Embed Size (px)
Citation preview
Fibrinolysis or Primary PCI: Fibrinolysis or Primary PCI:
Does “One Size Fits All” for AcuteDoes “One Size Fits All” for Acute
Myocardial Infarction Patients?Myocardial Infarction Patients?
Luiz Alberto MattosLuiz Alberto MattosInstituto Dante Pazzanese de CardiologiaInstituto Dante Pazzanese de Cardiologia
Sao Paulo, Brazil Sao Paulo, Brazil
Fibrinolysis or Primary PCI: Fibrinolysis or Primary PCI:
Does “One Size Fits All” for AcuteDoes “One Size Fits All” for Acute
Myocardial Infarction Patients?Myocardial Infarction Patients?
Luiz Alberto MattosLuiz Alberto MattosInstituto Dante Pazzanese de CardiologiaInstituto Dante Pazzanese de Cardiologia
Sao Paulo, Brazil Sao Paulo, Brazil
Reperfusion for Acute Myocardial Reperfusion for Acute Myocardial InfarcInfarction tion
Primary PCI is the “Gold-Standard” TreatmentPrimary PCI is the “Gold-Standard” Treatment
Circulation, November 14 Th, 2006 Circulation, November 14 Th, 2006
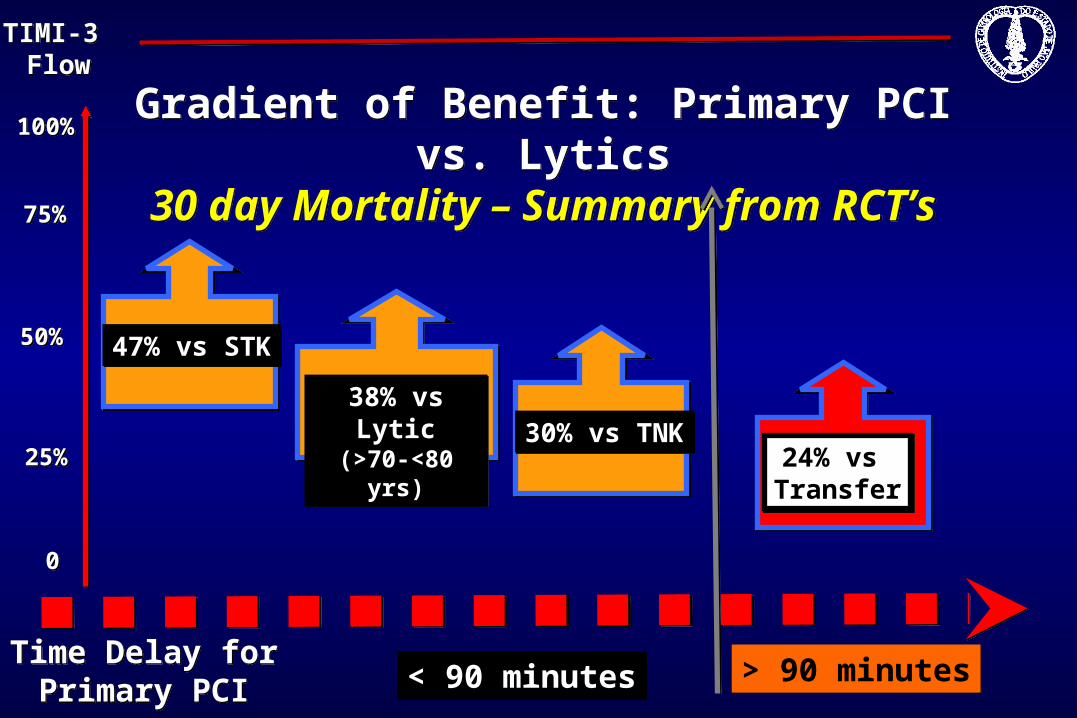
Time Delay forPrimary PCI
Time Delay forPrimary PCI < 90 minutes< 90 minutes > 90 minutes> 90 minutes
00
100%100%
50%50%
Gradient of Benefit: Primary PCI vs. Lytics
30 day Mortality – Summary from RCT’s
Gradient of Benefit: Primary PCI vs. Lytics
30 day Mortality – Summary from RCT’s
47% vs STK47% vs STK
24% vs Transfer24% vs Transfer
25%25%
75%75%
30% vs TNK30% vs TNK38% vs Lytic(>70-<80 yrs)
38% vs Lytic(>70-<80 yrs)
TIMI-3 Flow
TIMI-3 Flow
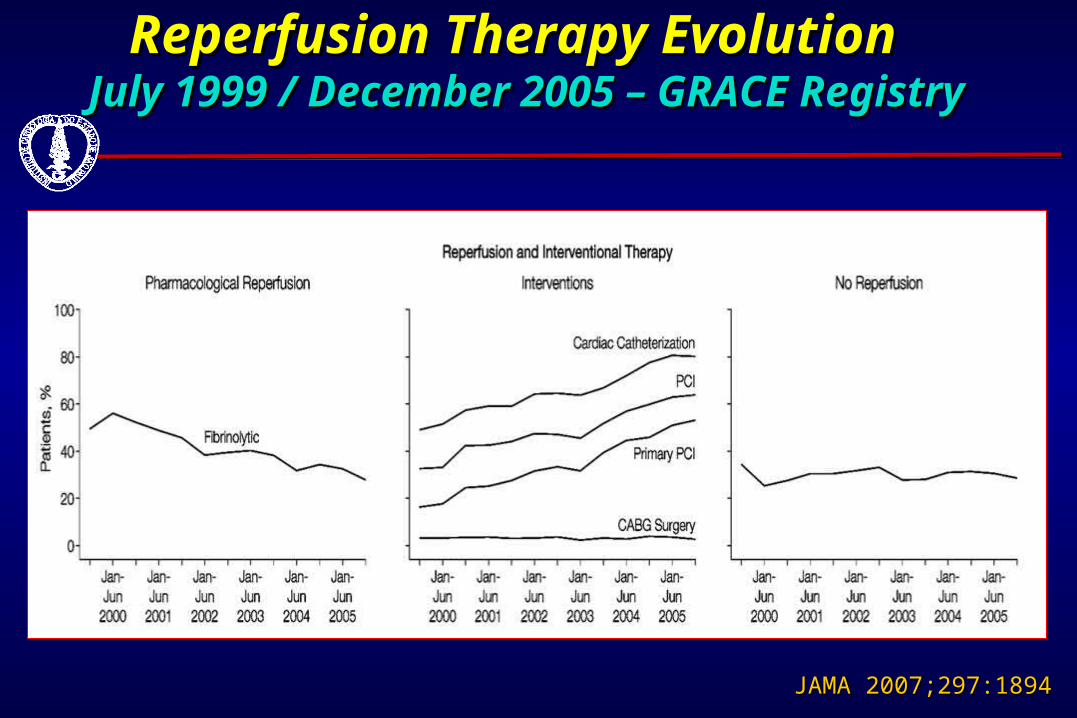
Reperfusion Therapy Evolution Reperfusion Therapy Evolution July 1999 / December 2005 – GRACE RegistryJuly 1999 / December 2005 – GRACE Registry
JAMA 2007;297:1894JAMA 2007;297:1894
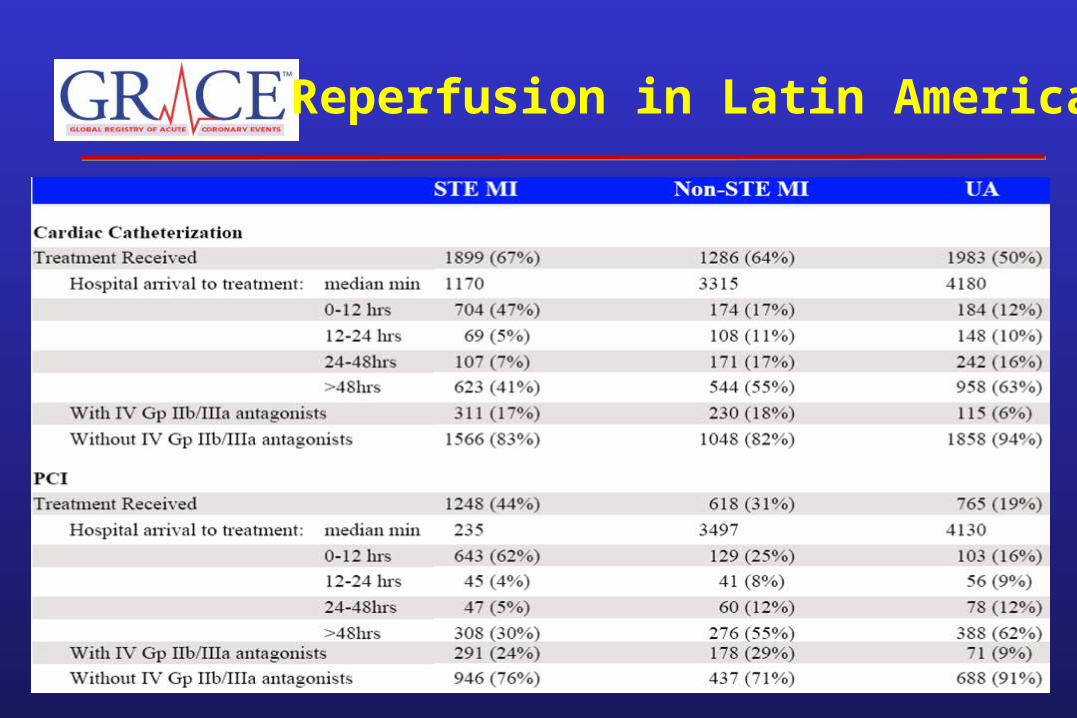
Reperfusion in Latin America
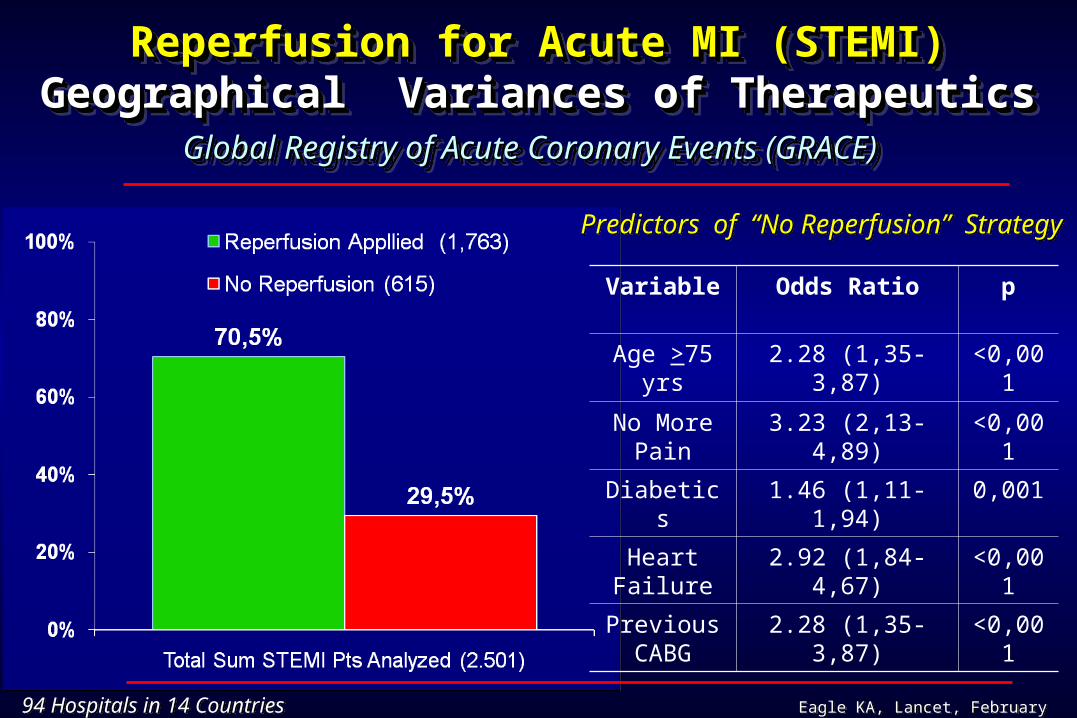
Reperfusion for Acute MI (STEMI)Reperfusion for Acute MI (STEMI)Geographical Variances of TherapeuticsGeographical Variances of Therapeutics Global Registry of Acute Coronary Events (GRACE) Global Registry of Acute Coronary Events (GRACE)
