Embed Size (px)
Citation preview
4 Ahn J, Yu K, Stolzenberg-Solomon R, et al. Genome-wide association study ofcirculating vitamin D levels. Hum Mol Genet 2010;19:2739–45.
5 Wang TJ, Zhang F, Richards JB, et al. Common genetic determinants of vitamin Dinsufficiency: a genome-wide association study. Lancet 2010;376:180–8.
6 Cooper JD, Smyth DJ, Walker NM, et al. Inherited variation in vitamin D genes isassociated with predisposition to autoimmune disease type 1 diabetes. Diabetes2011;60:1624–31.
7 Hingorani A, Humphries S. Nature’s randomised trials. Lancet 2003;366:1906–8.
8 Plant D, Ibrahim I, Lunt M, et al. Correlation of C-reactive protein haplotypes withserum C-reactive protein level and response to anti-tumor necrosis factor therapy inUK rheumatoid arthritis patients: results from the Biologics in Rheumatoid ArthritisGenetics and Genomics Study Syndicate cohort. Arthritis Res Ther 2012;14:R214.
9 Prevoo ML, van ’t Hof MA, Kuper HH, et al. Modified disease activity scores thatinclude twenty-eight-joint counts. Development and validation in a prospectivelongitudinal study of patients with rheumatoid arthritis. Arthritis Rheum1995;38:44–8.
10 van Gestel AM, Prevoo ML, van ’t Hof MA, et al. Development and validation ofthe European League Against Rheumatism response criteria for rheumatoid arthritis.Comparison with the preliminary American College of Rheumatology and the WorldHealth Organization/International League Against Rheumatism Criteria. ArthritisRheum 1996;39:34–40.
Fibrosis biomarkers in isolated Raynaud’sphenomenon: too little, too soon?
Raynaud’s phenomenon (RP) can be the first manifestation ormay be present before the development of an overt systemicsclerosis (SSc).1
Enhanced liver fibrosis (ELF) test, an algorithm combining tissueinhibitors of matrix metalloproteinases (TIMP-1), hyaluronic acid(HA) and aminoterminal propeptide of type III procollagen (PIIINP),has been related to several measures of fibrosis in SSc patients.2–4
We evaluated whether these biomarkers could discriminatebetween primary and secondary RP.
Consecutive adult patients with RP at the first rheumatologicevaluation were recruited from February 2011 to May 2012with ethics committee approval. Exclusion criteria were historyof any fibrosing disorder, organ transplantation, hepatocellularcarcinoma or treatment with interferon. One patient wasexcluded for interferon treatment. Fifteen limited cutaneous SScand 15 diffuse cutaneous (dc) SSc were studied.5 All patientsprovided a written informed consent.
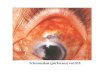
All subjects underwent clinical evaluation and capillaroscopy.6
Sera were tested for anti-nuclear antibodies (ANA) on HEp2cells; anti-dsDNA by ELISA; anti-extractable nuclear antigens
(anti-ENA) by ELISA (Phadia, Freiburg, Germany) and DotBlot(EUROIMMUN AG Luebeck, Germany). ELF score was deter-mined blindly (iQur Limited, London, UK).7
Patients were classified as primary RP (pRP),8 RP secondaryto suspected SSc (ie, capillaroscopy or ANA positive with orwithout anti-ENA positivity and without any symptoms suggest-ive for SSc) and very early SSc.9
Demographic features of the 109 enrolled subjects are shownin table 1. Our cohort of patients is consistent with publishedseries10 showing a higher female prevalence, similar percentageof ANA and anti-ENA positivities and abnormal capillaroscopy.
