Embed Size (px)
Citation preview

FHCA 2014 Annual Conference & Trade Show
CE Session #28 – Risk Management and Reporting Precision for ALFs Wednesday, July 9 – 2:30 to 3:30 p.m.
Crystal K – Assisted Living
Upon completion of this presentation, the learner will be able to:
apply basic risk management concepts to assisted living operations;
navigate incident decision making and reporting; and
compare aspects of Florida’s ALF Risk Management and Quality Assurance program to the Adverse Incident Reporting System.
Seminar Description: Florida’s assisted living facilities operate with specific resident protections, including reporting adverse incidents and allegations of abuse, neglect and exploitation. While risk management and quality assurance programs are voluntary in assisted living (except for those with the ECC specialty license), these concepts of managed risk are accessible to all ALFs and arguably already part of daily operations, though perhaps informally and undocumented. This session will review regulatory requirements for adverse incident and abuse reporting and explore how concepts of risk management connect with assisted living. Presenter Bio(s): Dorene Bissonette, RN Clinical Risk Manager has been with Opis Management Resources for the last 17 years. Serving the past four years as Clinical Risk Manager, she has covered their Assisted Living Center as well as Skilled Nursing Centers. In 2012, she completed the ALF Core Training. Dorene graduated from Cazenovia College in Upstate New York in 1977 and then completed her Nursing Education with Crouse Irving Memorial Hospital School of Nursing in Syracuse, N.Y. She lives in Palm Coast Florida. Lee Ann Griffin is the Director of Quality & Regulatory Services for Florida Health Care Association. Over a 15-year career, Lee Ann has developed extensive expertise in the rules, laws, and policy interpretations for nursing homes and assisted living facilities. Lee Ann holds a degree in Information Studies, has worked as a CNA, served as an appointee to the Florida Board of Nursing’s CNA Council and, most recently, completed the ALF Administrator’s Core Training.

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 1
Risk Management and Reporting Requirements for Florida’s Assisted Living Facilities
Risk Management and Reporting Requirements for Florida’s Assisted Living Facilities
Doreen Bissonette, RNClinical Risk Manager, OPIS
Lee Ann GriffinDirector/Quality & Regulatory ServicesFlorida Care Association
Defining Risk ManagementDefining Risk Management
The process to identify, control, and minimize the impact of uncertain events (DHS)
The likelihood that a threat will harm an asset and deciding on actions to reduce it (FEMA)
Figuring out which attacks are worth worrying about and spending money on and which are better left ignored (DeRugy)
The process to identify, control, and minimize the impact of uncertain events (DHS)
The likelihood that a threat will harm an asset and deciding on actions to reduce it (FEMA)
Figuring out which attacks are worth worrying about and spending money on and which are better left ignored (DeRugy)
July 2014Risk Management & Reporting Requirements for FL's ALFs 2

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 2
Risk Management FocusRisk Management Focus
Financial
Litigation
Disaster
Health Care
Enterprise
Financial
Litigation
Disaster
Health Care
Enterprise
July 2014Risk Management & Reporting Requirements for FL's ALFs 3
Risk Management UniversalsRisk Management Universals
Harm: unwanted consequences or losses
Uncertainty: an event may or may not happen
Allocation of resources to prevent or mitigate
Harm: unwanted consequences or losses
Uncertainty: an event may or may not happen
Allocation of resources to prevent or mitigate
July 2014Risk Management & Reporting Requirements for FL's ALFs 4

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 3
What’s your risk appetite?What’s your risk appetite?
High ToleranceHigh Tolerance You are okay if some risks
can’t be controlled
You ask: how much is that costing?
You see resident falls as a consequence of aging and declining abilities
Survey fines are a part of doing business
The only policies you have are those required by regulation
You are okay if some risks can’t be controlled
You ask: how much is that costing?
You see resident falls as a consequence of aging and declining abilities
Survey fines are a part of doing business
The only policies you have are those required by regulation
Low ToleranceLow Tolerance You are overcomplying with
regulations
You focus most on preventing high drama events with a low probability
You tend to internalize every fall
Survey fines are a reflection of your job
Your facility policies read like national best practices
You are overcomplying with regulations
You focus most on preventing high drama events with a low probability
You tend to internalize every fall
Survey fines are a reflection of your job
Your facility policies read like national best practices
6
Ranking Risks (to Residents)Ranking Risks (to Residents)
Outcome or ImpactOutcome or Impact Catastrophic
Major
Moderate
Minor
Insignificant
Catastrophic
Major
Moderate
Minor
Insignificant
Likelihood to HappenLikelihood to Happen Almost certain
Likely
Moderate
Unlikely
Remote
Almost certain
Likely
Moderate
Unlikely
Remote
July 2014Risk Management & Reporting Requirements for FL's ALFs 7

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 4
July 2014Risk Management & Reporting Requirements for FL's ALFs 8
Directing resources
Preparing for the High/Very HighPreparing for the High/Very High
Resident Expectations
Third Parties
Employee Management
Incident Response
Resident Expectations
Third Parties
Employee Management
Incident Response
July 2014Risk Management & Reporting Requirements for FL's ALFs 9

