Embed Size (px)
Citation preview
Fertility Preservation Practices Among Ontario Oncologists
Samantha Yee & Esme Fuller-Thomson & Angela Lau &
Ellen M. Greenblatt
Published online: 11 January 2012# Springer Science+Business Media, LLC 2012
Abstract This study explores the attitudes, knowledge, andreferring behaviors in fertility preservation among Ontariophysicians providing adult cancer care. Ontario physicianswith specialties in medical oncology, radiation oncology,gynaecologic oncology, and urology were invited to com-plete a 48-item questionnaire. A total of 152 questionnaireswere available for analysis with a response rate of 23.7%.Seventy-four percent of the physicians indicated that theyrarely or never modified cancer treatment due to concernabout future fertility. Differences were found in fertilitypreservation knowledge among respondents in differentmedical specialties (p<0.01) and clinical settings (p<
0.05). The frequency of initiating a referral was stronglyassociated with knowing where to refer patients (p<0.001).The odds of knowing where to refer cancer patients washigher for physicians who work in a teaching hospital (p<0.01) and a cancer centre (p<0.01) compared with thosewho primarily work in a community setting. About 45% didnot know where to refer female patients, and 69.7% rarelyever made a fertility preservation consultation referral fortheir female patients. The majority of respondents had pos-itive attitudes despite their lack of current knowledge incryopreservation services and fertility preservation optionsthrough assisted reproductive technologies. Our findingsprovide further insights of the relevance of consideringphysicians’ medical backgrounds and practice settings whendesigning training modules to raise their awareness in fer-tility preservation issues.
Keywords Oncology . Fertility preservation . Oncologists .
Cancer patients . Assisted reproductive technology
Introduction
The incidence rates of cancer are rising in Canada. CanadianCancer Society estimates that in 2011, over 93,000 men and84,000 women were newly diagnosed with cancer, includ-ing over 2,500 men and 4,200 women are in their reproduc-tive years (age range, 20–39) [1]. Medical advances indiagnostic techniques and cancer treatment have greatlyimproved the survival chance of cancer patients, whichmeans more cancer patients are able to survive cancer andlive a productive life following treatment.
Unfortunately, malignancy of some cancer types, andcancer therapy such as surgery, chemotherapy, and radiationmay pose significant threats to fertility. Some cancer
J Canc Educ (2012) 27:362–368DOI 10.1007/s13187-011-0301-4
S. Yee (*) : E. M. GreenblattCenter for Fertility and Reproductive Health,Mount Sinai Hospital,250 Dundas Street West, Suite 700,Toronto, Ontario M5T 2Z5, Canadae-mail: [email protected]
E. M. Greenblatte-mail: [email protected]
S. Yee : E. Fuller-ThomsonFactor-Inwentash Faculty of Social Work, University of Toronto,Toronto, Ontario, Canada
E. Fuller-Thomsone-mail: [email protected]
E. M. GreenblattDepartment of Obstetrics and Gynaecology, University of Toronto,Toronto, Ontario, Canada
A. LauDepartment of Physiology, Faculty of Medicine,University of Toronto,Toronto, Ontario, Canada
A. Laue-mail: [email protected]

patients never regain full reproductive potential [2, 3]. Al-though fertility is of great concern to many reproductive-aged cancer patients who have not yet started or completedtheir family at the time of cancer diagnosis, retrospectivestudies on cancer survivors have found that the majority donot recall having fertility discussions with their oncologists[4–6]. This suggests that patients are not routinely informedabout the potential fertility risks and available fertility pres-ervation (FP) options when receiving cancer care [7–11, 13].
The underutilization of FP services is highly associatedwith the absences of FP discussion and referrals by manyphysicians [7–12]. Studies conducted in the USA suggestthat oncologists selectively inform cancer patients about thepotential fertility risks based on certain patient demograph-ics and characteristics [8–10]. However, Canadian researchdata are very limited. Only a few psychosocial researchpapers have explored cancer survivors’ and health careproviders’ perspectives on oncology sperm banking[14–16]. Besides, quantitative data related to Canadianphysicians’ perspectives on FP are not available. Little isknown if Canadian physicians also share similar attitudesand practice behaviors with regard to FP as suggested by theexisting research literature conducted in the USA. Extrapo-lation to the Canadian setting of research data collected inother countries could be problematic due to differences inhealth care delivery models and health care philosophies.The purpose of this pilot survey was to assess the attitudes,knowledge, and practice behaviors in FP among physiciansproviding adult cancer care in Ontario, Canada.