Reperfusion for Acute MI (STEMI)Reperfusion for Acute MI (STEMI)Geographical Variances of TherapeuticsGeographical Variances of Therapeutics Global Registry of Acute Coronary Events (GRACE) Global Registry of Acute Coronary Events (GRACE)
94 Hospitals in 14 Countries94 Hospitals in 14 Countries Eagle KA, Lancet, February 2, 2002Eagle KA, Lancet, February 2, 2002
Variable Odds Ratio p
Age >75 yrs 2.28 (1,35-3,87) <0,001
No More Pain
3.23 (2,13-4,89) <0,001
Diabetics 1.46 (1,11-1,94) 0,001
Heart Failure
2.92 (1,84-4,67) <0,001
Previous CABG
2.28 (1,35-3,87) <0,001
Predictors of “No Reperfusion” Strategy Predictors of “No Reperfusion” Strategy
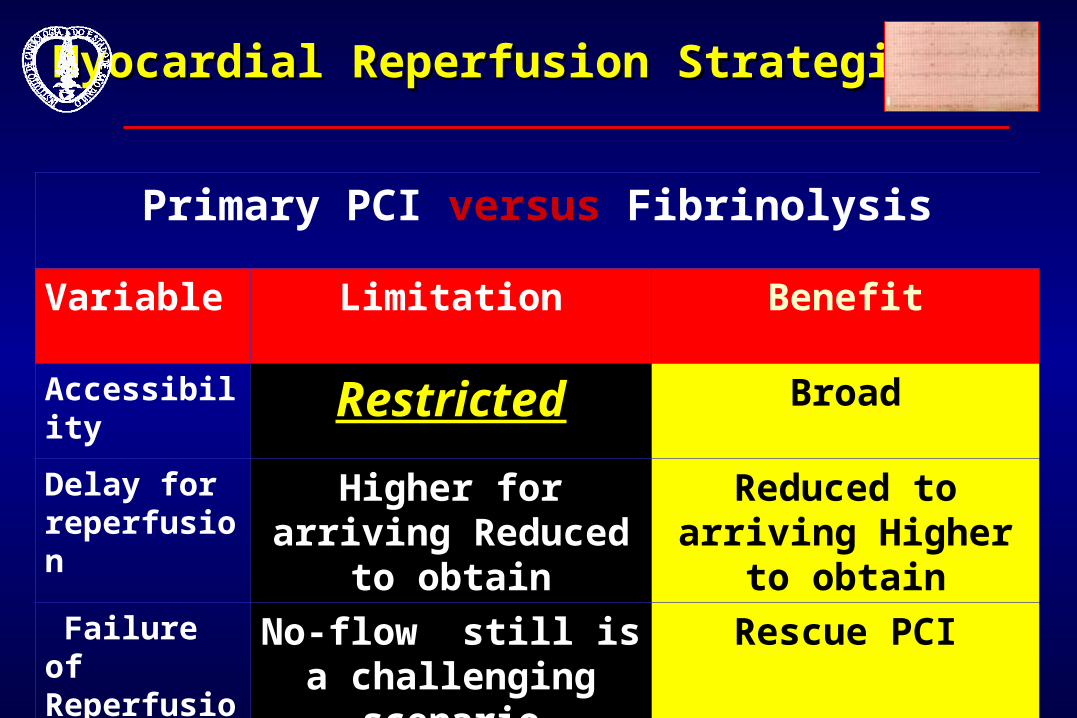
Myocardial Reperfusion StrategiesMyocardial Reperfusion Strategies
Primary PCI versus Fibrinolysis
Variable Limitation Benefit
Accessibility
Restricted Broad
Delay for reperfusion
Higher for arriving Reduced to obtain
Reduced to arriving Higher to obtain
Failure of Reperfusion
No-flow still is a challenging scenario
Rescue PCI
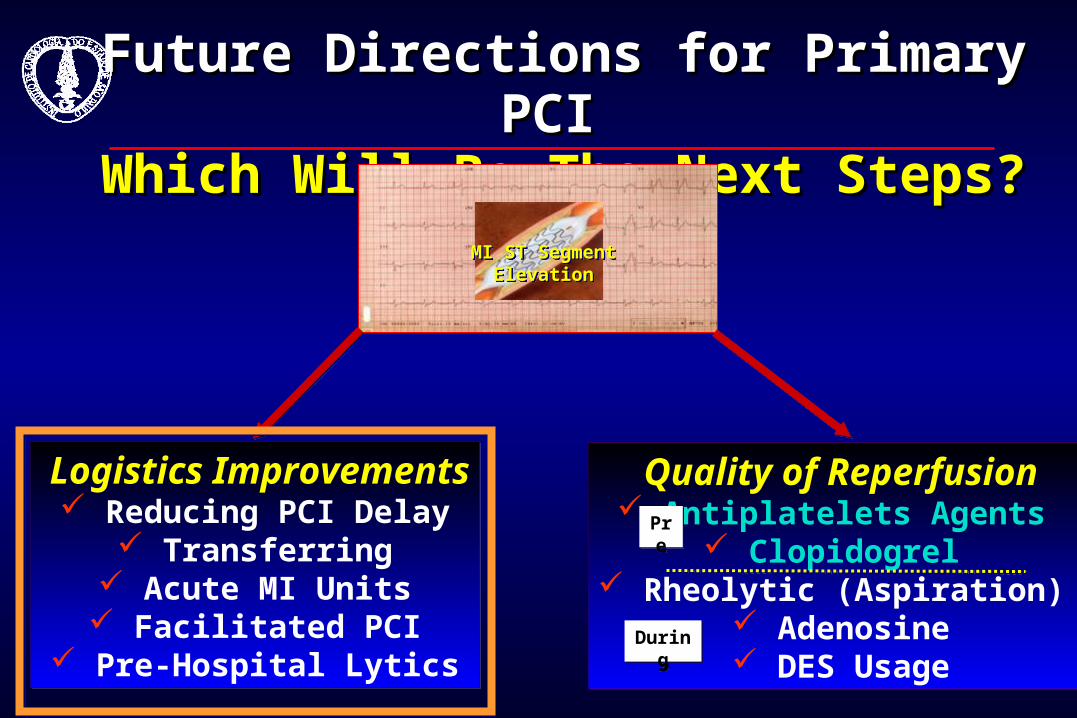
Future Directions for Primary PCIFuture Directions for Primary PCI Which Will Be The Next Steps?Which Will Be The Next Steps?
MI ST SegmentElevation
MI ST SegmentElevation
Logistics Improvements Reducing PCI Delay
Transferring Acute MI Units Facilitated PCI
Pre-Hospital Lytics
Logistics Improvements Reducing PCI Delay
Transferring Acute MI Units Facilitated PCI
Pre-Hospital Lytics
Quality of Reperfusion Antiplatelets Agents
Clopidogrel Rheolytic (Aspiration)
Adenosine DES Usage
Quality of Reperfusion Antiplatelets Agents
Clopidogrel Rheolytic (Aspiration)
Adenosine DES Usage
Pre
Pre
During
During
1.1. Optimizing Logistical Intake – MI Hubs Optimizing Logistical Intake – MI Hubs
Multidisciplinary Approach ProtocolsMultidisciplinary Approach Protocols
