Embed Size (px)
Citation preview

BritishJournal ofOphthalmology 1994; 78: 266-270
Fibrous dysplasia of the orbit
K Bibby, R McFadzean
AbstractTwelve patients with fibrous dysplasia of theorbit are reviewed and the ophthalmic findingsdescribed. Three case histories are presentedin detail. Six patients were managed conserva-tively; four have shown radiological progres-sion of the disease. Six patients underwentsurgery. A conservative procedure, compris-ing debulking dysplastic bone, was carried outin four - all required further surgery includingradical excision in two patients. Two subjectshad primary radical operations. No recurrencewas encountered in the four patients who hadundergone radical surgery. It would appearthat fibrous dysplasia is not a disease confinedto adolescence but may continue into adult-hood, and even middle age. Patients may neverrequire surgery, but require follow up for lateprogression. If surgical intervention is deemednecessary, an attempt should be made toexcise all dysplastic bone, since progressionof the disease after conservative surgery isrelatively common.(BrJ Ophthalmol 1994; 78: 266-270)
Leicester Royal InfirmaryK BibbyR McFadzeanCorrespondence to:Ms Kim Bibby, LeicesterRoyal Infirmary, LeicesterLEIAccepted for publication23 September 1993
Fibrous dysplasia is a benign, slowly progressivedisorder of bone, where normal cancellous boneis replaced by fibrous tissue and immature wovenbone. It presents in childhood or early adoles-cence,' typically arresting at puberty.2The lesions were first described by von
Recklinghausen in 1891,3 but it was Lichtensteinin 1938 who recognised the condition as adistinct entity and suggested the name 'fibrousdysplasia'.4 The condition occurs in the mono-stotic form, where only one or contiguous bonesare involved, or polyostotic form where severaldistinct areas of the skeleton are affected.Fibrous dysplasia can occur in conjunction withskin pigmentation and endocrine disorders(Albright's syndrome).5 The disease has beenprevalent for a long time; it was described in theskeleton of a seventh century Anglo Saxon,6 andin a skull found in Tennessee, dated AD 1480(plus or minus 130 years, carbon dating).7More than 1500 cases were reported in the
literature up until 1971,8 but estimates of the
Table I Fibrous dysplasia - bones affected
PatientBone 1 2 3 4 5 6 7 8 9 10 11 12 Total
Frontal - + - - + + - + + + + + 8Sphenoid + + + + + + + 7Optic foramen + + + + + + 6Ethmoid - + + . . . . . .2Maxilla - + + . . . . . .2Occiput - - + . . .+ 2Parietal - - +. . . . . ..1Petrous temporal - - +. . . . . ..1Pterygoid - +. . . . . . . . . . .1Mandible - +.
frequency of fibrous dysplasia of the craniofacialbones vary from 'rare' (5/764 cases of orbitaltumours at the Mayo Clinic over 26 years)9 to 'notuncommon' (144 cases of fibrous dysplasia of theskull).'0The aetiology remains obscure, but the condi-
tion is widely believed to be a congenital anomalyof bone forming mesenchyme.4 Hypothesesinclude misdifferentiation of mesenchymaltissue,4 an 'arrest of bone maturation in thewoven bone stage','" and a 'disturbance ofpostnatal cancellous bone maintenance'. 12 Atraumatic aetiology has been suggested but notwidely supported." 14
Seventy per cent of cases involve only onebone/contiguous bones and are classed as mono-stotic, while 30% of cases are polyostotic. 13 Skullinvolvement occurs in 10-27% of patients withmonostotic, and in 50% of patients with poly-ostotic disease.'5 Almost 100% of patients withextensive disease have skull involvement,'5"'8 butmost patients with affected craniofacial boneshave the monostotic form of the disease. 19 20
Ocular complications have been classified intoprimary and secondary processes.2' Primarycomplications include involvement of the frontalbone with proptosis; the skull base with extra-ocular muscle palsies and trigeminal neuralgia;the optic canal with visual loss and optic atrophy;the sphenoid bones with chiasmal compression;and the maxillary bone with epiphora. Second-ary complications comprise malignant change,ossifying fibroma formation, and development ofa mucocele. Malignant transformation mostcommonly takes the form of sarcomatouschange, occurring spontaneously in 0 5% ofcases.22
Other tumours known to develop in areas offibrous dysplasia include cutaneous fibro-myxoma23 and meningioma.24
Materials and methodsTwelve patients with orbital fibrous dysplasiaunderwent full neuro-ophthalmic assessment, 10patients presenting for initial diagnosis and twofor follow up after management elsewhere. Allpatients had a skull x ray with serial films toassess progress. Five patients underwent com-puted tomography (CT) and two patients hadmagnetic resonance imaging (MRI).
