Embed Size (px)
Citation preview

Elung at 8Hz (cmH20/L)0 50 100 150 200 250 300 350
PaO
2 (m
mH
g)
0
200
400
600
800 CarbocholOleic AcidCombined Regression (n=54, R=0.860)Carbochol Regression (n=28, R=0.934)Oleic Acid Regression (n=26, R=0.764)
A
Rlung at 8Hz (cmH20/L/s)0 2 4 6 8 10
PaO
2 (m
mH
g)
0
200
400
600
800 CarbocholOleic AcidCombined Regression (n=54, R=0.685)Carbochol Regression (n=28, R=0.914)Oleic Acid regression (n=26, R=0.479)
B
Elung at 4Hz - Elung at 0.2Hz (cmH20/L)0 50 100 150 200 250
PaO
2 (m
mH
g)
0
200
400
600
800 CarbocholOleic AcidCombined Regression (n=54, R=0.817)Carbochol Regression (n=28, R=0.910)Oleic Acid Regression (n=26, R=0.708)
Cbaseline initial dose final dose
PaO
2 (mm
Hg)
PaC
o2 (mm
Hg)*10
0
100
200
300
400
500
MODERATESheep #3
0 2 4 6 8
Res
ista
nce
(cm
H20
/L/s
)
0
5
10
15
Frequency (Hz)0 2 4 6 8
Ela
stan
ce (c
mH
20/L
)
-50
0
50
100
150
Frequency (Hz)
baseline initial dose final dose
PaO
2 (mm
Hg)
PaC
o2 (mm
Hg)*10
0
100
200
300
400
500
600
700
800
MILDSheep #5
0 2 4 6 8
Res
ista
nce
(cm
H20
/L/s
)
0
1
2
3
4
5
6
baselineinitial dosefinal dose
F vs Rresp_ev1 F vs Col 8 F vs Rresp_ev5
Frequency (Hz)0 2 4 6 8
Ela
stan
ce (c
mH
20/L
)
0
20
40
60
80
Frequency (Hz)
PaO2PaO2
baseline initial dose final dose
PaO
2 (mm
Hg)
PaC
o2 (mm
Hg)*10
0
100
200
300
400
500
600
700
SEVERESheep #4
0 2 4 6 8
Res
ista
nce
(cm
H20
/L/s
)
0
5
10
15
20
25
Frequency (Hz)0 2 4 6 8
Ela
stan
ce (c
mH
20/L
)
0
100
200
300
Frequency (Hz)
baseline 5 min post 15 min post
PaO
2 (mm
Hg)
PaC
o2 (mm
Hg)*10
0
100
200
300
400
500
600
700PaO2PaCO2
MILDSheep #1
0 2 4 6 8
Res
ista
nce
(cm
H20
/L/s
)
0
1
2
3
4
5
6 baseline15 min postalbuterol
F vs Rresp_ev2 F vs Rresp_ev10
Frequency (Hz)0 2 4 6 8
Ela
stan
ce (c
mH
20/L
)
-40
-20
0
20
40
60
Frequency (Hz)
baseline initial dose final dose
PaO
2 (mm
Hg)
PaC
o2 (mm
Hg)*10
0
100
200
300
400
500
600
700
SEVERESheep #4
0 2 4 6 8
Res
ista
nce
(cm
H20
/L/s
)
0
5
10
15
20
25
30
Frequency (Hz)0 2 4 6 8
Ela
stan
ce (c
mH
20/L
)
0
100
200
300
Frequency (Hz)
baseline 5 min post 15 min post
PaO
2 (mm
Hg)
PaC
o2 (mm
Hg)*10
0
100
200
300
400
500
600
700MODERATE
Sheep #5
0 2 4 6 8
Res
ista
nce
(cm
H20
/L/s
)
0
2
4
6
8
10
12
14
Frequency (Hz)0 2 4 6 8
Ela
stan
ce (c
mH
20/L
)
-20
0
20
40
60
80
Frequency (Hz)
OVWFl
ow (L
iters
/sec
)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
EVW
Flow
(Lite
rs/s
ec)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
A B
0 2 4 6 8 10 12
Time (s)
Volum
e (L)
Flow (
L/s) 0.4
0.0
-0.4
-0.8
0.6
0.4
0.2
0.0
inspiration
expiration
OVWFl
ow (L
iters
/sec
)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
EVW
Flow
(Lite
rs/s
ec)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
A B
0 2 4 6 8 10 12
Time (s)
Volum
e (L)
Flow (
L/s) 0.4
0.0
-0.4
-0.8
0.6
0.4
0.2
0.0
inspiration
expiration
OVWFl
ow (L
iters
/sec
)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
EVW
Flow
(Lite
rs/s
ec)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
A B
0 2 4 6 8 10 12
Time (s)
Volum
e (L)
Flow (
L/s) 0.4
0.0
-0.4
-0.8
0.6
0.4
0.2
0.0
OVWFl
ow (L
iters
/sec
)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
EVW
Flow
(Lite
rs/s
ec)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
A B
OVWFl
ow (L
iters
/sec
)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
EVW
Flow
(Lite
rs/s
ec)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
A B
OVWFl
ow (L
iters
/sec
)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
EVW
Flow
(Lite
rs/s
ec)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
A B
OVWFl
ow (L
iters
/sec
)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
EVW
Flow
(Lite
rs/s
ec)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
A B
OVWFl
ow (L
iters
/sec
)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
EVW
Flow
(Lite
rs/s
ec)
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
Time (seconds)0 2 4 6 8 10 12
Vol
ume
(Lite
rs)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
A B
0 2 4 6 8 10 12
Time (s)
Volum
e (L)
Flow (
L/s) 0.4
0.0
-0.4
-0.8
0.6
0.4
0.2
0.0
inspiration
expiration
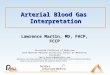
Figure 4. Oleic Acid Injury mechanics and ABG results. (A) a mild responder, (B) a moderate responder, and (C) a severe responder. Solid lines indicate lung R and E; dashed lines indicate respiratory system R and E. The top panels display arterial blood gas measurements, which were taken periodically. The middle and the bottom panels display the dynamic R and E estimates calculated from the EVW.