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 5
Resident ExpectationsResident Expectations
Marketing Escalating resident
expectations
Admissions Unlimited levels of care
Marketing Escalating resident
expectations
Admissions Unlimited levels of care
July 2014Risk Management & Reporting Requirements for FL's ALFs 10
Third PartiesThird Parties
Private duty aides
3rd party providers
Private duty aides
3rd party providers
July 2014Risk Management & Reporting Requirements for FL's ALFs 12

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 6
3rd Party ProvidersAdministrators must:
3rd Party ProvidersAdministrators must:
• Take action to assist in facilitating the provision of services, and
• Coordinate with the provider to meet the specific service goals
• Unless resident declines• Review annually
• Does not represent a guarantee
• Take action to assist in facilitating the provision of services, and
• Coordinate with the provider to meet the specific service goals
• Unless resident declines• Review annually
• Does not represent a guarantee
July 2014Risk Management & Reporting Requirements for FL's ALFs 13
Employee ManagementEmployee Management
Employee Policies
Exit interviews
Employee Policies
Exit interviews
July 2014Risk Management & Reporting Requirements for FL's ALFs 14

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 7
Incident and Investigation ReportsIncident and Investigation Reports
Writing the report Writing the report
July 2014Risk Management & Reporting Requirements for FL's ALFs 15
Priority 1:Resident is safe.
Writing the Internal ReportWriting the Internal Report
Why To make management aware something has occurred
When Upon becoming aware of incident
What Employees can recognize what is and what is not a
documentable incident
Why To make management aware something has occurred
When Upon becoming aware of incident
What Employees can recognize what is and what is not a
documentable incident
July 2014Risk Management & Reporting Requirements for FL's ALFs 16

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 8
Florida’s Risk Management and Reporting Environment for Assisted Living
Florida’s Risk Management and Reporting Environment for Assisted Living
Risk Management and Quality Assurance Program
External Incident Reporting
Risk Management and Quality Assurance Program
External Incident Reporting
July 2014Risk Management & Reporting Requirements for FL's ALFs 17
Comparing Provisions, s. 429.23, F.S.Comparing Provisions, s. 429.23, F.S.
RM & QA Program AI Reporting
External
Mandatory
Specific definition
Some legal protections
Internal
Voluntary
Specific purpose
Some protections
July 2014Risk Management & Reporting Requirements for FL's ALFs 18
Some legal protectionsSome protections

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 9
ALF Risk Management and Reporting ProtectionsALF Risk Management and Reporting Protections
Risk Management and Quality Assurance Program
Risk Management and Quality Assurance Program No specific authority for
the Agency for Health Care Administration to have access to internal working incident reports and investigation papers not externally reported through AI or ANE
Agency cannot release records of a RMQA Committee (s.400.119, F.S.)
No specific authority for the Agency for Health Care Administration to have access to internal working incident reports and investigation papers not externally reported through AI or ANE
Agency cannot release records of a RMQA Committee (s.400.119, F.S.)
Adverse Incident Reporting
Adverse Incident Reporting
Confidential as provided by law, not discoverable or admissible in any civil or administrative action Except in disciplinary
proceedings re: an individual licensee
s. 429.23 (9), F.S.
Confidential as provided by law, not discoverable or admissible in any civil or administrative action Except in disciplinary
proceedings re: an individual licensee
s. 429.23 (9), F.S.
July 2014 19
Internal Risk Management and Quality Assurance ProgramInternal Risk Management and Quality Assurance Program
Voluntary
Purpose Assess
Resident care practices
Facility incident reports
Deficiencies
Adverse incident reports
Resident grievances
Develop plans of action to correct and quickly identify quality differences
Voluntary
Purpose Assess
Resident care practices
Facility incident reports
Deficiencies
Adverse incident reports
Resident grievances
Develop plans of action to correct and quickly identify quality differences
July 2014Risk Management & Reporting Requirements for FL's ALFs 21

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 10
Adverse Events in ContextAdverse Events in Context
Adverse Event An injury resulting from a medical intervention
Adverse events may not be errors
Adverse events may not be preventable A patient who has surgery and dies from
pneumonia postoperatively is an adverse event Due to poor instrument cleaning?
Due to a difficult surgery and recovery?
Not all adverse events result in harm
Adverse Event An injury resulting from a medical intervention
Adverse events may not be errors
Adverse events may not be preventable A patient who has surgery and dies from
pneumonia postoperatively is an adverse event Due to poor instrument cleaning?
Due to a difficult surgery and recovery?
Not all adverse events result in harmJuly 2014Risk Management & Reporting Requirements for FL's ALFs 22
Florida’s Adverse EventsIncidentsFlorida’s Adverse EventsIncidents
Florida’s take on Adverse Events They are called adverse incidents
They are always preventable
They are within the control of the ALF
They result in certain outcomes
Not every bad thing that happens in an ALF in an adverse incident
ANE is not always an adverse incident Resident to resident in some cases, or family member or guest
Ask: how would the facility have prevented the ANE from occurring?
Florida’s take on Adverse Events They are called adverse incidents
They are always preventable
They are within the control of the ALF
They result in certain outcomes
Not every bad thing that happens in an ALF in an adverse incident
ANE is not always an adverse incident Resident to resident in some cases, or family member or guest
Ask: how would the facility have prevented the ANE from occurring? 23

