Embed Size (px)
Citation preview
7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 1/10
REFRACTIVE SURGERY
The effect of hinge location on corneal sensation and dry eye
after LASIK: a systematic review and meta-analysis
Yi-fan Feng & Ji-guo Yu & Dan-dan Wang & Jun-hua Li &
Jin-hai Huang & Jie-liang Shi & Ting Ye & Qin-mei Wang &
Yun-e Zhao
Received: 14 January 2012 /Revised: 18 May 2012 /Accepted: 24 May 2012 /Published online: 15 June 2012# Springer-Verlag 2012
Abstract
Background The aim of this meta-analysis is to investigatethe possible effect of hinge location on corneal sensation
and dry eye syndrome after laser-assisted in situ keratomi-
leusis (LASIK).
Methods A comprehensive literature search was conducted
in the PubMed, EMBASE, and Cochrane Controlled Trials
Register to identify potentially relevant randomized con-
tro lled tr ia ls (RCTs ) o f c o mp arin g th e e ffe cts o f
horizontal-hinge flaps and vertical-hinge flaps on corneal
sensation and dry eye after LASIK. Meta-analyses were
pe rf orme d fo r co rn ea l se ns atio n, te ar brea k-up ti me
(TBUT), Schirmer's I test and corneal fluorescein staining
(CFS) at 1 week, 1, 3, and 6 months postoperatively. Results Eight RCTs (657 eyes) investigating the effects of
hinge location on the corneal sensation and dry eye syn-
drome after LASIK were identified. The results showed that
the horizontal-hinge group causes less loss of sensation than
the vertical-hinge group, and the difference was significant
at 3-month postoperative ( p00.01). The TBUT value was
significantly larger and a lower percentage of patients with
CFS in the horizontal-hinge group than in the vertical-hinge
group at 1-month postoperative ( p00.007 and p00.01,
respectively) and 3-month ( p00.03 and p00.009, respec-
tively); Schirmer's I test values were also higher in thehorizontal-hinge group, but the difference did not reach
statistically significance at each postoperative period.
Conclusions According to the available data, we suggest
that hinge location may have some effect on corneal sensa-
tion and dry eye syndrome after LASIK at the early postop-
erative period. However, there was no significant difference
between the groups at 6 months after surgery. Further well-
organized, prospective, randomized studies involving more
patients are warranted.
Keywords Laser-assisted in situ keratomileusis . Hinge
position . Corneal sensation . Dry eye
Introduction
Dry eye syndrome is a frequent postoperative complication
of laser-assisted in situ keratomileusis (LASIK) [1]. Al-
though estimates of the incidence of dry eye syndrome vary
widely (from 3 – 59 % [1 – 3]), almost all patients will have
transient dry eye during the immediate postoperative period.
These symptoms, such as mild irritation, foreign-body sen-
sation to pain, photophobia, and fluctuating visual acuity
between blinks, are considered to be associated with sever-
ing of the corneal nerves in LASIK surgery [4]. Corneal flap
creation and ablation of the stroma during LASIK cause the
innervation damage to afferent sensory nerves, which can
produce a relative loss of corneal sensation. This loss of
sensation appears to be a significant contributing factor to
the reduction in tear secretion, tear film stability, blink rate,
and conjunctival goblet cell density [5, 6].
Because of the variability in corneal innervation patterns,
altering flap characteristics in LASIK may affect postoperative
Proprietary interest The authors have no proprietary or commercial
interests in any material discussed in this article. The authors have full
control of all primary data and agree to allow Graefes Archive for
Clinical and Experimental Ophthalmology to review data upon request.
