-
8/13/2019 File 85742
1/13
Downloaded from UvA-DARE, the institutional repository of the
University of Amsterdam (UvA)
http://dare.uva.nl/document/85742
File ID 85742Filename CHAPTER 4 MR Imaging of neuropathic feet
in leprosy patients with
suspected osteomyelitis
SOURCE (OR PART OF THE FOLLOWING SOURCE):Type DissertationTitle
Clinical applications of Dixon chemical shift MR imaging: Morbus
Gaucher,
Morbus HansenAuthor M. MaasFaculty Faculty of MedicineYear
2002Pages 168 + 76ISBN 909015888X
FULL BIBLIOGRAPHIC DETAILS:
http://dare.uva.nl/record/107697
CopyrightIt is not permitted to download or to
forward/distribute the text or part of it without the consent of
the author(s) and/or
copyright holder(s), other than for strictly personal,
individual use.UvA-DARE is a service provided by the library of the
University of Amsterdam (http://dare.uva.nl)
http://dare.uva.nl/http://dare.uva.nl/record/107697http://dare.uva.nl/document/85742
-
8/13/2019 File 85742
2/13
MRR Imaging of neuropath ic fee t inl e p ros yy pa t i e n t s
w i th s u s pe c t e dos teo m yel i t i s sM a r i o o M a a s l,
Er ik J . Sl im l*4, A g n e s F . H o e k s m a 4 ,Add J . v a n
de r Kleij 3, E r i k M . A k k e r m a n \
G e ra rdd J . d e n H e e te n ' , Wi l li a m R . F a b e r
2
Dep a r t m en t t o f R ad i o l o g y ' , De rm a t o l o g y
' ' an d S u rg e ry 1 , Acad em i c Med i ca l C en t e ra n dd t
h e d e p a r t m e n t of R e h a b i l i t a t i o n , J a n v a
n B r e e m e n I n s t i t u t e 4 ,A m s t e r d a m , , t h e N
e t h e r l a n d s
Submitted Submitted
433
-
8/13/2019 File 85742
3/13
Chapterr 4INTRODUCTION NThee invasion by Mycobacterium leprae of
Schwann cells with the resultingperipherall nerve damage can lead
to a so-called neuropathic foot.Ulcerationn and infection
(cellulitis or osteomyelitis) are importantcomplications.. Repeated
injury secondary to the neuropathy may lead totarsall
disintegration with osteolysis, fragmentation and progressive
boneresorption.. In extreme cases dissolution of the mid-foot
results inseparationn of the forefoot and the hindfoot, changing
all biomechanicsandd weight bearing areas [1,11,12,22]. The
neuro-osteoarthropathy in thefoott is a cause of considerable
morbidity in leprosy [9,12,22,26].Therefore,, when a patient with a
neuropathic foot presents himself with awarmm foot, it is a
clinical challenge to discriminate betweenneuro-osteoarthropathyy
and an ongoing osteomyelitis. Especially, this isdifficultt in the
presence of an ulcer, because an ulcer itself leads toincreasedd
local temperature [10,22].Variouss diagnostic modalities have been
investigated in the analysis ofosteomyelitiss in neuropathic feet
[5,13,24,28]. Magnetic ResonanceImagingg (MRI) has been described
as an important modality to assessosteomyelitiss in the neuropathic
foot of diabetic patients [16,18-20,27].Tissuee characterisation
and spatial resolution facilitate identification ofassociatedd soft
tissue pathology [2-4,16,30]. To detect subtle bonemarroww
pathology, such as a low-grade chronic infection, it is
mandatorytoo use fat-suppression sequences with the use of contrast
administration[19-21]. . A homogeneous fat-suppression in the
entire field of view bothbeforee and after intravenous contrast
material (Gadolinium-chelate (Gd))iss required, to avoid artefacts
and misreading [23]. This can adequately beachievedd by the use of
two-point Dixon chemical shift imaging (TPDCSI)[14,19]. .Thee
radiological literature available on MRI and osteomyelitis
inneuropathicc feet nearly exclusively concerns diabetic foot
pathology, beingthee most frequent cause of neuropathic feet in the
western world.However,, leprosy is an important cause of
neuropathic feet worldwide.Accordingg to the latest World Health
Organization (WHO) information atthee end of the year 2000 597.232
cases are on treatment, and 719.330neww cases are reported
[29].