Indications for surgical intervention com-prised a deterioration in visual function, dis-figurement, and intractable pain. Tissue wassent for histology from all surgically treatedpatients and a diagnostic biopsy alone wascarried out in two patients.
ResultsThere were five male and seven female patients.Age at diagnosis ranged from 5 years to 45 years,
266
on 4 January 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.78.4.266 on 1 April 1994. D
ownloaded from

Fibrous dysplasia ofthe orbit
Table 2 Fibrous dysplasia - symptoms
Symptom Number ofpatients affected
Visual upset 4Proptosis 5Craniofacial swelling 5Headaches/periorbital pain 5Epiphora 1
with an average age of 18 years. Eleven patientshad idiopathic fibrous dysplasia, and one hadAlbright's syndrome. The skull bones affectedare shown in Table 1. Most commonly involvedwere the frontal bone (eight patients) and thesphenoid bone (seven patients). Bilateral lesionsoccurred in three patients, one of whom hadextensive skeletal involvement. Optic foraminalchanges on plain x ray were noted in six patients.The mean follow up period was 8 years,
ranging from 1 to 30 years.
SYMPTOMSThe presenting symptoms are shown in Table 2.Two patients were asymptomatic and diagnosedafter routine skull x ray following a trivial headinjury, while the patient with Albright's syn-drome presented with increased skin pigmenta-tion and precocious puberty.
Table 3 Ophthalmicfindings
DownwardVisual Ocular motilty Proptosis displacement
Patients acuity Field loss deficit (mm) (mm) Disc
1 CF Centrocaecal scotoma - 3-5 - Swollen2 NPL - 10° Exotropia* 3 0 - Pale3 6/18 Central scotoma - 2 5 - Normal4 6/6 Slight constriction - - - Normal5 6/6 - - 40 - Normal6 6/6 Enlarged blind spot Decreased elevation 10-0 2-0 Swollen7 6/6 - - - - Normal8 6/6 - - 2-0 - Normal9 6/6 - - - 2-0 Normal10 6/6 Temporal constriction - 2-0 - Normal11 6/6 - - 3 0 2-0 Normal12 6/6 - - 11-0 - Pale
CF=counting fingers; NPL=no perception of light.*This patient had a history of amblyopia.
... ,
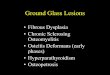
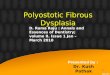
Figure I Computed tomogram ofpatient 1. Well defined mass at the apex ofthe right orbit,involving the greater wing ofthe sphenoid and surrounding the opticforamen.
Table 4 Effects ofsurgery
Patient Preoperative Postoperative
1 Visual acuity - counting fingers Visual acuity - 6/60Centrocaecal scotoma Reduced3-5 mm Proptosis No proptosis
2 No perception of light No change3 mm Proptosis 1 mm Proptosis
5 Constricted visual field Full field6 Enlarged blind spot Full field
10mm Proptosis 4mm Proptosis10 Temporal field defect Reduced12 11 mm Proptosis 4mm Proptosis
OPHTHALMIC SIGNSThe presenting ophthalmic signs are shown inTable 3. The commonest sign was proptosis innine patients, accompanied by downward dis-placement of the globe in three patients. Loss ofvisual acuity in three patients ranged from 6/18to no perception of light.
OTHER FINDINGSOne patient developed conductive deafnesssecondary to secretory otitis media after block-age of the Eustachian tube.
MANAGEMENT AND OUTCOMESix patients were managed conservatively, with amean follow up period of 4 5 years (range 1 to 7years). Four patients have shown radiologicalprogression without significant change in visualfunction, while in two patients the diseaseappears to have arrested clinically and radio-logically at the ages of 25 and 29 years.