ClinicalTrials.gov identifier NCT01507025
Y.-f. Feng : J.-g. Yu : D.-d. Wang : J.-h. Li : J.-h. Huang :
J.-l. Shi : T. Ye : Q.-m. Wang : Y.-e. Zhao (*)
The Affiliated Eye Hospital of Wenzhou Medical College, School
of Optometry and Ophthalmology, Wenzhou Medical College,
No. 270, Xueyuan Road,
Wenzhou, Zhejiang Province, China
e-mail: [email protected]
Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366
DOI 10.1007/s00417-012-2078-5

7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 2/10
corneal sensation and dry eye disease. Some studies have
reported that postoperative corneal sensation may be higher
and recovery faster in eyes with horizontal-hinge flaps (nasal-
or temporal) than in eyes with vertical-hinge flaps (superior) [7,
8]. However, some other studies were unable to confirm differ-
ences in the effect of hinge position on corneal sensation and
dry-eye symptoms [9, 10]. Currently, no systematic review of
this subject is available. This study reviewed the publishedliterature and performed a meta-analysis aimed to investigate
the effects of hinge location on corneal sensation and dry eye
symptoms after LASIK.
Materials and methods
This meta-analysis was performed according to a predeter-
mined protocol described in the following paragraphs [11, 12].
Search strategy
Two reviewers (Y.F.F. and J.G.Y.) independently searched
the following electronic databases: PUBMED, EMBASE,
and the Cochrane Controlled Trials Register, and the last
search was performed on November 15, 2011. The follow-
ing keywords were used: laser in situ keratomileusis,
LASIK, hinge position corneal sensation, and dry eye. There
was no language restriction on the publications. All relevant
studies were obtained and assessed to determine whether
they met standard quality criteria for inclusion in the study.
In addition, the reference lists of original reports and review
articles retrieved through the search were reviewed for ad-
ditional studies not yet included in the computerized
databases.
Trials selection
Studies fulfilling the following inclusion criteria were in-
cluded in the present meta-analysis: (1) each trial should be
a prospective randomized controlled clinical trial (RCT), (2)
the age of the patient population should be over 18 years, (3)
the patients were scheduled to undergo LASIK and assigned
to horizontal-hinge flap (HF) group or vertical-hinge flap
(VF) group, (4) at least one of following outcomes was
assessed: corneal sensation, tear break-up time (TBUT),
Schirmer's I test, and the proportion of patients with corneal
fluorescein staining (CFS). Exclusion criteria were as fol-
lows: (1) non-RCTs, (2) patients who had a previous oph-
thalmic surgery or ocular surface disorders, and (3) the raw
data were not completed. If more than one version of the
same study was retrieved, only the most recent was used.
Two reviewers (Y.F.F. and J.G.Y.) separately evaluated stud-
ies based on inclusion and exclusion criteria, and discrep-
ancies were resolved by discussion.
Data extraction
Data extraction was performed according to the customized
protocol by two reviewers (Y.F.F. and J.G.Y.) independently.
A customized form was used to record the following data:
the authors of the study, the year of publication, information
on study design (whether randomization, allocation conceal-
ment, intention-to-treat (ITT) analysis, double blind or sin-gle blind), location of trial, length of study, number of
subjects, patient age, sex, and the preoperative mean spher-
ical equivalent refraction (SE).
Qualitative assessment
The RCTs were analyzed for their quality based on the
Delphi list for quality assessment of randomized clinical
trials [13]. For each trial, a quality score was calculated,
where “yes” was scored as one point for a certain quality
item and “no” and “don’t know” were scored as zero points.
The quality of individual study was then determined bygiving a total additive score to each study. Based on these
assessments and the Cochrane Collaboration guidelines, the
two reviewers (Y.F.F. and J.G.Y.) independently evaluated
the studies, and disagreements were resolved by discussion.
Outcome measures
The outcome parameters for inclusion were corneal sensation,
TUBT, Schirmer's I test, and the proportion of patients with
CFS. Studies presented results at varying follow-up periods,
and we chose to analyze results at 1 week and 1, 3, and
6 months due to their common presence in most study reports.
In absence of continuous outcome values reported in a
table or text, the values were measured when presented in a
figure. Figures used to extract data were electronically
scanned and viewed at full screen size (1024×768 pixels)
and a digital ruler was used to measure. All figures were
read by the same researcher (Y.F.F.).
Statistical analysis
Original data were obtained from the articles as much as
possible; data that could not be obtained were to be calcu-
lated when necessary. When standard deviation (SD) was
not available, it was calculated using the sample sizes and
standard error. When neither an SD nor a standard error of
end point measurement was available, baseline SD was used
as an estimate of the SD of any time point postoperatively.
