsthat ream (twisting)—specifically, a sharp-edged toolfor enlarging or tapering holes (see Figure 3B). Endo-dontic reamers cut by being tightly inserted intothe canal, twisted clockwise one quarter- to one half-turn to engage their blades into the dentin, and thenwithdrawn—penetration, rotation, and retraction. Thecut is made during retraction. The process is thenrepeated, penetrating deeper and deeper into the canal.When working length is reached, the next size instru-ment is used, and so on.
FILESThe tighter spiral of a file (see Figure 3A) establishes acutting angle (rake) that achieves its primary action onwithdrawal, although it will cut in the push motion aswell. The cutting action of the file can be effected ineither a filing (rasping) or a reaming (drilling) motion.In a filing motion, the instrument is placed into thecanal at the desired length, pressure is exerted againstthe canal wall, and while this pressure is maintained,the rake of the flutes rasps the wall as the instrument iswithdrawn without turning. The file need not contactall walls simultaneously. For example, the entire lengthand circumference of large-diameter canals can befiled by inserting the instrument to the desired work-ing distance and filing circumferentially around all ofthe walls.
Figure 3 ISO Group I, K-style endodontic instruments. A, K-style file. B,K-style reamer. C, K-flex file.
816 / Endodontics

To use a file in a reaming action, the motion is thesame as for a reamer—penetration, rotation, and retrac-tion. The file tends to set in the dentin more readily thanthe reamer and must therefore be treated more gingerly.Withdrawing the file cuts away the engaged dentin.
To summarize the basic action of files and reamers,it may be stated that either files or reamers may beused to ream out a round, tapered apical cavity butthat files are also used as push-pull instruments toenlarge by rasping certain curved canals as well as theovoid portion of large canals. In addition, copiousirrigation and constant cleansing of the instrumentare necessary to clear the flutes and prevent packingdebris at or through the apical foramen.
Oliet and Sorin18 evaluated endodontic reamersfrom four different manufacturers and found ‘‘consid-erable variation in the quality, sharpness of the cuttingedges, cross sectional configuration, and number offlutes of the 147 different reamers tested.’’ They furtherfound that ‘‘triangular cross sectional reamers cut withgreater efficiency than do the square cross sectionalreamers,’’ but the failure rate of the triangular instru-ments was considerably higher. Webber et al.19 foundthat ‘‘instruments with triangular cross sections wereinitially more efficient but lost sharpness more rapidlythan square ones of the same size.’’
Oliet and Sorin18 also found that ‘‘wear does notappear to be a factor in instrument function, but ratherinstruments generally fail because of deformation or
fracture of the blades. Once an instrument becamepermanently distorted, additional rotation only causedadditional distortion, with minimum cutting fre-quently leading to fracture.’’ A more recent in vitrostudy of stainless steel files demonstrated that signifi-cant wear and potential loss of efficiency occurred afteronly one use of 300 strokes. It was proposed thatendodontic instruments should be available in sterilepackaging for single-patient use.20 Another study con-cluded that stainless steel instruments, in small sizes,should be used once, and the No. 30 could be used threetimes. The No. 30 nickel–titanium instruments, how-ever, ‘‘even after five times, did not show appreciableabnormalities in shape.’’21 Of course, this study wasdone with one type of hand nickel–titanium files, andthere was no assessment of instrumentation time ascompared with stainless steel files.21
Webber et al.19 used a linear cutting motion inmoist bovine bone and found that ‘‘there was a widerange of cutting efficiency between each type of rootcanal instrument, both initially and after successiveuse.’’ Similar findings were found when comparingK-type files with five recently introduced brands inthree different sizes, Nos. 20, 25, and 30.22 Significantdifferences were noted in the in vitro cutting effi-ciency among the seven brands. Wear was exhibitedby all instruments after three successive 3-minute testperiods. Depth of groove is also a significant factor inimproving cutting ability (Figure 4).
Figure 4 Comparison between two competing brands of endodontic instruments showing widely different cutting ability related to the depth of theblade groove.
Chapter 26 / Endodontics Instruments and Armamentarium / 817

Neal et al.23 also studied the cutting ability ofK-type files. A wide variance in the cutting abilityof individual files was found. This study appears toconfirm what dentists have long noted: the widevariance in cutting ability among individual instru-ments, even from the same manufacturer. Contraryto the study by Newman et al.,22 this study reportedan insignificant role played by wear in decreasingthe cutting ability of regular K-type stainless steelfiles.23 Current studies have shown that stainless steelhand files have better cutting efficiency than nickel–titanium hand files and are not adversely affected bysodium hypochlorite.24,25 A study by Schafer26 alsodemonstrated that the cross-sectional design ofstainless steel hand files has more of an influenceon cutting efficiency than the number of flutes. Intwo other studies that compared a recently intro-duced stainless steel file with one that has been inuse for 20 years, it was confirmed that stainless steelfiles that are more flexible have less machining effi-ciency than a stiffer file.27,28
Studies by Oliet and Sorin,18 Webber et al.,19 andNeal et al.23 all alluded to certain weaknesses in K-style instruments. In addition, Luks29 has shownthat the smaller reamers and files may be easilybroken by twisting the blades beyond the limits ofthe metal until the metal separated. On the otherhand, Gutierrez et al.30 found that although theinstrument did not immediately break, a progres-sion of undesirable features occurred. Locking andtwisting clockwise led to unwinding and elongationas well as the loss of blade cutting edge and blunt-ing of the tip. With continued clockwise twisting, areverse ‘‘roll-up’’ occurred. Cracks in the metaleventually developed that finally resulted in break-age. These findings were unusual in that breakagewould have normally resulted long before ‘‘roll-up’’
occurred. It may reflect a variance in the quality ofmetal used by manufacturing companies. Thispoint was borne out in a study by Lentine,31 inwhich he found a wide range of values within eachbrand of instrument as well as between brands.
An additional study of 360 � clockwise rotation(ISO revision of ADA Specification No. 28) foundonly 5 K-style files failing of 100 instruments tested.They were sizes 30 to 50, all from one manufac-turer.17
Attempts to ‘‘unscrew’’ a locked endodontic file alsopresent a problem. Chernick et al.32 demonstratedthat ‘‘endodontic files twisted in a counterclockwisemanner were extremely brittle in comparison withthose twisted in a clockwise manner.’’ They warnedthat dentists ‘‘should exercise caution when ‘backing-off’ embedded root canal instruments.’’ This findingwas supported by Lautenschlager et al.,33 who foundthat ‘‘all commercial files and reamers showed ade-quate clockwise torque, but were prone to brittlefracture when placed in counterclockwise torsion.’’
By contrast, Roane and Sabala34 found that clock-wise rotation was more likely (91.5%) to produceseparation and/or distortion than counterclockwiserotation (8.5%) when they examined 493 discardedinstruments. Seto et al.7 also found greater rotationalfailure in clockwise rotation and greater failure aswell in machined stainless steel K-files over twistedK-files.
Sotokawa35 also studied discarded instrumentsand indicted metal fatigue as the culprit in breakageand distortion. ‘‘First a starting point crack developson the file’s edge and then metal fatigue fans outfrom that point, spreading towards the file’s axialcenter’’ (Figure 5). Sotokawa35 also classified thetypes of damage to instruments (Figure 6). He foundthe No. 10 file to be the most frequently discarded.
818 / Endodontics

Figure 5 Instrument breakage. A, Initial crack across the shaft near the edge of the blade, Type V (original magnification �1,000). B, Full fracture of filebroken in a 30� twisting simulation, Type VI (original magnification �230).
A
B
Figure 6 A, Sotokawa’s classification of instrument damage. Type I, Bent instrument. Type II, Stretching or straightening of twist contour. Type III,Peeling-off metal at blade edges. Type IV, Partial clockwise twist. Type V, Cracking along axis. Type VI, Full fracture. B, Discarded rotary nickel–titaniumfiles showing visible defects without fracture. All files show unwinding, indicating a torsional defect, and are very dangerous to be used further.Reproduced with permission from Sattapan B, Nervo GJ, Palamara JEA, Messer, HH. J Endod 2000;26:161.
Chapter 26 / Endodontics Instruments and Armamentarium / 819

Haikel et al.36 compared instrument fracturebetween traditional K and Hedstrom files and thenewer ‘‘hybrid’’ instruments. They found that ‘‘theinstruments with triangular cross sections, in parti-cular the Flexofile (Dentsply/Maillefer, Tulsa, OK),were found to be the most resistant to fracture.’’Starting-point cracks and ductile fracture as well asplastic deformations and axial fractures were found(Figure 7). Schafer and Tepel37 showed that thecross-sectional design had more to do with a stain-less steel files flexibility and its ability to resist frac-ture than the number of flutes.
Rowan et al.38 compared rotation and torque tofailure of stainless steel and nickel–titanium files ofvarious sizes. An interesting relation was noted. Stain-less steel had greater rotations to failure in a clockwisedirection, and the nickel–titanium was superior in acounterclockwise direction. Despite these differences,the actual force to cause failure was the same. It shouldbe noted that the test instrument used in this study isnot the one specified in ADA Specification No. 28. Toovercome the problems chronicled above—distortion,fracture—Walia et al.39 suggested that nickel–titanium,with a very low modulus of elasticity, be substitutedfor stainless steel in the manufacture of endodonticinstruments.
TIP MODIFICATIONEarly interest in the cutting ability of endodonticinstruments centered around the sharpness, pitch,and rake of the blades. By 1980, interest had alsodeveloped in the sharpness of the instrument tip and
the tip’s effect in penetration and cutting as well as itspossible deleterious potential for ledging and/or trans-portation—machining the preparation away from thenatural canal anatomy.
Villalobos et al.40 noted that tip design, as much asflute sharpness, led to improved cutting efficiency. Feltet al.41 designed experiments to exclude tip designbecause the tip might ‘‘overshadow the cutting effectsof flute design.’’ Later, it was reported that ‘‘tips dis-played better cutting efficiency than flutes’’ and thattriangular pyramidal tips outperformed conical tips,which were least effective.42,43
At the same time that a pitch was being made forthe importance of cutting tips, other researchers wereredesigning tips that virtually eliminated their cuttingability. Powell et al.44,45 began modifying the tips ofK-files by ‘‘grinding to remove the transition angle’’from tip to first blade.
By 1988, Sabala et al.46 confirmed previous findingsthat the modified tip instruments exerted ‘‘less trans-portation and more inner curvature preparation. Themodified files maintained the original canal curvaturebetter and more frequently than did the unmodifiedfiles.’’
Powell et al.45 noted that each stainless steel ‘‘file’smetallic memory to return to a straight position,increases the tendency to transport or ledge and even-tually to perforate curved canals.’’ This action takesplace on the outer wall, the convex curvature of thecanal. They pointed out that when this tip ‘‘angle isreduced, the file stays centered within the originalcanal and cuts all sides (circumference) more evenly.’’This modified-tip file has been marketed as the
Figure 7 Instrument fracture by cracks and deformation. A, Broken Hedstrom file with starting point at (i) (far right) spreading to cracks (S) and ductilefracture (F). B, Broken K-Flex file with plastic deformations at (D) and axial fissure at (Fs). Reproduced with permission from Haikel Y, et al. J Endod1991;17:217.
820 / Endodontics

Flex-R-file (Moyco/Union Broach, Miller Dental,Bethpage, NY) (Figure 8).
Rounded-tipped files, developed by Roane,34 werecompared with other files with triangular cross-sections and various forms of tip modification.Although the round-tipped files were the least effi-cient, they prepared canals more safely and with lessdestruction than did the other files.47 This study wasdone with stainless steel hand files in plastic blockswith balanced forces instrumentation.47
HEDSTROM FILESH-type files are made by cutting the spiraling flutesinto the shaft of a piece of round, tapered, stainlesssteel wire. Actually, the machine used is similar to ascrew-cutting machine. This accounts for the resem-blance between the Hedstrom configuration and awood screw (Figure 9A).
It is impossible to ream or drill with this instru-ment. To do so locks the flutes into the dentin muchas a screw is locked in wood. To continue the drillingaction would fracture the instrument. Furthermore,the file is impossible to withdraw once it is locked inthe dentin and can be withdrawn only by backing offuntil the flutes are free. This action also ‘‘separates’’files. Zinelis and Margelos48 stated that fatigue is theprimary cause of failure of Hedstrom files, whereasKosti et al.49 feel that the instrumentation techniquethat is used with the Hedstrom files also can contri-bute to their failure. Kazemi et al.50 used two differentmaterials to fabricate identical Hedstrom type ofinstruments. One set was made with stainless steel
and the other with nickel–titanium. These files werethen tested for flexibility and resistance to fracture.The torsional moment for the stainless steel files was
Figure 8 Flex-R-file with noncutting tip. A, Note rounded tip. B, ‘‘Nose’’ view of a noncutting tip ensures less gouging of the external wall and reducedcavity transport. From Ingle JI, Bakland LK. Endodontics, 5th ed. 2002, Ingle JI. et al. Endodontic Cavity Preparation. Page 483.
Figure 9 ISO Group I, H-style instruments. A, Maillefer Hedstrom file resem-bling a wood screw. B, Modified Hedstrom file (left) with noncutting tip.‘‘Safety’’ Hedstrom (right) with flattened noncutting side to prevent ‘‘stripping.’’Reproduced with permission from Keate KC, Wong M. J Endod 1990;16:488.
Chapter 26 / Endodontics Instruments and Armamentarium / 821

significantly higher than the nickel–titanium althoughthe angular deflection for the nickel–titanium wassignificantly higher than the stainless steel.50
Hedstrom files cut in one direction only—retraction.Because of the very positive rake of the flute design, theyare more efficient as files per se.51–55 Yguel-Henry et al.54
reported on the importance of the lubricating effect ofliquids on cutting efficiency, raising this efficiency by30% with H-style files and 200% with K-files. Mizrahiet al.,52 however, reported the proclivity that H-files havefor packing debris at the apex. On the other hand, ElDeeb and Boraas55 found that H-files tended not to packdebris at the apex and were the most efficient.
Hedstrom files are not to be used in a torquingaction. For this reason, ADA Specification No. 28could not apply, and a new specification, No. 58, wasapproved by the ADA and the American NationalStandards Committee.56
H-STYLE FILE MODIFICATIONThe Hyflex file (Coltene/Whaledent/Hygenic, Mahwah,NJ) in cross-section presents an ‘‘S’’ shape rather thanthe single-helix teardrop cross-sectional shape ofthe true Hedstroem file. The ‘‘S’’ File (J-S Dental,Ridgefield, CT) also appears to be a variation of theH-style file in its double-helix configuration. Reportson this instrument are very favorable.57 Buchananhas further modified the Hedstroem file, the SafetyHedstrom (Sybron-Endo/Kerr), which has a noncuttingside to prevent ledging in curved canals (Figure 9, B).
U-FILEAn instrument for which there is no ISO or ANSI/ADA specification as yet is the U-File. It is marketedas ProFiles, GT Files (Dentsply/Tulsa Dental, Tulsa,OK), and LIGHTSPEED (LightSpeed TechnologyInc., San Antonio, TX). The U-File’s cross-sectionalconfiguration has two 90 � cutting edges at each of thethree points of the blade (Figure 10). The flat cuttingsurfaces act as a planing instrument and are referredto as radial lands. A noncutting pilot tip ensures thatthe file remains in the lumen of the canal, thus avoid-ing transportation and ‘‘zipping’’ at the apex. The filesare used in both a push-pull and rotary motion and
are very adaptable to nickel–titanium rotary instru-ments. ProFiles are supplied in a variety of tapers andISO tip sizes of 15 through 80.
GT ProFiles, developed by Buchanan in the U-design, are unusual in that the cutting blades extendup the shaft only 6 to 8 mm rather than 16 mm, andthe tapers start at 0.06 mm/mm (instead of 0.02), aswell as 0.08 and 0.10, tapered instruments. They aremade of nickel–titanium and come as hand instru-ments and rotary files. GT instruments all start with anoncutting tip ISO size 20.
LIGHTSPEED LSXThe distinctive design of LightSpeed instruments (DiscusDental, Culver City, CA) maximizes flexibility and allowslarger apical preparations without unnecessary removal ofdentin. The LSX has a non-cutting shaft and very shortblade. After making straight-line access to about mid-root, the coronal third is flared with the instrument ofchoice (not with the LSX). After flaring, at least a #15K-file is used to obtain patency to working length (WL).A #20 LSX and sequentially larger sizes are used to preparethe apical third. The final apical instrument size (FAS) is
Figure 11 The newly designed LightSpeed LSX NiTi rotary instrument (Discus Dental, Culver City, CA) maximizes flexibility that allows for enlargedapical preparations. The distinctive cutting head terminates a noncutting shaft. It should be used at 2500-3000 RPM and irrigation is required throughoutthe enlarging procedure. The new LSX is used to prepare a tapered and circular apical preparation in an ovoid canal.
Figure 10 Cross-sectional view of a U-File reveals six corners in cuttingblades compared with four corners in square stock and three corners intriangular stock K-files. Courtesy of John McSpadden.
822 / Endodontics

the blade size that encounters 4mm or more of cuttingresistance apically. A 4mm step back with the next larger(than the FAS) instrument completes the apical prepara-tion. The mid-root is then cleaned and tapered with thenext two or three sequentially larger LSX sizes, blendingmid-root instrumentation with the previously preparedcoronal third. Recapitulation usually is necessary onlyonce – with the FAS – at the end of canal preparation. Thenew LSX is to be used at 2500 rpm, and irrigation isrequired throughout the procedure.
GATES GLIDDEN MODIFICATIONAnother hand instrument also designed for apical pre-paration was the Flexogate (Dentsply/Maillefer), but itis no longer manufactured. Briseno et al.62 comparedFlexogates and Canal Master (Brasseler, Savannah, GA)in vitro and found Flexogates less likely to cause apicaltransportation.
QUANTEC ‘‘FILES’’The Quantec instrument (Sybron-Endo/Kerr), althoughcalled a ‘‘file,’’ was more like a reamer. It was notdesigned to be used in the file’s push-pull action butrather in the reamer’s rotary motion. The radial lands ofthe Quantec were slightly relieved to reduce frictionalcontact with the canal wall, and the helix angle is con-figured to remove debris. It is no longer manufactured.
HAND INSTRUMENT CONCLUSIONSThe literature is replete with references to the superiorityof one instrument or one method of preparation over all
others.55,63–66 Quite true is Briseno’s67 statement,‘‘Regardless of the instrument type, none was able toreproduce ideal results; however, clinically acceptableresults could be obtained with all of them.’’ All too oftenclinicians report success with instruments and techniqueswith which they are most comfortable. No ulteriormotive is involved, but often a report reflects badly onan instrument when it is the clinician’s inexperience withan unfamiliar technique that is unknowingly beingreported. Stenman and Spangberg68 said it ‘‘is difficultto assess, as results from published investigations oftenvary considerably.’’
BARBED BROACHESBarbed broaches are short-handled instruments usedprimarily for vital pulp extirpation. They are also usedto loosen debris in necrotic canals or to remove paperpoints or cotton pellets. ISO Specification No. 63 setsthe standards for barbed broaches. Rueggenbergand Powers69 tested all sizes of broaches from threemanufacturers and found significant differences in shape,design, and size, as well as results from torsion anddeflection tests. The authors warned that a ‘‘jammedbroach’’ should be removed vertically without twisting.
Broaches are manufactured from round wire, thesmooth surface of which has been notched to form barbsbent at an angle from the long axis (Figure 12A). Thesebarbs are used to engage the pulp as the broach is rotatedwithin the canal until it begins to meet resistance againstthe walls of the canal. The broach should never be forcedinto a canal beyond the length where it first begins tobind. Forcing it farther apically causes the barbs to be
Figure 12 A, Barbed broach. As a result of a careless barbing process, the effective shaft diameter is greatly reduced. Size ‘‘coarse.’’ B, Ductile failure of size‘‘xx fine’’ barbed broach fractured after axial twisting greater than 130�. Reproduced with permission from Rueggenberg FA, Powers JM. J Endod 1988;14:133.
Chapter 26 / Endodontics Instruments and Armamentarium / 823

compressed by the canal walls. Subsequent efforts towithdraw the instrument will embed the barbs in thewalls. Increased withdrawal pressure to retrieve theinstrument results in breaking off the embedded barbsor the shaft of the instrument itself at the point ofengagement (Figure 12B). A broken barbed broachembedded in the canal wall is seldom retrievable.
Nickel–Titanium Endodontic
Instruments
A new generation of endodontic instruments, madefrom nickel–titanium, has added a new dimension tothe practice of endodontics.70,71 The superelasticity ofnickel–titanium, the property that allows it to returnto its original shape following significant deformation,differentiates it from other metals, such as stainlesssteel, that sustain deformation and retain permanentshape change. These properties make nickel–titaniumendodontic files more flexible and better able to con-form to canal curvature, resist fracture, and wear lessthan stainless steel files (see Chapter 25B, ‘‘Introduc-tion of Nickel–Titanium Alloy to Endodontics’’).
SUPERELASTICITYAlloys such as nickel–titanium, that show superelasti-city, undergo a stress-induced martensitic transforma-tion from a parent structure, which is austenite. Onrelease of the stress, the structure reverts back toaustenite, recovering its original shape in the process.Deformations involving as much as a 10% strain canbe completely recovered in these materials, as com-pared with a maximum of 1% in conventional alloys.
In a study comparing piano wire and a nickel–titaniumwire, Stoeckel and Yu71 found that a stress of2,500 MPa was required to stretch a piano wire to 3%strain, as compared with only 500 MPa for a nickel–titanium wire. At 3% strain, the music wire breaks. Onthe other hand, the nickel–titanium wire can bestretched much beyond 3% and can recover most ofthis deformation on the release of stress. The super-elastic behavior of nickel–titanium also occurs over alimited temperature window. Minimum residualdeformation occurs at approximately room tempera-ture.71 A composition consisting of 50 atomic percentnickel and 50 atomic percent titanium seems ideal,both for instrumentation and manufacture.
MANUFACTUREToday, nickel–titanium instruments are precisionground into different designs (K style, Hedstrom,
Flex-R, U-files, and drills) and are made in differentsizes and tapers. The nickel–titanium alloy is difficultto machine as the properties of the alloy can be chan-ged during the manufacturing process. Variables suchas feed rate, lubrication, and heat treating during thefabrication process can influence the final product.72
Just now there are new manufacturing methods thatemploy casting of the alloy or stamping wire blanks.In addition, spreaders and pluggers are also available.Nickel–titanium instruments are as effective as or betterthan comparable stainless steel instruments in machin-ing dentin, and nickel–titanium instruments are morewear resistant.73 U and drill designs make it possible touse mechanical (i.e., rotary handpiece) instrumentation.Moreover, rotary motors now offer the potential forimproved torque control with automatic reversal thatmay decrease rotary instrument breakage.
Finally, nickel–titanium files are biocompatible andappear to have excellent anticorrosive properties.74 Inaddition, implantation studies have verified thatnickel–titanium is biocompatible and acceptable as asurgical implant.75
With the ability to machine flutes, many newdesigns such as radial lands have become available.Radial lands allow nickel–titanium files to be used asreamers in a 360� motion as opposed to the tradi-tional reamers with more acute rake angles. Althoughthe most common use of this new design has been as arotary file, the identical instrument is available as ahand instrument. In addition, a converter handle isavailable that allows the operator to use the rotary fileas a hand instrument.
TORSIONAL STRENGTH AND SEPARATIONThe clinician switching from stainless to nickel–titaniumhand instruments should not confuse nickel–titanium’ssuperelastic characteristics with its torsional stren-gth and so assume that it has super strength. Thismisconception has led to unnecessary file breakagewhen first using this new metal. Studies indicatethat instruments, whether stainless steel or nickel–titanium, meet or exceed ANSI/ADA SpecificationNo. 28. However, when reviewing the literature onthis subject the results are mixed. Canalda-Sahliet al.76 found nickel–titanium files (Nitiflex and Navi-flex) (Dentsply) to be more flexible than the stainlessfiles tested (Flexofile and Flex-R). However, the stain-less steel files were found to be more resistantto fracture. Both types of metal exceeded all ANSI/ADA specifications. Canalda-Sahli et al.,77 in anotherstudy, compared identical instruments: CanalMaster(aka LIGHTSPEED) stainless steel and CanalMaster
824 / Endodontics

nickel–titanium. Within these designs, the nickel–titanium values were superior in all aspects to those ofstainless steel of the same design.
Tepel et al.12 looked at bending and torsionalproperties of 24 different types of nickel–titanium,titanium–aluminum, and stainless steel instruments.They found the nickel–titanium K-files to be the mostflexible, followed in descending order by titanium–aluminum, flexible stainless steel, and conventionalstainless steel. When testing for resistance to fracturefor 21 brands, however, they found that No. 25 stain-less steel files had a higher resistance to fracture thantheir nickel–titanium counterpart.
Wolcott and Himel13 compared the torsional prop-erties of stainless steel K-type and nickel–titanium U-type instruments. As in previous studies, all of thestainless steel instruments showed no significant dif-ference between maximum torque and torque at fail-ure, whereas the nickel–titanium instruments showeda significant difference between maximum torque andtorque at failure. Essentially, this means that the timebetween ‘‘windup’’ and fracture in nickel–titaniuminstruments is extended, which could lead to a falsesense of security.
While studying cyclic fatigue using nickel–titaniumLightSpeed instruments, Pruett et al.78 determinedthat canal curvature and the number of rotationsdetermined file breakage. Separation occurred at thepoint of maximum curvature of the shaft.
Cyclic fatigue should be considered a valid term,even for hand instrumentation, in light of the factthat many manufacturers are placing handles onfiles designed for rotational use. From these studies,it seems that if the clinician is changing from ahigh-torque instrument, such as stainless steel, toa low-torque instrument, such as nickel–titanium,it would be wise to know that nickel–titaniuminstruments are more efficient and safer when usedpassively. Although instrument breakage should berare, any instrument, hand or rotary, can break. Itis the clinician’s knowledge and experience, alongwith the manufacturer’s quality control, that willultimately minimize breakage. If breakage occurs,the fractured piece can occasionally be removed orbypassed using ultrasonics and hand instruments inconjunction with magnification. Dentists havingproblems with file breakage should seek help inevaluating one’s technique. One should practiceon extracted teeth until a level of confidence isreached that will help ensure safe and efficientpatient care.
The following is a list of situations that placenickel–titanium hand or rotary instruments at riskalong with suggestions for avoiding problems.
Nickel–Titanium Precautions and Prevention
1. Often too much pressure is applied to the file.Never force a file! These instruments require apassive technique. If resistance is encountered,stop immediately, and before continuing, increasethe coronal taper and negotiate additional length,using a smaller, 0.02 taper stainless steel hand file.Stainless steel files should be used in sizes smallerthan a No. 15. If one is using more finger pressurethan that required to break a No. 2 pencil lead,too much pressure is being used.
2. Canals that join abruptly at sharp angles are oftenfound in roots such as the mesiobuccal root ofmaxillary molars, all premolars, and mandibularincisors and the mesial roots of mandibular molars.The straighter of the two canals should first beenlarged to working length and then the other canal,only to where they join. If not, a nickel–titanium filemay reverse its direction at this juncture, bendingback on itself and damaging the instrument.
3. Curved canals that have a high degree andsmall radius of curvature are dangerous.78 Suchcurvatures (over 60 � and found 3 to 4 mmfrom working length) are often seen in thedistal canals of mandibular molars and thepalatal roots of maxillary first molars.
4. Files should not be overused! Clinicians haveexperienced more fracture after files have been useda number of times. Remember that all uses of a fileare not equal. A calcified canal stresses the file morethan an uncalcified canal. A curved canal stressesthe file more than a straight canal. One must alsobear in mind operator variability and the use oflubricants, which will affect stress. Consider dis-carding a file after abusive use in calcified orseverely curved canals even though it has been usedonly in one tooth. Use new files in hard cases andolder files in easier cases. No one knows the max-imum or ideal number of times a file can be used.Follow manufacturers’ instructions. Once only isthe safest number.
5. Instrument fatigue occurs more often during theinitial stages of the learning curve. The clinicianchanging from stainless steel to nickel–titaniumshould take continuing education courses withexperienced clinicians and educators, followed
Chapter 26 / Endodontics Instruments and Armamentarium / 825

by in vitro practice on plastic blocks andextracted teeth.
6. Ledges that develop in a canal allow space fordeflection of a file. The nickel–titanium instru-ment can then curve back on itself. A nickel–titanium instrument should not be used to bypassledges.
7. Teeth with ‘‘S’’-type curves should be approachedwith caution! Adequate flaring of the coronalthird to half of the canal, however, will decreaseproblems in these cases. It may also be necessaryto go through a series of instruments an addi-tional time or two in more difficult cases.
8. If the instrument is progressing easily in a canaland then feels as if it hits bottom, do not applyadditional pressure! This will cause the instru-ment tip to bind. Additional pressure appliedat this point may cause weakening or even break-age of the instrument. In this situation, removethe instrument and try a smaller, 0.02 taperhand instrument, either stainless steel or nickel–titanium, carefully flaring and enlarging the unin-strumented apical portion of the canal.
9. Avoid creating a canal the same size and taper ofthe instrument being used. On removal from thecanal, the debris pattern on the file should beexamined. Debris should appear on the middleportion of the file. Except for negotiating calci-fied canals and enlarging the apical portion ofthe canal, the tip and coronal section of the fileshould not carry debris. Avoid cutting with theentire length of the file blade. This total or fric-tional fit of the file in the canal will cause theinstrument to lock. If this occurs, rotate theinstrument in a counterclockwise direction andremove it from the canal. The greater the dis-tance a single file is advanced into the canal, thegreater will be the chance of files ‘‘locking up.’’When the file feels tight throughout the length ofblade, it is an indication that the orifice andcoronal one-third to two-thirds of the canalneed increased taper. Instruments of varyingdesign and/or taper can be used to avoid fric-tional fit. Nickel–titanium instruments withtapers from 0.04, 0.06, and greater, as well asGates Glidden drills and sonic/ultrasonic instru-ments, serve this purpose well.
10. Sudden changes in the direction of an instrumentcaused by the operator (i.e., jerky or jabbingmovements) must be avoided. A smooth gentlereaming or rotary motion is most efficient.
11. As with any type instrument, poor access prepara-tion will lead to procedural errors.
12. Advancing or pushing an instrument into a canalin too large an increment causes it to act as a drillor piston and greatly increases stress on the metal.Except for the most difficult cases and the neces-sity of using small instruments, the tip should notbe used to cut into or drill into the canal; itshould act only as a guide. Regardless of thetechnique being used, nickel–titanium instru-ments should be advanced in small incrementswith a more passive pressure than that used withstainless steel.
13. Do not try to make nickel–titanium do more thanit is designed to do.
14. Inspection of instruments, particularly usedinstruments, by staff and doctor is critical. Priorto insertion and on removal, look at theblade. Rotate the file, looking for deflections oflight. This indicates a damaged instrument. Alsoremember that, unlike stainless steel, nickel–titanium has an excellent memory. The file shouldbe straight. If any bend is present, the instrumentis fatigued and should be replaced.
15. Do not assume that the length of files is alwaysaccurate; measure each file. Some files are longerfrom handle to tip than others. Files may alsobecome longer or shorter if they are unraveledor twisted.
COMPARATIVE STUDIESNickel–titanium instruments function differently thanthose made of stainless steel, even when the cross-sectional design, taper, flutes, and tip are identical.Himel et al.79 compared hand nickel–titanium filingof plastic blocks with curved canals to stainless steelfiling.
Working length was maintained significantlymore often (p < .05) in the nickel–titanium groupthan in the stainless steel group. There was noledging of canals using the more flexible nickel–titanium files compared with 30.4% ledging whenstainless steel files were used. Apical zippingoccurred 31.7% less often with the Nitinol files.79
Stripping of the canal walls was less with thenickel–titanium files. An observation from thesestudies was the creation of a smooth belly shapeon the outer aspect of the apical third of the canalsinstrumented with nickel–titanium instruments.This seemed to replace the ledging that occurredwith stainless steel.
Using computed tomography, Gambill et al.80
reamed extracted teeth with either stainless
826 / Endodontics

steel or nickel–titanium files and reported that thenickel–titanium files caused less canal transporta-tion, removed less dentin, were more efficient, andproduced more centered canals. On the other hand,not all studies are in agreement concerning cuttingefficiency. Tepel et al.81 tested 24 brands of handinstruments specifically for cutting efficiency. Theyfound that flexible stainless steel files were moreefficient than nickel–titanium. However, they didnot address the quality of the completed canal.
Elliot et al.82 used resin blocks to compare stainlesssteel (Flexofiles) and nickel–titanium (Nitiflex)instruments used with either a balanced force orstep-back technique. They concluded that it is prefer-able to use nickel–titanium instruments in a balancedforce technique and stainless steel in a filing techniquebecause stainless steel files can be precurved. Consid-ering these results, nickel–titanium instrumentsshould be used as reamers, not files.
ROTARY NICKEL–TITANIUM FILESIt needs to be emphasized that the previously statedguidelines apply to all of the rotary nickel–titaniumfiles that are and will be available. Just as most ofthe preceding papers apply to hand nickel–titaniumfiles, there now exists an extensive body of litera-ture on rotary nickel–titanium files. This literaturecovers a variety of aspects from the metallurgy ofthe files to how well they clean and shape the canalsystem.
A number of studies have utilized a variety of testinstruments to investigate the properties of new andused nickel–titanium rotary files. These researchershave used such things as X-ray diffraction (XRD),scanning electron microscopy (SEM), microhardnesstesting, differential scanning calorimetry (DSC), andtemperature-modulated DSC (TMDSC). In a seriesof studies, Kuhn et al.83,84 have shown that the alloyof various files (both new and used) is fully austeni-tic at room temperature by means of XRD and DSC.They also exposed the files to various heat treatmentsto determine what if any influence these treatmentswould have on the flexibility of the files. Kim et al.85
performed cryogenic treatment on nickel–titaniuminstruments. They showed that the microhardnessof the files was increased but that there was nonoticeable change in cutting efficiency, nor was thereany change in the crystalline phase composition ofthe files. Although these results did show some dif-ferences, it is doubtful that the differences are clini-cally relevant. Brantley et al.86 looked at two differenttypes of rotary files as well as the wire blanks that
were used to fabricate the files. They compared newfiles with ones that had been used to instrumentcanals in extracted teeth. Their analysis with DSCshowed that although there were differences betweenthe files and the blanks, all of the instruments werestill fully austenitic at room temperature. In anotherstudy that compared the wire blanks with the finalproduct (ProFile instruments), Bahia et al.87 foundthat cyclic loading did change the wire blanks as wellas the instruments. However, these changes did notcompromise the instruments, nor did DSC or XRDdemonstrate any significant differences. Anotherstudy utilized DSC to compare five types of rotarynickel–titanium files and correlate these findingswith torsional and bend testing of these instruments.It was seen that a lower transformation temperatureas disclosed by DSC was correlated with an instru-ment that required a higher torsional load to fail anda higher load to bend to the maximum deflection of4 mm.88 Clinically, this would equate to an instru-ment that had increased stiffness. Whether thiswould be a noticeable increase in stiffness woulddepend in some degree on the operator. Some ofthese studies have remarked on machining defectsthat are revealed by SEM and speak to the possiblerelationship of these defects to the clinical failure ofthe instruments.
FATIGUE AND FLEXIBILITY OF ROTARYNICKEL–TITANIUM FILESThere have been a number of approaches to ascer-taining the fatigue and flexibility of rotary nickel–titanium files. Some have looked at mathematicalmodels and employed finite element analysis todevelop theoretical values. In a comparison of atriple U (ProFile) versus triple helix (HERO 642)theoretical cross-sections, it was determined thatthe triple U was more flexible but had less torsionalstrength.89 When these same cross-sections wereused to calculate theoretical torsional and bendingmoments, it was determined that the triple Umodel had a larger and higher range for torsionalstress and a higher maximum stress value.90 Thetranslation of these values into determining theclinical usability of the respective instruments isnot easily done because there are so many othervariables such as rpm, canal curvature, canal radiusof curvature, and insertion rate/force that must alsobe considered.
In another study utilizing a computer model, theProTaper instrument was compared with the ProFileinstrument. Although the ProTaper was shown to be
Chapter 26 / Endodontics Instruments and Armamentarium / 827

a stiffer instrument, it was also shown that the stressdistribution during torsional loading and bendingloads was more evenly distributed. The authors sug-gest that the ProTaper design will accumulate lessstress during usage and thus would be indicated forinstrumenting small curved canals.91
In a finite element analysis of existing nickel–titaniuminstruments, it was confirmed that as the cross-sectionalarea of the files increases, the file is more resistantto torsional forces.92 Such an interpretation is limitedby a number of factors including heat treating duringmanufacture, modification of the nickel–titaniumalloy used, and changes in any number of parametersduring fabrication such as feed rate or newness ofthe machining tools. A series of studies, more closelyrelated to the clinical usage of rotary nickel–titaniumfiles, have brought out some interesting results. Onestudy stated that there was no significant differencein fatigue resistance between new and used ProFileinstruments after clinical usage. However, the usedinstruments did fail sooner when rotated in a 90 � curvedtube.93 Another study states there is a significant differ-ence between the fatigue resistance of new and usedfiles and that larger files will fail sooner after theyare used.94,95 A clinical usage study by Bahia et al.96
confirmed these results. These results werethen verified in another study by Bahia et al.97 doneunder more controlled conditions. They demonstratedthat a used file will fail sooner than a new file. A numberof other studies have verified these results.98–101 Whenother parameters are addressed such as angle and radiusof curvature, it is seen that an increase in the angle ofcurvature or a decrease in the radius of curvature causesfiles to fail sooner.99,102,103 It is also seen that a larger fileis more resistant to torque.104–106
When Gates Glidden drills were fabricated fromnickel–titanium, it was shown that the larger the sizeof the drill, the sooner it would fail when rotated in adevice that imparted a bend to the instrument whilebeing rotated.107 An interesting sidelight in one reportdemonstrated that dry heat sterilization seemed toincrease the files’ ability to resist fatigue.98 However,it required five cycles of dry heat sterilization toachieve these results. One could question the advisa-bility of using a rotary file many times. Finally, a studylooked at the cross-sectional geometry of five differenttypes of rotary nickel–titanium files and determinedthat as the cross-section area increased, the filebecame more resistant to bending.108 This wouldseem to verify the theoretical studies that were men-tioned previously.
FORCES ENCOUNTEREDDuring canal preparation, forces are generated by theinsertion of the rotating file into the canal system. In aseries of studies utilizing a test instrument developed byBlum et al.,109 they reported some interesting findings.They have shown that the crown-down technique withProFile instruments produced less force than the step-back technique. In another study, they demonstratedthat forces were lowest when there was less engagementof the file with the canal walls.110 When the same type ofstudy was done with the ProTaper instrument in nar-row and large canals, the same conclusions werereached. The more a file was in contact with the canalwall, the higher the forces on the instrument and thecanal wall.111 These results were confirmed by othersutilizing different test instruments and test methods.When Quantec rotary files were used in extracted teeth,it was seen that a file with a larger taper generated moreforces particularly in a smaller canal.112 Peters113 con-firmed these findings; when a ProTaper instrument wasused in smaller canals, higher forces were generated.When a step-back technique utilizing RaCe rotarynickel–titanium instruments was compared with Pro-File instrumentation, it was found that the RaCe instru-ments produced less force in the canal system.114
Another study compared the use of a sequence of0.04 tapered instruments with a sequence using 0.04and 0.06 instruments. The sequence using the two dif-ferent tapers produced less force.115 A study performedwith photoelastic material showed that with less engage-ment of the canal wall, there were smaller forces gener-ated.116 It was also shown that when more flutes perunit length are engaged, higher forces are the result.117
Lubrication also influences the forces that can be gen-erated during canal instrumentation. In particular, theuse of an EDTA chelation solution significantly reducedmaximum torque values for ProFile instruments.118
SEPARATION AND DISTORTIONA separated instrument is an undesirable occurrenceduring endodontic therapy. Unfortunately, it is verydifficult to avoid when any type of rotary instrumentis used in the canal system. Two recent studies lookedat file separation and distortion. In one, only one filetype (ProFile Series 29) was utilized. These files wereused in only one patient before being discarded. Thefailure rate (separation) was less than 1%. The distor-tion rate was 15%. It is not known how many canalswere treated with any one instrument.119 A similarstudy looked at the LightSpeed instrument and found
828 / Endodontics

that for a total of 3,543 canals treated, the separationrate was 1.3%.120 When ProFile instruments wereused by dental students in their preclinical simulationlaboratory, there was a separation rate of 0.31%.121 Aclinical study that compared ProFile with ProTapersystems found a separation rate of 7% for ProFile and14% for ProTaper.122 In this study, each instrumentwas used in at least four molars or 20 premolars or 50incisors and canines. It would seem that these instru-ments were over used. In the other study, over 7,000instruments of 8 different types were examined. Theoverall distortion rate was 12% and the fracture ratewas 5%. However, these instruments were not dis-carded after being used in one patient. The meanuse of the distorted instruments was three times, andthe mean use of the undistorted instruments was fourtimes.123 In both studies, the patient treatment wasdone by endodontists. In other studies, an attempt hasbeen made to delineate what factors are important inthe distortion or separation of these files.
A series of studies considered rpm as a primaryfactor. Two studies concluded that higher rpmresulted in more separation and distortion.124,125
Another concluded that lower rpm resulted in morefile distortion, but none were fractured in thestudy.126 When two different file types were comparedat the same rpm, there were no significant differ-ences.127 When canal curvature was factored in,Zelada et al.128 stated that rpm was not a significantfactor but that a canal curvature of greater than 30 �
was significant. However, when some of the sameresearchers did a similar study, they concluded thata higher rpm did result in more separated files.129
They also stated that the angle of curvature was asignificant factor in file breakage whereas the radiusof curvature was not a factor. Yared et al.130 consid-ered other factors in a series of studies. In one study,they used sets of ProFile instruments up to 10 times.They concluded that a higher rpm resulted in moredeformation and separation of the instruments. Theyalso showed that changing the torque setting for themotors did not influence the results. In the finalanalysis, they determined that operator experiencewas a significantly important factor. In another study,they looked at the use of an air motor and comparedit with a high-torque motor and a low-torque motor.There were no significant differences.131 When a simi-lar study was done at a higher rpm setting, there wereno significant differences when comparing the airmotor with a high- or low-torque electric motor.132
Finally, they looked at operator experience as a factorwith the ProTaper instrument. They concluded thatoperator experience was a significant factor in instru-
ment separation and deformation. Unfortunately, theuse of a low-torque motor did not prevent the inex-perienced operator from separating or deformingfiles.133
A study affirming the comparison between the elec-tric and air motors showed that there were no sig-nificant differences in file distortion when either ofthese types of motors was used.134 In addition toconsidering separation and distortion of files, therehave been those who have looked at the wear ofnickel–titanium rotary files. Interestingly, they havefound that in some aspects the files improve withuse. That is, metal strips and pitted surfaces decreasedafter being used.135 When a similar study was per-formed on GT rotary files, Tripi et al.136 found thatthe frequency of defects such as disruption of thecutting edge, fretting, and craters increased. Both ofthese studies were done on human teeth. A study ofProTaper S1 instruments used clinically determinedthat multiple uses of these instruments resulted inmicrocrack formation in instruments that were notseparated. It was also found that debris was seen to betrapped in crack-like structures.137
SURFACE TREATMENTIn an effort to decrease the effects of usage, therehave been attempts to modify the surface of thenickel–titanium alloy by various means. Thesemethods include ion implantation138,139 and vapordeposition140–142 by various modalities. All of thesemethods were successful in changing the chemical com-position of the nickel–titanium alloy surface as deter-mined by XRD and other testing methods. However,in two studies, the efficacy of the vapor deposition wasnot confirmed by testing the wear or cutting effi-ciency.140,142 In two studies by Rapisarda et al.,138,139
they determined that there was better cutting efficiencyand less wear because of the changes in the surface of theinstruments. Schafer141 confirmed these findings byverifying that a vapor deposition of titanium nitridedid increase the cutting efficiency of the instruments.However, when one considers the additional cost ofmodifying these instruments, there is a question as towhether the gain in wear resistance or cutting efficiencywarrants the additional expense for an instrument thatis already considered to be disposable after as little asone use.
IRRIGANTS AND STERILIZATIONThe most common irrigant used during endodonticinstrumentation is sodium hypochlorite. It is
Chapter 26 / Endodontics Instruments and Armamentarium / 829