Six patients underwent surgery. A conserva-tive operation, comprising debulking andreshaping dysplastic bone, was carried out infour patients but all required further surgery,including a radical excision in two patients. Twopatients had primary radical surgery.The surgical and overall outcomes are shown
in Tables 4 and 5 respectively. Followingsurgery, field defects improved in four patientsand proptosis was reduced substantially in fourpatients. However, after conservative surgery allfour patients developed recurrent disease,requiring further operations. In one patient thedisease remains active after 30 years. No recur-rence was encountered in two patients who hadradical procedures after conservative operations,or in two patients who had primary radicalsurgery. The mean follow up period after radicalsurgery was 3 3 years (range 2 to 7 years).
Postoperative complications developed inthree patients, in the form of transient verticaldiplopia following frontal bone resection in twopatients, and a postoperative subdural haema-toma requiring surgical drainage in one patient.There were no long term sequelae.
CASE ILLUSTRATIONS
CASE 1A 13-year-old boy complained of graduallydeteriorating vision in the right eye for 6 months.Visual acuity in the right eye was reduced tocounting fingers at 1 metre, with an afferent
267
on 4 January 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.78.4.266 on 1 April 1994. D
ownloaded from

Bibby, McFadzean
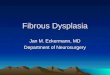
Figure 2 Computed tomogram ofpatient I following radical surgery, with slight residual softtissue scarring at the orbital apex.
pupillary defect and papilloedema. The rightvisual field showed a dense centrocaecal scotomaand there was 3-5 mm of axial proptosis of theright eye. The left eye appeared healthy.A CT scan revealed a well defined calcified
mass involving the right medial sphenoid(greater wing) and anterior clinoid process,extending around the optic foramen (Fig 1).A right frontotemporal craniotomy was
performed and the dysplastic bone excised com-pletely. Histology confirmed the diagnosis.Visual acuity improved to 6/60 and the centro-caecal scotoma was reduced. The disc swellingand proptosis resolved.A follow up CT scan showed complete
removal of the lesion (Fig 2). This patient hasbeen followed up for 3 5 years with no evidenceof recurrence.
CommentRadical excision resulted in an improvement invisual function and cosmetic appearance in thispatient.
CASE 2A 35-year-old female presented with facial asym-metry, at the age of 5 years. When aged 6 years
Table 5 Summary ofmanagement and outcome
Age at Duration of Number ofoperations Presentdiagnosis active disease age
Patient (years) (years) Conservative Radical Present condition (years)
1 13 1* - 1 No evidence of fibrous dysplasia 162 5 30 5 - Active 353 32 2 - - Active 344 12 5 - - Active (Albright's) 175 13 12* 1 1 No evidence offibrous dysplasia 276 10 2* 2 1 No evidence offibrous dysplasia 197 19 - - Static. 258 23 - - Static- 299 13 7 - - Active 2010 18 4 4 - Static 3311 9 1 - - Active 1012 45 5* - 1 No evidence offibrous dysplasia 51
*Progress of disease halted by radical surgery.
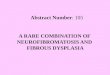
Figure 3 Skull x ray ofpatient 2 (lateral view), showingextensive involvement ofthe left side ofthe skull andfacialbones.
decompressive surgery to the left maxilla forproptosis and upward displacement of the globewas carried out. Gradual deterioration in thevisual acuity in the left eye occurred at the age of10 years and the left orbit was decompressed.Visual acuity continued to decrease in the left eyeuntil by the age of 14 years she had no perceptionof light owing to bony occlusion of the opticforamen. At the age of 21 she underwent furthercosmetic surgery and when aged 24 years afurther decompression of the left orbit wasrequired to reduce proptosis. There was noapparent progression of the disease processduring the next 8 years. At the age of 32 years shebecame pregnant for the first time and during thesixth month ofher pregnancy noticed an increasein the size ofher left mandible with lumps on herhard palate. Three years later she again becamepregnant when the swellings of the left mandibleand maxilla further increased in size. A recentskull x ray showed extensive sclerotic bonychange involving the left frontal bone, ethmoid,inferior orbital margin, nasal bone, pterygoidplate, maxilla, and mandible (Fig 3).
This patient is presently awaiting furthersurgery.
CommentDespite five conservative procedures this patientcontinues to deteriorate both functionally andcosmetically.