Materials and Methods
A questionnaire was constructed based on clinical experi-ences, a comprehensive literature review, and related surveyquestionnaires available in published literature [8–10, 17,18]. Five oncologists and two urologists reviewed the ques-tionnaire to provide feedback for face and content validity.Several revisions were made until consensus was reached.The final questionnaire included 48 questions tailored to thedomains of knowledge, attitudes, and practice behaviors inoncology FP.
Research ethics approval was obtained from Mount SinaiHospital’s Research Ethics Board prior to data collection.The sampling frame included Ontario physicians in fourmedical specialties: radiation oncology, medical oncology,gynaecologic oncology, and urology. Urologists were in-cluded because they are the physician group most likely tomanage testicular or prostate cancer. A list of 27 gynaeco-logic oncologists was identified from another source.1 Anonline directory search was conducted in August 2009 of the
College of Physicians and Surgeons of Ontario’s website(CPSO, www.cpso.on.ca), which has the contact informa-tion of all physicians who are licensed to practice in Ontario.A total of 641 physicians met the inclusion criteria. Sur-geons were not included in the sampling frame because theCPSO directory does not identify the subspecialty of surgi-cal oncology. The first research package was mailed inOctober 2009, followed by a second mailing in January2010 to nonrespondents. A general FP brochure was includ-ed in the first mailing to give the prospective subjects ageneral introduction of the research topic.
A total of 38 physicians were unable to be reached bymail for various reasons, including incorrect mailing ad-dress, relocation of practice outside the province, and med-ical leave. Fourteen physicians declined participation. Atotal of 152 surveys were available for analysis with aresponse rate of 23.7% (152/641). The numbers of surveyrespondents and prospective subjects within each specialtywere as follows: (a) medical oncology, 42/150 (28%); (b)radiation oncology, 53/185 (28.6%); (c) gynecologic oncol-ogy, 11/24 (45.8%); and (d) urology, 46/244 (18.9%).
Data analyses were conducted using Statistical Package forthe Social Sciences version 17.0. Four categorical demograph-ic variables, i.e., gender, medical specialty, practice setting,and graduation year grouping, were used for bivariate andmultivariate analyses to assess respondents’ knowledge, atti-tudes, and referral patterns through Chi-square tests, analysisof variance (ANOVA), and logistic regression models. Allstatistical tests were two-sided, and a p value of <0.05 wasconsidered to be statistically significant. A 95% confidenceinterval (CI) was used for odds ratios (OR) in the logisticregression models.
Results
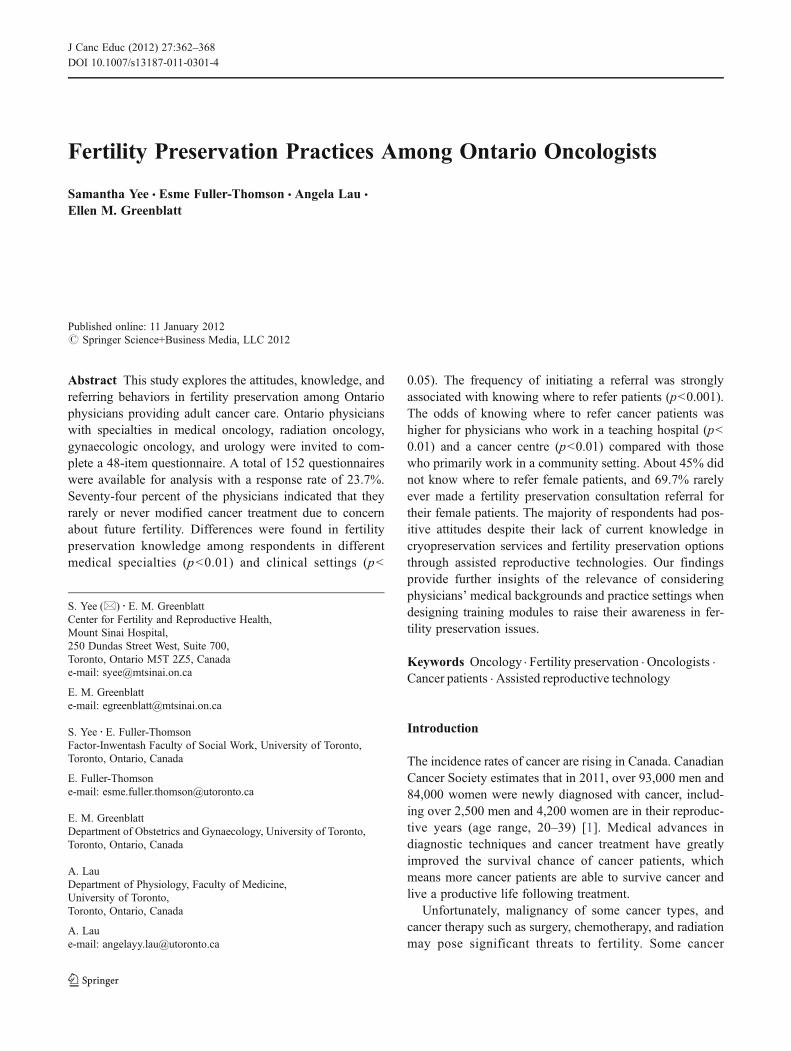
Table 1 summarizes the demographics of respondents andnonrespondents grouped by gender, medical specialty, prac-tice setting, and medical school graduation year. No signif-icant difference was observed, other than a relatively highercomposition of nonrespondents (42.9%) who practiced inthe community and a much higher composition of respond-ents (53.3%) from cancer centers. The predominate cancertypes treated by the respondents were urologic cancer(52%), testicular cancer (40.8%), and breast cancer(38.8%), which are all associated with high risk to fertility.