important to know whether this or any other irrigantwill have a deleterious effect on canal instruments.Haikel143 showed that even lengthy exposure tosodium hypochlorite did not cause nickel–titaniumfiles to fail at lower torsional moment values. Inanother study, Haikel25 determined that the samelong-term exposure to sodium hypochlorite did notdecrease the cutting efficiency of nickel–titanium files.Stokes144 determined that nickel–titanium files have avery high corrosion resistance even when immersed infull-strength sodium hypochlorite. A more recentstudy by Darabara et al.145 showed that nickel–tita-nium files were highly corrosion resistant whenexposed to sodium hypochlorite or R-EDTA. Theseinstruments are also sterilized and, depending onclinical circumstances, may be sterilized multipletimes before being discarded. Mize et al.15 lookedat LightSpeed nickel–titanium instruments andfound that multiple sterilization cycles did notinfluence the cyclic fatigue of these instruments.In a study that compared nickel–titanium files withstainless steel files, it was shown that even 40 ster-ilization cycles had no effect on the torsionalmoment at failure for either file type.146
CANAL CLEANLINESSCleaning the canal system is a primary goal in endo-dontic therapy. Many instrumentation techniques andinstruments have been developed to accomplish thisimportant task. When only the removal of smear layerwas considered, it was shown that the Quantec Series2000 instruments removed significantly more of thesmear layer in the apical third of the canal systemwhen compared with K-file hand instrumentation.147
Smear layer production by K3 was compared withProFile, and it was found that K3 instruments pro-duced less of a smear layer in the apical third of thecanal system. However, both instruments did producea smear layer.148 In a comparison of RaCe and Pro-Taper rotary files, there was no difference in canalcleanliness, but in the apical third, the RaCe systemdid produce significantly less smear layer.149 Whenthe K3 system was compared with the NiTi-TEE sys-tem, there were no significant differences in canalcleanliness or smear layer removal.150 When the K3system was compared with the RaCe system and theMtwo system, the Mtwo system was significantly bet-ter at cleaning the canal, but there were no significantdifferences for removal of the smear layer.151
Another study that compared nickel–titanium instru-mentation with stainless steel hand files showed thatcanal cleanliness was equivalent if the size of the master
apical file was the same. However, with an increase insize of the apical preparation, it was found that acleaner canal was the result regardless of the instrumenttype that was used.152 A similar study was performedutilizing GT files. All parameters except the size of theapical preparation were kept the same. The results werea larger apical preparation that left a canal system sig-nificantly cleaner.153 These results are somewhat contra-dicted by the following studies. When Ahlquist et al.154
compared stainless steel instrumentation with ProFiles,they found that the stainless steel instrumentation pro-duced a significantly cleaner canal system in the apicalthird of the canal. When canal shape or curvature wasconsidered, the results were similar. Barbizam et al.155
found that oval canals were cleaned significantly betterby hand instrumentation with stainless steel K-files.Schafer156 reported the same results with stainlesssteel K-Flexofiles as compared with K3 rotary nickel–titanium files. Iqbal et al.157 demonstrated that a com-bination technique was the best. The use of modifiedstainless steel Hedstrom files in combination with Pro-File instrumentation produced the cleanest canals. Inanother study by Schafer,158 hand instrumentation wascompared with engine-driven stainless steel files andmotor-driven ProFile instruments. None of the instru-ments produced a completely clean canal especially inthe apical third of the canal system. Hand instru-mentation with Hedstrom files produced the cleanestcanals. When another engine-driven system of stain-less steel files was compared with the ProFile or theHERO 642, it was shown that the HERO 642 pro-duced the least amount of smear layer.159 A morerecent development in automated handpieces AET(Anatomic Endodontic Technology) utilizing stain-less steel instruments was compared with the ProFilesystem and hand instrumentation with K-Flexofiles.The AET system produced significantly cleaner canalwalls with significantly less smear layer.160 Theseresults were to be expected because the AET systemspecifies that the apical third of the canal is to beprepared with hand instruments.
No canal system can be properly prepared withoutthe use of irrigants. Gambarini161 compared threeirrigation regimes and concluded that the cleanestcanal system was produced by a combination ofEDTA, sodium hypochlorite, and a surfactant. Light-Speed instrumentation was compared with ProFilewith two different irrigation techniques. There werediffering results at different levels, but essentially therewere no differences, particularly when considerationis given to the larger apical instrumentation with theLightSpeed group.162 When canal curvature wasbrought in as a variable, it was shown that the RaCe
830 / Endodontics

instrument system produced a significantly cleanercanal system than the ProTaper instrument system.163
In a comparative study with the Mtwo system, theProTaper system produced a canal system that was asclean as the Mtwo system.164 It may be presumed, ifthe canal system is being cleaned, that there is areduction or elimination of bacteria. A group of stu-dies has confirmed this presumption. Dalton et al.165
compared stainless steel K-file instrumentation of thecanal system with ProFile Series 29. There were nosignificant differences in the reduction of bacterialcounts with saline irrigation. Another study comparedhand nickel–titanium filing with the GT system withthe ProFile Series 29 preparation of the canal system.There was no significant difference in bacterial countswith saline as an irrigant.166
If sodium hypochlorite was used as an irrigant,there were no significant differences in the reduct-ion of bacterial counts when comparing handnickel–titanium preparation of the canal system withthe GT system of canal preparation.167 If a combina-tion of irrigants (5.25% NaOCl, EDTA, and calciumhydroxide) was used with GT rotary instrumentation,bacterial counts were significantly reduced. It was alsoconfirmed that larger apical instrumentation resultedin the removal of more bacteria.168
As in the past, an additional concern with canalinstrumentation is the amount of apical extrusion ofdebris. Ferraz et al.169 compared two different stain-less steel hand filing techniques (step-back versusbalanced forces) with three different nickel–titaniuminstrument systems (ProFile versus Quantec 2000 ver-sus Pow-R). As expected, there was significantly moredebris extruded through the apical foramen by thestep-back filing technique. In looking at the amountof bacteria that were extruded past the apex, a com-parison was made between the ProTaper systemand the GT system. There were no significantdifferences.170 Unfortunately, these results were notcompared with hand instrumentation or any otherinstrumentation technique. A recent study made com-parisons between three rotary systems (ProTaperversus ProFile versus HERO). All systems producedapical extrusion of debris. ProTaper caused the extru-sion of significantly more debris.171 The questionremains as to how much bacteria or debris the bodycan tolerate. It is doubtful any instrumentation tech-nique would be able to eliminate extruding any bac-teria or debris.
A final concern in the cleanliness of the canal sys-tem is whether or not the instruments themselves maybe clean before use or be able to be cleaned after being
used. Linsuwanont et al.172 showed that new rotarynickel–titanium files have metal filings and debrispresent on them. This will vary from manufacturerto manufacturer and from lot to lot. They also deter-mined that most files can not be rendered completelyclean after use. When a similar study utilized pre-soaking in an enzymatic cleaner and an ultrasonicbath, it was found that the enzymatic cleaner didnot have a significant effect. However, the ultrasonicbath did render the instruments significantly cleanerbut was not able to remove calcium hydroxide depos-its on all of the files.173
CANAL SHAPEJust as canal anatomy may limit one’s ability to cleanthe canal system, it also limits one’s ability to shapethe canal system before placing the obturation mate-rial. A major concern with any instrumentation sys-tem or technique is whether or not the canal systemwill be distorted in some fashion. When Schafer24
compared hand nickel–titanium files with stainlesssteel files of the same cross-sectional geometry, hefound that the nickel–titanium files removed lessmaterial than the stainless steel files. Another studycompared hand filing of the canal system betweennickel–titanium GT files, nickel–titanium K-files,and stainless steel K-files. In this study, Song et al.174
found significantly less transportation with thenickel–titanium files. Whenever, in a series of studies,stainless steel hand filing was compared with eithernickel–titanium hand filing or nickel–titanium rotaryfiles, there was significantly less transportation of thecanal system with the nickel–titanium files. Thisapplied to LightSpeed nickel–titanium rotary files,GT nickel–titanium rotary files, ProFile Series 29,ProFile rotary files, Pow-R, K3, RaCe, and HERO642 files.156,175–182 However, there were two excep-tions. When Peters et al.183 utilized high-resolutioncomputed tomography to assess canal transportation,they found that the ProFile system transported themost when compared with stainless steel hand filesor LightSpeed rotary nickel–titanium files. The otherexception was the study by Imura et al.184 that com-pared stainless steel Flex-R filing of the canal systemwith two rotary nickel–titanium systems andfound that all of the instruments transported the canalsystem to some degree. However, when handnickel–titanium filing was compared with rotarynickel–titanium filing, there were no significant differencesin canal transportation.185–187 The same results wereusually obtained when various rotary nickel–titanium
Chapter 26 / Endodontics Instruments and Armamentarium / 831

files were compared with each other. That is, there were nosignificant differences in canal transportation. This appliedto ProFile versus Naviflex,188 HERO 642 versus QuantecSC,189 ProTaper versus K3,190 Flexmaster versus HERO642,191 ProFile versus GT rotary versus Quantec versusProTaper,192 and ProTaper versus GT rotary.193 Of course,there were exceptions. When ProTaper was comparedwith RaCe, the RaCe instruments had significantly lesstransportation.163 However, when ProTaper was com-pared with ProFile Series 29, there was significantly moretransportation at 4 mm from the working length with theProFile Series 29 files.194 But, ProFile instruments showedsignificantly less transportation than K3 files depending oncanal curvature.195
In later studies, some of the previous comparisonswere confirmed and some were not confirmed. A studydone in simulated S-shaped canals in plastic blockscompared the ProTaper system with K3 and RaCeinstruments. It was found that the ProTaper systemcaused significantly more widening of the canal.196
However, the clinical relevance of the results are ques-tionable when one considers that the differences incanal widening were on the order of tenths of a milli-meter. When comparing Mtwo with K3 and RaCe, itwas found that the Mtwo system was significantlybetter at maintaining canal curvature.151 Again, whatis the clinical relevance of the results when it was foundthat the differences in canal curvature were less thantwo degrees? When Paque et al.149 compared ProTaperwith RaCe in extracted teeth, they found no significantdifferences for canal straightening or canal shape.
What needs to be remembered here is that canalanatomy should dictate what instruments can be usedand how they should be used. Any instrument orinstrumentation system can cause irreversible damageto the canal system. Any instrument or instrumenta-tion system can produce excellent results if they areproperly employed.
Rotary nickel–titanium files are not only used toprepare the canal system, they are also used to removegutta-percha during re-treatment procedures. Onestudy showed that ProFile instrumentation aloneleaves significantly less gutta-percha debris after re-treatment.197 However, other studies have shown nodifferences when compared with other rotary systemsor hand filing with chloroform.198,199 One study didshow that hand K-files left significantly less debris thanthe Quantec SC system.200 Other studies have looked ata number of different methodologies to remove eithergutta-percha or a polymer-based material. When K-filesactivated by the M4 or Endo-gripper automated hand-
pieces were compared with K-files alone or K3 rotaryfiles, there were no overall differences in removinggutta-percha.201 When H-files were compared with theProFile system, there were no significant differences.202
In a study comparing H-files, Flexmaster, ProTaper,and RaCe, it was determined that RaCe was significantlybetter than Flexmaster of H-files. It was also determinedthat there were no significant differences between Pro-Taper and all the other techniques.203
Finally, when H-files were compared with RaCe forthe removal of gutta-percha or a polymer-based mate-rial, there were no significant differences between thetechniques.204 In all of these studies, there was notechnique or instrumentation system that was ableto remove all of the obturation materials. One wouldnot expect that this could occur because it is notpossible to completely clean any canal system.
NITI SPREADERSThere are also nickel–titanium spreaders developedfor use in canal obturation. Berry et al.205 showedthese spreaders could penetrate further than stainlesssteel spreaders when used in curved canals. Schmidtet al.206 compared penetration depth and forcerequired to insert the spreader to place with a mastercone in place in a curved canal. The nickel–titaniumspreaders required less force and penetrated deeperthan stainless steel spreaders. Gharai et al.207 con-firmed these results and tested the adequacy of theobturation by subjecting the molar teeth to a micro-leakage test. The nickel–titanium finger spreadersproduced significantly less force, but there were nosignificant differences in microleakage.
ENGINE-DRIVEN INSTRUMENTSEngine-driven instruments can be used in three typesof contra-angle handpieces: a full rotary handpiece,latch or friction grip, a reciprocating/quarter-turnhandpiece, or a special handpiece that imparts a ver-tical stroke but with an added reciprocating quarter-turn that ‘‘cuts in’’ when the instrument is stressed. Inaddition, there are battery-powered, slow-speed hand-pieces that are combined with an apex locator,designed to prevent apical perforations. Because theinstruments used in these handpieces are generallydesigned for the type of action delivered, it is best todescribe the handpiece before discussing their instru-ments.
832 / Endodontics

ROTARY CONTRA-ANGLE HANDPIECEINSTRUMENTSInstrumentation with a full rotary handpiece is bystraight-line drilling or side cutting. Mounted withround or tapered burs or diamond points, full rotarycontra-angle handpieces can be used to develop coro-nal access to canal orifices. Special reamers may beused to funnel out orifices for easier access, to cleanand shape canals with slow-turning nickel–titaniumreamer-type instruments, and to prepare post channelsfor final restoration of the tooth.
Because some of these instruments (stainless) donot readily bend and should be used in perfectlystraight canals and because they are often misdirectedor forced beyond their limits, they can cause perfora-tions or break.
One solution to these problems is to use a slowerhandpiece: the Medidenta/Micro Mega MM 324reduction gear Handpieces (Medidenta/Micro Mega,Woodside, NY), the Aseptico Electric Motor Hand-piece (Aseptico International, Woodinville, WA), theQuantec ETM Electric torque control motor (Sybron-Endo, Irving, CA), and the Moyco/Union BroachSprint EDM Electronic Digital Motor handpiece(Miller Dental). These electric motors are specificallydesigned to power the new nickel–titanium instru-ments in canal preparation. The speeds vary from300 rpm suggested for ProFiles (Tulsa Dental) to2,000 rpm recommended for LightSpeed instruments.
Electric handpieces are available wherein not onlythe speed can be controlled but the torque as well,that is, the speed and torque can be set for a certainsize instrument and the handpiece will ‘‘stall’’ andreverse if the torque limit is exceeded. Some of thesemotors are the Aseptico ITR Motor handpiece (Asep-tico International), the Nouvag TCM ENDO motor(Nouvag, Switzerland), the Endo-Pro Electric (Medi-denta/Micro Mega), and the ProTorq motor hand-piece (Micro Motors Inc., Santa Ana, CA).
There is also the Morita Tri Auto-ZX (J. MoritaUSA Inc., Irvine, CA), a cordless, battery-powered,endodontic, slow-speed (280 rpm) handpiece with abuilt-in apex locator. It uses rotary nickel–titaniuminstruments held by a push-button chuck. The TriAuto-ZX has three automatic functions: The hand-piece automatically starts when the file enters the canaland stops when the file is removed. If too much pres-sure is applied, the handpiece automatically stops andreverses rotation. It also automatically stops andreverses rotation when the file tip reaches the apicalstop, as determined by the built-in apex locator. TheTri Auto-ZX works in a moist canal.
RECIPROCATING HANDPIECEA commonly used flat plane reciprocating hand-piece is the Giromatic (Medidenta/Micro Mega).It accepts only latch-type instruments. In thisdevice, the quarter-turn motion is delivered 3,000times per minute. Kerr has the M4 Safety Hand-piece (Sybron-Kerr, Orange, CA), which has a 30 �
reciprocating motion and a chuck that locks regularhand files in place by their handles (Figure 13). TheKerr Company recommends their Safety HedstromInstrument be used with the M4. Zakariasenet al.208,209 found the M4, mounted with SafetyHedstrom files, to be somewhat superior to ‘‘step-back
Figure 13 The M4 Safety Handpiece reciprocates in a 30� motion andlocks regular hand files in place. The manufacturer recommends thatSafety Hedstrom files be used. Courtesy of Sybron-Endo/Kerr.
Chapter 26 / Endodontics Instruments and Armamentarium / 833

hand preparations and a shorter time of preparation.’’Hulsman and Stryga210 found much the same for boththe M4 and the Giromatic.
The Endo-Gripper (Moyco/Union Broach) is asimilar handpiece, with a 10:1 gear ratio and a 45 �
turning motion. As with the Kerr M4, the Endo-Gripper also uses regular hand, not contra-angle,instruments. Union Broach recommends their Flex-R and Onyx-R files. In a comparison of nickel–titanium rotary engine-driven instruments with theEndo-Gripper and the Kerr M4, it was found thatthere were no significant differences among thegroups for the direction of transportation. The onenickel–titanium rotary instrument that did have sig-nificant transportation has subsequently been rede-signed.211
Giromatic handpiece instrumentation was noteffective when broaches were used. Hedstroem-typefiles and K-style reamers were more effective.212–214
Micro Mega recommends that Rispi Sonic or Triocutinstruments be used with the Giromatic handpiece.The reports are mixed, however, between ‘‘zipping’’ atthe apical foramen versus round, tapered prepara-tion.215–218
VERTICAL STROKE HANDPIECEThe vertical stroke handpiece is driven either by airor electrically that delivers a vertical stroke rangingfrom 0.3 to 1 mm. The more freely the instrumentmoves in the canal, the longer the stroke. The hand-piece also has a quarter-turn reciprocating motionthat ‘‘kicks in,’’ along with the vertical stroke, whenthe canal instrument starts to bind in a tight canal. Ifit is too tight, the motion ceases, and the operatorreturns to a smaller file. The Canal Finder System(Marseille, France) uses the A-file, a variation of theH-file.
Rotary Instruments
Two of the most historic and popular engine-driveninstruments are Gates Glidden drills and Peeso ream-ers (drills) (Figure 14, A and B). Gates Glidden drillsare an integral part of instrumentation techniques forboth initial opening of canal orifices and deeper pene-tration in both straight and curved canals. GatesGlidden drills are designed to have a weak spot inthe part of the shaft closest to the handpiece so that, ifthe instrument separates, the separated part can beeasily removed from the canal. They come in sizes1 through 6.
In a laboratory study, Luebke and Brantley219
tested two brands of Gates Glidden drills by clamp-ing the head of the drill and then twisting the han-dles either clockwise or counterclockwise. There wasno specific pattern to their fracture except that somebroke at the head and some high on the shaft nearthe shank. Luebke and Brantley220,221 later repeatedthe experiment, allowing the drill head to turn as itwould in a clinical situation. This time, all of thedrills fractured near the shank, ‘‘a major departurefrom the previous test.’’
The Peeso reamer (Dentsply/Maillefer) is mostoften used in preparing the coronal portion of theroot canal for a post and core. One must be careful touse the ‘‘safe-ended’’ Peeso drill to prevent lateralperforation. Gutta-percha should have previouslybeen removed to post depth with a hot plugger.
ULTRASONIC AND SONIC HANDPIECESInstruments used in the handpieces that move near orfaster than the speed of sound range from standard K-type files to special broach-like instruments. ‘‘Ultra-sonic endodontics is based on a system in whichsound as an energy source (at 20 to 25 kHg) activatesan endodontic file resulting in three-dimensional acti-vation of the file in the surrounding medium.’’222
‘‘The main debriding action of ultrasonics was initi-ally thought to be by cavitation, a process by which
A B
Figure 14 Engine-driven instruments used in a slow-speed handpiece.A, Gates Glidden drills come in sizes 1 through 6, end cutting or non–end cutting, and are used extensively in enlarging the straight part of thecanal. B, Peeso reamer (drill) used primarily for post preparation. Photoscourtesy of Dentsply/Maillefer.
834 / Endodontics

bubbles formed from the action of the file, becomeunstable, collapse, and cause a vacuum-like ‘implo-sion.’ A combined shock, shear and vacuum actionresults.’’222 Ultrasonic handpieces use K-files as acanal instrument. Before a size 15 file can fully func-tion, however, the canal must be enlarged with handinstruments to at least a size 20.
Although Richman223 in 1957 must be creditedwith the first use of ultrasonics in endodontics, Mar-tin and Cunningham224–232 were the first to develop adevice, test it, and see it marketed in 1976. Ultimatelynamed the Cavitron Endodontic System (no longermanufactured), it was followed on the market by theEnac unit (Osada Electric Co., Los Angeles, CA) andthe Piezon Master 400 (Electro Medical Systems, SA,Switzerland).
These instruments all deliver an irrigant/coolant,usually sodium hypochlorite, into the canal space whilecleaning and shaping are carried out by a vibrating K-file.The results achieved by the ultrasonic units have rangedfrom outstanding224–239 to disappointing.240–244 What isthe explanation for such a wide variance in results? Theanswer seems to lie in the extensive experimentation onultrasonic instruments carried out by Ahmad et al.245–247
They thoroughly studied the mechanisms involved andquestioned the role that cavitation and implosion play inthe cleansing process. It is believed that a different phy-sical phenomenon, ‘‘acoustic streaming,’’ is responsiblefor the debridement. They concluded that ‘‘transientcavitation does not play a role in canal cleaning with theCaviEndo unit; however, acoustic streaming does appearto be the main mechanism involved.’’245 They pointedout that acoustic streaming ‘‘depends on free displace-ment amplitude of the file’’ and that the vibrating file is‘‘dampened’’ in its action by the restraining walls of thecanal.
Ahmad et al.246 found that the smaller files gen-erated greater acoustic streaming and hence muchcleaner canals. After canals are fully prepared, bywhatever means, they recommended returning witha fully oscillating No. 15 file for 5 minutes with afree flow of 1% sodium hypochlorite. In anotherstudy, Ahmad et al.247 found that root canals hadto be enlarged to the size of a No. 40 file to permitenough clearance for the free vibration of the No.15 file at full amplitude. Others, including Martin,the developer, have recommended that the No. 15file be used exclusively.227,241 The efficacy of ultra-sonography to thoroughly debride canals followingstep-back preparation was demonstrated by Archeret al.248 There was a difference in cleanlinessbetween canals needle-irrigated during preparationand those canals prepared and followed by 3 min-
utes of ultrasonic instrumentation with a No. 15file and 5.25% sodium hypochlorite.
Walmsley and Williams249 reached similar conclu-sions about the oscillatory pattern of endosonic files.They pointed out that the greatest displacementamplitude occurs at the unconstrained tip and thatthe greatest restraint occurs when the instrument isnegotiating the apical third of a curved canal. This isthe damping effect noted by Ahmad et al.,245 the lackof freedom for the tip to move freely to either cut orcause acoustic streaming to cleanse. Krell et al.250
observed the same phenomenon that the irrigantcould not advance to the apex ‘‘until the file couldfreely vibrate.’’ Lumley and Walmsley251 reportedbetter results if K-files were precurved when used incurved canals.
Ahmad et al.252 noted another interesting phenom-enon about ultrasonic canal preparation—that, con-trary to earlier reports, ultrasonics alone actuallyincreased the viable counts of bacteria in simulatedroot canals. This was felt to be caused by the lack ofcavitation and the dispersal effects of the bacteria byacoustic streaming. On substitution of sodium hypo-chlorite (2.5%) for water, however, all of the bacteriawere killed, proving once again the importance ofusing an irrigating solution with bactericidal proper-ties.
Ahmad and Pitt Ford253 also compared two ultra-sonic units—CaviEndo versus Enac. They evaluatedcanal shape and elbow formation: ‘‘There was nosignificant difference . . . in the amount of apicalenlargement.’’ They did find, however, that the Enacunit had a greater propensity for producing‘‘elbows,’’ as well as apical deviation and change ofwidth. Ahmad254 suggested that ‘‘the manufacturersof ultrasonic units consider different file designs.’’She found the K-Flex to be more efficient than theregular K style.
ULTRASONIC CONCLUSIONSOne can draw the conclusion that ultrasonic endo-dontics has added to the practice of root canaltherapy. There is no question that canals are betterdebrided if ultrasonic oscillation with sodiumhypochlorite is used at the conclusion of cavitypreparation. But the files must be small and loosein the canal, particularly in curved canals, toachieve optimum cleansing.
SONIC HANDPIECESThe principal sonic endodontic handpiece availabletoday is the Micro Mega 1500 (or 1400) Sonic Air
Chapter 26 / Endodontics Instruments and Armamentarium / 835

Endo System (Medidenta International, Inc.;Wood-side, NY) (Figure 15). Like the air rotor handpiece,it attaches to the regular airline at a pressure of 0.4MPa. The air pressure may be varied with an adjus-table ring on the handpiece to give an oscillatoryrange of 1,500 to 3,000 cycles per second. Tap waterirrigant/coolant is delivered into the preparation fromthe handpiece.
Walmsley et al.255 studied the oscillatory patternof sonically powered files. They found that out in theair, the sonic file oscillated in a large ellipticalmotion at the tip. When loaded, as in a canal, theyfound that the oscillatory motion changed to a long-itudinal motion, up and down, ‘‘a particularly effi-cient form of vibration for the preparation of rootcanals.’’
The strength of the Micro Mega sonic handpiecelies in the special canal instruments used and theability to control the air pressure and hence theoscillatory pattern. The three choices of file thatare used with the Micro Mega 1500 are the RispiSonic, the Shaper Sonic, and the Trio Sonic (Med-identa International, Inc.) (Figure 16). The RispiSonic resembles the old rat-tail file. The ShaperSonic resembles a barbed broach. The Trio Sonicresembles a triple-helix Hedstroem file. All of theseinstruments have safe-ended noncutting tips.
The Rispi Sonic has 8 cutting blades and the ShaperSonic has 16. The ISO sizes range from 15 to 40.
Because graduated-size instruments have varying shaftsizes, the instrument must be tuned with the unit’stuning ring to optimum tip amplitude of 0.5 mm. Aswith the ultrasonic canal preparation, these instru-ments must be free to oscillate in the canal, to raspaway at the walls, and to remove necrotic debris andpulp remnants. To accommodate the smallest instru-ment, a size 15, the canal must be enlarged to theworking length with hand instruments through sizeNo. 20. The sonic instruments, with the 1.5 to 2.0 mmsafe tips, begin their rasping action this far removedfrom the apical stop. This is known as the ‘‘soniclength.’’ As the instrument becomes loose in the canal,the next-size instrument is used, and then the nextsize, which develops a flaring preparation. The sonicinstruments are primarily for step-down enlarging,not penetration.
Three commonly held objectives of shaping theroot canal are (1) developing a continuous tapering
Figure 15 Micro Mega 1500 Sonic Air handpiece. Activated by pressurefrom the turbine air supply, the Micro Mega 1500 can be mounted withspecial instruments easily adjusted to the length of the tooth. Waterspray serves as an irrigant. Photo courtesy of Medidenta/Micro Mega.
A B C
Figure 16 Three instruments used with the Micro Mega 1500 Sonic Airhandpiece. A, Rispi Sonic. B, Shaper Sonic. C, Trio Sonic (aka Heliosonicor Triocut). Courtesy of Medidenta/Micro Mega.
836 / Endodontics

conical form, (2) making the canal narrow apicallywith the narrowest cross-sectional diameter at itsterminus, and (3) leaving the apical foramen in itsoriginal position spatially. To satisfy these require-ments, two of the sonic instruments have beenquite successful. Dummer et al.256 found the RispiSonic and Shaper Sonic files to be the most suc-cessful, the Trio Sonic less so. ‘‘In general, theShaper Sonic files widened the canals more effec-tively than the Rispi Sonic files, whilst theHeliosonic [Trio Sonic] files were particularly inef-fective . . . .’’256
Bolanos et al.257 found essentially the same results.They recommended that the Shaper Sonic files be usedfirst and that the remaining two-thirds of the canal befinished with the Rispi Sonic. Ehrlich et al.258 com-pared canal apical transport using Rispi Sonic and TrioSonic files versus hand instrumentation with K-files.They found no difference in zipping among the threeinstruments. Tronstad and Niemczyk259 also tested theRispi and Shaper files against other instruments. Theyreported no complications (broken instruments, per-forations, etc.) with either of the Sonic instruments.Miserendino et al.260 also found that the ‘‘Micro Megasonic vibratory systems using Rispi Sonic and Shaperfiles were significantly more efficient than the othersystems tested.’’
COMPARISONS IN EFFICACY AND SAFETYOF AUTOMATED CANAL PREPARATIONDEVICESBefore making an investment in an automated endo-dontic device, one should know the comparativevalues of the different systems and their instruments.Unfortunately, the ultimate device and instrumenthas not been produced and tested as yet. Some arebetter in cutting efficiency, some in following narrowcurved canals, some in producing smooth canals,and some in irrigating and removing smear layer,but apparently none in mechanically reducing bac-terial content.
As stated above, Miserendino et al.260 found that thecutting varied considerably. They ranked the Rispi Sonicfile at the top, followed by the Shaper Sonic, the Enac‘‘U’’ file (Osada Electric Co.), and the CaviEndo K-file.
Tronstad and Niemczyk’s259 comparative studyfavored the Canal Finder System in narrow, curvedcanals. On the other hand, the Rispi and Shaper files inthe Micro Mega Sonic handpiece proved the mostefficacious ‘‘in all types of root canals.’’ The CavitronEndo System was slow, blocked and ledged canals, andfractured three files in severely curved canals. They
also found the Giromatic with Rispi files to be effectivein wide straight canals, less so in curved canals, wherefour Rispi files fractured.
Bolanos et al.257 also tested the Giromatic withRispi files against the Micro Mega Sonic handpiecewith Rispi and Shaper files. They found the RispiSonic best in straight canals, the Shaper Sonic bestin curved canals, and both better than the Giromatic/Rispi and/or hand instrumentation with K-Flex files.The Shaper files left the least debris and the Giro-matic/Rispi left ‘‘an extensive amount of debris.’’
Kielt and Montgomery261 also tested the MicroMega Sonic unit with Trio Sonic files against theultrasonic Cavitron Endo and Enac units with K-files.Even though others found the Trio Sonic files lesseffective (than the Rispi or Shaper files), Kielt andMontgomery261 concluded that ‘‘overall the Medi-denta unit was superior to the other endosonicsystems and to the hand technique (control).’’ Zakar-iasen et al.262 reported success in combining handinstrumentation with sonic enlargements using theMicro Mega 1500.
Walker and del Rio263 also compared the efficacyof the Cavitron Endo and Enac ultrasonic unitsagainst the Micro Mega Sonic unit and found ‘‘nostatistically significant difference among the groups,however, liquid extruded from the apical foramen in84% of their test teeth.’’ They felt that ‘‘sodiumhypochlorite may improve the debridement of thecanal.’’
Yahya and El Deeb264 tested ultrasonic units againstsonic units. The researchers found the Micro MegaSonic to be the fastest in preparation time and causedthe ‘‘least amount of straightening of the canals.’’ Onthe other hand, Reynolds et al.265 found hand pre-paration with the step-back technique superior tosonic and ultrasonic preparation except in the impor-tant apical area, where they were similar. Lumleyet al.266 found that ultrasonic and sonic files bestcleaned ovoid canals.
Lev et al.267 prepared the cleanest canals using thestep-back technique followed by 3-minute use of aCaviEndo ultrasonic file with sodium hypochlorite.
Stamos et al.268 also compared cleanliness followingultrasonic debridement with sodium hypochlorite ortap water. Using water alone, the Enac system wasmore effective, but when sodium hypochlorite wasused, the CaviEndo unit (which has a built-in tank)was superior. They also reported ultrasonic prepara-tion to be ‘‘significantly faster’’ than hand instrumen-tation.
Goldman et al.269 tested sonic versus ultrasonicunits and concluded that they were all effective in
Chapter 26 / Endodontics Instruments and Armamentarium / 837

canal preparation but judged the Micro Mega SonicAir System, using Rispi and Shaper Sonic files, ‘‘as thebest system tested.’’
Pugh et al.270 compared four techniques accordingto the amount of debris extruded from the apex. Thesonic technique extruded the least and hand instru-mentation the most debris. Ultrasonic was halfwaybetween. Whether the debris discharged into the api-cal tissue contains bacteria was of the utmost impor-tance. Using sterile saline as an irrigant, Barnettet al.271 found sodium hypochlorite to be four timesmore effective than sterile saline. Fairbourn et al.272
found essentially the same thing.
COMPARATIVE CONCLUSIONOF AUTOMATED DEVICESIt appears safe to say that no one automated device willanswer all needs in canal cleaning and shaping. Handinstrumentation is essential to prepare and cleanse theapical canal, no matter which device, sonic or ultra-sonic, is used. Recent research has confirmed theprevious findings. Sonic or ultrasonic instrumentation
is significantly better than hand instrumentation of thecanal system as far as producing a cleaner canalsystem.273–275 In one study, Lee et al.276 confirmed thatultrasonic instruments perform better in a larger canalspace. In a similar study by van der Sluis et al.,277 it wasfound that there was a tendency for ultrasonic irriga-tion to produce a cleaner canal system in a larger canal,but the differences were not significant. Another studyby Lee et al.278 demonstrated that the volume of irri-gant is also essential in ridding the canal system ofdentinal debris.
References
1. Ingle JI. A standardized endodontic technique using newlydesigned instruments and filling materials. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1961;14:83–91.
2. Ingle JI, LeVine M. The need for uniformity of endodonticinstruments, equipment and filling materials. In: Transac-tions of the 2nd international conference of endodontics.Philadelphia: Univ. of Pennsylvania Press; 1958. pp. 123–43.
3. American Dental Association Council on Dental Materials,Instruments and Equipment. Revised ANSI/ADA specificationno. 28 for root canal files and reamers, type-K, type-K for handuse. Chicago: American Dental Association Press; 2002.
4. Kerekes K. Evaluation of standardized root canal instru-ments and obturating points. J Endod 1979;5:145–50.
5. Serene TP, Loadholt C. Variations in same-size endodonticfiles. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1984;57:200–2.
6. Cormier CJ, von Fraunhofer JA, Chamberlain JH. A com-parison of endodontic file quality and file dimensions.J Endod 1988;14:138–42.
7. Seto BG, Nicholls JI, Harrington GW. Torsional properties oftwisted and machined endodontic files. J Endod 1990;16:355–60.
8. Keate KC, Wong M. A comparison of endodontic file tipquality. J Endod 1990;16:486–91.
9. Stenman E, Spangberg L. Machining efficiency of endodonticK-files and Hedstroem files. J Endod 1990;16:375–82.
10. Stenman E, Spangberg L. Root canal instruments are poorlystandardized. J Endod 1993;19:327–34.
11. Canalda-Sahli C, Brau-Aguade E, Berastegui-Jimeno E. Acomparison of bending and torsional properties of K-filesmanufactured with different metallic alloys. Int EndodJ 1996;29:185–9.
12. Tepel A, Schafer E, Hoppe W. Properties of endodontichand instruments used in rotary motion. Part 3: resistanceto bending and fracture. J Endod 1997;23:141–5.
13. Wolcott J, Himel VT. Torsional properties of nickel-titaniumversus stainless steel endodontic files. J Endod997;23:217–20.
Table 1 Dimensions in Millimeters (Revision of ADASpecification No. 28 Added Instrument Sizes 08 and110–150 to the Original Specification Diameter [Tolerance± 0.02 mm])
Handle Size D1 mm D2 mm D3 mmColorCode
08 0.08 0.40 0.14 Gray
10 0.10 0.42 0.16 Purple
15 0.15 0.47 0.21 White
20 0.20 0.52 0.26 Yellow
25 0.25 0.57 0.31 Red
30 0.30 0.62 0.36 Blue
35 0.35 0.67 0.41 Green
40 0.40 0.72 0.46 Black
45 0.45 0.77 0.51 White
50 0.50 0.82 0.56 Yellow
55 0.55 0.87 0.61 Red
60 0.60 0.92 0.66 Blue
70 0.70 1.02 0.76 Green
80 0.80 1.12 0.86 Black
90 0.90 1.22 0.96 White
100 1.00 1.32 1.06 Yellow
110 1.10 1.42 1.16 Red
120 1.20 1.52 1.26 Blue
130 1.30 1.62 1.36 Green
140 1.40 1.72 1.46 Black
150 1.50 1.82 1.56 White
New diameter measurement point (D3) was added 3 mm from the tip of the
cutting end of the instrument. Handle color coding is official. From Ingle and
Bakland, Endodontics, 5th ed., 2002, Table 10-1, Ingle, JI et al, Endodontic
cavity preparation.
838 / Endodontics

14. Mitchell BF, James GA, Nelson RC. The effect of autoclavesterilization on endodontic files. Oral Surg Oral Med OralPathol Oral Radiol Endod 1983;55:204–7.
15. Mize SB, Clement DJ, Pruett JP, Carnes DL. Effect of ster-ilization on cyclic fatigue of rotary nickel-titanium endo-dontic instruments. J Endod 1998;24:843–7.
16. Schafer E. Relationship between design features of endodon-tic instruments and their properties. Part 2. Instrumentationof curved canals. J Endod 1999;25:56–9.
17. Roth WC, Gough RW, Grandich RA, Walker WA. A studyof the strength of endodontic files. J Endod 1983;9:228–32.
18. Oliet S, Sorin SM. Cutting efficiency of endodontic reamers.Oral Surg Oral Med Oral Pathol Oral Radiol Endod1973;36:243–52.
19. Webber J, Moser JB, Heuer MA. A method to determine thecutting efficiency of root canal instruments in linear motion.J Endod 1980;6:829–34.
20. Kazemi RB, Stenman E, Spangberg LSW. The endodonticfile is a disposable instrument. J Endod 1995;21:451–5.
21. Filho IB, Esberard M, Leonardo RD, del Rio CE. Micro-scopic evaluation of three endodontic files, pre- and post-instrumentation. J Endod 1998;24:461–4.
22. Newman JG, Brantley WA, Gerstein H. A study of thecutting efficiency of seven brands of endodontic files inlinear motion. J Endod 1983;9:316–22.
23. Neal RG, Craig RG, Powers JM. Cutting ability of K-typeendodontic files. J Endod 1983;9:52–7.
24. Schafer E, Lau R. Comparison of cutting efficiency andinstrumentation of curved canals with nickel-titanium andstainless-steel instruments. J Endod 1999;25:427–30.
25. Haikel Y, Serfaty R, Wilson P, et al. Cutting efficiency ofnickel-titanium endodontic instruments and the effect ofsodium hypochlorite treatment. J Endod 1998;24:736–9.
26. Schafer E. Relationship between design features of endodon-tic instruments and their properties. Part 1. Cutting effi-ciency. J Endod 1999;25:52–5.
27. Dearing GJ, Kazemi RB, Stevens RH. An objective evaluationcomparing the physical properties of two brands of stainless steelendodontic hand files. J Endod 2005;31:827–30.
28. Dearing GJ, Kazemi RB, Stevens RH. A comparison of themachining efficiency of two brands of stainless steel endo-dontic hand files. J Endod 2005;31:873–6.
29. Luks S. An analysis of root canal instruments. J Am DentAssoc 1959;58:85–92.
30. Gutierrez JH, Gigoux C, Sanhueza I. Physical and chemicaldeterioration of endodontic reamers during mechanical pre-paration. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1969;28:394–403.
31. Lentine FN. A study of torsional and angular deflection ofendodontic files and reamers. J Endod 1979;5:181–91.
32. Chernick LB, Jacobs JJ, Lautenschlauger EP, Heuer MA. Tor-sional failures of endodontic files. J Endod 1976;2:94–7.
33. Lautenschlager EP, Jacobs JJ, Marshall GW, Heuer MA.Brittle and ductile torsional failures of endodontic instru-ments. J Endod 1977;3:175–8.
34. Roane JB, Sabala C. Clockwise or counterclockwise. J Endod1984;10:349–53.
35. Sotokawa T. An analysis of clinical breakage of root canalinstruments. J Endod 1988;14:75–82.
36. Haikel Y, Gasser P, Allemann C. Dynamic fracture of hybridendodontic hand instruments compared with traditionalfiles. J Endod 1991;17:217–20.
37. Schafer E, Tepel J. Relationship between design features ofendodontic instruments and their properties. Part 3. Resistanceto bending and fracture. J Endod 2001;27:299–303.
38. Rowan MB, Nicholls JI, Steiner J. Torsional properties ofstainless steel and nickel-titanium endodontic files. J Endod1996;22:341–5.
39. Walia H, Brantley WA, Gerstein H. An initial investigationof the bending and torsional properties of Nitinol root canalfiles. J Endod 1988;14:346–51.
40. Villalobos RL, Moser JB, Heuer MA. A method to determinethe cutting efficiency of root canal instruments in rotarymotion. J Endod 1980;6:667–71.
41. Felt RA, Moser JB, Heuer MA. Flute design of endodonticinstruments: Its influence on cutting efficiency. J Endod1982;8:253–9.
42. Miserendino LJ, Moser JB, Heuer MA, Osetek EM. Cuttingefficiency of endodontic instruments. Part 2: analysis of tipdesign. J Endod 1986;12:8–12.
43. Miserendino LJ, Moser JB, Heuer MA, Osetek EM. Cuttingefficiency of endodontic instruments. Part 1: a quantitative com-parison of the tip and fluted regions. J Endod 1985;11:435–41.
44. Powell SE, Simon JHS, Maze BB. A comparison of the effectof modified and nonmodified instrument tips on apicalconfiguration. J Endod 1986;12:293–300.
45. Powell SE, Wong PD, Simon JHS. A comparison of the effectof modified and nonmodified tips on apical canal config-uration. Part II. J Endod 1988;14:224–8.
46. Sabala CL, Roane JB, Southard LZ. Instrumentation ofcurved canals using a modified tipped instrument: a com-parison study. J Endod 1988;14:59–64.
47. Dummer PMH, Al-Omari MAO, Bryant S. Comparison ofthe performance of four files with rounded tips during shap-ing of simulated root canals. J Endod 1998;24:364–71.
48. Zinelis S, Margelos J. Failure mechanism of hedstroemendodontic files in vivo. J Endod 2002;28:471–3.
49. Kosti E, Zinelis S, Lambrianidis T, Margelos J. A compara-tive study of crack development in stainless-steel Hedstromfiles used with step-back or crown-down techniques.J Endod 2004;30:38–41.
Chapter 26 / Endodontics Instruments and Armamentarium / 839

50. Kazemi R, Stenman E, Spangberg L. A comparisonof stainless steel and nickel-titanium H-type instruments ofidentical design: Torsional and bending tests. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2000;90:500–6.
51. Machian GR, Peters DD, Lorton L. The comparative effi-ciency of four types of endodontic instruments. J Endod1982;8:398–402.
52. Mizrahi SJ, Tucker JW, Seltzer S. A scanning electron micro-scopic study of the efficacy of various endodontic instru-ments. J Endod 1975;1:324–33.
53. Miserendino LJ, Brantley WA, Walia HD, Gerstein H. Cuttingefficiency of endodontic hand instruments. Part 4. Compar-ison of hybrid and traditional designs. J Endod 1988;14:451–4.
54. Yguel-Henry S, Vannesson H, von Stebut J. High precision,simulated cutting efficiency measurement of endodonticroot canal instruments: influence of file configuration andlubrication. J Endod 1990;16:418–22.
55. El Deeb ME, Boraas JC. The effect of different files on thepreparation shape of curved canals. Int Endod J 1985;18:1–7.
56. American National Standards Institute/ADA specificationno. 58 for root canal files, Type H (Hedstroem). J Am DentAssoc 1989;118:239–40.
57. Stenman E, Spangberg LSW. Machining efficiency of Flex-R,K-Flex, Trio-Cut and S-Files. J Endod 1990;16:575–9.
58. Wildey WL, Senia S. A new root canal instrument andinstrumentation technique: a preliminary report. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1989;67:198–207.
59. Leseberg DA, Montgomery S. The effects of Canal Master,Flex-R, and K-Flex instrumentation on root canal config-uration. J Endod 1991;17:59–65.
60. Wildey WL, Senia ES, Montgomery S. Another look at rootcanal instrumentation. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1992;74:499–507.
61. Baumgartner JC, Martin H, Sabala CC, et al. Histomorpho-metric comparison of canals prepared by four techniques.J Endod 1992;18:530–4.
62. Briseno BM, Kremers L, Hamm G, Nitsch C. Comparison bymeans of a computer-supported device of the enlargingcharacteristics of two different instruments. J Endod1993;19:281–7.
63. Cirnis GJ, Boyer TJ, Pelleu GB. Effect of three file types onthe apical preparations of moderately curved canals. J Endod1988;14:441–4.
64. Sepic AO, Pantera EA, Neaverth EJ, Anderson RW. A com-parison of Flex-R files and K-type files for enlargement ofseverely curved molar root canals. J Endod 1989;15:240–5.
65. Calhoun G, Montgomery S. The effects of fourinstrumentation techniques on root canal shape. J Endod1988;14:273–7.
66. Alodeh MHA, Dummer PMH. The comparison of the abilityof K-files and Hedstroem files to shape simulated root canalsin resin blocks. Int Endod J 1989;22:226–35.
67. Briseno BM, Sonnabend E. The influence of different rootcanal instruments on root canal preparation: an in vitrostudy. Int Endod J 1991;24:15–23.
68. Stenman E, Spangberg LSW. Machining efficiency of endo-dontic files: a new methodology. J Endod 1990;16:151–7.
69. Rueggenberg FA, Powers JM. Mechanical properties ofendodontic broaches and effects of bead sterilization.J Endod 1988;14:133–7.
70. Civjan S, Huget EF, DeSimon LB. Potential applications ofcertain nickel-titanium (nitinol) alloys. J Dent Res1975;54:89–96.
71. Stoeckel D, Yu W. Superelastic Ni-Ti wire. Wire J Int 1991March: 45–50.
72. Thompson SA. An overview of nickel-titanium alloys used indentistry. Int Endo J 2000;33:297–310.
73. Kazemi RB, Stenman E, Spangberg LSW. Machining effi-ciency and wear resistance of nickel-titanium endodonticfiles. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1996;81:596–602.
74. Serene TP, Adams JD, Saxena A. Physical tests, in nickel-titanium instruments: application in endodontics. St. Louis:Ishiyaku EuroAmerica; 1995.
75. Hsich M, Yu F. The basic research on NiTi shape-memoryalloy-anti-corrosive test and corrosive test and histologicalobservation. Chin Med J 1982;1:105–20.
76. Canalda-Sahli C, Brau-Aguade E, Berastequi-Jimeno E. Acomparison of bending and torsional properties of K filesmanufactured with different metallic alloys. Int EndodJ 1996;29:185–9.
77. Canalda-Sahli C, Brau-Aguade E, Berastegui-Jimeno E. Tor-sional and bending properties of stainless steel and nickel-titanium CanalMaster U and Flexogate instruments. EndodDent Traumatol 1996;12:141–5.
78. Pruett JP, Clement DJ, Carnes DL. Cyclic fatigue testingof nickel-titanium endodontic instruments. J Endod1997;23:77–85.
79. Himel VT, Ahmed KM, Wood DM, Alhadainy HA. Anevaluation of Nitinol and stainless steel files used by dentalstudents in a laboratory proficiency exam. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1995;79:232–7.
80. Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless steel hand file instrumentation usingcomputed tomography. J Endod 1996;22:369–75.
81. Tepel J, Schafer E, Hoope W. Properties of endodontic handinstrumentation used in rotary motion. Part 1. Cuttingefficiency. J Endod 1995;21:418–21.
82. Elliot LM, Curtis RV, Pitt Ford TR. Cutting pattern of nickeltitanium files using two preparation techniques. Endod DentTraumatol 1998;14:10–15.
83. Kuhn G, Tavernier B, Jordan L. Influence of structure onnickel-titanium endodontic instruments failure. J Endod2001;27:516–20.
840 / Endodontics