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 11
FL’s Adverse Incident DefinedFL’s Adverse Incident Defined
An event over which facility personnel could exercise control rather than as a result of the resident’s condition and results in:
1. Death2. Brain or spinal damage3. Permanent disfigurement4. Fracture or dislocation of bones and joints5. Any condition that required medical attention to which the resident has
not given his or her consent, including failure to honor advanced directives
6. Any condition that requires the transfer of the resident from the facility to a unit providing more acute care due to the incident rather than the resident’s condition before the incident; or
7. An event that is reported to law enforcement or its personnel for investigation
Resident elopement, if the elopement places the resident at risk of harm or injury.
An event over which facility personnel could exercise control rather than as a result of the resident’s condition and results in:
1. Death2. Brain or spinal damage3. Permanent disfigurement4. Fracture or dislocation of bones and joints5. Any condition that required medical attention to which the resident has
not given his or her consent, including failure to honor advanced directives
6. Any condition that requires the transfer of the resident from the facility to a unit providing more acute care due to the incident rather than the resident’s condition before the incident; or
7. An event that is reported to law enforcement or its personnel for investigation
Resident elopement, if the elopement places the resident at risk of harm or injury.
24
Reporting Adverse IncidentsReporting Adverse Incidents
Incident
Day 1
Day 15
July 2014Risk Management & Reporting Requirements for FL's ALFs 25

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 12
Abuse, Neglect, and ExploitationAbuse, Neglect, and Exploitation
Report to the Central Abuse Hotline, managed by the Department of Children and Families immediately 1/800-962-2873
Reports are based on: Knowledge of, or a reasonable cause to suspect ANE
Report to the Central Abuse Hotline, managed by the Department of Children and Families immediately 1/800-962-2873
Reports are based on: Knowledge of, or a reasonable cause to suspect ANE
July 2014Risk Management & Reporting Requirements for FL's ALFs 26
Incident Reporting Decision TreeIncident Reporting Decision Tree
Begin investigation
Apply regulatory definitions to decide whether or not the incident is:• abuse, neglect, or exploitation – or gives you a
reasonable cause to suspect that ANE may have occurred, or
• a possible or definite adverse incident
What constitutes closure of responding to an incident?
Begin investigation
Apply regulatory definitions to decide whether or not the incident is:• abuse, neglect, or exploitation – or gives you a
reasonable cause to suspect that ANE may have occurred, or
• a possible or definite adverse incident
What constitutes closure of responding to an incident?
July 2014Risk Management & Reporting Requirements for FL's ALFs 27

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 13
Agency’s Online ReportingAgency’s Online Reporting
Note to Lee Ann: Consider showing the screen shots and advising about the incorrect nature of what’s asked as part of the reporting format
Note to Lee Ann: Consider showing the screen shots and advising about the incorrect nature of what’s asked as part of the reporting format
July 2014Risk Management & Reporting Requirements for FL's ALFs 28
External Perspective of an IncidentExternal Perspective of an Incident
Residents are assessed (non-nursing sense of the word), cared for, and protected
All incidents are investigated Status as an adverse incident has been ruled out
Status as an allegation of abuse, neglect, or exploitation has been ruled out
Reporting timeframes were met
Residents are assessed (non-nursing sense of the word), cared for, and protected
All incidents are investigated Status as an adverse incident has been ruled out
Status as an allegation of abuse, neglect, or exploitation has been ruled out
Reporting timeframes were met
July 2014Risk Management & Reporting Requirements for FL's ALFs 29

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 14
Incident Response:Staff TrainingIncident Response:Staff Training
Do not major on the minor
Focus on the tasks that always have to be done regardless of the incident type Resident care response (elopement, harm, etc.)
How to write on an internal reporting form
Focus on the triggers for bumping up to a higher response level
Tailor the training to the employee response level
Do not major on the minor
Focus on the tasks that always have to be done regardless of the incident type Resident care response (elopement, harm, etc.)
How to write on an internal reporting form
Focus on the triggers for bumping up to a higher response level
Tailor the training to the employee response level
July 2014Risk Management & Reporting Requirements for FL's ALFs 30
Parting WordsParting Words
Know thyself and thine own risk appetite
Prepare for the high/very high risk outcomes
Understand your internal Risk Management and Quality Assurance Program
Know the triggers for external incident reporting
Make sure staff training matches your priorities
If all else fails, do your best for the resident and document that
Know thyself and thine own risk appetite
Prepare for the high/very high risk outcomes
Understand your internal Risk Management and Quality Assurance Program
Know the triggers for external incident reporting
Make sure staff training matches your priorities
If all else fails, do your best for the resident and document that
July 2014Risk Management & Reporting Requirements for FL's ALFs 31

Risk Management and Reporting Requirements in ALFs
5/21/2014
2014 Copyright Florida Health Care Association 15
Thank youThank you
Doreen Bissonette, RNClinical Risk Manager, [email protected]
Lee Ann GriffinDirector/Quality & RegulatoryFlorida Care [email protected]
Doreen Bissonette, RNClinical Risk Manager, [email protected]
Lee Ann GriffinDirector/Quality & RegulatoryFlorida Care [email protected]
Risk Management & Reporting Requirements for FL's ALFs

