Embed Size (px)
DESCRIPTION
Fever and Rash. Dr. Orli Megged Infectious Diseases Unit Shaare Zedek Medical Center. How do you describe this rash?. Multiple erythematous macules and/or papules, a few millimeters to 1 cm in size. Symmetric distribution on trunk and extremities. Dermatologic Terminology. Macule Papule - PowerPoint PPT Presentation
Citation preview

Fever and Rash
Dr. Orli MeggedInfectious Diseases Unit
Shaare Zedek Medical Center


How do you describe this rash?
Multiple erythematous macules and/or papules, a few millimeters to 1 cm in size.Symmetric distribution on trunk and extremities

Dermatologic Terminology
• Macule• Papule• Nodule• Vesicle• Bulla• Pustule• Petechia• Purpura• Ecchymoses• Erythroderma

Macule
Flat, nonpalpable circumscribed area of change in the skin color, may be any size.

Papule
Solid raised skin lesion with a distinct borders, generally < 5 mm in diameter.

Nodule
Palpable, solid, round, or ellipsoidal lesion > 5 mm diameter

Vesicle (blister)
Circumscribed, elevated lesion that is < 5 mm in diameter containing serous (clear) fluid.

Bulla
A vesicle with a diameter > 5 mm.

Pustule
Superficial, elevated lesion that contains pus.

Petechia
A small (1-2mm) red or purple discolorations on the skin, caused by a minor hemorrhage (do not blanch on applying pressure)
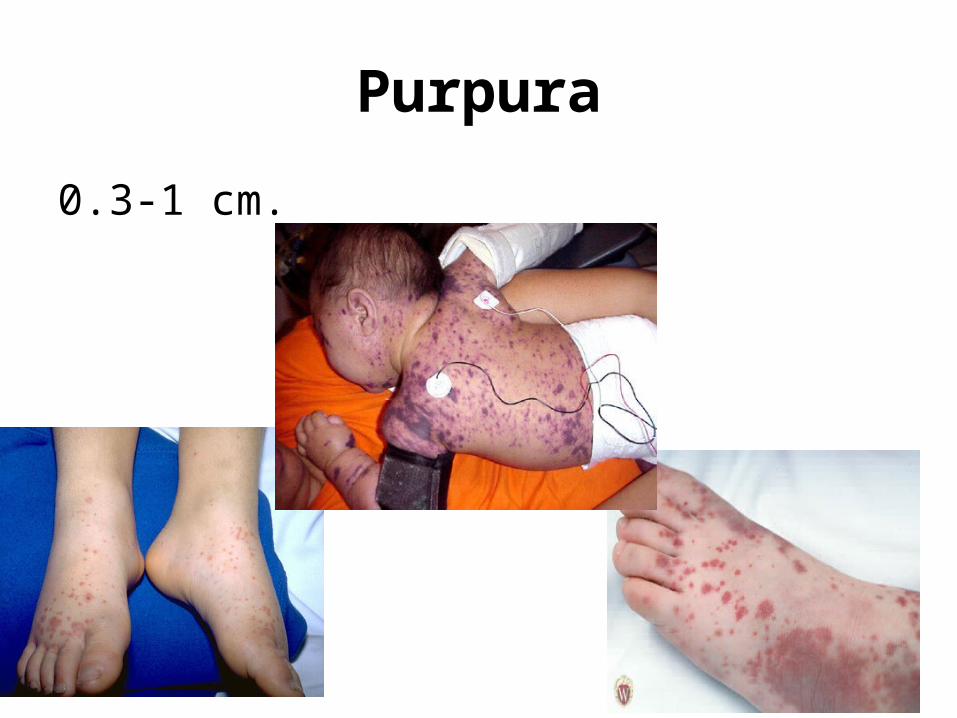
Purpura
0.3-1 cm.

Ecchymoses
Greater than 1 cm.

Erythroderma
Erythema that affects nearly the entire cutaneous surface (“red man”)

Describing rash• Color• Margination• Shape• Palpation• Number• Arrangement - Generalized,
Symmetric, Flexural, Extensor, Palmoplantar, Photo-distributed
• Confluence

Asking the right questions
• Site of onset, rate & direction of spread.• Distribution, configuration and arrangement of the
lesion?• Is there erythema, hypo, or hyperpigmentation?• Are there secondary characteristics such as scale?• Is pruritus present?• Is the patient taking any meds (prescription, OTC,
herbal)• Travel History?• Immune Status?

