Embed Size (px)
Citation preview

Fever of Unknown Origin-A Practical Approach
Dr.Murat AkovaHacettepe University School of MedicineSection of Infectious DiseasesAnkara, Turkey
ESCMID Online Lecture Library
© by author

Definitions•Classical FUO
– 3 w persisting fever, >38 ºC – >2 hospital visiting or 3 d in hospital evaluation
•Nosocomial FUO– Fever absent at admission and persisting in
hospital >3 d, >38 ºC
•Immundeficiency-related FUO– 3 d persisting fever, >38 ºC – Cultures negative at 48 h
•HIV-related FUO– Outpatient >3 w, in patient >3 d persisting fever,
>38 ºC– Confirmed HIV-positive patient
Infect Dis Clin N Am 2007;21:917
ESCMID Online Lecture Library
© by author

Causes of FUO 12 Centers, 154 Patients
Küçükardalı Y, et al. Int J Infect Dis 2008; 12: 71
ESCMID Online Lecture Library
© by author
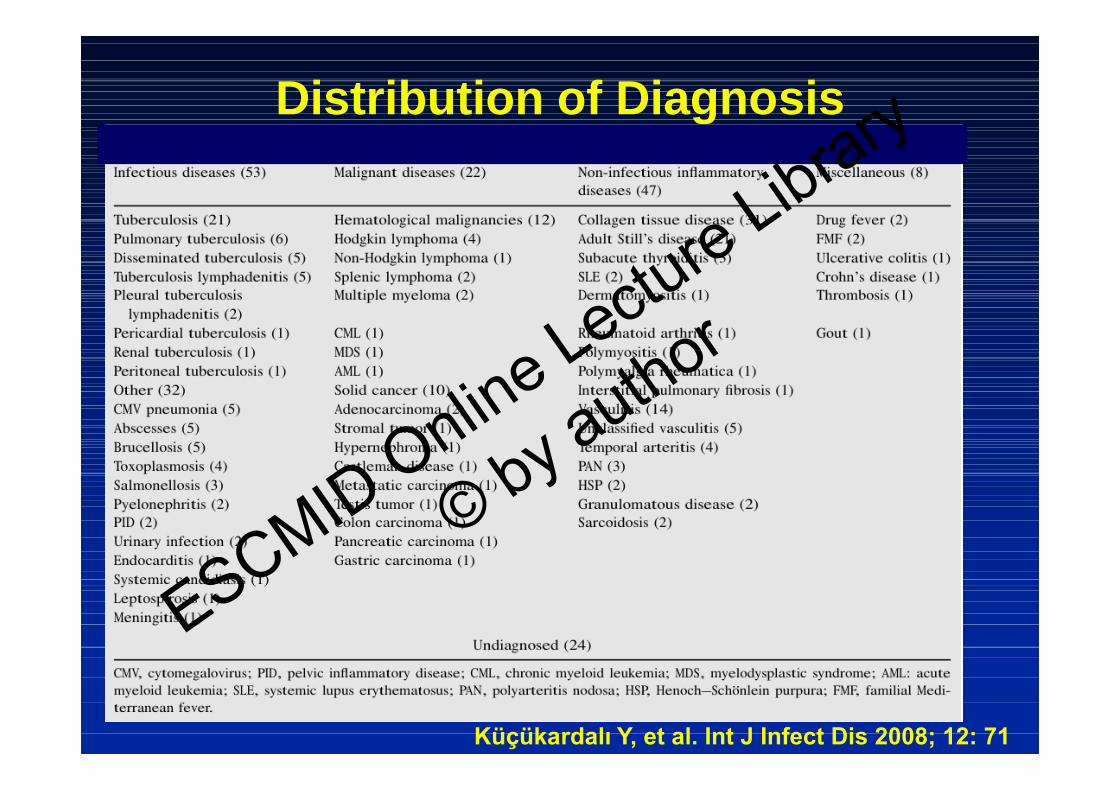
Distribution of Diagnosis
Küçükardalı Y, et al. Int J Infect Dis 2008; 12: 71
ESCMID Online Lecture Library
© by author

