Embed Size (px)
Citation preview
FIBROUS DYSPLASIA (FD)
By : Dwi Damar Andriyani
Consultant : dr. Edy Moeljono, Sp.Rad (K)RA
TEXT BOOK READING DAVID SUTTON VOL.2PAGE 1130-1140
Sutton page 1130-1140
Congenital skeletal anomalies Skeletal dysplasia
1. Cleidocranial dysplasia
2. Picnodisostosis
3. Acroosteolisis
4. Osteogenesis imperfecta
5. Fibrogenesis imperfecta
6. Osteopetrosis
7. ........
8. Fibrous dysplasia
9. .......
40. Achondrogenesis
Chromosomal disorder
Introduction
Aetiology : unknown Female>male Bone may be affected
– Pelvis– Femur– Skull– Spine/vertebral collapse unusual
Usually found incidentally/ follow pathological fracture
Onset : 10-30 yr old or first decade Prognosis : worse when lesion occurs early in life
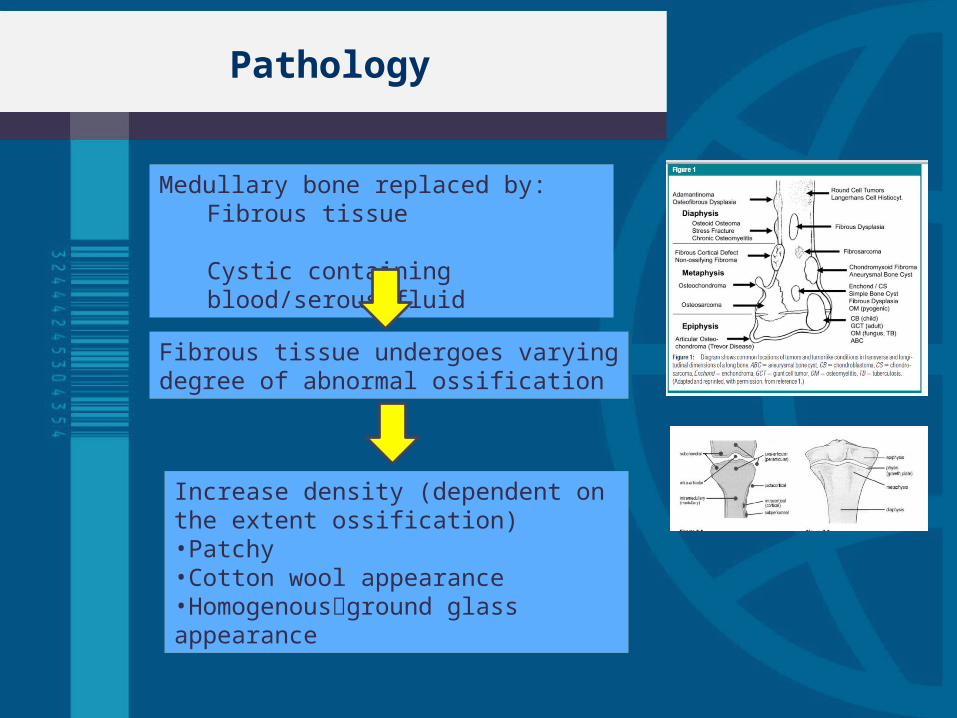
Pathology
Medullary bone replaced by:Fibrous tissue Cystic containing blood/serous fluid
Fibrous tissue undergoes varying degree of abnormal ossification