CASE 6A 10-year-old boy developed painless proptosisof the left eye. Initial visual acuity was 6/6 rightand left, pupillary reactions and extraocularmovements were normal, optic discs werehealthy, and visual fields full. A left frontal
268
on 4 January 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.78.4.266 on 1 April 1994. D
ownloaded from

Fibrous dysplasia ofthe orbit
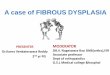
Figure 4 Patient 6. Note left proptosis and downward displacement ofthe globe, withfrontalis overaction to compensatefor left ptosis.
craniotomy was performed to debulk dysplasticbone for cosmetic reasons. At 2 years' follow uphe complained of intermittent blurring of visionin the left eye. Visual acuity was 6/6 right and leftand the pupillary reactions were normal, butthere was diminished elevation of the left eye,with vertical diplopia on upgaze. The left opticdisc was swollen, left proptosis had increased to10 mm, and there was 2 mm downward displace-ment of the globe and a mild ptosis (Fig 4). Theleft visual field demonstrated an enlarged blindspot.A CT scan showed a large oval lesion affecting
the roof and medial wall of the left orbit withextension into the nasal cavity and displacementof the nasal septum. The optic canal was spared(Fig 5). A bifrontal craniotomy and block dissec-tion was carried out. The medial wall and roof ofthe left orbit were excised with all dysplasticbone. Histology confirmed the diagnosis.
Postoperatively he made a good recovery.
Figure S Computed tomogram ofpatien 6 showing oval lesion involving medial wall of theleft orbit and extending into the nasal cavity. The nasal septum is displaced.
Visual acuity was maintained at 6/6, ocularmovements are full, the left optic disc swellingresolved, and the left proptosis was reduced to4 mm.
CommentAn initial conservative decompression wasinsufficient to control the functional and cos-metic effects of the disease process. Secondaryradical excision has proved beneficial in thispatient.
DiscussionIn nine of our 12 patients the aetiology of thefibrous dysplasia was unknown (idiopathic),which is the common experience.'025 Twopatients attributed their fibrous dysplasia tominor trauma, but it is likely that the associationwas purely incidental.The frontal and sphenoid bones were affected
most frequently, as in two other series,'8 26 27 andthe optic foramen was involved in half ourpatients, a higher proportion than in two otherseries: 10 of 50 patients'8 and five of 16 patients.28This discrepancy may reflect the prolongedfollow up of some of our patients.Three patients demonstrated a decrease in
visual acuity - more than in one series,28 whereonly two of 16 children had reduced visual acuity(although this may have been because of theiryoung age), but less than in a further series of 10patients, of whom eight suffered loss of visualacuity.'8 Visual field defects noted in five of ourpatients are not extensively documented in theliterature, although a central scotoma wasrecorded in one patient29 and a bitemporalhemianopia in another.30
In common with other series, the most fre-quent ophthalmic sign was proptosis, affectingnine of our 12 patients.27283'-33 Although sixpatients had radiological evidence of opticforaminal involvement only two developed opticatrophy, and one papilloedema. It is recognisedthat compressive optic neuropathy does notalways supervene, even with anatomical narrow-ing of the optic canal.27 Formerly, it was believedthat the progression of fibrous dysplasia sloweddown or stopped during adolescence.2 However,many exceptions to this premise are to befound16 43v6 including five patients in this serieswhose disease progressed after their teenageyears. Only three patients demonstrated spon-taneous arrest of their disease, and late reactiva-tion occurred during pregnancy in one patientafter 8 quiescent years. Reactivation or exacerba-tion of active disease is particularly liable tooccur during gestation.37-39
Conservative surgery was previously regardedas the treatment of choice.352 However, therecurrence rate following conservative opera-tions was significant at 25% in two series," 26 andin 20 -of 41 patients, 13 of 16, and 13 of 15patients in other series.2 17 28 Radical surgery wasavoided as it was thought that the disease mayhave a self-limiting course and there was a risk ofcomplete excision causing more deformity and/or functional loss than the disease itself. Follow-ing recent advances in anaesthesia and cranio-
269
.....