Timeline for Adverse Incident Reporting Requirements429.23, Florida Statutes, applicable to Assisted Living Facilities
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Report possible Adverse Incidents to the Agency for Health Care Administration* Online: http://ahca.myflorida.com/reporting/index.shtml (within 1 business day after occurrence)
Incident
Report results of investigation of incident to the Agency, with determination of “Adverse” or “Not an Adverse Incident”:
Online: http://ahca.myflorida.com/reporting/index.shtml (within 15 days of occurrence)
Resources429.23, F.S.
58A-5.0241, FAC59A-35.110, FAC
ALF Adverse Incident Information at http://ahca.myflorida.com/reporting/
alf_advincd_info.shtmlL. Griffin 3-2013
Adverse incident means:
An event over which facility personnel could exercise control rather than as a results of the resident’s condition, and
results in one of the following:1. Death;2. Brain or spinal damage;3. Permanent disfigurement;4. Fracture or dislocation of bones or joints;5. Any condition that required medical attention to which the resident has not given his or her consent, including failure to honor advanced directives;7. Any condition that required the transfer of the resident, within or outside the facility, to a unit providing a more acute level of care due to the adverse incident, rather than the resident’s condition before the incident; or8. An event that is reported to law enforcement or its personnel for investigation; or
Resident elopement, if the elopement places the resident at risk of harm or injury.
* “If it is determined within the 1 day reporting timeframe that an event does not meet the statutory definition of an adverse incident, no 1 day report is required.”
Agency for Health Care Administration, May 11, 2012.
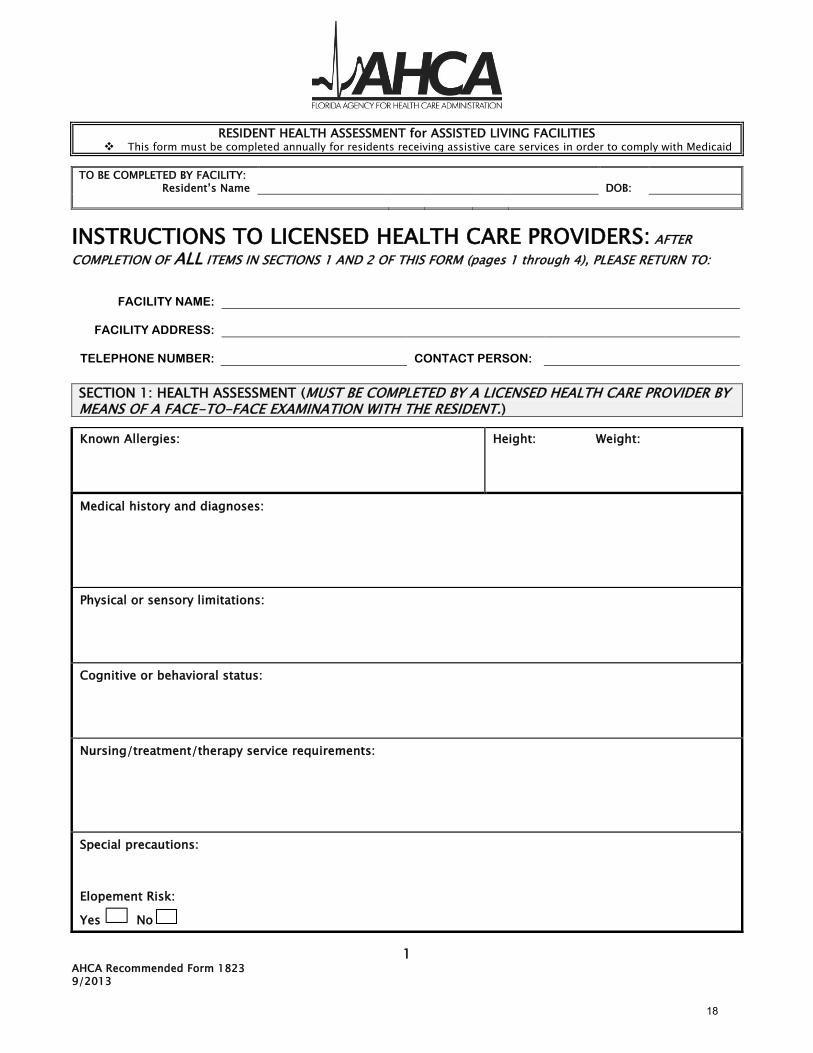
1 AHCA Recommended Form 1823 9/2013
RESIDENT HEALTH ASSESSMENT for ASSISTED LIVING FACILITIES This form must be completed annually for residents receiving assistive care services in order to comply with Medicaid
TO BE COMPLETED BY FACILITY: Resident’s Name
DOB:
INSTRUCTIONS TO LICENSED HEALTH CARE PROVIDERS: AFTER
COMPLETION OF ALL ITEMS IN SECTIONS 1 AND 2 OF THIS FORM (pages 1 through 4), PLEASE RETURN TO:
FACILITY NAME:
FACILITY ADDRESS:
TELEPHONE NUMBER:
CONTACT PERSON:
SECTION 1: HEALTH ASSESSMENT (MUST BE COMPLETED BY A LICENSED HEALTH CARE PROVIDER BY MEANS OF A FACE-TO-FACE EXAMINATION WITH THE RESIDENT.)
Known Allergies:
Height: Weight:
Medical history and diagnoses:
Physical or sensory limitations:
Cognitive or behavioral status:
Nursing/treatment/therapy service requirements:
Special precautions:
Elopement Risk:
Yes No
18