A list of 15 items was provided for respondents to indicatewhich factors they would consider when deciding to initiatethe FP discussion. Respondents can check off multiple itemson the list. “Age” (91.4%), “desire to have children” (78.9%),“cancer prognosis” (66.4%), “urgency to begin cancer treat-ment” (53.9%), and “type of cancer” (38.2%) were the five topranked factors they would consider.1 Gynecologic Oncology Group of Ontario
J Canc Educ (2012) 27:362–368 363
Physicians were asked to indicate how often they wouldmodify cancer treatment due to concerns about fertilityissues. The vast majority (61.2%) said they “rarely” modi-fied cancer treatment, 23.7% “sometimes,” 2.6% “often,”and 12.5% “never.” Approximately two thirds (66%) of therespondents agreed that all cancer patients with fertility risksdue to cancer treatment should be offered the chance to
cryopreserve gametes, and 67% disagreed that the successrates of assisted reproductive treatments are too low tojustify FP.
Table 2 lists the responses from physicians regardingwhether they would recommend FP to cancer patients underdifferent scenarios with mixture of gender, fertility risklevels, and weeks in delaying cancer treatment.
A list of resources was provided for respondents toindicate what types of materials they usually use whendiscussing FP with patients. Almost all (96.6%) relied onverbal communication. A total of 30.8% and 39% of therespondents did not know the estimated costs of spermbanking and oocyte/embryo cryopreservation procedures,respectively.
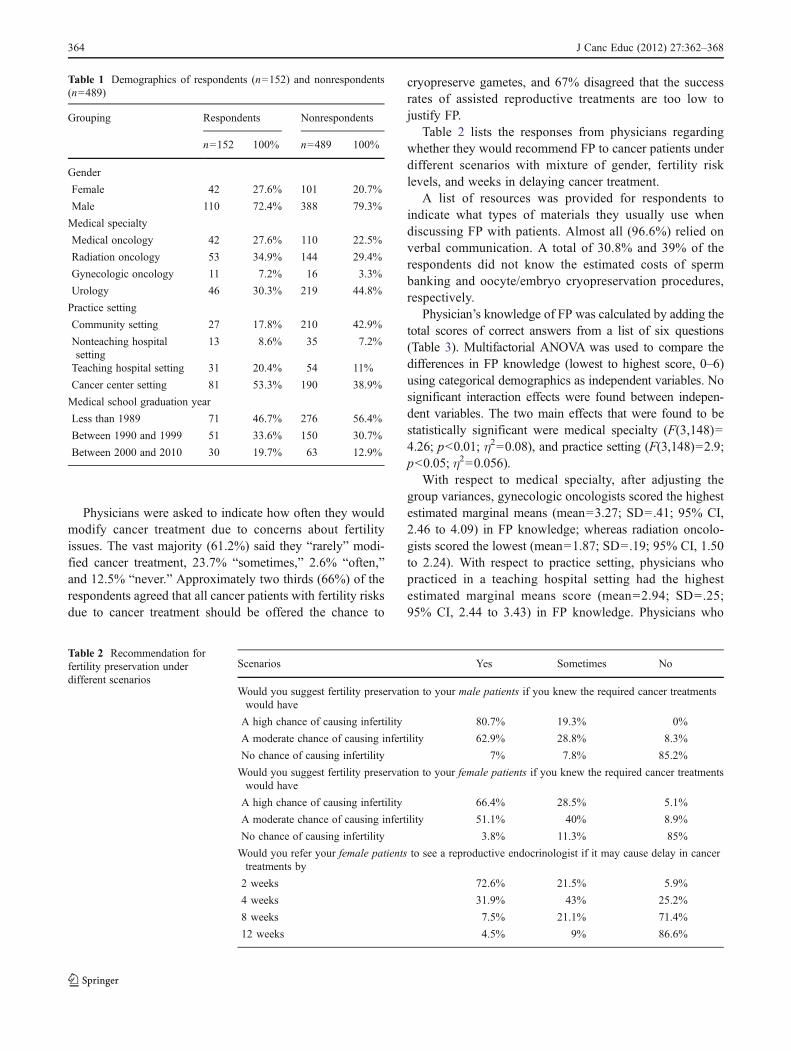
Physician’s knowledge of FP was calculated by adding thetotal scores of correct answers from a list of six questions(Table 3). Multifactorial ANOVA was used to compare thedifferences in FP knowledge (lowest to highest score, 0–6)using categorical demographics as independent variables. Nosignificant interaction effects were found between indepen-dent variables. The two main effects that were found to bestatistically significant were medical specialty (F(3,148)04.26; p<0.01; η200.08), and practice setting (F(3,148)02.9;p<0.05; η200.056).