How would you describe this rash?

DD bullous rash
• Viral• Bacterial• Drugs• Allergic Contact Dermatitis• Autoimmune blistering diseases
of the skin• ….

Hand foot and mouth (Coxsackie)

Varicella

Varicella – Chicken Pox
Varicella Zoster Virus• Incubation period: 10 – 21 days• Infectious: 2d prior to rash – 5d after• Vaccinations – live attenuated:
– Varilrix– MMRV

Herpes Zoster

DD bullous rash
• Bacterial

(Staphylococcal) Bullous Impetigo


Metronidazole Induced Bullous Fixed Drug
Eruptions

Contact dermatitis

How would you describe this rash?

DD petechial/pupuric rash
•Meningococcal disease
•Rickettsial infection
•Endocarditis
•Sepsis
•Viral (enterovirus)
•Viral hemorrhagic fevers
•“Noninfectious” TTP, HSP, vasculitis, etc.

Meningococcemia

Meningococcemia
• Neisseria meningitidis• Gram-negative diplococci• Strains are grouped based on a
polysaccharide capsule• A, B, C, Y and W135

Meningococcemia
• Petechial rash
• With or without meningitis
• Case fatality rate is between 8-15%

Rickettsia Conorii
• Intracellular, slow-growing gram-negative bacterium
• Mediterranean spotted fever (MSF)• Common dog tick is the vector in the
Mediterranean.

Spotted fever
• Incubation 2-14 days, median 7 days• Fever, myalgia, headache, GI• Rash - typically begins around the
wrists and ankles. • Involvement of the palms and soles -
characteristic

Rickettsia Conorii

Endocarditis – Splinter, Osler, Janeway

Enterovirus

Henoch–Schönlein purpura

HSP
• Systemic vasulitis, palpable purpura
• Deposition of immune complexes containing IgA
• Mainly in children• Symptoms: joint &
abdominal pain• Complications: irreversible
kidney damage

How would you describe this rash?

DD: Maculo Papular rash• Viral
• Bacterial
• Other Infections: Secondary Syphilis, Lyme
• Kawasaki’s
• Drugs
• Rheum: SLE, Reiter’s Syndrome

Viral
• Measles• Rubella• Parvo• EBV• CMV• HHV6• Adeno• Entero• WNF

Bacterial
• Strep pyogenes (Scarlet Fever) • Staph aureus (TSS) • Meningococcemia • Spotted fever

Cases
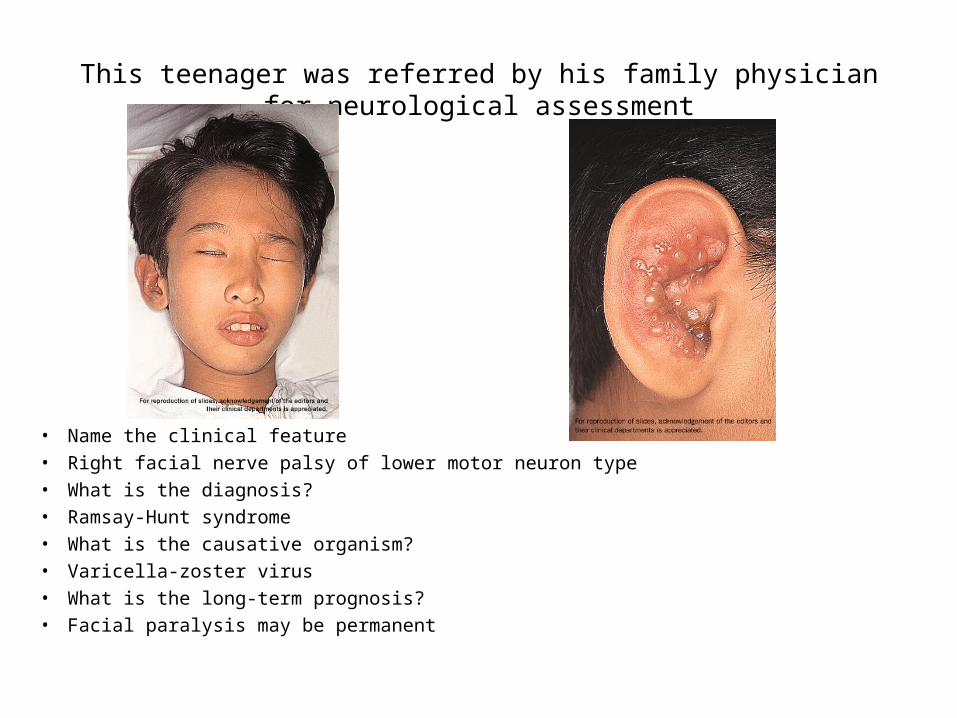
This teenager was referred by his family physician for neurological assessment
• Name the clinical feature• Right facial nerve palsy of lower motor neuron type• What is the diagnosis?• Ramsay-Hunt syndrome• What is the causative organism?• Varicella-zoster virus• What is the long-term prognosis?• Facial paralysis may be permanent