AHCA Recommended Form 1823
2
TO BE COMPLETED BY FACILITY: Resident’s Name
DOB:
SECTION 1: HEALTH ASSESSMENT (MUST BE COMPLETED BY A LICENSED HEALTH CARE PROVIDER BY MEANS OF A FACE-TO-FACE EXAMINATION WITH THE RESIDENT.)
A. To what extent does the individual need supervision or assistance with the following?
Key I = Independent S = Needs Supervision A = Needs Assistance T = Total Care
Indicate by a checkmark () in the appropriate column below the extent to which the individuals is able to perform each of the activities of daily living. If “needs supervision” or “needs assistance” is indicated, please explain the extent and type of supervision or assistance needed in the comments column.*
ACTIVITIES OF DAILY LIVING I S* A* T COMMENTS*
Ambulation
Bathing
Dressing
Eating
Self Care (grooming)
Toileting
Transferring
B. Special Diet Instructions
Regular Calorie Controlled No Added Salt Low Fat/Low Cholesterol
Other, please describe:
C. Does the individual have any of the following conditions/requirements? If yes, please include an explanation in the comments column.
STATUS YES/N0 (Y/N) COMMENTS
1. A communicable disease, which could be transmitted to other residents or staff?
2. Bedridden?
3. Any stage 2, 3, or 4 pressure sores?
4. Pose a danger to self or others?
5. Require 24-hour nursing or psychiatric care?
D. In your professional opinion, can this individual's needs be met in an assisted living facility, which is not a medical, nursing or psychiatric facility? Yes No ___
Comments (Use additional page if necessary):
19
AHCA Recommended Form 1823
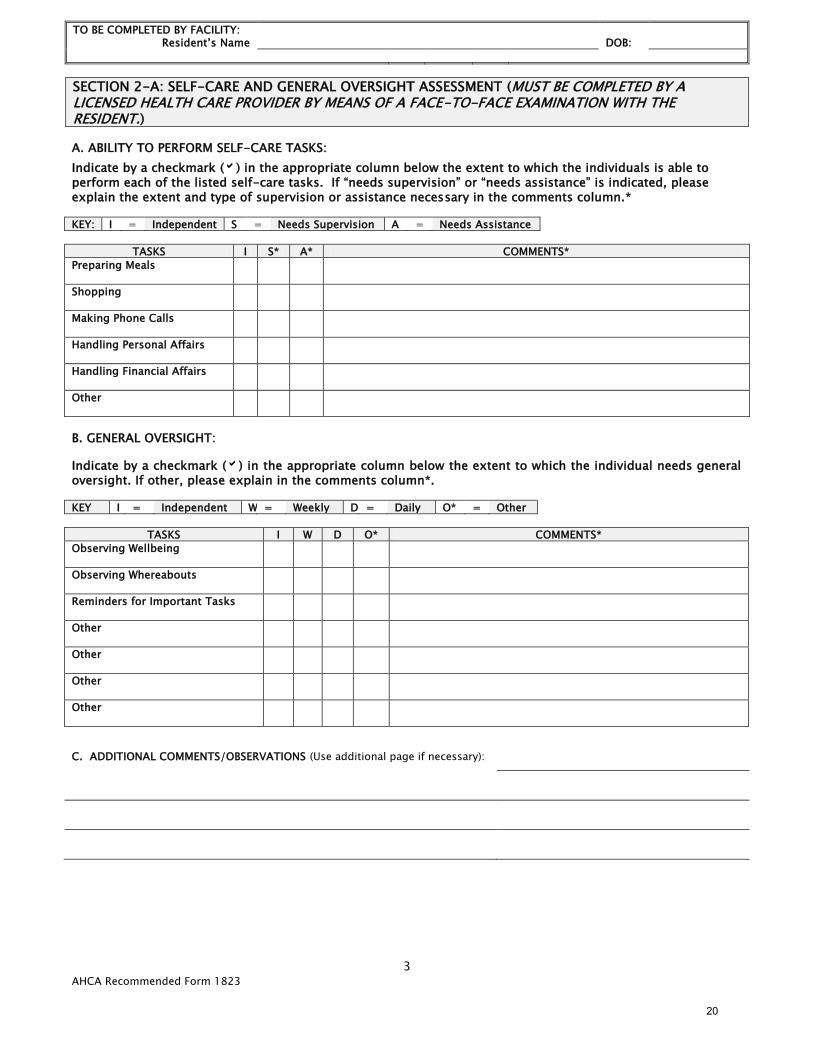
3
TO BE COMPLETED BY FACILITY: Resident’s Name
DOB:
SECTION 2-A: SELF-CARE AND GENERAL OVERSIGHT ASSESSMENT (MUST BE COMPLETED BY A LICENSED HEALTH CARE PROVIDER BY MEANS OF A FACE-TO-FACE EXAMINATION WITH THE RESIDENT.)
A. ABILITY TO PERFORM SELF-CARE TASKS:
Indicate by a checkmark () in the appropriate column below the extent to which the individuals is able to perform each of the listed self-care tasks. If “needs supervision” or “needs assistance” is indicated, please explain the extent and type of supervision or assistance necessary in the comments column.* KEY: I = Independent S = Needs Supervision A = Needs Assistance
TASKS I S* A* COMMENTS*
Preparing Meals
Shopping
Making Phone Calls
Handling Personal Affairs
Handling Financial Affairs
Other
B. GENERAL OVERSIGHT:
Indicate by a checkmark () in the appropriate column below the extent to which the individual needs general oversight. If other, please explain in the comments column*.
KEY I = Independent W = Weekly D = Daily O* = Other
TASKS I W D O* COMMENTS*
Observing Wellbeing
Observing Whereabouts
Reminders for Important Tasks
Other
Other
Other
Other
C. ADDITIONAL COMMENTS/OBSERVATIONS (Use additional page if necessary):
20