With respect to medical specialty, after adjusting thegroup variances, gynecologic oncologists scored the highestestimated marginal means (mean03.27; SD0 .41; 95% CI,2.46 to 4.09) in FP knowledge; whereas radiation oncolo-gists scored the lowest (mean01.87; SD0 .19; 95% CI, 1.50to 2.24). With respect to practice setting, physicians whopracticed in a teaching hospital setting had the highestestimated marginal means score (mean02.94; SD0 .25;95% CI, 2.44 to 3.43) in FP knowledge. Physicians who
Table 1 Demographics of respondents (n0152) and nonrespondents(n0489)
Grouping Respondents Nonrespondents
n0152 100% n0489 100%
Gender
Female 42 27.6% 101 20.7%
Male 110 72.4% 388 79.3%
Medical specialty
Medical oncology 42 27.6% 110 22.5%
Radiation oncology 53 34.9% 144 29.4%
Gynecologic oncology 11 7.2% 16 3.3%
Urology 46 30.3% 219 44.8%
Practice setting
Community setting 27 17.8% 210 42.9%
Nonteaching hospitalsetting
13 8.6% 35 7.2%
Teaching hospital setting 31 20.4% 54 11%
Cancer center setting 81 53.3% 190 38.9%
Medical school graduation year
Less than 1989 71 46.7% 276 56.4%
Between 1990 and 1999 51 33.6% 150 30.7%
Between 2000 and 2010 30 19.7% 63 12.9%
Table 2 Recommendation forfertility preservation underdifferent scenarios
Scenarios Yes Sometimes No
Would you suggest fertility preservation to your male patients if you knew the required cancer treatmentswould have
A high chance of causing infertility 80.7% 19.3% 0%
A moderate chance of causing infertility 62.9% 28.8% 8.3%
No chance of causing infertility 7% 7.8% 85.2%
Would you suggest fertility preservation to your female patients if you knew the required cancer treatmentswould have
A high chance of causing infertility 66.4% 28.5% 5.1%
A moderate chance of causing infertility 51.1% 40% 8.9%
No chance of causing infertility 3.8% 11.3% 85%
Would you refer your female patients to see a reproductive endocrinologist if it may cause delay in cancertreatments by
2 weeks 72.6% 21.5% 5.9%
4 weeks 31.9% 43% 25.2%
8 weeks 7.5% 21.1% 71.4%
12 weeks 4.5% 9% 86.6%
364 J Canc Educ (2012) 27:362–368
practiced in a nonteaching hospital setting scored the lowest(mean01.92; SD0 .39; 95% CI, 1.16 to 2.69).
One quarter (24.8%) of the respondents indicated thatthey did not know where to refer patients for sperm banking,and one half (49.7%) rarely ever made a referral. The figuresare even more disconcerting for female patients: 45% ofdoctors did not know where to refer females for FP consul-tation and 69.7% of doctors rarely ever made a referral. Chi-square tests were conducted to evaluate if the frequency ofmaking referrals and knowing where to refer patients wereindependent. After excluding cases with missing values inanalyses, it was found that the frequency of referring malecancer patients was highly dependent on knowing where asperm banking facility was located (χ2 (1, N0134)020.354;p<0.001). Similarly, the frequency of referring female can-cer patients for fertility consultation was highly dependenton knowing where to send the referrals (χ2 (1, N0139)021.194; p<0.001).