When only the p value for the difference between the two
groups was reported, the SD was calculated according to the
p value and the sample sizes.
Statistical analysis was performed using RevMan
software (version 5.0; Cochrane Collaboration, Oxford,
358 Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366

7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 3/10
United Kingdom). Summary estimates, including 95 %
confidence intervals (CIs), were calculated. For contin-
uous outcome, means and standard deviations were used
to calculate the weighted mean difference (WMD; e.g.,
corneal sensation, TBUT, Schirmer's I test). For dichot-
omous outcomes, the odds ratio (OR; e.g., proportions
of CFS) was calculated.
Statistical heterogeneity was tested using the Chi-squareand I2 statistic. Fixed-effects models were used unless sig-
nificant evidence of statistical heterogeneity or clinical di-
versity was found. However, for results showing significant
heterogeneity (I2>50 %), a random-effects meta-analysis
was performed by DerSimonian-Laird method [14]. This
model can yield wider CI, which would reduce the hetero-
geneity. A p value less than 0.05 was considered statistically
significant. Potential publication bias was examined using a
funnel plot [15].
Results
Literature search
The combined search identified a total of 302 publications.
However, only 11 articles were considered potentially rele-
vant. Of the 11 publications, three finally were excluded for
non-randomized design [16], animal model [17], and no
measurable outcomes [18]. Thus, the remaining eight RCTs
published between 2003 and 2009 were included in this
meta-analysis [7 – 10, 19 – 22].
A total of 366 participants with 657 eyes in eight
included studies were enrolled in this meta-analysis; 328
eyes assigned to the VF group and 329 eyes to the HF
group. Sample sizes in these studies ranged from 20 to
106. The mean age was ranged between 26.5 and
40.8 years and the follow-up time was 6~ 12 months.
Of the eight RCTs, six studies reported random selec-
tion of VF in one eye and HF in the other eye in each
patient [8 – 10, 19, 21, 22]. Corneal flap was created by
mechanical microkeratome in six studies [7 – 9, 19, 20,
22] and by femtosecond laser in remaining two studies
[10, 21] (Table 1). The included trials are also assessed
on their quality (Table 2).
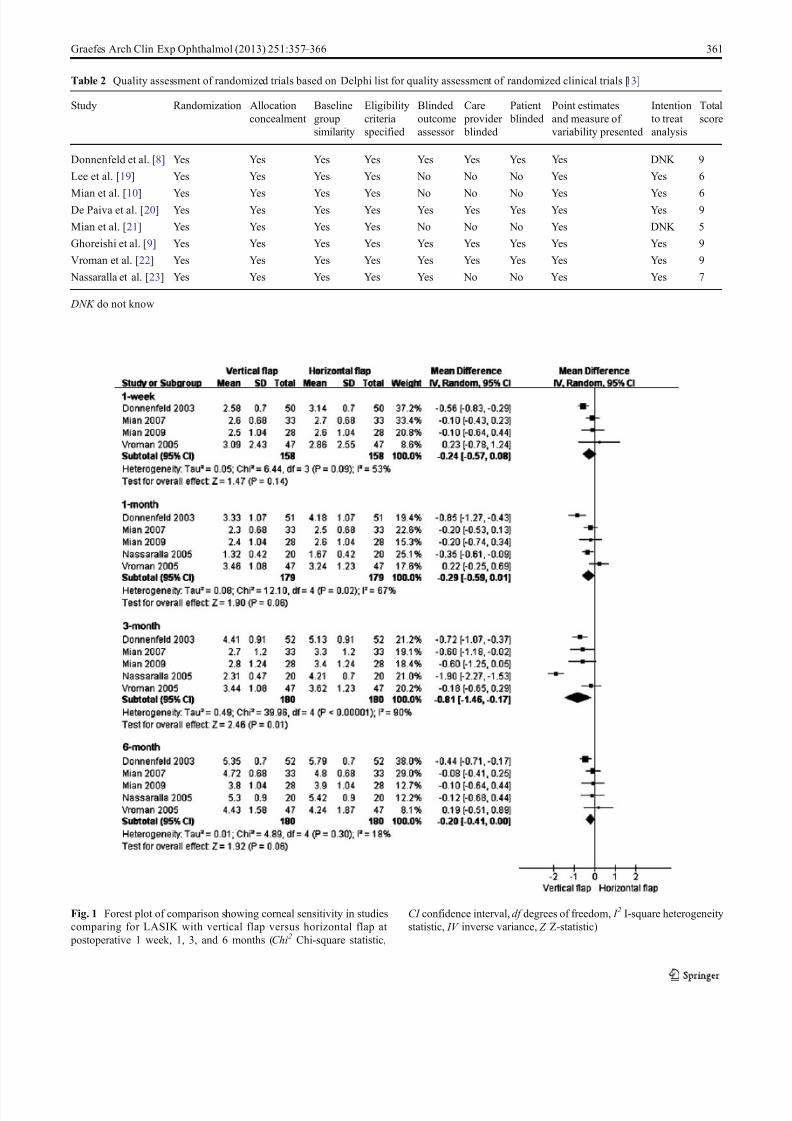
Corneal sensitivity
Five studies reported corneal sensitivity by using the