AHCA Recommended Form 1823
4
TO BE COMPLETED BY FACILITY: Resident’s Name
DOB:
SECTION 2-B: SELF-CARE AND GENERAL OVERSIGHT ASSESSMENT—MEDICATIONS (MUST BE COMPLETED BY A LICENSED HEALTH CARE PROVIDER BY MEANS OF A FACE-TO-FACE EXAMINATION WITH THE RESIDENT.)
A. Please list all current medications prescribed below (additional pages may be attached):
MEDICATION
DOSAGE
DIRECTIONS FOR USE
ROUTE
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
B. Does the individual need help with taking his or her medications (meds)? Yes No . If yes, please place a checkmark () in front of the appropriate box below:
Needs Assistance with Self-Administration of Medications This allows unlicensed staff to assist with orals and topical medication.
Needs Medication Administration Not all ALFs have licensed staff to provide this service.
Able to Administer w/o Assistance
C. ADDITIONAL COMMENTS/OBSERVATIONS (Use additional page if necessary):
NOTE: MEDICAL CERTIFICATION IS INCOMPLETE WITHOUT THE FOLLOWING INFORMATION:
NAME OF EXAMINER (Please Print):
SIGNATURE OF EXAMINER:
MEDICAL LICENSE #:
ADDRESS OF EXAMINER:
TELEPHONE #:
TITLE OF EXAMINER (Please check the appropriate box): MD DO ARNP PA
DATE OF EXAMINATION:
21

5 AHCA Recommended Form 1823 9/2013
TO BE COMPLETED BY FACILITY: Resident’s Name
DOB:
SECTION 3: SERVICES OFFERED OR ARRANGED BY THE FACILITY FOR THE RESIDENT (MUST BE COMPLETED BY THE ALF ADMINISTRATOR OR DESIGNEE.)
Note: This section must be completed for all residents based on needs identified in Sections 1 and 2 of this form, or electronic documentation, which at a minimum includes the elements below. The facility may attach the resident’s service plan, care plan, or community living support plan to this document to satisfy this requirement provided the documentation captures the information listed below.
# (Column 1) Needs Identified
from Sections 1 & 2
(Column 2) Service Needed
(Column 3) Service Frequency
& Duration
(Column 4) Service Provider Name
(Column 5) Date Service
Began
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
NAME OF RECIPIENT OR GUARDIAN: (Please Print) SIGNATURE OF RECIPIENT OR GUARDIAN: NAME OF ADMINISTRATOR OR DESIGNEE: (Please Print) SIGNATURE OF ADMINISTRATOR OR DESIGNEE:
Does the facility intend to use this form to satisfy the Medicaid assessment for assistive care services? Yes No
If yes, page 6 is required to be completed. If no, Stop.
22

AHCA Recommended Form 1823
6
CERTICATE OF MEDICAID NECESSITY
THIS PAGE MUST ALSO BE FILLED OUT FOR RESIDENTS THAT RECEIVE
MEDICAID ASSISTIVE CARE SERVICES
Resident Name ________________________________________ DOB ____________
This is to certify that this recipient is in need of an integrated set of assistive care services on a 24-hour basis,
including at least two of the following four service components on a daily basis (check as applicable):
____ Assistance with activities of daily living, which is defined as individual assistance with ambulating,
transferring, bathing, dressing, eating, grooming, and/or toileting.
____ Assistance with instrumental activities of daily living, which is defined as individual assistance with
shopping for personal items, making telephone calls, managing money, etc.
____ Health support, which is defined as observing the resident’s whereabouts and well-being; reminding
the resident of any important tasks; and recording and reporting any significant changes in appearance,
behavior, or state of health to the health care provider, designated representative, or case manager.
____ Assistance with self-administration of medication, which is defined as assistance with or
supervision of self-administration of medication as permitted by law.
HEALTH CARE PROVIDER
Facility Name: ____________________________________________
License Number: __________________________________________
Administrators’ Signature: ___________________________________
Date Signed: ____________________________________________
CERTIFICATION OF MEDICAL NECESSITY:
Physician/Physician Assistant/
Advanced Registered Nurse Practitioner/
Registered Nurse: ____________________________________________
Date: ____________________________________________
The resident service log is still required for Medicaid residents.
23