84. Kuhn G, Jordan L. Fatigue and mechanical propertiesof nickel-titanium endodontic instruments. J Endod2002;28:716–20.
85. Kim JW, Griggs JA, Regan JD, et al. Effect of cryogenictreatment on nickel-titanium endodontic instruments. IntEndo J 2005;38:364–71.
86. Brantley WA, Svec TA, Iijima M, et al. Differential ScanningCalorimetric studies of nickel-titanium rotary endodonticinstruments after simulated clinical use. J Endod2002;28:774–8.
87. Bahia MGA, Martins RC, Gonzalez BM, Buono VTL. Phy-sical and mechanical characterization and the influence ofcyclic loading on the behavior of nickel-titanium wiresemployed in the manufacture of rotary endodontic instru-ments. Int Endo J 2005;38:795–801.
88. Miyai K, Ebihara A, Hayashi Y, et al. Influence of phasetransformation on the torsional and bending properties ofnickel-titanium rotary endodontic instruments. Int EndoJ 2006;39:119–26.
89. Turpin Y, Chagneau F, Vulcain J. Impact of two theoreticalcross-sections ontorsional and bending stresses of nickel-tita-nium root canal instrument models. J Endod 2000;26:414–17.
90. Turpin YL, Chagneau F, Bartier O, et al. Impact of torsionaland bending inertia on root canal instruments. J Endod2001;27:333–6.
91. Berutti E, Chiandussi G, Gaviglio I, Ibba A. Comparativeanalysis of torsional and bending stresses in twomathematical models of nickel-titanium rotary instruments:ProTaper versus ProFile. J Endod 2003;29:15–19.
92. Xu X, Eng M, Zheng Y, Eng D. Comparative study oftorsional and bending properties for six models ofnickel-titanium root canal instruments with different cross-sections. J Endod 2006;32:372–5.
93. Yared GM, Bou Dagher FE, Machtou P. Cyclic fatigue ofProFile rotary instruments after clinical use. Int EndoJ 2000;33:204–7.
94. Gambarini G. Cyclic fatigue of ProFile rotary instrumentsafter prolonged clinical use. Int Endo J 2001;34:386–9.
95. Gambarini G. Cyclic fatigue of nickel-titanium rotary instru-ments after clinical use with low- and high-torque endodon-tic motors. J Endod 2001;27:772–4.
96. Bahia MGA, Buono VTL. Decrease in the fatigue resistanceof nickel-titanium rotary instruments after clinical use incurved canals. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2005;100:249–55.
97. Bahia MGA, Melo MCC, Buono VTL. Influence of simulatedclinical use on the torsional behavior of nickel-titaniumrotary endodontic instruments. Oral Surg Oral Med OralPathol Oral Radiol Endod 2006;101:675–80.
98. de Melo MCC, Bahia MGA, Buono VTL. Fatigue resistanceof engine-driven rotary nickel-titanium endodontic instru-ments. J Endod 2002;28:765–9.
99. Booth JR, Scheetz JP, Lemons JE, Eleazer PD. A comparisonof torque required to fracture three different nickel-titaniumrotary instruments around curves of the same angle butof different radius when bound at the tip. J Endod2003;29:55–7.
100. Yared G, Kulkarni K. An in vitro study of the torsionalproperties of new and used rotary nickel-titanium files inplastic blocks. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2003;96:466–71.
101. Ullmann CJ, Peters OA. Effect of cyclic fatigue on staticfracture loads in ProTaper nickel-titanium rotary instru-ments. J Endod 2005;31:183–6.
102. Li U-M, Lee B-S, Shih C-T, et al. Cyclic fatigue of endodon-tic nickel titanium rotary instruments: Static and dynamictests. J Endod 2002;28:448–51.
103. Best S, Watson P, Pillier R, et al. Torsional fatigue andendurance limit of a size 30.06 ProFile rotary instrument.Int Endo J 2004;37:370–3.
104. Peters OA, Kappeler S, Bucher W, Barbakow F. Engine-drivenpreparation of curved root canals: Measuring cyclic fatigueand other physical parameters. Aust Endo J 2002;28:11–17.
105. Guilford WL, Lemons JE, Eleazer PD. A comparison oftorque required to fracture rotary files with tips bound insimulated curved canal. J Endod 2005;31:468–70.
106. Yao JH, Schwartz SA, Beeson TJ. Cyclic fatigue of three typesof rotary nickel-titanium files in a dynamic model. J Endod2006;32:55–7.
107. Luebke NH, Brantley WA, Alapati SB, et al. Bending fatiguestudy of nickel-titanium Gates Glidden drills. J Endod2005;31:523–5.
108. Schafer E, Dzepina A, Danesh G. Bending properties ofrotary nickel-titanium instruments. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2003;96:757–63.
109. Blum JY, Cohen A, Machtou P, Micallef JP. Analysis offorces developed during mechanical preparation of extractedteeth using Profile NiTi rotary instruments. Int EndoJ 1999;32:32–46.
110. Blum J, Machtou P, Micallef J. Location of contact areas onrotary profile instruments in relationship to the forces devel-oped during mechanical preparation on extracted teeth. IntEndo J 1999;32:108–14.
111. Blum J-Y, Machtou P, Ruddle C, Micallef JP. Analysis ofmechanical preparations in extracted teeth using ProTaperrotary instruments: Value of the Safety Quotient. J Endod2003;29:567–75.
112. Sattapan B, Palamara J, Messer H. Torque during canalinstrumentation using rotary nickel-titanium files. J Endod2000;26:156–60.
113. Peters OA, Peters CI, Schonenberger K, Barbakow F. ProTa-per rotary root canal preparation: assessment of torque andforce in relation to canal anatomy. Int Endo J 2003;36:93–9.
Chapter 26 / Endodontics Instruments and Armamentarium / 841

114. da Silva FM, Kobayashi C, Suda H. Analysis of forces devel-oped during mechanical preparation of extracted teeth usingRaCe rotary instruments and ProFiles. Int EndoJ 2005;381:17–21.
115. Schrader C, Peters OA. Analysis of torque and force withdifferently tapered rotary endodontic instruments in vitro.J Endod 2005;31:120–3.
116. Mayhew J, Eleazer P, Hnat W. Stress analysis of humantooth root using various root canal instruments. J Endod2000;26:523–4.
117. Diemer F, Calas P. Effect of pitch length on the behavior ofrotary triple helix root canal instruments. J Endod2004;30:716–18.
118. Peters OA, Boessler C, Zehnder M. Effect of liquid andpaste-type lubricants on torque values during simulatedrotary root canal instrumentation. Int Endo J 2005;38:223–9.
119. Arens FC, Hoen MM, Steiman HR, Dietz GC. Evaluation ofsingle-use rotary nickel-titanium instruments. J Endod2003;29:664–6.
120. Knowles KI, Hammond NB, Biggs SG, Ibarrola JL. Incidenceof instrument separation using LightSpeed rotary instru-ments. J Endod 2006;32:14–16.
121. Di Fiore PM, Genov KI, Komaroff E, et al. Fracture ofProFile nickel-titanium rotary instruments: a laboratorysimulation assessment. Int Endo J 2006;39:502–9.
122. Shen Y, Cheung GSP, Bian Z, Peng B. Comparison of defectsin ProFile and ProTaper systems after clinical use. J Endod2006;32:61–5.
123. Parashos P, Gordon I, Messer HH. Factors influencingdefects of rotary nickel-titanium endodontic instrumentsafter clinical use. J Endod 2004;30:722–5.
124. Gabel W, Hoen M, Steiman R, et al. Effect of rotational speedon nickel-titanium file distortion. J Endod 1999;25:752–4.
125. Dietz D, Di Fiore P, Bahcall J, Lautenschlager E. Effect ofrotational speed on the breakage of nickel-titanium rotaryfiles. J Endod 2000;26:68–71.
126. Daugherty DW, Gound TG, Comer TL. Comparison offracture rate, deformation rate, and efficiency between rotaryendodontic instruments driven at 150 rpm and 350 rpm.J Endod 2001;27:93–5.
127. Tygesen YA, Steiman HR, Ciavarro C. Comparison of dis-tortion and separation utilizing Profile and Pow-R nickel-titanium rotary files. J Endod 2001;27:762–4.
128. Zelada G, Varela P, Martin B, et al. The effect of rotationalspeed and the curvature of root canals on the breakage ofrotary endodontic instruments. J Endod 2002;28:540–2.
129. Martin B, Zelada G, Varela P, et al. Factors influencingthe fracture of nickel-titanium rotary instruments. Int EndoJ 2003;36:262–6.
130. Yared GM, Bou Dagher FE, Machtou P. Influence of rota-tional speed, torque and operator’s proficiency on ProFilefailures. Int Endo J 2001;34:47–53.
131. Yared GM, Bou Dagher FE, Machtou P. Failure of ProFileinstruments used with high and low torque motors. IntEndo J 2001;34:471–5.
132. Yared G, Sleiman P. Failure of ProFile instruments used withair, high torque control, and low torque control motors.Oral Surg Oral Med Oral Pathol Oral Radiol Endod2002;93:92–6.
133. Yared G, Bou Dagher F, Kulkarni K. Influence of torquecontrol motors and the operator’s proficiency on ProTaperfailures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2003;96:229–33.
134. Bortnick KL, Steiman HR, Ruskin A. Comparison ofnickel-titanium file distortion using electric and air-drivenhandpieces. J Endod 2001;27:57–9.
135. Eggert C, Peters O, Barbakow F. Wear of nickel-titaniumLightspeed instruments evaluated by scanning electronmicroscopy. J Endod 1999;25:494–7.
136. Tripi TR, Bonaccorso A, Tripi V, et al. Defects in GT rotaryinstruments after use: An SEM study. J Endod 2001;27:782–5.
137. Peng B, Shen Y, Cheung GSP, Xia TJ. Defects in ProTaper S1instruments after clinical use: longitudinal examination. IntEndo J 2005;38:550–7.
138. Rapisarda E, Bonaccorso A, Tripi T, et al. The effect ofsurface treatments of nickel-titanium files on wear and cut-ting efficiency. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2000;89:363–8.
139. Rapisarda E, Bonaccorso A, Tripi TR, et al. Wear of nickel-titanium endodontic instruments evaluated by scanningelectron microscopy: Effect of ion implantation. J Endod2001;27:588–92.
140. Tripi TR, Bonaccorso A, Rapisarda E, et al. Depositions ofnitrogen on NiTi instruments. J Endod 2002;28:497–500.
141. Schafer E. Effect of physical vapor deposition on cuttingefficiency of nickel-titanium files. J Endod 2002;28:800–2.
142. Tripi TR, Bonaccorso A, Condorelli GG. Fabrication of hardcoatings on NiTi instruments. J Endod 2003;29:132–4.
143. Haikel Y, Serfaty R, Wilson P, et al. Mechanical properties ofnickel-titanium endodontic instruments and the effect ofsodium hypochlorite treatment. J Endod 1998;24:731–5.
144. Stokes OW, Di Fiore PM, Barss JT, et al. Corrosion in stain-less-steel and nickel-titanium files. J Endod 1999;25:17–20.
145. Darabara M, Bourithis L, Zinelis S, Papadimitriou GD.Susceptibility to localized corrosion of stainless steel andNiTi endodontic instruments in irrigating solutions. IntEndo J 2004;37:705–10.
146. Hilt B, Cunningham C, Shen C, Richards N. Torsionalproperties of stainless-steel and nickel-titanium files aftermultiple autoclave sterilizations. J Endod 2000;26:76–80.
147. Bertrand M, Pizzardini P, Muller M, et al. The removalof the smear layer using the Quantec system. A studyusing the scanning electron microscope. Int Endo J1999;32:217–24.
842 / Endodontics

148. Kum K-Y, Kazemi RB, Cha BY, Zhu Q. Smear layer produc-tion of K3 and ProFile Ni-Ti rotary instruments in curvedroot canals: A comparative SEM study. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2006;101:536–41.
149. Paque F, Musch U, Hulsmann M. Comparison of root canalpreparation using RaCe and ProTaper rotary Ni-Ti instru-ments. Int Endo J 2005;38:8–16.
150. Jodway B, Hulsmann M. A comparative study of root canalpreparation with NiTi-TEE and K3 rotary Ni-Ti instru-ments. Int Endo J 2006;39:71–80.
151. Schafer E, Erler M, Dammaschke T. Comparative study onthe shaping ability and cleaning efficiency of rotary Mtwoinstruments. Part 2. Cleaning effectiveness and shaping abil-ity in severely curved root canals of extracted teeth. Int EndoJ 2006;39:203–12.
152. Lumley PJ. Cleaning efficacy of two apical preparation regi-mens following shaping with hand files of greater taper. IntEndo J 2000;33:262–5.
153. Usman N, Baumgartner JC, Marshall JG. Influence of instru-ment size on root canal debridement. J Endod 2004;30:110–12.
154. Ahlquist M, Henningsson O, Hultenby K, Ohlin J. Theeffectiveness of manual and rotary techniques in the cleaningof root canals: a scanning electron microscope study. IntEndo J 2001;34:533–7.
155. Barbizam JVB, Fariniuk LF, Marchesan MA, et al. Effective-ness of manual and rotary instrumentation techniques forcleaning flattened root canals. J Endo 2002;28:365–6.
156. Schafer E, Schlingemann R. Efficiency of rotarynickel-titanium K3 instruments compared with stainlesssteel hand K-Flexofile. Part 2. Cleaning effectiveness andshaping ability in severely curved root canals of extractedteeth. Int Endo J 2003;36:208–17.
157. Iqbal MK, Karabucak B, Brown M, Menegazzo E. Effect ofmodified Hedstrom files on instrumentation area producedby ProFile instruments in oval canals. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2004;98:493–8.
158. Schafer E, Zapke K. A comparative scanning electron micro-scopic investigation of the efficacy of manual and automatedinstrumentation of root canals. J Endod 2000;26:660–4.
159. Jeon I-S, Spangberg LSW, Yoon T-C, et al. Smear layerproduction by 3 rotary reamers with different cutting bladedesigns in straight root canals: A scanning electron micro-scope study. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2003;96:601–7.
160. Zmener O, Pameijer CH, Banegas G. Effectiveness in clean-ing oval-shaped root canals using Anatomic EndodonticTechnology, ProFile and manual instrumentation: a scan-ning electron microscope study. Int Endo J 2005;38:356–63.
161. Gambarini G. Shaping and cleaning the root canal system: ascanning electron microscopic evaluation of a new instru-mentation and irrigation technique. J Endod 1999;25:800–3.
162. Peters O, Barbakow F. Effects of irrigation on debris and smearlayer on canal walls prepared by two rotary techniques: ascanning electron microscopic study. J Endod 2000;26:6–10.
163. Schafer E, Vlassis M. Comparative investigation oftwo rotary nickel-titanium instruments: ProTaper versusRaCe. Part 2. Cleaning effectiveness and shaping ability inseverely curved root canals of extracted teeth. Int EndoJ 2004;37:239–48.
164. Foschi F, Nucci C, Montebugnoli L, et al. SEM evaluation ofcanal wall dentine following use of Mtwo and ProTaper NiTirotary instruments. Int Endo J 2004;37:832–9.
165. Dalton BC, Orstavik D, Phillips C, et al. Bacterial reductionwith nickel-titanium rotary instrumentation. J Endod1998;24:763–7.
166. Siqueira J, Lima K, Magalhaes F, et al. Mechanical reductionof the bacterial population in the root canal by three instru-mentation techniques. J Endod 1999;25:332–5.
167. Siqueira JF, Rocas IN, Santos SRLD, et al. Efficacy of instru-mentation techniques and irrigation regimens in reducingthe bacterial population within root canals. J Endod2002;28:181–4.
168. McGurkin-Smith R, Trope M, Caplan D, Sigurdsson A.Reduction of intracanal bacteria using GT rotary instrumen-tation, 5.25% NaOCl, EDTA, and Ca(OH)2. J Endod2005;31:359–63.
169. Ferraz CCR, Gomes NV, Gomes BPFA, et al. Apical extru-sion of debris and irrigants using two hand and threeengine-driven instrumentation techniques. Int EndoJ 2001;34:354–8.
170. Er K, Sumer Z, Akpinar KE. Apical extrusion of intracanalbacteria following use of two engine-driven instrumentationtechniques. Int Endo J 2005;38:871–6.
171. Tanalp J, Kaptan F, Sert S, et al. Quantitative evaluation ofthe amount of apically extruded debris using 3 differentrotary instrumentation systems. Oral Surg Oral Med OralPathol Oral Radiol Endod 2006;101:250–7.
172. Linsuwanont P, Parashos P, Messer H. Cleaning of rotary nickel-titanium endodontic instruments. Int Endo J 2004;37:19–28.
173. Aasim SA, Mellor AC, Qualtrough AJE. The effect of pre-soaking and time in the ultrasonic cleaner on the cleanlinessof sterilized endodontic files. Int Endo J 2006;39:143–9.
174. Song YL, Bian Z, Fan B, et al. A comparison of instrument-centering ability within the root canal for three contempor-ary instrumentation techniques. Int Endo J 2004;37:265–71.
175. Shadid DB, Nicholls JI, Steiner JC. A comparison of curvedcanal transportation with balanced force versus Lightspeed.J Endod 1998;24:651–4.
176. Pettiette M, Metzger S, Phillips C, Trope M. Endodonticcomplications of root canal therapy performed by dentalstudents with stainless-steel K-files and nickel-titanium handfiles. J Endod 1999;25:230–4.
Chapter 26 / Endodontics Instruments and Armamentarium / 843

177. Barthel C, Gruber S, Roulet J. A new method to assess theresults of instrumentation techniques in the root canal.J Endod 1999;25:535–8.
178. Park H. A comparison of Greater Taper files, ProFiles, andstainless steel files to shape curved root canals. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2001;91:715–18.
179. Schafer E. Shaping ability of Hero 642 rotary nickel-titaniuminstruments and stainless steel hand K-Flexofiles in simu-lated curved root canals. Oral Surg Oral Med Oral PatholOral Radiol Endod 2001;92:215–20.
180. Tasdemir T, Aydemir H, Inan U, Unal O. Canal preparationwith Hero 642 rotary Ni-Ti instruments compared withstainless steel hand K-file assessed using computed tomogra-phy. Int Endo J 2005;38:402–8.
181. Guelzow A, Stamm O, Martus P, Kielbassa AM. Compara-tive study of six rotary nickel-titanium systems and handinstrumentation for root canal preparation. Int EndoJ 2005;38:743–52.
182. Schirrmeister JF, Strohl C, Altenburger MJ, et al. Shapingability and safety of five different rotary nickel-titaniuminstruments compared with stainless steel hand instrumen-tation in simulated curved root canals. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2006;101:807–13.
183. Peters OA, Laib A, Gohring TN, Barbakow F. Changes inroot canal geometry after preparation assessed byhigh-resolution computed tomography. J Endod 2001;27:1–6.
184. Imura N, Kato AS, Novo NF, et al. A comparison of mesialmolar root canal preparations using two engine-driveninstruments and the balanced-force technique. J Endod2001;27:627–31.
185. Deplazes P, Peters O, Barbakow F. Comparing apical pre-parations of root canals shaped by nickel-titanium rotaryinstruments and nickel-titanium hand instruments. J Endod2001;27:196–202.
186. Peters OA, Schonenberger K, Laib A. Effects of four Ni-Ti preparation techniques on root canal geometryassessed by micro computed tomography. Int Endo J2001;34:221–30.
187. Kaptan F, Sert S, Kayahan B, et al. Comparative evaluationof the preparation efficacies of HERO Shaper and Nitiflexroot canal instruments in curved root canals. OralSurg Oral Med Oral Pathol Oral Radiol Endod2005;100:636–42.
188. Ottosen S, Nicholls J, Steiner J. A comparison of instrumenta-tion using naviflex and profile nickel-titanium engine-drivenrotary instruments. J Endod 1999;25:457–60.
189. Hulsmann M, Schade M, Schafers F. A comparative study ofroot canal preparation with HERO 642 and Quantec SCrotary Ni-Ti instruments. Int Endo J 2001;34:538–46.
190. Bergmans L, Van Cleynenbreugel J, Beullens M, et al. Pro-gressive versus constant tapered shaft design using NiTirotary instruments. Int Endo J 2003;36:288–95.
191. Hulsmann M, Gressman G, Schafers F. A comparativestudy of root canal preparation using FlexMaster andHERO 642 rotary Ni-Ti instruments. Int Endo J2003;36:358–66.
192. Yun H, Kim SK. A comparison of the shaping abilities of 4nickel-titanium rotary instruments in simulated root canals.Oral Surg Oral Med Oral Pathol Oral Radiol Endod2003;95:228–33.
193. Veltri M, Mollo A, Pini PP, et al. In vitro comparison ofshaping abilities of ProTaper and GT rotary files. J Endod2004;30:163–6.
194. Iqbal MK, Firic S, Tulcan J, et al. Comparison of apicaltransportation between ProFile and ProTaper NiTi rotaryinstruments. Int Endo J 2004;37:359–64.
195. Ayar LR, Love RM. Shaping ability of ProFile and K3 rotaryNi-Ti instruments when used in a variable tip sequence insimulated curved root canals. Int Endo J 2004;37:593–601.
196. Yoshimine Y, Ono M, Akamine A. The shaping effects ofthree nickel-titanium rotary instruments in simulated S-shaped canals. J Endod 2005;31:373–5.
197. Sae-Lim V, Rajamanickam I, Lim B, Lee H. Effectiveness ofProFile .04 taper rotary instruments in endodontic retreat-ment. J Endod 2000;26:100–4.
198. Ferreira JJ, Rhodes JS, Pitt Ford TR. The efficacy of gutta-percha removal using ProFiles. Int Endo J 2001;34:267–74.
199. Barrieshi-Nusair KM. Gutta-percha retreatment: Effective-ness of nickel-titanium rotary instruments versus stainlesssteel hand files. J Endod 2002;28:454–6.
200. Betti LV, Bramante CM. Quantec SC rotary instrumentsversus hand files for gutta-percha removal in root canalretreatment. Int Endo J 2001;34:514–19.
201. Masiero AV, Barletta FB. Effectiveness of different techni-ques for removing gutta-percha during retreatment. IntEndo J 2005;38:2–7.
202. Kosti E, Lambrianidis T, Economides N, Neofitou C. Ex vivostudy of the efficacy of H-files and rotary ni-ti instrumentsto remove gutta-percha and four types of sealer. Int EndoJ 2006;39:48–54.
203. Schirrmeister JF, Wrbas K-T, Meyer KM, et al. Efficacy ofdifferent rotary instruments for gutta-percha removal inroot canal retreatment. J Endod 2006;32:469–72.
204. Schirrmeister JF, Meyer KM, Hermanns P, et al. Effective-ness of hand and rotary instrumentation for removinga new synthetic polymer-based root canal obturationmaterial (Epiphany) during retreatment. Int EndoJ 2006;39:150–6.
205. Berry KA, Loushine RJ, Primack PD, Runyan DA. Nickel-titanium versus stainless steel finger spreaders in curvedcanals. J Endod 1998;24:752–4.
206. Schmidt K, Walker T, Johnson J, Nicoli B. Comparison ofnickel-titanium and stainless-steel spreader penetration andaccessory cone fit in curved canals. J Endod 2000;26:42–4.
844 / Endodontics

207. Gharai SR, Thorpe JR, Strother JM, McClanahan SB. Com-parison of generated forces and apical microleakage usingnickel-titanium and stainless steel finger spreaders in curvedcanals. J Endod 2005;31:198–200.
208. Zakariasen KA, Zakariasen KL. Comparison of hand, hand/sonic, and hand/mechanical instrumentation methods.J Dent Res 1994;73:215.
209. Zakariasen KL, Buerschen GH, Zakariasen KA. A compar-ison of traditional and experimental instruments for endo-dontic instrumentation. J Dent Res 1995;74:100.
210. Hulsman M, Stryga F. Comparison of root canal preparationusing different automated devices and hand instrumenta-tion. J Endod 1993;19:141–5.
211. Kosa D, Marshall G, Baumgartner J. An analysis of canalcentering using mechanical instrumentation techniques.J Endod 1999;25:441–5.
212. Molven O. A comparison of the dentin removing abilityof five root canal instruments. Scand J Dent Res1970;78:500–11.
213. O’Connell DT, Brayton SM. Evaluation of root canalpreparation with two automated endodontic handpieces.Oral Surg Oral Med Oral Pathol Oral Radiol Endod1975;39:298–303.
214. Klayman S, Brilliant J. A comparison of the efficacy of serialpreparation versus Giromatic preparation. J Endod 1975;1:334–7.
215. Weine FS, Kelly RF, Bray KE. Effect of preparation withendodontic handpieces on original canal shape. J Endod1976;2:298–303.
216. Harty F, Stock C. The Giromatic system compared with handinstrumentation in endodontics. Br Dent J 1974;137:239–44.
217. Felt RA, Moser JB, Heuer MA. Flute design of endodonticinstruments: its influence on cutting efficiency. J Endod1982;8:253–9.
218. Spyropoulos S, El Deeb ME, Messer HH. The effect ofGiromatic files on the preparation shape of severely curvedcanals. Int Endod J 1987;20:133–42.
219. Luebke NH, Brantley WA. Physical dimensions and tor-sional properties of rotary endodontic instruments.I. Gates-Glidden drills. J Endod 1990;16:438–41.
220. Luebke NH. Performance of Gates-Glidden drill with anapplied deflection load. J Endod 1989;15:175.
221. Luebke NH, Brantley WA. Torsional and metallurgical prop-erties of rotary endodontic instruments. II Stainless steelGates-Glidden drills. J Endod 1991;17:319–23.
222. Johnson TA, Zelikow R. Ultrasonic endodontics: a clinicalreview. J Am Dent Assoc 1987;114:655–7.
223. Richman MJ. The use of ultrasonics in root canal therapyand root resection. J Dent Med 1957;12:12–18.
224. Cunningham WT, Martin H. A scanning electron micro-scope evaluation of root canal debridement with the endo-
sonic ultrasonic synergistic system. Oral Surg Oral Med OralPathol Oral Radiol Endod 1982;53:527–31.
225. Martin H. Ultrasonic disinfection of the root canal. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1976;42:92–9.
226. Martin H, Cunningham WT, Norris JP, Cotton WR. Ultra-sonic versus hand filing of dentin: a quantitative study.Oral Surg Oral Med Oral Pathol Oral Radiol Endod1980;49:79–81.
227. Martin H, Cunningham WT, Norris JP. A quantitative com-parison of the ability of diamond and K-type files to removedentin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1980;50:566–8.
228. Martin H, Cunningham WT. The effect of endosonic andhand manipulation on the amount of root canal materialextruded. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1982;53:611–13.
229. Martin H, Cunningham WT. An evaluation of postoperativepain incidence following endosonic and conventional rootcanal therapy. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1982;54:74–6.
230. Cunningham WT, Martin H, Forrest WR. Evaluation of rootcanal debridement with the endosonic ultrasonic synergisticsystem. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1982;53:401–4.
231. Cunningham WT, Martin H. A scanning electron microscopeevaluation of root canal debridement with the endosonicultrasonic synergistic system. Oral Surg Oral Med Oral PatholOral Radiol Endod 1982;53:527–31.
232. Cunningham WT, Martin H, Pelleu GB, Stoops DE. A com-parison of antimicrobial effectiveness of endosonic and handroot canal therapy. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1982;54:238–41.
233. Cameron JA. The use of ultrasonics in the removal of thesmear layer: a scanning electron microscope study. J Endod1983;9:289–92.
234. Scott GL, Walton RE. Ultrasonic endodontics: the wear ofinstruments with usage. J Endod 1986;12:279–83.
235. Krell KV, Neo J. The use of ultrasonic endodontic instru-mentation in the retreatment of a paste-filled endodontictooth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1985;60:100–2.
236. Yamaguchi M, Matsumori M, Ishikawa H et al. The use ofultrasonic instrumentation in the cleansing and enlargementof the root canal. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1988;65:349–53.
237. Cameron JA. The effect of ultrasonic endodontics onthe temperature of the root canal wall. J Endod1988;14:554–9.
238. Haidet J, Reader A, Beck M, Meyers W. An in vivo compar-ison of the step-back technique versus a step-back/ultrasonictechnique in human mandibular molars. J Endod1989;15:195–9.
Chapter 26 / Endodontics Instruments and Armamentarium / 845

239. Briggs PFA, Gulabivala K, Stock CJR, Setchell DJ. The den-tine-removing characteristics of an ultrasonically energizedK-file. Int Endod J 1989;22:259–68.
240. Pedicord D, El Deeb ME, Messer HH. Hand versus ultra-sonic instrumentation: its effect on canal shape and instru-mentation time. J Endod 1986;12:375–81.
241. Chenail BL, Teplitsky PE. Endosonics in curved root canals.Part II. J Endod 1988;14:214–17.
242. Baker MC, Ashrafi SH, Van Cura JE, Remeikis NA. Ultra-sonic compared with hand instrumentation: a scanningelectron microscope study. J Endod 1988;14:435–40.
243. Krell KV, Johnson RJ. Irrigation patterns of ultrasonic files.Part II. Diamond coated files. J Endod 1988;14:535–7.
244. Walsh CL, Messer HH, El Deeb ME. The effect of varying theultrasonic power setting on canal preparation. J Endod1990;16:273–8.
245. Ahmad M, Pitt Ford TR, Crum LA. Ultrasonic debridementof root canals: an insight into the mechanisms involved.J Endod 1987;13:93–101.
246. Ahmad M, Pitt Ford TR, Crum LA. Ultrasonic debridementof root canals: acoustic streaming and its possible role.J Endod 1987;13:490–9.
247. Ahmad M, Pitt Ford TR, Crum LA, Walton AJ. Ultrasonicdebridement of root canals: acoustic cavitation and its rele-vance. J Endod 1988;14:486–93.
248. Archer R, Reader A, Nist R, et al. An in vivo evaluation of theefficacy of ultrasound after step-back preparation in man-dibular molars. J Endod 1992;18:549–52.
249. Walmsley AD, Williams AR. Effects of constraint on the oscil-latory pattern of endosonic files. J Endod 1989;15:189–94.
250. Krell KV, Johnson RJ, Madison S. Irrigation patterns duringultrasonic canal instrumentation. Part I. K-type files.J Endod 1988;14:65–8.
251. Lumley PJ, Walmsley AD. Effect of precurving on the per-formance of endosonic K-files. J Endod 1992;18:232–6.
252. Ahmad M, Pitt Ford TR, Crum LA, Wilson RF. Effectivenessof ultrasonic files in the disruption of root canal bacteria.Oral Surg Oral Med Oral Pathol Oral Radiol Endod1990;70:328–32.
253. Ahmad M, Pitt Ford TR. Comparison of two ultrasonic unitsin shaping curved canals. J Endod 1989;15:457–62.
254. Ahmad M. Shape of the root canal after ultrasonic instru-mentation with K-Flex files. Endod Dent Traumatol1990;6:104–8.
255. Walmsley AD, Lumley PJ, Laird WR. The oscillatory patternof sonically powered endodontic files. Int EndodJ 1989;22:125–32.
256. Dummer PMH, Alodeh MHA, Doller R. Shaping of simu-lated root canals in resin blocks using files activated by asonic handpiece. Int Endod J 1989;22:211–25.
257. Bolanos OR, Sinai IH, Gonsky MR, Srinivasan R. A compar-ison of engine and air-driven instrumentation methods withhand instrumentation. J Endod 1988;14:392–6.
258. Ehrlich AD, Boyer TJ, Hicks ML, Pelleu GB. Effect of sonicinstrumentation on the apical preparation of curved canals.J Endod 1989;15:200–3.
259. Tronstad L, Niemczyk SP. Efficacy and safety tests of sixautomated devices for root canal instrumentation. EndodDent Traumatol 1986;2:270–6.
260. Miserendino LJ, Miserendino CA, Moser JB, et al. Cuttingefficiency of endodontic instruments. Part III. Comparisonof sonic and ultrasonic instrument systems. J Endod1988;14:24–30.
261. Kielt LW, Montgomery S. The effect of Endosonic instrumen-tation in simulated root canals. J Endod 1987;13:215–19.
262. Zakariasen KL, Zakariasen KA, McMinn M. Today’s sonics:using the combined hand/sonic endodontic technique. J AmDent Assoc 1992;123:67–78.
263. Walker TL, del Rio CE. Histological evaluation of ultrasonicand sonic instrumentation of curved root canals. J Endod1989;15:49–59.
264. Yahya AS, El Deeb ME. Effect of sonic versus ultrasonicinstrumentation on canal preparation. J Endod1989;15:235–9.
265. Reynolds MA, Madison S, Walton RE, et al. An in vitrohistological comparison of the step-back, sonic and ultraso-nic instrumentation techniques in small curved canals.J Endod 1987;13:307–14.
266. Lumley PJ, Walmsley AD, Walton RE, Rippin JW. Cleaningof oval canals using ultrasonic or sonic instrumentation.J Endod 1993;19:453–7.
267. Lev R, Reader A, Beck M, Meyers W. An in vitro compar-ison of the step-back technique versus a step-back/ultra-sonic technique for 1 and 3 minutes. J Endod1987;13:523–30.
268. Stamos DE, Sadeghi EM, Haasch GC, Gerstein H. An in vitrocomparison study to quantitate the debridement ability ofhand, sonic and ultrasonic instrumentation. J Endod1987;13:434–40.
269. Goldman M, Sakurai-Fuse E, Turco J, White RR. A siliconemodel method to compare three methods of preparing theroot canal. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1989;68:457–61.
270. Pugh RJ, Goerig AC, Glaser CG, Luciano WJ. A compar-ison of four endodontic vibration systems. Gen Dent1989;37:296–301.
271. Barnett F, Trope M, Khoja M, Tronstad L. Bacteriologicstatus of the root canal after sonic, ultrasonic and handinstrumentation. Endod Dent Traumatol 1985;1:228–31.
272. Fairbourn DR, McWalter GM, Montgomery S. The effect offour preparation techniques on the amount of apicallyextruded debris. J Endod 1987;13:102–8.
846 / Endodontics

273. Jensen S, Walker T, Hutter J, Nicoll B. Comparison of thecleaning efficacy of passive sonic activation and passiveultrasonic activation after hand instrumentation inmolarroot canals. J Endod 1999;25:735–8.
274. Sabins RA, Johnson JD, Hellstein JW. A comparison of thecleaning efficacy of short-term sonic and ultrasonic passiveirrigation after hand instrumentation in molar root canals.J Endod 2003;29:674–8.
275. Gutarts R, Nusstein J, Reader A, Beck M. In vivo debride-ment efficacy of ultrasonic irrigation following hand-rotaryinstrumentation in human mandibular molars. J Endod2005;31:166–70.
276. Lee SJ, Wu MK, Wesselink PR. The efficacy of ultrasonic irriga-tion to remove artificially placed dentine debris from different-sized simulated plastic root canals. Int Endo J 2004;37:607–12.
277. van der Sluis LWM, Wu M-K, Wesselink PR. The efficacy ofultrasonic irrigation to remove artificially placed dentine deb-ris from human root canals pre-pared using instruments ofvarying taper. Int Endo J 2005;38:764–8.
278. Lee SJ, Wu MK, Wesselink PR. The effectiveness of syringeirrigation and ultrasonics to remove debris from simulatedirregularities within prepared root canal walls. Int EndoJ 2004;37:672–8.
Chapter 26 / Endodontics Instruments and Armamentarium / 847

D. ELECTRONIC APEX LOCATORS
ADAM LLOYD, JOHN I. INGLE
The dentin–cementum junction has been recom-mended as an ideal apical termination for root canalpreparation.1–3 The position of this histologic entityvaries around the internal circumference of the canalby up to 3 mm across opposing walls.4,5 It is locatedapproximately 1 mm away from the apical foramen.6
An apical constriction usually occurs in the region ofthe dentin–cementum junction and often forms anatural apical matrix. It is the narrowest portal ofentry of the pulpal vasculature from the periapicaltissues and would be the smallest wound followingpulp removal.7 The topography of the apical constric-tion is variable8 and undetectable radiographically.Kuttler9 investigated the root apices of teeth andprovided a dimensional analysis of the apical mor-phology. He noted that the distance from the apicalconstriction to the vertex of the root increased withage and was recorded as between 0.5 and 0.6 mm.This distance was considered as a measurement tosubtract from the radiographic apex to approximatethe location of the apical constriction.10
Working length, the apical extent of canal prepara-tion and obturation, is often the main variable indetermining success or failure.11–16 Seltzer et al.17
were the first to report greater success in terminatingcleaning and obturating the root canal system justshort of the radiographic apex, rather than overfillingor underfilling. Sjogren et al.18 investigated endodon-tic outcomes over an 8- to 10-year period in over 350patients. They reported the best outcome was whenthe root canal filling was between 0 to 2 mm short ofthe radiographic apex. Distances beyond the radio-graphic apex, or more than 2 mm short of this point,resulted in significantly lower success rates. Thesefindings are in agreement with research conductedby other investigators14–19 and most recently bymeta-analysis of the literature.20
Chugal21 found variations in success rate of teethroot filled at different levels. Teeth with normal pre-operative pulps and periapical tissues enjoyed a highersuccess rate when filled over 1 mm from the radio-graphic apex. On the other hand, teeth with necroticpulps and apical periodontitis showed greater success
when the canal filling was closer to the level of theradiographic apex. From all the evidence cited, it isclearly prudent to be able to accurately prepare andfill root canals to a predetermined location in thecanal short of the actual apical foramen—ideally thedentin–cementum junction.
The common method of determining root canallength for the past 100 years has been by radio-graphy (see Chapter 15A, ‘‘Endodontic Radiogra-phy’’). This method unfortunately often leads toinaccuracies, even though various techniques forimproved radiographic length determination havebeen developed.22–29 Interpretation of the file’sposition on the radiograph and the surroundinganatomy is also prone to errors when using thebisecting angle technique.29 Estimation of the canallength often varies greatly from actual workinglength. The long-cone paralleling technique hasbeen shown to be more accurate.29 Furthermore,radiographs only provide a two-dimensional repre-sentation of the three-dimensional object and canalso be interpreted differently between clini-cians.30,31 In fact, reports of observer agreement indetermining file position found that agreementdecreased as the distance from the radiographicapex increased.32
Many digital radiographic techniques do not easilypermit obtaining endodontic working films with thelong-cone paralleling technique, which necessitatesusing the bisecting angle method.33 The use of digitalradiography has reduced radiation exposure ofpatients,34,35 increased the speed of delivery, and cre-ated the ability to ‘‘enhance’’ images.36 However, stu-dies have shown that digital radiographs have nogreater resolution than conventional radiographs.37–41
In addition to radiography, tactile sensation hasbeen used with questionable success, plus the draw-backs cited about radiographic length determination,along with the increasing concern about radiationexposure, the introduction and development ofthe electronic apex locator (EAL) has been receivedwith enthusiasm by clinicians performing endodonticprocedures.
848

The first reported use of electric current to mea-sure root canal working length was in 1918 byCuster.42 He noted a marked increase in the con-ductivity of a tooth at the apical foramen when thecanal was dry or filled with a nonconductive med-ium. By placing a broach inside a tooth and apply-ing a voltage across it and the alveolus, Custer wasable to identify the apical foramen by observing achange in the value on the milliammeter of thetime.42
Suzuki43 found that an electrode placed on the oralmucosa, and an instrument placed in the root canal,gave consistent measurements of electrical resistance.This is the basis for the resistance-based EALs. As theadvancing file, surrounded by insulating dentin andcementum, approaches the conductive periodontalligament, the resistance decreases until the circuit iscomplete.
Sunada44 used this principle to create a device,using direct current, to estimate the root canal lengthin vivo. He found that when the file reached the canalterminus, regardless of tooth shape, tooth type, or ageof the patient, the resistance measured was consistentat 6.5 KW. Furthermore, the same resistance wasrecorded when the file encountered an accidental per-foration.44
Direct current apex locators have also been asso-ciated with patients experiencing electric shocks.45–46
Suchde and Talim45 proposed changing to alternatingcurrent, which would result in less tissue damage andincreased stability of the electrolyte’s resistance in awet canal. The disadvantage, however, in determiningcanal length in this manner, is the change in thecapacitance of the circuit, along with many othervariables that affect accuracy.45,47 Meredith and Gula-bivala48 discovered that impedance in a tooth andperiradicular tissues consists of resistive and capaci-tance circuits that provide a model for EALs.
The first generation of EALs was based on resis-tance, and the resistance was measured between thetwo electrodes to determine location within a canal.The second generation employed single-frequencyimpedance, in which impedance measurementsinstead of resistance was used to measure locationwithin a canal. The improvement of the second overthe first generation was essentially that it wouldgather more information. Impedance is a complexproperty comprised of resistance and capacitance.Whereas resistance has constant amplitude, impe-dance is sinusoidal. The frequency of an impe-dance-based unit can be varied to compensate forcanal conditions. The third generation of EAL wassimilar to the second, but it used multiple frequen-
cies to determine distances from the end of the canal.The fourth generation of EALs breaks impedancedown into its primary components (resistance andcapacitance) and measures them independently dur-ing use. This eliminates erroneous readings becausedifferent combinations of these properties providethe same impedance reading. This prevents EALsfrom being ‘‘jumpy’’ and erratic. Multiple frequen-cies are still used to compensate for canal conditions.The Elements Diagnostic Unit (SybronEndo, Glen-dora, CA) (Figure 1) does not make calculationsinternally as third-generation units do. Instead, allcombinations of capacitance and resistance relatingto location within the canal have been loaded into amatrix database within the unit (Figure 2). Thisdecreases processing time, making the displayedinformation much more stable.
Accuracy of Electronic Apex Locators
A concern for accuracy in determining working lengthhas generated many investigations using variousEALs. Concern for accuracy also affected its accep-tance for use in practices which has varied from 10%in the United States to 90% in Japan.49–54
RESISTANCE-BASED ELECTRONIC APEXLOCATORSAs the file approaches the periodontal ligament, thevoltage change divided by the current (amperes)results in decreasing resistance, per Ohm’s law, untila value of 6.5 KW is reached.44 The accuracy ofresistance-based apex locators can be high providedcertain conditions are adhered to. Dry canals providedthe most accurate readings. Strong electrolytes such asendodontic irrigants, purulence, excess hemorrhage,or pulp tissue lead to inaccurate and even unstableresults.55–59 In 1969, Bramante and Berbert60 lookedat the first commercially available apex locator, theRoot Canal Meter, and found it to be consistentlymore accurate than radiographs in the palatal rootsof maxillary molars and premolars. The originaldevice, however, often elicited a painful response bythe patient. Further refinements were made in laterEAL models measuring resistance such as the Endo-dontic Meter and the Endodontic Meter S II.61 Themore recent resistance-based apex locators providedaccurate location of the apical constriction 55 to 75%of the time.62 However, their accuracy was still dimin-ished in the presence of fluids.63
Chapter 26 / Endodontics Instruments and Armamentarium / 849

Figure 2 Matrix database for the Elements Diagnostic software: The left axis identifies the measured resistance in ohms, the right axis identifies themeasured capacitance in microfarads, and the vertical axis illustrates the resultant apex location that is displayed. It is shown in segments on the unitdisplay, ‘‘41 segments’’ being the ‘‘0’’ reading, ‘‘37 segments’’ being ‘‘0.5 mm,’’ and so on.
Figure 1 The Sybron Elements Diagnostic Unit is an example of a current electronic apex locator with a vitality scanner. A, Elements Diagnostic Unit; B,file clip; C, vitality probes; D, lip hook; E, satellite.
850 / Endodontics