444
-
8/13/2019 File 85742
4/13
-
8/13/2019 File 85742
5/13
Chapterr 4Clinicall outco m e after 6 m on th s follow-up was
retrospectively evalu atedinn cases where his topathology or cul
ture was not avai lable or notconclu sive.. A com bina tion of cl
inical criteria was ev aluate d in aconsensuss reading by a
dermatologist (WRF), a physiatris t (AFH) and asur ge onn (AJvdK).
The cl inical cri teria th at were evalu ated w ere res po ns eonn
ant ibiot ic t rea tment , na ture of surgical t rea tment when
performed,persis tent t s igns of inflammation, s tatus of the
ulcer, change in deformity.DiagnosticDiagnostic criteria MRI)AA
total n u m b er of 24 MR stu die s in 12 adu lt leprosy pa t ie
nts (9 ma le, 3female; ; mean age 63 years; age range 45-81 years)
were included forevalu at ion. . Of the se 2 4 MR studie s 18 were
performed be ca us e of cl inicalsu sp icio nn of osteom yelitis.
Follow-up MRI w as performed in 6 p at ie nt s (6MRII studies).MRI
MRIMRII examination was performed using a 1.5 Tesla Vision
(Siemens, Erlangen,Germany).. All MRI studies were performed
following the Dixon protocol[6,14,15].. This protocol consisted of:
sagittal turbo-STIR (short tau inversionrecovery)) (3mm),
Tl-weighted Dixon sequence with in- and opposed-phaseimages,,
sagittal dual echo T2-weighted FSE (Fast Spin Echo) (3mm); after
theintravenouss administration of Gadolinium chelate (0,1 millirnol
per kilogram ofbodyy weight) Tl-weighted Dixon sequence with in-
and opposed phase images[6,14,15]. .Too evaluate the MRI studies
signs were used as described in literatureconcerningg diabetic
neuropathic feet [16,19,20,27], Typical, primary MRI signsaree
decreased marrow signal intensity on Tl-weighted images, increased
signalintensityy on fat suppressed T2-weighted and/or fast STIR
images, and focalmarroww enhancement after Gadolinium-enhanced
fat-suppressed Tl-weightedimagess [14,17,20,21,28], Secondary MRI
signs are: the presence of a cutaneousulcer,, cellulitis, a soft
tissue mass, a soft tissue abscess, a sinus tract, andcorticall
interruption [21,30]. One musculoskeletal radiologist
(MM)retrospectivelyy evaluated the images blinded to all clinical
information exceptthee knowledge of clinical suspicion for
osteomyelitis. The signal intensity of thebonee marrow on
Tl-weighted in and out of phase Dixon images, fast STIRimagess and
Gadolinium enhanced Tl-weighted in and out of phase Dixonimagess
(primary s igns) was classif ied as normal or abnormal on a
data
4 6
-
8/13/2019 File 85742
6/13
MRII and osteomyelitis in leprosy patientscollectingg form. The
secondary signs were classified as present or absent.Furthermore,,
the site of involvement was noted (medial arch, centralcompartmentt
or lateral arch) [8,12].RESULTS S
linical linical findingsInn 8 patients there was one event of
suspected osteomyelitis. In 4 patientstheree were multiple events
of suspected osteomyelitis; in 3 patients thereweree 2 events of
suspected osteomyelitis, and in 1 pat ient there were 4eventss of
suspected osteomyelitis. The foot of involvement was 6
timesrightright and 12 times left. The location of the ulcer was 2
times at the medialside,, 14 times at the lateral side, and 2 times
an ulcer was present at themediall and lateral side.Thee results of
the gold standard are listed in table 1. When evaluatingresultss
from bone biopsy or bone culture and/or preset clinical
criteria,withoutt detailed knowledge of the MRI results, the
diagnosis osteomyelitiswass made in 16 of 18 events (88.9 ).