--..,..-.r
ooki.
on 4 January 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.78.4.266 on 1 April 1994. D
ownloaded from

Bibby, McFadzean
facial/plastic surgery, primary radical excisionwas carried out on five patients without recur-rence after 9 years of follow up, while excision ofall dysplastic bone in another three patientsproduced good functional and cosmetic results,although the follow up period was not specified.43The four patients who underwent radical opera-tions in our series have demonstrated no recur-rence of the disease during an average follow upperiod of 3 3 years, while all four patients whoinitially had conservative surgery requiredfurther operations. Two patients treated byconservative surgery have required four and fiveoperations respectively and a sixth operation isproposed for the latter.Four of five patients with visual field loss have
improved postoperatively and all have improvedcosmetically. Similar results were recorded intwo other series"" and a recent case report.29 Inaccordance with the rate of complications forcraniofacial surgery in the literature2843"4 onlyone of our patients developed a significant post-operative problem in the form of a subduralhaematoma, but after surgical drainage therehave been no long term sequelae. Attempts toarrest the disease process by radiotherapy in thepast have been abandoned owing to an unaccept-able 44% malignant transformation rate.2245
ConclusionReview of the histories of our 12 patients makesit apparent that fibrous dysplasia is not a diseaseconfined to adolescence but may continue intoadulthood and sometimes middle age. Somepatients may never require surgery, but dorequire regular follow up for late progression,particularly during pregnancy. If surgical inter-vention is deemed necessary, an attempt shouldbe made to excise all dysplastic bone and effect acure. Progression of the disease after conserva-tive surgery seems to be relatively common.
We thank Mr T A H Hide, consultant neurosurgeon, for referralof these cases for neuro-ophthalmic assessment, Mrs JuneCunningham, medical photographer, for the illustrations, andMiss Rachel Gowing for careful preparation of this manuscript.
1 Rootman J. Diseases of the orbit. Philadelphia: Lippincott,1988: 356-9.
2 Nager GT, Kennedy DW, Kopstein E. Fibrous dysplasia: areview of the disease and its manifestations in the temporalbone. Ann Otol Rhinol Laryngol 1982; 92 (suppl): 5.
3 Von Recklinghausen F. Die Fibrose oder deformierendeOstitis, die Osteomalacie und die oesteoplastische carcinosein ihren gegenseitigen Beziehungen. Festschrift RudolfVirchow zum 13. Oktober, Berlin: 1891.
4 Lichtenstein L, Jaffe HL. Polyostotic fibrous dysplasia. ArchSurg 1938; 36: 874-98.
5 Albright F, Butler MA, Hampton AO, Smith P. Syndromecharacterized by osteitis fibrosa disseminata, areas ofpigmentation and endocrine dysfunction with precociouspuberty in females. N EnglJ Med 1937; 216: 727-46.
6 Wells C. Polyostotic fibrous dysplasia in a 7th century Anglo-Saxon. BrJ Radiol 1963; 36: 925-6.
7 Gregg JB, Reed A. Monostotic fibrous dysplasia in thetemporal bone: a late prehistoric occurrence. Am J PhysAnthropol 1980; 52: 587-93.
8 Slow IN, Stern D, Friedman EW. Osteogenic sarcoma arisingin pre-existing fibrous dysplasia: report of case. J Oral Surg1971; 29: 126-9.
9 Henderson JW. Orbital tumors. 2nd ed. New York: Brian CDecker, 1980: 70-4.
10 Van TilburgW. Fibrous dysplasia. In: Vinken PJ, Bruyn GW,eds. Handbook of clinical neurology. Vol 14. Amsterdam:North Holland, 1972: 163-212.
11 Reed RJ. Fibrous dysplasia of bone. Arch Pathol 1%3; 75:480-95.
12 Aegerter EE, Kirkpatrick JA Jr. Orthopedic diseases. 3rd ed.Philadelphia: Saunders, 1968: 182-92.
13 Schlumberger HG. Fibrous dysplasia of single bones (mono-stotic fibrous dysplasia). Mil Surg 1947; 99: 504-27.
14 Reese AB. Fibrous dysplasia of bone. In: Tumours of the eye.3rd ed. London: Harper and Row, 1976: 326-7.
15 Windolz F. Cranial manifestations of fibrous dysplasia ofbone. AmJ Roentgen 1957; 58: 51-63.
16 Harris WH, Dudley HR Jr, Barry JR. The natural history offibrous dysplasia. J BoneJt Surg 1962; 44A: 207-33.
17 Leeds N, Seaman WB. Fibrous dysplasia of the skull and itsdifferential diagnosis. Radiology 1962; 78: 570-82.
18 Sassin JF, Rosenberg RN. Neurological complications offibrous dysplasia of the skull. Arch Neurol (Paris) 1968; 18:363-9.