Increase density (dependent on the extent ossification)•Patchy•Cotton wool appearance•Homogenousground glass appearance
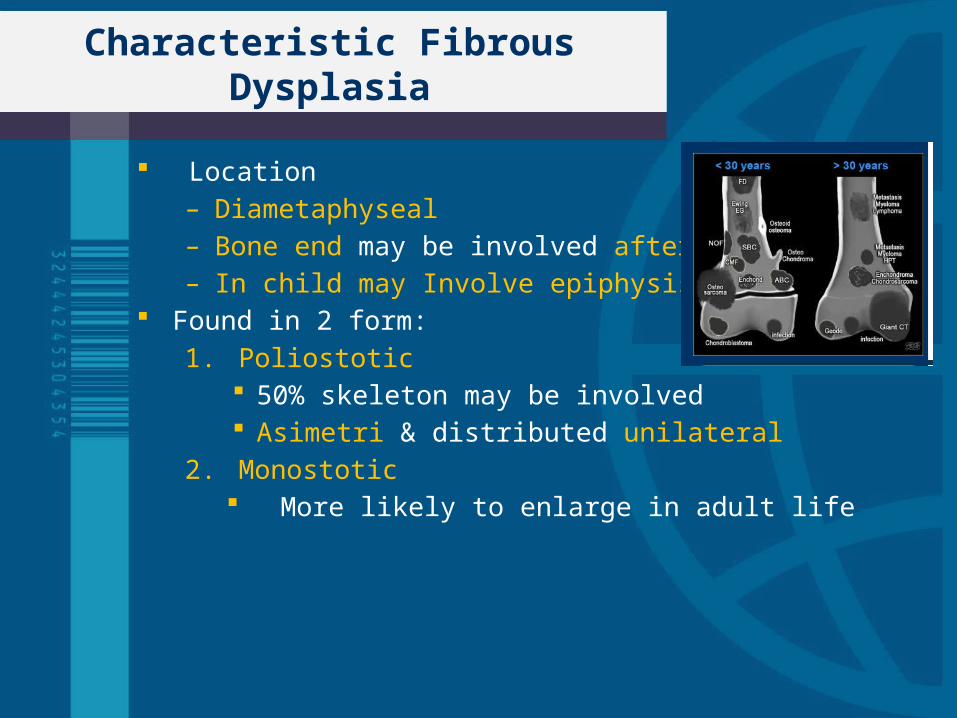
Characteristic Fibrous Dysplasia
Location– Diametaphyseal– Bone end may be involved after fusion– In child may Involve epiphysis
Found in 2 form:
1. Poliostotic 50% skeleton may be involved Asimetri & distributed unilateral
2. Monostotic More likely to enlarge in adult life