Tablee 1 Results of clinical follow-up in diagnosing
osteomyelitisEvent t
2 23 34 45 56 67 78 89 9
Gold ds tandard d
Pos sPos sPos s
Pos s
Clinical loutcome e
Pos s
Pos s
Pos sPos sPos s
Event t
10 0
11 112 213 314 415 516 617 718 8
Gold ds tandard d
Pos sPos s
Pos sPos s
Clinical loutcome e
Pos s
Neg gPos sNeg g
Pos s
4 7
-
8/13/2019 File 85742
7/13
C h a p t e r r 4DiagnosticDiagnostic findings MRI)I nn a t o t
a l n u m b e r of 1 8 e v e n t s of s u s p e c t e d o s t e o m
y e l i t i s w e e n c o u n t e r e d1 7 7 MR I e x a min a t io
n s p o s i t i v e fo r p r ima ry MR s ig n s fo r o s t e o my e
l i t i s(9 4 . 4 %) .. D e c re a s e d s ig n a l o n T l i n a n
d o u t o f p h a s e o n 1 6 MR I (8 8 . 9 %) ,increasedd s igna l
on T2 on 13 MRI (72 .2%) , fas t SE STIR on 13 MRI( 7 2. 2% ) ,, a
n d f oc al ly m a r r o w e n h a n c e m e n t af te r g a d o l
i n i u m - e n h a n c e d fa tsu p p re s s e d d T l o n 1 7 MR
I (9 4 .4 %) (T ab le 2 ) .
Tablee 2 Primary MRI signs: number of positive findings on
various MRIsequ ences s
P o s i t i v ee p r i m ary s i g n
Numberr of MRI (%)
T l l
166 (88.9%)
T2 2
133 (72.2%)
STIR R
133 (72.2%)
C o n t r a s t t
177 (94.4%)
T h e e s e c o n d a r y s i g n s w e r e p o s i t i v e i n
a l l M R I e x a m i n a t i o n s ( 1 0 0 % ) .C e l l u l it i
ss w a s p r e s e n t i n a ll c a s e s ( 1 0 0 % ) . A c u t a n
e o u s u l c e r i n t h e r e g i o no ff t h e s u s p e c t e d
o s t e o m y e l i t i s w a s a l s o p r e s e n t i n a ll c a
s e s ( 1 0 0 % ) .C o r t i c a ll i n t e r r u p t i o n w a s f
o u n d i n 1 6 i n v e s t i g a t i o n s ( 8 8 . 9 % ) . A s i n
u s t r a c tw a s s p r e s e n t in 5 c a s e s ( 2 7 . 7 % ) . A
s oft t i s s u e a b s c e s s w a s p r e s e n t i n 3c a s e ss
( 1 6 . 6 % ) . A s of t t i s s u e m a s s w a s f o u n d o n t
w o o c c a s i o n s ( 11 .1 % )(Tablee 3).
Tablee & Presence of positive secondary MRI signsPosi t ive
es e c o n d a r y ys ign n
Nu m b er r o fMRII (%)
Ce l lu l i t i s s
18 8(100% ) )
Ulce r r
18 8(100% ) )
Co r t i ca l li n t e r r u p t i o n n
17 7(88.9% ) )
S i n u s st ra c t t
5 5(27 .7% ) )
Soft tt i s s u e ea b s c e s s s
3 3(16.6% ) )
Soft tt i s s u e em a s s s
2 2(11.1%) )
4 8
-
8/13/2019 File 85742
8/13
MRII an d os t eom ye l i t i s in l ep r o s y pa t i e n t
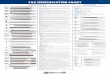
sAnn ex am pl e of pos i t i ve p r i m ar y s i gn s an d s ec on
da r y s i gns a t t h e l a t e r a lsidee of the foot is shown in
f igure 1.
Figuree la Two-point Dixon fatsuppressionn image of the right
foot of a79-year-oldd female patient. Note thedegradationn of the
plantar fat with thepresencee of soft t issue edema(interruptedd
arrow) and the high signalintensityy in the partly destroyed
cuboidbonee (non-interrupted arrow).