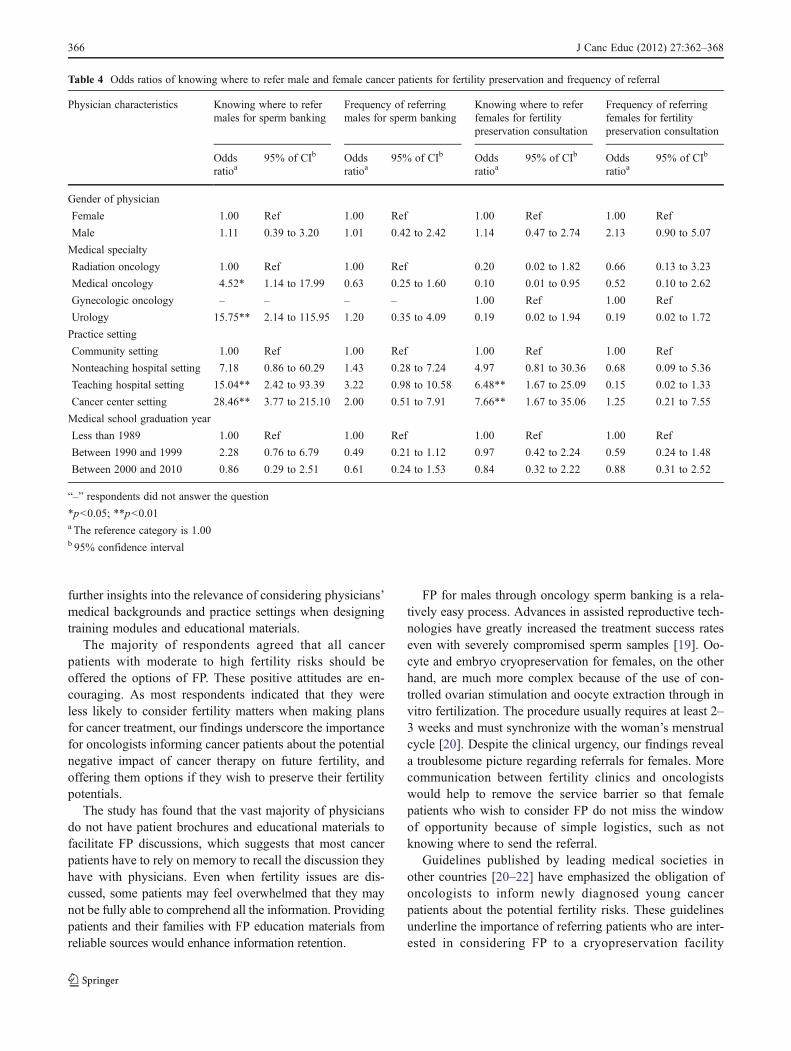
Logistic regression models were used to analyze the oddsratios of knowing where to refer cancer patients and thefrequency of making referrals (i.e. ‘never and rarely’ versus‘sometimes and always’), using the four categorical demo-graphic variables as predictors. The results were shown inTable 4.
In comparison to radiation oncologist, the odds ofknowing where to refer male cancer patients were quitehigh for medical oncologists (OR04.52; 95% CI, 1.14 to17.99; p<0.05) and were even higher for urologists(OR015.75; 95% CI, 2.14 to 115.95; p<0.01). Physi-cians who worked in a teaching hospital (OR015.04;95% CI, 2.42 to 93.39; p<0.01), or a cancer center(OR028.46; 95% CI, 3.77 to 215.10; p<0.01), had sub-stantially high odds ratios of knowing where to refermale patients compared with those who mainly practicedin a community setting. No statistically significant differ-ences in all four categorical demographic variables werefound when frequency of making sperm banking referralswas used as an outcome variable.
For female cancer patients, the odds of knowing where torefer patients for FP consultation were much higher forphysicians who worked in a teaching hospital (OR06.48;95% CI, 1.67 to 25.09; p<0.01) or a cancer center (OR0
7.66; 95% CI, 1.67 to 35.06, p<0.01) in comparison todoctors working in community setting. Other demographiccharacteristics were not associated with the frequency ofreferrals for FP consultation.