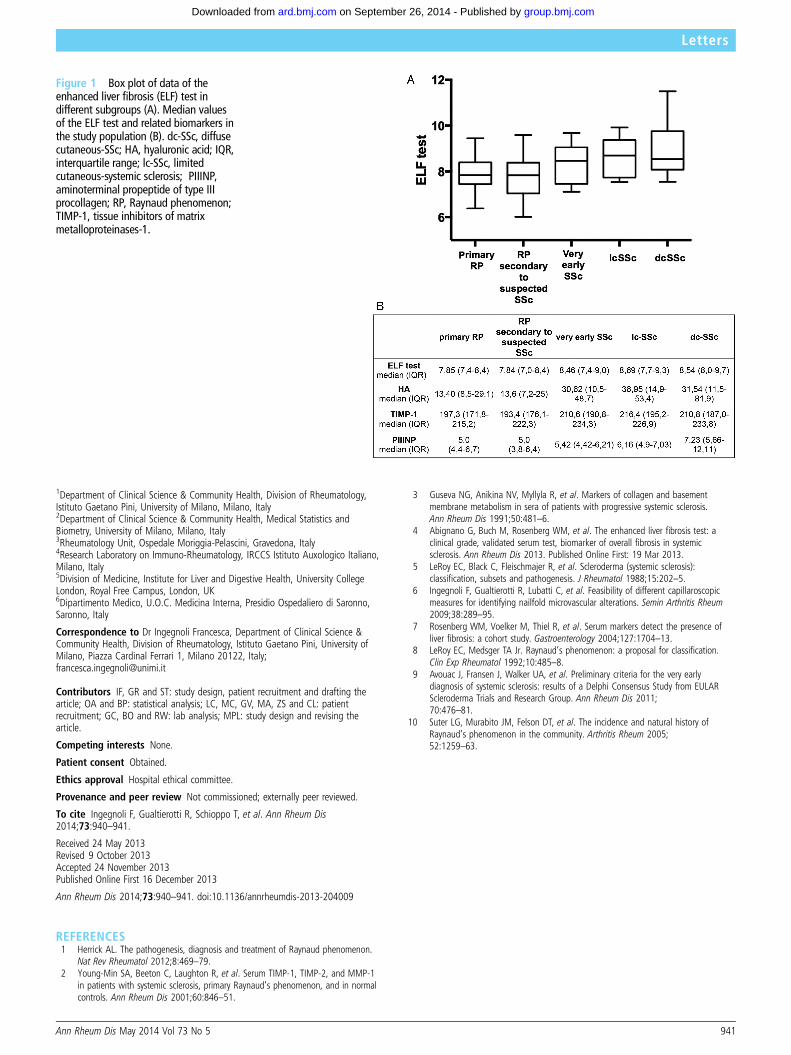
A significant increasing trend was observed with one-way ana-lysis of variance (ANOVA) in rank transformation from pRP todcSSc for ELF test, HA and PIIINP (p<0.001, p<0.001 andp=0.0036, respectively) (figure 1). These data associated withthe lack of correlation with capillaroscopic microvascular abnor-malities are in agreement with a recent study4 suggesting thepotential role of ELF test as a fibrosis index in overt SSc.
The ELF test, HA and TIMP-1 displayed a significant increasein relation to age (p<0.0001, p<0.0001 and p=0.001, respect-ively). For this reason, non-parametric regression models onranks were used to adjust for age and the results were confirmedonly for ELF test and PIIINP. None of these biomarkers wasrelated with RP duration.
Among multiple post hoc pairwise comparisons (Bonferronimethod), RP secondary to suspected SSc showed significant dif-ference for the ELF test and HA versus very early SSc (p=0.014for both comparisons), although not confirmed after adjustingfor age. Therefore, age should be considered in designing a spe-cific algorithm for SSc.
The ELF test receiver operating characteristic (ROC) curveshowed a poor discriminating ability between pRP versus very earlySSc area under the curve (AUC)=0.641, 95% CI 0.466 to 0.815.
We report for the first time that the ELF is not able to discrim-inate between primary and secondary RP. It is useful to speculatethat the fibrotic process is not clearly detectable in very earlystages of SSc when likely the ongoing vasculopathy is playing amajor role and precedes fibrosis development.