Cochet – Bonnet esthesiometer [7, 8, 10, 21, 22]. Because
statistically significant heterogeneity was evident for the
outcome of corneal sensitivity, a random-effects model
was used to combine the data. Analysis of these data
showed that the mean decrease in corneal sensation was
significantly greater in the VF group compared to the HF
group 3 months postoperatively (WMD −0.81; 95 % CI
−1.46 to −0.17; p00.01). There was no significant differ-
ence between the two groups at postoperative 1-week
(WMD −0.24; 95 % CI −0.57 to 0.08; p00.14), 1-month
(WMD −0.29; 95 % CI −0.59 to −0.01; p00.06) and 6-
month (WMD −0.20; 95 % CI −0.41 to 0.00; p00.06)
(Fig. 1).
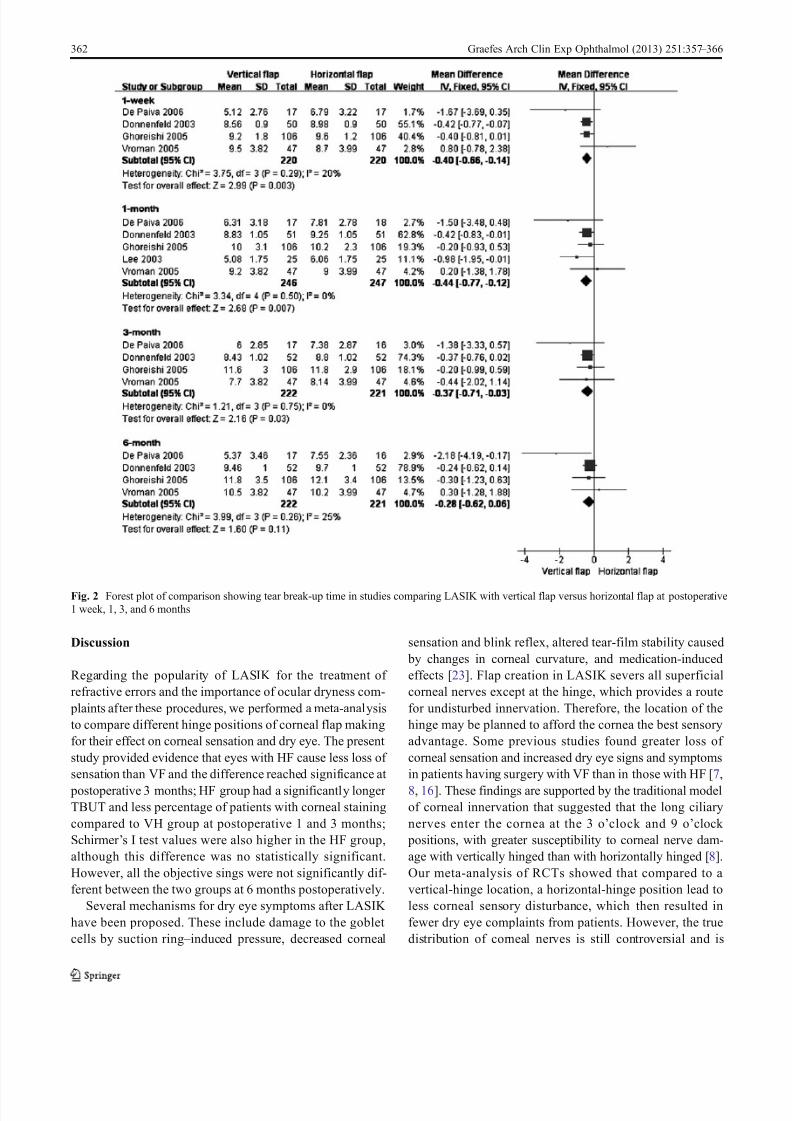
Tear break-up time
Five studies reported data for the TUBT [8, 9, 19, 20, 22]. In
one study, the 2-month results were used as a proxy for 1-
month results [19]. Analysis of these data showed that the
mean decrease in TBUT was significantly greater in the VF
group compared to the HF group at 1 week (WMD −0.40;
95 % CI −0.66 to −0.14; p00.003), 1-month (WMD −0.44;
95 % CI −0.77 to −0.12; p00.007) and 3-month (WMD
−0.37; 95 % CI −0.71 to −0.03; p00.03) postoperative
visits. There was no significant difference between the two