Discussion
Findings from this pilot study contribute to the extremelylimited psychosocial based research literature on oncologyFP in Canada. There are several major findings based on themultivariate analyses. First, gynecologic oncologists, aswell as physicians who worked in a teaching hospital set-ting, were most knowledgeable in FP through the use ofassisted reproductive technologies. Second, the frequency ofFP referrals was highly dependent on the physician ofknowing where to refer male and female patients. Third,there were significant differences in referral patterns amongphysicians from different medical specialties and clinicalsettings. Urologists were the most knowledgeable physiciangroup regarding where to refer men for sperm banking.Physicians who worked in teaching hospitals or cancercenters were also much more likely than community physi-cians to know where to refer both male and female cancerpatients, possibly due to greater exposure to recent clinicaldevelopments through academic and hospital rounds. Theymay also have more access to services provided by otherdisciplines such as nurses and social workers in an inter-professional practice environment. There is a clear need toprovide physicians with training on the latest FP optionsthrough assisted reproductive technologies. Our study hasfound that there are significant variations in attitudes,knowledge, and referral patterns for FP among Ontariophysicians providing cancer care. The results provide
Table 3 Physicians’ knowledge in fertility preservation
Questions True False Don’tknow
With today’s cancer treatment, most patients will retain or regain adequate fertility post cancer treatment andtherefore cryopreservation is not necessary
11.2% 80.9%a 7.9%
Patients need to bank 3–6 semen samples before cancer treatment begins to make fertility preservationworthwhile
28.3% 29.6%a 42.1%
There is a maximum length of storage years for banked sperm and cryopreserved eggs/embryos 19.1% 30.3%a 50.6%
Egg banking is currently less efficient than sperm banking as oocytes are more sensitive to freezing than sperm 43.4%a 9.9% 46.7%
The main determinant of treatment success through assisted reproductive technology is the sperm count andsperm quality
35.5% 26.3%a 38.2%
With modern cryopreservation technologies, egg freezing is almost as promising as embryo freezing 19.7% 18.4%a 61.8%
a Correct answer
J Canc Educ (2012) 27:362–368 365
further insights into the relevance of considering physicians’medical backgrounds and practice settings when designingtraining modules and educational materials.
The majority of respondents agreed that all cancerpatients with moderate to high fertility risks should beoffered the options of FP. These positive attitudes are en-couraging. As most respondents indicated that they wereless likely to consider fertility matters when making plansfor cancer treatment, our findings underscore the importancefor oncologists informing cancer patients about the potentialnegative impact of cancer therapy on future fertility, andoffering them options if they wish to preserve their fertilitypotentials.
The study has found that the vast majority of physiciansdo not have patient brochures and educational materials tofacilitate FP discussions, which suggests that most cancerpatients have to rely on memory to recall the discussion theyhave with physicians. Even when fertility issues are dis-cussed, some patients may feel overwhelmed that they maynot be fully able to comprehend all the information. Providingpatients and their families with FP education materials fromreliable sources would enhance information retention.
FP for males through oncology sperm banking is a rela-tively easy process. Advances in assisted reproductive tech-nologies have greatly increased the treatment success rateseven with severely compromised sperm samples [19]. Oo-cyte and embryo cryopreservation for females, on the otherhand, are much more complex because of the use of con-trolled ovarian stimulation and oocyte extraction through invitro fertilization. The procedure usually requires at least 2–3 weeks and must synchronize with the woman’s menstrualcycle [20]. Despite the clinical urgency, our findings reveala troublesome picture regarding referrals for females. Morecommunication between fertility clinics and oncologistswould help to remove the service barrier so that femalepatients who wish to consider FP do not miss the windowof opportunity because of simple logistics, such as notknowing where to send the referral.
Guidelines published by leading medical societies inother countries [20–22] have emphasized the obligation ofoncologists to inform newly diagnosed young cancerpatients about the potential fertility risks. These guidelinesunderline the importance of referring patients who are inter-ested in considering FP to a cryopreservation facility