19 Calderon M, Brady HR. Fibrous dysplasia of bone with opticforamina involvement. AmJ7 Ophthalmol 1969; 68: 513-5.
20 Moore RT. Fibrous dysplasia of the orbit. Surv Ophthalmol1969; 13: 321-34.
21 Liakos GM, Walker CB, Carruth JAS. Ocular complicationsof craniofacial fibrous dysplasia. BrJ Ophthalmol 1979; 63:611-6.
22 Schwartz DT, Alpert M. The malignant transformation offibrous dysplasia. Amj Med Sci 1964; 247: 1-20.
23 Lick RF, Viehweger F. A contribution to the diagnosis offibrous dysplasia of the skeletal system. Fortschvitte aufdemGebiete der Roentgenstratliten und der Nukkarmedezin 1962;97: 33-8.
24 Frankel J, Lanotti F, Powell M, Schon K. Meningioma - anunrecognised complication of fibrous dysplasia of the skull?J Neurol Neurosurg Psychiatry 1989; 52: 546-7.
25 Lichtenstein I, Jaffe HL. Fibrous dysplasia of bone. ArchOphthalmol 1942; 33: 175-89.
26 Edgerton MJ, Persing JA, Jane JA. The surgical treatment offibrous dysplasia. Ann Surg 1985; 202: 459-79.
27 Shields JA. Diagnosis and management of orbital tumours.Philadelphia: Saunders, 1989.
28 Moore AT, Buncic JR. Fibrous dysplasia of the orbit inchildhood. Ophthalmology 1985; 92: 12-20.
29 Weisman JS, Major US, Helper RS, Vintners V. Reversiblevisual loss caused by fibrous dysplasia. Am J Ophthalmol1990; 110:244-9.
30 Weyand RD, Craig WM, Rucker CW. Unusual lesionsinvolving the chiasm. Proc Mayo Clinic 1952; 27: 505-15.
31 Mortada A. Fibrous dysplasia of the orbital bones.BrJr Ophthalmol 1961; 45: 737-40.
32 Schonder A. Fibrous dysplasia of the bone with proptosis.AmJ Dis Child 1977; 131: 678-9.
33 Friot JM, Bleicher B, Galoisy C, Bretagne MC, Chobaut JC,Wayoff M. Four cases of exophthalmos of unusual naso-sinus origin. Revue d'oto-neuro-ophtalmologie 1978; 50:141-9.
34 Frazer AK, Hannah RH, Buxton PH. Fibrous dysplasia of theethmoid presenting with proptosis. Br J Surg 1969; 56:300-7.
35 Ramsey HE, Strong EW, Frazell EL. Fibrous dysplasia of thecraniofacial bones. AmJ7 Surg 1968; 116: 542-7.
36 Chen YR, Fairholm D. Fronto-orbito-sphenoidal fibrousdysplasia. Ann Plast Surg 1985; 15: 190-203.
37 Hunter D, Turnbull HL. Hyperparathyroidism; generalisedosteitis fibrosa. BrJ Surg 1931; 32: 203-84.
38 Dockerty MD, Ghormley BK, Kennedy RLJ, Pugh DG.Albright's syndrome. Arch Intern Med 1945; 75: 357-75.
39 Bonduelle M, Claisse R. Dysplasie Fibreuse des os etSyndrome d'Albright leur place nosologique. Sem Hop Pan's1948; 24: 514-21.
40 Gass JDM. Orbital and ocular involvement in fibrous dys-plasia. South MedJ 1965; 58: 324-9.
41 Rychener RO, Murfey F. Periorbital fibrous dysplasia. TransAm Ophthalmol Soc 1955; 53: 155-74.
42 Feiring W, Feiring EH, Davidoff ML. Fibrous dysplasia ofthe skull.J Neurosurg 1951; 8: 377-97.
43 Munro IR, Chen YR. Radical treatment for fronto-orbitalfibrous dysplasia: the chain-link fence. Plast Reconstr Surg1981; 67: 719-30.
44 Whitaker LA, Munro IR, Salyer KE, Jackson IT, Ortiz-Monasterio F, Marchac D. Problems and complications in793 craniofacial operations. Reconstr Surg 1979; 64:198-203.
45 Huvos AG, Higinbotham NL, Miller TR. Bone sarcomasarising in fibrous dysplasia. J Bone_Joint Surg (Am) 1972; 54:1047-56.
270
on 4 January 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.78.4.266 on 1 April 1994. D
ownloaded from