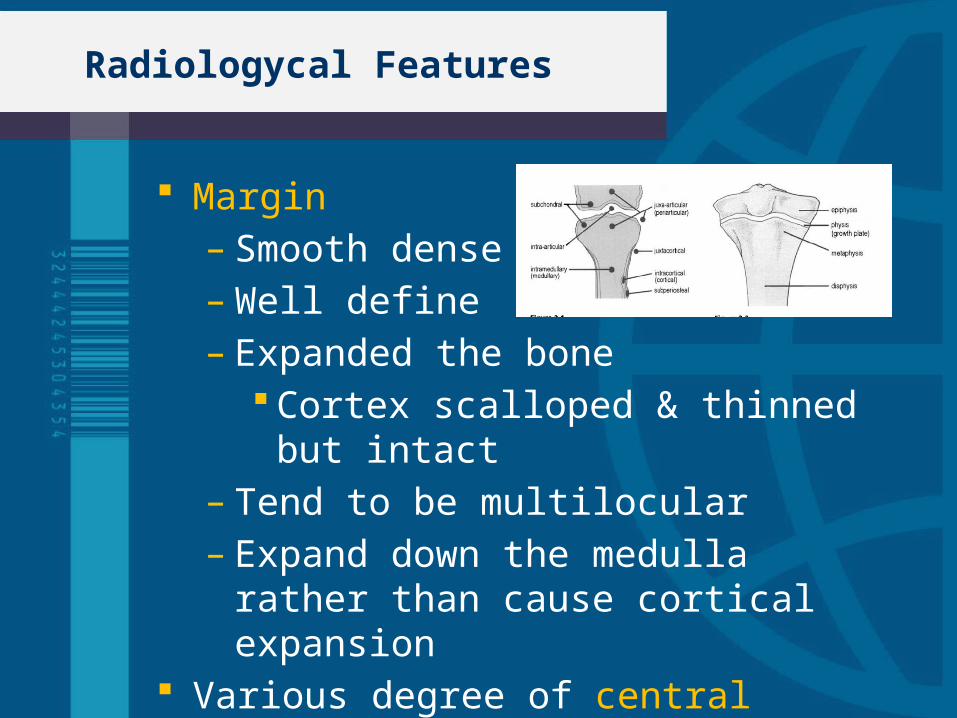
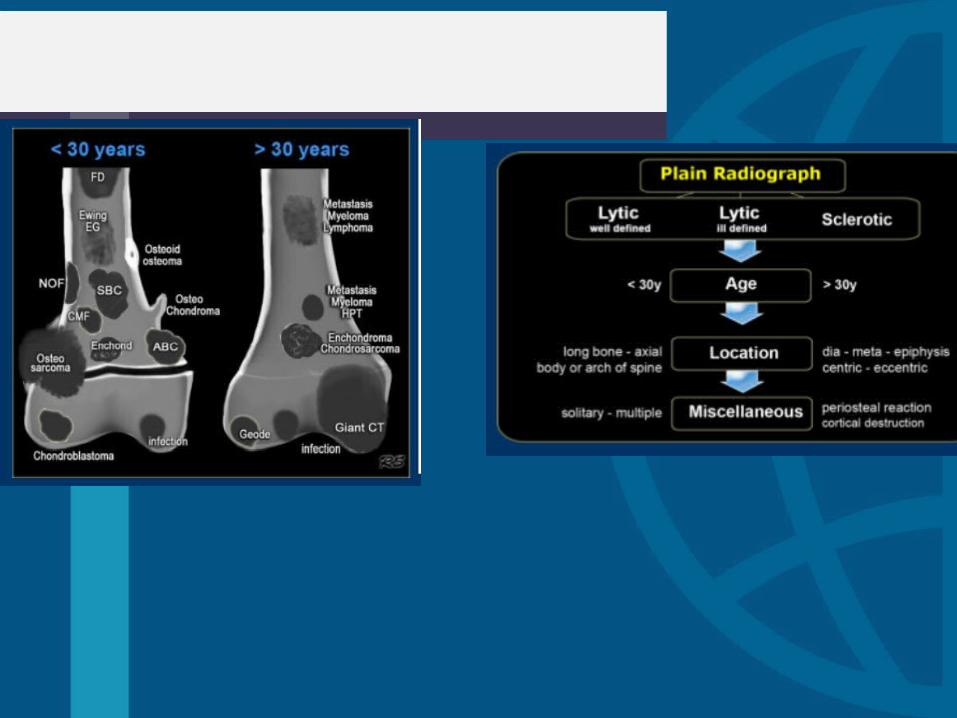
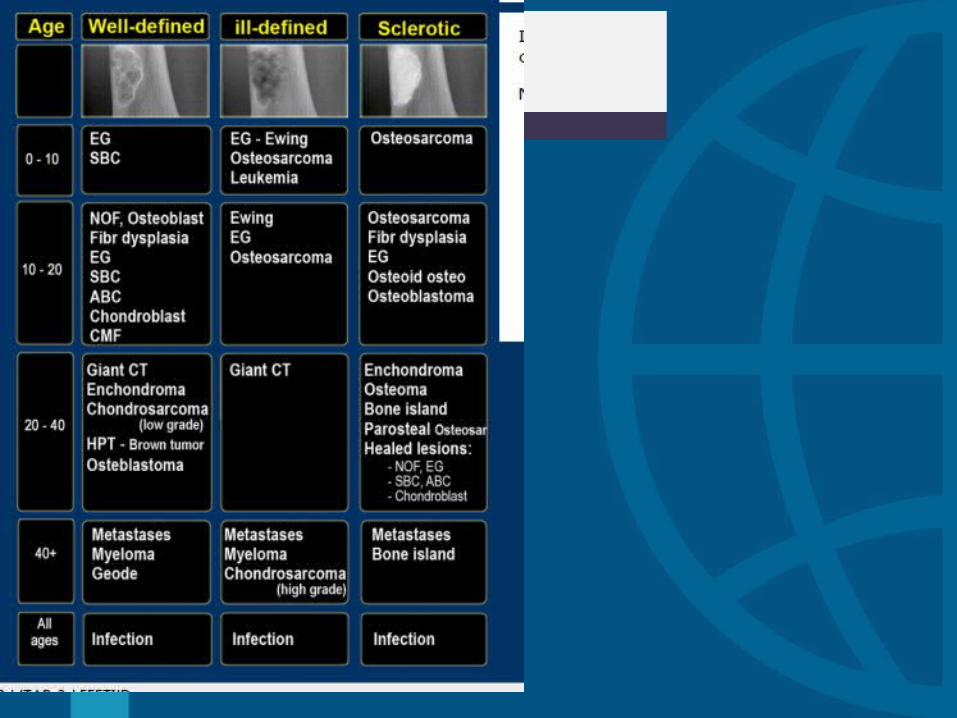
Radiologycal Features
Margin– Smooth dense– Well define– Expanded the bone
Cortex scalloped & thinned but intact– Tend to be multilocular– Expand down the medulla rather than
cause cortical expansion Various degree of central ossification
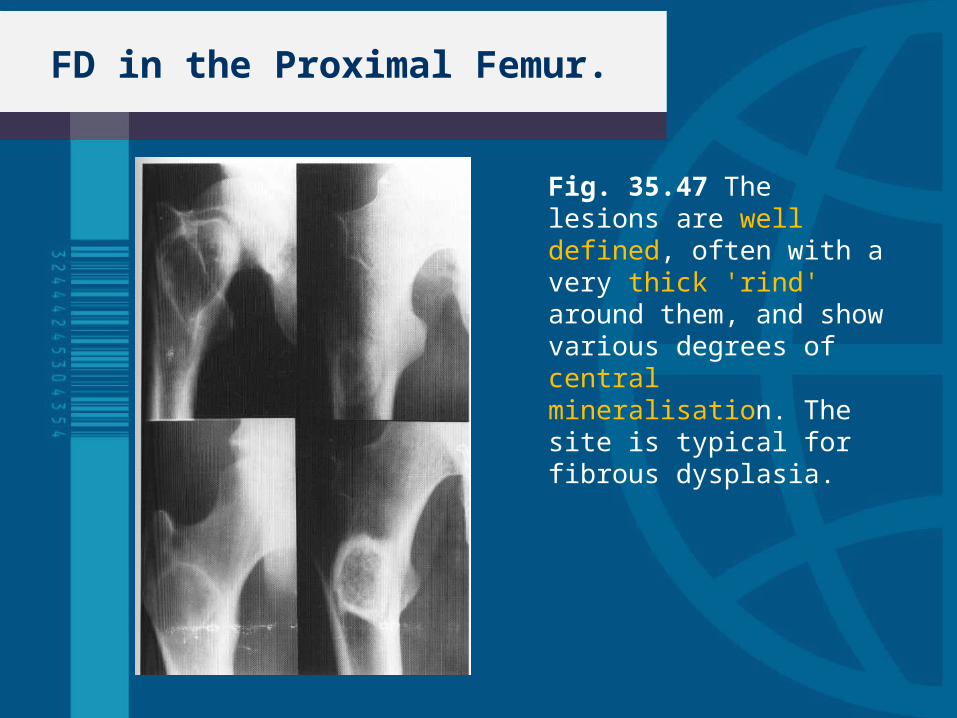
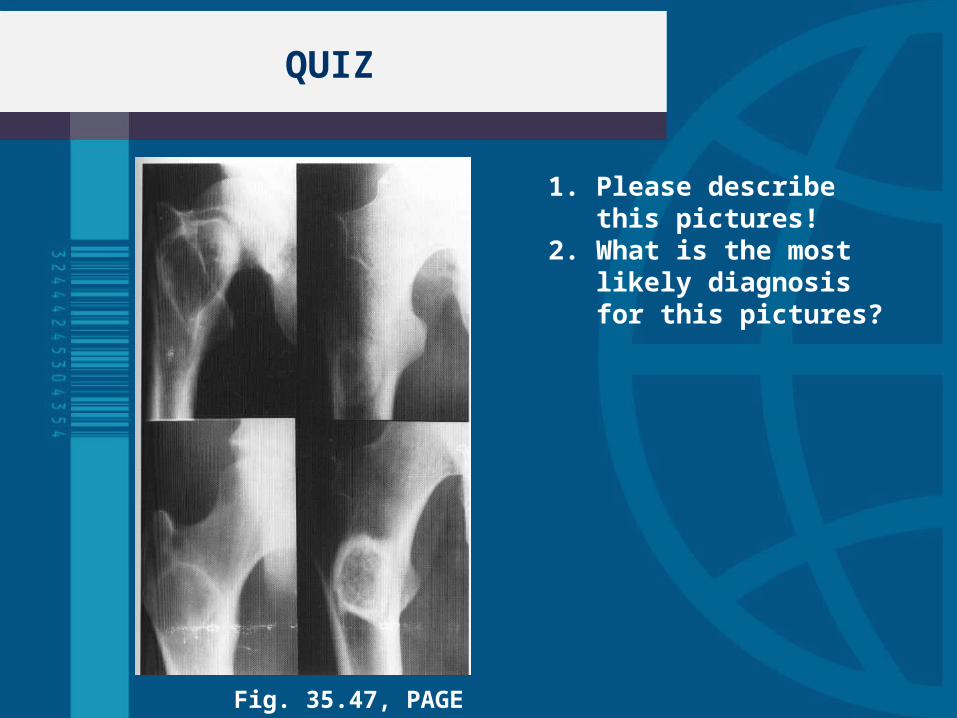
FD in the Proximal Femur.