Table 4 Odds ratios of knowing where to refer male and female cancer patients for fertility preservation and frequency of referral
Physician characteristics Knowing where to refermales for sperm banking
Frequency of referringmales for sperm banking
Knowing where to referfemales for fertilitypreservation consultation
Frequency of referringfemales for fertilitypreservation consultation
Oddsratioa
95% of CIb Oddsratioa
95% of CIb Oddsratioa
95% of CIb Oddsratioa
95% of CIb
Gender of physician
Female 1.00 Ref 1.00 Ref 1.00 Ref 1.00 Ref
Male 1.11 0.39 to 3.20 1.01 0.42 to 2.42 1.14 0.47 to 2.74 2.13 0.90 to 5.07
Medical specialty
Radiation oncology 1.00 Ref 1.00 Ref 0.20 0.02 to 1.82 0.66 0.13 to 3.23
Medical oncology 4.52* 1.14 to 17.99 0.63 0.25 to 1.60 0.10 0.01 to 0.95 0.52 0.10 to 2.62
Gynecologic oncology – – – – 1.00 Ref 1.00 Ref
Urology 15.75** 2.14 to 115.95 1.20 0.35 to 4.09 0.19 0.02 to 1.94 0.19 0.02 to 1.72
Practice setting
Community setting 1.00 Ref 1.00 Ref 1.00 Ref 1.00 Ref
Nonteaching hospital setting 7.18 0.86 to 60.29 1.43 0.28 to 7.24 4.97 0.81 to 30.36 0.68 0.09 to 5.36
Teaching hospital setting 15.04** 2.42 to 93.39 3.22 0.98 to 10.58 6.48** 1.67 to 25.09 0.15 0.02 to 1.33
Cancer center setting 28.46** 3.77 to 215.10 2.00 0.51 to 7.91 7.66** 1.67 to 35.06 1.25 0.21 to 7.55
Medical school graduation year
Less than 1989 1.00 Ref 1.00 Ref 1.00 Ref 1.00 Ref
Between 1990 and 1999 2.28 0.76 to 6.79 0.49 0.21 to 1.12 0.97 0.42 to 2.24 0.59 0.24 to 1.48
Between 2000 and 2010 0.86 0.29 to 2.51 0.61 0.24 to 1.53 0.84 0.32 to 2.22 0.88 0.31 to 2.52
“–” respondents did not answer the question
*p<0.05; **p<0.01a The reference category is 1.00b 95% confidence interval
366 J Canc Educ (2012) 27:362–368

promptly. Unfortunately, practice guidelines have not yetbeen developed by Canadian medical societies to providephysicians with guidance of best practice models that aregeared to the Canadian health care system. Practice guide-lines are much needed so that all reproductive-aged cancerpatients wishing to preserve fertility receive standardizedand best care.
There are several limitations to the current study. First,only Ontario physicians who were involved in cancer carewere surveyed. Ontario is the most populous province inCanada [23] and it has more than one third (37%) of thenation’s new cancer cases [1]. Ontario also has the highestconcentration of fertility specialists, sperm banking facili-ties, and fertility clinics in Canada [24] and therefore it wasan ideal location of this pilot study. Despite that, general-ization of findings to a wider Canadian physician populationmust be made with caution. Second, the sampling framedid not include surgeons or paediatric physicians provid-ing cancer care. Third, the questionnaire was constructedspecifically for this study and we did not investigatetest–retest reliability. Fourth, although the inclusion of ageneral FP brochure in the mailing may bias the knowl-edge score, the results show that the majority of respond-ents’ knowledge in FP was still inadequate. Finally, theresponse rate of 23.7% is suboptimal, although it issimilar to the response rate in other studies of oncolo-gists’ attitudes and knowledge in FP (e.g., 15% [25, 26],24% [9], 28% [8], and 32% [11]). As our comparison ofresponders and nonresponders indicated differences withrespect to their practice setting, it is possible that thosewho chose to respond to our survey were more sensitiveto and knowledgeable about oncology-related fertilityissues due to their practice environment.
Despite these limitations, our findings suggest that al-though the majority of physicians had positive attitudestoward FP, deficits and gaps in knowledge exist. Inconsis-tency in practice behaviors and variations in referral patternswere found. Understandably, oncologists would be hesitantto discuss fertility risks with cancer patients if they do nothave updated knowledge on FP options, the location ofcryopreservation facilities, and the types of FP servicesoffered by fertility clinics. More Canadian research studiesare needed to explore how fertility concerns are beingaddressed during cancer care, and how physicians commu-nicate with cancer patients about the options of preservingfertility.
Acknowledgments The co-authors would like to express apprecia-tion to Abha Gupta MD, David Hodgson MD, Keith Jarvi MD, KirkLo MD, Orla McArdle MD, Joan Murphy MD, and Barry Rosen MDfor providing feedback on the questionnaire for validity purpose.
Funding Support Mount Sinai Hospital Rose Torno Bursary 2009awarded to the first author.
Presentation The findings were presented at the Canadian Fertilityand Andrology Society’s 56th Annual Meeting in Vancouver (29 Sept–2 Oct 2010), and the presentation received the Best Psychosocial Paperaward.