FUO in Elderly
•Collagen tissue diseases are more frequent–Polmyalgia rheumatica–Temporal arteritis
•Most frequent infectious diseases–Intraabdominal abscesses–Complicated UTI–Tuberculosis–Endocarditis
Clin Geriatr Med 2007;23:649
ESCMID Online Lecture Library
© by author
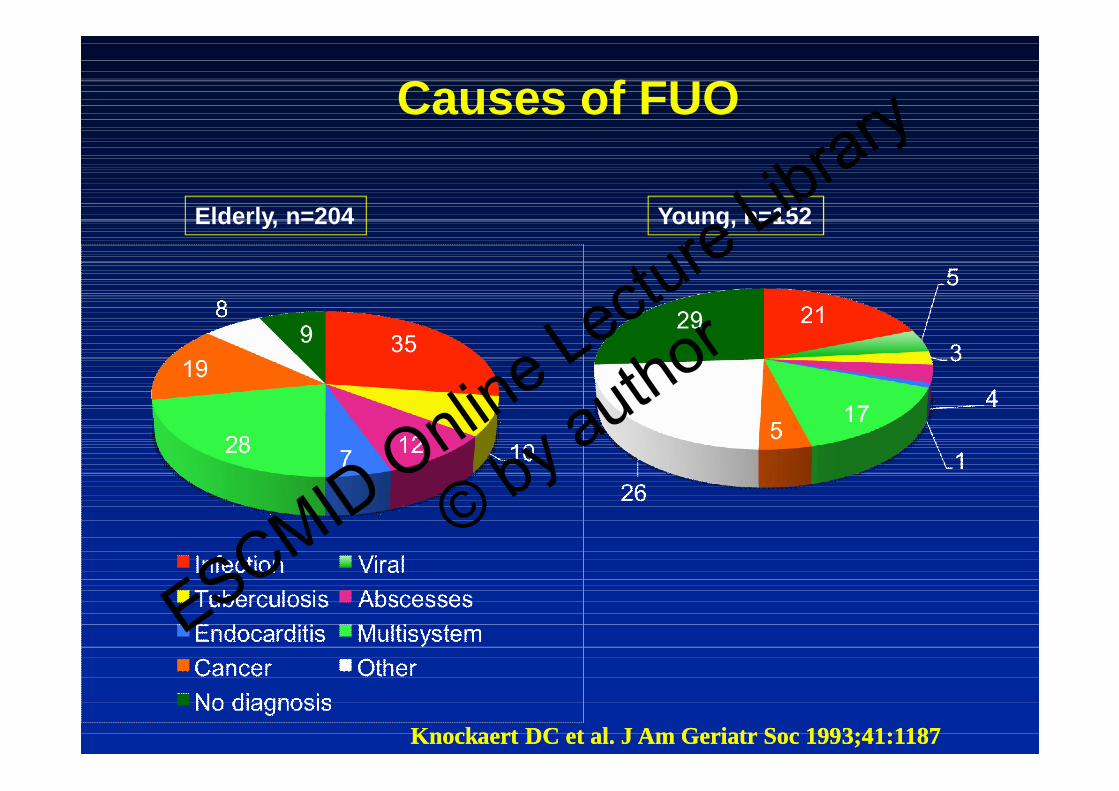
Causes of FUO
Elderly, n=204 Young, n=152
Knockaert DC et al. J Am Geriatr Soc 1993;41:1187Knockaert DC et al. J Am Geriatr Soc 1993;41:1187
ESCMID Online Lecture Library
© by author
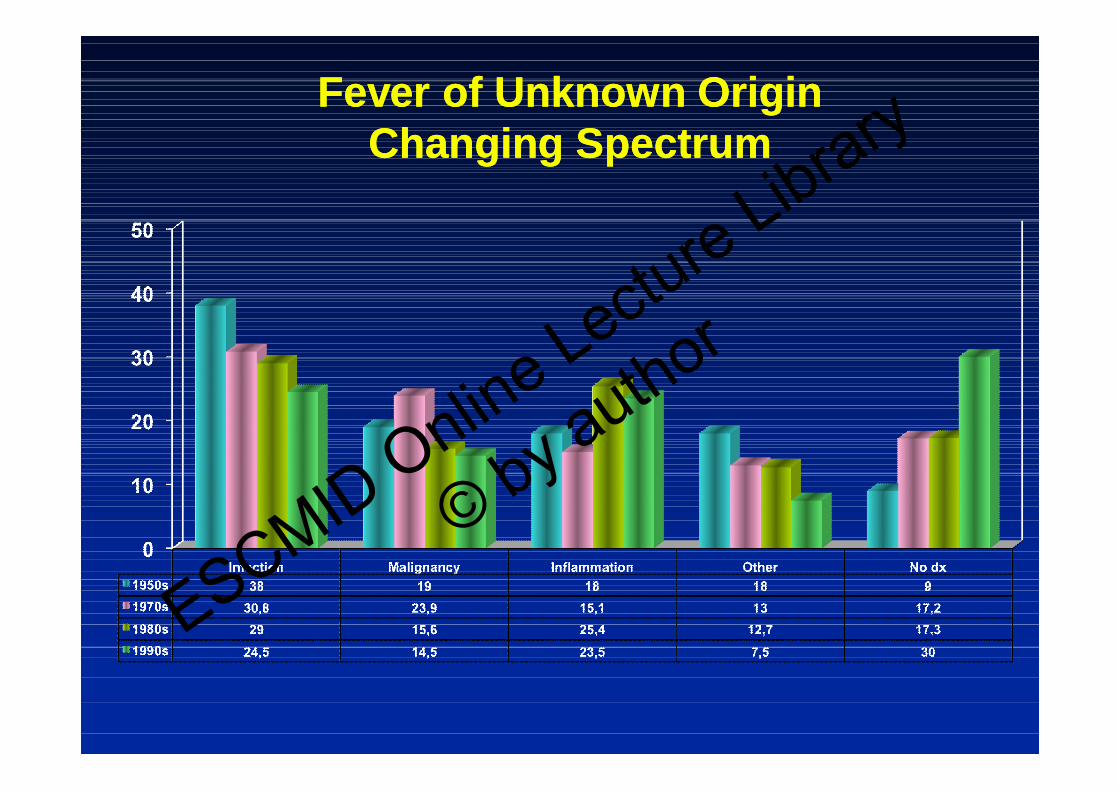
Fever of Unknown OriginFever of Unknown OriginChanging SpectrumChanging Spectrum
ESCMID Online Lecture Library
© by author