AHCA Recommended Form 1823
7
24

Abuse, Neglect and Exploitation Regulatory Summary s. 415.102 and .1034, Florida Statutes
2014
Abuse means any willful act or threatened act by a relative, caregiver, or household member which causes or is likely to cause significant impairment to a vulnerable adult’s physical, mental, or emotional health. Abuse includes acts and omissions.
Exploitation means a person who:
1. Stands in a position of trust and confidence with a vulnerable adult and knowingly, by deception or intimidation, obtains or uses, or endeavors to obtain or use, a vulnerable adult’s funds, assets, or property with the intent to temporarily or permanently deprive a vulnerable adult of the use, benefit, or possession of the funds, assets, or property for the benefit of someone other than the vulnerable adult; or
2. Knows or should know that the vulnerable adult lacks the capacity to consent, and obtains or uses, or endeavors to obtain or use, the vulnerable adult’s funds, assets, or property with the intent to temporarily or permanently deprive the vulnerable adult of the use, benefit, or possession of the funds, assets, or property for the benefit of someone other than the vulnerable adult.
(b) “Exploitation” may include, but is not limited to:
1. Breaches of fiduciary relationships, such as the misuse of a power of attorney or the abuse of guardianship duties, resulting in the unauthorized appropriation, sale, or transfer of property;
2. Unauthorized taking of personal assets;
3. Misappropriation, misuse, or transfer of moneys belonging to a vulnerable adult from a personal or joint account; or
4. Intentional or negligent failure to effectively use a vulnerable adult’s income and assets for the necessities required for that person’s support and maintenance.
Neglect means the failure or omission on the part of the caregiver or vulnerable adult to provide the care, supervision, and services necessary to maintain the physical and mental health of the vulnerable adult, including, but not limited to, food, clothing, medicine, shelter, supervision, and medical services, which a prudent person would consider essential for the well-being of a vulnerable adult. The term “neglect” also means the failure of a caregiver or vulnerable adult to make a reasonable effort to protect a vulnerable adult from abuse, neglect, or exploitation by others. “Neglect” is repeated conduct or a single incident of carelessness which produces or could reasonably be expected to result in serious physical or psychological injury or a substantial risk of death.
Mandatory Reporting is required for any person – including, but not limited to nursing home staff; assisted living facility staff; adult day care center staff; adult family-care home staff; social worker; or other professional adult care, residential, or institutional staff – who knows, or has reasonable cause to suspect, that a vulnerable adult has been or is being abused, neglected, or exploited.
1-800-962-2873 or www.dcf.state.fl.us/programs/abuse/report.shtml
Florida Health Care Association 25
Mail To: P. O. Box 1459, Tallahassee, Florida 32302-1459 Telephone: (850) 224-3907 Fax: (850) 681-2075
www.fhca.org
ALFs with Extended Congregate Care Specialty License I. ALFs with an ECC license must use concepts of risk management (429.07 (3)(b) 3. f., F.S.)
a. Managed risk is defined in statute (429.02 (14), F.S.). II. ALFs must allow residents to share responsibility in decision-making (429.07 (3)(b) 3. e., F.S.)
a. Shared responsibility is defined in statute (429.02 (22), F.S.). Regulatory Authority: 429.07 License required; fee.— 3. A facility that is licensed to provide extended congregate care services must: e. Allow residents or, if applicable, a resident’s representative, designee, surrogate, guardian, or attorney in fact to make a variety of personal choices, participate in developing service plans, and share responsibility in decision-making. f. Implement the concept of managed risk. 429.02 Regulatory Definitions (14) “Managed risk” means the process by which the facility staff discuss the service plan and the needs of the resident with the resident and, if applicable, the resident’s representative or designee or the resident’s surrogate, guardian, or attorney in fact, in such a way that the consequences of a decision, including any inherent risk, are explained to all parties and reviewed periodically in conjunction with the service plan, taking into account changes in the resident’s status and the ability of the facility to respond accordingly. (22) “Shared responsibility” means exploring the options available to a resident within a facility and the risks involved with each option when making decisions pertaining to the resident’s abilities, preferences, and service needs, thereby enabling the resident and, if applicable, the resident’s representative or designee, or the resident’s surrogate, guardian, or attorney in fact, and the facility to develop a service plan which best meets the resident’s needs and seeks to improve the resident’s quality of life.
________________________________________________________________________________________
Street Address: 307 West Park Avenue, Tallahassee, FL 32301-1427 26