References
1. Canadian Cancer Society’s Steering Committee (2011) CanadianCancer Statistics 2011. Available at: http://www.cancer.ca.Accessed 5 December 2010
2. Crha I, Ventruba P, Zakova J et al (2009) Survival and infertilitytreatment in male cancer patients after sperm banking. Fertil Steril91:2344–2348
3. Hickey M, Peate M, Saunders CM et al (2009) Breast cancer inyoung women and its impact on reproductive function. HumReprod Update 15:323–339
4. Partridge AH, Gelber S, Peppercorn J et al (2004) Web-basedsurvey of fertility issues in young women with breast cancer. JClin Oncol 22:4174–4183
5. Chapple A, Salinas M, Ziebland S et al (2007) Fertility issues: theperceptions and experiences of young men recently diagnosed andtreated for cancer. J Adolesc Health 40:69–75
6. Duffy C, Allen S, Clark M (2005) Discussions regarding repro-ductive health for young women with breast cancer undergoingchemotherapy. J Clin Oncol 23:766–773
7. Quinn GP, Vadaparampil ST, Bell-Ellison BA et al (2008) Patient–physician communication barriers regarding fertility preservationamong newly diagnosed cancer patients. Soc Sci Med 66:784–789
8. Zapzalka DM, Redmon JB, Pryor JL (1999) A survey of oncolo-gists regarding sperm cryopreservation and assisted reproductivetechniques for male cancer patients. Cancer 86:1812–1817
9. Schover LR, Brey K, Lichtin A et al (2002) Oncologists’ attitudesand practices regarding banking sperm before cancer treatment. JClin Oncol 20:1890–1897
10. Quinn GP, Vadaparampil ST, Gwede CK et al (2007) Discussion offertility preservation with newly diagnosed patients: oncologists’views. J Cancer Surviv 1:146–155
11. Quinn GP, Vadaparampil ST, Lee JH et al (2009) Physician referralfor fertility preservation in oncology patients: a national study ofpractice behaviors. J Clin Oncol 27:5952–5957
12. Anderson RA, Weddell A, Spoudeas HA et al (2008) Do doctorsdiscuss fertility issues before they treat young patients with cancer?Hum Reprod 23:2246–2251
13. Schover LR, Brey K, Lichtin A et al (2002) Knowledge andexperience regarding cancer, infertility, and sperm banking inyounger male survivors. J Clin Oncol 20:1880–1889
14. Achille MA, Rosberger Z, Robitaille R et al (2006) Facilitators andobstacles to sperm banking in young men receiving gonadotoxicchemotherapy for cancer: the perspective of survivors and healthcare professionals. Hum Reprod 21:3206–3216
15. Nagel K, Neal M (2008) Discussions regarding sperm bankingwith adolescent and young adult males who have cancer. J PediatrOncol Nurs 25:102–106
16. Yee S, Fuller-Thomson E, Dwyer C et al (2011) “Just what thedoctor ordered”: factors associated with oncology patients’decision to bank sperm. Can Urol Assoc J. doi:10.5489/cuaj.10084
17. Vadaparampil ST, Clayton H, Quinn GP et al (2007) Pediatriconcology nurses’ attitudes related to discussing fertility preserva-tion with pediatric cancer patients and their families. J PediatrOncol Nurs 24:255–263
J Canc Educ (2012) 27:362–368 367

18. Vadaparampil ST, Quinn GP, King LM (2008) Institutionalavailability of fertility preservation. Clin Pediatr 47:302–305
19. Selk A, Belej-Rak T, Shapiro H, Greenblatt E (2009) Use of anoncology sperm bank: a Canadian experience. Can Urol Assoc J3:219–222
20. Lee SJ, Schover LR, Partridge AH et al (2006) American Societyof Clinical Oncology recommendations on fertility preservation incancer patients. J Clin Oncol 24:2917–2931
21. Ethics Committee of the American Society for Reproductive Med-icine (2005) Fertility preservation and reproduction in cancerpatients. Fertil Steril 83:1622–1628
22. British Fertility Society (2003) A strategy for fertility services forsurvivors of childhood cancer. Hum Fertil 6:A1–A40
23. Statistics Canada: Population by year, by province and territory,2009. Available at: http://www40.statcan.gc.ca/l01/cst01/demo02a-eng.htm. Accessed 5 December 2011
24. Canadian Fertility and Andrology Society. IVF Clinics. Availableat http://www.cfas.ca/index.php?option0com_content&view0article&id0259&Itemid0274. Accessed 5 December 2011
25. Forman EJ, Anders CK, Behera MA (2010) A nationwide surveyof oncologists regarding treatment-related infertility and fertilitypreservation in female cancer patients. Fertil Steril 94:1652–1656
26. Köhler T, Kondapalli LA, Shah A et al (2011) Results from thesurvey for preservation of adolescent reproduction (SPARE) study:gender disparity in delivery of fertility preservation message toadolescents with cancer. J Assist Reprod Genet 28:269–277
368 J Canc Educ (2012) 27:362–368














![Fertility Preservation Options for Female Cancer Patients ... · fertility preservation methods and resources [11-13]. This review will provide updated information on the options](https://img.pdfslide.us/doc/110x75/5f96e2e723578314826b34f5/fertility-preservation-options-for-female-cancer-patients-fertility-preservation.jpg)