Rare and Emerging Causes of Rare and Emerging Causes of FUOFUO
•Babesiosis, Erlichiosis, Bartonellosis, Lyme disease
•Persistant Yersinia infection
•Parvovirus infections
•HHV-8
•Pneumocystis jirovecii infection
•Kikuchi necrotizing lymphaadenitis
•Inflammatory pseudotumor of lymph nodes
•Castleman disease
•Macrophage activation syndromeESCMID Online Lecture Library
© by author

•Schnitzler disease
•B12 vitamin deficiency
•Occult haematoma
•Aortic dissection
•Lineer IgA dermatosis
•Chronic fatigue syndrome
•Anticonvulsant hypersensitivity
•Minocycline hypersensitivity
Rare and Emerging Causes of Rare and Emerging Causes of FUOFUO
ESCMID Online Lecture Library
© by author

Hereditary Periodic Fever SyndromesHereditary Periodic Fever Syndromes
ESCMID Online Lecture Library
© by author
A Patient with Fever and Lymphadenopathy
•25 y, male, from an eastern city of Turkey
•Fever, >39 C, persisting >1 month
•Axiller lymphanedopathy
•Multiple skin nodules, some pustulating
•Patchy infiltration in both lungs ESCMID Online Lecture Library
© by author
Cont…
•He was given parenteral sulbactam-ampicillin in another hospital w no success
• Thoracoabdominal CT scan revelaed multiple abscesses in both liver and spleen and multiple noduler infiltration in both lungs
•Axillary lymph node biopsy reveals microabscesses with diffuse PMNL infiltration
ESCMID Online Lecture Library
© by author

Cont…
•The patient reports working in a horse farm–Several horses recently dying due to an
unknown disease
•Micro lab reports Burkholderia cepacia growing in the blood cultures
ESCMID Online Lecture Library
© by author