Internal Risk Management and Quality Assurance Program and Adverse Incident Reporting Regulatory Authority
s. 429.23, F.S.; s. 58A-5, FAC; s. 59A-35, FAC 2014
Florida Statute 429.23 Internal risk management and quality assurance program; adverse incidents and reporting requirements.— (1) Every facility licensed under this part may, as part of its administrative functions, voluntarily establish a risk management and quality assurance program, the purpose of which is to assess resident care practices, facility incident reports, deficiencies cited by the agency, adverse incident reports, and resident grievances and develop plans of action to correct and respond quickly to identify quality differences. (2) Every facility licensed under this part is required to maintain adverse incident reports. For purposes of this section, the term, “adverse incident” means: (a) An event over which facility personnel could exercise control rather than as a result of the resident’s condition and results in: 1. Death; 2. Brain or spinal damage; 3. Permanent disfigurement; 4. Fracture or dislocation of bones or joints; 5. Any condition that required medical attention to which the resident has not given his or her consent, including failure to honor advanced directives; 6. Any condition that requires the transfer of the resident from the facility to a unit providing more acute care due to the incident rather than the resident’s condition before the incident; or 7. An event that is reported to law enforcement or its personnel for investigation; or (b) Resident elopement, if the elopement places the resident at risk of harm or injury. (3) Licensed facilities shall provide within 1 business day after the occurrence of an adverse incident, by electronic mail, facsimile, or United States mail, a preliminary report to the agency on all adverse incidents specified under this section. The report must include information regarding the identity of the affected resident, the type of adverse incident, and the status of the facility’s investigation of the incident. (4) Licensed facilities shall provide within 15 days, by electronic mail, facsimile, or United States mail, a full report to the agency on all adverse incidents specified in this section. The report must include the results of the facility’s investigation into the adverse incident. (5) Each facility shall report monthly to the agency any liability claim filed against it. The report must include the name of the resident, the dates of the incident leading to the claim, if applicable, and the type of injury or violation of rights alleged to have occurred. This report is not discoverable in any civil or administrative action, except in such actions brought by the agency to enforce the provisions of this part. (6) Abuse, neglect, or exploitation must be reported to the Department of Children and Family Services as required under chapter 415. (7) The information reported to the agency pursuant to subsection (3) which relates to persons licensed under chapter 458, chapter 459, chapter 461, chapter 464, or chapter 465 shall be reviewed by the agency. The agency shall determine whether any of the incidents potentially involved conduct by a health care professional who is subject to disciplinary action, in which case the provisions of s. 456.073 apply. The agency may investigate, as it deems appropriate, any such incident and prescribe measures that must or may be taken in response to the incident. The agency shall review each incident and determine whether it potentially involved conduct by a
27

Internal Risk Management and Quality Assurance Program and Adverse Incident Reporting Regulatory Authority
s. 429.23, F.S.; s. 58A-5, FAC; s. 59A-35, FAC 2014
health care professional who is subject to disciplinary action, in which case the provisions of s. 456.073 apply. (8) If the agency, through its receipt of the adverse incident reports prescribed in this part or through any investigation, has reasonable belief that conduct by a staff member or employee of a licensed facility is grounds for disciplinary action by the appropriate board, the agency shall report this fact to such regulatory board. (9) The adverse incident reports and preliminary adverse incident reports required under this section are confidential as provided by law and are not discoverable or admissible in any civil or administrative action, except in disciplinary proceedings by the agency or appropriate regulatory board. (10) The Department of Elderly Affairs may adopt rules necessary to administer this section.
Administrative Rule 58A-5.0241 Adverse Incident Report.
(1) INITIAL ADVERSE INCIDENT REPORT. The preliminary adverse incident report required by Section 429.23(3), F.S., must be submitted within one (1) business day after the incident on AHCA Form 3180-1024, Assisted Living Facility Initial Adverse Incident Report-1 Day, January 2006, and incorporated by reference. The form shall be submitted via electronic mail to [email protected]; on-line at http://ahca.myflorida.com/reporting/index.shtml; by facsimile to (850)922-2217; or by U.S. Mail to AHCA, Florida Center for Health Information and Policy Analysis, 2727 Mahan Drive, Mail Stop 16, Tallahassee, Florida 32308-5403, telephone (850)412-3731. AHCA Form 3180-1024 is available from the Florida Center for Health Information and Policy Analysis at the address stated above. The Initial Adverse Incident Report is in addition to, and does not replace, other reporting requirements specified in Florida Statutes.
(2) FULL ADVERSE INCIDENT REPORT. For each adverse incident reported under subsection (1) above, the facility shall submit a full report within fifteen (15) days of the incident. The full report shall be submitted on AHCA Form 3180-1025, Assisted Living Facility Full Adverse Incident Report-15 Day, dated January 2006, and incorporated by reference. The methods for obtaining and submitting the form are set forth in subsection (1) of this rule.
59A-35.110 Reporting Requirements; Electronic Submission.
(2) Electronic submission of information.
(a) The following required information must be reported through the Agency’s Internet site at http://www.ahca.myflorida.com/reporting/index.shtml:
2. Assisted living facilities:
a. Adverse incident reports required pursuant to Sections 429.23(3) and (4), F.S., and Rule 58A-5.0241, F.A.C.
(b) The licensee must retain the receipt issued from the Internet site indicating that their transaction was accepted.
(c) If the Agency’s Internet site is temporarily out of service, the required reports may be submitted by mail or facsimile as follows:
2. Adverse incident reports are sent to the Agency for Health Care Administration, Florida Center for Health Information and Policy Analysis, 2727 Mahan Drive, MS 16, Tallahassee, FL 32308 or facsimile to (850)922-2217.
28