LOW-FREQUENCY APEX LOCATORSThe resistance-based circuit proved insufficient to accu-rately and consistently measure root canal length.48,64,65
Impedance rather than resistance became the char-acteristic used to mark the depth of canal penetra-tion. In 1972, the Sono-Explorer was introduced byInoue64,66 on the premise that although the manyparameters that determine impedance are varied indifferent canals under altered conditions, the impe-dance between the oral mucosa and depth of thegingival sulcus should be coincident with the impe-dance value of a circuit across the oral mucosa andthe periodontal ligament. Thus, the device wouldindicate the canal terminus when the two impe-dance values approached each other. The frequencyof the impedance was heard as an audible ‘‘markertone’’ that signaled the endpoint of the canal, gen-erated by low-frequency oscillation. The device hadto be calibrated at the periodontal sulcus beforeeach use. This involved placing a file, shieldedalong its length except for its tip, into the gingivalsulcus, and listening for the ‘‘gingival crevicesound.’’ A file was then introduced into the canal,and when the sound became identical to the ‘‘gin-gival crevice sound,’’ the canal terminus had beenreached. A disadvantage of the first model Sono-Explorer was the depth at which the probe couldbe placed into the gingival sulcus. If the referencetuner was placed deeper than 0.5 mm into the crevicewhen tuning the device, the gingival frequencyincreases resulted in the tip of the file protrudingthrough the apical foramen.67 The Sono-Explorer IIrectified this with a coated gingival frequency me-asuring probe, but the accuracy still remained disap-pointing.
HIGH-FREQUENCY APEX LOCATORSThe Endocater was introduced by Hasegawa in197959,62 with the premise that operating with ahigh-frequency wave (400 kHz) as a measuring cur-rent produces a more stable single electrode.68,69 Thedevice is able to perform accurate measurements inthe presence of electrolytes and pulp tissue due to thefile having a special coating except for the exposedtip, thereby decreasing the variable capacitive prop-erties.70 Accuracy with the Endocater has beenreported between 67 and 93.4%.62,65,71 A problemoccurred in constricted canals when the coating ofthe file caused it to bind prematurely.65 In addition,the coating did not withstand repeated autoclaving.72
Fouad et al.62 tested the Endocater with uncoatedfiles and found grossly inaccurate results.
VOLTAGE GRADIENT APEX LOCATORSCuster42 and subsequently Sunada44 relied on a con-stant resistance value of 6.5 KW between the canaland the periodontal membrane, and Ushiyama73
used both monopolar and bipolar electrodes coatedin lacquer with just the tip exposed, similar to theEndocater. Ushiyama found the voltage gradient wasgreatest at the most constricted point in the canal,where the current density is the highest. The princi-ple of Ushiyama’s device differs from Sunada’s44
resistance-based device in that separate electrodesare used to apply current to the probe and to recordthe voltage. Ushiyama pointed out a potential flaw inthe resistance value of 6.5 KW quoted by Sunada44
reporting that this more likely reflected the resistanceof the metal electrode in contact with the canal con-tents, as a result of the polarization produced. Theeffect was minimized by Ushimaya’s coated electro-des. Further investigation, using the monopolar andbipolar electrodes, respectively, were found to besuccessful in all but two cases tested.74 Unfortu-nately, the thickened bipolar electrodes did not allowthem to travel freely to the constriction in narrowcanals.
DUAL-FREQUENCY ELECTRONIC APEXLOCATORSIn 1990, Saito and Yamashita75 investigated the useof the Endex, developed by Yamaoka, describing themethod of determining the canal terminus as thedifference between two impedance values at twodifferent frequencies. Calibration of the device inthe coronal region is required to compensate forthe dielectric capacity of the electrolyte in the canal.The findings from the study concluded that there wereno differences in locating the apical foramen whendifferent file sizes were used, a different apical diameterwas encountered, or in the presence of saline, 5%sodium hypochlorite, 14% EDTA, or 3% hydrogenperoxide. The Endex was also marketed under the Apitbrand name and further studied by Fouad et al.,63 whoalso found the Endex superior to other apex locators inthe presence of electrolytes, especially where the apicalforamen was widened.
In 1993, Frank and Torabinejad,76 using theEndex, took canal measurements of 99 teeth in vivoand were able to locate the file tip, in moist canals, towithin 0.5 mm of the apical constriction in nearly90% of the specimens. Mayeda et al.77 studied theEndex to determine whether there were differencesin accuracy in vital or necrotic cases in vivo, finding
Chapter 26 / Endodontics Instruments and Armamentarium / 851

that there was no statistical difference based on pul-pal status, and that generally file tips were foundbetween +0.50 mm to 0.86 mm from the apical fora-men.
Felippe and Soares78 investigated 350 extractedteeth in vitro and found the Endex to locate theapical foramen within 0 to 0.5 mm in 96.5% of thespecimens studied. Arora and Gulabivala79 com-pared the Endex with the RCM Mark II EAL in vivo.They used sodium hypochlorite, pus, water, andvital and necrotic pulp tissue as possible electrolytes.They also exposed a radiograph before extracting thetooth and then examined the file position visually.What was evident from the study was an overesti-mation of the file’s position based solely on theradiograph, with the file extending beyond the fora-men. The extensions were affected by the canal’scontents. The Endex was found to be within0.5 mm of the apical foramen 71.7% of the time,whereas the RCM Mark II AEL had only a 43.5%rate of accuracy. The Endex performed betterthan the RCM Mark II in the presence of sodiumhypochlorite.
MULTIPLE-FREQUENCY ELECTRONICAPEX LOCATORSBy the ratio method of canal length determination,these dual-frequency AELs overcame differences inthe changing dielectric constant of different electro-lytes left in the root canal system.80,81 The position ofthe file tip is derived from the simultaneous measure-ment of the impedance of two different frequenciesthat are used to calculate the quotient of the impe-dances. The Root ZX (J. Morita Manufacturing Co.,Kyoto, Japan) was one of these. It was initially intro-duced between 1991 and 1994 by Kobayashi andSuda.82 The Root ZX simultaneously uses two wave-forms, a high (8 kHz) and low (400 Hz) frequencywaveform. As the content of the fluid changes withinthe root canal, the ratio of the impedances would bemodified by the same rate as each other, yielding aratio that would not differ. This results in the samepositioning of the file tip regardless of the canal con-tents.82 In vitro studies of the Root ZX have shownit to be accurate in the presence of electrolytes.83
Varying concentrations of sodium hypochloritemade no significant difference in performance.84,85
The accuracy of the Root ZX has been reported torange from 64% to 100%. If 1.0 mm difference isdeemed acceptable, the accuracy is reported at100%.86 Lesser deviations from the apical constrictionare reproducible.87,88
The Bingo 1020 (Forum Technologies, RishonLeZion, Israel) compared favorably with the RootZX regardless of canal contents or irrigants. Bothwere deemed more reliable than the radiographicinterpretation.89 An in vitro study also found theBingo 1020 and the Root ZX performed equally wellin the hands of clinicians with varying degrees ofexperience.90 The Bingo 1020 is also marketed asthe Raypex 4 (Roydent Dental Products, JohnsonCity, TN) and as the ProPex (Dentsply Maillefer,Ballaigues, Switzerland).
Welk et al.91 tested the accuracy of the five-fre-quency Endo Analyzer Model 8005 (Analytic, SybronDental, Orange, CA) against the Root ZX and foundthe latter able to locate the apical foramen ±0.5 mmover 90% of the time with a mean difference less the0.2 mm, compared with the Endo Analyzer at over1.0 mm. Lucena-Martin et al.92 found the Root ZXto be consistently reliable at 85%. A similar clinicalcomparison was conducted in Hungary in 2006,where Gyorfi et al.93 determined the working lengthsof 10 canals using radiographs and then comparedthese findings with four different apex locators. TheRoot ZX and the Foramatron D10 (Parkell Co.,Edgewood, NY) agreed with the radiographic analy-sis in all 10 canals. The Apex Finder AFA 7005(Analytic, Sybron Dental) agreed on seven canalsand the ProPex (Dentsply Maillefer) agreed on fivecanals.
Tselnik et al.94 recently tested the Elements Diag-nostic EAL (Sybron Endo, Sybron Dental, Orange,CA) against the Root ZX in vivo. Both devices wereaccurate to 75% of the time to ±0.5 mm from theminor diameter. Haffner et al.95 reported a similarfinding for the latter at 78%. Plotino et al.96 testedthe Root ZX, the Elements Diagnostic Unit, and theProPex unit and found their accuracy at 97.4, 94.3,and 100%, respectively, although the majority of theProPex readings were beyond the apex.
In 2005, Goldberg et al.97 compared the Root ZX,the ProPex (Dentsply Maillefer), and the NovApex(Forum Technologies) for accuracy in re-treatmentcases. At 0.5 mm from the foramen, they reported anaccuracy level of 95, 80, and 85%, respectively.
Foramina of unusual width can cause unreliableapex locator readings, particularly if a fine diameterfile is used. However, Ebrahim et al.98 concluded thatwhen a tight-fitting file was used to determine work-ing length of canals with large diameter foramina, theForamatron D10 (Parkell Co.) and the Root ZX weresignificantly more accurate than the Apex NRG (Kib-butz Afikim, Israel) or the Apit 7 (Osada, Tokyo,Japan).
852 / Endodontics

A number of other studies have been done assessingthe qualities of these newest AELs. It was found, forinstance, that stainless steel and nickel–titanium fileswere equally effective as canal ‘‘electrodes.’’99 It wasalso noted that EALs are effective devices in determin-ing resorptive defects and their location100 and inmeasuring the working length in resorbing deciduousteeth.101
Morita has modified the Root ZX, applying theprinciple to the Solfy ZX, marketed only in Japan,which enables the operator to stop at any distancefrom the desired length,68 as well as the Tri-Auto ZXand the Dentaport ZX that combine the apex locatorwith plug-in and/or cordless battery-operated hand-pieces that have an auto-reverse feature when theapex is reached or if the instrument binds in thecanal.102–104
Parameters for Use of Electronic Apex
Locators
The original apex locators proved to be more reli-able in a dry canal than in the presence of saline ordistilled water.45 Manufacturers of newer modelsclaim the ability of their apex locators to work inboth dry and wet conditions, including in the pre-sence of blood, pulp tissue, and the common endo-dontic irrigants. Although these claims have nowshown the accuracy to be between 83 and96%,59,83,84,88,105,106 there are other factors thatneed to be considered in using an apex locator inpractice. Contemporary root canal preparationwith nickel–titanium rotary endodontic instru-ments typically involves crown-down preparationsand some form of preflaring and removal of coro-nal obstructions. It has been shown that preflaringincreases the accuracy of EAL.107,108 Further-more, the choice of file alloy, stainless steel, ornickel–titanium appears to have no bearing on apexlocator accuracy.90 Choosing a file that closelymatches the canal diameter appears to no longer bea concern in locating the working length, with stu-dies showing files of sizes much smaller than thecanal, working equally well.106,109 Contact of the fileor probe to metallic restorations or fluid in contactwith the metallic restorations will cause the apexlocator to give a false reading.
Garofalo et al.110 connected EALs directly to apacemaker in an in vitro study and found that fourof five EALs showed no effect on cardiac pacemakerfunction. However, the Bingo 1020 produced an
irregular pace recording and oscilloscope pattern.Wilson et al.111 recently demonstrated no effect onimplanted cardiac pacemakers or cardioverters/defi-brillators with either the Root ZX or the ElementsDiagnostic EALs. However, manufacturers of EALscontinue to warn against the use of their devices inpatients with cardiac pacemakers. It is recommendedto contact the patient’s physician or cardiologist forspecific guidance regarding the use of any electricaldevices.
References
1. Grove C. Why canals should be filled to the dentinocementaljunction. J Am Dent Assoc 1930;17:293–6.
2. Kettle Y. Microscopic investigation of root apexes. J AmDent Assoc 1955;50:544–52.
3. Kuttler Y. A precision and biologic root canal filling technic.J Am Dent Assoc 1958;56:38–50.
4. Ponce EH, Vilar Fernandez JA. The cemento-dentino-canaljunction, the apical foramen, and the apical constriction:evaluation by optical microscopy. J Endod 2003;29:214–19.
5. Gutierrez JH, Aguayo P. Apical foraminal openings inhuman teeth. Number and location. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1995;79:769–77.
6. Smulson MH, Hagen JC, Ellenz SJ. Pulpo-periapical pathol-ogy and immunologic considerations. In: Weine FS, editor.Endodontic therapy. 5th ed. St. Louis: Mosby-Yearbook Inc.;1996. pp. 166–7.
7. Ricucci D, Langeland K. Apical limit of root canal instru-mentation and obturation, part 2. A histological study. IntEndod J 1998;31:394–409.
8. Dummer PM, McGinn JH, Rees DG. The position andtopography of the apical canal constriction and apical fora-men. Int Endod J 1984;17:192–8.
9. Kuttler Y. Microscopic investigation of root apexes. J AmDent Assoc 1955;50:544–52.
10. Stein TJ, Corcoran JF. Radiographic ‘‘working length’’ revis-ited. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1992;74:796–800.
11. Bender IB, Seltzer S, Soltanoff W. Endodontic success—areappraisal of criteria. II. Oral Surg Oral Med Oral PatholOral Radiol Endod 1966;22:790–802.
12. Bender IB, Seltzer S, Soltanoff W. Endodontic success—areappraisal of criteria. I. Oral Surg Oral Med Oral PatholOral Radiol Endod 1966;22:780–9.
13. Matsumoto T, Nagai T, Ida K, et al. Factors affectingsuccessful prognosis of root canal treatment. J Endod1987;13:239–42.
Chapter 26 / Endodontics Instruments and Armamentarium / 853

14. Kerekes K. Radiographic assessment of an endodontic treat-ment method. J Endod 1978;4:210–13.
15. Kerekes K, Tronstad L. Long-term results of endodontictreatment performed with a standardized technique. J Endod1979;5:83–90.
16. Harty FJ, Parkins BJ, Wengraf AM. Success rate in root canaltherapy. A retrospective study of conventional cases. Br Dent J1970;128:65–70.
17. Seltzer S, Soltanoff W, Sinai I, et al. Biologic aspects ofendodontics. III. Periapical tissue reactions to root canalinstrumentation. Part II. Oral Surg Oral Med Oral PatholOral Radiol Endod 1968;26:694–705.
18. Sjogren U, Haglund B, Sundqvist G, Wing K. Factors affect-ing the long-term results of endodontic treatment. J Endod1990;16:498–504.
19. Swartz DB, Skidmore AE, Griffin JA, Jr. Twenty years ofendodontic success and failure. J Endod 1983;9:198–202.
20. Schaeffer MA, White RR, Walton RE. Determining the opti-mal obturation length: a meta-analysis of literature. J Endod2005;31:271–4.
21. Chugal NM, Clive JM, Spangberg LS. A prognostic modelfor assessment of the outcome of endodontic treatment:effect of biologic and diagnostic variables. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2001;91:342–52.
22. Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgeno-graphic investigation of 7,275 root canals. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1972;33:101–10.
23. Green D. Double canals in single roots. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1973;35:689–96.
24. Vertucci FJ. Root canal anatomy of the human permanentteeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1984;58:589–99.
25. Burch JG, Hulen S. The relationship of the apical foramen tothe anatomic apex of the tooth root. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1972;34:262–8.
26. Palmer MJ, Weine FS, Healey HJ. Position of the apicalforamen in relation to endodontic therapy. J Can Dent Assoc1971;37:305–8.
27. Ingle JI. PDQ Endodontics. Hamilton, Ont.: BC Decker;2005. p. 125.
28. Olson AK, Goerig AC, Cavataio RE, Luciano J. The ability ofthe radiograph to determine the location of the apical fora-men. Int Endod J 1991;24:28–35.
29. Forsberg J. A comparison of the paralleling and bisecting-angleradiographic techniques in endodontics. Int Endod J 1987;20:177–82.
30. Tidmarsh BG. Radiographic interpretation of endodonticlesions—a shadow of reality. Int Dent J 1987;37:10–15.
31. Goldman M, Pearson AH, Darzenta N. Endodonticsuccess—who’s reading the radiograph? Oral Surg OralMed Oral Pathol Oral Radiol Endod 1972;33:432–7.
32. Cox VS, Brown CE, Jr., Bricker SL, Newton CW. Radio-graphic interpretation of endodontic file length. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1991;72:340–4.
33. Forsberg J. Radiographic reproduction of endodontic ‘‘work-ing length’’ comparing the paralleling and the bisecting-angletechniques. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1987;64:353–60.
34. Brunton PA, Abdeen D, MacFarlane TV. The effect of anapex locator on exposure to radiation during endodontictherapy. J Endod 2002;28:524–6.
35. Saad AY, al-Nazhan S. Radiation dose reduction duringendodontic therapy: a new technique combining an apexlocator (Root ZX) and a digital imaging system (Radio-VisioGraphy). J Endod 2000;26:144–7.
36. Shearer AC, Horner K, Wilson NH. Radiovisiographyfor length estimation in root canal treatment: an in-vitrocomparison with conventional radiography. Int Endod J1991;24:233–9.
37. Martinez-Lozano MA, Forner-Navarro L, Sanchez-Cortes JL,Llena-Puy C. Methodological considerations in the determi-nation of working length. Int Endod J 2001;34:371–6.
38. Melius B, Jiang J, Zhu Q. Measurement of the distancebetween the minor foramen and the anatomic apex by digitaland conventional radiography. J Endod 2002;28:125–6.
39. Radel RT, Goodell GG, McClanahan SB, Cohen ME. In vitroradiographic determination of distances from workinglength files to root ends comparing Kodak RVG 6000, SchickCDR, and Kodak insight film. J Endod 2006;32:566–8.
40. Velders XL, Sanderink GC, van der Stelt PF. Dose reductionof two digital sensor systems measuring file lengths. OralSurg Oral Med Oral Pathol Oral Radiol Endod1996;81:607–12.
41. Piepenbring ME, Potter BJ, Weller RN, Loushine RJ. Mea-surement of endodontic file lengths: a density profile plotanalysis. J Endod 2000;26:615–18.
42. Custer LE. Exact methods of locating the apical foramen.Natl Dent Assoc J 1918;5:815–19.
43. Suzuki K. Experimental study on iontophoresis. J Jpn Sto-matol 1942;16:411–29.
44. Sunada I. New method for measuring the length of the rootcanal. J Dent Res 1962;41:375–87.
45. Suchde RV, Talim ST. Electronic ohmmeter. An electronicdevice for the determination of the root canal length. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1977;43:141–50.
46. Kim E, Lee SJ. Electronic apex locator. Dent Clin North Am2004;48:35–54.
47. O’Neill LJ. A clinical evaluation of electronic root canalmeasurement. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1974;38:469–73.
48. Meredith N, Gulabivala K. Electrical impedance measure-ments of root canal length. Endod Dent Traumatol1997;13:126–31.
854 / Endodontics

49. Whitten BH, Gardiner DL, Jeansonne BG, Lemon RR. Cur-rent trends in endodontic treatment: report of a nationalsurvey. J Am Dent Assoc 1996;127:1333–41.
50. Saunders WP, Chestnutt IG, Saunders EM. Factors influen-cing the diagnosis and management of teeth with pulpal andperiradicular disease by general dental practitioners. Part 2.Br Dent J 1999;187:548–54.
51. Chandler NP, Koshy S. Radiographic practices of dentistsundertaking endodontics in New Zealand. DentomaxillofacRadiol 2002;31:317–21.
52. Yoshikawa G, Sawada N, Wettasinghe KA, Suda H. Survey ofendodontic treatment in Japan. J Endod 2001;27:236.
53. Hommez GM, Braem M, De Moor RJ. Root canal treatmentperformed by Flemish dentists. Part 1. Cleaning and shaping.Int Endod J 2003;36:166–73.
54. Bjørndal L, Reit C. The adoption of new endodontic tech-nology amongst Danish general dental practitioners. IntEndod J 2005;38:52–8.
55. Nekoofar MH, Ghandi MM, Hayes SJ, Dummer PM.The fundamental operating principles of electronic root canallength measurement devices. Int Endod J 2006;39:595–609.
56. Gordon MPJ, Chandler NP. Electronic apex locators. IntEndod J 2004;37:425–37.
57. McDonald NJ. The electronic determination of workinglength. Dent Clin North Am 1992;36:293–307.
58. Venturi M, Breschi L. A comparison between two electronicapex locators: an in vivo investigation. Int Endod J2005;38:36–45.
59. Fouad AF, Krell KV. An in vitro comparison of five root canallength measuring instruments. J Endod 1989;15:573–7.
60. Bramante CM, Berbert A. A critical evaluation of somemethods of determining tooth length. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1974;37:463–73.
61. Kobayashi C, Suda H. A basic study on the electronic rootcanal length measurement: Part 4. A comparison of 6 apexlocators. Jpn J Conserv Dent 1993;36:185–92.
62. Fouad AF, Krell KV, McKendry DJ, et al. Clinical evaluationof five electronic root canal length measuring instruments.J Endod 1990;16:446–9.
63. Fouad AF, Rivera EM, Krell KV. Accuracy of the Endex withvariations in canal irrigants and foramen size. J Endod1993;19:63–7.
64. Inoue N. An audiometric method for determining the lengthof root canals. J Can Dent Assoc 1973;39:630–6.
65. McDonald NJ, Hovland EJ. An evaluation of the ApexLocator Endocater. J Endod 1990;16:5–8.
66. Inoue N. Dental ‘stethoscope’ measures root canal. DentSurv 1972;48:38–9.
67. Inoue N, Skinner DH. A simple and accurate way to mea-suring root canal length. J Endod 1985;11:421–7.
68. Kobayashi C. Electronic canal length measurement. OralSurg Oral Med Oral Pathol Oral Radiol Endod1995;79:226–31.
69. Iizuka H, Hasegawa K, Takei M, et al. A study on electricmethod for measuring root canal length. J Nihon Univ SchDent 1987;29:278–86.
70. Hasegawa K, Iizuka H, Takei M, et al. A new method andapparatus for measuring root canal length. J Nihon Univ SchDent 1986;28:117–28.
71. Keller ME, Brown CE, Jr., Newton CW. A clinical evaluationof the Endocater—an electronic apex locator. J Endod1991;17:271–4.
72. Himel VT, Schott RN. An evaluation of the durability ofapex locator insulated probes after autoclaving. J Endod1993;19:392–4.
73. Ushiyama J. New principle and method for measuring theroot canal length. J Endod 1983;9:97–104.
74. Ushiyama J, Nakamura M, Nakamura Y. A clinical evalua-tion of the voltage gradient method of measuring the rootcanal length. J Endod 1988;14:283–7.
75. Saito T, Yamashita Y. Electronic determination of root canallength by newly developed measuring device. Influences ofthe diameter of apical foramen, the size of K-file and theroot canal irrigants. Dent Jpn 1990;27:65–72.
76. Frank AL, Torabinejad M. An in vivo evaluation of Endexelectronic apex locator. J Endod 1993;19:177–9.
77. Mayeda DL, Simon JH, Aimar DF, Finley K. In vivo mea-surement accuracy in vital and necrotic canals with theEndex apex locator. J Endod 1993;19:545–8.
78. Felippe MC, Soares IJ. In vitro evaluation of an audiometricdevice in locating the apical foramen of teeth. Endod DentTraumatol 1994;10:220–2.
79. Arora RK, Gulabivala K. An in vivo evaluation of theENDEX and RCM Mark II electronic apex locators in rootcanals with different contents. Oral Surg Oral Med OralPathol Oral Radiol Endod 1995;79:497–503.
80. Kobayashi C, Suda H, Sunada I. A basic study on the electro-nic root canal measurement. Part 2. Measurement usingimpedance analyzer. Jpn J Conserv Dent 1991;34:1208–21.
81. Kobayashi C, Okiji T, Kawashima N, et al. A basic study onthe electronic root canal length measurement: Part 3.Newly designed electronic root canal length measuringdevice using division method. Jpn J Conserv Dent1991;34:1442–8.
82. Kobayashi C, Suda H. New electronic canal measuringdevice based on the ratio method. J Endod 1994;20:111–14.
83. Jenkins JA, Walker WA, III, Schindler WG, Flores CM. An invitro evaluation of the accuracy of the root ZX in the pre-sence of various irrigants. J Endod 2001;27:209–11.
84. Weiger R, John C, Geigle H, Lost C. An in vitro comparisonof two modern apex locators. J Endod 1999;25:765–8.
Chapter 26 / Endodontics Instruments and Armamentarium / 855

85. Tinaz AC, Sevimli LS, Gorgul G, Turkoz EG. The effects ofsodium hypochlorite concentrations on the accuracy of anapex locating device. J Endod 2002;28:160–2.
86. Pagavino G, Pace R, Baccetti T. A SEM study of in vivoaccuracy of the Root ZX electronic apex locator. J Endod1998;24:438–41.
87. Vajrabhaya L, Tepmongkol P. Accuracy of apex locator.Endod Dent Traumatol 1997;13:180–2.
88. Shabahang S, Goon WW, Gluskin AH. An in vivo evaluationof Root ZX electronic apex locator. J Endod 1996;22:616–18.
89. Kaufman AY, Keila S, Yoshpe M. Accuracy of a new apexlocator: an in vitro study. Int Endod J 2002;35:186–92.
90. Tinaz AC, Maden M, Aydin C, Turkoz E. The accuracy ofthree different electronic root canal measuring devices: an invitro evaluation. J Oral Sci 2002;44:91–5.
91. Welk AR, Baumgartner JC, Marshall JG. An in vivo compar-ison of two frequency-based electronic apex locators. J Endod2003;29:497–500.
92. Lucena-Martin C, Robles-Gijon V, Ferrer-Luque CM, deMondelo JM. In vitro evaluation of the accuracy of threeelectronic apex locators. J Endod 2004;30:231–3.
93. Gyorfi A, et al. An in vivo comparison of different apex locatorsduring endodontic treatment. Hungarian Society of Endodon-tology and Dent-Maxillo-Facial-Radiological Section of theHungarian Dental Association. June 04, 2006.
94. Tselnik M, Baumgartner JC, Marshall JG. An evaluation ofroot ZX and elements diagnostic apex locators. J Endod2005;31:507–9.
95. Haffner C, Folwaczny M, Galler K, Hickel R. Accuracy ofelectronic apex locators in comparison to actual length—anin vivo study. J Dent 2005;33:619–25.
96. Plotino G, Grande NM, Brigante L, et al. Ex vivo accuracy ofthree electronic apex locators: Root ZX, elements diagnosticunit and apex locator and propex. Int Endod J2006;39:408–14.
97. Goldberg F, Marroquin BB, Frajlich S, Dreyer C. In vitroevaluation of the ability of three apex locators to determinethe working length during retreatment. J Endod 2005;31:676–8.
98. Ebrahim AK, Wadachi R, Suda H. Ex vivo evaluation offour different apex locators to determine the working lengthin teeth with various foramen diameters. Aust Dent J 2006;51(3):258–62.
99. Thomas AS, Hartwell GR, Moon PC. The accuracy of theRoot ZX electronic apex locator using stainless-steel andnickel-titanium files. J Endod 2003;29:662–3.
100. Goldberg F, De Silvio AC, Manfre S, Nastri N. In vitromeasurement accuracy of an electronic apex locator in teethwith simulated apical root resorption. J Endod 2002;28:461–3.
101. Mente J, Seidel J, Buchalla W, Koch MJ. Electronic determi-nation of root canal length in primary teeth with and with-out root resorption. Int Endod J 2002;35:447–52.
102. Alves AM, Felippe MC, Felippe WT, Rocha MJ. Ex vivo evalua-tion of the capacity of the Tri Auto ZX to locate the apicalforamen during root canal retreatment. Int Endod J2005;38:718–24.
103. Kobayashi C, Yoshioka T, Suda H. A new engine-drivencanal preparation system with electronic canal measuringcapability. J Endod 1997;23:751–4.
104. Grimberg F, Banegas G, Chiacchio L, Zmener O. In vivodetermination of root canal length: a preliminary report usingthe Tri Auto ZX apex-locating handpiece. Int Endod J2002;35:590–3.
105. Meares WA, Steiman HR. The influence of sodium hypo-chlorite irrigation on the accuracy of the Root ZX electronicapex locator. J Endod 2002;28:595–8.
106. Ebrahim AK, Yoshioka T, Kobayashi C, Suda H. The effectsof file size, sodium hypochlorite and blood on the accuracyof Root ZX apex locator in enlarged root canals: an in vitrostudy. Aust Dent J 2006;51:153–7.
107. Ibarrola JL, Chapman BL, Howard JH, et al. Effect of pre-flaring on Root ZX apex locators. J Endod 1999;25:625–6.
108. Davis RD, Marshall JG, Baumgartner JC. Effect of earlycoronal flaring on working length change in curved canalsusing rotary nickel-titanium versus stainless steel instru-ments. J Endod 2002;28:438–42.
109. Nguyen HQ, Kaufman AY, Komorowski RC, Friedman S.Electronic length measurement using small and large files inenlarged canals. Int Endod J 1996;29:359–64.
110. Garofalo RR, Elias N, Dorn SO, Kuttler S. Effect of electronicapex locators on cardiac pacemaker function. J Endod2002;28:831–3.
111. Wilson BL, Broberg C, Baumgartner JC, et al. Safety ofelectronic apex locators and pulp testers in patients withimplanted cardiac pacemakers or cardioverter/defibrillators.J Endod 2006;32:847–52.
856 / Endodontics

E. LASERS IN ENDODONTICS
ADAM STABHOLZ, JOSHUA MOSHONOV, SHARONIT SAHAR-HELFT, JEAN-PAUL ROCCA
The rapid development of laser technology, as well asa better understanding of laser interaction with bio-logical tissues, has widened the spectrum of possibleapplications of lasers in endodontics. The develop-ment of new delivery systems, including thin andflexible fibers as well as new endodontic tips, hasmade it possible to apply this technology to variousendodontic procedures, including pulpal diagnosis,pulp capping/pulpotomy, cleaning and disinfectingthe root canal system, obturation of the root canalsystem, endodontic retreatment, and apical surgery.
Although interest in the clinical use of laser systemsfor endodontic procedures is increasing, there are stillsome concerns associated with their use, mainly, lackof sufficient well-designed clinical studies that clearlydemonstrate advantages of lasers over conventionalmethods and techniques. Selection of suitable wave-lengths from the various laser systems requiresadvanced training and an educated understanding ofthe different characteristics in each laser system. Thepurpose of this chapter is to describe the principles ofoperation and discuss possible clinical applications oflasers in endodontics.
Principles of Operation
Dental lasers used today for clinical procedures andresearch operate in the infrared, visible, or ultravioletrange of the electromagnetic spectrum1 (Figure 1).The word LASER is an acronym for Light Amplifica-tion by the Stimulated Emission of Radiation.Although ‘‘L’’ stands for light, the actual physicalprocess that takes place within the laser device isamplification by stimulated emission of radiation. Alight beam is composed of packets of energy known asphotons such as produced by a light bulb or otherlight sources. The natural state of an atom when all itselectrons are moving around its nucleus is the groundstate. When an atom is excited by an external energy
source, an electron moves to a higher energy level. Asthe atom tendency is to revert to its ground level, theelectron falls back to its basic orbit, while emittingenergy in the form of photons.2 This emission is called‘‘spontaneous emission’’ because it occurs withoutadditional interference and results in the formationof ‘‘individual’’ waves from each atom not in phasewith one another that is, a non-coherent, broadbandspectrum (polychromatic) light.
The laser beam, on the other hand, implies stimu-lated emission of radiation. It is a single wavelength(monochromatic), collimated (very low divergence),coherent (photons in phase), and intense.2 The laserprinciple accounts for the creation of this kind oflight: The construction of a light source based onstimulated emission of radiation requires an activemedium, a collection of atoms or molecules. Theactive medium that can be a gas, liquid, or a solidmaterial and is contained in a glass or ceramic tubehas to be excited to emit the photons by stimulatedemission. Energy in the form of electric current or aflash lamp is applied to the medium, and once thereare more atoms in the excited state than in the groundstate, a population inversion is created. By adding amirror to each end of the laser medium, a populationof photons can be directed back and forth through themedium stimulating the emission of radiation frommultiple excited electrons. Some of the photons pro-duced can be released by allowing them to passthrough one of the mirrors. The light can be coupledto a delivery device and used as a ‘‘surgical’’ beam3
(Figure 2).3
The medium producing the beam is what identifiesthe laser and distinguishes one from another. Differ-ent types of lasers used in dentistry, such as carbondioxide (CO2), erbium (Er), and neodymium (Nd),and various other substances used in the medium[e.g., yttrium, aluminum, garnet (YAG) and yttrium,scandium, gallium, garnet (YSGG)], and argon, diode,and excimer types, all produce light of a specific
857

wavelength. The CO2, the Er:YAG, the Er, Cr:YSGG,and the Nd:YAG lasers emit invisible beams in theinfrared range (10.6mm, 2.94 mm, 2.79 mm, and 1.06mm, respectively). The Argon laser emits a visible lightbeam at 488 or 514 nm, while the excimer lasers emitinvisible ultraviolet light beams at various predeter-mined wavelengths (ArF, 193 nm; KrF, 248 nm; andXeCl, -308 nm).4
Laser photons interact with tissue in one of fourways: they are transmitted through tissue, reflectedfrom tissue, scattered within tissue, or absorbed bytissue.5 Transmission of light transfers energythrough the tissue without any interaction and thusdoes not cause any effect or injury. Reflection resultsin little or no absorption, so that there is no thermaleffect on the tissue. When scattered, light travels indifferent directions and energy is absorbed over a
greater surface area, producing a less intense and lessprecise thermal effect; when absorbed, light energy isconverted into thermal energy (Figure 3).6 A singlelaser device cannot perform all the required func-tions as the beam is absorbed or reflected accordingto its wavelength and the color of the objectimpacted.3
The particular properties of each type of laser andthe specific target tissue render them suitable for var-ious procedures. The CO2 laser is highly absorbed byall biological soft and hard tissues and thus is mosteffective in tissues with high water content, such as thesoft tissues of the oral cavity. However, its high thermalabsorption makes this laser unsuitable for drilling andcutting enamel and dentin as damage to the dentalpulp may occur.7
The Er:YAG laser is the most efficient for drillingand cutting enamel and dentin as its energy is wellabsorbed by water as well as by hydroxyapatite. Argonlasers are more effective on pigmented or highly vas-cular tissues, whereas Nd:YAG laser photons aretransmitted through tissues by water and interact wellwith dark pigmented tissue.
The excimer lasers generate light in the ultravioletrange of the electromagnetic spectrum and functionby breaking molecular bonds and reducing the tissueto its atomic constituents before their energy is dis-sipated as heat. Different types of lasers may havevarious effects on the same tissue, and the same lasercan have varying effects on diverse tissue.
Unlike the CO2 and the Er:YAG lasers, theNd:YAG, argon, and excimer laser beams can bedelivered through fiber optic, allowing greater
Figure 2 Schematic diagram of a laser.
Figure 1 The wavelengths of various types of lasers according to their emission spectra.
858 / Endodontics

accessibility to different areas and structures in theoral cavity.7 The extent of the interaction of laserenergy with a tissue is generally determined by twodependent variables: the specific wavelength of thelaser emission and the optical characteristics of theparticular target tissue.5 These variables dictateabsorption (i.e., the ability to effect tissue changesand generation of heat) and are important for pulpprotection.8 The clinician controls four parameterswhen operating the laser: (1) the level of appliedpower (power density), (2) the total energy deliv-ered over a given surface area (energy density), (3)the rate and duration of the exposure (pulse repeti-tion), and (4) the mode of energy delivery to thetarget tissue (i.e., continuous versus pulsed energyand direct contact or no contact with the targettissue).
Pulpal Diagnosis
A diagnosis of pulp vitality may be, at times, difficultto assess, in view of the fact that current vitality testsare poor indicators. A false diagnosis may lead to anunnecessary removal of the pulp tissue. Histologicalevaluation of the exact state of the pulp tissue is notfeasible since an opening into the pulp chamber willresult with the need to remove this tissue and subse-
quently perform a root canal treatment. Laser Dop-pler flowmetry (LDF) was developed to assess bloodflow in micro vascular systems. It also can be used as adiagnostic system for measurements of blood flow inthe dental pulp.9,10 Laser Doppler flowmetry (LDF),is discussed in Chapter 14C.
Pulp Capping and Pulpotomy
Pulp capping, as defined by the American Associationof Endodontists,11 is a procedure in which a dentalmaterial such as calcium hydroxide Ca(OH)2 ormineral trioxide aggregate (MTA) is placed over apulpal wound to encourage the formation of repara-tive dentin. Pulpotomy entails surgical removal of thecoronal portion of the pulp as a means of preservingthe remaining radicular pulp tissues.
Pulp capping is recommended when the exposureis very small, 1.0 mm or less,12,13 and the patients areyoung; pulpotomy is recommended when the youngpulp is already exposed to caries and the roots are notyet fully formed (open apices). The traditionally usedpulp capping agent is Ca(OH)2.14,15 When it isapplied to pulp tissue, a necrotic layer is producedsubjacent to which a dentin bridge is expected toform. The same may occur when a pulpotomy proce-dure is done. The disadvantage of both techniques is
Figure 3 Four basic types of laser interactions occur when light hits the target tissue: reflection, scattering, transmission, and absorption.
Chapter 26 / Endodontics Instruments and Armamentarium / 859

that the necrotic zone may allow bacterial growth ifthe restoration permits microleakage that results inpulpal problems.
MTA shows favorable results when applied toexposed pulp. It produces more dentinal bridging in ashorter period of time with significantly less inflamma-tion than when Ca(OH)2 is used. However, 3 to 4 hoursare necessary for complete setting of the MTA.16–18
The success rate of pulp capping, whether direct orindirect, ranges from 44 to 97%. In pulpotomy, thesame agents are used until root formation has beencompleted. It is debatable whether full root canaltreatment should then be initiated.19,20 Both pulpcapping and pulpotomy are more fully discussed inChapter 35, ‘‘Vital Pulp Therapy’’ and Chapter 36,‘‘Endodontic Considerations in Dental Trauma.’’
Since the introduction of laser to dentistry, severalstudies have shown the effect of various laser deviceson dentin and pulpal tissue. While the ruby lasercaused pulpal damage, Melcer et al.21 showed that theCO2 laser produced new mineralized dentin formationwithout cellular modification of pulpal tissue whentooth cavities were irradiated in beagles and primates.Shoji et al.22 applied CO2 laser to the exposed pulps ofdogs, using a focused and defocused laser mode and awide range of energy levels (3, 10, 30, and 60 W).Charring, coagulation necrosis, and degeneration ofthe odontoblastic layer occurred, although no damagewas detected in the radicular portion of the pulp. Jukicet al.23 used CO2 and Nd:YAG lasers with an energydensity of 4 and 6.3 J/cm2, respectively, on exposedpulp tissue. In both experimental groups, carboniza-tion, necrosis, an inflammatory response, edema, andhemorrhage were observed in the pulp tissue. In somespecimens, a dentinal bridge was formed.
In patients in whom direct pulp capping treatment wasindicated, Moritz et al.24 used the CO2 laser. An energylevel of 1 W at 0.1-second exposure time with 1-secondpulse intervals was applied until the pulps exposed areaswere completely irradiated. They were then dressed withCa(OH)2 (Kerr Life, Orange, CA). In the control group,the pulps were only capped with Ca(OH)2. Symptomswere recorded and vitality tests were made after 1 weekand monthly for 1 year: 89% of the experimental grouphad no symptoms and responded normally to vitality testsversus only 68% of the control.
The importance of pulp capping that considerablyimproves the prognosis of the tooth justifies the questfor new techniques and technologies: the most recentliterature reports more predictable results (~90%)with capping performed using laser of different wave-lengths, compared to traditional procedures thatreport a success rate of approximately 60%. Laser
technology proved effective in improving the prog-nosis of pulp capping procedures on teeth affected bydeep caries pathology.25
The laser and Vitrebond (3M Espe, St. Paul, MN)direct pulp cap produce a significantly more predict-able pulp response after the first 6 months than theDycal (Dentsply International, York, PA) direct pulpcap. The survival rate of teeth treated with the laserand Vitrebond direct pulp cap is significantly greaterthan those treated with Dycal direct pulp cap overintervals of 9 to 54 months. Direct pulp capping is aworthwhile procedure that should be performed whenindicated, especially in light of the 90.3% survival rateachieved with the laser and Vitrebond direct pulp capat 54 months.26
In cases of deep and hypersensitive cavities, indirectpulp capping could be considered. A reduction in thepermeability of the dentin, achieved by sealing thedentinal tubules, is of paramount importance. Nd:YAGand 9.6 mm CO2 lasers can be used for this purpose.The 9.6 mm CO2 laser beam is well absorbed by thehydroxyapatite of enamel and dentin and causes tissueablation, melting, and re-solidification.27 The use of a9.6 mm CO2 laser did not cause any noticeable damageto the pulpal tissue in dogs.28 The effect of the Nd:YAGlaser on intrapulpal temperature was investigated byWhite et al.29 They found that the use of pulsed aNd:YAG laser, with an energy of below 1 W, a 10-Hzrepetition rate and overall 10-second exposure time, didnot significantly elevate the intrapulpal temperature.According to their results, these may be considered safeparameters, as the remaining dentinal thickness in cav-ity preparations cannot be measured in vivo. It isrecommended, therefore, that clinicians choose laserparameters lower than these safety limits.
In a study of the effects of Nd:YAG laser pulpotomyon human primary molars, it was shown that 66 outof 68 laser-treated teeth were clinically successful withno signs or symptoms of pathosis. The clinical successrate was 97% and the radiographic success rate was94.1%. In the formocresol control group (69 teeth),the clinical success was 85.5% and the radiologicalsuccess was 78.3%.30 More clinical studies arerequired to verify the advantages of the use of lasersin pulp capping and pulpotomy procedures.
Cleaning and Disinfecting the Root Canal
System
Bacterial contamination of the root canal systemis considered the principal etiologic factor for the
860 / Endodontics

development of pulpal and periapical lesions.31–33
Obtaining a root canal system free of irritants is amajor goal of root canal therapy. Biomechanicalinstrumentation of the root canal system has beensuggested to achieve this task. However, because ofthe complexity of the root canal system, it has beenshown that the complete elimination of debris andachievement of a sterile root canal system is verydifficult34,35 and that a smear layer containing bac-teria, covering the instrumented walls of the rootcanal, is formed.36–38
The smear layer consists of a superficial layer on thesurface of the root canal wall approximately 1 to 2 mmthick and a deeper layer packed into the dentinal tubulesto a depth of up to 40 mm.38 It contains inorganic andorganic substances including microorganisms and necro-tic debris.39 In addition to the possibility that the smearlayer may be infected, it can also protect the bacteriaalready present in the dentinal tubules by obstructingintra-canal disinfection agents.40 Pashley41 consideredthat a smear layer containing bacteria or bacterial pro-ducts might provide a reservoir of irritants. Thus, com-plete removal of the smear layer would be consistent withthe elimination of irritants from the root canal system.42
Peters et al.43 moreover demonstrated that 35% of thecanals’ surface area remained unchanged followinginstrumentation of the root canal prepared with fourNi-Ti preparation techniques.
Because most currently used intra-canal medica-ments have a limited anti-bacterial spectrum and alimited ability to diffuse into the dentinal tubules, ithas been suggested that newer treatment strategiesdesigned to eliminate microorganisms from the rootcanal system should be considered. These mustinclude agents that can penetrate the dentinal tubulesand destroy the microorganisms, located in areasbeyond the host defense mechanisms, where theycannot be reached by locally administered antibacter-ial agents.44
Numerous studies have documented that CO2,45
Nd:YAG,45–47 argon,45,48 Er,Cr:YAG,49 and Er:YAG50,51
laser irradiation has the ability to remove debris andsmear layer from the root canal walls followingbiomechanical instrumentation. The task of cleaningand disinfecting a root canal system that containsmicroorganisms gathered in a biofilm became verydifficult; certain bacterial species become more virulentwhen harbored in biofilm, demonstrating strongerpathogenic potential and increased resistance toantimicrobial agents as biofilm has the ability to pre-vent the entry and action of such agents.52
Bergman et al.53 tried to define the role of laser as adisinfection tool by using Nd:YAG laser irradiation on
some endodontic pathogens ex vivo. They concludedthat Nd:YAG laser irradiation is not an alternative buta possible supplement to existing protocols for canaldisinfections, as the properties of laser light may allowa bactericidal effect beyond 1 mm of dentin. Endo-dontic pathogens that grow as biofilms are difficult toeradicate even upon direct laser exposure.
However, there are several limitations that may beassociated with the intra-canal use of lasers that cannotbe overlooked.54 The emission of laser energy from thetip of the optical fiber or the laser guide is directedvertically along the root canal and not necessary later-ally to the root canal walls.55 Thus, it is almost impos-sible to obtain uniform coverage of the canal surfaceusing a laser.54,55 Furthermore, thermal damage to theperiapical tissues is potentially possible, so safety of theprocedures must always be considered.55 Direct emis-sion of laser irradiation from the tip of the opticalfiber in the vicinity of the apical foramen of a toothmay result in transmission of the irradiation beyondthe foramen into periapical tissues. This, in turn, mayalso be hazardous in teeth in close proximity to themental foramen or to the mandibular nerve.55 In theirreview, Lasers in Endodontics, Matsumoto et al.56
emphasized the possible limitations of the use of lasersin the root canal system. They suggested that ‘‘removalof smear layer and debris by laser is possible, howeverit is difficult to clean all root canal walls, because thelaser beam is emitted straight ahead, making it almostimpossible to irradiate the lateral canal walls.’’ Theystrongly recommended improving the endodontic tipto enable irradiation of all areas of the root canal walls.The Er:YAG laser has gained increasing popularityamong clinicians following its approval by the USFood and Drug Administration for use on dental hardtissues.57
Stabholz et al.55 recently reported the developmentof a new endodontic tip to be used with an Er:YAGlaser system. The beam of the Er:YAG laser is deliv-ered through a hollow tube, with an endodontic tipthat allows lateral emission of the irradiation (side-firing), rather than direct emission through a singleopening at its far end. This new endodontic side-firing spiral tip was designed to fit the shape and thevolume of root canals prepared by Ni-Ti rotaryinstrumentation. It emits the Er:YAG laser irradiationlaterally to the walls of the root canal through a spiralslit located all along the tip. The tip is sealed at its farend, preventing the transmission of irradiation to andthrough the apical foramen of the tooth (Figures 4and 5).
The efficacy of the endodontic1 side-firing spiral tip,in removing debris and smear layer from distal and
Chapter 26 / Endodontics Instruments and Armamentarium / 861

palatal root canals of freshly extracted human molars,was examined. Scanning electron microscopy (SEM) ofthe lased root canal walls revealed clean surfaces, free ofsmear layer and debris.55 The dentinal tubules in theroot run a relatively straight course between the pulpand the periphery, in contrast to the typical S-shapedcontours of the tubules in the tooth crown.41 Studieshave shown that bacteria and their byproducts, presentin infected root canals, may invade the dentinaltubules. Their presence in the tubules of infectedteeth, at junction, was also reported.58,59 These findings
justify the rationale and need for developing effectivemeans of removing the smear layer from root canalwalls following biomechanical instrumentation. Thiswould allow disinfectants and laser irradiation to reachand destroy microorganisms harbored in the dentinaltubules.
In various laser systems used in dentistry, theemitted energy can be delivered into the root canalsystem by a either thin optical fiber (Nd:YAG,KTP-Nd:YAG, Er;YSGG, argon, and diode) or by ahollow tube (CO2 and Er:YAG). Thus, the potential
B
C
A
Figure 4 An 18-year-old patient came to the endodontic clinic complaining about a bad taste in her mouth and a lesion on the gums in the anterior areaof the mouth. The clinical examination revealed a sinus tract opening close to the apex of the maxillary right lateral incisor. A, The radiograph showed anarea of internal resorption and a large radiolucent area around the root apex. A diagnostic/length measurement radiograph suggested the presence ofroot perforation associated with the internal resorption. The patient was given the option of root canal treatment with poor prognosis, or replacing thetooth with an implant. The patient chose endodontic treatment. B, After cleaning and shaping the canal, Ca(OH)2 was placed and replaced after 3months. After 6 months, the sinus tract was still present with no sign of healing. C, The patient was offered the opportunity to have the tooth treatedwith the newly developed prototype of the RCLase Side Firing Spiral Tip that might provide better disinfection of the root canal system. The pictureshows the RCLase tip positioned in the contra angle (left) and the radiograph shows the tip inside the root canal. D, Radiograph shows the lateral incisorfollowing completion of the root canal filling using warm gutta-percha technique. E, A two-year follow-up radiograph shows complete healing of theperiapical lesion. The sinus tract had disappeared and the patient was free of symptoms.
862 / Endodontics