A 12-year-old epileptic boy, developed fever, dry cough and tachypnoea. He was seen by a family physician, who
prescribed symptomatic treatment and a course of antibiotics. A generalized skin rash appeared 2 days afterwards
What is the clinical feature?Erythema multiforme What are the possible etiologies?- Drugs e.g. carbamazepine, phenobarbitone- Infections e.g. herpes simplex, mycoplasma or streptococcus- Idiopathic

Several pupils of a kindergarten were seen because of acute onset of fever, itchy skin lesions at the extremities and sore
throat.
• Name the diagnosis• Hand, foot and mouth disease• What is the most likely causative organism?• Usually Coxsackievirus A16 or Enterovirus 71• Complications?• Aseptic meningitis. Enterovirus 71 may cause
meningoencephalitis or polio-like acute flaccid paralysis

6-month-old infant with vesicular skin lesions, distributed on the area corresponding to the L3 dermatome.
• What is the diagnosis? • Herpes zoster• The infant did not have a history of chickenpox before. What further information
would you ask?• Maternal chickenpox during pregnancy• What is the prognosis?• Possible recurrent herpes zoster during infancy

• A 2-year-old child with fever, vomiting, diarrhea, conjunctival injection and rapidly spreading generalized erythema . The BP was not recordable. He developed acute renal failure and ARDS.

• What is the clinical feature of the face and trunk?
• Erythroderma• What is your presumptive diagnosis?• Toxic shock syndrome• What is the likely causative organism?• Staphylococcus aureus, Streptococcus
pyogenes• What is the current proposed
pathogenesis of the condition?• T cell activation by toxins behaving as
superantigens, TSST-1

• What physical sign would you expect when the child recovers?
• Cutaneous desquamation usually at the extremities but can be generalized.
• What are the risk factors for recurrence?• Tampons

• A 1y old girl was hospitalized because of 2 days of fever 40oC, and a perineal rash. 1 day later she developed a bilateral conjunctival injection. There was also cough and rhinorrhoea.
• Non-pitting edema of the distal extremities were alse noted. On the fourth day of illness, there was intense redness of the lips.

• A diffuse erythematous maculopapular rash began to appear on the face and then spread to involve the trunk and the limbs over the next 2 days.
• At the same time, a tender firm swelling developed at the right upper cervical region.

List four differential diagnosis1. Kawasaki disease2. Measles3. Scarlet fever4. Stevens-Johnson syndrome
She was treated with oral aspirin and IVIG.

• What advice should be given to the patient if she required long-term aspirin?
• There is a risk of Reye syndrome if the patient developed varicella or influenza.
• Recommend immunization with influenza vaccine.• Recommend immunization with varicella vaccine. Aspirin
should be temporarily discontinued for 6 weeks following immunization. IVIG might interfere with the development of vaccine-induced immunity.
• She should be advised to discontinue aspirin during the incubation period following a significant exposure to varicella, as well as throughout the duration of varicella. The antiplatelet agent can be replaced by dipyridamole.

The end…..

![SerologicalEvidenceof Rickettsia ExposureamongPatientswith ...downloads.hindawi.com/journals/ipid/2020/4905783.pdf · Rickettsia infection includes fever, eschar, and rash [6]; however,](https://img.pdfslide.us/doc/110x75/604d43e7c243f216ab359e57/serologicalevidenceof-rickettsia-exposureamongpatientswith-rickettsia-infection.jpg)