Relating Heterogeneous Lung and Respiratory System Mechanics ToGas Exchange Function During Mechanical Ventilation
C. Bellardine1, E.P. Ingenito2, A. Hoffman3, F. Lopez4, W. Sanborn4, and K.R. Lutchen1
1Biomedical Engineering, Boston University, Boston, MA, 2Pulmonary Division, Brigham and Women's Hospital, Boston, MA, 3Tufts Veterinary School of Medicine, N. Grafton, MA, 4Puritan Bennett/Tyco Healthcare, Pleasanton, CA
INTRODUCTION• Mechanical ventilation is required when a patient cannot generate sufficient pressures to maintain ventilation. The lungs’ ability to generate these pressures is governed primarily by the elastic recoil and the resistance of the respiratory system (E and R).
• With lung disease, R and E become elevated and increasingly more frequency dependent. The R and E from 0.1 to 8 Hz reflect the level and pattern of lung disease [1] and these data would aid in evaluating the efficacy of mechanical ventilation. Modern clinical ventilators apply simple flow waveforms containing energy primarily at one frequency. Therefore, the frequency dependence of R and E cannot be tracked.
• We have recently invented new broadband ventilation patterns known as Enhanced Ventilator Waveforms (EVWs) which contain discrete frequencies (from 0.1 to 8 Hz) blended to provide a tidal breath followed by a passive exhalation [2] (Figure 1). In principle, these waveforms allow for estimation of R and E from 0.1 to 8 Hz during ventilation.
OBJECTIVE AND METHODS
1. Lutchen, K.R. and B. Suki. “Understanding pulmonary mechancis using the forced oscillation technique.” Bioengineering Approaches to Pulmonary Physiology and Medicine. 1996.2. Kaczka, D.W., E. Ingenito, and K.R. Lutchen. “A technique to determine inspiratory impedance during mechanical ventilation: Implications for flow limited patients.” Annals of Biomedical Engineering. 27: 340-355, 1999.
RESULTS I (Figure 3: Bronchoconstriction)
Figure 2. The EVW was implemented in a prototype of the NPB840 (Puritan Bennett/Tyco Healthcare) ventilator shown above.
Figure 3. Bronchoconstriction mechanics and ABG results. (A) a mild responder, (B) a moderate responder, and (C) a severe responder. Solid lines indicate lung R and E; dashed lines indicate respiratory system R and E. The top panels display arterial blood gas measurements, which were taken periodically. The middle and the bottom panels display the dynamic R and E estimates calculated from the EVW. Data corresponding to baseline, final response, and Albuterol is shown.
• To advance the delivery of an EVW for routine clinical ventilation and evaluate whether features of dynamic R and E reflecting specific abnormalities in lung mechanical function with arterial blood gas levels.
•The EVW was applied in 5 sheep before and after a bronchial challenge and an oleic acid model of lung injury.
• We measured dynamic inspiratory R and E via the EVW and arterial O2 and CO2 levels throughout the development of each lung injury model.
Figure 1. EVW flow and volume are plotted vs. time. Note the enhanced frequency content in the inspiratory flow waveform and also the passive expiratory sections.
• In all sheep, the EVW sustains ventilation similarly to conventional ventilation but the EVW permitted insight on the level and distribution of lung disease.
• Data during bronchoconstriction revealed a range of constriction conditions from mild and homogeneous to severe and heterogeneous with airway closures. Often there was lack of complete improvement in R and E with albuterol or recruitment maneuvers. This was consistent with a pattern of airway closures that would not reopen.
• In both models of lung distress, the EVW revealed the progression of the disease and showed that the extent of the defects in ventilation were consistent with the heterogeneity of constriction and airway closure.
•Detailed analysis of all data (Figure 5-7) indicated that the degradation in PaO2 (gas exchange) was highly correlated with features of dynamic R and E associated with functional airway closures and heterogeneities. Both features would imply degradation in ventilation distribution leading to poor ventilation-perfusion matching.