Figuree lb Same patient after intravenousgadoliniumm chelate
administration. Note themark edd en ha nce m en t at the lateral
side ofthee foot both in the soft tissue (cellulitis)(interruptedd
arrow) and in the cuboid bone(osteomyelitis)) (non-interrupted
arrow).
TheThe sites of involvement MR I)T h ee s i te s of i n v o l v
e m e n t : m e d i a l - c e n t r a l - l a t e r a l , o n M RI
w e r e a n a l y s e d .Th ee a r e a s of o s t eo m ye l i t i s
wer e l oca t e d a t t he m ed i a l s i t e (MTP1 j o i n t , o
sm e t a t a r s a ll 1, c u n e i f o r m 1, n a v i c u l a r b o
n e ) i n 3 e v e n t s , m e d i a l / c e n t r a l i n22 ev en t
s , ce n t r a l ( MTP 2 - 3 , o s m e t a t a r s a l 2 - 4 ) i n
3 ev en t s , la t e r a l ( MTP4 - 5 5 j o i n t , o s m e t a t a
r s a l 4 - 5 , c u b o i d , c a l c a n e u s ) i n 9 e v e n t s
. In 1 p a t i e n ta l l l t h ree areas were involved .
Follow-upFollow-up MRI)Si xx f o l l ow- up MRI wer e ma d e a f
te r an t i b i o t i c t r ea t m en t . M ean t i me off o l l
ow- upp w a s 5 m o n t h s . A co m pl e t e hea l i ng of t he u
l ce r oc cu r r ed i n t wopa t i en t s s w i t h a no r ma l f o
l l ow- up MRI .
-- 49 -
-
8/13/2019 File 85742
9/13
Chapterr 4TwoTwo patients had an improved but still abnormal
MRI; the MRI changesthatt were seen were a reduction but still
present zone of enhancement ofthee bone marrow. Both patients
eventually showed a complete clinicalremission.. The foot of the
pat ient that showed an unchanged follow-upMRII despite continued
antibiotics eventually was amputated.
DISCUSSION NOsteomyelitiss is a well-known complication in
patients with neuropathicfoott pathology
[4,13,16,19,20,24,26,28,30]. These patients may developulcerss that
persist over a long period of time. In this way spread ofinfectionn
per continuitatem can cause an infection of the osseousstructuress
in the foot. Clinical examination lacks specificity in this
patientgroup,, since by clinical examination alone it is difficult
to differentiatebetweenn cellulitis, osteomyelitis and
neuro-osteoarthropathy [22,26]. MRimagingg is potential powerful in
the evaluation of the neuropathic foot; itiss useful for the
evaluation of presence and extent of osteomyelitis, as wellass for
the identification of the presence and extent of associated
softtissuee abnormalities that may have clinical importance, such
as cellulitis,abscess,, and sinus tract [4,16,18-21,27,30], Nearly
all data available onMRII and neuropathic feet concern patients
suffering from diabetes. As farass we know this is the first report
on the use of MRI as a diagnosticproceduree in neuropathic leprosy
feet suspected for osteomyelitis.Whenn analyzing the primary MRI
signs for osteomyelitis we found in ourpopulationn that in 17 out
of 18 events (94.4 ) primary MRI signs werepositive.. Decreased
signal intensity on in and out of phase Tl-weightedimagess and the
marrow enhancement after gadolinium administration
onfat-suppressedd Tl were the most frequent encountered
abnormalities. Inourr retrospective analysis (gold standard and/or
clinical outcome) 16 outoff 18 events were diagnosed as positive
for osteomyelitis. Comparing thisevaluationn with the primary MRI
signs there was agreement in 17 out of188 events. The disagreement
found in one patient was caused by theprimaryy MRI sign focal
marrow enhancement after contras tadministration.. Therefore, we
conclude that these primary signs, used inevaluatingg MRI
examinations in diabetics can adequately be used toanalyzee MRI
examinations in leprosy patients with longstandingcomplicatedd
neuropathic feet.