A B
C
D
Figure 5 A, Radiograph of a 42-year-old male patient with a suspected vertical root fracture on the second mandibular right molar. The tooth had beenrestored 12 years earlier after root canal therapy. He reported several episodes of pain and swelling during the past several years. B, At the firstappointment, the leaky restoration and the screw post were removed, the distal root canal was thoroughly cleaned and irrigated using sodiumhypochlorite, and Ca(OH)2 dressing was placed. C, On a later appointment, the canal was treated with the prototype of the RCLase Side Firing Spiral Tip.D, The endodontic treatment was completed 6 months later (May 2003). Follow-up radiographs that were taken 1, 2 and 4 years after the completion ofthe endodontic treatment show complete healing of the periapical lesion.
Chapter 26 / Endodontics Instruments and Armamentarium / 863

bactericidal effect of laser irradiation can be effectivelyutilized for additional cleansing and disinfecting ofthe root canal system following biomechanical instru-mentation. This effect was extensively studied usinglasers such as CO2,60,61 Nd:YAG,62–65 KTP-Nd:YAG,66
excimer,67,68 diode,69 and Er:YAG.70–72
The emerging consensus is that laser irradiationemitted from laser systems adapted to dentistry hasthe potential to kill microorganisms. In most cases,the effect is directly related to the amount of irradia-tion and to its energy level.
Obturation of the Root Canal System
The purpose of obturating the prepared root canalspace is twofold: (1) to eliminate all avenues of leak-age from the oral cavity or from the periapical tissuesand (2) to seal within the system any irritants thatcannot be fully removed during the cleaning andshaping procedures.73 The rationale in introducinglaser technology to assist in obturating the root canalsystem is based on two major assumptions: the abilityto use the laser irradiation as a heat source for soft-ening the gutta-percha to be used as obturating mate-rial and for conditioning the dentinal walls beforeplacing an obturating bonding material.
The concept of thermoplasticized compaction is notnew and covers any technique based entirely on heatsoftening gutta-percha combined primarily with verticalcompaction. The pioneering technique using verticalcompaction of warm gutta-percha was described 40 yearsago by Schilder74 as a way to fill canals in all dimensionsand is an example of thermoplasticized compaction.
The first laser-assisted root canal filling procedureinvolved using the wavelength of Argon 488 nm laser.This wavelength that can be transmitted through dentinwas used to polymerize a resin that was placed in themain root canal. The ability of this biomaterial topenetrate into accessory root canals was tested and itwas shown that the resin in the lateral canals was readilypolymerized at low energy levels (30m W). Further useof this wavelength became irrelevant due to its unsui-table properties in other dental procedures.75
Anic and Matsumoto76 were the first to comparedifferent root canal filling techniques for single-rootedteeth. Lateral condensation, vertical condensation,low-temperature gutta-percha (Ultrafil, Coltene/Wha-ledent, New York, NY), and laser-cured resin withdifferent wavelengths (Argon, CO2, and Nd-YAG)were the techniques used. The apical sealing abilityachieved by the various filling techniques was com-pared by measuring the apical dye penetration follow-ing placement of the samples in a 1% solution of
methylene blue. Gutta-percha softened with Argonlaser created an apical seal similar to that obtainedwith lateral condensation and Ultrafil techniques.
Maden et al.77 used the dye penetration method tomeasure apical leakage by comparing lateral conden-sation, System B technique, and Nd-YAG softenedgutta-percha. No statistically significant differenceswere reported. In another study, Anic and Matsu-moto78 demonstrated that the temperature elevationinduced on the outer root surface when Nd-YAG andArgon lasers were used ranged from 12.9
�C (Argon
laser) to 14.4�C (Nd-YAG laser). Such an increase in
temperature may be detrimental to the tissues of theattachment apparatus of the teeth. The implication ofsuch methodologies remains questionable.
In order to examine whether laser irradiationimproves the adhesion of endodontic materials tothe dentinal walls and thus reduce apical leakage, Parket al.79 used different sealers and two root canal fillingtechniques. Using an Nd-YAG laser irradiation at theend of the root canal preparation (5 W, 20 Hz), theyconcluded that Nd-YAG irradiation reduced apicalleakage regardless of the sealer or the technique used.
Kimura et al.80 used Er-YAG laser (170 to 250 mJ, 2Hz) and showed that irradiation of the root canal did notaffect apical leakage following obturation when comparedwith conventional methods. They later demonstrated thatthe use of Nd-YAG laser was useful for the reduction ofapical leakage.81 Because Nd:YAG laser irradiation is verywell absorbed by black color, an absorbent paper pointsoaked with black ink was introduced to working lengthand the apical root canal walls were painted.81
Significant improvement in the quality of the apicalsealing of root canals was reported by Gekelman et al.82
who used an Nd:YAG laser (100 mJ/pulse, 1 W,10 Hz). It has also been demonstrated that applicationof Er-YAG laser beam (200 mJ, 4 Hz) for 60 secondsenhanced the adhesion of epoxy resin-based sealers incomparison with zinc oxide–eugenol-based root canalsealers.83
The clinical evidence from reported studies con-cerning the use of lasers to assist in obturating rootcanals is currently not sufficient. For example, it hasnot been determined whether the use of an opticalfiber as a heat source to soften gutta-percha is safe forthe surrounding structures of the tooth. It is also notclear if the softening of gutta-percha is homogeneousin all parts of the filling when vertical condensationtechniques were described.84 The significant role ofendodontic sealers, when warm gutta-percha comp-action techniques are employed, has been clearlydemonstrated.85 It is recognized that root canal sealersaffect the quality of the apical seal of vertically
864 / Endodontics

condensed gutta-percha and that without a sealer sig-nificantly more apical leakage occurs.
Some questions remain concerning the effectivenessof lasers contributing to the obturating procedures ofroot canals: what is the most suitable wavelength andwhat are adequate parameters? These areas should beexplored and assessed.
Endodontic Retreatment
Endodontic failures can be attributed to inadequacies incleaning, shaping, and obturation, iatrogenic events, orre-infection of the root canal system. Regardless of theinitial cause, the sum of causes is bacterial contamina-tion. The objective of non-surgical retreatment is toeliminate from the root canal space sources ofirritation to the attachment apparatus.86 Some of thesefailures may be managed by endodontic retreatment,proven to be effective in eliminating clinical and radio-graphic signs of pathosis. A variety of techniques havebeen described to remove deficient root canal filling and/or metallic obstructions that may lead to undesirableresults87 (see Chapter 31 ‘‘Retreatment of Non-HealingEndodontic Therapy and Management of Mishaps’’)
The rationale for using laser irradiation in non-surgicalretreatment may be ascribed to the need to remove foreignmaterial from the root canal system that may otherwise bedifficult to remove by conventional methods. Farge et al.88
examined the efficacy of the Nd-YAP laser (1340 nm) inroot canal retreatment (200 mJ and a frequency of 10 Hz).They attempted to remove gutta-percha and zincoxide–eugenol sealer previously placed. In addition, theyalso reported an attempt to remove silver cones andbroken instruments. They concluded that using laserradiation alone would not completely remove debrisand obturating materials from the root canal.
Yu et al.89 used an Nd-YAG laser at three outputpowers (1, 2, 3 W) to remove gutta-percha and brokenfiles from root canals. They were able to remove fillingmaterial in more than 70% of the samples while brokenfiles were removed 55% of the time.
Anjo et al.90 reported that the time required forremoval of any root canal-filling materials using laserablation was significantly shorter than that requiredusing conventional methods. It appeared that followinglaser irradiation, some orifices of dentinal tubules wereblocked with melted dentin. They concluded thatNd:YAG laser irradiation is an effective technique forremoval of root canal-filling materials and may offeradvantages over conventional methods.
The efficacy of the Er-YAG laser in removing zincoxide sealers and phenoplastic resins has also been stu-died.91 In straight root canals, laser irradiation with
250 mJ/pulse and 10 Hz frequency was useful in elim-inating zinc oxide sealers.
Hand instruments without the use of any specificsolvent were also used. In curved root canals, how-ever, the procedure had to be stopped because of therisk of lateral root perforation. Under the sameexperimental conditions when laser irradiation wasdelivered to remove phenoplastic resins, ledging ofthe root canal occurred and it was not possible toreturn to the previously established working length.
A clinical advantage that should be further explored isthe possibility of eliminating the use of toxic solventswhen removing semi-solid materials from root canals.Although it was shown89–92 that root canal-filling materi-als can be removed from the root canal using lasers, suchas the Nd:YAG and the Er:YAG, the decisive advantage inusing lasers for this purpose still remains to be confirmed.
Apical Surgery
Surgical endodontic therapy is indicated when teethhave responded poorly to conventional treatment orwhen they cannot be treated appropriately by non-surgical means. The goal of endodontic surgery is toeliminate the disease and prevent its recurrence.93 Sur-gical options should be considered only when betterresults cannot be achieved by non-surgical treatment.94,95
Egress of irritants from the root canal system into theperiapical tissues is considered the main cause of failurefollowing apicoectomy and apical filling. The irritantspenetrate mainly through gaps between the filling andthe dentin.96 A second possible pathway for irritants toegress into the periapical tissues is through dentinaltubules on the cut root surface. It has been shown thatthe dentin of apically resected roots is more permeableto fluids than the dentin of non-resected roots.97
The first attempt to use a laser in endodontic surgerywas performed by Dr. Weichman at the University ofSouthern California (at the suggestion of Dr. Ingle). Heattempted to seal the apical foramina of extracted teethfrom which the pulps had been extirpated.98 The apicesof those specimens were irradiated using a high powerCO2 laser. Melting of the cementum and dentin wasobserved with a ‘‘cap’’ formation that could, however,be easily removed.
Miserendino99 used a CO2 laser to irradiate the apexof a tooth during apicoectomy. He described theadvantages associated with laser application for peria-pical surgery such as improved hemostasis and con-current visualization of the operative field. He alsoemphasized the potential sterilizing effect of the con-taminated root apex as well as the reduction inpermeability of the root surface dentin. Moreover, he
Chapter 26 / Endodontics Instruments and Armamentarium / 865

described re-crystallization of the apical root dentinthat appeared to be smooth and suitable for placementof an apical filling material. Duclos et al.100 used a CO2
laser to perform apicoectomies in patients and advo-cated the use of a mini contra-angle head for efficientdelivery of the laser irradiation at a 90� angle to theroot apexes of teeth in the posterior areas.
However, unfavorable results of an in vivo study ondogs where the success rate following apicoectomiesusing the CO2 laser was not improved have failed tosupport the rationale previously described by Miseren-dino.99 A prospective study of two apical preparationswith and without CO2 laser, in which 320 cases wereevaluated, did not show that CO2 laser use improvedthe healing process.102 In vitro studies103–106 withNd:YAG lasers have shown a reduction in penetrationof dye or bacteria through resected roots. It was sug-gested that the reduced permeability in the lased speci-mens was probably the result of structural changes inthe dentin following laser application.104 AlthoughSEM examination showed melting, solidification, andre-crystallization of the hard tissue, the structuralchanges were not uniform and the melted areasappeared connected by areas that looked like those inthe non-lased specimens. It was postulated that this wasthe reason why the permeability of the dentin wasreduced, but not completely eliminated. It is reasonableto assume that homogenously glazed surfaces would beless permeable than partially glazed ones.
Ebihara et al.107 used Er:YAG laser for apical cavitypreparations of extracted teeth. They found no signifi-cant difference in dye penetration between the laser-treated groups and those in which ultrasonic tips wereused. These results were not surprising as the Er:YAGlaser neither melts nor seals the dentinal tubules; there-fore, any reduction in dentin permeability should notbe expected. A different result was obtained by Gouw-Soares et al.108 who evaluated the marginal permeabilityin teeth after apicoectomy and apical dentin surfacetreatment using two different lasers (Er:YAG and9.6 mm TEA CO2). Both laser systems showed a reduc-tion of permeability to methylene blue dye.
Recently it has been reported that when using anEr:YAG laser in a low output power in apical surgery,it was possible to resect the apex of extracted teeth.Smooth and clean resected surfaces devoid of charringwere observed.109,110 It was also found that althoughthe cutting speed of the Er:YAG laser was slightlyslower than conventional high-speed burs, absenceof discomfort and vibration and less chance for con-tamination at the surgical site, as well as reduced riskof trauma to adjacent tissues may compensate for theadditional time required.111
In a 3-year clinical study, Gouw-Soares et al.112
reported a new protocol for use in apical surgery. AnEr-YAG laser was used for osteotomy and root resec-tion, whereas the Nd:YAG laser irradiation served toseal the dentinal tubules to reduce possible bacterialcontamination of the surgical cavity. Improvement inhealing was achieved by the use of a LILT Ga-Al-Asdiode laser. The radiographic follow-up showed signif-icant decrease in the radiolucent periapical areas withno adverse clinical signs and symptoms.112
The preparation of apical cavities by Er:YAG laser andultrasonics was also studied by Karlovic et al.113 Theyfound lower values of microleakage when the root endcavities were prepared with the Er:YAG laser irrespectiveof the material used to seal those cavities.
It has been suggested that after the appropriate wave-length to melt the hard tissues of the tooth has beenestablished, the main contribution of laser technology tosurgical endodontics is to convert the apical dentin andcementum structure into a uniformly glazed area thatdoes not allow egress of microorganisms through dent-inal tubules and other openings in the apex of the tooth.Hemostasis and sterilization of the contaminated rootapex will have an additional significant input.114
References
1. Coluzzi DJ. An overview of laser wavelengths used in den-tistry. Den Clin N Am 2000;44:753–65.
2. Harris DM, Pick RM. Laser physics. In: Miserendino LJ and PickRM. Lasers in dentistry. Chicago: Quintessence; 1995.
3. Nelson SJ, Berns MW. Basic laser physics and tissue inter-actions. Contemp Dermatol 1982;2:1–15.
4. Sulewski JG. Historical survey of laser dentistry. Dent Clin NAm 2000;44:717–52.
5. Dederich DN. Laser tissue interaction. Alpha Omegan1991;84:33–6.
6. Miserendino LJ, Levy G, Miserendino CA. Laser interactionwith biologic tissues. In: Miserendino LJ and Pick RM.Lasers in dentistry. Chicago: Quintessence, 1995.
7. Goodis HE, Pashley D, Stabholz A. Pulpal effects of thermal andmechanical irritants In: Hargreaves KM, Goodies HE. Seltzer’sand Bender’s Dental Pulp. Chicago: Quintessence; 2002.
8. Arcoria CJ, Miserendino LJ. Laser effects on the dental pulp.In: Miserendino LJ, Pick RM. Lasers in dentistry. Chicago:Quintessence; 1995.
9. Kimura Y, Wilder-Smith P, Matsumoto K. Lasers in endo-dontics: a review. Int Endod J 2000;33:173–85.
10. Cohen S, Liewehr F. Diagnostic procedures. In: Cohen S, BurnsRC. Pathways of the pulp. 8th ed. St. Louis:Mosby; 2002.
866 / Endodontics

11. American Asoociation of Endodontics. Glossary of endo-dontic terms. 7th ed. AAE, Chicago,IL 2003.
12. Isermann GT, Kaminski EJ. Pulpal response to minimal expo-sure in presence of bacteria and Dycal. J Endod 1979;5:322–7.
13. Cvek M, Cleaton-Jones PE, Austin JC, et al. Pulp reaction toexposure after experimental crown fractures or grinding inadult monkeys. J Endod 1982;8:391–7.
14. Cvek M: Endodontic treatment of traumatized teeth. In:Andreasen JO. Traumatic injuries of the teeth, 2nd ed.Philadelphia:WB Saunders; 1981.
15. Seltzer S, Bender IB. Pulp capping and pulpotomy. In: SeltzerS, Bender IB. The dental pulp, biologic considerations indental procedures. 2nd ed. Philadelphia: JB Lippincott;1975.
16. Torabinejad M, Chivian N. Clinical applications of mineraltrioxide aggregate. J Endod 1999;25:197–20.
17. Pitt-Ford TR, Torabinejad M, Abedi HR. Mineral trioxideaggregate as a pulp capping material. J Am Dent Assoc1996;27:1491.
18. Myers K, Kaminski E, Lautenschlager EP. The effect of mineraltrioxide aggregate on the dog pulp. J Endod 1996;22:198–202.
19. Klein H, Fuks A, Eidelman E, et al. Partial pulpotomyfollowing complicated crown fracture in permanent incisors:a clinical and radiographical study. J Pedod 1985;9(2):142–7.
20. Fuks AB, Chosack A, Klein H, et al. Partial pulpotomy as atreatment alternative for exposed pulps in crown-fracturedpermanent incisors. Endod Dent Traumatol 1987;3:100–102.
21. Melcer J, Chaumate MT, Melcer F, et al. Preliminary report ofthe effect of CO2 laser beam on the dental pulp of the MacacaMulatta primate and the beagle dog. J Endod 1985;11:1–5.
22. Shoji S, Nakamura M, Horiuchi H. Histopathological changesin dental pulps irradiated by CO2 laser: a preliminary reporton laser pulpotomy. J Endod 1985;11:379–84.
23. Jukic S, Anic I, Koba K. The effect of pulpotomy using CO2
and Nd:YAG lasers on dental pulp tissue. Int Endod J1977;30:175–188.
24. Moritz A, Schoop U, Goharkhay K. The CO2 laser as an aidin direct pulp capping. J Endod 1998;24:248–51.
25. Olivi G, Genovese MD, Maturo P, Docimo R. Pulp capping:advantages of using laser technology. Eur J Peadiatr Dent2007;8:89–95.
26. Santucci PJ. Dycal versus Nd:YAG laser and Vitrebond fordirect pulp capping in permanent teeth. J Clinc Laser MedSurg. 1999;17:69–75.
27. Fried D, Glena RE, Featherstone JD, et al. Permanent andtransient changes in the reflectance of CO2 laser-irradiateddental hard tissues at lambda = 9.3, 9.6, 10.3, and 10.6microns and at fluences of 1-20 J/cm2. Lasers Surg Med1997;20:22–31.
28. Wigdor HA, Walsh JT Jr. Histologic analysis of the effect ondental pulp of a 9.6-microm CO2 laser. Laser Surg Med2002;30:261–6.
29. White JM, Fagan MC, Goodis HE. Intrapulpal temperaturesduring pulsed Nd:YAG laser treatment, in vitro. J Period-ontol 1994;65:255–9.
30. Jeng-fen Liu. Effects of Nd:YAG laser pulpotomyon humanprimary molars. J Endod 2006;32:404–7.
31. Kakehashi S, Stanley HR, Fitzgerald RJ. The effect of surgicalexposures of dental pulps in germ-free and conventionallaboratory rats. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1965;20:340–9.
32. Bergenholz G. Microorganisms from necrotic pulps of trau-matized teeth. Odontol Revy 1974;25:347–58.
33. Moller AJ, Fabricius L, Dahlen G, et al. Influenceon periapical tissues of indigenous oral bacteria and necroticpulp tissue in monkeys. Scand J Dent Res 1981;89:475–84.
34. Bystrom A, Sundquist G. Bacteriologic evaluation of theefficacy of mechanical root canal instrumentation in endo-dontic therapy. Scand J Dent Res 1981;89:321–8.
35. Sjogren U, Hagglund B, Sundquist G, et al. Factors affectingthe long-term results of endodontic treatment. J. Endod1990;16:498–504.
36. McComb D, Smith DC. A preliminary scanning electronmicroscope study of root canals after endodontic proce-dures. J Endod 1975;1:238–42.
37. Moodnik RM, Dorn SO, Feldman MJ, et al. Efficacy ofbiomechanical instrumentation; a scanning electron micro-scopy study. J Endod 1976;2:261–6.
38. Mader CL, Baumgartner JC, Peters DD. Scanning electronmicroscopic investigation of the smeared layer on root canalwalls. J Endod 1984;10:477–83.
39. Torabinejad M, Handysides R, Khademi AA, et al. Clinicalimplications of the smear layer in endodontics: A review.Oral Surg Oral Med Oral Pathol Oral Radiol Endod2002;94:658–66.
40. Haapasalo M, Orstavik D. In vitro infection and disinfectionof dentinal tubules. J Dent Res 1986;66:1375–9.
41. Pashley DH. Smear layer physiological considerations. OperDent (Suppl) 1984;3:13–29.
42. Drake DR, Wiemann AH, Rivera EM, et al. Bacterial reten-tion in canal walls in vitro: effect of smear layer. J Endod1994;20:78–82.
43. Peters OA, Schonenberger K, Laib A. Effects of four Ni-Tipreparation techniques on root canal geometry assessedby micro computed tomography. Int Endod J 2001;34:221–30.
44. Oguntebi BR. Dentin tubule infection and endodontic ther-apy implications. Int Endod J 1994;27:218–22.
45. Anic I, Tachibana H, Matsumoto K, et al. Permeability,morphologic and temperature changes of canal dentin wallsinduced by Nd:YAG, CO2 and argon lasers. Int Endod J1996; 29:13–22.
46. Harashima T, Takeda FH, Kimura, et al. Effect of Nd:YAGlaser irradiation for removal of intracanal debris and smear
Chapter 26 / Endodontics Instruments and Armamentarium / 867

layer in extracted human teeth. J Clin Laser Med Surg1997;15:131–5.
47. Saunders WP, Whitters CJ, Strang R, et al. The effect ofan Nd:YAG pulsed laser on the cleaning of the root canaland the formation of a fused apical plug. Int Endod J1995;28:213–20.
48. Moshonov J, Sion A, Kasirer J, et al. Efficacy of argon laserirradiation in removing intracanal debris. Oral Surg OralMed Oral Pathol Oral Radiol Endod 79;1995:221–5.
49. Yamazaki R, Goya C, Yu DG, et al. Effect of Erbium, Chro-mium:YSGG laser irradiation on root canal walls: A scanningelectron microscopic and thermographic study. J Endod2001;27:9–12.
50. Takeda FH, Harashima T, Kimura Y, et al. Efficacy ofEr:YAG laser irradiation in removing debris and smear layeron root canal walls. J Endod 1998;24:548–51.
51. Kimura Y, Yonaga K, Yokoyama K, et al. Root surfacetemperature increase during Er:YAG laser irradiation of rootcanals. J Endod 2002;28:76–8.
52. Svenstater G, Bergenholz G. Biofilms in endodontic infec-tions. Endod Topics 2004; 9:27–36.
53. Bergmans L, Moisiadis P, Teughels W, et al. Bactericidaleffects of Nd:YAG laser irradiation on some endodonticpathogens ex vivo. Int Endodo J 2006;39:547.
54. Goodis HE, Pashley D, Stabholz A. Pulpal effects of thermaland mechanical irritants. In: Hargreaves KM, Goodis HE.Seltzer and Bender’s dental pulp. Carol Stream IL: Quintes-sence publishing 2002.
55. Stabholz A, Zeltzser R, Sela M, et al. The use of lasers indentistry: principles of operation and clinical applications.Compend 2003;24:811–24.
56. Matsumoto K. Lasers in endodontics. Dent Clin of NorthAm 2000;44:889–906.
57. Cozean C, Arcoria CJ, Pelagalli J, et al. Dentistry for the 21st
century? Erbium:YAG laser for teeth. J Am Dent Assoc1997;128:1080–7.
58. Ando N, Hoshino E. Predominant obligate anaerobes invad-ing the deep layers of root canal dentine. Int Endod J1990;23:20–7.
59. Armitage GC, Ryder MI, Wilcox SE. Cemental changes inteeth with heavily infected root canals. J Endod1983;9:127–30.
60. Zakariasen KL, Dederich DN, Tulip J, et al. Bactericidalaction of carbon dioxide laser radiation in experimental rootcanals. Can J Microbiol 1986;32:942–6.
61. Le Goff A, Morazin-Dautel A, Guigand M, et al. An evalua-tion of the CO2 laser for endodontic disinfection. J Endod1999;25:105–8.
62. Moshonov J, Orstavik D, Yamauchi S, et al. Nd:YAG laserirradiation in root canal disinfection. Endod Dent Trauma-tol 1995;11:220–4.
63. Fegan SE, Steiman HR. Comparative evaluation of the anti-bacterial effects of intracanal Nd:YAG laser irradiation: Anin vitro study. J Endod 1995;21:415–7.
64. Rooney J, Midda M, Leeming J. A laboratory investigationof the bactericidal effect of Nd:YAG laser. Br Dent J1994;176:61–4.
65. Gutknecht N, Moritz A, Conrads G. Bactericidal effect of theNd:YAG laser in in vitro root canals. J Clin Laser Med Surg1996;14:77–80.
66. Nammour S, Kowaly k, Powell L, et al. External temperatureduring KTP-Nd:YAG laser irradiation in root canals: an in-vitro study. Lasers Med Science 2004;19:27–32.
67. Stabholz A, Kettering J, Neev J, et al. Effects of XeCl excimerlaser on Streptococcus mutans. J Endod 1993;19:232–5.
68. Folwaczny M, Liesenhoff T, Lehn N, et al. Bactericidal actionof 308nm excimer-laser radiation: An in vitro investigation.J Endod 1998;24:781–5.
69. Gutknecht N, Alt T, Slaus G, et al. A clinical comparison ofthe Bactericidal effect of the diode laser and a 5% sodiumhypochlorite in necrotic root canals J Oral Laser Applica-tions 2002;2:151–7.
70. Mehl A, Folwaczny M, Haffner C, et al. Bactericidal effects of2.94m Er:YAG laser irradiation in dental root canals. J Endod1999;25:490–3.
71. Dostalova T, Jelinkova H, Housova D, et al. Endodontictreatment with application of Er:YAG laser waveguide radia-tion disinfection. J Clin Laser Med Surg 2002;20:135–9.
72. Schoop U, Moritz A, Kluger W, et al. The Er;YAG laser inendodontics: results of an in vitro study. Lasers Surg Med2002;30:360–4.
73. Gutmann JL, Whitherspoon DE. Obturation of the cleanedand shaped root canal system. In: Cohen S, Burns RC. Path-ways of the pulp 8th ed. St. Louis MO: Mosby;2002.
74. Schilder H. Filling root canals in three dimensions. DentClin North Am 1967;11:723–9.
75. Potts TV, Petrou A. Laser photopolymerization of dentalmaterials with potential endodontic applications. J Endod1990;16:265–8.
76. Anic I, Matsumoto K. Comparison of the sealing ability oflaser softened, laterally condensed and low-temperaturethermoplasticized gutta-percha. J Endod 1995;21:464–9.
77. Maden M, Gurgul G, Tinaz AC. Evaluation of apical leakageof root canals obturated with Nd:YAG laser-softened gutta-percha, System-B, and lateral condensation techniques.Contemp Dent Pract 2002;15:16–26.
78. Anic I, Matsumoto K. Dentinal heat transmission inducedby a laser-softened gutta-percha obturation technique.J Endod. 1995;21:470–4.
79. Park DS, Yoo HM, Oh TS. Effect of Nd:YAG laser irradia-tion on the apical leakage of obturated root canals: anelectrochemical study. Int Endod J 2001;4:318–21.
868 / Endodontics

80. Kimura Y, Yonaga K, Yokoyama K, et al. Apical leakage ofobturated canals prepared by Er:YAG laser. J Endod2001;27:567–70.
81. Kimura Y, Yamazaki R, Goya C, et al. A comparative studyon the effects of three types of laser irradiation at the apicalstop and apical leakage after obturation. J Clin Laser MedSurg 1999;17:261–6.
82. Gekelman D, Prokopowitsch I, Eduardo CP. In vitro study ofthe effects of Nd:YAG laser irradiation on the apical sealing ofendodontic fillings performed with and without dentin plugs.J Clin Laser Med Surg 2002;20:117–21.
83. Sousa-Neto MD, Marchesan MA, Pecora JD,et al. Effect ofEr:YAG laser on adhesion of root canal sealers. J Endod.2002;28:185–7.
84. Blum JY, Parahy E, Machtou P. Warm vertical compactionsequences in relation to gutta-percha temperature. J Endod1997;23:307–11.
85. Yared GM, Bou Dagher F. Sealing ability of the verticalcondensation with different root canal sealers. J Endod1996;21:6–8.
86. Ruddle CJ. Non surgical endodontic retreatment. In: CohenS, Burns RC. Pathways of the pulp. 8th ed. St. Louis MO:Mosby;2002.
87. Hulssman R. Methods for removing metal obstructionsfrom the root canal. Endod Dent Traumatol 1983;9:223–23.
88. Farge P, Nahas P, Bonin P. In vitro study of a Nd-YAP laserin endodontic retreatment. J Endod 1998;42:359–3.
89. Yu DG, Kimura Y, Tomita Y, et al. Study on removal effectsof filling materials and broken files from root canals usingpulsed Nd:YAG laser. J Clin Laser Med Surg 2000;18:23–8.
90. Anjo T, Ebihara A, Takeda A, et al. Removal of two types ofroot canal filling material using pulsed Nd-YAG laser irra-diation. Photomed Laser Surg 2004;22:470–6.
91. Warembourg P, Rocca JP, Bertrand MF: Efficacy of anEr:YAG laser to remove endodontic pastes. An in vitro.J Oral Laser Appl 2001;1:43–7.
92. Viducic D, Jukic S, Karlovic Z, et al. Removal of gutta-perchausing an Nd-YAG laser. Int Endod J 2003;36:670–3.
93. Carr GB. Surgical endodontics. In: Cohen S, Burns RC.Pathways of the pulp. 6th ed. St. Louis MO: Mosby;1994.
94. Gutmann JL. Principles of endodontic surgery for the gen-eral practitioner. Dent Clin North Am 1984;28:895–908.
95. Leubke RG. Surgical endodontics. Dent Clin North Am1974;18:379.
96. Stabholz A, Shani J, Friedman S, et al. Marginal adaptationof retrograde fillings and its correlation with sealability.J Endod 1985;11:218–23.
97. Ichesco E, Ellison R, Corcoran J. A spectrophotometricanalysis of dentinal leakage in the resected root [Abstract].J Endod 1986;12:129.
98. Weichman JA, Johnson FM. Laser use in endodontics. Apreliminary investigation. Oral Surg Oral Med Oral PatholOral Radiol Endod 1971;31:416–20.
99. Miserendino LL. The laser apicoectomy: endodonticapplication of CO2 laser for periapical surgery. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1988;66:615–9.
100. Duclos P, Behlert V, Lenz P. New technique of surgicaltreatment of periapical lesions using carbon dioxide laser.Rev. Odontostomatol 1990;19:143–50.
101. Friedman S, Rotstein I, Mahamid A. In vivo efficacy ofvarious retrofills and of CO2 laser in apical surgery. Endo-don Dent Traumatol 1991;7:19–25.
102. Bader G, Lejeune S. Prospective study of two retrogradeendodontic apical preparations with and without the use ofCO2 laser. Endod Dent Traumatol 1998;14:75–8.
103. Stabholz A, Khayat A, Ravanshad SH, et al. Effects ofNd:YAG laser on apical seal of teeth after apicoectomy andretrofill. J Endod 1992;18:371–5.
104. Stabholz A, Khayat A, Weeks DA, et al. Scanning electronmicroscopic study of the apical dentine surfaces lased withNd:YAG laser following apicectomy and retrofill. Int Endod J1992;25:288–91.
105. Arens DL, Levy GC, Rizoiu IM. A comparison of dentinpermeability after bur and laser apicoectomies. Compen-dium 1993;14:1290–7.
106. Wong WS, Rosenberg PA, Boylan RJ, et al. A comparison ofthe apical seals achieved using retrograde amalgam fillings andthe Nd:YAG laser. J Endod 1994;20:595–7.
107. Ebihara A, Wadachi, Sekine Y, et al. Application of Er:YAGlaser to retrograde cavity preparation. J Japan Soci LaserDent 1998;9:23–31.
108. Gouw-Soares S, Stabholz A, Lage-Marques JL, et al. Compara-tive study of dentine permeability after apicectomy and surfacetreatment with 9.6 micrometer TEA CO2 and Er:YAG laserirradiation. J Clin Laser Med Surg 2004;22:129–39.
109. Paghdiwala AF. Root resection of endodontically treatedteeth by Er:YAG laser radiation. J Endod 1993;19:91–4.
110. Komori T, Yokoyama K, Matsumoto Y, Matsumoto K.Er:YAG and Ho:YAG laser root resection of extractedhuman teeth. J Clin Laser Med Surg 1997;15:9–3.
111. Komori T, Yokoyama K, Takato T, Matsumoto K. Clinicalapplication of the Er:YAG laser for apicoectomy. J Endod1997;23:748–50.
112. Gouw-Soares S, Tanji E, Haypek P, et al. The use ofEr:YAG, Nd:YAG and Ga-Al-As. Lasers in periapicalsurgery: a three year clinical study. J Clin Surg Med2001;19:193–8.
113. Karlovic Z, Pezelj-Ribaric S, Miletic I, et al. Er-YAG laserversus ultrasonic in preparation of root-end cavities.J Endod 2005; 31:821–3.
114. Stabholz A, Sahar-Helft S, Moshonov J. Lasers inendodontics. Dent Clin N Am 2004;48:809–32.
Chapter 26 / Endodontics Instruments and Armamentarium / 869

F. VISUAL ENHANCEMENT
JAMES K. BAHCALL
Visualization during surgical and conventionalendodontic treatment has historically been limited totwo-dimensional dental radiography representative ofa three-dimensional biologic system and what couldbe seen with the naked eye (perhaps enhanced byloupes). Today, endodontic treatment is to a largeextent viewed as a microsurgical procedure. The prin-ciple upon which all microsurgery is based is theobservation that the hand can perform remarkablyintricate micromanipulations as long as the eye cansee a magnified field and it can be interpreted by themind.1 Magnification affects vision by increasingthe size of an image on the retina. ‘‘Visual image’’ isthe basic parameter used to describe how large some-thing appears, and is expressed in units of degree orcycles/degree.2 The use of optical magnificationinstruments such as loupes, microscopes, endoscopes,and orascopes enables the endodontist to magnify aspecified treatment field beyond that perceived by thenaked eye.
Optical Definitions
Working Distance: The distance measured from thedentist’s eye to the treatment field being viewed.
Depth of Field: The amount of distance between thenearest and furthest objects that appear in accep-tably sharp focus.
Convergence Angle: The aligning of two oculars to besure they are pointing at the identical distanceand angle to the object or treatment field.
Field of View: The area that is visible through opticalmagnification.
Viewing Angle: The angular position of the opticsallowing for a comfortable viewing position forthe operator.
Loupes
Dental loupes are the most common magnificationsystem used in dentistry. All loupes use convergentlenses to form a magnified image.3 The simplest formof optical magnification is single-lens loupes (ie, jewe-ler’s flip-down magnifiers). Single lenses have a fixedfocal length and working distance.4 The advantages ofthese types of loupes are low cost and light weight asthey are made of plastic. The disadvantage of single-lens loupes is poor image resolution compared withmulti-lens glass optics (telescopic loupes and micro-scopes).5 Because single-lens loupes provide a setworking distance, the dentist may find the ergonomicsincorrect and may need to compensate with poorbody posture, causing the possible neck and backstrain.
In order to overcome the disadvantages of single-lens loupe optics, the use of multi-lens optic system isrecommended. This type of glass multi-lens configura-tion is known as a Galilean optical system (Figure 1). Itprovides a higher level of magnification, improveddepth of field and working distance, and higher opticalresolution compared with single-lens optics.4 Tele-scopic loupes use Galilean optics. Ideal magnificationwith telescopic loupes is �2.5. This offers a goodcompromise between weight, optical performance,and cost. Galilean lens systems cannot offer magnifica-tion much greater than �2.5 without incurringweight, size, and image resolution problems.5 Silberrecommends the use of �2.5 operating loupes becausemagnification of loupes greater than �2.5 limits thedepth of field and working distance during treatment.1
Any head movement of the operator, while usingloupes with magnification greater than �2.5, will movea treatment field in and out of focus, very distractingand irritating to the clinician. When need for highermagnification is required (up to �6), prism optics are
870

available. This optical system is based on the Keplarianastronomic telescope, which uses five lenses and twoprisms. The advantages of this optical system are super-ior optical clarity and a flatter view from edge to edge.However, the disadvantages are expense and addedweight to loupes.5 And as the magnification in loupesincreases, the need for more illumination is required.6
Loupe manufacturers have designed portable clip-on
light sources to accommodate demand for increasedlight.
Microscopes
Baumann7 was the first to report the use and benefitsof an operating microscope for conventional endo-dontics. Since then, the use of the surgical operatingmicroscope (SOM) has evolved in the field of endo-dontics as an invaluable optical magnification instru-ment8–10 (Figure 2). Today, this visual evolution inendodontics, from using loupes and headlamps to theuse of the microscope, parallels a similar transitionin medical specialties, such as ophthalmology andneurosurgery.11 On January 1, 1998, the AmericanDental Association Accreditation Standards forAdvanced Specialty Education Programs in Endodon-tics were revised; formal microscope training must beincluded in surgical and nonsurgical endodontictreatment.11
The magnification needs in endodontic treatmentrange from �3 to �30.12 A SOM accommodates thesemagnification requirements. Although loupes canhave a magnification as high as �6, they are not ableto provide the same depth of field at �6 magnifica-tion compared with the microscope,1 and fiber opticlight source of the SOM provides two to three timesthe light emitted from a surgical headlamp.13
Similar to loupes, microscopes use the Galileanlens system. The magnification of the SOM is
Figure 1 Diagram of Galilean optics. Illustration courtesy of Designs forVision, Inc., Ronkonkoma, NY.
Figure 2 Clinical use of surgical operating microscope. Photo courtesy of Jedmed, St. Louis, MO.
Chapter 26 / Endodontics Instruments and Armamentarium / 871

determined by the magnification power of the eye-piece, the focal length of the binoculars, the magni-fication changer factor, and the focal length of theobjective lens (Figure 3).12,14 The eyepiece has adjus-table diopter settings ranging from –5 to +5. Dioptersettings help the clinician focus the lens of the eyesand adjust for refractive error, which is the degree towhich a person needs to wear corrective eyeglasses.12
The benefits of using an SOM for optical magnifi-cation in conventional endodontic treatment are welldocumented in the literature.15–19 They are increasedvisualization of the treatment field, enhanced visuali-zation in locating canals, aid in the removal ofseparated instruments, diagnosis of micro fractures,perforation repair, and case documentation.
The advantages of using an SOM during surgicalendodontic treatment are enhanced view of the surgi-cal treatment field, need for taking fewer radiographsduring the surgical procedure, and the ability to docu-ment the treatment.20
When viewing an endodontic treatment fieldthrough a microscope, the use of a standard dental
mirror or micromirror is usually required, inconjunction with the microscope, to overcome theangulation difficulties of certain tooth positions inthe mouth. Saunders and Saunders15 have stated thatthe most common reasons for endodontists not usingthe SOM during treatment: positional difficulties,inconvenience, and increased treatment time.
Rod–Lens Endoscope
The use of a rod–lens endoscope in endodonticswas first reported in 1979.21 In 1996, the rod–lensendoscope was recommended as a magnificationinstrument for conventional and surgical endodonticprocedures.22,23 The rod–lens endoscope (Figure 4) ismade up of rods of glass working in junction with acamera, light source, and monitor (Figure 5). Theoption of a digital recorder (either streaming videoor still capture) may be added to the system fordocumentation.
The rod–lens endoscope allows clinicians’ greatermagnification than that achieved with loupes or amicroscope, with optical resolution comparablewith that of microscopes and/or loupes. Althoughthe endoscope can be used as a visualization instru-ment for conventional endodontic treatment, it canbe bulky and difficult to maintain a fixed field ofvision compared with a microscope. A fixed field ofvision is defined as ‘‘viewing a treatment field fromone single angle and distance.’’24 The use of theendoscope is therefore recommended for visualiza-tion of surgical endodontic treatment.22–27 The
Figure 3 A schematic diagram of the surgical operating microscope.The eyepiece connected to binocular field glasses allows adequate focallength. The objective lens increases the magnification. The magnificationchanger adds to the flexibility of the microscope.
Figure 4 A rod–lens endoscope (Jedmed, St. Louis, MO).
872 / Endodontics

visualization advantage, in surgical endodontictreatment, the endoscope provides over the micro-scope, is the ability to view a surgical treatmentfield in a nonfixed field of vision. This is definedas the ability to view a treatment field at variousangles and distances without losing depth of fieldand focus.24
The recommended rod–lens endoscope sizes, forendodontic surgical application, are a 2.7 mm lensdiameter, 70� angulation, 3 cm length rod–lens, anda 4 mm lens diameter, 30� angulation, and 4 cmlength rod–lens.24 A pair of �2 to �2.5 loupes shouldbe used for visualization prior to the use of the endo-scope.1,24 Loupes aid the endodontist during surgerywhen reflecting gingival tissue, removing cortical andmedullary bone, and isolating root ends. The clinicianshould hold the endoscope while the assistant retractsgingival tissue and suctions.24 This maintains goodeye–hand coordination during examination or treat-ment. The clinician and the assistant(s) view themagnified image on the monitor.
Hemostasis of the surgical field must be obtainedbefore the endoscope is used because the scopecannot provide a discernible image when placed inblood. The warmth of the blood can also createlens condensation and a blurred image. If thisoccurs, the use of suction and irrigation, or anantifogging agent, will eliminate the fogging effect.The tips of the endoscope should be placed onbone around the surgical crypt in order to stabilizethe scope. Prior to usage, a protective metal sheathis placed over the endoscope to add rigidity andallow the endoscope to be held in a stable position.It is not recommended to use the endoscope to alsoretract gingival tissue while viewing a surgical treat-ment field. This will not allow free movement ofthe scope by the operator while also having diffi-culty keeping the gingival tissue out of the line ofsight.
Orascope
An orascope is a fiber optic endoscope and like therod–lens endoscope works in injunction with acamera, light source, and monitor. Fiber optics aremade of plastics and therefore are small, lightweight,and flexible. It is important to note that imagequality from fiber optic magnification has a directcorrelation with the number of fibers and size of thelens used. The fiber optic endoscope is designed forintracanal visualization.28 The orascope has a 0.8mm tip diameter and 0� lens and the working por-tion is 15 mm in length (Figure 6). The orascope is
Figure 5 Endoscope visual system (EVS) (Jedmed, St. Louis, MO).
Figure 6 An orascope (Jedmed, St. Louis, MO).
Chapter 26 / Endodontics Instruments and Armamentarium / 873

made up of 10,000 parallel visual fibers. Each visualfiber is between 3.7 and 5.0 mm in diameter. A ringof much larger light transmitting fibers surroundsthe visual fibers for illumination of a treatment field(Figure 7).
Prior to the placement of the 0.8 mm fiber opticscope, it is recommended that �2 to �2.5 loupes or aSOM be used for conventional endodontic visualiza-tion during access to the canal(s). A canal must beprepared to a minimum size of a 90 file in the coronal15 mm of the canal. If the canal is under-instrumen-ted, a wedging of the orascope may damage some ofthe fiber optic bundles within the scope. The propercanal enlargement also allows the full 15 mm of thescope to penetrate within the canal. The canal mustalso be dried before the 0.8 mm fiber optic scope isplaced. Although the scope will see through sodiumhypochlorite, this solution has a high light-refractoryindex. This will cause greater amounts of light thatwill be reflected, thus making it difficult to see detailsof the canal.
The focus and depth of field of an orascope isfrom 0 mm to infinity. This allows the orascope toprovide imaging of the apical third of the root with-
out actually having to be placed in this region of thecanal.
Similar to the endoscope, the endodontist holds theorascope while viewing the image from the monitor.28
Temperature and humidity difference between thedental operatory and the canal can cause moisture tocondense on the fiber optic lens, causing fogging. Theuse of a lens antifog solution helps eliminate lenscondensation build-up.
Microscope–Endoscope Combination
In conventional and surgical endodontic treatment,there are different visualization parameters for eachtype of treatment, when magnification beyond loupesis required. Although both the microscope androd–lens endoscope can be used for magnificationfor either type of endodontic treatment, the advan-tages for using a microscope for conventionalendodontic treatment and a rod–lens endoscope forsurgical visualization led to the development of amicroscope coupler (Jedmed, St. Louis, MO) thatenables the endodontists to combine both technolo-gies (Figure 8). The combination unit also allows forthe use of the orascope and digital documentation.
Magnification versus Differentiation
Magnification is defined as making an object or treat-ment field greater in size. Differentiation is defined asmaking something distinct or specialized.29 The needto differentiate a magnified treatment field, whenlooking for a fracture in conventional endodontictherapy, or in surgical endodontic therapy whentrying to identify the periodontal ligament space, anisthmus, or marginal leakage around a previous root-end filling, is important. Methylene blue, a nontoxic,biocompatible dye, can be used in conjunction withendodontic visualization instruments to help differ-entiate a treatment field in order to aid the endodon-tist in identifying etiology30 (Figure 9).
Figure 7 Cross-section of orascope probe showing the distribution offiber optic image bundle and the light transmission fibers.
874 / Endodontics