2.2. Speed Up Admittance and TransferSpeed Up Admittance and Transfer
Better Quality-of-Care ProcessBetter Quality-of-Care Process
3-Challenging Priorities for 3-Challenging Priorities for Primary Coronary InterventionPrimary Coronary Intervention
www.d2balliance.org
D2B Alliance is a vehicle to disseminate knowledge and
promote improvement

More than 1,000 hospitalsjoined the effort
Recommended Strategy* Baseline Follow-up
EM activation 52% 60%Single call 31% 37%Cath team < 30 min 81% 89%Prompt data feedback 61% 79%Activate from PH ECG 33% 41%D2B Team 64% 85%
* All differences are significant P< 0.001
The Use of Strategies Changedin D2B Alliance Hospitals
Harvard Medical School
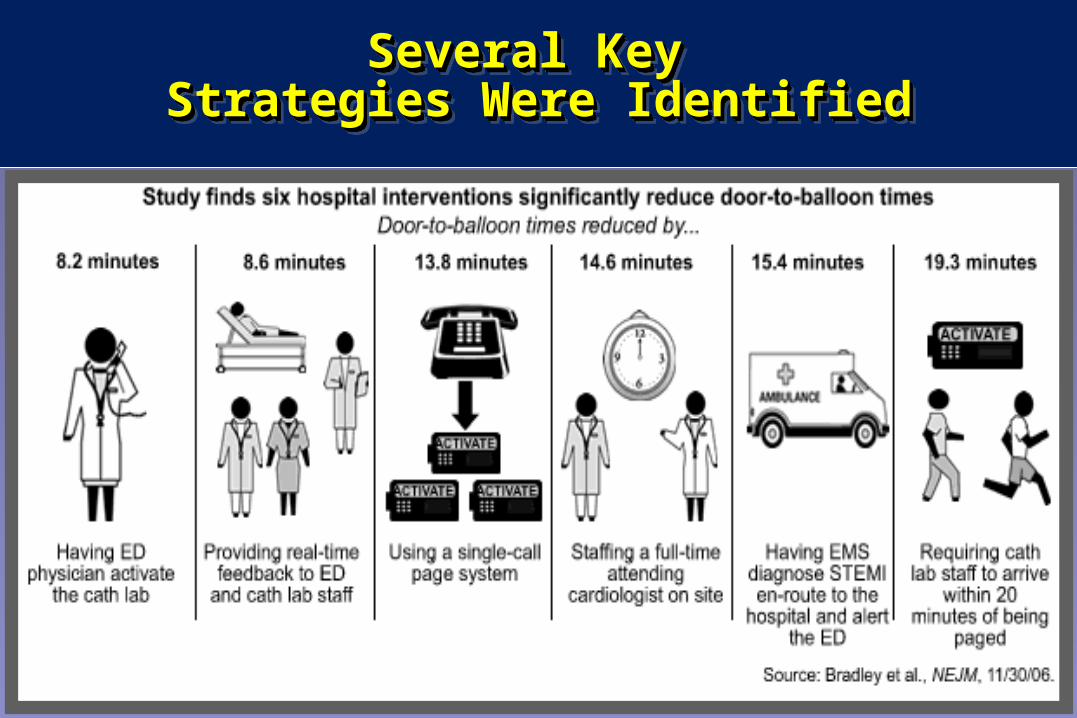
Several Key Several Key Strategies Were IdentifiedStrategies Were Identified
Several Key Several Key Strategies Were IdentifiedStrategies Were Identified
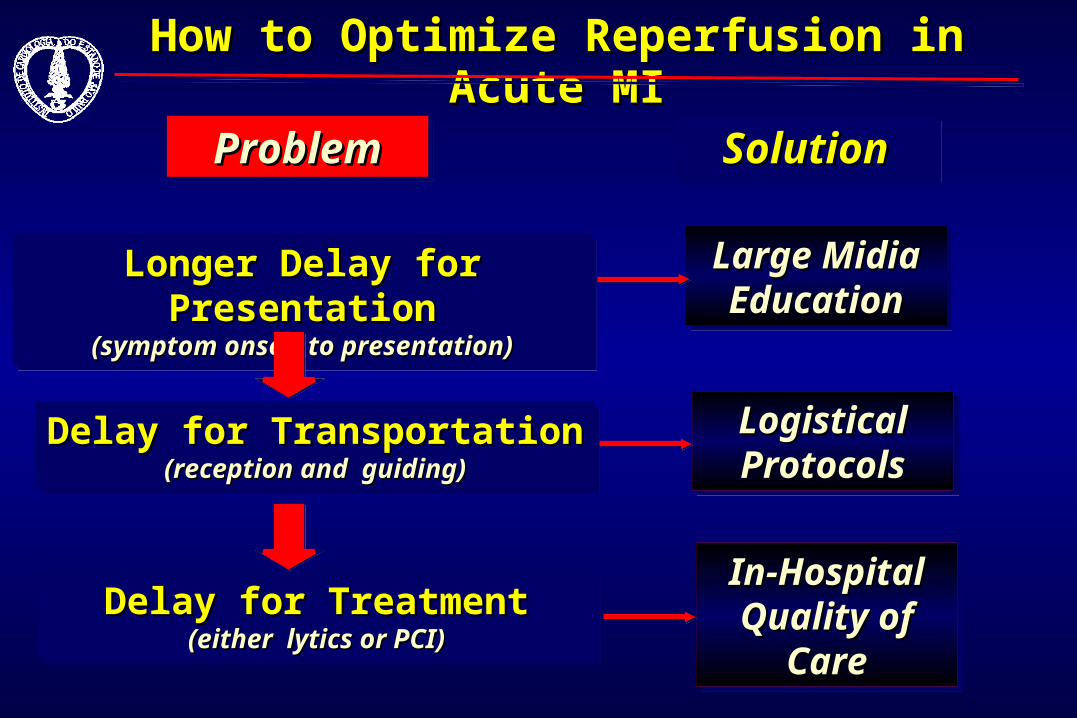
How to Optimize Reperfusion in Acute MIHow to Optimize Reperfusion in Acute MI
ProblemProblemProblemProblem SolutionSolutionSolutionSolution
Longer Delay for PresentationLonger Delay for Presentation(symptom onset to presentation)(symptom onset to presentation)
Longer Delay for PresentationLonger Delay for Presentation(symptom onset to presentation)(symptom onset to presentation)
Large Midia Large Midia EducationEducation
Large Midia Large Midia EducationEducation
Delay for TransportationDelay for Transportation(reception and guiding)(reception and guiding)
Delay for TransportationDelay for Transportation(reception and guiding)(reception and guiding)
Logistical Logistical ProtocolsProtocolsLogistical Logistical ProtocolsProtocols
Delay for TreatmentDelay for Treatment(either lytics or PCI)(either lytics or PCI)
Delay for TreatmentDelay for Treatment(either lytics or PCI)(either lytics or PCI)
In-Hospital In-Hospital Quality of Quality of
CareCare
In-Hospital In-Hospital Quality of Quality of
CareCare