Cont…
•Upon being informed by the history of the patient Burkholderia mallei as confirmed in the cultures• Phenotypic testing
• 16S ribosomal RNA-gene sequencing
–He was given iv cefatzidim for two weeks, then po cipro for 6 months w complete recoveryESCMID Online Lectu
re Library
© by author
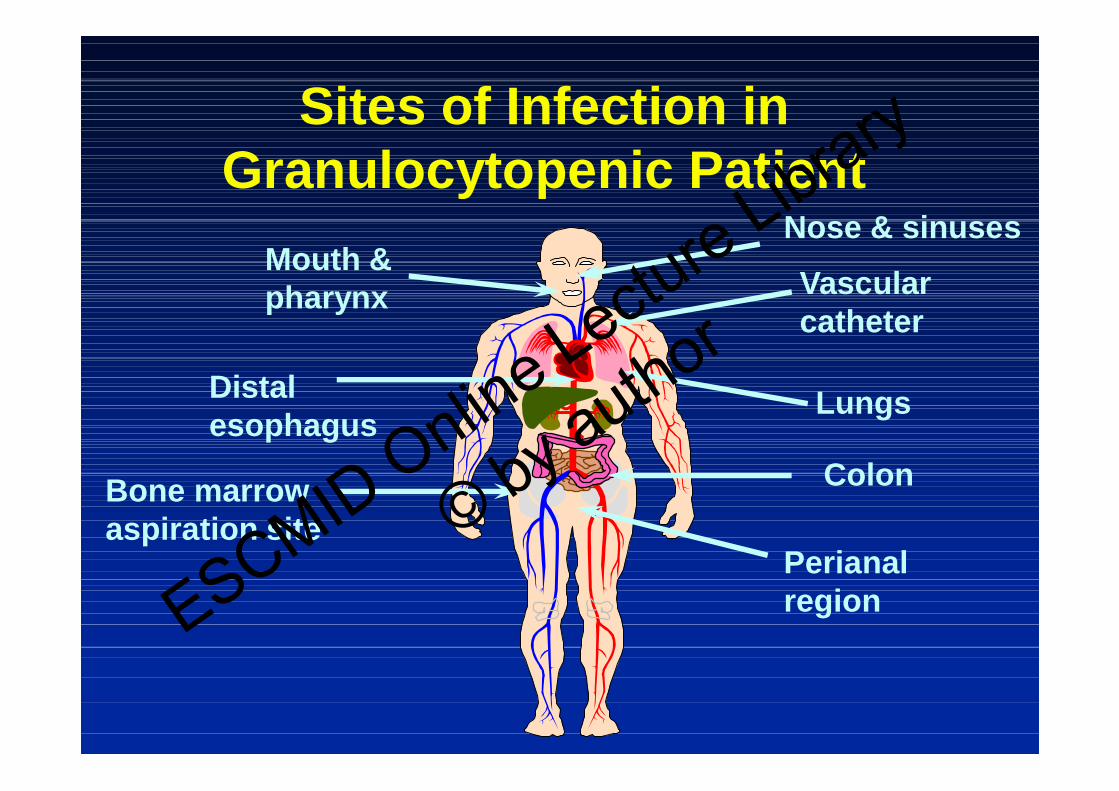
Sites of Infection in Granulocytopenic Patient
Mouth & pharynx Vascular
catheter
LungsDistalesophagus
Colon
Perianalregion
Bone marrowaspiration site
Nose & sinuses
ESCMID Online Lecture Library
© by author
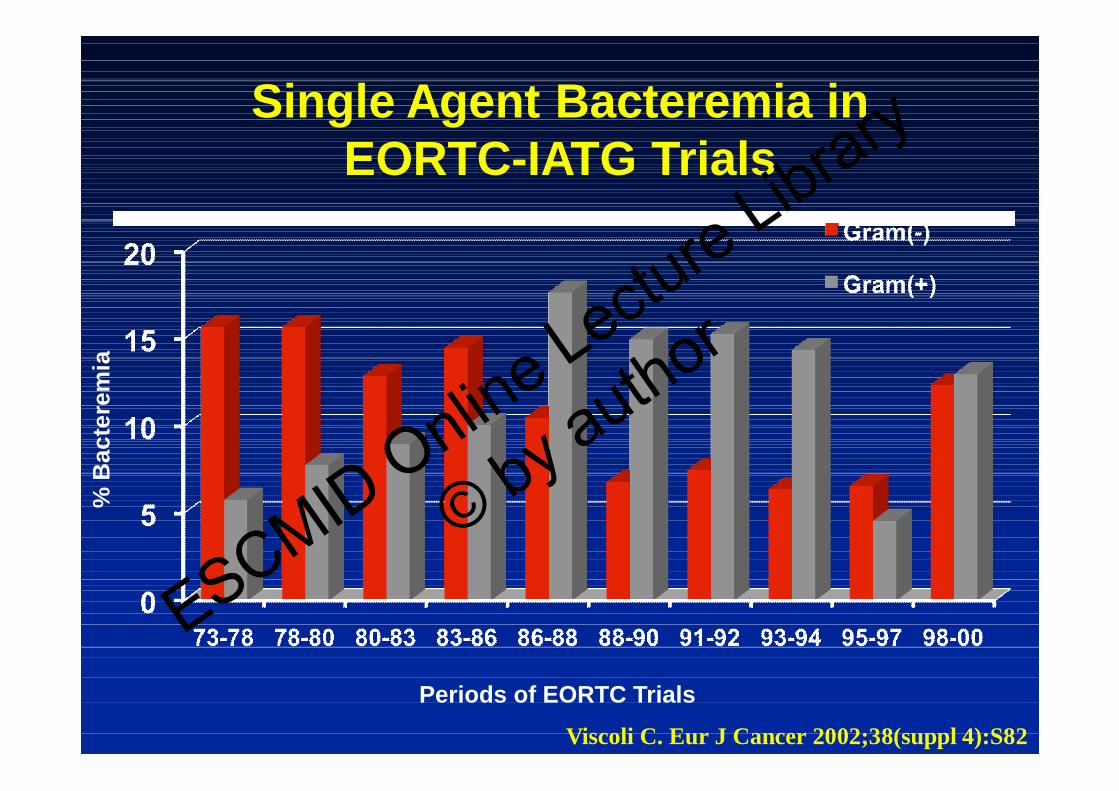
Single Agent Bacteremia in EORTC-IATG Trials
Periods of EORTC Trials
% B
ac
tere
mia
Viscoli C. Eur J Cancer 2002;38(suppl 4):S82
ESCMID Online Lecture Library
© by author