A B
Figure 9 A, Magnification of a root end without differentiation. B, Magnification of a root end with methylene blue added for differentiation.
Figure 8 Combination microscope–endoscope visualization system (Jedmed, St. Louis, MO).
Chapter 26 / Endodontics Instruments and Armamentarium / 875

Summary
The ability to enhance vision during endodonticprocedures has significantly increased the comfort levelof endodontists in terms of identifying fracture lines,locating minuscule canal orifices, and confidently deter-mining anatomic variations in teeth and supportingstructures. Technological advances are continuouslybeing made in advanced vision equipment, promisingan even brighter future.
References1. Silber S. Microsurgery. Baltimore: William & Wilkins Co;
1979. p. 1.
2. Kagan J, Gehly J, Wilson H. The effect of vibration on visionduring microsurgery. Microsurgery 1983;4:209–14.
3. Shanelec DA. Optical principles of loupes. J Can Dent Assoc1992;20:25–32.
4. Kanca J, Jordan PG. Magnification systems in clinical dentis-try. J Can Dent Assoc 1995;61:851–6.
5. Millar BJ. Focus on loupes. Br Dent J 1998;185:504–8.
6. Caplan SA. Magnification in dentistry. J Esthet Dent1990;2:17–21.
7. Baumann RR. How may the dentist benefit from the operat-ing microscope? Quintessence Int 1977;5:17–18.
8. Selden HS. The Role of the dental operating microscope inendodontics. Penn Dent J 1986;53:36–7.
9. Selden HS. The role of a dental operating microscope inimproved nonsurgical treatment of ‘‘calcified’’ canals. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1989;68:93–8.
10. Carr GB. Microscopes in endodontics. J Calif Dent Assoc1992;20:55–61.
11. Mines P, Loushine R, West L, et al. Use of the microscope inendodontics: a report based on a questionnaire. J Endod1999;25:755–8.
12. Rubinstein R. The anatomy of the surgical operating micro-scope and operating positions. Dent Clin North Am1997;41:391–4.
13. Mounce R. Surgical operating microscopes in endodontics:the quantum leap. Dent Today 1993;12:88–91.
14. Nunley JA. Microscopes and microinstruments. Hand Clinics1985;1(2):197–204.
15. Saunders WP, Saunders EM. Conventional endodontics and theoperating microscope. Dent Clin North Am 1997;41:415–27.
16. Coelho de Carvalho MC, Zuolo ML. Orifice locating with amicroscope. J Endod 2000;26:532–4.
17. Gorduysus MO, Gorduysus M, Friedman S. Operating Micro-scope improves negotiation of second mesiobuccal canals inmaxillary molars. J Endod 2001;27:683–6.
18. Buhrley LJ, Barrows MJ, BeGole EA, Wenkus CS. Effect ofmagnification on locating the MB2 canal in maxillary molars.J Endod 2002;28:324–7.
19. Kim S. The microscope and endodontics. Dent Clin NorthAm 2004;48:11–18.
20. Rubinstein R. Endodontic microsurgery and the surgicaloperating microscope. Compendium 1997;18:659–72.
21. Detsch S, Cunningham W, Langloss J. Endoscopy as an aid toendodontic diagnosis. J Endod 1979;5:60–2.
22. Held S, Kao Y, Well D. Endoscope-an endodontic applica-tion. J Endod 1996;22:327–9.
23. Shulman B, Leung B. Endoscopic surgery: an alternative tech-nique. Dent Today 1996;15:42–5.
24. Bahcall J, Barss J. Orascopic visualization technique for con-ventional and surgical endodontics. Int EndodJ 2003;27:128–9.
25. von Arx T, Montagne D, Zwinggi C, Lussi A. Diagnosticaccuracy of endoscopy in periradicular surgery—a compar-ison with scanning electron microscopy. Int Endod J2003;36:691–9.
26. Taschieri S, Del Fabbro M, Testori T, et al. Endodonticsurgery using 2 different magnification devices: preliminaryresults of a randomized controlled study. J Oral MaxillofacSurg 2006;64:235–42.
27. Bahcall J, Di Fiore P, Poulakidas T. An endoscopic techniquefor endodontic surgery. J Endod 1999;25:132–5.
28. Bahcall J, Barss J. Fiberoptic endoscope usage for intracanalvisualization. J Endod 2001;27:128–9.
29. Bahcall J, Barss J. Orascopy: a vision for the new millennium,Part 2. Dent Today 1999;18:82–4.
30. Cambruzzi J. Methylene blue dye: an aid to endodontic sur-gery. J Endod 1985;11:311–14.
876 / Endodontics

CHAPTER 27
PREPARATION OF CORONAL
AND RADICULAR SPACES
OVE A. PETERS, RAVI S. KOKA
It has been well established over the past 30 yearsthat endodontic disease, the presence of apical perio-dontitis, has a microbial pathogenesis.1,2 Conse-quently, root canal treatment is performed to treatendodontic disease by eradicating bacteria from theroot canal space. It is widely accepted that disinfec-tion and subsequent obturation of the root canalspace require mechanical enlargement of the maincanals,3 and the vast majority of techniques andinstruments today are based on this objective. There-fore, this chapter will focus on the principles ofpreparation of coronal and radicular canal spaces; itbreaks this down into two distinct steps: first, pre-paration of the coronal access cavity and second,radicular canal shaping.
Coronal Access Cavity Preparation
The objective of the coronal access preparation is toprovide a smooth free-flowing tapered channel fromthe orifice to the apex that allows instruments, irri-gants, and medicaments to attempt cleaning andshaping of the entire length and circumference ofthe canal, with as minimal a loss of structural integrityto the tooth as possible. The access preparation gen-erally refers to that part of the cavity from the occlusaltable to the canal orifice. However, its design isdependent on the position and curvature of the entirelength of the canal, not just the position of the orifice,and is therefore not a simple cavity.
In this first section on coronal access cavity prepara-tion, the section on principles is intended for all teeth ingeneral. The following sections will deal with the indi-vidual nuances in access preparation for each tooth.
General Principles
‘‘DO NO HARM’’No practitioner performs treatment with the intent toharm and yet substandard quality does occur. Theproblem seems to stem partially from a lack of aware-ness and knowledge. In addition, the daily stresseswithin the practice environment compound this issue,and the stage is set for inadvertently causing harm ordamage to the tooth and ultimately the patient. Tominimize the frequency of harm clinicians may cause,learning and awareness should be lifelong objectives.A ‘‘mindful practice’’ is the objective that continu-ously monitors and reevaluates results and techniquesover time with introspection.
CONFIRMATION OF ETIOLOGY OF PULPALPATHOSISPart of the objective of the access preparation is toconfirm the etiology of pulpal breakdown assessedduring diagnosis. The only proven etiological factorsare bacterial contamination (via caries, coronal leak-age under restorations, fractures) and trauma (e.g.,resorption, thermal, mechanical, and physical). Asthe pulp chamber is entered, the clinician mustvisually inspect the state of its contents to check thatit matches with the preoperative diagnosis. It is dis-concerting to expose the vital tissue when a preopera-tive diagnosis of necrosis has been made. Also theetiology of the pulpal breakdown has to be discerned.At times, it is easy to confirm the etiology, for exam-ple, the presence of a carious lesion, but in the absenceof obvious clinical evidence, the practitioner mustmake a conscious effort to search for the cause. Clini-cally, presentation of microleakage and cracks is
877

extremely subtle and difficult to detect. Staining,high-power magnification under a microscope, tran-sillumination may all help discover these sources.
ASSESSMENT OF RESTORABILITYAlthough it is tempting to develop an ‘‘endodonticsmode’’ mindset, once root canal treatment has beendiagnosed, another major objective is to check therestorability of the tooth prior to root canal treat-ment. Existing restorations, caries, and unsupportedenamel and dentin should be removed and theremaining tooth structure examined under a micro-scope. The operator should search for the presence ofcracks, height, and thickness of the remaining dent-inal walls for ferrule effect, the relationship of theremaining coronal tooth margins relative to the oss-eous crest, root length, location of the furcation,amount and quality of attached gingiva, and positionof the tooth in the arch. This can result in severaladvantages:4
• Before root canal treatment is started, the patientcan be forewarned of risks, benefits, and alterna-tives of any further procedures and/or costs torestore the tooth completed, for example, crownlengthening, gingivectomy, extrusion, or placementof orthodontic bands.
• A more educated opinion on long-term prognosiscan be provided by the clinician to enable thepatient to choose whether root canal treatment orimplant therapy is more beneficial.
• Leakage of bacteria back into the root canal spaceunder a preexisting defective restoration can beprevented.
• Cracks on the remaining tooth structure can bemore readily assessed. This may change the clini-cian’s decision to extract versus restore, to placebuild up immediately, to perform cuspal reductionor warn the patient more emphatically of thechance of fracture postoperatively.
However, in certain situations it can be argued that aportion of the restoration should be left in placeuntil the root canal treatment is almost complete.This provides a circumferential matrix to enable aseal by the rubber dam or help hold the clamp inplace (as long as no leakage can be seen under highermagnification).
A more difficult situation arises when an existingcrown is present on the tooth that requires endodontictreatment. Accessing through a crown has several dis-tinct disadvantages: the amount of remaining toothstructure, the quality of the build-up restoration, theextent of any decay, and the quality of the crown sealcannot be thoroughly assessed. In fact, Abbott4 foundthat there was less than 60% chance to detect caries,fractures, and marginal breakdown, without completeremoval of restorations. All of these factors have aprofound effect on the long-term success of the rootcanal treatment, and longevity of the tooth. However, itis impractical to suggest removing all crowns prior toroot canal treatment, and therefore a careful assessmentof the integrity of the crown must be attemptedthrough history-taking and clinical examination beforeand during treatment.
STRAIGHT-LINE ACCESSIt is well documented that to prepare the apical thirdof the canal circumferentially, a straight path for thecutting instrument from the orifice to the apex isimperative.5,6 As the curvature of the canal increases,a file that enters into the canal is deflected at its tip bythe force exerted by the dentin. However, accordingto Newton’s Law, the file tip exerts back an equal andopposite reaction upon the dentin, that is, force onthe outer dentinal surface of the canal as the fileattempts to straighten back to its original dimension.If the dentin exerts a greater force than the file, the filebends, but this changes as the file size increases. Even-tually, the file will cut the dentin rather than bend. Atthis point, the outer dentinal wall of the curvature iscut preferentially, known as gouging, which is thestart of ledging and transportation. This effect isaccentuated with cutting-tip files compared with non-cutting tips and with a vertical filing motion versusrotational motion.
A concomitant problem develops as the file tipexerts a force back on the dentin. A fulcrum pointdevelops, which is the most protuberant point ofcontact on the furcal dentinal surface. Therefore, pre-ferential cutting occurs on the furcal surface also, thesite of a most common procedural error, known asstripping that can lead to perforation.
The term ‘‘straight-line access’’ (SLA) describes apreparation that provides a straight or outwardly
878 / Endodontics

flared, unimpeded path from the occlusal surface tothe apex. This allows the file to reach the apex withminimal deflection (Figure 1). The main corollary is
that it has to be accomplished without compromisingthe furcal surface of the canal that could ultimatelylead to strip perforation. Access is continually
A
B C
Figure 1 Straight line access in a mandibular third molar A, The orifice opening and path of insertion preoperatively is indicated by a black line. The mesialwall had to be cut to obtain a straight-line access B, The handles of the files are standing upright without crossing over each other indicating adequate Straight-line access C, However, often the distal canals are angled such that the file handles project out of the orifice mesially while still maintaining SLA.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 879

adjusted until the selected master apical file (MAF)reaches the working length (WL) without undue stressupon it. A more aggressive SLA is required as the sizeof the file used and/or the degree of canal curvatureincreases. In this context, ‘‘aggressive’’ suggests thatthe orifice wall leading to the canal has to be movedand flared more obtusely toward the correspondingline angle.
The diameter of the apical preparation also effectsthe access preparation. To prepare a larger apicaldiameter, correspondingly larger, stiffer files that havea stronger tendency to straighten the canal have to betaken to the apex. In order to avoid stripping on thefurcal surface or transporting the apex, one mustachieve SLA beforehand. Unfortunately, the literaturedoes not provide a consensus on the ideal apicaldiameter. However, in vitro studies have measuredcanal diameters.7,8 Other studies9–12 have measuredcanal cleanliness after a small versus larger diameterapical preparation and have shown better cleanlinesswith the larger diameters. One study, however, foundthat improvement gained with larger diameters wasnot statistically significant and concluded that smallapical diameters were sufficient for adequate bacterialreduction.13
Radiographically, canal curvature in the mesiodistalplane can be directly observed; however, Cunninghamand Senia14 demonstrated that canals possess a three-dimensional curvature. Therefore to obtain an SLA,sometimes tooth structure must be removed more onthe buccal or the lingual surface than just on the mesialor the distal surface.
SLA involves the selective removal of the outercanal tooth structure to protect the furcal surface.Various methods have been advocated for this. Theso-called ‘‘anticurvature’’ filing (see below) involvescutting only on the outward stroke away from thefurcal surface but is not effective beyond curvatures.Gates Glidden (GG) burs allow the selective removalof dentin when used with a laterally directed motionand similarly stiffer nickel–titanium (NiTi) rotarieshave significant lateral cutting ability (Paque F andPeters OA, unpublished data).
Peters et al.,15,16 using microcomputed tomogra-phy, have shown that significant portions of canals
are not touched during instrumentation due to theirregularities and curvature of the canals. This reiter-ates the importance of achieving SLA.
Mannan et al.5 tested whether SLA would allowmechanical cleaning of all the walls of the root canalin a single-rooted anterior tooth with a simple rootcanal anatomy. They prepared three types of accesscavity designs: a ‘‘lingual cingulum’’ just coronal tothe cingulum, a ‘‘lingual conventional’’ where thecavity was extended to within 2 mm of the incisaledge, and an access cavity involving the ‘‘incisal edge’’but not the labial surface. They found that none of thecavity designs allowed complete planing of the rootcanal walls although the incisal edge design allowed agreater proportion of the root canal walls to be filedthan the other two. This study, however, determinedthe MAF size as three sizes larger than the first file tobind, which had already been shown by otherresearchers to be an ineffective technique to properlyclean the apical canal third.8 Another possible defi-ciency was that they did not extend the access cavitiesonto the labial surface, which is often necessary fortrue SLA as shown earlier.17,18 However, the study didemphasize that SLA provides the best chance of deb-ridement of the entire canal.
THREE-DIMENSIONAL POSITIONOF TEETH IN JAWSThe true three-dimensional position that teeth hold ineach jaw cannot be assessed accurately by clinical orradiographic perspectives. Therefore, using the occlu-sal table of the tooth as a guide to the location of thechamber can be quite misleading. Figure 2 shows thelingual and mesial inclination of the mandibularmolars, the mesial inclination of the maxillary molars,and the labial inclination of all the incisors.19 Corre-spondingly, when accessing, the bur must be angled tomimic these inclinations in both mesiodistal and buc-colingual planes. However, other factors that limit theideal angulation come into consideration. A compro-mise is reached, for example, trying to avoidencroaching on the incisal edge when accessing ante-rior teeth, or trying to avoid breaking through amarginal ridge. Improper angulation results in the
880 / Endodontics

common occurrence of unnecessary gouging of thedentinal walls that weakens the remaining tooth struc-ture and in extreme cases leads to external perforation(Figure 3).
Part of the reason that these angulations are hard totransfer to the clinical setting is that the operator usuallysits in the 10, 11, or 12 O’clock position with the patientreclined. This can be disorienting. The tooth is not viewedfrom the perspective shown in the figure, and is not in linewith any external horizontal or vertical plane landmarks.
The operator has to physically move to view the angle ofthe bur relative to the patient’s vertical and horizontalplanes. This is similar to taking a radiograph by theparalleling technique.
EXTERNAL ROOT SURFACE AS A GUIDEExternal root anatomy is determined by the internalpulp. The mesenchymal pulp tissue gives rise toodontoblasts that in turn lay down the dentin. As
Figure 2 Schematic views of the three-dimensional positions of teeth in jaws in frontal and saggital views with long axes of the teeth displayed. It isprudent during access to mimic these angulations to avoid unnecessary gouging. Root types are indicated by symbols on arrows. A, Maxilla. Note the mesialand buccal angulation of the molars and proclination of the anteriors. B, Mandible. Note the mesial and lingual angulation of the molars and proclination ofthe anteriors. Adapted 2007 with permission from Dempster et al., J Am Dent Assoc 67:779, 1963, Copyright ª American Dental Association.19
Chapter 27 / Preparation of Coronal and Radicular Spaces / 881

the long axis of the tooth cannot be seen in theclinical setting, the next best guide is the externalroot surface. Acosta and Trugeda20 sequentiallyreduced the clinical crowns of 134 extracted maxil-lary molars and examined the pulp chamber at thelevel of the pulpal floor. They found the pulp cham-ber in the center of the tooth, closely matching itsouter contour and maintaining the same distancefrom the mesial, distal, buccal, and lingual surfaces.
This finding was confirmed more recently usingmathematical models based on microtomographydata.21 It was noted that the shape of the pulpchamber was trapezoidal, and it was thereforerecommended shaping the access preparation in thesame way.20
In another study,22 500 teeth were used of which400 were sectioned at the cementoenamel junction(CEJ), 50 buccolingually, and 50 mesiodistally. The
A
B C
Figure 3 Examples of unnecessary gouging of axial or furcation dentin due to improper angulation of the bur during access preparation. A, Preoperativeand postoperative radiographs showing gouging of furcal dentin in the entrance to the mesiobuccal canals due to underextension of the mesial wallduring initial instrumentation. B, Proper angulation was maintained allowing minimal tooth structure loss. C, Vertical instead of distal angulation whilesearching for distal canals.
882 / Endodontics

patterns in orifice location, size, color, shape, andseveral conclusions were noted (Figure 4):Law of Centrality: The floor of the pulp chamber is
always located in the center of the tooth at thelevel of the CEJ.
Law of Concentricity : The walls of the pulp chamber arealways concentric to the external surface of the toothat the level of the CEJ, that is, the external root surfaceanatomy reflects the internal pulp chamber anatomy.
Law of the CEJ: The distance from the external surface ofthe clinical crown to the wall of the pulp chamber isthe same throughout the circumference of the toothat the level of the CEJ—the CEJ is the mostconsistent repeatable landmark for locating theposition of the pulp chamber.
Law of Symmetry 1: Except for the maxillary molars,the orifices of the canals are equidistant from aline drawn in a mesial–distal direction, throughthe pulp chamber floor.
Law of Symmetry 2: Except for the maxillary molars,the orifices of the canals lie on a line perpendicularto a line drawn in a mesial–distal direction acrossthe center of the floor of the pulp chamber.
Law of Color Change: The color of the pulp chamberfloor is always darker than the walls.
Law of Orifice Location 1: The orifices of the rootcanals are always located at the junction of thewalls and the floor.
Law of Orifice Location 2: The orifices of the rootcanals are located at the angles in the floor–walljunction.
Law of Orifice Location 3: The orifices of the root canalsare located at the terminus of the rootdevelopmental fusion lines.
As the external root surface is a reliable guide, it canbe quite frustrating to place the rubber dam, whichcompletely obscures it. Therefore, in difficult cases, itis prudent to prepare the initial access shape and findthe pulp chamber or at least one orifice prior torubber dam placement. Alternatively, multiple teethcan be isolated by clamping one tooth more posteriorso that the CEJ and the relationship of adjacent teethare visible and palpable on the treated tooth. TheSilker-Glickman clamp (Silk Pages Publishing, Deer-wood, MN) was designed for this purpose. Otherwise,a single tooth clamp may be used and the dam flossedbetween the mesial contacts.
KNOWLEDGE OF PERCENTAGES FOR THENUMBER OF CANALS WITHIN A ROOTIt has been known that roots contain multiple complexcanal systems since at least 1925 as described by Hessand Zurcher.23 Since then, research has focused ondetermining their classification and incidence. Data forcanal numbers and configurations extracted fromselected references are presented in Chapter 6, ‘‘Mor-phology of teeth and their root canal systems’’. Somefactors that affect such data have been noted, for exam-ple, methods and materials, type of magnification, invivo, ex vivo, but many factors have not been noted, forexample, case report articles, ethnic groups, age groups,
Figure 4 The pulp chamber is usually centered at the cementoenameljunction (CEJ) level allowing the use of external root surfaces as a guidefor access. The distance from the pulp chamber to the outer contourindicated by arrows. Fl, floor of the pulp chamber. Reprinted withpermission from Krasner P and Rankow HJ.22
Chapter 27 / Preparation of Coronal and Radicular Spaces / 883

individual interpretation of classification systems by thevarious researchers.
From the material presented in Chapter 6, ‘‘Mor-phology of teeth and their root canal systems’’, it canbe extrapolated that studies report the incidence ofmultiple canals from 0% to as high as 95% forcertain roots. Therefore the clinician must, toincrease chances of finding them, have a thoroughknowledge of the number, incidence, location, andthe variability of the canal systems of each tooth androot, in order to design the access cavity. Selectiveremoval of otherwise solid tooth structure can bejustified only when the operator is confident of theknowledge that further canal systems may exist moreapically and that the subsequent weakening of thetooth is offset by the significant advantage to long-term prognosis in finding another canal system.
MINDSETKnowing that roots can have multiple complex canalsystems, how zealous should the clinician be in look-ing for them? Obviously, the downside in removingthe tooth structure to look for canals without successis the decrease in structural integrity and reducedlong-term prognosis. Also, clinicians are trained toconserve as much tooth structure as possible. A toothshould be entered under the assumption that everyroot has multiple canals. This assumption can beproved wrong only after adequate searching, definedby objective criteria, for example, troughing throughthe lighter-colored dentin of the walls compared tothe darker dentin of the pulpal floor or drillingapproximately 5 to 7 mm below the furcal floor.Clinicians can then regularly self-assess, by compar-ison to the actual figures presented in the variousstudies and by discussion with peers. There is a bal-ance between selectively extending the access cavity tosearch for canals and unnecessary overextension—theart is in determining this line.
MAGNIFICATION/MICROSCOPELittle controversy remains over the effectiveness of thedental operating microscope. Several studies haveshown that it increases the dentist’s ability to find canals,allows precise repair of perforations, aids in removingseparated files, and improves surgical visibility (seeChapter 26F, Visual Enhancement for more details).
Clinical Armamentarium
Access preparation requires few standard hand instru-ments, but a wide range of equipment for differing
situations. The basic requirements are a mirror, a DG16-type endodontic explorer (e.g., HuFriedy, Chicago, IL),high- and slow-speed handpieces, a range of burs, anda microscope. A standard set of burs (Figure 5) shouldinclude at least a #2 round diamond, a #1 round carbide, atransmetal bur (Dentsply Maillefer, Ballaigues, Switzer-land), various cylindrical diamonds (e.g., 859–010, 859–012, 859–014, BrasselerUSA, Savannah, GA), and anEndoZ bur (Dentsply Maillefer).
The following are accessory items for differing situa-tions or routine use depending on the practitioner’spreference. Bendable and differently sized heads ofmirrors (eie2, San Diego, CA) allow improved man-euverability and visibility but can be particularly help-ful in cases of difficult access due to the distal locationof the tooth or the patient’s inability to open widely(see Figure 5). An endodontic explorer that is finerthan the regular DG16 is also available, the MicroJW17 endodontic explorer (CK Dental, Orange, CA).
Some clinicians find the Micro-Openers andMicro-Debriders (Dentsply Maillefer) helpful. Theformer have 7 mm of K-type flutes in 0.04 and 0.06tapers in ISO sizes #10 and #15, and the latter have16 mm of Hedstrom-type cutting flutes in sizes #20and #30. Both are mounted as a handheld instrumentat a double angle and can be useful for initial orificelocation and widening.
BURSSafe-ended diamonds and tungsten carbide burs thatdo not cut at their tip, for example, Endo Access,Endo Z burs, LA Axxess burs (SybronEndo, Orange,CA), can be beneficial in avoiding gouging. However,these burs are wide and should be used for finalrefinement after precise extension has already beendetermined with thinner cylindrical diamonds. TheMueller bur (BrasselerUSA) is a latch-grip surgicallength round carbide bur available in sizes 0.9, 1.0,1.2, 1.4, 1.6, and 1.8 mm diameters. Similarly, MunceDiscovery burs (CJM Engineering, Santa Barbara, CA)are 34-mm-long, narrow-shafted, nonflexible roundcarbide burs available in sizes 1/4 (0.5 mm diameter),1/2 (0.6 mm), 1 (0.8 mm), 2 (1.0 mm), 3 (1.2 mm),and 4 (1.4 mm). The extended length of both theseburs reduces the head of the handpiece blocking theoperator’s view. The Munce burs are not as flexible asthe Mueller burs due to a slightly greater shaft dia-meter and are available in smaller sizes. Both theseburs are useful for deep troughing to find canals,opening isthmuses, or reaching separated instrumentsand seem to leave an easier-to-read dentin surfacethan ultrasonics (see Figure 5).
884 / Endodontics

ROTARY INSTRUMENTSFor gaining SLA in the coronal portion of the canals,rotary instruments that selectively cut laterally areuseful to minimize excess removal of the furcal den-tin. GG drills (sizes 1 (ISO #50), 2 (#70), 3 (#90),4 (#110), 5 (#130), and 6 (#150)) have been used formany years and are efficient and relatively inexpen-
sive. Some of the stiffer NiTi rotaries also have lateralcutting ability.
ACCESSORY INSTRUMENTSThe Stropko Irrigator (Vista Dental Products, Racine,WI) is an adapter that connects to the air/water syr-inge and accepts standard Luer-lock needle tips for
A B
C D
E
Figure 5 Examples of armamentarium for access and inspection of pulp chambers. A, Mirrors with variable head sizes and bendable shafts. B, Bur blockused in the practice of one of the authors (R.K.). C, Additional typical burs used for access: #2 round diamond, tapered diamond, EndoZ bur. D, MunceDiscovery burs. E, Various ultrasonic tips. Images courtesy of Dr. Gary Carr, Dr. Cliff Ruddle and C.J.M. Engineering, Solvang, CA, USA.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 885

pinpoint irrigation or aeration. It regulates air orwater flow to between 2 and 7 psi and provides a veryprecise delivery. It aids visibility at high-power mag-nification under a microscope.
Ultrasonically powered instruments with well-adapted tips from various manufacturers have nowbecome indispensable (see Figure 5E). They allow fordeep troughing with minimal collateral tooth structureremoval. Visibility is better than with burs, and the tipscan be diamond-coated to increase their efficiency.However, all tips develop significant heat and can causenecrosis of the surrounding bone if used without acoolant. Some practitioners finish their access prepara-tions with sandblasting or finishing burs; this practicemay have an impact on composite bonding.24
Clinical Guidelines
PREOPERATIVE CLINICAL GUIDELINESDetermination of the point of penetration: Usually entryis in the center of the occlusal table but in certain teeth(e.g., maxillary molars) it is deceiving, as the center ofthe occlusal table does not reflect the center of the pulpchamber. Anatomy and strategies for access is detailedin sections on individual teeth below.
Assessment of occlusal and external root form: Oncethe point of entry has been determined, the bur’s angula-tion in three dimensions has to be mentally envisaged.This is determined by taking into account the angulationof the teeth in the jaws (see Figure 2) and assessing theexternal root surface at the level of the CEJ.
Radiographic measurement of the depth of the pulpchamber roof from the occlusal table: The initial bur inthe high-speed handpiece is placed against a radio-graph or a measurement determined from a calibrateddigital image.
Assessment of complicating factors: Rotations/tip-ping of tooth, calcifications (stones, deep restorations,buccal/lingual restorations (mid-root calcification),root length, width, curvature) affect the angle of entryand the degree of extension of the access cavity in thehorizontal and vertical dimensions.
Radiographic assessment: Angled views should betaken in an attempt to visualize the breadth of the rootsand the centeredness of the canal within it. One also hasto assess the angle at which the canal leaves the pulpchamber—the root may not seem curved but if there is asharp angle between the chamber and the canal, SLA willrequire a significant reduction of the orifice walls. To aidin orientation, the access preparation can be startedwithout rubber dam until the pulp chamber is located.
Access Cavity Preparation
Access cavity design has undergone changes through-out the years. Originally, it was thought that thecavities should be round in anterior teeth, oval inpremolars, and triangular in molars. This gave wayto triangular cavity shapes in anterior teeth and quad-rilateral shapes in molars.25
It was considered acceptable to state ‘‘make accesscavities large.’’ Also, ‘‘make them like an inlay pre-paration,’’ where circumferentially around the accesscavity, every point coronal from the pulpal floor iswider. However, these protocols resulted in excessive,unnecessary tooth structure removal. With the adventof microscopes, visibility has greatly improved and farmore precision is now possible. Therefore, an accesscavity should be made in such a way that only thattooth structure necessary for the objectives of cleaningand shaping is removed, and absolutely no more. Ithas been shown by several researchers that a differenceof 0.5 to 1 mm of the remaining dentin tooth structurecan improve a tooth’s fracture resistance with statisti-cal significance. Sorensen and Engelman26 showed that1 mm of ferrule significantly increased fracture resis-tance, while Libman and Nicholls27 demonstrated thatthere was a significant improvement between 1 and1.5 mm of dentin ferrule height. A 5-year prospectiveclinical study28 showed that the remaining dentinthickness and height affected survivability but foundno difference in survivability among cast post and core,prefabricated post and core, and composite-only cores.Tan et al.29 showed a significant difference between auniform, circumferential 2-mm ferrule and a nonuni-form ferrule with only 0.5 mm proximal but 2 mmbuccal and lingual dentin height (see Chapter 40,Restoration of Endodontically treated Teeth).
It must be remembered that just having remainingouter tooth structure around the access preparation isnot sufficient; the long-term prognosis is more accu-rately assessed after both access preparation andcrown preparation are completed. A developing con-cern is that full porcelain crowns require more dentinremoval to allow adequate strength to the crowns andare becoming more popular due to their improvedesthetics. Therefore, the practitioner should not basethe access cavity design on the ease of visibility, butonly on removing what is absolutely necessary and nomore. The common retort is that restricting the accesscavity will jeopardize the success of the root canaltreatment, as visibility will be impaired. However, itwill be shown that all the objectives necessary forcleaning and shaping can be adequately met, withoutrestriction of visibility or instrument access, as
886 / Endodontics

unnecessary tooth structure removal is avoided. If theaccess cavity has to be extended to facilitate visibility,it should be done with precision.
An access cavity should be considered specific andindividual for each tooth and for each patient, as is aclass II restorative cavity or crown preparation. Theaccess cavity will vary according to the degree ofcurvature within the canal (i.e., the angle at whichthe canal leaves the pulp chamber may be very differ-ent from the root curvature), the position of the canalapex relative to its cusp tip, canal length, degree ofcalcification, size, shape, and position of the tooth inthe jaw. It is suggested that only the initial entry pointon the occlusal table should be based on a standar-dized protocol but once the pulp chamber has beenfound, the cavity should be ‘‘tailor-made.’’
The sequence of steps for access preparation will bediscussed here and can also be followed in Figure 6.The first objective is to penetrate through the occlusalsurface. Penetrating enamel or precious metal is pre-dictable using a high-speed handpiece with a tungstencarbide bur. Porcelain and nonprecious metals, how-ever, present more difficulties, in particular with chip-ping when a steel round bur is used. Diamond burseasily penetrate porcelain but are generally much lessefficient with metal. Stokes and Tidmarsh30 evaluatedthe cutting efficiency of diamond and tungsten car-bide burs through metal crowns. They tested coarsegrit round and dome-ended cylinder diamonds andsix-bladed tungsten carbide cross-cut fissure or roundburs. They found that for precious alloys, tungstencarbide burs were significantly quicker. For the
A B C D E F
G H I J K L
M N
Figure 6 Sequential steps in endodontic access preparation on an extracted lower molar. Initial entry A, with bur is angled toward buccal and distal;narrow entry is sufficient to find the pulp chamber B, A K-file size #10 or #15 is then used to find the position of orifices to determine points of extensionC, Further extension based on the position of orifices D, and a file is now placed into the coronal portion of the canal to determine the location of therestrictive dentin. The restriction can be seen under the microscope at the orifice level, and further extension of the occlusal surface is not warranted atthis time. The buccal surface is undercut to remove the pulp chamber roof minimizing the removal of occlusal dentin/enamel E, Similar extension is donefor lingual, mesial, and distal surfaces F, Large pulp stones are removed by sectioning, not widening the cavity G, Once the restrictive dentin at theorifice is removed, a file starts to contact the entire wall. Now only that slice of dentin contacted by the file from the occlusal surface to the orifice levelis cut with a flared-out angle with a narrow tapered diamond bur H, so that a slot-shaped preparation starts to develop I, This is repeatedly extendedafter checking each time for location of dentinal contact with a file J, Completed access preparation shows straight-line access (SLA) into themesiobuccal K, and mesiolingual canal L, after root canal filling. The fin between the mesiobuccal and mesiolingual canals can be identified under themicroscope as blind-ended. In case of less than ideal visibility, the mesial wall would have to be straightened and flared for deeper access and visibility.M, A clinical example of a file placed at working length (WL) without undue strain from the outer wall and precisely in its slot. A similar clinical exampleshows gutta-percha cones prior to taking master cone radiograph N.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 887

precious alloys, though no difference initially, afterfive cavity preparations, only the dome-ended cylin-der diamond cuts significantly faster than other burtypes. They found the diamond burs to be smootherwith less ‘‘chatter’’ during cutting than the tungstencarbide burs. They concluded that cutting efficiencyappears to relate not only to grit size but to bur shape aswell. Teplitsky and Sutherland31 showed that of the 56porcelain crowns, none fractured after access preparationwith diamond burs, whereas tungsten carbide burs dulledrapidly and were ineffective. Cohen and Wallace32
showed that of the Dicor crowns cemented with zincphosphate, porcelain chipped and the seal was lost afteraccessing. However, when a bondable cement was used(polycarboxylate), none of the crowns lost retention.When penetrating a porcelain-fused-to-metal crown,the porcelain should be removed with a dome-endedcylindrical or a #2 round diamond and the nonpreciousmetal penetrated with a #1 round carbide bur or a tung-sten carbide transmetal bur.
The second objective is to find the pulp chamber. Anarrow opening is maintained initially and the penetrat-ing bur is taken to a premeasured depth gauged bymeasuring the distance between the cusp tip and the pulpchamber roof from the preoperative radiograph. As theaccess preparation has not yet been extended, the clin-ician relies on having premeasured the depth and correctjudgment of the angle of penetration of the bur based onthe parameters described above. If the pulp chamber islarge and the angulation is correct, the bur can be felt to‘‘drop’’ through into the chamber. However, relying onthis feeling is dangerous for it is unpredictable. If thechamber is calcified or deep, the ‘‘drop’’ is often notdiscernable, and unnecessary gouging of the walls orfloor or even perforation can occur, if the clinician isnot exactly on target. Therefore, the bur should penetrateonly to the premeasured distance, and if the chamber isnot found, the access should be minimally extended intoa narrow slot in the anticipated direction of the canalsusing the microscope with good illumination to look forsigns of the chamber. Often a pulp horn may already beexposed or the cavity already overextended in certainspots. Extending the cavity without visualization usuallyresults in unnecessary tooth structure loss, and thereforeextreme care must be paid. When searching for the pulpchamber, tapered instruments should never be forcedbut be allowed to cut their own way with a light touchby the operator. When forced, they will act as a wedge.This may cause the enamel to ‘‘check’’ or ‘‘craze’’ and willmaterially weaken the tooth.
The third objective is to ‘‘unroof’’ the dentin thatcovers the pulp chamber. This is carefully done underthe microscope with a thin needle diamond cylinder
(e.g., #859–010, BrasselerUSA) so as to avoid unneces-sary widening of the isthmus. The bur is angled toundercut the occlusal surface thereby maintaining asmuch tooth structure as possible. Ultrasonic tips canalso be used very precisely to accomplish this. Roundburs should be avoided during access preparation otherthan perhaps for initial penetration as they cause indis-criminate gouging of the walls. Safe-ended cutting burscan be used but their width is rather large for use atthis time. In this step, the clinician depends mostly onthe ‘‘feel’’ of the bur deep inside the tooth, against theroof and walls of the pulp chamber, to judge theextensions that are necessary.
The entire roof of the pulp chamber is removed. In thisoperation high-speed equipment should be operatedwith vision and is not generally employed in a blind areawhere reliance on tactile sensation is necessary.
The fourth objective is to obtain uniform contact ofthe file with the access cavity wall. A file is placed inone of the canals and is viewed under the microscopeto evaluate the specific points along its length where itis being held up by the access cavity or the canal dentin.Then, with a thin needle diamond, only that area of thecavity wall is relieved. The file is reinserted and theprocess repeated until the file contacts dentin evenlyalong its length in the chamber without undue strain. Ifthe restraining dentin is determined to be within thecoronal portion of the canal, GG burs or other instru-ments that can cut a ‘‘relief channel’’ laterally may beused, rather than extend the entire wall.
The fifth objective is to obtain SLA. The clinicianmust assess the degree of taper to be imparted to thedentin access wall in the one line the file is uniformlycontacting. A radiograph can be used to help assess.This single ‘‘slice’’ of dentin is then flared out to anobtuse angle relative to the pulp chamber floor, creat-ing a slot-like extension. All other points of the wallsare kept flared in or undercut or at as acute an angle aspossible that allows complete visibility of the floorwhen viewed under a microscope. The floor andcanals will not be visible in one view—the mirrorhas to be moved.
The diameter of the bur that cuts the slot extensionshould only be the maximum diameter of the largestfile that is necessary at the canal orifice. A taper is notrequired for that part of the access preparationbetween the orifice and the occlusal table as compac-tion forces for obturation will not apply. The ‘‘010’’suffix of cylinder and tapered diamond burs connotesthe maximum cutting shaft diameter is 1 mm and of‘‘012’’ is 1.2 mm, etc. It should be remembered thatwith natural hand movement, the diameter of the cutmade by these burs would be still larger. Therefore,
888 / Endodontics

usually a #859–010 is large enough. The operatorshould also be aware of the maximum diameters ofthe files chosen, for example, GG4 (1.1 mm) andProTaper (1.2 mm). A 35/0.06 Profile is 1.3 mm atD16, which will necessitate a larger access cavity thanis usually required for cleaning and shaping. An ori-fice diameter can generally be maintained between 0.9and 1.1 mm for adequate cleaning and shaping whileminimizing the loss of root strength.
The canal access slot is continually moved to theouter surface to prevent cutting on the furcal surfaceduring cleaning and shaping as the larger files thatrequire more and more space are introduced.
The mesiodistal width of the access preparation canbe kept as small as possible. It has been shown thatthe average dimensions between walls at the pulpchamber floor are 2.2 mm mesiodistally and 5.1 mmbuccolingually.20 Examples of basic access cavity pre-parations, before individual slot extensions for SLA, aswell as plates covering common clinical errors, may beseen on the DVD accompanying this text.
Maxillary Central Incisors
ANATOMY AND MORPHOLOGYThe tip of the root and the incisal edge are on themidline from a proximal view (Figure 7).33 It is veryrare for these roots to have true second canals34,35 butquite common to have lateral canals. The roots arestraight and have the least incidence of dilacerations.36
Kasahara et al.37 used 510 extracted maxillary centralincisors with no abnormalities and decalcified them innitric acid for 48 hours. They suggested that over 60%showed accessory canals that were impossible to cleanmechanically. Most lateral branches were small, 80%were size #10 reamer or less, and 3% were larger thana #40 reamer. Eighty percent of all apical foramina
were located within 0.5 mm of the apex and 95%within 1 mm.
There are many case reports showing two canals(and one showing four canals) but usually thecrowns and/or roots are unusually large, suggestingfusion, gemination, or presence of a dens-in-dente.However, case reports of maxillary centrals withtwo roots/canals and normal crowns have beenreported.38,39
CLINICALInitial penetration should be approximately in themiddle of the lingual surface of the tooth, just abovethe cingulum almost perpendicular to the lingual sur-face. After locating the canal, long tapered diamondscan be used to extend the access into a roughly trian-gular outline. However, this extension when carriedout under the microscope can be made precisely toeach tooth to only uncover the pulp chamber andhorns and to provide continuous smooth walls downthe chamber into the canal.
Even though it has been shown that a better SLAcan be achieved through an incisal access cavity,18
the lingual approach is used in order to maintainas much tooth structure on the labial surface aspossible for esthetic reasons. The reciprocal com-promise is that a lingual triangle is formed, whichhas to be removed to achieve SLA. In fact,LaTurno and Zillich18 showed that only 10% ofthe 50 maxillary central canals examined projectedsolely onto the lingual surface with an SLA. Eighty-four percent of the configurations involved at leastthe incisal edge and 6% were solely on the buccal(Figure 8).
After initial penetration into the chamber, theaccess cavity has to be extended precisely in both thelabiolingual and mesiodistal dimensions. In the labio-lingual plane, there are two particular areas generallydescribed as the lingual and labial triangles that have
Chapter 27 / Preparation of Coronal and Radicular Spaces / 889

to be removed to obtain an SLA. However, the lab-ial triangle can often be a quadrilateral as shown inFigure 9.
With regard to mesiodistal extension, all accesscavities should uncover the pulp horns, but specialattention has to be paid to the maxillary incisors asthe pulp horns are not in the direct line of vision of
the access cavity. If even minute amounts of tissueremain in the pulp horns, they will subsequently dis-color the remaining tooth structure over time. Com-plete extensions can be accomplished by feeling theextension of the pulp horns under each mesial anddistal angle with a cowhorn explorer (HuFriedy). Fineextensions that require opening with a half-round
A
B
Figure 7 Example of a maxillary central incisor showing labial, mesial, and incisal views A, The access preparation can be assessed from a more incisalview and a lingual view B, The width of the preparation in the cingulum is 1.1 mm. Note also the extension of the mesial and distal incisal areas to openup the pulp horns.
890 / Endodontics

carbide bur often occur. These extensions should beblended into the main access chamber so that residualdebris, sealer, or gutta-percha does not becometrapped and cause discoloration. Younger patientshave more pronounced pulp horns and require parti-cular care to remove the remaining potential tissue.
Due to the lingual approach, the points of restrictionon the files are against the coronal portion of the lingualwall and the most incisal portion of the labial wall.Khademi40 suggests notching the midpoint on the labialpreemptively to accommodate the larger files more easily.
There is a debate as to how far the incisal extensionshould be taken. As we know that most anterior teethhave a better SLA from the buccal or the incisal surface,the operator has to assess on a case-by-case basis andsometimes the extension will be more aggressive thanothers.
Maxillary Lateral Incisors
ANATOMY AND MORPHOLOGYThese teeth have a function very similar to centralsand are therefore similar except for a smaller scale inall dimensions except root length. They have morerounded incisal angles and the root typically curves tothe distal although some can be straight or curving tothe mesial. There is often a deep developmentalgroove running along the cingulum on the lingualsurface.33
Again it is very rare to find more than onecanal,34,35 but several case reports have shown morecanals with separate apices.41–44 The pulp horns maynot be quite as pronounced, but the concept of lingualshelf removal and extending the pulp horns till it canbe verified with a cowhorn explorer that the angles aresmooth still holds.
Regarding SLA, LaTurno and Zillich18 as well asZillich and Jerome17 showed that of the 131 teethexamined, only 0.8% of canals had a coronal projec-tion that was entirely lingual and did not involve theincisal or buccal surfaces with 16% entirely on thebuccal (see Figure 9). Therefore, the clinician shouldbe more fastidious about the removal of the lingualtriangle for these teeth. Compounding the difficultyof achieving SLA from a lingual approach is thatthese teeth tend to have a curvature to the distal.
It must also be noted that incisors can have manyanomalies that severely increase the difficulty in treat-ment of these cases, for example, radicular palatalgrooves, fusion with supernumerary teeth, gemina-tion, dens invaginatus, dens evaginatus, incompleteapical closure; it is beyond the scope of this chapterto cover these treatment protocols.
A B
Figure 8 Impact of initial entry into pulp chambers of incisor teeth, fromlabial (1) to incisal (2) and the usual oral access (3). A, Schematicdiagrams for maxillary and mandibular incisors. B, Original micrographswith access from incisal (top) and oral (bottom). Reprinted with permis-sion from Sonntag D et al.6
Chapter 27 / Preparation of Coronal and Radicular Spaces / 891