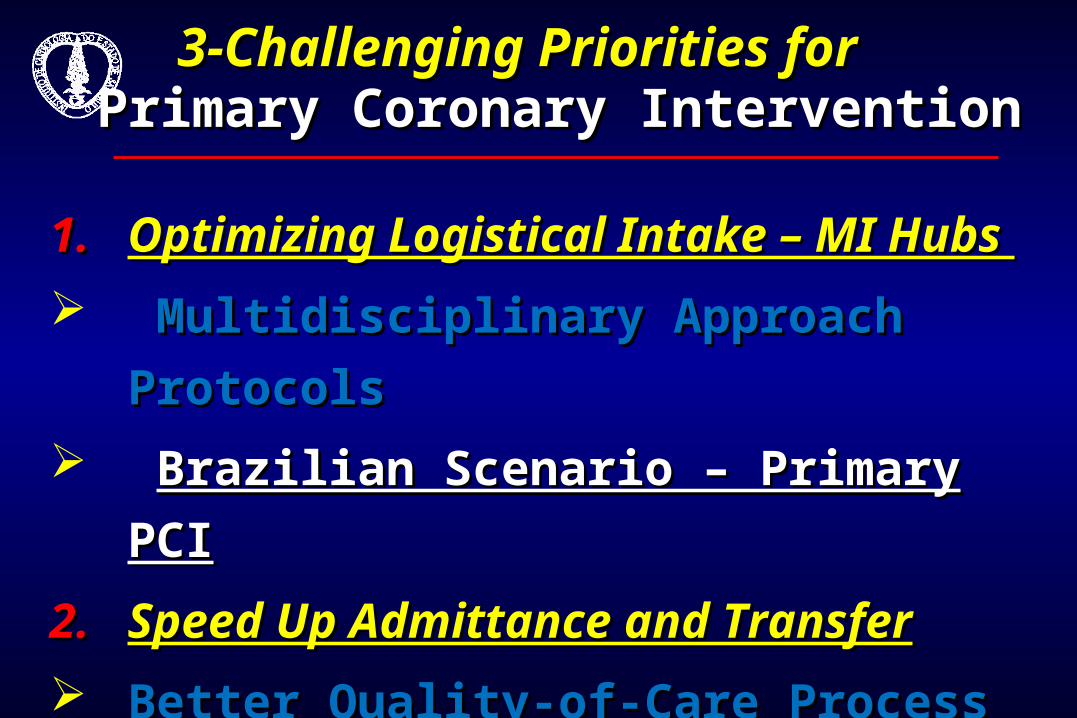
1.1. Optimizing Logistical Intake – MI Hubs Optimizing Logistical Intake – MI Hubs
Multidisciplinary Approach ProtocolsMultidisciplinary Approach Protocols
Brazilian Scenario – Primary PCIBrazilian Scenario – Primary PCI
2.2. Speed Up Admittance and TransferSpeed Up Admittance and Transfer
Better Quality-of-Care ProcessBetter Quality-of-Care Process
3-Challenging Priorities for 3-Challenging Priorities for Primary Coronary InterventionPrimary Coronary Intervention

1)1) 33 years in Brazil, from diagnostic 33 years in Brazil, from diagnostic
to interventional cardiology to interventional cardiology
(1975-2008) – (1975-2008) – www.sbhci.org.br
2)2) Gather nearly 1,000 interventional Gather nearly 1,000 interventional
cardiologists spread in 26 of 27 cardiologists spread in 26 of 27
federative statesfederative states
3)3) Strongly committed to board Strongly committed to board
certification, medical education and certification, medical education and
quality of care in clinical practicequality of care in clinical practice
4)4) Open elections each 2-year periodOpen elections each 2-year period
5)5) Annual Scientific Meeting since Annual Scientific Meeting since
1976, that receive up to 1,000 health 1976, that receive up to 1,000 health
professionals professionals
SBHCI – Brazilian Society SBHCI – Brazilian Society of Interventional Cardiologyof Interventional Cardiology
200 million people 70.000 PCI’s year =
0,3/1,000 <30% DES Usage
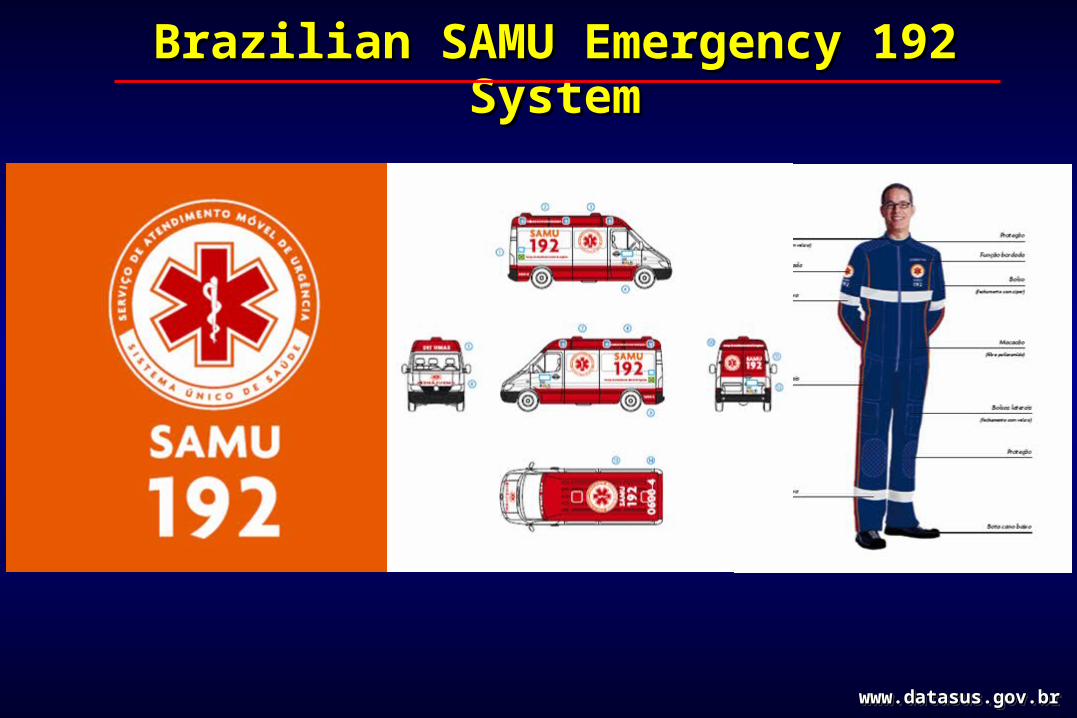
Brazilian SAMU Emergency 192 SystemBrazilian SAMU Emergency 192 System
www.datasus.gov.brwww.datasus.gov.brwww.datasus.gov.brwww.datasus.gov.br
SAMU (Serviço de Atendimento Móvel de Urgência) Reintrodução no SUS Brasileiro – Abril de 2004 Disque 192 – Atendimento em até 12 minutos
452 ambulâncias UTI já entregues Sistema de Gestão Pública Mista