Distribution of BSI in 2652 Cancer Patients- SCOPE Project%
o
f p
atie
nts
Wisplinghoff, et al. Clin Infect Dis 2003;36:1103
* ** P<.001
ESCMID Online Lecture Library
© by author

Etiology of MicrobiologicallyDocumented Secondary Infections
Akova M, et al. Clin Infect Dis 2005;40:239
Microbiologically documentedInfections, n=50
Gram-positive bacteria,n=25
n=129 secondary inf.
ESCMID Online Lecture Library
© by author

Initial Empirical Approach
IDSA. Clin Infect Dis 2002;34:730
ESCMID Online Lecture Library
© by author

No Guidelines or Evidence-based Recommendations are Available for the
Management of FUO
ESCMID Online Lecture Library
© by author
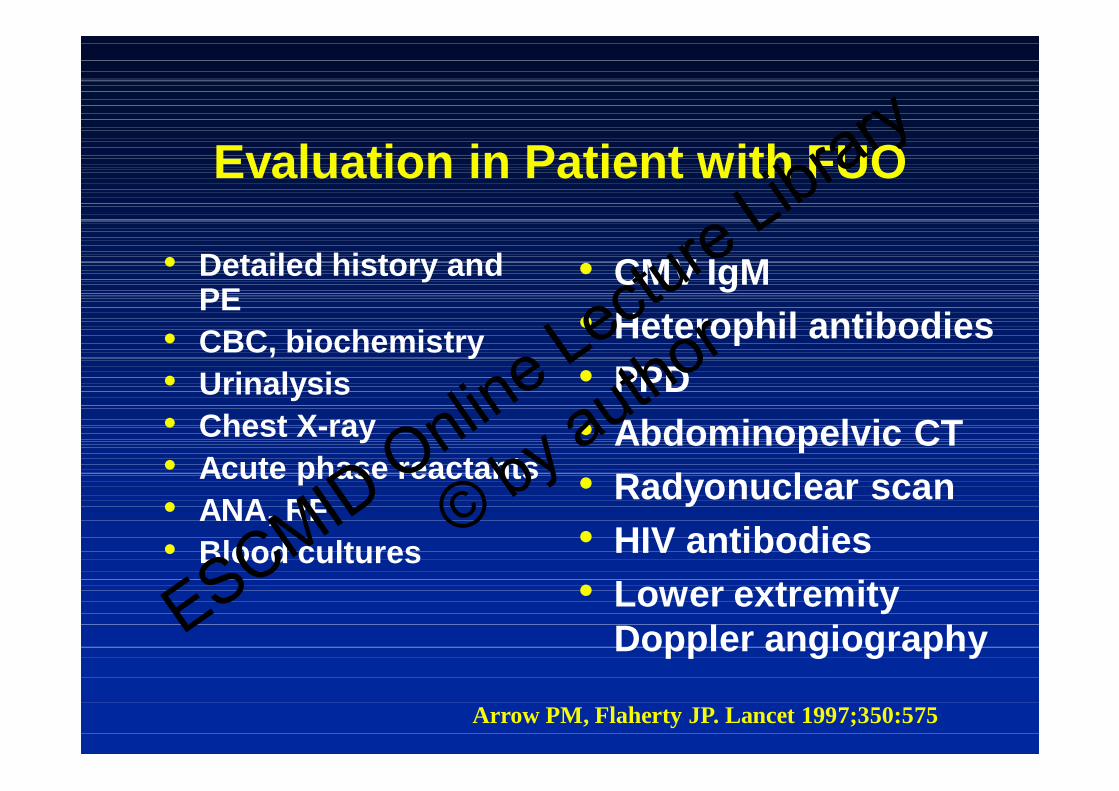
Evaluation in Patient with FUO
• Detailed history and PE
• CBC, biochemistry• Urinalysis• Chest X-ray• Acute phase reactants• ANA, RF• Blood cultures
•CMV IgM
•Heterophil antibodies
•PPD
•Abdominopelvic CT
•Radyonuclear scan
•HIV antibodies
•Lower extremity Doppler angiography
Arrow PM, Flaherty JP. Lancet 1997;350:575
ESCMID Online Lecture Library
© by author

