Embed Size (px)
Citation preview

Fetal and neonatal physiology
The endocrine regulation of growth
89,90

Hormone secretion of the fetus
Maternal steroid hormones and thyroid hormones cross the placenta.
Pancreas: Insulin/Glucagon (8th week) Diabetes mellitus of the mother!
Thyroid hormones: (10th week) Cretinism!
Adrenal cortex: (16th week) Androgens
Cortisol Surfactant
Testis: (8th week) Testosterone, Müllerian duct regression factor
Makrosomie (over 5 kg birth weight)

Fetal circulation
HbF (α2γ2)
HbF exhibits a low affinity
for 2,3-DPG
+
Higher Hb concentration
Botalli
Arantii
vascular resistance is high in the lung
(hypoxic pulmonary vasoconstriction)
Umbilical
vein
Umbilical
arteries
upper part
of the body
lower part
of the body
right
ventricle
gut
O2 saturation (%)
% of cardiac output
liver
Placenta

Breathing
1) increase in the surface area available for gas exchange
2) fall in pulmonary vascular resistance
ad 1) Amniotic fluid is pressed out by the birth process.
Mild hypoxia and hypercapnia, as well as cold skin trigger the first breath.
Amniotic fluid is absorbed from the respiratory system (reabsorption of Na+ and water).
+Surfactant production
Perfusing its body by breathing independently instead of utilizing placental
oxygen is the first challenge of a newborn.
ad 2) Breathing increases pO2 in the lung, that dilates pulmonary blood vessels.
Local release of endothelial prostacyclin and NO.

At birth removal of the placental
circulation increases systemic
vascular resistance, whereas
pulmonary expansion decreases
pulmonary vascular resistance.
At birth left atrial pressure begins
to exceed the right atrial pressure,
causing the foramen ovale to
close.
Closure of the ductus arteriosus
completes the separation between
pulmonary and systemic
circulation (reduced prostaglandin
E2 levels).
Changes in the circulation at and around birth
before birth after birth
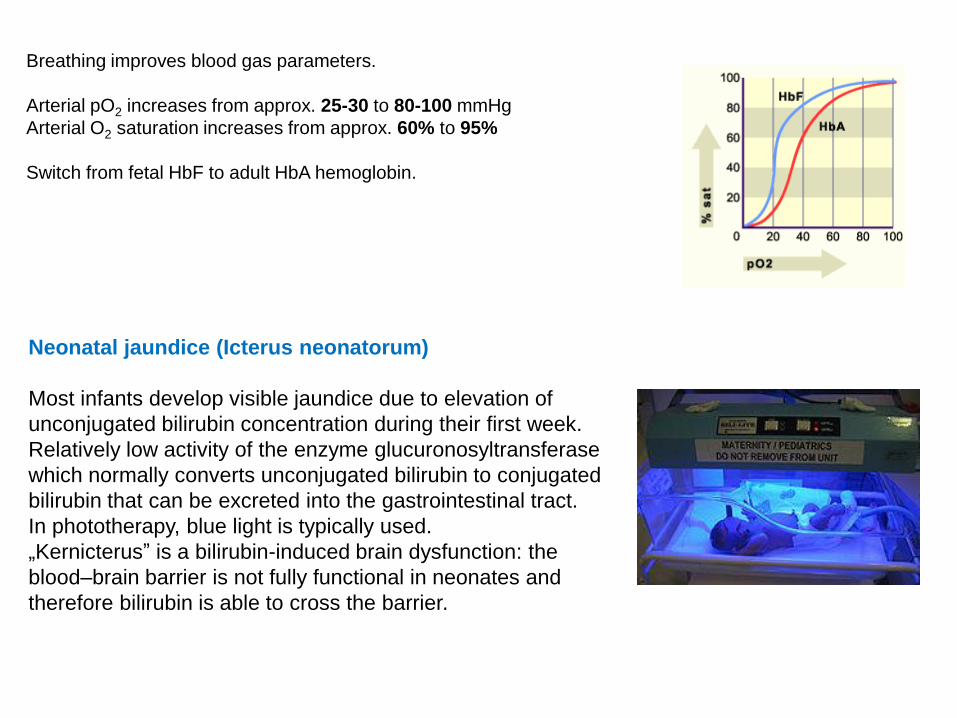
Breathing improves blood gas parameters.
Arterial pO2 increases from approx. 25-30 to 80-100 mmHg
Arterial O2 saturation increases from approx. 60% to 95%
Switch from fetal HbF to adult HbA hemoglobin.
Neonatal jaundice (Icterus neonatorum)
Most infants develop visible jaundice due to elevation of
unconjugated bilirubin concentration during their first week.
Relatively low activity of the enzyme glucuronosyltransferase
which normally converts unconjugated bilirubin to conjugated
bilirubin that can be excreted into the gastrointestinal tract.
In phototherapy, blue light is typically used.
„Kernicterus” is a bilirubin-induced brain dysfunction: the
blood–brain barrier is not fully functional in neonates and
therefore bilirubin is able to cross the barrier.