A B C
D E F
Figure 9 Potential design of access into a maxillary incisor with schematic drawings based on an original radiograph A, The preoperative relation of thecanal within the root can be estimated B, note how the true straight-line access (SLA) is labial to the incisal edge C, The initial access entry site andangulation D, tan-colored highlights) show the restrictive dentin impeding SLA. The completed lingual access preparation with SLA E, can be comparedto a completed access preparation done from a labial approach F, Note how far more tooth structure may be conserved with a labial access but at thecost of disrupting the labial esthetic surface.
892 / Endodontics

Maxillary Canines
ANATOMY AND MORPHOLOGYThe labiolingual measurement of the crown is about1 mm greater than that of the maxillary central incisorand the mesiodistal measurement is approximately1 mm less (Figure 10). The position of the cusp tip
relative to the long axis of the root is in line with thecenter of the root tip in the labial view but lies labialin the proximal view.33 LaTurno and Zillich18 showedthat none of the 48 maxillary canines examined pro-jected solely onto the lingual surface with an SLA.About 98% of the configurations involved the incisaledge (of which 43% involved incisal and lingual) and2.1% were purely on the buccal. Usually one root
A
B
Figure 10 Example of a maxillary canine showing labial, mesial, and incisal views A, The access preparation can be assessed from a more incisal viewand a lingual view B.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 893

canal is present,34,35 but cases with two canals havealso been reported45 (see Figure 8).
CLINICALThese teeth have a point of entry just about thecingulum with the tip of the bur aiming for the centerpoint at the CEJ level. The occlusal outline form isoval as the single pulp horn does not tend to fan outto the mesial or distal; however it is broad labiolin-gually. Again, this is checked with a cowhorn explorerand is adjusted according to the individual tooth. Theextension to the buccal or lingual is done only asnecessary to clearly uncover the horns and to allowunheeded insertion of any file.
It is usually the longest tooth and the largest root inthe mouth and is critical to the occlusion. The canaloften curves apically. As with the central and lateralincisors, the lingual triangle must be removed. Themain difficulty with these teeth is that they can belong—often over 30 mm. This will affect the accesscavity in that to provide an adequate apical prepara-tion size, SLA becomes more important.
Maxillary First Premolars
ANATOMY AND MORPHOLOGYFrom the occlusal aspect, the tooth resembles roughlya hexagonal structure, and it is much broader bucco-lingually than mesiodistally (Table 1, Figure 11). As inall posterior maxillary teeth, the measurement fromthe buccal cusp tip to the lingual cusp tip is less thanthe buccolingual measurement of the root at its cer-vical level. As more of the buccal cusp is seen than thelingual, the access preparation is angled buccallyinto the cervical areas but not extended to the samedegree on the occlusal table. There is a marked
Table 1 Summary of Studies Detailing Root and Root Canal Anatomy of Maxillary First Premolars
Author Year
Number
ofTeeth
Method
One
Coronal
Canal
Two
Coronal
Canals
Three
Coronal
Canals
One
Apical
Foramen
Two
Apical
Foramina
Three
Apical
Foramina
Carns46 1973 100 Vacuum-drawn polyester cast resin, decalcified 9% 85% 6% 22% 72% 6%
Vertucci 47 1979 400 Decalcified, dye injected, cast in resin, microscope 8% 87% 5% 26% 69% 5%
Walker48 1987 100 Radiographic in vitro 13% 87% 0% 36% 64% 0%
Pecora49 1991 240 Decalcified, India ink-dyed, gelatin injection 17.1% 80.4% 2.5% Not specified Not specified Not specified
Caliskan45 1995 100 Dyed, decalcified, stereomicroscope x12 4% 97% 0% 10% 90% 0%
Kartal50 1998 300 Decalcified, ink dye, microscope x0.6–4 8.66% 89.64% 1.66% 9.66% 88.64% 1.66%
Pineda34 1972 259 Radiographic in vitro 26.2% 73.3% 0.5% 50.1% 49.4% 0.5%
Kerekes51 1977 20 Sectioned, microscope 10% 80% 10% 10% 80% 2%
Bellizzi52 1985 514 Radiographic in vivo 6.2% 90.5% 3.3% Not examined Not examined Not examined
Green53 1973 50 Ground sections, microscope 8% 92% 0% 34% 66% 0%
Sert54 2004 200 Decalcified, dyed 10.5.% 85% 4.5% 28.5% 68.5% 3%
A
B
Figure 11 Example of a maxillary first premolar showing buccal, mesial,and occlusal views A, and a typical access preparation B, Note how thebuccal part of the preparation has been extended mesiodistally toexplore a potential second buccal canal.
894 / Endodontics

developmental depression on the mesial surface thatextends from just below the mesial contact pointbetween the roots and ends at the bifurcation. Thereis also a well-defined developmental groove in theenamel of the mesial marginal ridge that runs intothe central groove on the occlusal table. This can bedeceiving during access as off-angulation of the burcan result in perforation. It must be assumed that atleast two canals are present, and the third canal isshown to exist in high enough numbers that theaccess preparation must be designed to search for it(either mesiobuccal or distobuccal canals, abbreviatedMB or DB). When three canals are present, the pulpchamber morphology resembles that of a maxillarymolar, and they have been termed ‘‘mini-molars.’’The width of the access can be kept minimal betweenthe canal orifices.
CLINICALThe point of entry is centrally in the fossa, aiming atthe center point at the CEJ. The outline is an elon-gated slot and can extend almost to the cusp tipsdepending on the angle. However, the operator mustsearch for a third canal—usually the mesiobuccalcanal. If three canals are found, the orientation is verysimilar to that of the maxillary molar (Figure 12).
Maxillary Second Premolar
ANATOMY AND MORPHOLOGYThe occlusal table is very similar to that of the firstpremolar (see Figure 11), presenting without a
A
B
Figure 12 Two examples of maxillary first premolars with three canals that were endodontically treated. A clinical view of the access cavity is provided in A.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 895

depression in the mesial root surface (Figure 13). It hasa more rounded crown form and has a single rootwhen compared with the first premolar. Internally,the incidence of two canals is significantly less but
when present they are not spaced so far apart fromeach other.
Maxillary First Molar
ANATOMY AND MORPHOLOGYIt is the largest tooth in the maxillary arch with fourwell-defined cusps and a supplemental cusp of Cara-belli of the mesiolingual cusp (Tables 2–4, Figure 14).From the occlusal view, it has a roughly rhomboidaloutline. The distobuccal cusp becomes progressivelysmaller on the second and third maxillary molars.There are two major fossae (central fossa mesial tothe oblique ridge and the distal fossa distal to theoblique ridge) and two minor fossae (the mesial anddistal triangular fossae that lie just distal to themesial marginal ridge and just mesial to the distalmarginal ridge, respectively). The oblique ridgecrosses the occlusal surface from the ridge of thedistobuccal cusp to the distal ridge of the mesiolin-gual cusp.
CLINICALFor the purpose of access cavities, the molars can beviewed as having a triangular arrangement of the
Table 2 Summary of Studies Detailing Root and Root Canal Anatomy of the Mesiobuccal Root of First Maxillary Molars
Author Year
Number
of Teeth Method
One
Coronal
Canal
Two
Coronal
Canals
Three
Coronal
Canals
One
Apical
Foramen
Two
Apical
Foramina
Three
Apical
Foramina
Gilles55 1990 21 SEM and decalcified, injected ink dye,
microscope
9.5% 90.5% 61.9% 38.1%
Buhrley56 2002 58 Clinically in vivo & Microscope 28.9% 71.1% Not examined Not examined
Fogel57 1994 208 Clinically in vivo and loupes, headlamps 29.8% 71.2% 68.3% 31.7%
Pomeranz58 1974 71 In vivo clinical 72% 28% 0% 89% 11% 0%
Seidberg59 1973 100 Sectioned 38% 62% 0% 75% 25% 0%
Thomas60 1993 216 Radiography ex vivo—radiopaque
infusion of canals
26.4% 61.1% 12.5% 53.7% 33.8% 12.5%
Kulild61 1990 51 Ex vivo accessed, ground sections,
microscope
3.9%% 96.1% 0% 54.2% 45.8%
Al-Shalabi62 2000 83 Dye, decalcified, cleared, microscope
x20 magnification
19.3% 79.5% 1.2% 34.9% 63.9% 1.2%
Vertucci35 1984 100 Decalcified, dye injected, cast in resin,
microscope
45% 55% 0% 82% 18% 0%
Pineda34 1972 262 Radiographic ex vivo 39.3% 60.7% 0% 51.5% 48.5% 0%
Caliskan45 1995 100 Dyed, decalcified,
stereomicroscope x12
34% 66% 0% 75% 25% 0%
Weine63 1999 300 Radiographic ex vivo 42% 58% 0% 66.2% 33.8% 0%
Alavi64 2002 52 Dyed, decalcified 32.7% 65.4% 1.9% 53.8% 46.2% 0%
Imura65 1998 42 Root canal treatment ex vivo, decalcified 19% 81%‘ 0% 28.6% 71.4% 0%
Sert54 2004 200 Decalcified, dyed 6.5% 92.5% 1% 61% 39% 0%
Weine66 1969 208 Sectioned 48.6% 51.4% 0% 86.1% 13.9% 0%
Stropko67 1999 168 Clinically in vivo (microscope only) 13.1% 86.9% 0% 54.8% 45.2% 0%
Wasti68 2001 30 Decalcified, ink dye, x10 dissecting microscope 33.3% 66.7% 0% 56.6% 43.4% 0%
Ng69 2001 90 Ink dye, decalcified 30% 67.8% 2.2% 57.8% 41.1% 1.1%
Figure 13 Example of a maxillary second premolar showing buccal,mesial, and occlusal views. The access preparation is virtually identicalto the one of maxillary first premolar (see Figure 11).
896 / Endodontics

Table 3 Summary of Studies Detailing Root and Root Canal Anatomy of the Distobuccal Root of First Maxillary Molars
Author Year
Number
of Teeth Method
One
Canal
Coronally
Two
Canals
Coronally
Three
Canals
Coronally
One
Apical
Foramen
Two
Apical
Foramina
Three
Apical
Foramen
Thomas60 1993 208 Radiography ex vivo, radiopaque infusion of canals 95.7% 2.4% 1.9% 96.2% 1.9% 1.9%
Al-Shalabi62 2000 81 Dye, decalcified, cleared, microscope x20 magnification 97.5% 2.5% 0% 97.5% 2.5% 0%
Vertucci35 1984 100 Decalcified, dye injected, cast in resin, microscope 100% 0% 0% 100% 0% 0%
Pienda34 1972 262 Radiographic ex vivo 96.4% 3.6% 0% 96.4% 3.6% 0%
Caliskan45 1995 100 Dyed, decalcified, stereomicroscope x12 98% 2% 0% 98% 2% 0%
Alavi64 2002 52 Dyed, decalcified 98.1% 1.9% 0% 100% 0% 0%
Sert54 2004 200 Dyed, decalcified 90.5% 9.5% 0% 97% 3% 0%
Wasti68 2001 30 Decalcified, ink dye, x10 dissecting microscope 83.3% 16.7% 0% 83.3% 16.7% 0%
Ng69 2001 90 Ink dye, decalcified 94.5% 4.4% 1.1% 97.8% 1.1% 1.1%
Table 4 Summary of Studies Detailing Root and Root Canal Anatomy of the Palatal Root of First Maxillary Molars
Author Year
Number
of Teeth Method
One
Canal
Coronally
Two
Canals
Coronally
Three
Canals
Coronally
One
Apical
Foramen
Two
Apical
Foramina
Three
Apical
Foramen
Thomas60 1993 216 Radiography ex vivo, radiopaque infusion of canals 97.7% 2.3% 0% 98.2% 1.8% 0%
Al-Shalabi62 2000 82 Dye, decalcified, cleared, microscope x20 magnification 98.8% 1.2% 0% 98.8% 1.2% 0%
Vertucci35 1984 100 Decalcified, dye injected, cast in resin, microscope 100% 0% 0% 100% 0% 0%
Pineda34 1972 262 Radiographic ex vivo 100% 0% 0% 100% 0% 0%
Caliskan45 1995 100 Dyed, decalcified, stereomicroscope x12 93% 7% 0% 97% 3% 0%
Alavi64 2002 52 Dyed, decalcified 100% 0% 0% 100% 0% 0%
Sert54 2004 200 Dyed, decalcified 94.5% 4% 1.5% 96% 2.5% 1.5%
Wasti68 2001 30 Decalcified, ink dye, x10 dissecting microscope 66.7% 33.3% 0% 66.7% 33.3% 0%
Ng69 2001 90 Ink dye, decalcified 100% 0% 0% 100% 0% 0%
Figure 14 Example of a maxillary molar shown in buccal, mesial palatal and occlusal views. A, Access into both mesiobuccal canals and distobuccal andpalatal canals is gained B, Note that the preparation has not been extended much on the occlusal table for the distobuccal canal as the canal projectsdistally naturally. All canals accept a size #40 or #50 hand file to working length (WL); access preparations may have to be extended further slightly toaccommodate larger step-back files.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 897

cusps (without the distolingual cusp). In fact theaccess cavity is made without encroaching ontothe distolingual cusp and is usually kept mesial tothe oblique ridge.
Maxillary molars are widely recognized as beingone of the most difficult teeth to treat endodontically.They can present with mild to severe curvatures andusually have two or three canals in any root (but mostcommonly in the mesiobuccal root). Locating thesecond mesiobuccal canal (MB2) orifice routinely canbe difficult as it is often buried under a bridge ofdentin. The canal can have a severe curvature tothe mesial and the buccal in its coronal section andis usually much smaller than the principal first mesio-buccal canal (MB1) (Figure 15). A dentin bridge mayoccur due to the secondary dentin formation fromaging and/or reparative dentin from carious attack orrestorative procedures. This secondary or reparativedentin is usually whiter than the pulpal floor and canbe selectively removed under magnification. The accessshape should be quadrilateral to allow for troughing2–3 mm lingual to MB1 to search for MB2 (Figure 16).The clinician should keep an eye on the mesial externalroot surface as a guide to avoid perforating furcally ormesially. Endodontists have reported troughing wellover 4 mm below the pulpal floor before uncoveringthe MB2 orifice. In the following, each root will bedescribed separately (Figure 17).
In principle, all maxillary molars can be accessedfollowing a similar strategy. Entry should be in themesial fossa and should be kept small initially. Under
Figure 15 A, B, Schematic diagrams of maxillary molar access preparation based on the original radiograph C, Access penetration and angulation showsan initial narrow opening on the occlusal surface. D, E, Dentin (blue areas) is removed carefully so that a file can stand upright to show exactly where theaccess preparation must be extended further. Note how the distobuccal wall does not need to be extended significantly as it naturally projects distally.
Figure 16 Variations in access cavity shapes in maxillary molars.
898 / Endodontics

higher-power magnification, it can be extended selec-tively. Initial penetration may be aimed at the largepalatal canal orifice. There is ample evidence todemonstrate that the mesiobuccal root has a secondcanal with such frequency that it must be accommo-dated for in the initial access and always searched for.In vivo, Stropko67 reported finding two canals in73.2% of first molars before using the microscopeand 93% after; 90% of the MB2s were negotiable tothe apex. He classified it as a canal if he could instru-ment 4 mm into it. Baldassari-Cruz et al.70 locatedMB2 canals in 51% of the cases with the naked eyecompared to 82% with the microscope.
Gilles and Reader55 found that the mean distance ofMB2 orifice from MB1 was 2.31 mm (range 0.7 to3.75 mm). Kulild and Peters61 found that the distancebetween MB1 and MB2 was on average 1.82 mm andthe orifice was to the lingual of MB1. However, theMB2 orifice can sometimes be found close to or evenin the palatal canal orifice (Figure 18). While twomesiobuccal orifices are most common, three can alsobe present (Figure 19).
The mesiobuccal canals have two separate apicalforamina or, more commonly, join to exit at one fora-men (Figure 20). In contrast, the distobuccal root isconical and usually straight but may have a slightcurvature to the mesial. Although far more infrequentthan the mesiobuccal root, the distobuccal root canalso have a second canal that almost invariably joinsthe main (DB) canal to a common apex. It can befound lingually to the main canal and usually in avisible fin connecting the DB canal to the palatal canal.The incidence of two DB canals ranges from 2% to 9%.
The access preparation for the DB canals does nothave to be extended as far toward its line angle as themesial canals. The distal canal is distally inclined andso the file projects out of the orifice to the mesialnaturally. Therefore, the transverse ridge can usuallybe preserved (see Figure 15).
The palatal root is broad mesiodistally and its canalmirrors it. Therefore the access should be extendedmesiodistally. The extent to which it has to beextended palatally can be deceiving as the orifice cor-onally projects palatally naturally and therefore thefile does not seem to contact the palatal wall towardthe orifice. However, the apical third often curves tothe buccal, and to reach the apex with large files, oneneeds to extend the palatal wall slot palatally and flarethe coronal mid thirds of the canal. Again, a file isinserted and only that area of the dentin that contactsthe file is removed to achieve SLA. This can also beaccomplished using an ultrasonic tip.
Figure 17 A, The isthmus between the two mesiobuccal canals istroughed and no further fin or isthmus is evident. B, Measurement oftroughing depth with a periodontal probe gives the practitioner anobjective perspective. C, Incorrect angulation of ultrasonic tip duringtroughing due to inadequate extension of the mesial wall resulting in theremoval of furcal dentin.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 899

Figure 18 The MB2 canal can be located anywhere along the fin betweenthe MB1 and palatal canals. A, Second mesiobuccal orifice was found inthe entrance (arrowhead) to the palatal canal and shows how the custom-ary extension was inadequate. B, Obturation and the distance betweenMB1 and MB2. C, Proximity of MB2 to the palatal orifice.
A
B
C
Figure 19 Clinical examples of maxillary molars with three mesiobuccalcanal orifices.
900 / Endodontics

Also the palatal canal can split into two, and thereforethe access preparation needs be extended mesiodistally(Figure 21). In such oval-shaped canals,8 simple instru-mentation with round cross-section files will not suffice forcomplete debridement of the canals (see Figure 14A).
Maxillary Second Molars
ANATOMY AND MORPHOLOGYMaxillary second molars are very similar in form andfunction to the maxillary first molars with some varia-tions (Table 5). The mesiobuccal and mesiolingual cuspsare larger but the distobuccal and distolingual cusps aresmaller. The cusp of Carabelli is usually absent. The
buccolingual diameter of the crown is about equal tothe first, but the mesiodistal diameter is approximately1 mm less. There are two types of maxillary secondmolars when viewed from the occlusal aspect:
(1) Rhomboidal: four-cusp outline similar to the firstmolars but more rounded. This is the morecommon form.
(2) Triangular: three-cusp form more similar to thethird molar form where the distolingual cusp ispoorly developed.
The roots are usually closer together than the firstmolar’s and can also have two or three fused roots.The canal system can vary from one large canal, twocanals, or three or four canals. The palatal root can
Figure 20 Radiographs illustrating possible variations in the anatomy of mesiobuccal root canal system of maxillary first molars. A, Two canals joiningin the coronal root canal third. B, Widely separated canals but joining to a common apex. C, Separate apical foramina.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 901

Figure 21 Radiographs illustrating variations in the palatal root canal anatomy. A, First molar showing one wide canal. B, Two canals in another firstmaxillary molar. C, Apical bifurcations in the palatal root.
Table 5 Summary of Studies Detailing Root and Root Canal Anatomy of the Mesiobuccal Root of Second Maxillary Molars
Author Year
Number
of Teeth Method
One
Coronal
Canal
Two
Coronal
Canals
Three
Coronal
Canals
One
Apical
Foramen
Two
Apical
Foramina
Three
Apical
Foramina
Vertucci35 1984 100 71% 57% 2% 76% 23% 1%
Pomeranz58 1974 29 Clinical in vivo 62% 38% 0% 76% 24% 0%
Caliskan45
Sert54 2004 200 Decalcified, dyed 41% 57% 2% 76% 23.5% 0% (0.5%
four foramina)
Pineda34 1972 294 64.6% 35.4% 0% 72.8% 27.2% 0%
Eskoz71 1995 67 Radiographic in vitro 59.7% 40.3% 0% 80.6% 19.4% 0%
Gilles55 1990 37 SEM and decalcified, injected ink dye, microscope 29.7% 70.2% 0% 62.1% 37.8% 0%
Kulild61 1990 32 6.3% 93.7% 54.2% 45.8%
Buhrley56 2002 36 Clinically in vivo, microscope 63.9% 36.1%
Alavi64 2002 65 Dyed, decalcified 41.5% 55.4% 3.1%% 53.8% 44.6% 1.5%
Imura65 1998 30 Root canal treatment ex vivo, sectioned, decalcified 33.3% 66.7% 0% 53.3% 46.7% 0%
Ng69 2001 77 Ink dye, decalcified 49.3% 48.1% 2.6% 74% 26% 0%
902 / Endodontics

also have two separate roots with separate canalswithin each. The occlusal table is smaller.
CLINICALAccess is more complicated due to the tooth being furtherback in the arch and more difficult to reach. Shorter lengthburs may sometimes be needed. Gilles and Reader55 foundthat the mean diameter of the MB2 orifice in the secondmolars was 0.42 mm with a range of 0.15 to 1.00 mm. Themean distance from MB1 orifice to MB2 orifice was2.6 mm (range 0.9 to 3.9 mm). The distobuccal canalcan sometimes be hidden under a large shelf of dentin.The orifice appears on the same line joining the mesio-buccal and palatal canals. However, during cleaning andshaping, the shelf must be carefully removed so that thefurcal surface is not encroached upon.
The palatal root usually has one canal, as describedin vitro (see Table 6–18). Peikoff et al.72 found in vivo
that only 1.4% of maxillary second molars had twopalatal roots and two palatal canals.
Maxillary Third Molars
ANATOMY AND MORPHOLOGYFrom an occlusal viewpoint, this tooth usually pre-sents with a heart-shaped triangular outline similarto the second molar. The distolingual cusp is typi-cally small and often completely absent. Unlike themandibular third molars, these teeth tend to haveunderdeveloped crowns. The roots are often fusedforming one large root.
CLINICALAlavi et al.64 found that 50.9% of third maxillarymolars had three separate roots of which 45.5% had two
Table 6 Summary of Studies Detailing Root and Root Canal Anatomy of Mandibular Incisors
Author Year ToothNumberof Teeth Method
One
CoronalCanal
Two
CoronalCanals
Three
CoronalCanals
One
ApicalForamen
Two
ApicalForamina
Three
ApicalForamina
Rankine-Wilson73 1972 Both 111 Radiographic ex vivo 59.5% 40.5% 94.6% 5.4%
Pineda34 1972 Central 179 Radiographic ex vivo 72.4% 26.6% 97.9% 2.1%
Lateral 184 Radiographic ex vivo 76.2% 23.8% 98.7% 1.3%
Madeira74 1973 Central 683 Dyed, rendered
transparent
by clearing agents
88.7% 11.3% 99.7% 0.3%
Lateral 650 Dyed, rendered
transparent
by clearing agents
88.2% 11.9% 99.3% 0.8%
Benjamin75 1974 Both 364 Radiographic ex vivo 58.6% 41.4% 98.7 1.3%
Vertucci35 1984 Central 100 Decalcified, dye injected,
cast in resin, microscope
70% 30% 97% 3%
Lateral 100 Decalcified, dye injected,
cast in resin, microscope
75% 25% 98% 2%
Caliskan45 1995 Central 100 Dyed, decalcified,
stereomicroscope x12
69% 29% 2% 96% 2% 2%
Lateral 100 Dyed, decalcified,
stereomicroscope x12
69% 31% 98% 2%
Kartal76 1992 Both 100 Dyed, decalcified,
cleared, microscope
55% 44% 1% 92% 7% 1%
Miyashita77 1997 Both 1,085 Ink dye, decalcified,
naked eye
87.6% 12.4% 98.3% 1.7%
Sert54 2004 Central 200 Decalcified, ink dye 33.5% 65% 2.5% 87% 11% 2%
Lateral 201 Decalcified, ink dye 36.8% 62.7% 0.5% 90% 9.5% 0.5%
Bellizzi78 1983 Central 254 Radiographic in vivo 83.1% 16.9% Not
examined
Not
examined
Lateral 163 Radiographic in vivo 79.8% 20.2% Not
examined
Not
examined
Walker79 1988
Central 100 Radiographic ex vivo 78% 22% 99% 1%
Lateral 100 Radiographic ex vivo 68% 32% 99% 1%
Green53 73 Both 500 Ground sections, microscope 79% 21% 96% 4%
Al-Qudah80 06 Both 450 Decalcified, cleared, naked eye 73.8% 26.2% 91.4% 8.7%
Chapter 27 / Preparation of Coronal and Radicular Spaces / 903

or more canals in the mesiobuccal root. About 45.7% hadfused roots, 2% had C-shaped canals, and 2% had fourseparate roots. Therefore, modifications must be made inaccessing these teeth compared to first and second molarsto accommodate these anatomical variations.
Mandibular Central and Lateral
Incisors
ANATOMY AND MORPHOLOGYThe mandibular central incisor is usually the smal-lest tooth in the mouth, having a little more thanhalf the mesiodistal diameter of the maxillary centralincisor; however, the labiolingual diameter is onlyabout 1 mm less (Table 6, Figure 22). Bilateralsymmetry is usually evident with central incisors.33
There are slight differences between central and lat-eral incisors, but the most important with regard toaccess is that the crowns of lateral incisors are not assymmetrical as central incisors from the incisal viewas they curve distally to accommodate the curvatureof the arch and correspondingly the cingulum isdisplaced slightly to the distal. Lateral incisors arealso slightly larger than the centrals; this is thereverse relationship found in the maxillary incisors.33
The incisal edge relative to the long axis of the rootin the proximal view is lingually placed—this is clini-cally corroborated by LaTurno and Zillich’s study.18
However, this should have little bearing on the accesspreparation, and the two teeth can be approached withthe same criteria. It is important to note that often themost bulbous or the broadest lingual aspect of thetooth is below the free gingival margin. Therefore,using the free gingival margin to determine the extentof lingual extension of the access cavity can leave itunderextended. One has to use a probe to palpate thecontour of the crown below the free gingival margin.
CLINICALAccording to LaTurno and Zillich,18 incisors do nothave SLA projections entirely on the lingual; all invol-ved the incisal edge and/or the facial surface (6%projected completely onto the buccal) (see Figure 8).Mauger et al.81 in a similar study found that an idealSLA was at the incisal edge in 72.4% and in 27.6% wasfacial of the incisal edge. They also found that as the
wear of the incisal edge increased, the ideal accessmoved from the facial toward the incisal. Similarly,Sonntag et al.6 showed that a shift toward the incisaledge resulted in more adequate preparation and infact less loss of hard tissue.
The entry point for access should be just above thecingulum with the bur angled perpendicularly to thesurface of the entry point. As these teeth are narrowmesiodistally, the main concern is the width of thepreparation. No more than a #1/2 round bur or a longthin cylindrical diamond is used to initiate the access,followed by a cylindrical diamond bur to extend onlyas a slot in a labiolingual dimension. The main pointbeing that unnecessary extension toward the mesio-distal surface is avoided. Even the thinnest bur willprovide an adequate width once collateral handmovement is taken into account. The disadvantage isof course that visibility is restricted and therefore theuse of microscopes becomes paramount.
Once the chamber or the canal is found, the accesscan be precisely widened for each individual toothaccording to its SLA projection. The other point isthat 40% of mandibular incisors have two canals—buccal and lingual with only 2 to 3% having separateapical foramina (Figure 23). The lingual is by far theharder to locate because the angulation of these teethin the jaws is proclined (see Figure 2). It is natural forthe hand to angle the bur toward the buccal (therebyrunning the risk of gouging the labial wall). Thelingual canal lies 1 to 3 mm away from the buccal,directly under the cingulum. Even when two canalsare present, there is often a fin or a groove with pulptissue between them (see Figure 23).
In summary, finding extra canals requires convic-tion that they are there and extending the access tolook for them. Although the two canals seldom exit asseparate apices, bacterial by-products from the necro-tic tissue in the unfilled canal can communicate withthe periodontal ligament via lateral canals or througha poor apical seal.
Mandibular Canines
ANATOMY AND MORPHOLOGYThese teeth are very similar to their maxillary coun-terparts and can be described in relation to them
904 / Endodontics

A
B
Figure 22 A, Example of a mandibular incisor showing labial, mesial, and incisal views. B, The access preparation can be assessed from a more incisalview and a lingual view. Note how the lingual extension of the access preparation extends well into the cingulum.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 905

(see Figure 18A). Mandibular canines are usually nar-rower than maxillary canines (approximately 1 mm) andshorter in root length by 1 to 2 mm (Figure 24). Themesial edge is almost straight and therefore the accesscavity can be prepared more to the mesial of the centerpoint of the lingual surface. Also the cusp tip is inclinedmore to the lingual, similar to the incisors.33 Accordingto LaTurno and Zillich,18 none have SLA projectionsentirely to the lingual; 90% involved the incisal edge orincisal edge and buccal surface with 4% entirely on thebuccal. Canine crowns are asymmetrical with a larger
distal half. Therefore, the access preparation can bestarted just slightly to the mesial of the mid-point mesio-distally, and checked that it corresponds to the centerpoint at the CEJ. Similar to their maxillary counterparts,mandibular canines extend buccolingually, albeit to asmaller extent.
Heling et al.82 reported a mandibular canine withtwo roots and three canals but did not state whethertwo or three apical foramina were present. Orguneserand Kartal83 reported a case of a three-canal mandibu-lar canine with two apical foramina.
Figure 23 Radiographs illustrating variations of lower incisors with two canals. A, Although usually both canals exit from a common apex, they can,B, have two separate or a figure eight-shaped foramen.
906 / Endodontics

CLINICALThe shape of the preparation ranges from an oval to arounded slot depending on the size of the pulp chamberinside. As canines have large roots, the MAF (Box 1) isalso large (size #40 to #60). Therefore, after creating atapered preparation via step-back or rotary files, the
A
B
Figure 24 A, Example of a mandibular canine showing labial, mesial, and incisal views. B, The access preparation can be assessed from a more incisalview and a lingual view. Note that the access is extended lingually to look for a second, usually lingually located canal.
Box 1 Descriptors of Canal Shaping Procedures
WL Working length
WW Working width
IAF (IAR) Initial apical file/rotary
MAF (MAR) Master apical file/rotary
FF (FR) Final file/rotary
Chapter 27 / Preparation of Coronal and Radicular Spaces / 907

coronal orifice will be larger than for incisors mesiodis-tally (Figure 25).
Mandibular First Premolars
ANATOMY AND MORPHOLOGYThe mandibular first premolars have characteristicsof a small canine because of a sharp buccal cusp(only occluding cusp) and a small lingual cusp thatsometimes resemble a cingulum (Table 7, Figure26). There is a characteristic mesiolingual develop-mental groove that makes the tooth asymmetrical.
From the occlusal view, the outline is diamond-shaped and similar to the mandibular canine. Theseteeth have a variable root anatomy. The crown islingually inclined that makes searching for a lingualcanal difficult. Therefore, the access has to beextended further to the lingual to search for it. Thisfeels counterintuitive, as the lingual cusp is verysmall.
Nallapati88 reported a case where both first andsecond premolars had type V anatomy, that is, threecanals with separate apices, while Baisden et al.85
reported the possibility of C-shaped canal anatomyin mandibular premolars.
Figure 25 Radiographs of a treatment sequence illustrating two canals in a mandibular canine.
Table 7 Summary of Studies Detailing Root and Root Canal Anatomy of Mandibular First Premolars
Author YearNumberof Teeth Method
One
CoronalCanal
Two
CoronalCanals
Three
CoronalCanals
One
ApicalForamen
Two
ApicalForamina
Three
ApicalForamina
Vertucci35,84 78/84 400 Decalcified, dye injected, cast in resin,
microscope
70% 29.5% 0.5% 74% 25.5% 0.5%
Pineda34 72 202 Radiographic ex vivo 69.3% 29.8% 0.9% 74.2% 24.9% 0.9%
Baisden85 92 106 Serial sections, stereomicroscope x12 74% 26% 76% 24%
Caliskan45 95 100 Dyed, decalcified, stereomicroscope x12 64% 30% 6% 75% 19% 6%
Zillich86 73 1,287 Radiographic ex vivo 75.1% 24.5% 0.4% 77.2% 22.5% 0.4%
Yoshioka87 04 139 Ink-dyed, demineralized 80.6% 15.1% 4.3% (three
to four canals)
Not
reported
Not
reported
Not
reported
Sert54 04 200 Decalcified, ink-dyed 60.5% 38.5% 1% 89.5% 9.5% 1%
Green53 73 50 Ground sections and microscope 86% 14% 0% 90% 10% 0%
908 / Endodontics

CLINICALThe entry point is in the middle of the central groove,and the bur is directed to the buccal. Again, the accessshape is an oval slot. As the crown is linguallyinclined, the access cavity will result in the removalof more of the buccal cusp than the lingual(Figure 27).
Mandibular Second Premolar
ANATOMY AND MORPHOLOGYUnlike the maxillary premolars, the mandibular sec-ond premolar is quite distinct from its neighboringfirst premolar (Figure 28). It resembles the first onlyfrom the buccal aspect but is otherwise larger. Thetooth has two forms from the occlusal aspect, themore common three-cusp type and the two-cusp
type. With the three-cusp type, the buccal cusp isthe largest followed by the mesiolingual cusp and thenthe distolingual. The occlusal outline is square. Thetwo-cusp form is more rounded and has a smallerocclusal table. Case reports detailing four89–91 and five92
coronal canals but only one showing four apical for-amina have also been reported.89
CLINICALAccess is similar to first mandibular premolars, takingoverall dimensions into account.
Mandibular First Molars
ANATOMY AND MORPHOLOGYThe occlusal surface of mandibular first molars has onemajor (or central) and two minor (mesial and distal)
A B
Figure 26 A, Example of a mandibular first premolar showing buccal, mesial, and occlusal views. B, The access preparation can be assessed from anocclusal view.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 909

triangular fossae (Tables 8 and 9, Figure 29). Theseteeth usually have two distinct buccal and two lingualcusps and one distal cusp. The buccal cusp tips arelocated more to the midline on the occlusal table com-pared to the lingual cusp tips that are almost directlyover the outer surface at the ‘‘neck’’ of the tooth. There-fore, access preparations often encroach on the buccalcusp tip (mesiobuccal) but rarely onto the lingual.
Mandibular molars are known to have complexanatomy and like their upper counterparts can bedeceptively difficult to treat, as the radiographiccanal anatomy can appear simple in two dimensions.
There are usually four canals but three and fivecanals are well documented and one, two, and sixcanals have been reported. It is important to notethat there is almost always a concavity on the furcalside of both the mesial and distal roots; thereforecare must be taken during cleaning and shaping toavoid strip perforation. The roots start to bifurcate3 mm below the CEJ. This gives a sense of the depthat which furcal perforation is possible. As the accesscavity determines cleaning and shaping, the accesscavity has to be designed to allow for protection ofthe furcal surfaces during instrumentation.
Figure 27 A, B, Two examples of lower first premolars with two canals. C, Photographs of an extracted tooth demonstrate a C-shaped root crosssection and suggest the impossibility of adequately cleaning and shaping the entire canal system.
910 / Endodontics

Both mesial and distal roots are broad and usuallyhave two canals and often have an interconnecting finthat can be extremely variable in its persistence at the
apex. Mannocci et al.100 found that of the 20 mesial rootsobserved with microcomputed tomography, 17 had isth-muses in one or more of the sectioned apical five
Table 8 Summary of Studies Detailing Root and Root Canal Anatomy of the Mesial Root of Mandibular First Molars
Author Year
Numberof
Teeth Method
OneCoronal
Canal
TwoCoronal
Canals
ThreeCoronal
Canals
FourCoronal
Canals
OneApical
Foramen
TwoApical
Foramina
ThreeApical
Foramina
FourApical
Foramina
Gulabivala93 2002 118 Vacuum applied, dyed,
decalcified, methyl
salicylate
3.4% 89.8% 5.9% 0.8% 35.6% 60.2% 3.4% 0.8%
Sert54 2004 200 Decalcified and dyed 2% 94% 4% 51% 47.5% 1.5%
Zaatar94 1998 49 Vacuum-drawn Duralay resin 6.2% 91.8% 2% 63.3% 36.7% 0%
Skidmore95 1971 45 Vacuum-drawn polyester
cast resin, decalcified
6.7% 93.3% 44.4% 55.6%
Pineda34 1972 300 Radiographic ex vivo 12.8% 87.2% 0% 43% 57% 0%
Vertucci35 1984 100 Decalcified, dye
injected, cast in resin,
microscope
12% 87% 1% 40% 59% 1%
Caliskan45 1995 100 Dyed, decalcified,
stereomicroscope x12
~4% ~96% ~3% 37% 56.6% 3.4%
Walker96 1988 100 Radiographic ex vivo 3% 96% 1% 24% 75% 1%
Wasti68 2001 30 Decalcified, ink-dyed, x10
dissecting microscope
0% 96.7% 3.3% 23% 73.7% 3.3%
Pomeranz97 1981 61 Clinical in vivo Not
reported
Not
reported
11.5% Not
reported
Not
reported
1.6% Not
reported
Fabra-
Campos981985 145 Radiographic clinical
in vivo
0% 97.2% 2.8% Not
reported
Not
reported
0%
Da Costa99 1996 199 Decalcified, India ink-dyed
gelatin injection
7.5% 92.7% 54.8% 45.4%
A B
Figure 28 A, Example of a mandibular second premolar showing buccal, mesial, and occlusal views. B, The access preparation can be assessed from anocclusal view.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 911

Table 9 Summary of Studies Detailing Root and Root Canal Anatomy of the Distal Root of Mandibular First Molars
Author Year
Number
of
Teeth Method
One
Coronal
Canal
Two
Coronal
Canals
Three
Coronal
Canals
Four
Coronal
Canals
One
Apical
Foramen
Two
Apical
Foramina
Three
Apical
Foramina
Four
Apical
Foramina
Gulabivala93 2002 118 Vacuum applied, dyed,
decalcified,
methyl salicylate
59.3% 34.7% 5.1% 0.8% 66.9% 28% 4.3% 0.8%
Sert54 2004 200 Decalcified and dyed 53.5% 45.5% 1% 87% 12% 1%
Zaatar94 1998 49 Vacuum–drawn
Duralay resin
8.2%% 91.8% 0% 83.7% 16.3%% 0%
Skidmore95 1971 45 Vacuum-drawn polyester
cast resin, decalcified
71.1% 28.9% 88.9% 11.1%
Pineda34 1972 300 Decalcified, dye injected,
cast in resin,
microscope
70% 27% 0% 85.7% 14.3% 0%
Vertucci35 1984 100 Decalcified, dye
injected, cast in resin,
microscope
70% 30% 0% 85% 15% 0%
Caliskan45 1995 100 Dyed, decalcified,
stereomicroscope x12
60% 52% 2% 81% 17% 2%
Walker96 1988 100 Radiograpic in vitro 55% 45% 0% 72% 28% 0%
Wasti68 2001 30 Decalcified, ink dye, x10
dissecting microscope
30% 70% 0% 56.7% 43.3% 0%
Fabra-Campos98 1985 145 Radiographic clinical in vivo 50.34% 49.6% 0% Not
reported
Not
reported
Not
reported
Da Costa99 1996 199 Decalcified, India ink-dyed
gelatin injection
78.9% 21.1% 90.5% 9.5%
Figure 29 Example of a mandibular molar showing buccal mesial occlusal views. For access preparations, please see Figures 6 and 30.
912 / Endodontics

millimeters. Only four of the 17 roots had an isthmusthat was continuous from its coronal beginning to itsapical end, the other 13 had sections with and withoutthe isthmus. The third section from the apex had thehighest incidence of isthmuses (50%). Two distal rootscan occur but are rare—however, reported to be moreprevalent in the South East Asian population.
CLINICALThe important point to note with the mandibularmolars is the degree to which they are lingually andmesially inclined.19 To prevent unnecessary gouging ofthe axial walls of the access preparation, the bur shouldmimic this angulation of the tooth in the mandible.
The entry point is just mesial to the central pit. Initially,the access preparation should not be extended furtherdistally as the distal canals project mesially toward theocclusal table. Once the angle of the canals has beendetermined with files, the decision can then be made toextend the access distally if needed. However, the accesswill be located largely in the mesial half of the tooth, asSLA for the mesial canals will dictate. Sometimes it isnecessary to encroach on the mesiobuccal cusp tip toachieve SLA (Figure 30).
The groove between the mesiobuccal/mesiolingualand distobuccal/distolingual canals must always betroughed with a bur and/or ultrasonics and checked withfiles to search for mesial canals (Figure 31)—this can bebest accomplished with a microscope.
Figure 30 A, Access preparation in a mandibular molar with moderate/severe root curvature. B, Hand files can be placed to length in all three mesialcanals after adequate access and canal preparation. C, However, the access preparation requires an extreme extension for the mesiobuccal andmesiolingual canals due to the root curvature.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 913

Figure 31 Anatomical variations in lower first molars and the potential for a negative clinical outcome. A, Tooth diagnosed with a failing root canaltreatment that had had an apicoectomy completed 8 months earlier. The postoperative buccal and distal views show three mesial canals with separateportals of exit, probably causing the persistent infection. B, Mandibular third molar with preoperative view as well as straight and distal postoperativeviews. This tooth presented with three mesial canals; typically the middle mesial canal joins either the mesiobuccal or the mesiolingual canal early and isa more common form than the one in A. C, Tooth diagnosed with radix entomolaris. The distolingual root often has a significant curvature in thebuccolingual plane and can therefore be deceptively difficult to treat.
914 / Endodontics