Tests for Which Evidence ExistsTests for Which Evidence Exists
••Abdominal CTAbdominal CT
••Nuclear imagingNuclear imaging
••Duke criteriaDuke criteria
••Liver biopsyLiver biopsy
••Temporal arterial biopsyTemporal arterial biopsy
••Lower extremity Doppler Lower extremity Doppler
ultrasound imagingultrasound imaging
ESCMID Online Lecture Library
© by author

Nuclear ImagingNuclear Imaging
TcTc--based tests(99mbased tests(99m--Tc BW Tc BW 250/183) 250/183)
Sensitivity Specificity
9393--94%94% 4040--7575%%
Indium 111 IgGIndium 111 IgGIndium 111Indium 111--labeled leucocyteslabeled leucocytes 4545--82%82% 69-86%
GaGa--67 scintigraphy67 scintigraphy 67%67% 78%78%
Fluodeoxyglucose PETFluodeoxyglucose PET 84%84% 86%86%
Semin Nucl Med 2009;39:81-87
ESCMID Online Lecture Library
© by author

Liver BiopsyLiver Biopsy
Diagnostic yield in FUO 14Diagnostic yield in FUO 14--17%17%
No correlation with No correlation with hepatomegaly or alterations in hepatomegaly or alterations in liver function testsliver function tests
Complication:Complication: 0.0670.067--0.32 %0.32 %Mortality: Mortality: 0.0090.009--0.12 %0.12 %ESCMID Online Lectu
re Library
© by author

TTeemporal Arterial Biopsymporal Arterial Biopsy
Incidence in FUO 16Incidence in FUO 16--17%17%
Complications are rare (facial nerve paralysis, skin necrosis)
Temporal arterial duplex ultrasonographyTemporal arterial duplex ultrasonography
HaloStenosisOcclusion
SSensitivity and specificity 93%ensitivity and specificity 93%ESCMID Online Lecture Library
© by author
Prognosis in FUO
•Variable depending on the cause of FUO– Worse in elderly and patients with malignancy
•Delay in diagnosis is related with worse outcome– Intraabdominal infection– Miliary tuberculosis– Disseminated fungal infection– Recurrant pulmoner emboli
•Fever subsides within >4 weeks w/o sequela in patients w/o a diagnosis– 5-year mortality 3.2%ESCMID Online Lectu
re Library
© by author