Regulation of growth Fertilized egg adult person
Hyperplasia: increase in number of cells
Hypertrophy: enlargement of cells
+ Differentiation
Intrauterine growth: (approx. 50 cm)
Genetic information
Maternal environment (nutrition, drugs, alcohol)
Metabolic (eg. diabetes mellitus of the mother)
Hormones
Insulin
Insulin-like growth factor-2 (IGF-2)
Human placental lactogen
(Thyroid hormones)
Extrauterine growth:
Growth hormone
Insulin-like growth factor-1 (IGF-1)
Androgens, estrogens
Hormones regulating Ca++ (Parathormone, Calcitonin, Calcitriol)
Thyroid hormones (GH synthesis )
Glucocorticoids (oversecretion inhibits normal growth)
Cretinism

Growth factors
1) Increasing cell mass by stimulating the production and/or inhibiting the
degradation of macromolecules
2) Increasing cell number by stimulating the rate of cell division, referred to as
mitogenic activity
3) Increasing cell number through increased cell survival due to inhibition of
apoptosis
Epidermal growth factor
Fibroblast growth factor
Platelet derived growth factor
Insulin-like growth factors
Nerve growth factor

Growth hormone receptor signalling pathways.
Reprinted from TRENDS in Endocrinology and Metabolism 12(6), J. Herrington and C. Carter-Su, Signaling
pathways activated by the growth hormone receptor, 252-257, 2001, with permission from Elsevier,
The activated JAK2 molecule
phosphorylates itself and the
cytoplasmic domain of the GH
receptor on tyrosine residues.
These phosphotyrosines form
binding sites for signaling
proteins.
Growth hormone receptor
Growth hormone (GH)
Janus
Homology between GH, prolactin and hPL
Secreted in the acidophilic cells (40 % of the anterior pituitary)
Phosphorylation
+
New protein synthesis

Growth hormone
Polypeptide (191 amino acids)
Effects:
Metabolic effects
Protein metabolism: synthesis of proteins (anabolic effect)
Fat metabolism: mobilization of stored fat (lipolysis)
Carbohydrate metabolism:
„anti-insulin” effect:
decreased insulin sensitivity of cells
decreased glucose uptake into some tissues
increased hepatic glucose output
Growth promoting effect
Liver (muscle, kidney etc.):
secretion of somatomedins (Insulin-like growth factors)
„insulin-like” activity
increased glucose uptake
increased protein synthesis
stimulated chondrocyte proliferation
doping

Somatomedin - Insulin-like growth factor
Insulin-like growth factor-1 (IGF-1) Insulin-like growth factor-2 (IGF-2)
Polypeptide
It is secreted by the liver and other tissues in response to stimulation by growth
hormone.
While GH appears to be the main regulator of the IGF-1 gene, control over the IGF-2 gene is less clear.
(IGF-2 regulates growth of the fetus before birth.)
liver
pre-pro-IGF-1
pre-pro-IGF-2

Growth hormone-releasing hormone
Growth hormone-
inhibiting hormone
epiphyseal
growth
Liver
Lipolysis
Glykogenolysis
Protein synthesis
glucose
amino acids
free fatty acids
GHRH
Inheritance,
exercise, sleep, stress
Estrogens
Androgens
Growth hormone
stomach
hours
GH
GHRH
Somatostatin
10 p.m. 10 a.m.
T3, T4

Overproduction of growth hormone
Childhood:
Gigantism
Adulthood:
Acromegaly
Growth hormone deficiency
Childhood:
Dwarfism (proportional)
Adulthood:
metabolic symptoms
17.09.2009. Guinness World Record
8.2. 2011. 251 cm

Enlargement of hands and feet (increase in ring size
and shoe size)
Increased prominence of jaw and/or forehead
Thickened skin
Hyperglycemia
(Stimulation of prolactin receptors)
overuse of growth hormone

Laron-dwarfs

Pygmy is a term used for various ethnic groups whose average height is unusually
short; adult men grow to less than 150 cm in average height.
Pygmy peoples

Growth percentile chart is to compare a child’s weight and
height percentile to the average child

Extracted growth hormone was used
since late 1950s until late 1980s when
its use was replaced by recombinant
GH.
Growth Hormone therapy
beginning
of the therapy
7 11 years

