146 cidades atendidas = >100 milhões de pessoas 32 centrais telefônicas com médicos 24 horas Investimento inicial de 297 milhões de reais
(150 milhões de dólares americanos)
SAMU (Serviço de Atendimento Móvel de Urgência) Reintrodução no SUS Brasileiro – Abril de 2004 Disque 192 – Atendimento em até 12 minutos
452 ambulâncias UTI já entregues Sistema de Gestão Pública Mista
146 cidades atendidas = >100 milhões de pessoas 32 centrais telefônicas com médicos 24 horas Investimento inicial de 297 milhões de reais
(150 milhões de dólares americanos)
Reperfusion for Acute MIReperfusion for Acute MIExpediting the Triage Process for the Treatment Expediting the Triage Process for the Treatment
1. EMS prompt activation of Invasive Cardiology Group
2. “Singe-call” activation of all professionals involved
3. Invasive Cardiology set-up in average of 30 minutes
4. Constant feed-back review of time to treatment and quality-of-care of the system
5. Central and Respected Managing
6. Multidisciplinary team effort
7. Pre hospital EKG analysis for speed up the process
1. EMS prompt activation of Invasive Cardiology Group
2. “Singe-call” activation of all professionals involved
3. Invasive Cardiology set-up in average of 30 minutes
4. Constant feed-back review of time to treatment and quality-of-care of the system
5. Central and Respected Managing
6. Multidisciplinary team effort
7. Pre hospital EKG analysis for speed up the process
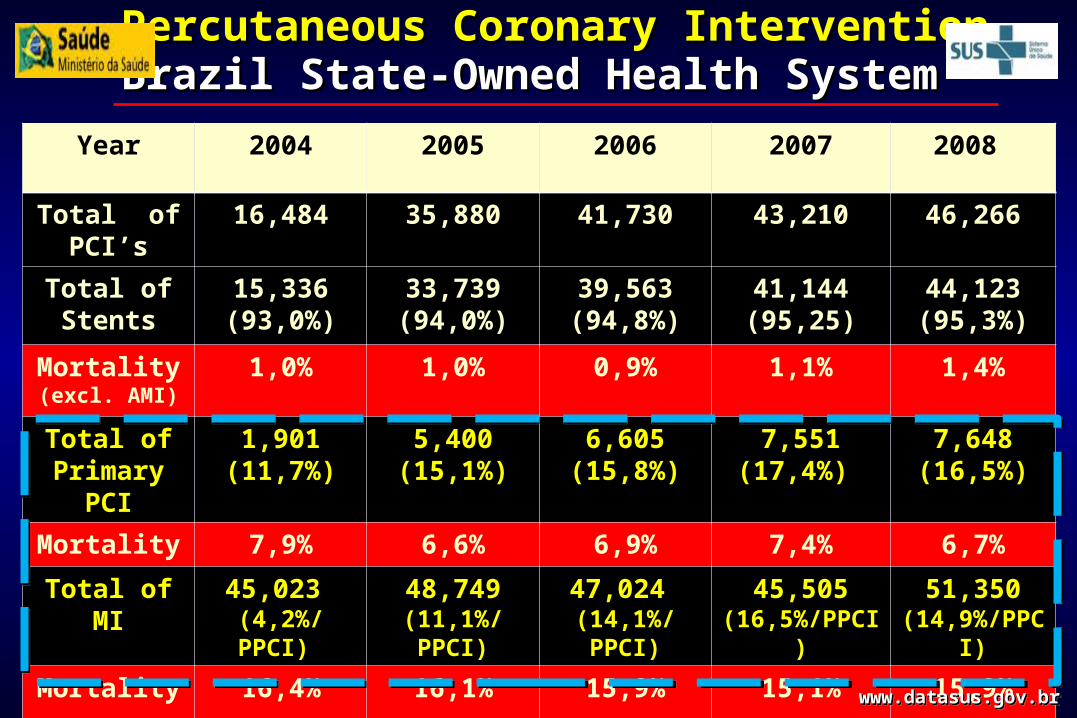
Percutaneous Coronary InterventionPercutaneous Coronary InterventionBrazil State-Owned Health System Brazil State-Owned Health System
Year 2004 2005 2006 2007 2008
Total of PCI’s
16,484 35,880 41,730 43,210 46,266
Total of Stents
15,336 (93,0%)
33,739 (94,0%)
39,563 (94,8%)
41,144 (95,25)
44,123 (95,3%)
Mortality (excl. AMI)
1,0% 1,0% 0,9% 1,1% 1,4%
Total of Primary PCI
1,901 (11,7%)
5,400 (15,1%)
6,605 (15,8%)
7,551 (17,4%)
7,648 (16,5%)
Mortality 7,9% 6,6% 6,9% 7,4% 6,7%
Total of MI 45,023 (4,2%/PPCI)