Fig. 35.47 The lesions are well defined, often with a very thick 'rind' around them, and show various degrees of central mineralisation. The site is typical for fibrous dysplasia.
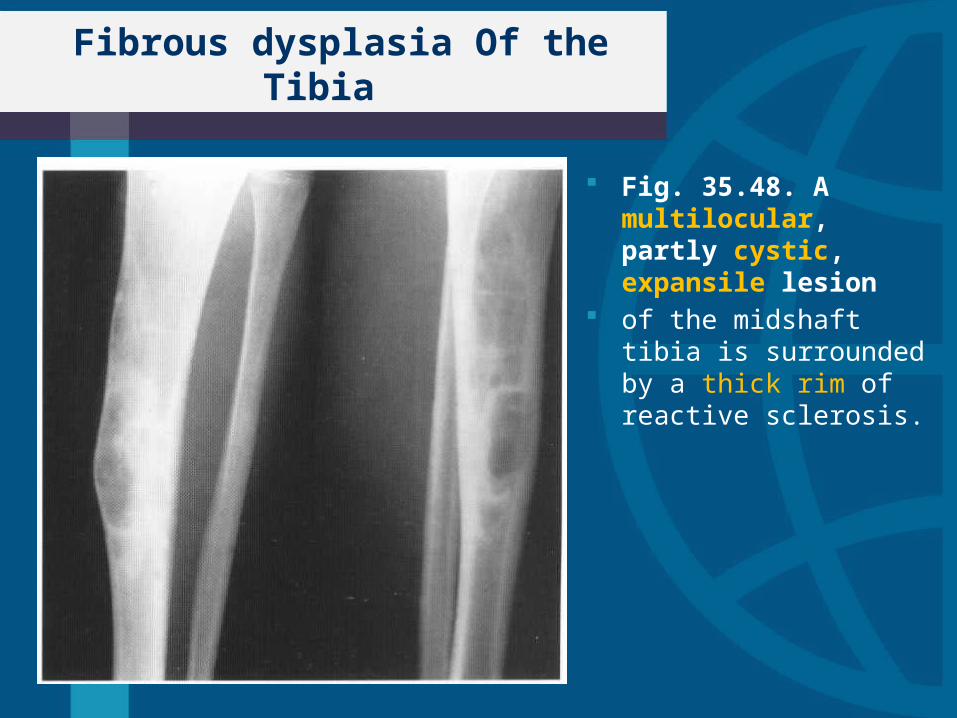
Fibrous dysplasia Of the Tibia
Fig. 35.48. A multilocular, partly cystic, expansile lesion
of the midshaft tibia is surrounded by a thick rim of reactive sclerosis.
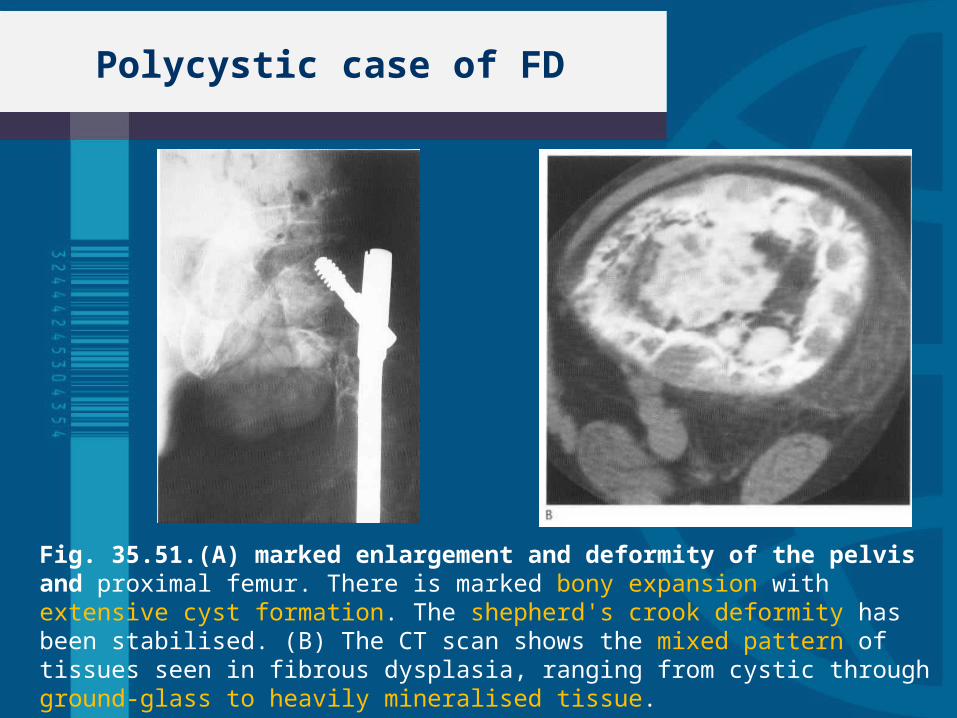
Polycystic case of FD
Fig. 35.51.(A) marked enlargement and deformity of the pelvis and proximal femur. There is marked bony expansion with extensive cyst formation. The shepherd's crook deformity has been stabilised. (B) The CT scan shows the mixed pattern of tissues seen in fibrous dysplasia, ranging from cystic through ground-glass to heavily mineralised tissue.