50
-
8/13/2019 File 85742
10/13
MRII and osteomyeli t is in leprosy patientsOff the secondary MR
signs ulcer and celluli t is were present in al l cases.Thee areas
on MRI suspected of osteomyeli t is were in continuity with
theulcer. . The relat ion between ulcer and osteomyeli t is has
also beendes crib edd in dia be tes [5]. In con tr as t to diab
etic feet only a mino rity ofexaminationss revealed a sinus tract
or soft t issue abscess in ourpop ulatio nn [21]; it se em s that
th ese lat ter seco nd ary sign s areinfrequentlyy found in
leprosy. However, the presence of an ulcer andcelluli t iss is
common in leprosy patients with longstanding neuropathicfeett
suspected for osteomyeli t is . Contrary to diabetic foot l i
terature thesecondaryy MRI signs seem of no addit ional value in
diagnosingosteomyeli t iss in a population of leprosy patients with
longstandingneuropathicc foot disease. However, the value of these
findings in a patientpopu lationn of leprosy pa tie nts with neu ro
pa thy a nd clinical susp icion ofinflammation,, without
longstanding disease was not evaluated in thiss tudy. . For th is
purpose a s tudy is current ly conducted.Thee present s tudy
demonstrates in 9 events MRI changes suspected forosteomyelitiss at
the lateral side only (50%). In a minority of events thesecha nge
ss were found at th e m edial s ide only (16.7%). This is in con
tra st tothee resul ts found in a rec en t study of asy m pto m
atic ne ur op ath ic feet inleprosyy patients in which 90 percent
of the MRI changes were located atthee medial site of the foot
[15]. Most likely the biomechanics in the twopatientt groups (cl
inically unsuspected versus cl inically suspected inlong stand ingg
ne ur op at hic foot disease) are different. Biom echa
nicalanalysiss in early tarsal disintegration shows the highest s
tress to occurduringg the push off phase in the bones of the
lateral foot arch [12].Perhapss this is caused by inversion due to
paralysis of the lateralmusculature. . An analysis of the walking
cycle in two groups of leprosypatientss with neuropathic feet with
and without cl inical abnormalit iesmayy be of addit ional value in
order to analyse the stress distribution.Whenn a leprosy patient
with longstanding neuropathic foot disease issus pe cte dd of
osteom yeli t is clinical exa min ation la ck s specifici ty. C on
tra sten ha nc edd MRI with th e u s e of two -point Dixon che m
ical shift im aging, a sfat- sup pre sss ion tec hn iqu e is a
valua ble tech niq ue to dete ct o steomy eli t is .Thee primary MR
signs known from li terature, concerning diabeticneuropathicc foot
can adequately be assessed. MRI can serve as a one stepdiagnosticc
strategy to diagnose osteomyeli t is in leprosy patients with
alongstandingg neuropathic foot problem.
- 5 1 1 -
-
8/13/2019 File 85742
11/13
Chap t e r r 4SUMMARY YT h i ss s t u d y w a s u n d e r t a k
e n t o a n a l y z e t h e M RI f i n d i n g s in l e p r o s yp
a t i e n t ss w i t h n e u r o p a t h i c f ee t, s u s p e c t
e d fo r o s t e o m y e l i t i s . A s f ar a s w ek n o w ,, n o
p a p e r s c o n c e r n i n g o s t e o m y e l i t is a n d M R
I i n n e u r o p a t h i c l e p r o s yfee t t a re present .W e
e i n c l u d e d M R I e x a m i n a t i o n of 18 e v e n t s of
s u s p e c t e d o s t e o m y e l i t is i n1 22 l e p r o s y p