groups at the 6-month visits (WMD −
0.28; 95 % CI−
0.62 to0.06; p00.11) (Fig. 2).
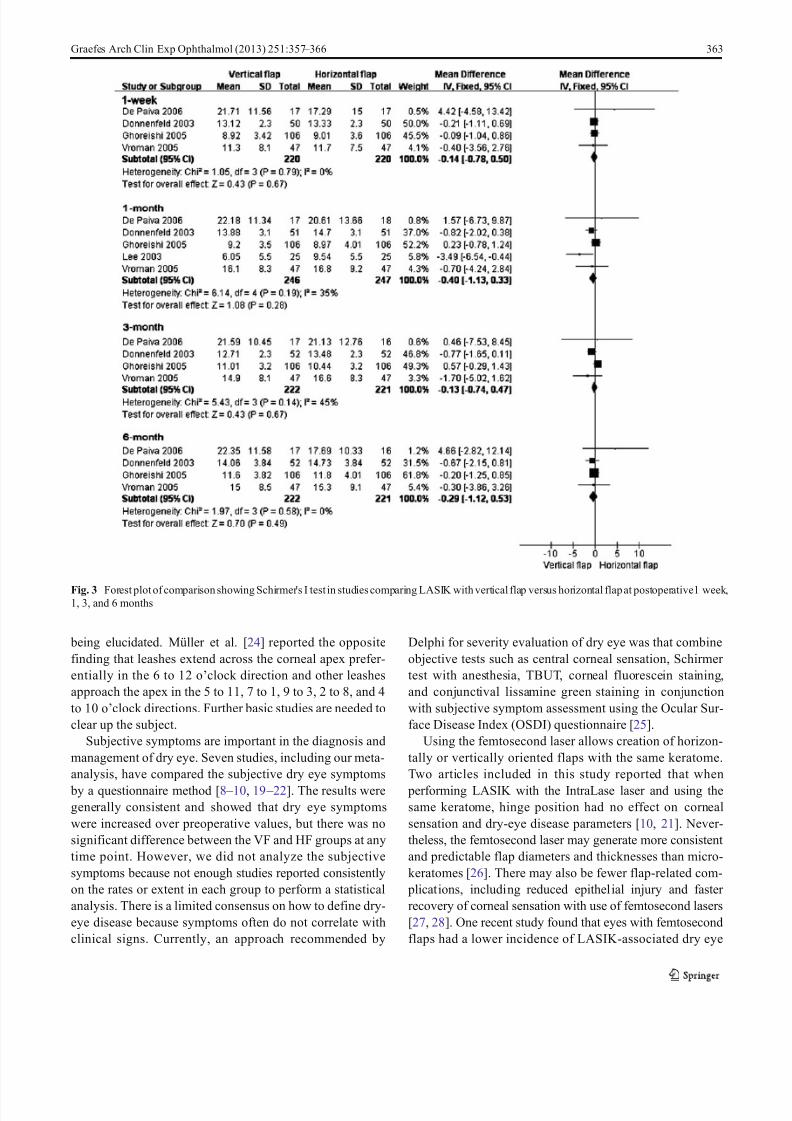
Schirmer's I test
Five studies reported data for the Schirmer ’s I score [8, 9,
19, 20, 22]. Analysis of these data showed that there was no
significant difference in the mean decrease in Schirmer ’s I
score between the VF group and the HF group at 1 week
(WMD −0.14; 95 % CI −0.78 to 0.50; p00.67), 1 month
(WMD −0.40; 95 % CI −1.13 to 0.33; p00.28), 3 months
(WMD −0.13; 95 % CI −0.74 to 0.47; p00.67), 6 months
(WMD0−
0.29, 95 % CI −
1.12 to 0.53, p00.49) postopera-
tively. (Fig. 3)
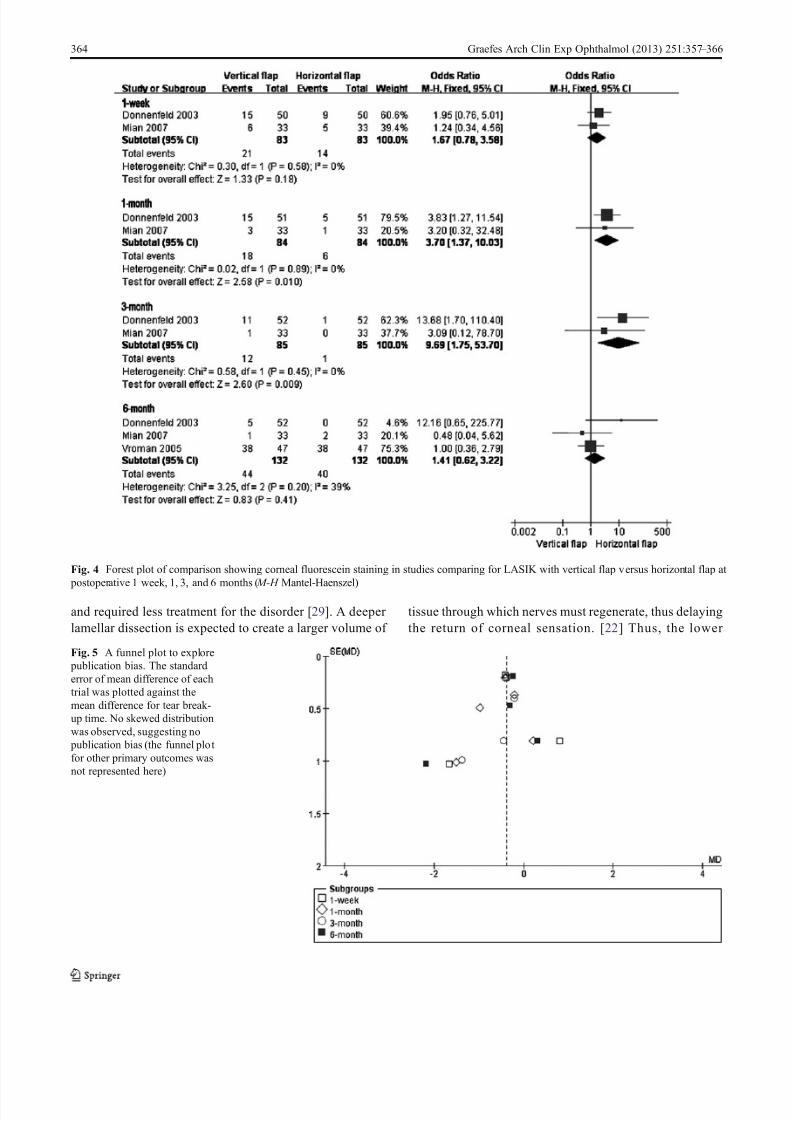
Corneal fluorescein staining
Three studies reported data for proportion of patients
with corneal fluorescein staining [8, 10, 22]. Analysis of
these data showed that the VF group showed a signif-
icantly greater percentage of patients with CFS com-
pared to the HF group at 1 month (OR 3.7; 95 % CI
1.37 to 10.03; p00.01) and 3 months (OR 9.69; 95 %
CI 1.75 to 53.70; p00.009) postoperatively. There was
no significant difference between the two groups at
pos toper ative 1 week (OR 1.7 4; 95 % CI 1.3 7 to
10.03; p00.01) and 6 months (OR 3.7; 95 % CI 1.37
to 10.03; p00.01) (Fig. 4).