•Degradation of ventilation is not apparent by quantifying the mean level of constriction in the lung, however, is highly evident by mechanical measures sensitive to the heterogeneity of disease in the lung and airway closure.
• Figure 8 suggest that on the order of 40-50% of the parallel alveoli can become derecruited before blood gases are affected, after which blood gases degrade rapidly. By tracking a patient’s low frequency elastance from some baseline condition, one can identify mechanical conditions for which gas exchange, while currently normal, are at risk of becoming rapidly degraded unless effective recruitment maneuvers are performed.
• We conclude that the EVW is a viable new ventilation method that can simultaneously provide clinically unique information regarding the mean level and heterogeneity of lung constriction as well as mechanical conditions that might lead to sudden degradation in gas exchange function in the lung. This unique information could be the basis to of more knowledgeable and effective clinician intervention with regards to treatment and ventilator weaning strategies.
Figure 6. Correlations between PaO2 levels and an (A) index of airway closure as calculated from RESPIRATORY SYSTEM elastance and (B) index of heterogeneity as calculated from RESPIRATORY SYSTEM resistance. Data from bronchoconstriction protocol (via carbochol) is shown in blue and from oleic acid injury protocol is shown in red. The linear regressions for the carbochol (blue-dashed), oleic acid (red-dashed), and combined data (black-solid) are also shown with the respective n and R-values noted in the legend.
RESULTS III (Figure 5 and 6: Correlations)
(A) (B) (C)
RESULTS II (Figure 4: RDS Model)
REFERENCES
(A) (B) (C)
Eresp at 0.2Hz (cmH20/L)0 20 40 60 80 100
PaO
2 (m
mH
g)
0
200
400
600
800
CarbocholOleic AcidCombined Regression (n=49, R=0.867)Carbochol Regression (n =28, R=0.862)Oleic Acid Regression (n =21, R=0.865)
A
Rresp at 0.2Hz - Rresp at 8Hz (cmH20/L/s)0 2 4 6 8 10 12 14 16 18
PaO
2 (m
mH
g)
0
200
400
600
CarbocholOleic AcidCombined Regression (n=49, R=0.655)Carbochol Regression (n=28, R=0.921)Oleic Acid Regression (n=21, R=0.677)
B
Elung at 0.2Hz (cmH20/L)0 10 20 30 40 50 60 70 80
PaO
2 (m
mH
g)
0
200
400
600
800 CarbocholOleic AcidCombined Regression (n=54, R=0.855)Carbochol Regression (n=28, R=0.838)Oleic Acid Regression (n=26, R=0.894)
A
Rlung at 0.2Hz - Rlung at 8Hz (cmH20/L/s)0 2 4 6 8 10 12 14 16 18
PaO
2 (m
mH
g)
0
200
400
600
CarbocholOleic AcidCombined Regression (n=54, R=0.825)Carbochol Regression (n=28, R=0.918)Oleic Acid Regression (n=26, R=0.714)
B
Figure 5. Correlations between PaO2 levels and an (A) index of airway closure as calculated from LUNG elastance and (B) index of heterogeneity as calculated from LUNG resistance. Data from the bronchoconstriction protocol (via carbochol) is shown in blue and from the oleic acid injury protocol is shown in red. The linear regressions for the carbochol (blue-dashed), oleic acid (red-dashed), and combined data (black-solid) are also shown with the respective n and R-values noted in the legend.
RESULTS III (Figure 7: Correlations)
% Non-ventilated Lung(calculated using Elung at 0.2 Hz)
0 20 40 60 80
% B
asel
ine
PaO
2
0
20
40
60
80
100
% Non-ventilated Lung(calculated using Eresp at 0.2 Hz)
0 20 40 60 80
% B
asel
ine
PaO
2
0
20
40
60
80
100
% Non-ventilated
Lung100*
)2.0()2.0(
1
HzEHzEbaseline
• We recast data from Figure 5A and Figure 6A to examine the relationship between loss of lung units participating in ventilation and degradation in PaO2 levels.
• Considering the lung as a set of parallel gas exchanging units, we can derive the following relationship to reflect percent non-ventilated lung :
RESULTS IV (Figure 8: % Non-ventilated Lung)
Figure 7. Correlations between PaO2 levels and an (A) index of airway wall shunting as calculated from LUNG elastance, (B) index of airway resistance as calculated from LUNG resistance, and (C) index of heterogeneity as calculated from LUNG elastance. Data from the bronchoconstriction protocol (via carbochol) is shown in blue and from the oleic acid injury protocol is shown in red. The linear regressions for the carbochol (blue-dashed), oleic acid (red-dashed), and combined data (black-solid) are also shown with the respective n and R-values noted in the legend. Similar results were found for RESPIRATORY SYSTEM data.
SUMMARY
Figure 8. Percent baseline PaO2 vs % non-ventilated lung (A) calculated from Elung at 0.2 Hz and (B) from Eresp at 0.2 Hz. A Gompertz 3-parameter model was fit to the data for visual effect.
A B