a t i e n t s . A ll p a t i e n t s w i t h l o n g s t a n d i n
g n e u r o p a t h i c fo otp r ob l ems s wer e c l i n i ca l l
y s us pec t ed f o r o s t eomye l i t i s . A l l pa t i en t su
n d e r w e n tt t h e M R I p r o t o c o l w i t h t h e i n c l
u s i o n o f t w o - p o i n t D i x o nc h e m i c a l l s h if t
i m a g i n g a s f a t - s u p p r e s s i o n s e q u e n c e
.For r t h e MRI ev a l u a t i o n we u s e d s i gn s t h a t a r
e de s c r i be d i n l i t e r a t u r e f o rde t ec t i ngg os t
eomye l i t i s i n d i abe t i c f ee t . The p r i mar y MRI s i
gns wer epos i t i vee i n 17 o f 18 pa t i e n t s . Th e s ec on
da r y MRI s i g ns wer e pos i t i ve in1 0 0 % % o f p a t i e n
t s .O u rr r e s u l t s s ho w t h a t MRI wi t h t he u s e o f
t w o- p o i n t D i xo n ch em i ca l s h if ti m ag i n gg i s a
p r om i s i ng d i ag no s t i c mod a l i t y to de t ec t o s t
eo my e l i t i s in t h ep r e s e n c e e of n e u r o - o s t e
o a r t h r o p a t h i c c h a n g e s i n p a t i e n t s w i t h
l e p r o sy .W h e n e v e rr a v a i l a b l e M R I c o u l d p
l a y a n i m p o r t a n t r o l e i n d e t e c t i n go s t e o
m y e l i t i s s i n l e p r o s y p a t i e n t s w i t h l o n g
s t a n d i n g n e u r o p a t h i c f e e t ,s u s p e c t e d d
f o r o s t e o m y e l i t i s .REFEREN ES S1.. Br an ds m a JW,
Macdonald MRC, Warren AG, Cross H, Sch wa rtz RJ, Solomon
S,, Kazen R, Gravem PE, Shrinivasan H. Assessment and
examination of theneurologicallyy impaired foot. Leprosy Review
2001; 72:263-275.
2.. Br ash PD, Foster JE} Anthony P, Tooke JE. Magnetic
resonance imagingtechniquess demonstrates soft t issue damage in
the diabetic foot . Diabet Med1999;; 16:55-61.
3.. Bra sh PD, Foster JE , Ven nart W, Daw J, Tooke JE .
Magnetic reso nan ceimagingg reveals Micro-haemorrhage in the feet
of diabetic patients with ahistoryy of Ulce ration. Diabet Med
1996; 1 3:9 73- 978 .
4.. Craig JG , Am in MB, Wu K, Eyler WR, va n Holsb eeck MT,
Bouffard JA, Shiraz iK.. Osteomyelitis of the diabetic foot: MR
imaging-pathologic correlation.Radiologyy 1997; 203:849-855.
5.. Crim JR , Seeger LI. Ima ging ev alu atio n of oste om ye
litis. Crit Rev DiagnImagingg 1994; 35:201.
6.. Dixon WT. Simple proton spectroscopic imaging. Radiology
1984;153:189-194. .
52
-
8/13/2019 File 85742
12/13
M R II a n d o s t e o m y e l i t i s i n l e p r o s y p a t i
e n t s7 .. F a b e r W R , H o e k s m a AF , v a n d e r K le ij
AJ , Ma as M, D i j k s t r a P F . D i ag n o s t i c
p r o c e d u r e s s f or s u s p e c t e d o s t e o m y e l i
t i s i n n e u r o p a t h i c fe et of l e p r o s y p a t i e n
t s .In t t J L epr 1 99 8 ; 66 :29A .
8 .. G o o d w i n D W , S a l o n e n D C , Y u J S , B r o s c
h m a n n J , T r u d e l l D J , R e s n i c k D L .P l a n t a r
r c o m p a r t m e n t s of t h e fo ot: M R a p p e a r a n c e i
n c a d a v e r s a n d d i a b e t i cp a t i e n t s .. R a d i
ol o gy 1 9 9 5 ; 1 9 6 : 6 2 3 - 6 3 0 .
9 .. G u o c h e n g Z , W e n z h o n g L, L i a n g b i n Y ,
Z h o n g m i n Y , X i a n g s h e n g C , T i s h e n g Z ,G a n
y u n n Y . An ep i d em i o l o g i ca l s u rv ey of d e fo rm i
t i e s an d d i s ab i l i t i e s a m o m g1 4 , 2 5 7 7 c a s e
s of l e p r o s y i n 1 1 c o u n t r i e s . L e p r o s y re v
ie w 1 9 9 3 ; 6 4 : 1 4 3 - 1 4 9 .