Publication bias
Publication bias was assessed for all pooled WMDs and OR
with confidence intervals and shown as a funnel plot in
Fig. 5. No evidence of publication bias was found.
Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366 359
7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 4/10
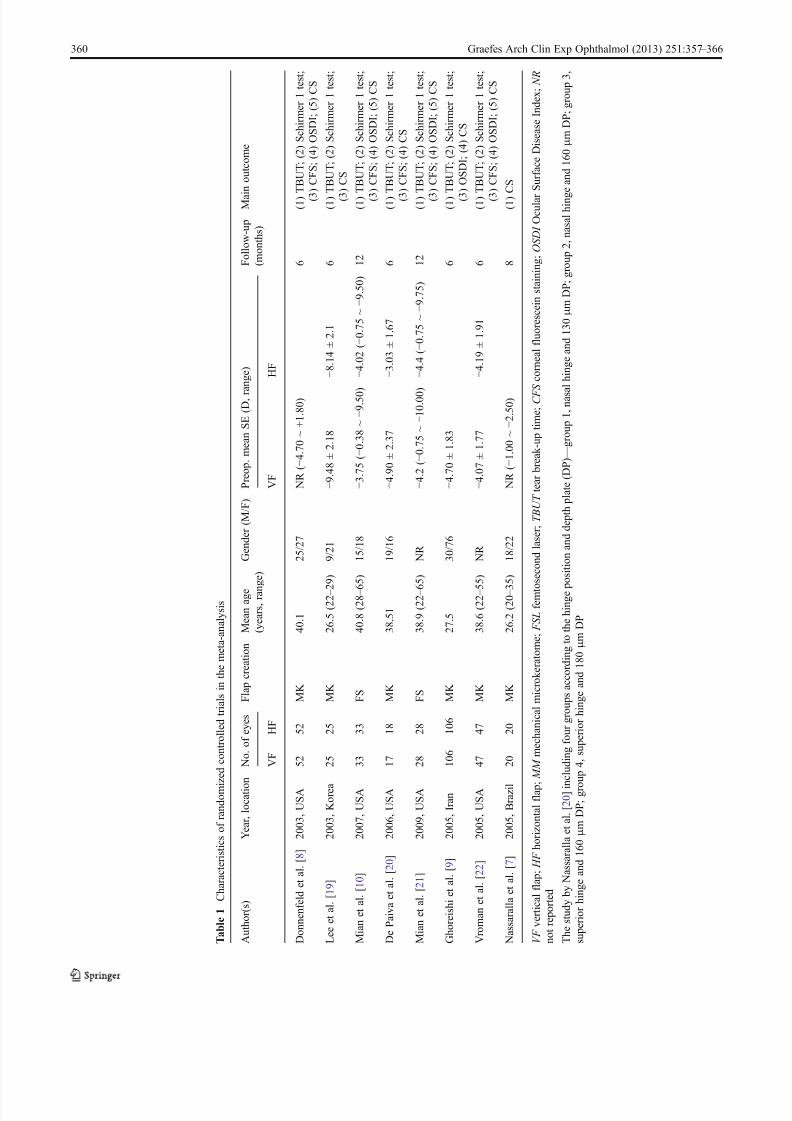
T a b l e 1
C h a r a c t e r i s t i c s o
f r a n
d o m i
z e
d c o n t r o l l e d t r i a l s i n t h e m e t a - a n a
l y s i s
A u t h o r ( s )
Y e a r , l o c a t i o
n
N o . o f e y e s
F l a p c r e a t i o n
M e a n a g e
( y e a r s , r a n
g e )
G e n d e r ( M / F )
P r e o p . m e a n S E ( D , r a n g e )
F o l l o w - u p
( m o n t h s )
M a i n o u t c o m e
V F
H F
V F
H F
D o n n e n f e l d e t a l . [ 8 ]
2 0 0 3 , U S A
5 2
5 2
M K
4 0 . 1
2 5 / 2 7
N R ( − 4 . 7 0 ~ + 1 . 8 0 )
6
( 1 )
T B U T ; ( 2 ) S c h i r m e r 1 t e s t ;
( 3
) C F S ; ( 4 ) O S D I ; ( 5 ) C S
L e e e t a l . [ 1 9 ]
2 0 0 3 , K o r e a
2 5
2 5
M K
2 6 . 5 ( 2 2 – 2
9 )
9 / 2 1
− 9 . 4 8 ± 2 . 1 8
− 8 . 1 4 ± 2 . 1
6
( 1 )
T B U T ; ( 2 ) S c h i r m e r 1 t e s t ;
( 3
) C S
M i a n e t a l . [ 1 0 ]
2 0 0 7 , U S A
3 3
3 3
F S
4 0 . 8 ( 2 8 – 6
5 )
1 5 / 1 8
− 3 . 7 5 ( − 0 . 3 8 ~ − 9 . 5 0 )
− 4 . 0 2 ( − 0 . 7 5 ~ − 9 . 5 0 )
1 2
( 1 )
T B U T ; ( 2 ) S c h i r m e r 1 t e s t ;
( 3
) C F S ; ( 4 ) O S D I ; ( 5 ) C S