Francesca Ingegnoli,1 Roberta Gualtierotti,1 Tommaso Schioppo,1
Annalisa Orenti,2 Patrizia Boracchi,2 Chiara Lubatti,1 Claudio Mastaglio,3
Valentina Galbiati,3 Antonella Murgo,1 Silvana Zeni,1 Claudia Grossi,4
Orietta Borghi,4 William Rosenberg,5 Laura Castelnovo,6
Luigi Meroni Pier1,4
Table 1 Characteristics of the study cohort
Primary RP (No. 50)RP secondaryto suspected SSc (No. 43) Very early SSc (No. 16) lcSSc (No. 15) dcSSc (No. 15)
Female No. (%) 47 (94%) 40 (93%) 12 (75%) 14 (93.3%) 13 (86.7%)Age median (IQR) years 44.5 (28.7–56.2) 43 (30–53) 57.5 (43.7–69.7) 67 (60–74) 65 (40–74)RP duration median (IQR) months 60 (22.5–120) 36 (12–120) 36 (17.2–112.3) 120 (48–252) 48 (24–60)ANA positivityNo. (%)
0 (0%) 30 (69.8%) 16 (100%) 15 (100%) 15 (100%)
Anti-ENA positivityNo. (%)Antigen
0 (0%) 11 (25.6%)▸ 6 CENP A▸ 4 CENP B▸ 3 Ro52▸ 1 PM100▸ 1 PM75▸ 1 NOR90▸ 1 KU
14 (87.5%)▸ 8 CENP A▸ 8 CENP B▸ 3 Scl70▸ 5 Ro52▸ 1 PM100▸ 1 Th/To
3 (20%)▸ 3 CENP A▸ 3 CENP B▸ 2 Ro52▸ 1 SS-B▸ 1 PM75
12 (80%)▸ 11 Scl70▸ 4 Ro52▸ 1 SS-B
Capillaroscopy abnormalNo. (%)
0 (0%) 12 (27.9%) 16 (100%) 15 (100%) 15 (100%)
ANA, anti-nuclear antibodies; anti-ENA, anti-extractable nuclear antigen; CENP, centromere protein; dcSSc, diffuse cutaneous systemic sclerosis; IQR, interquartile range; lcSSc, limitedcutaneous systemic sclerosis; RP, Raynaud’s phenomenon; SS, Sjögren’s syndrome.
940 Ann Rheum Dis May 2014 Vol 73 No 5
Letters
group.bmj.com on September 26, 2014 - Published by ard.bmj.comDownloaded from
1Department of Clinical Science & Community Health, Division of Rheumatology,Istituto Gaetano Pini, University of Milano, Milano, Italy2Department of Clinical Science & Community Health, Medical Statistics andBiometry, University of Milano, Milano, Italy3Rheumatology Unit, Ospedale Moriggia-Pelascini, Gravedona, Italy4Research Laboratory on Immuno-Rheumatology, IRCCS Istituto Auxologico Italiano,Milano, Italy5Division of Medicine, Institute for Liver and Digestive Health, University CollegeLondon, Royal Free Campus, London, UK6Dipartimento Medico, U.O.C. Medicina Interna, Presidio Ospedaliero di Saronno,Saronno, Italy
Correspondence to Dr Ingegnoli Francesca, Department of Clinical Science &Community Health, Division of Rheumatology, Istituto Gaetano Pini, University ofMilano, Piazza Cardinal Ferrari 1, Milano 20122, Italy;[email protected]
Contributors IF, GR and ST: study design, patient recruitment and drafting thearticle; OA and BP: statistical analysis; LC, MC, GV, MA, ZS and CL: patientrecruitment; GC, BO and RW: lab analysis; MPL: study design and revising thearticle.
Competing interests None.
Patient consent Obtained.
Ethics approval Hospital ethical committee.
Provenance and peer review Not commissioned; externally peer reviewed.
To cite Ingegnoli F, Gualtierotti R, Schioppo T, et al. Ann Rheum Dis2014;73:940–941.
Received 24 May 2013Revised 9 October 2013Accepted 24 November 2013Published Online First 16 December 2013
Ann Rheum Dis 2014;73:940–941. doi:10.1136/annrheumdis-2013-204009
REFERENCES1 Herrick AL. The pathogenesis, diagnosis and treatment of Raynaud phenomenon.
Nat Rev Rheumatol 2012;8:469–79.2 Young-Min SA, Beeton C, Laughton R, et al. Serum TIMP-1, TIMP-2, and MMP-1
in patients with systemic sclerosis, primary Raynaud’s phenomenon, and in normalcontrols. Ann Rheum Dis 2001;60:846–51.