The distal canal is ovoid or figure eight-shapedbuccolingually if only one canal is present, and amicroscope should be used to confirm this. Therecan be a second distal canal that bifurcates in theapical third—to minimize chances of missing these;the walls of the preparation should be divergent,and the clinician should be able to see the entiresurface of the buccal and distal walls of the canal tothe apex with a microscope. It is advisable to ‘‘feel’’the wall of the canal with precurved files for areasin the middle and apical thirds of the canal where theinstruments may stick.
It is easy to assume that the canals curve only to themesial or the distal, but because these roots are sobroad, they always have a curvature in the buccolingualdimension that cannot be assessed radiographically.Cunningham and Senia14 showed that of the 100mesial roots of mandibular molars, all demonstratedcurvature in mesiobuccal and mesiolingual canals inboth buccal and proximal view radiographs. Theyreported a reduction of canal curvature after coronalflaring. It is important to remember that the flaring willhave to occur in both the mesial and buccal planes formesiobuccal canals as well as in mesial and lingualplanes for mesiolingual canals. Similar planes need tobe addressed respectively for the distobuccal and dis-tolingual canals. Fabra-Campos101 found that 4 molarsout of 145 had five canals that were confirmed radio-graphically—the extra canal was the middle mesialcanal in the mesial root.
The presence and impact of furcation canals hasbeen widely discussed. Vertucci and Williams,102
using decalcification and staining, found that of the100 mandibular first molars, 46% had furcationcanals and 13% had a single lateral canal fromthe floor to the interradicular region. Of these,57.1% extended from the center of the pulp floor,28.5% arose from the mesial aspect of the floor, and14.4% extended from the distal aspect. In 23%, lateralcanals were found originating in the coronal third(distal root 80%, mesial 20%). Finally, in 10% of thecases, both lateral and furcation canals were found.Vertucci and Anthony103 used scanning electronmicroscope (SEM) and found 32% of mandibularfirst molars and 24% of mandibular second molars,a total of 56% with accessory canals. Although rela-tively uncommon, mandibular first molars can alsohave C-shaped canals.104,105 In a study on Burmesesubjects, about 10.1% of observed teeth had an extradistal root on the lingual aspect (radix entomolaris).106
Gulabivala et al.93 found an additional distolingualroot with one canal and one apical foramen 12.7%of the time (see Figure 31C).
Mandibular Second Molars
ANATOMY AND MORPHOLOGYGenerally, mandibular second molars differ from thefirst molars in their capacity for variation (Figure 32).Usually the crowns and roots of second molars aresmaller than the first molars by less than a millimeterin all dimensions. The occlusal table is more symme-trical and rectangular with four equally apportionedcusps; a fifth cusp is not present. The roots of thesecond molars are inclined more distally, in relationto the occlusal table, than the first molars, but less thanthe third molars. Therefore, the access cavity may haveto be extended more toward the mesial marginal ridgethan for first molars. The roots, and therefore canals,are usually closer together and can be fused to a singleconical root with varying internal anatomy or oftenC-shaped canal systems. Cooke and Cox107 were thefirst to report C-shaped configurations in mandibularmolars. Weine et al.108 evaluated 811 endodonti-cally treated second molars and reported 7.6% hadC-shaped canal systems.
CLINICALThe entry point of the access cavity should be mesialto the central pit similar to the first molars, but maynot require the same degree of mesial extension if theroots are closer together. Otherwise, a similar pre-paration as for the first molar can be made. CleaningC-shaped canals is unpredictable as there are manydifferent types with several subtypes. The access cav-ity will follow the curvature of the canals.
According to Melton,109 C-shaped canals can bedivided into three categories:Category I: The continuous C-shaped canal is any
C-canal outline without any separation.Category II: The ‘‘semicolon’’-shaped canal—referred
to canal configurations in which dentin separatesone distinct canal from a buccal or a lingual C-shaped canal in the same section.
Category III: Simply with two or more discrete andseparate canals.
Mandibular Third Molars
ANATOMY AND MORPHOLOGYThird molars have significant variations and anoma-lies. They are usually less developed, with oversizedcrowns and undersized roots. Due to the lack of spacein the jaws, they are often impacted and may have
Chapter 27 / Preparation of Coronal and Radicular Spaces / 915

very curved roots. They may have four or five cusps.Usually, when in good alignment and occlusion, thecrown is likely to have four cusps and is similar to thesecond molar. Usually third molars have two roots—amesial and a distal root that can be bifurcated orfused. When fully erupted and in functional occlu-sion, third molars provide excellent protection for thefirst and second molars by spreading the occlusalload. In such situations, keeping these teeth is bene-ficial and therefore knowledge of their anatomy andmorphology is important.
CLINICALSimilar to mandibular first molars, anatomical varia-tions will require modifications compared to acces-sing first and second molars.
Procedural Mishaps
Successful endodontic treatment originates from awell-designed and executed access preparation. Theopposite is also true; errors during root canal
Figure 32 Variations in mandibular second molar anatomy. A, Common anatomy. B, Apical bifurcation. C, Dilacerated roots. D, Four separate apicalforamina. E, F, C-shaped configuration.
916 / Endodontics

treatment can often be traced back to a problemoriginating from an inadequate access preparation.Errors generally stem from two access cavity charac-teristics: underextension and overextension.
UNDEREXTENSIONNot opening up the access cavity across the width ofthe root sufficiently can result in the operator missingcanals. They can often be buried under calcified dentin.However, if the canal is found but the cavity is notextended away from the furcation sufficiently, the filewill preferentially cut the furcal dentin causing a stripperforation. Another possibility, of not extending theaccess far enough, is that the coronal canal curvature isnot removed. This will increase chances of instrumentseparation as the file tries to go around more than onecurve, or transportation at the apex as the coronalcanal curvature renders the file tip uncontrollable.Underextension of the access preparation also limitsthe final diameter of the apical preparation size. Inanterior teeth, if the pulp horns are not adequatelyexposed and cleaned, the remaining pulpal tissue willcause coronal discoloration.
OVEREXTENSIONGenerally, overextension will cause unnecessaryremoval of tooth structure that weakens the remain-ing crown and ultimately decreases the long-termprognosis of restoration, and therefore the tooth.With the acceptance of implants that have goodlong-term prognosis, remaining tooth structure willbe the critical determinant between these two treat-ment choices.
Effect of Access Cavity Preparation on
Structural Integrity
There is little debate that endodontic treatment weak-ens teeth resulting in an increased susceptibility tofracture (Figure 33).110 But it has been widely statedthat this may be due to endodontic treatment result-ing in increased brittleness of the dentin.111–114 How-ever, it does not seem that root canal treatmentchanges the quality of the dentin, except some moist-ure loss,115 and it is thought that weakening of thetooth is more a result of tooth structure loss.
Using strain gauges in extracted premolars, Reehet al.116 showed that endodontic procedures reducedthe relative cuspal stiffness by only 5%. This was incontrast to an occlusal cavity preparation (20%), an
MO/DO cavity (46%), and an MOD cavity prepara-tion (63%). Howe and McKendry117 examined 40freshly extracted noncarious, unrestored humanmandibular first and second molars, prepared endo-dontic access preparations and/or MOD amalgamcavities, and then subjected them to increasingocclusal load until fracture. They found that anendodontic access cavity, or a conservative MODcavity, fractured at the same load (225.5 and222.4 kg, respectively). On the other hand, an accesscavity with both marginal ridges breached fracturedwith significantly less load (121.7 kg). Intact teethfractured at significantly more force (341.4 kg) thanall other groups. They suggested that when accesscavities are kept conservative and proximal toothstructure remains intact, simple restoration of accesscavities might suffice.
Sedgley and Messer118 studied whether loss of pulpvitality resulted in changes in tooth structure as mea-sured by biomechanical properties (punch shearstrength, toughness, load to fracture, and microhard-ness). Twenty-three matched pairs of teeth wereobtained where one tooth in each pair had endodontictreatment while the other was vital. Teeth were extractedand for comparison, data were collected immediatelyafter extraction and after 3 months. The authors foundno significant differences in punch shear strength,toughness, and load to fracture between groups. Vitaldentin was 3.5% harder than the endodontically treatedmatched pair. They suggested that the dentin does notchange in character but rather it is the cumulative lossof tooth structure from caries, restorative, and endo-dontic procedures that increases the susceptibility tofracture. Another possibility is that loss of pressorecep-tion or an elevated pain threshold may allow largerloads without triggering a protective response.
In a study similar to experiments by Reeh et al.,116
Panitvisai and Messer119 measured actual cuspaldeflection (rather than relative cuspal stiffness) andused more extensive cavity preparations (no toothstructure between access cavity and box preparation)to simulate clinical situations more closely. They used13 extracted human mandibular molars and used aramped load of 100 N to the mesial cusps. Increas-ingly extensive MO or MOD cavities were prepared,tested, and finally followed by an access preparation.They found that cuspal deflection increased withincreasing cavity size, with the greatest deflection afteraccess preparation when cuspal deflections of morethan 10 �m were observed. They reiterated the impor-tance of cuspal coverage to minimize marginal leakageand cuspal fracture.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 917

Figure 33 A, Improper angulation of the bur resulted in furcal perforation. B, Underextension of the mesial wall causing a strip perforation in themesiolingual canal.
918 / Endodontics

Radicular Preparations
OBJECTIVESUpon the completion of the coronal access cavityand the identification of root canal orifices, pre-paration of the root canal system is initiated. Rootcanal preparation serves two main objectives:mechanical and chemical elimination of intracanaltissue and pathogens, aided by antimicrobial sub-stances and by optimized root canal fillings.120–122
A well-executed root canal preparation is a pre-requisite for success (Figure 34).
Using anaerobic culturing, a reduction of intracanalbacteria after canal preparation has been demon-strated to a level of 10 to 100 CFU/mL,9,123–127 but
it is highly unlikely that any root canal is renderedsterile in a clinical setting. Both clinically successfuland failing cases illustrate the presence of bacteria andimmune cells.128–130 However, in using stringent cri-teria for assessing healing of apical periodontitis, thatis, the reconstitution of a lamina dura around theentire root perimeter131 as well as the absence ofinflammatory cells, only 6% of endodontically treatedteeth were deemed successful.128 The fate of bacteriainitially remaining in inaccessible canal areas, regard-less of the clinical technique,132 has been a matter ofspeculation: do they die from starvation,133 are theykilled by sealer components134 or can they survive andcause posttreatment disease?135 On the other hand, acomparison of histological and clinical material
Figure 34 Examples of root canal-treated first maxillary and mandibular molars in which cleaning and shaping was done adhering to the principles laidout in this chapter. Radiographs represent situation immediately after root canal filling.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 919

presented in Figure 35 demonstrates that histologicalsuccess is present only if microbial contamination isabsent.136
Furthermore, it was recently shown that well-filledand presumably well-shaped canals may still be asso-
ciated with failing root canal treatments, mainly dueto the fact that microorganisms remain in inaccessibleareas of the root canal system.137,138 Consequently,rather than ‘‘sterilizing’’ root canal systems, intracanalprocedures are tailored to reduce microbial burden,
Figure 35 Healing is commonly detected by clinical and radiographic appearances and only occasionally it is possible to assess the outcome of rootcanal treatment histologically. Both cases shown here had preoperative diagnoses of chronic periapical periodontitis and were extracted fornonendodontic reasons. A, During the 13-year follow-up period of this case, the mesial root apex of this mandibular molar did not present completehealing of the original radiolucency, despite the absence of symptoms. The obvious reason was the presence of bacteria, as shown in the histologicalimages. B, In this mandibular molar, the periapical region of the distal root exhibited radiographic healing, contrary to the mesial root, where a verticalfracture was the ultimate reason for extraction. Radiographic features of healing were confirmed by the histological picture, showing fibrous uninflamedtissue in the apical part of the root canal and calcified tissue. The latter did not completely obturate the lumen, as shown by serial sections. Imagescourtesy of Dr. Domenico Ricucci.
920 / Endodontics

so that it becomes compatible with success, by creat-ing conditions prohibiting regrowth and persistentinfection.
Apparently, a threshold may be reached withdifferent disinfection and preparation paradigms(Figure 36) that depend on numbers, virulence, andlocation of surviving microorganisms. The objectiveof root canal preparation, therefore, is to provide anenvironment in which periapical disease is preventedor the body’s immune system achieves healing peria-pical disease.
A futuristic vision of ideal endodontic treatment isto replace necrotic or irreversibly inflamed pulp tissue
with new healthy pulp tissue. Revascularization ofempty pulp spaces in juvenile teeth may occur, butit is an ongoing topic of investigation and many openquestions are yet to be solved.139,140
Because this ultimate goal is not yet obtainable,clinicians still have to deal with contaminated andinflamed pulp tissue. Rendering or keeping rootcanals bacteria-free during endodontic treatment isone of the most important goals to achieve successfulhealing or to maintain periapical health.141 To reiter-ate, the prime condition under which medical profes-sionals work, nihil nocere or ‘‘do not harm,’’ shouldprevail in root canal treatments and canal preparationin particular, since obvious iatric errors are likely todecrease the prognosis of a case.
EVIDENCE AND STRATEGIES FORSHAPING THE ROOT CANAL SYSTEMThe first objective, elimination of tissue and patho-gens, is achieved by skillful instrumentation includ-ing copious irrigation and, if deemed necessary,interappointment medication. Mechanical instru-mentation alone is effective in reducing bacterialload,142,143 but should be complimented with irriga-tion to further eliminate microorganisms.144,145
Some authors have differentiated between the mereflushing action of saline142,146,147 and the added anti-microbial effect of the most widely used irrigant,sodium hypochlorite (NaOCl).148,149 Both of thoseactions are dependent on canal size and shape,10,150
but the latter depends also on factors such as NaOClturnover, the amount of available chlorine, and con-tact time (for a more detailed review of endodonticirrigants, see Chapter 28, Irrigants and IntracanalMedicaments).
The accessibility of the contaminated root canalareas is key to disinfecting efficacy. Thus, overall canalanatomy and in particular canal dimensions(reviewed in detail in Chapter 6, Morphology of teethand their root canal systems) play an integral role inradicular shaping (Figure 37). Two basic numericalconcepts govern root canal shaping procedures (seeBox 1): WL and apical size, recently also described asworking width.151
Clinical experience has shown periapical bonylesions to heal predictably if the offending tooth isextracted, thus removing all intracanal and adheringmicroorganisms. This observation supports thenotion that extraradicular bacteria play a minor rolein supporting periapical disease, insofar as they colo-nize the periapical lesion.152 Therefore, procedures
Figure 36 Proposed relationships between preparation size and elim-ination of bacteria as well as prepared canal surface. A, Based onbacterial sampling with a detection threshold of about 10 colony formingunits (CFU), this threshold, essentially a canal with negative culture, maybe reached on various pathways (colored lines in graph). B, Based onmicrocomputed tomography and analysis of cross sections, completepreparation of canal surface is unlikely. Again, values between 40 and60% treated surface may be obtained with various canal shapes andapical sizes.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 921

confined to the root canal space153–155 seem to beable to address most of the cases of endodontictreatment needs.
Varying concepts have been proposed regardingWL,155 partially depending on preoperative diagnoses.Clinical experience suggests that vital cases willbe clinically successful despite apparent short fills(Figure 38). This may be explained by the absence ofmicroorganisms in these cases, and a vital pulp stumpmay be beneficial for periapical health.156,157 How-ever, with existing periapical lesions and contami-nated canal systems, WL definitions closer to the apexmust be adopted. Classic studies suggest that a WLbetween 0 and 2 mm from the radiographic apex
Figure 38 Examples of two cases in which incomplete shaping andshort fills did not result in periapical pathosis. Patients indicated rootcanal treatments were performed A, 10 years and B, 27 years earlier.
Figure 37 Relationship between cross sections of roots and root canals.Following the principles of dentinogenesis, the pulp space has a verysimilar outline as the outer root contour. A, Sequence of microcomputedtomography slices (resolution 36 �m) of a second maxillary molar. B,Clinical or buccolingual view of the reconstructed outer contour and rootcanal system. C, Mesiodistal view clearly illustrating the existence of afourth canal, in this case a second distobuccal canal that merges intothe lingual (palatal). D, Schematic illustration for the required amount ofdentin removal in the coronal third for adequate access to middle andapical root canal thirds. Modified with permission from Peters OA. PractProced Aesthet Dent 2006;18:277.
922 / Endodontics

results more often in success (healing of periapicallesions) than shorter or longer fills (Figure 39).
One school of thought recommends the use of apatency file, a small, that is, size #10, K-file that isgently just pushed through an apical foramen withoutactually enlarging it. The purported benefit is to‘‘clean’’ a foramen and to avoid apical blockage; how-ever, a clinical benefit of this approach has not beendemonstrated so far. In fact, the patency technique iscontroversial and is not uniformly accepted or taughtin all US dental schools.158
On the other hand, a deleterious effect that couldhave been brought about by mechanically injuringperiapical tissues or by inoculating microorganisms159
may be suspected but was not conclusively demon-strated.160 This may be due to the fact that a con-taminated file that passes through canal spaces filledwith NaOCl is unlikely to carry any significant num-bers of microorganisms past the foramen.161 How-ever, the extrusion of debris is more likely if the apicalforamen is patent.162,163 Certainly, cleaning the fora-men, in the sense that the foramen is enlarged and
debris is mechanically removed with a small file, isunlikely.164
It should be stressed that the use of a patency file isdistinct from ‘‘apical clearing,’’ which is defined as atechnique to remove loose debris from the apicalextent, and involves sequentially rotating files two tofour sizes larger than the initial apical file at WL; thelargest apical file is then again rotated after a finalirrigation and drying.165 This technique may be usefulafter hand instrumentation166 but no effect has beenshown after rotary instrumentation.
It is commonly held that the use of a patency fileduring preparation would minimize the blocking ofcanal space with dentin mud and thus improvingshapes. However, Goldberg and Massone167 showedcanal transportation in more than half of their speci-mens shaped with stainless steel or NiTi K-files usedas patency files. Confining shaping procedures to thecanal space was already recommended by Schilder; hein fact stressed that the apical foramen should remainin its position and not be enlarged.3
The question then is where does the root canal end(Figure 40) and how close to that point can cliniciansestimate their WL. Histological studies indicated thepresence of the transition of the pulp to the periapicaltissue as well as dentin and cementum in the area ofconstriction (Figure 41).168 However, a constrictionin the classic sense may be absent.169 In fact, high-resolution tomographic studies suggest more compli-cated apical canal configurations than previouslyshown (Figure 42). Therefore, radiographic interpre-tation alone may not give the clinician a good esti-mate for WL determination.170–172 Indeed, shaping tothe radiographic apex, or even slightly short of it, willlead to frequent overinstrumentation.171,173
DETERMINATION OF WORKING LENGTHThe term ‘‘WL’’ (Figure 43 and Box 1) is defined inthe Glossary of Endodontic Terms as ‘‘the distancefrom a coronal reference point to the point at whichcanal preparation and obturation should termi-nate.’’174 The anatomical apex is the tip or the endof the root determined morphologically, whereas theradiographic apex is the tip or the end of the rootdetermined radiographically.174 It is well establishedthat root morphology and radiographic distortionmay cause the location of the radiographic apex tovary from the anatomical apex. The apical foramen isthe main apical opening of the root canal. It is ofteneccentrically located away from the anatomical or theradiographic apex.168,169,175,176 Kuttler’s168 investiga-tion showed that this deviation occurred in 68 to 80%
Figure 39 Relationship between the length of the fill and the presenceand absence of periapical pathosis. A, Cases with a diagnosis ofirreversible pulpitis. B, Cases with pulpal necrosis and periapical patho-sis. Reprinted with permission from Sjogren U et al.160
Chapter 27 / Preparation of Coronal and Radicular Spaces / 923

of teeth under investigation. An accessory foramen isan orifice on the surface of the root communicatingwith a lateral or an accessory canal.174 They may befound as a single foramen or as multiple foramina.The apical constriction (minor apical diameter) (seeFigures 40 and 43) is the apical portion of the rootcanal with the narrowest diameter. This position mayvary but is often 0.5 to 1.0 mm short of the center ofthe apical foramen.168,169 The constriction widensapically to the foramen (major diameter) and assumesa funnel shape.
Probably owing to its importance as a clinical entity,the apical third of the root canal and the foramen loca-tion have been the topic of numerous investiga-tions.7,168,169,175–183 Dummer et al.169 reported four basicvariations in the apical canal area that included about50% of cases where a constriction was present. They alsoreported 6% of their cases where the constriction was
probably blocked by cementum.169 The cementodentinaljunction is the region where the dentin and the cemen-tum are united; this is the point at which the cementalsurface terminates at or near the apex of a tooth.174 Ofcourse the cementodentinal junction is a histologicallandmark that cannot be located clinically or radiogra-phically. Langeland184 reported that the cementodentinaljunction does not always coincide with the apical con-striction. The location of the cementinodentinal junctionalso ranges from 0.5 to 3.0 mm short of the anatomicalapex.168,169,175,176 Therefore, it is generally accepted thatthe apical constriction is most frequently located 0.5 to1.0 mm short of the radiographic apex. It has beenpointed out by Ricucci153 that significant anatomicalvariation makes difficult the direct clinical use of theseaverage values as end points of canal preparation.Further problems exist in locating apical landmarksand in interpreting their positions on radiographs.
Figure 40 Microcomputed tomography reconstructions demonstrating external and internal anatomy of a maxillary anterior. The insert is a magnifiedview of an apical segment of 2 mm length showing no appreciable constriction (see arrowhead in larger image) and a cross-sectional diameter of theroot canal of approximately 300 �m.
924 / Endodontics

METHODOLOGICAL CONSIDERATIONSBefore determining a definitive WL, the coronal accessto the pulp chamber must provide a straight-line path-way into the canal orifice. Modifications in access pre-paration may be required to permit the instrument topenetrate, unimpeded, into the apical constriction.Similarly, a crown-down preparation, including WLdetermination after initial shaping, will alleviate thisproblem. The loss of WL during cleaning and shapingcan be a frustrating procedural error. Once the apicalpreparation is accomplished, it is useful to reassess the
WL since the WL may shorten as a curved canal isstraightened.185–187 WL may also be lost owing to ledgeformation or blockage of the canal.
As stated above, most dentists agree that the desiredend point is the apical constriction. Failure to accu-rately determine and maintain WL may result in thelength being too long and may lead to perforationthrough the apical constriction. Enlargement of theapical narrowing may lead to overfilling or overexten-sion and subsequently to increased incidence of post-operative pain. In addition, one might expect a
A
B
Figure 41 Comparison of radiographic and histological aspects of working length (WL). Teeth were extracted for nonendodontic reasons and processedfor routine histological examination. A, Radiograph indicates adequate fill just short of the apex; light micrograph demonstrates short fill with connectivetissue in the apical canal segment. B, Radiograph indicates adequate fill just short of the apex; light micrograph demonstrates overfill with someinflammatory cells surrounding the gutta-percha point. Images courtesy of Dr. Domenico Ricucci.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 925

prolonged healing period and lower successrate.153,155,188–190 Failure to determine and maintainWL accurately may also lead to shaping and cleaning
short of the apical constriction. Incomplete cleaningand underfilling may cause persistent discomfort, maysupport the continued existence of viable bacteria,
Figure 42 Apical root anatomy of the same mesiobuccal root of a maxillary molar assessed using scanning electron microscopy (SEM) and microcomputed tomography. A, SEM pictures of multiple apical foramina at x20 and x100 magnification. Bar indicates long diameter of 0.35 mm. B, Outercontour and canal segments illustrated with �CT at a resolution of 9 �m. Note that all canals merge and connect. Images courtesy of Dr. Ephraim Radzik.
Figure 43 Schematic diagram of the root apex and anatomical landmarks. The distance between the anatomical apex and the narrowest point of themain root canal varies substantially and changes with cementum deposition during aging.
926 / Endodontics

and thus contribute to a continued periapical lesionand ultimately a lowered rate of success.
In this era of improved illumination and magnifi-cation, WL determination should be to the nearestone-half millimeter, which is the maximum resolutionof the naked eye in working distance. The measure-ment should be made from a secure reference pointon the crown in close proximity to the straight-linepath of the instrument, a point that can be identifiedand monitored accurately. The length adjustment ofthe stop attachments should be made against the edge
of a sterile metric ruler or a gauge made specificallyfor endodontics (Figure 44). The requirements of anideal clinical method for determining WL includerapid location of the apical constriction in all pulpalconditions and all canal contents; easy measurement,even when the relationship between the apical con-striction and the radiographic apex is unusual; rapidperiodic monitoring and confirmation; patient andclinician comfort; minimal radiation to the patient;ease of use in special patients such as those with severegag reflex, reduced mouth opening, pregnancy; and
Figure 44 Sequence of steps in working length (WL) determination. A, Initial measurement. Tooth is measured on an orthogonal and diagnosticpreoperative radiograph. In this case the tooth seems to be about 23 mm long. B, Tentative WL, as a safety measure during coronal pre-enlargement andcrown-down, subtract 1 mm from tooth length and allow instruments to go to two-thirds of this length. C, After the coronal two-thirds of the canal havebeen prepared, advance the hand file to tentative full WL, using the electronic foramen locator, and expose the radiograph. D, Final radiograph after rootcanal filling and removal of rubber dam.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 927

cost effectiveness.172,191,192 To achieve the highestdegree of accuracy in WL determination, a combina-tion of several methods should be used. This is mostimportant in canals for which WL determination isdifficult.193 The most common methods are radio-graphic methods, digital tactile sense, patients’ responseto a file introduced into the canal, or a point to which apaper point can be placed and removed dry.194 How-ever, current electrical foramen locators (see Chapter26D, Electronic Apex Locators) greatly aid in determin-ing the narrowest cross-sectional diameter and widthand therefore in approximating WL.195
CLINICAL DETERMINATION OF WORKINGLENGTHMethods requiring formulas to determine WL havebeen largely abandoned. Bramante and Berbert196
reported great variability in formulaic determinationof WL, with only a small percentage of successful
measurements. The following items are essential toperform radiographic WL estimation:
1. Good, undistorted, preoperative radiographsshowing the total length and all roots of theinvolved tooth.
2. Adequate coronal access to all canals.3. An endodontic millimeter ruler.4. Working knowledge of the average length of all of
the teeth.5. A definite, repeatable plane of reference to an
anatomical landmark on the tooth, a fact thatshould be noted on the patient’s record.
To secure reproducible reference points, cuspsseverely weakened by caries or restoration may bereduced to a flattened surface, supported by dentin.Failure to do so may result in cusps or weak enamelwalls being fractured between appointments(Figure 45). Thus the original site of reference is lost.If this fracture is not accounted for, then there is the
Figure 45 Example of a root canal-treated tooth that presented with a fracture prior to placement of the planned definitive restoration. In this case, thepalatal root was preserved and crown was restored after placement of a post and core. A, Clinical sequence from temporized access to status aftersurgical extraction of the two buccal roots. B, Radiographs immediately after endodontic treatment, after surgery and at 1-year follow-up. Imagescourtesy of Dr. Craig Noblett.
928 / Endodontics

probability of overinstrumentation and overfilling. Toestablish the length of the tooth, a K-file with aninstrument stop on the shaft is needed. The exploringinstrument size must be small enough to negotiate thetotal length of the canal but large enough not to beloose in the canal. A loose instrument may move in orout of the canal after the radiograph and may alsocause errors in determining tooth lengths. Moreover,tips of fine instruments (size #08 and #10) are oftendifficult to see in a radiograph,197 as are NiTi instru-ments.
Clinically, it is advisable to estimate canal lengthsfrom a preoperative radiograph (see Figure 44).About 1.0 mm ‘‘safety allowance’’ for possible imagedistortion is deducted,198,199 the endodontic ruler isset to this tentative WL, and the stop on the instru-ment adjusted at this level (see Figure 44). Theinstrument is placed in the canal until the stop is atthe plane of reference unless pain is felt, in whichcase the instrument is left at this level and the rubberstop readjusted. An electric foramen locator (seeChapter 26D, Apex Locator) should be used to verifyand potentially further adjust the rubber stop. Aradiograph is exposed and the difference betweenthe end of the instrument and the end of the rootis determined.
Current apex locators are sufficiently precise200 toallow WL determination, thus reducing the frequencyof overinstrumentation when only radiographs areused.173,201 Even in cases of apical resorption andwide-open apices after root-end resection, these apexlocators are shown to be accurate.202,203 Therefore, itseems warranted to focus on the electronically deter-mined WL and to use the radiograph merely to avoidgross errors in case the apex locator does not appear towork correctly. This strategy eliminates approximationstrategies such as shortening WL, as suggested byWeine,204 to allow for apical resorption. Independentof the strategy, the final WL and the coronal point ofreference are recorded on the patient’s chart. Whentwo canals located in the buccolingual plane appear tobe superimposed, much confusion and time may besaved by several simple means. Occasionally, it isadvantageous to take individual radiographs of eachcanal with its length-of-tooth instrument in place. Apreferable method is to expose the radiograph from amesial–horizontal angle. This causes the lingual canalto always be the more mesial one in the image (MLM,also known as Clark’s rule). For any mesial- or distal-angulated radiographs, the SLOB (‘‘same lingual,opposite buccal’’) rule, or the Ingle MBD Rule(‘‘Shoot’’ from the Mesial and the Buccal root will beDistal), may be applied to locate instruments.
Radiographic WL determination, using conven-tional films alone, is accurate less than 90% of thetime,176,205,206 and it is unclear if digital radiographyis currently an improvement over conventional filmsregarding WL determination accuracy.207 In fact,inferior208 as well as superior209,210 results werereported for phosphor plate systems. Sensor-basedradiovisiography performed similar to films regardingaccuracy in some studies211–213 but was recentlyshown to be superior.214
Electronic foramen locators sometimes do notfunction accurately, for example, in cases where cur-rent may flow into the marginal gingiva or into metalrestorations causing erroneous readings. Therefore,additional methods such as tactile assessment anddetection of moisture on the tip of a paper point wererecommended.176 If the coronal portion of the canal isnot constricted, an experienced clinician may alsodetect an increase in resistance as the file approachesthe apical 2 to 3 mm. This detection is by tactile sense.In the apical region, the canal frequently features aconstriction or a smaller diameter before exiting theroot. There is also a tendency for the canal to deviatefrom the radiographic apex in this region,7,168,175 andboth these geometric features may be perceived by aclinician. However, Seidberg et al.194 reported anaccuracy in WL determination of just 64% usingdigital tactile sense. If the canals were preflared, itwas possible for an expert to detect the apical con-striction in about 75% of the cases.215 If the canalswere not preflared, determination of the apical con-striction by tactile sensation was possible in onlyabout one-third of the cases.216 Preflaring and subse-quently determining WL also reduce the amount andincidence of WL changes during the course of canalshaping procedures.186
All clinicians should be aware that this method, byitself, is often inexact. It is ineffective in root canalswith an immature apex and is highly inaccurate if thecanal is constricted throughout its entire length or ifthe canal has excessive curvature. Therefore, tactiledetection should be considered as a supplementary tohigh-quality, carefully aligned, parallel WL radio-graphs and/or an apex locator. Consequently, a surveyfound that few general practice dentists and no endo-dontists trust the digital tactile sense method of deter-mining WL by itself.217 Even the most experiencedspecialist would be prudent to use two or more meth-ods to determine accurate WLs in every canal.
In a root canal with an immature (i.e., wide open)apex, a relatively reliable means of determining WL isby gently passing the blunt end of a paper point intothe canal after profound anesthesia has been achieved.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 929

The moisture or blood on the portion of the paperpoint that passes beyond the apex may be an estima-tion of WL or the junction between the root apex andthe bone. In cases in which the apical constriction hasbeen lost owing to resorption or perforation, and inwhich there is no free bleeding or suppuration intothe canal, the moisture or blood on the paper point isan estimate of the amount the preparation overex-tended. This paper point measurement method is alsoa supplementary one. As stated earlier, nonsurgicalendodontic procedures should best be confined tothe root canal. This is true for files also, or paperpoints, in the process of WL determination. WLdetermination should be painless. Advancing aninstrument into a canal toward inflamed tissue maycause moderate to severe instantaneous pain. At theonset of the pain, the instrument tip may still beseveral millimeters short of the apical constriction.When pain is inflicted in this manner, little usefulinformation can be gained and considerable damageis done to the patient’s trust. When the canal contentsare necrotic, however, the passage of an instrumentinto the canal and past the apical constriction mayevoke only a mild awareness or possibly no reaction atall.
On the other hand, Langeland et al.184,218
reported that vital pulp tissue with nerves and ves-sels may remain in the most apical part of the maincanal even in the presence of a large periapicallesion. Finally, passing a file through necrotic canalcontents may inoculate bacteria-contaminated den-tin shavings into periapical tissues, thus supportingor causing apical periodontitis.219,220 However, Izuet al.161 showed that small files used as patency filesare unlikely to carry bacteria past a reservoir ofNaOCl.
CLINICAL DETERMINATIONOF WORKING WIDTHThe second factor to be considered is apical width orpreparation size. It is a matter of debate as to whichapical enlargement and more specifically which shapewould lead to an optimal reduction of the intracanalmicrobial load.221 Baumgartner’s group10,150 hasrecently attempted to address this question in vitro,and they concluded that an apical preparation size #20would be inferior to sizes #30 and #40 regarding canaldebridement but that a larger taper (e.g., 0.10) maypotentially compensate for smaller sizes. This notion issupported by an in vitro study on the efficacy ofultrasonically activated irrigation that demonstrated
better debridement with 0.10 taper preparation.222
Similarly, Mickel et al.,12 based on microbiologicalassays, as well as Khademi et al.,223 using SEM, foundthat apical preparation to size #30 is required to effec-tively clean root canals. Moreover, recent elegant ana-lyses, using a thermal imaging system, revealeddetailed relationships between MAF size, needle dia-meter, and insertion depth.224 Taken together, theseresults indicate that sufficient apical preparation sizeand the use of a small-caliber irrigation needle aredesirable to promote irrigation and hence antimicro-bial efficacy.
In situ, however, even larger apical preparationsizes were favored by results from Trope’sgroup,9,125,127 in particular, when an interappoint-ment dressing of calcium hydroxide was used. Inter-estingly, larger apical sizes (#40, taper 0.04 comparedto #20, taper 0.10) facilitated the application of cal-cium hydroxide medication in vitro.225
Most clinical outcome studies incorporate the fac-tor ‘‘apical preparation size’’ with often insufficientstatistical power and with conflicting results.226–228 Areview of the technical aspects of root canal treat-ments229 found that apical periodontitis was morefrequent with inadequate root canal fillings; however,they did not find evidence that canal instrumentationmethods, and in particular apical sizes, had any mea-surable effect on outcomes. Conversely, one result ofthe Toronto study230 on endodontic outcomesseemed to favor smaller preparations in conjunctionwith tapered shapes and vertically compacted gutta-percha over step-back preparation to larger apicalshapes (90% and 80% success, respectively). Againin contrast, using Periapical Index (PAI) scores deter-mined from radiographs, Ørstavik et al.231 did notfind any significant impact of preparation size onoutcomes.
It is not possible to determine canal diameters fromradiographs;151 however, �CT scans may be able togive more detailed information regarding root canalanatomy in vivo (Figure 46). The resolution of currentsystems is in the range of 100 �m, corresponding to asize #10 K-file, and hence not sufficient to determinecanal diameters with precision. Clinically, canal widthmay be determined by passing a series of K-files to WLto gauge, as suggested by Ruddle.232 This process maydepend on the file type and the amount of preflar-ing.8,233,234 Clearly, the first instrument that gives theclinician a sense of binding does not correspond to anycanal diameter. Wu et al.8 demonstrated that the dia-meter of the ‘‘binding’’ instrument was smallerthan the canals’ diameter in 90% of the cases witha difference of up to 0.19 mm. Unexpectedly,
930 / Endodontics

LightSpeed (LS) instruments (Discus Dental, CulverCity, CA) that possess a fine noncutting shaft did notperform better than K-files with 0.02 taper. Therefore,they concluded that it is uncertain that circumferentialremoval of dentin occurs based on the criterion thatone should prepare three sizes larger than the firstbinding file;8 this and also the criterion ‘‘clean dentinshavings’’ are not considered adequate to indicatesufficient apical preparation.235
It seems that preflaring, prior to any attempt atassessing canal diameter, is essential233,234 since itallows the probing file to approach the apical areawith less interferences. Tan and Messer233 indeedfound that K-files and LS instruments determinedapical sizes about one ISO size larger after preflaring.
In their study, LS instruments that were felt to bind atthe apex were almost two ISO sizes larger than K-files.
After preoperative canal size is estimated, workingwidth determination may be done. Jou et al.151 sug-gested definitions based on variations in cross-sectionalcanal shape. Their goal was to allow clinicians to obtaina more complete shape regarding instrumented surfacearea; this strategy is in line with current guide-lines.236,237 However, this goal may be unattainablewith current instrumentation techniques.120 In conclu-sion, there may be no practical way to objectivelydetermine a final file size that predictably allows com-plete instrumentation of canal walls. Consequently, allpotential mechanisms to increase irrigation efficacyshould be explored.
A
B
Figure 46 Potential of a clinically used high-resolution computed tomography to show root canal anatomy. Scans were done in vivo using an Accuitomocone beam machine (Morita, Tokyo, Japan). A, Reconstructed jaw segment with three teeth is shown after apicoectomy and retrograde fill of mesial rootof lower left first molar in clinical. B, Distally angled projection. Two teeth were segmented free from bone and are shown independently. Noteincomplete fill of mesial root and two merging canals in the distal root of the molar.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 931

Table 10 presents an overview of anatomical studiesdetailing physiological foramen diameters. There is anapparent variation in these measurements, probablydue to variation in experimental conditions. Conse-quently, there is also a great deal of variation inrecommended apical sizes, as shown in the left seg-ment of Table 10.
For example, apical sizes ranging from sizes #20 to#100 for maxillary molar roots have been recom-mended. Figure 47A illustrates apical dimensionsbefore and after shaping with two rotary instrumenta-tion paradigms.
A third as yet incompletely understood aspect ofcanal shape is taper. Some have expressed concernsthat the importance of root canal taper should beseen only in conjunction with root canal filling tech-niques, most notably vertical compaction.244 How-ever, as stated before, there are some experimental
evidences that taper may be connected to the abilityto clean the root canal system by improving irrigantaction.10,150,222 Limited microbiological data are con-flicting regarding the potential of smaller apical pre-parations with larger taper to disinfect root canalsystem.13,127 Using the amount of instrumented canalarea as a surrogate outcome for disinfecting capacity,no significant differences were found overall, compar-ing shapes with GT 20 0.10 taper to apical size #40with smaller tapers.245 However, there were signifi-cant differences when the apical canal segment wasevaluated for instrumented canal surface area (Paque F,unpublished data).
Schilder3 described five design objectives for cases tobe filled with gutta-percha, which are as follows:
• The shape should be a continuously tapering funnelfrom the apex to the access cavity.
Table 10 Measured Apical Diameters and Suggested Preparation Sizes for Mandibular and Maxillary Teeth, Taken fromRepresentative References over the Last 50 Years
Maxillary teeth
Reference Kuttler168 Green177 Kerekes51,238,239 Morfis180 Wu182 Briseno183 Grossman240 Sabala241 Tronstad242 Glickman243
Type 268 Teeth
In Vitro
110 Teeth
In Vitro
220 Teeth
In Vitro
213 Teeth
In Vitro
180 Teeth
In Vitro
1,097 Teeth
In Vitro
Suggestions Review Suggestion Suggestion
Centrals 25–35 45 30 34 80–90 80 70–90 35–60
Laterals 25–35 60 30 45 70–80 80 60–80 25–40
Canines 25–35 45 31 60–90 80 50–70 30–50
First premolars 25–35 20 50 21 37 30–40 60 35–90 25–40
One canal 70 30 60
Two canals 20 23
Second premolars 25–35 21 37 50–55 35–90 25–40
One canal 70 30 80
Two canals 35 23 45–60
Molars 25–35 30–55
Mesiobuccal 25 60 24 43 11–73 45 35–60 25–40
One canal 40 19 09–60
Two canals 40 19 11–44
Distobuccal 25 40 23 22 08–73 45 35–60 25–40
Palatal 35 40 30 29 08–69 60 80–100 25–40
Mandibular teeth
Centrals 25–35 70 26 37 40–50 60 35–70 25–40
Laterals 25–35 70 37 40–50 60 35–70 25–40
Canines 25–35 70 47 50–55 80 50–70 30–50
First premolars 25–35 35 27 35 30–40 35–70 30–50
One canal 20 80
Two canals 19 45–60
Second premolars 25–35 40 27 35 50–55 35–70 30–50
One canal 20 80
Two canals 13 45–60
Molars 25–35 30–55
Mesial root 25 60 26 38–45 10–64 45 35–45 25–40
Distal root 30 60 39 46 12–64 60 40–80 25–40
932 / Endodontics

• Cross-sectional diameters should be narrower atevery point apically.
• The root canal preparation should flow with theshape of the original canal.
• The apical foramen should remain in its originalposition.
• The apical opening should be kept as small aspractical.
There were also four important biological objec-tives that are as follows:
• Procedures should be confined to the roots them-selves.
• Necrotic debris should not be forced beyond theforamina.
• All tissues should be removed from the root canalspace.
• Sufficient space for intracanal medicaments andirrigation should be created.
These objectives form the basis for today’s qualitycriteria236,237 and also for the development of opera-tional techniques that will be described below indetail. All of these techniques rely on the adaptationof geometric forms, of either handheld or engine-
driven instruments to root canal anatomy, by way ofparticular instrumentation sequences and usage para-meters. However, an experimental, noninstrumenta-tion system for root canal cleaning has been tested invitro and in vivo;246,247 since neither this system norpotential alternatives are currently available for theclinic, mechanical preparation will be utilized to cleanand shape root canals for the foreseeable future.
In conclusion, the current strategy in radicularpreparation calls for the enlargement of root canals toa size sufficient to allow disinfection and subsequentroot canal filling.120 Available evidence to support aparticular shape in direct connection with any givenroot canal filling technique is limited to Allison et al.,248
who found a better seal when spreaders used for lateralcompaction could penetrate close to WL. Conse-quently, efforts continue to determine the best possibleroot canal shape for management of intracanal infec-tion by mechanical action, irrigant delivery, and place-ment of interappointment medicaments.
MEANS FOR RADICULAR SHAPINGHistorically, painful teeth were opened and sympto-matic pulps were treated with caustic substances or
Figure 47 Pre- and postoperative canal diameters after shaping with common instrument types. Measurements are from microcomputed tomographyreconstructions. A, Original data from 12 mesiobuccal canals shaped to an apical size #40 with FlexMaster (left panel, VDW) and ProTaper (right panel,Dentsply Maillefer). B, Dimension of selected rotary instruments for comparison.
Chapter 27 / Preparation of Coronal and Radicular Spaces / 933

cauterized with heat.249 Some of these procedures asearly as 1728 by Pierre Fauchard are said to haveincluded root canal fillings with lead or gold.250 Rootcanal systems have been shaped with mechanicalinstruments for more than 200 years.250–252 Accordingto Lilley251 at the end of the eighteenth century‘‘. . . only primitive hand instruments and excavators,some iron cautery instruments and only very few thinand flexible instruments for endodontic treatmenthad been available. . .’’.
The development of the first endodontic handinstruments by Edwin Maynard involved notching around wire (e.g., watch springs, piano wires) to createfine needles for pulp tissue extirpation and potentiallyshaping.253 In 1852, Arthur used small files to enlargeand shape root canals.254 Subsequently, textbooks inthe middle of the nineteenth century recommendedthat root canals should be enlarged with broaches:‘‘But the best method of forming these canals is witha three- or four-sided broach, tapering to a sharppoint, and its inclination corresponding as far aspossible with that of the fang. This instrument isemployed to enlarge the canal and give it a regularshape’’.122,252 In 1885, the GG drill and in 1904 theK-file were introduced, both of which are still in useto date. Standardization of instruments had been pro-posed by Trebitsch in 1929 and again by Ingle in1958122 but remains an issue today with NiTi rotaryinstruments.255 For a detailed description of variousinstrument types and alloys, the reader is referred toChapters 26B, ‘‘Introduction of Nickel-titanium Alloyto Endodontics’’ and Chapter 26C, ‘‘Instruments forCleaning and Shaping’’.
Instrument Movements While Shaping
WATCH-WINDINGThe least aggressive instrument action is most desir-able in the early phases of root canal instrumentation.Many clinicians232,256,257 recommend a ‘‘watch-winding’’movement with rotations of a quarter turn using small(size #08 or #10) K-files to reach WL or to explore thecanal prior to coronal flaring (see below). Importantly,copious irrigation and constant cleansing of the instru-ment with sterile gauze are necessary to clear the flutesand to prevent packing debris at or through the apicalforamen.
REAMINGReamers are instruments designed to enlarge or taperpreexisting spaces. Traditionally, endodontic reamers
were thought to cut by being inserted into the canal,twisted clockwise one-quarter to one-half turn toengage their blades into the dentin, and then with-drawn, that is, penetration, rotation, and retrac-tion.258 The cut is made during retraction. The pro-cess is then repeated, penetrating deeper and deeperinto the canal. When WL is reached, the next sizeinstrument is used, and so on. Reaming is a methodthat produces a round, tapered preparation, and thisis used only in perfectly straight canals. In such asituation, reamers can be rotated one-half turn beforeretracting. In a slightly curved canal, a reamer shouldbe rotated only one-quarter turn.
FILINGThe tighter spiral of a file establishes a rake angle thatachieves its primary cutting action on withdrawal,although it will cut in the push motion as well. Thecutting action of the file can be effected in either afiling or a reaming motion. In a filing motion, theinstrument is placed into the canal at the desiredlength, pressure is exerted against the canal wall, andwhile this pressure is maintained, the rake of the flutesrasps the wall as the instrument is withdrawn withoutturning. The file need not contact all walls simulta-neously. For example, the entire length and circum-ference of large-diameter canals can be filed by insert-ing the instrument to the desired working distanceand filing circumferentially around all of the walls.When using a file in a reaming action, the motion isobviously the same as for a reamer.258 Withdrawingthe file then cuts the engaged dentin. Filing is veryefficiently done with Hedstrom files while K-files arethe most popular instruments.259 One the other hand,the often advocated technique of circumferential fil-ing260 has been shown to leave significant canal areasunprepared.261 Finally, hand versions of current NiTirotary instruments, such as ProSystem GT (DentsplyTulsa Dental, Tulsa, OK) and ProTaper (DentsplyMaillefer), may be used in filing and reaming action.
ROTARY MOVEMENTSUntil the advent of NiTi alloy, continuous rotarymovement was thought undesirable for shaping curvedcanals due to the danger of instrument fractures.Nevertheless, it has been recommended to use stainlesssteel GG drills into the apical third of straight rootcanals,3,262 which have the potential of undesirablecanal shapes (Figure 48) and instrument fracture.Furthermore, strip perforations may occur with indis-criminate use of GG or Peeso drills.263,264 However, ithas been clearly established that continuous rotary
934 / Endodontics
























![Dl-reamer Technical Presentation External[2]](https://img.pdfslide.us/doc/110x75/577cb4901a28aba7118c8803/dl-reamer-technical-presentation-external2.jpg)