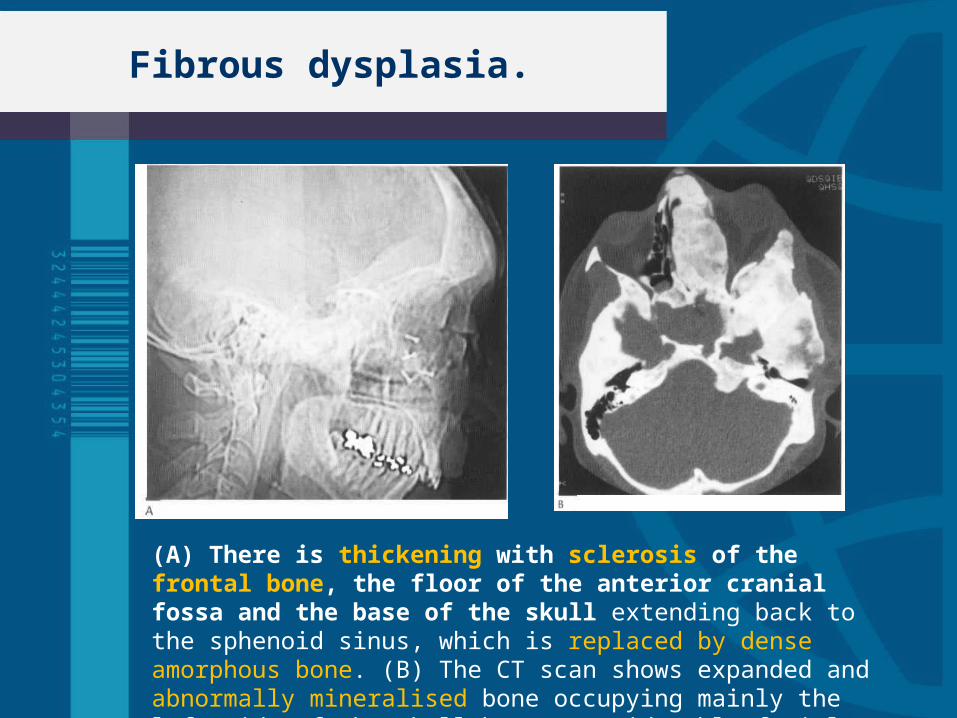
Fibrous dysplasia.
(A) There is thickening with sclerosis of the frontal bone, the floor of the anterior cranial fossa and the base of the skull extending back to the sphenoid sinus, which is replaced by dense amorphous bone. (B) The CT scan shows expanded and abnormally mineralised bone occupying mainly the left side of the skull base. Considerable facial deformity is present.
Resume
Fibrous dysplasia
1. Aetiology & Patology
2. Form– Polyostotic– Monostotic
3. Radialogical feature– Location : diametafisial, medulla– Margin
Well define, expansion to the cortex (cortex thin, scalloped, but intact)
– Center Varying degree central mineral ossification
QUIZ
1. Please describe this pictures!
2. What is the most likely diagnosis for this pictures?
Fig. 35.47, PAGE 1131

TERIMAKASIH