48,749(11,1%/ PPCI)
47,024 (14,1%/PPCI)
45,505 (16,5%/PPCI)
51,350 (14,9%/PPCI)
Mortality 16,4% 16,1% 15,9% 15,1% 15,9%
www.datasus.gov.brwww.datasus.gov.brwww.datasus.gov.brwww.datasus.gov.br
1.1. Optimizing Logistical Intake – MI Hubs Optimizing Logistical Intake – MI Hubs
Multidisciplinary Approach ProtocolsMultidisciplinary Approach Protocols
2.2. Speed Up Admittance and TransferSpeed Up Admittance and Transfer
Better Quality-of-Care ProcessBetter Quality-of-Care Process
3.3. Increase Operator ExpertiseIncrease Operator Expertise
Continuous Medical Education Continuous Medical Education
3-Challenging Priorities for 3-Challenging Priorities for Primary Coronary InterventionPrimary Coronary Intervention
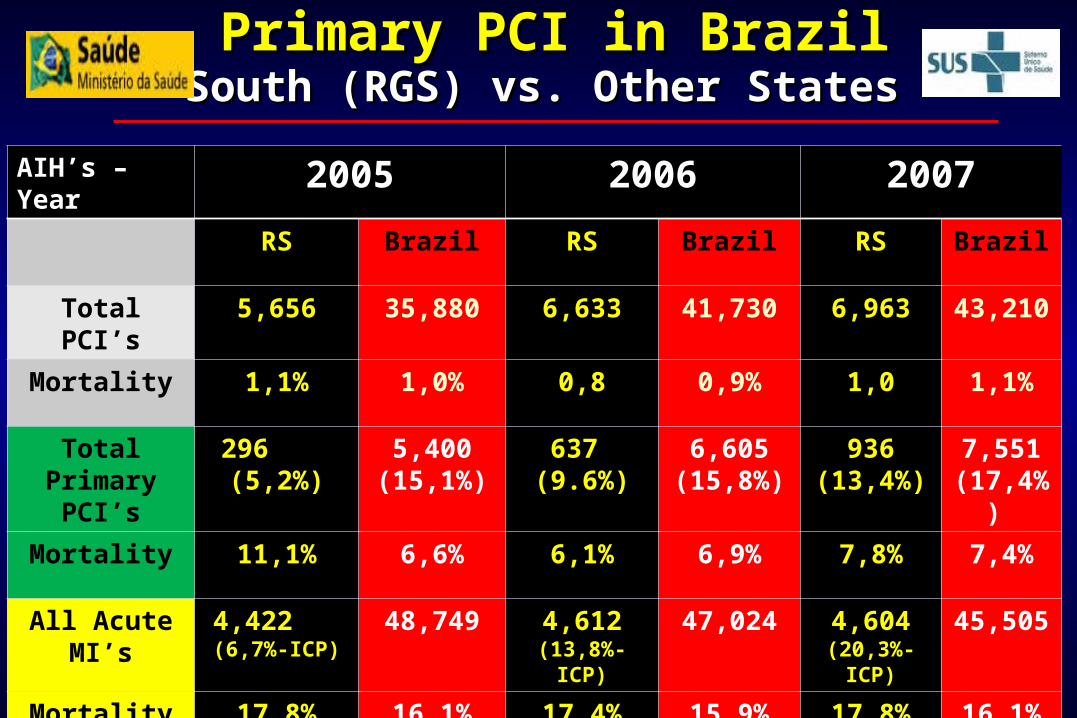
Primary PCI in BrazilPrimary PCI in BrazilSouth (RGS) vs. Other States South (RGS) vs. Other States
AIH’s – Year 2005 2006 2007RS Brazil RS Brazil RS Brazil
Total PCI’s 5,656 35,880 6,633 41,730 6,963 43,210
Mortality 1,1% 1,0% 0,8 0,9% 1,0 1,1%
Total Primary
PCI’s
296 (5,2%)
5,400 (15,1%)
637 (9.6%)
6,605 (15,8%)
936 (13,4%)
7,551 (17,4%)
Mortality 11,1% 6,6% 6,1% 6,9% 7,8% 7,4%
All Acute MI’s
4,422 (6,7%-ICP)
48,749 4,612 (13,8%-ICP)
47,024 4,604 (20,3%-ICP)
45,505
Mortality 17,8% 16,1% 17,4% 15,9% 17,8% 16,1%
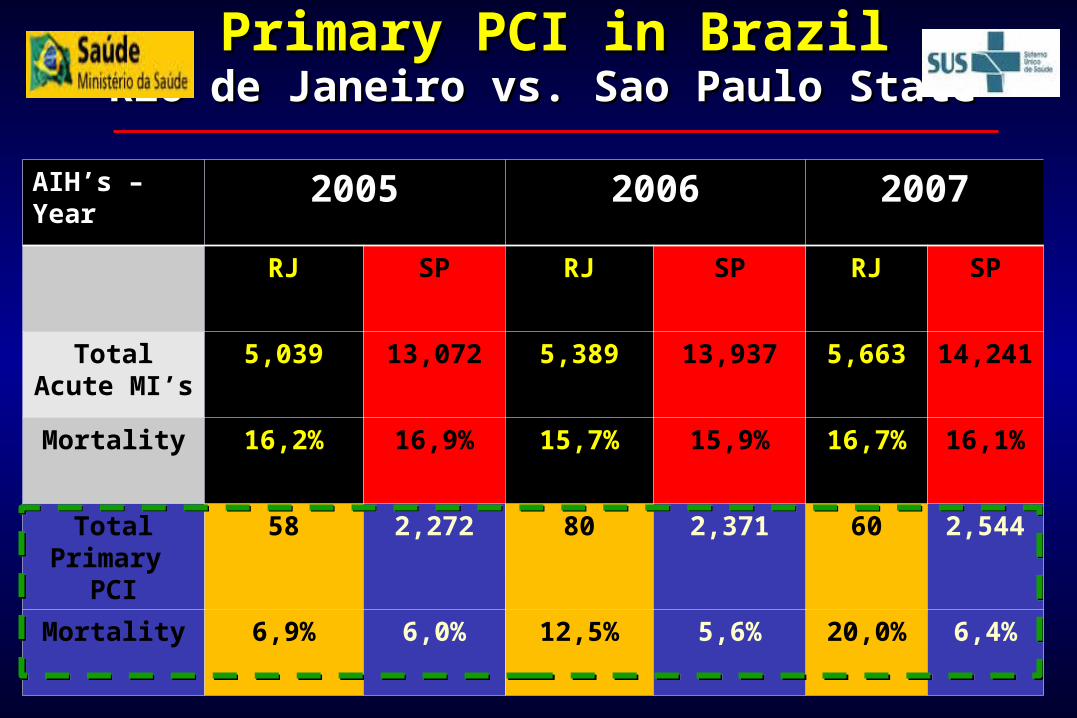
Primary PCI in BrazilPrimary PCI in BrazilRio de Janeiro vs. Sao Paulo State Rio de Janeiro vs. Sao Paulo State
AIH’s – Year 2005 2006 2007
RJ SP RJ SP RJ SP
Total Acute MI’s
5,039 13,072 5,389 13,937 5,663 14,241
Mortality 16,2% 16,9% 15,7% 15,9% 16,7% 16,1%
Total Primary PCI
58 2,272 80 2,371 60 2,544
Mortality 6,9% 6,0% 12,5% 5,6% 20,0% 6,4%
Continuous Update for Primary PCI Continuous Update for Primary PCI Improving Operator Experience Improving Operator Experience
Logistic and Pharmacological Enforces UpdateLogistic and Pharmacological Enforces Update Clopidogrel and beyondClopidogrel and beyond