10. . H o e k s m a A F , F a b e r W R . A s s e s s m e n t of
s k i n t e m p e r a t u r e v ia p a l p a t i o n of t h en e u
r o p a t h i c c f o o t . 1 s tw o r l d c o n g r e s s of I S P
R M 2 0 0 1 .11. . J a c o b S , P a t il M K. S t r e s s a n a l
y s e s i n t h r e e - d i m e n s i o n a l fo ot m o d e l s of
n o r m a la n dd d i a b e t i c n e u r o p a t h y . F r o n t i
e r s o f M e d i c a l a n d B io lo g ic a l E n g i n e e r i n
g1999; ; 1-17.
12. . J a c o b S , P a t il M K . T h r e e - d i m e n s i o n
a l f oo t m o d e l l i n g a n d a n a l y s i s of s t r e s s e
si nn n o r m a l a n d e a r ly s ta g e H a n s e n ' s d i s e a
s e w i t h m u s c l e p a r a l y s i s . J o u r n a l o fR e h
a b i l i t a t io nn R e s e a r c h a n d D e v e l o p m e n t 1
9 9 9 ; 3 6 : 2 5 2 - 2 6 3 .
13 . . L i p m an B T, C o l l ie r B D, C a r r e ra G F , e t
a l . De t ec t i o n of o s t eo m y e l i t i s i n t h en e u r
o p a t h i c c f oo t: n u c l e a r m e d i c i n e , M R I a n d
c o n v e n t i o n a l r a d i o g r a p h y . C l i nN u c l e a
r r M e d 1 9 9 8 ; 2 3 : 7 7 - 8 2 .
14. . M a a s M , D i j k s t r a P F , A k k e r m a n E M . U
n i f o r m f at s u p p r e s s i o n i n h a n d s a n dfee tt t
h r o u g h t h e u s e of t wo -p o i n t D i x o n ch em i ca l s
hi f t MR i m a g i n g . R ad i o l o g y1 9 9 9 ; ; 2 1 0 : 1 8 9
- 1 9 3 .
15.. M a a s M , S l im F J , A k k e r m a n E M , F a b e r W
R . M RI i n c l in i c al ly a s y m p t o m a t i cn e u r o p a
t h i c c le p r o s y f ee t: a b a s e l i n e s t u d y . I n t
J L e p r o s y a n d O t h e r M y c o b a c tD i s s 2 0 0 1 ; 6
9 : 2 1 9 - 2 2 4 .
16. . M a r c u s C D , L a d a m - M a r c u s V J , L e o n e
J , M a l g r a n g e D , B o n n e t - G r a u s s e r a n dF M ,,
M e n t a n e a u B P . M R i m a g i n g of o s t e o m y e l i t
i s a n d n e u r o p a t h i co s t e o a r t h r o p a t h yy i n
t h e f ee t of d i a b e t i c s . R a d i o g r a p h i c s 1 9 9
6 ; 1 6 : 1 3 3 7 - 1 3 4 8 .
17. . Mo o re TE , Yu h W TC , Ka t h o l MH , E l -K h o u ry
GY, C o r s o n J D . A b n o rm a l i t i e s o ft h ee fo o t i n
p a t i en t s w i t h d i ab e t e s m e l l i t u s : f i n d i n
g s o n MR i m ag i n g . AJ R 1 9 9 1 ;1 5 7 : 8 1 3 - 8 1 6 .
.
18.. M o r r i s o n W B , L ed e r m an n HP , S c h w e i t z
e r ME. MR i m ag i n g of t h e d i ab e t i c fo ot .M R I I C l
i n N o r t h A m 2 0 0 1 ; 9 : 6 0 3 - 6 1 3 .
19. . M o r r i s o n W B , L e d e r m a n n H P , S c h w e i
t z e r M E . M R i m a g i n g o f i n f l a m m a t o r yco n d i
t i o n s s o f t h e an k l e an d foo t. MR I C l i n No r t h Am
2 0 0 1 ; 9 : 6 1 5 -6 3 7 .
2 0 . . M o r r i s o n W B , S ch w e i t ze r ME, B o c k GW ,
Mi t ch e l l DG, H u m e EL , P a t h r i a MN,R e s n i c k k D .