1st Evaluation
>>3 w fever3 w fever
FUOFUO
Stop all medications
>>72 h persisting fever72 h persisting fever
Documentation of fever
<<72 h defervescence72 h defervescence
Drug feverDrug fever
Diagnostic AlgorithmDiagnostic Algorithm
ESCMID Online Lecture Library
© by author
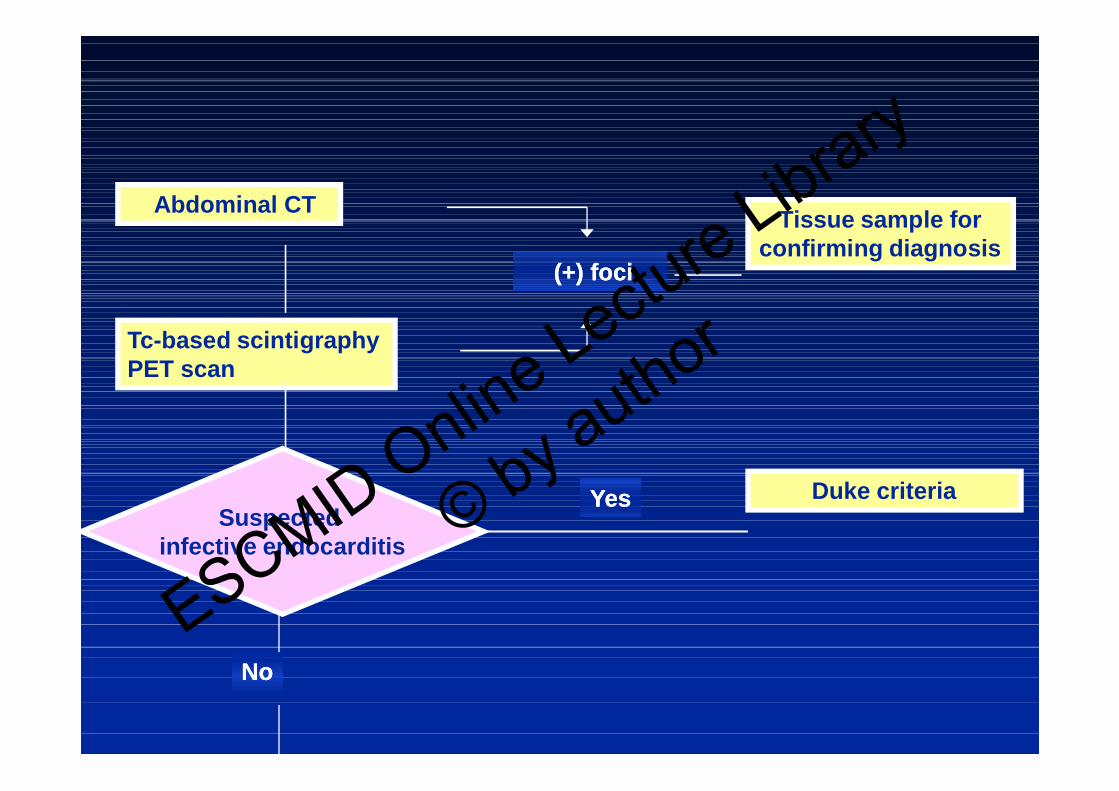
Abdominal CT
Tc-based scintigraphyPET scan
(+) foci(+) foci
Tissue sample for confirming diagnosis
YesYes Duke criteria
NoNo
Suspected infective endocarditis
ESCMID Online Lecture Library
© by author

Lower extremityDoppler
DVT (+)DVT (+)
LMWHLMWH
Fever persistsFever persists
YesYesTemporal arterybiopsy
NoNo
Liverbiopsy
LaparoscopyUndiagnosed FUOUndiagnosed FUOClinical
follow-up
Age >50
Clinicaldeterioration?
NoNo
YesYes
ESCMID Online Lecture Library
© by author
••The most frequent cause are infectionsThe most frequent cause are infections
••>200 causes have been desccribed in the >200 causes have been desccribed in the literatureliterature
••80% of patients can be diagnosed within 3 80% of patients can be diagnosed within 3 weeksweeks
••Clinical evaluation guides complex diagnostic Clinical evaluation guides complex diagnostic toolstools
ConclusionsConclusions--11
ESCMID Online Lecture Library
© by author

Conlusions-2
••Unjustified, blind diagnostic tools are Unjustified, blind diagnostic tools are ineffective and expose patients to ineffective and expose patients to unnecessary invasive proceduresunnecessary invasive procedures
••Mortality at the 1st year is highMortality at the 1st year is high
••LongLong--term prognosis are favorable in term prognosis are favorable in patients with an undiagnosed cause patients with an undiagnosed cause of FUOof FUOESCMID Online Lectu
re Library
© by author


![Fever of unknown origin (FUO): which are the factors influencing … · 2018. 3. 15. · Fever of unknown origin (FUO) was originally defined by Petersdorf and Beeson [1]asanillnessofmore](https://img.pdfslide.us/doc/110x75/60fe895bfa0f251e835ba0b5/fever-of-unknown-origin-fuo-which-are-the-factors-influencing-2018-3-15.jpg)