3 Guseva NG, Anikina NV, Myllyla R, et al. Markers of collagen and basementmembrane metabolism in sera of patients with progressive systemic sclerosis.Ann Rheum Dis 1991;50:481–6.
4 Abignano G, Buch M, Rosenberg WM, et al. The enhanced liver fibrosis test: aclinical grade, validated serum test, biomarker of overall fibrosis in systemicsclerosis. Ann Rheum Dis 2013. Published Online First: 19 Mar 2013.
5 LeRoy EC, Black C, Fleischmajer R, et al. Scleroderma (systemic sclerosis):classification, subsets and pathogenesis. J Rheumatol 1988;15:202–5.
6 Ingegnoli F, Gualtierotti R, Lubatti C, et al. Feasibility of different capillaroscopicmeasures for identifying nailfold microvascular alterations. Semin Arthritis Rheum2009;38:289–95.
7 Rosenberg WM, Voelker M, Thiel R, et al. Serum markers detect the presence ofliver fibrosis: a cohort study. Gastroenterology 2004;127:1704–13.
8 LeRoy EC, Medsger TA Jr. Raynaud’s phenomenon: a proposal for classification.Clin Exp Rheumatol 1992;10:485–8.
9 Avouac J, Fransen J, Walker UA, et al. Preliminary criteria for the very earlydiagnosis of systemic sclerosis: results of a Delphi Consensus Study from EULARScleroderma Trials and Research Group. Ann Rheum Dis 2011;70:476–81.
10 Suter LG, Murabito JM, Felson DT, et al. The incidence and natural history ofRaynaud’s phenomenon in the community. Arthritis Rheum 2005;52:1259–63.
Antitumour necrosis factor α treatmentreduces retinol-binding protein 4 serum levelsin non-diabetic ankylosing spondylitis patients
Increased cardiovascular (CV) mortality due to accelerated ath-erosclerosis occurs in ankylosing spondylitis (AS) patients.1 2
Beneficial effects of antitumour necrosis factor (anti-TNF)-αagents on disease activity and endothelial cell activation werereported in AS.3 4 Dramatic reduction of insulin resistance (IR)and improvement of insulin sensitivity after infliximab adminis-tration were also described in non-diabetic AS patients.5
We aimed to assess, for the first time, whether infliximabadministration in AS patients may alter levels of retinol-bindingprotein 4 (RBP-4), a protein released from adipocytes,
Figure 1 Box plot of data of theenhanced liver fibrosis (ELF) test indifferent subgroups (A). Median valuesof the ELF test and related biomarkers inthe study population (B). dc-SSc, diffusecutaneous-SSc; HA, hyaluronic acid; IQR,interquartile range; lc-SSc, limitedcutaneous-systemic sclerosis; PIIINP,aminoterminal propeptide of type IIIprocollagen; RP, Raynaud phenomenon;TIMP-1, tissue inhibitors of matrixmetalloproteinases-1.
Ann Rheum Dis May 2014 Vol 73 No 5 941
Letters
group.bmj.com on September 26, 2014 - Published by ard.bmj.comDownloaded from
doi: 10.1136/annrheumdis-2013-20400916, 2013
2014 73: 940-941 originally published online DecemberAnn Rheum Dis Francesca Ingegnoli, Roberta Gualtierotti, Tommaso Schioppo, et al. phenomenon: too little, too soon?Fibrosis biomarkers in isolated Raynaud's
http://ard.bmj.com/content/73/5/940.full.htmlUpdated information and services can be found at:
These include:
References http://ard.bmj.com/content/73/5/940.full.html#ref-list-1
This article cites 9 articles, 3 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on September 26, 2014 - Published by ard.bmj.comDownloaded from


![Occupational Injuries and Illnesses - LexisNexis[b] Secondary Raynaud's Phenomenon. The term secondary Raynaud's phenomenon is used to refer to the digital vasospasm (blood vessel](https://img.pdfslide.us/doc/110x75/5f069f7e7e708231d418e9a1/occupational-injuries-and-illnesses-b-secondary-raynauds-phenomenon-the-term.jpg)