Bivalirudin and IIb/IIIa Inhibitors Bivalirudin and IIb/IIIa Inhibitors
Mechanical and Intra-Procedural StrategiesMechanical and Intra-Procedural Strategies Direct Stenting: DES or BMSDirect Stenting: DES or BMS
To aspirate or not aspirate all culprit AMI vessels To aspirate or not aspirate all culprit AMI vessels
Rheolytic strategiesRheolytic strategies
No/Slow Flow ProphylaxisNo/Slow Flow Prophylaxis
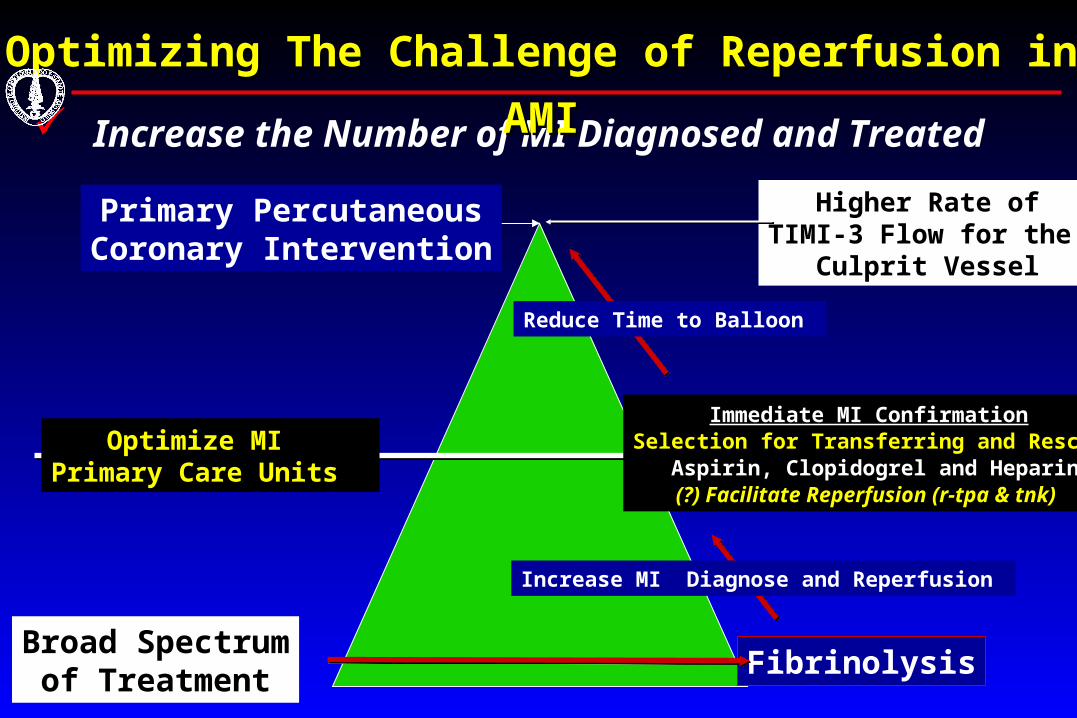
Increase the Number of MI Diagnosed and Treated
Optimizing The Challenge of Reperfusion in AMIOptimizing The Challenge of Reperfusion in AMI
Higher Rate ofTIMI-3 Flow for the
Culprit Vessel
Primary PercutaneousCoronary Intervention
FibrinolysisBroad Spectrum
of Treatment
Optimize MI Primary Care Units
Immediate MI ConfirmationSelection for Transferring and Rescue
Aspirin, Clopidogrel and Heparin(?) Facilitate Reperfusion (r-tpa & tnk)
Increase MI Diagnose and Reperfusion
Reduce Time to Balloon
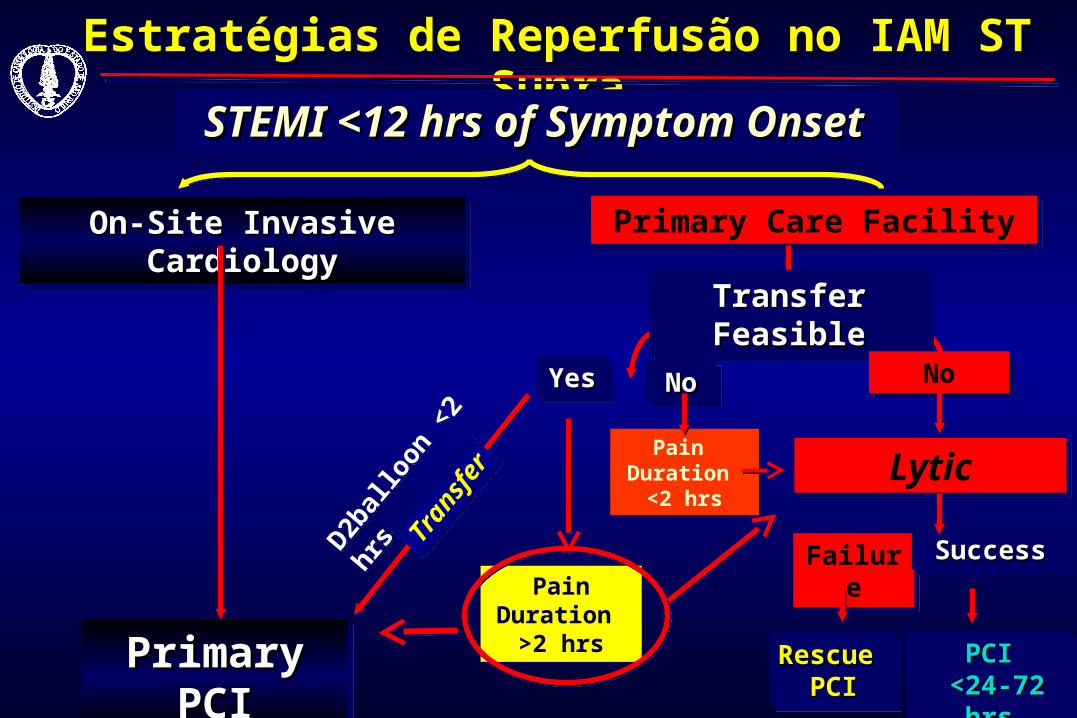
Estratégias de Reperfusão no IAM ST SupraEstratégias de Reperfusão no IAM ST Supra
STEMI <12 hrs of Symptom OnsetSTEMI <12 hrs of Symptom OnsetSTEMI <12 hrs of Symptom OnsetSTEMI <12 hrs of Symptom Onset
On-Site Invasive CardiologyOn-Site Invasive CardiologyOn-Site Invasive CardiologyOn-Site Invasive Cardiology
Primary PCIPrimary PCIPrimary PCIPrimary PCI
Primary Care FacilityPrimary Care Facility
Transfer FeasibleTransfer FeasibleTransfer FeasibleTransfer Feasible
YesYesYesYes NoNo
LyticLytic
FailureFailure SuccessSuccessSuccessSuccess
PCIPCI <24-72 hrs<24-72 hrs
PCIPCI <24-72 hrs<24-72 hrs
Rescue Rescue PCIPCI
Rescue Rescue PCIPCI
Tran
sfer
Tran
sfer
D2bal
loon
<2
hrs
D2bal
loon
<2
hrs
Pain Duration
>2 hrs
Pain Duration
>2 hrs
NoNoNoNo
Pain Duration
<2 hrs
Pain Duration
<2 hrs
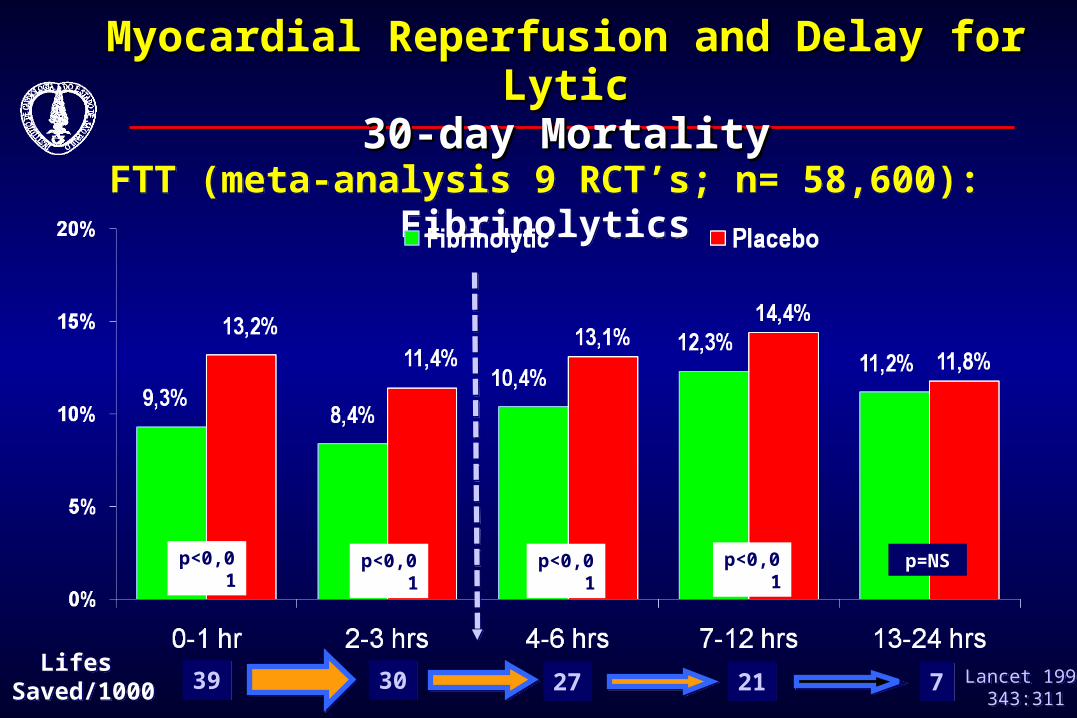
FTT (meta-analysis 9 RCT’s; n= 58,600): FibrinolyticsFTT (meta-analysis 9 RCT’s; n= 58,600): Fibrinolytics