D i a g n o s i s of o s t e o m y e l i t i s : U ti li ty of f a
t - s u p p r e s s e dc o n t r a s t - e n h a n c e d d M R i m
a g i n g . R a d io l og y 1 9 9 3 ; 1 8 9 : 2 5 1 - 2 5 7 .
5 3
-
8/13/2019 File 85742
13/13
Chapterr 42 1 . . Mo r r i s o n W B , S ch we i t ze r ME, Gran
v i l l e B a t t e W , R ad ack DP , R u s s e l KM.
Os t eo m y e l i t i ss of t h e fo ot : r e l a t i v e i m p
o r t an ce o f p r i m ary an d s e co n d a r y MRi m a g i n g g
s i g n s . R a d i o l o g y 1 9 9 8 ; 2 0 7 : 6 2 5 - 6 3 2 .
2 2 . . On v l ee GJ . Th e C h a rco t F o o t ; a c r i t i c
a l r ev i ew an d o b s e rv a t i o n a l s t u d y o f ag r o u
pp o f 6 0 p a t i e n t s , Th es i s 1 9 9 8 .
2 3 . . P e te rf y C G , L i n a r e s R, S t e i n b a c h L S
. R e c e n t a d v a n c e s i n m a g n e t i c r e s o n a n c
ei m a g i n gg of t h e m u s c u l o s k e l e t a l s y s t e m
. R a d C li n N o r t h A m e r i c a 1 9 9 4 ;3 2 : 2 9 1 - 3 1 1
. .
2 4 . . R es n i ck D , N i w ay a m a G . D i ag n o s i s of b
o n e an d J o i n t d i s o rd e r s 3 rd ed i t io n v ol4 .. C h
a p t e r 6 6 : Os t e o m y e l i t i s , s ep t i c a r t h r i t
i s an d s of t t i s s u e i n f ec t i o n :O r g a n i s m s ..
W B S a u n d e r s C o m p a n y P e n s y l v a n i a 1 9 9 5 ; 2
4 8 6 - 2 4 9 2 .25 . . R i d l ey DS , J o p l i n g W H. C l a s
s i f i c a t i o n o f Lep ro s y acco rd i n g t o i m m u n i t
y . Af i ve - g ro u pp s y s t e m . I n t e r n a t i o n a l J o
u r n a l of L e p r o s y a n d O t h e r M y c o b a t e r i a lD
i s e a s e s s 1 9 9 6 ; 3 4 ( 3 ) : 2 5 5 - 2 7 3 .
26 . . S c h o n LC , E a s l e y M E , W e i n fe ld S B . C h
a r c o t n e u r o a r t h r o p a t h y of t h e fo ot a n da n k
l e .. C l i n ic a l O r t h o p a e d i c s a n d R e l a te d R
e s e a r c h 1 9 9 8 ; 3 4 9 : 1 1 6 - 1 3 1 .
27 . . T e h r a n z a d e h J , W o n g E , W a n g F , S a d i
g h p o u r M . I m a g i n g o f o s t e o m y e l i t i s i nt h
e e m a t u r e s k e l e t o n . M RI C l in N o r t h A m 2 0 0 1
; 3 9 : 2 4 0 - 2 5 0 .
28 . . T o m as MB , P a t e l M, M arwi n S E , P a l e s t r o
C J . Th e d i ab e t i c foo t. Th e B r i t i s hJ o u r n a ll o
f R a d i o lo g y 2 0 0 0 ; 7 3 : 4 4 3 - 4 5 0 .
29 . . W o r l d Hea l t h Org an i za t i o n . W eek l y ep i
d em i o l o g i ca l r e co rd , 2 0 0 2 ; 77(1}: 1-8.h t t p : /
/ w w w . w h o . i n t / w e r r
3 0 . . Y u J S . D i a b e t ic fo ot a n d n e u r o a r t h r
o p a t h y m a g n e t i c r e s o n a n c e i m a g i n ge v a l
u a t i o n . . T o p i c s i n M a g n e t i c R e s o n a n c e I
m a g i n g 1 9 9 8 ; 9 : 2 9 5 - 2 3 0 .
5 4
http://www.who.int/werhttp://www.who.int/wer