Lancet 1994343:311
Lancet 1994343:311
p<0,01 p<0,01p<0,01 p<0,01 p=NS
Lifes Saved/1000
Lifes Saved/1000 3939 3030 2727 2121 77
Myocardial Reperfusion and Delay for LyticMyocardial Reperfusion and Delay for Lytic30-day Mortality30-day Mortality
Selecting the Best Reperfusion Strategy Selecting the Best Reperfusion Strategy Fibrinolysis and Primary PCIFibrinolysis and Primary PCI
Fibrinolysis is not unreasonable when:Fibrinolysis is not unreasonable when: PCI associated with unacceptable delay (Class I)PCI associated with unacceptable delay (Class I)
Short time from symptom onset (<2 hr) (Class I) with anticipated Short time from symptom onset (<2 hr) (Class I) with anticipated
door-to-balloon >2 hoursdoor-to-balloon >2 hours
Primary PCI is superior to Fibrinolysis in several Primary PCI is superior to Fibrinolysis in several clinical situations, particularly if:clinical situations, particularly if:
Competent personnel involvedCompetent personnel involved
DB times are <90 Min, PCI related Delay AcceptableDB times are <90 Min, PCI related Delay Acceptable
High Risk for Bleeding or Complication from MIHigh Risk for Bleeding or Complication from MI
Late PresentationLate Presentation
Selecting the Best Reperfusion Strategy Selecting the Best Reperfusion Strategy Fibrinolysis and Primary PCIFibrinolysis and Primary PCI
“ “ One Size, Definitely, One Size, Definitely,
Does Not Fit for All AMI’s… Does Not Fit for All AMI’s…
Logistics Sinergy is the way”Logistics Sinergy is the way”

The “Patient Size” Will Always Be #...The “Patient Size” Will Always Be #...Joint Efforts Are Mandatory !! Joint Efforts Are Mandatory !!
Rio de Janeiro, March 7 Th 2008
www.sbhci.org.br
Rio de Janeiro, March 7 Th 2008
www.sbhci.org.br
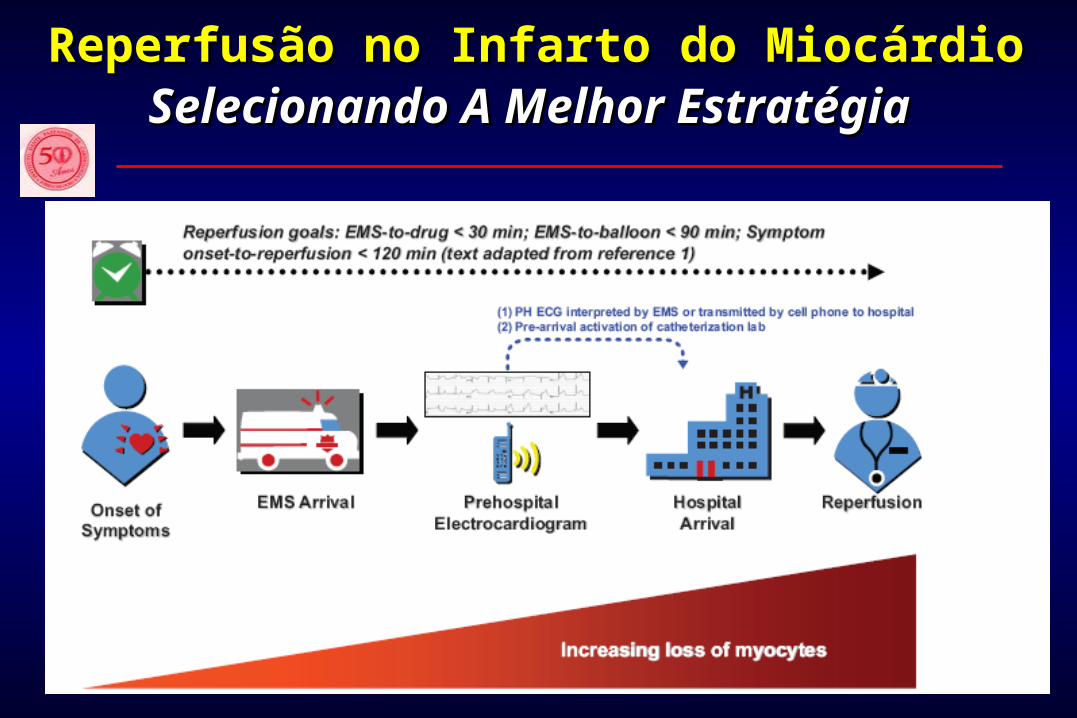
Reperfusão no Infarto do MiocárdioReperfusão no Infarto do MiocárdioSelecionando A Melhor EstratégiaSelecionando A Melhor Estratégia





