D e P a i v a e t a l . [ 2 0 ]
2 0 0 6 , U S A
1 7
1 8
M K
3 8 . 5 1
1 9 / 1 6
− 4 . 9 0 ± 2 . 3 7
− 3 . 0 3 ± 1 . 6 7
6
( 1 )
T B U T ; ( 2 ) S c h i r m e r 1 t e s t ;
( 3
) C F S ; ( 4 ) C S
M i a n e t a l . [ 2 1 ]
2 0 0 9 , U S A
2 8
2 8
F S
3 8 . 9 ( 2 2 – 6
5 )
N R
− 4 . 2 ( − 0 . 7 5 ~ − 1 0 . 0 0 )
− 4 . 4 ( − 0 . 7 5 ~ − 9 . 7 5 )
1 2
( 1 )
T B U T ; ( 2 ) S c h i r m e r 1 t e s t ;
( 3
) C F S ; ( 4 ) O S D I ; ( 5 ) C S
G h o r e i s h i e t a l . [ 9 ]
2 0 0 5 , I r a n
1 0 6
1 0 6
M K
2 7 . 5
3 0 / 7 6
− 4 . 7 0 ± 1 . 8 3
6
( 1 )
T B U T ; ( 2 ) S c h i r m e r 1 t e s t ;
( 3
) O S D I ; ( 4 ) C S
V r o m a n e t a l . [ 2 2 ]
2 0 0 5 , U S A
4 7
4 7
M K
3 8 . 6 ( 2 2 – 5
5 )
N R
− 4 . 0 7 ± 1 . 7 7
− 4 . 1 9 ± 1 . 9 1
6
( 1 )
T B U T ; ( 2 ) S c h i r m e r 1 t e s t ;
( 3
) C F S ; ( 4 ) O S D I ; ( 5 ) C S
N a s s a r a l l a e t a l . [ 7 ]
2 0 0 5 , B r a z i l
2 0
2 0
M K
2 6 . 2 ( 2 0 – 3
5 )
1 8 / 2 2
N R ( − 1 . 0 0 ~ − 2 . 5 0 )
8
( 1 )
C S
V F v e r t i c a
l f l a p ; H F h o r i z o n t a l f l a p ; M M m e c
h a n
i c a
l m
i c r o
k e r a t o m e ; F S L f e m t o s e c o n
d l a s e r ; T B U T t e a r
b r e a
k - u p t i m e ; C F S c o r n e a
l f l u o r e s c e
i n s t a
i n i n g ; O S D I O c u
l a r
S u r f a c e
D i s e a s e
I n d e x ; N R
n o t r e p o r t e
d
T h e s t u
d y
b y
N a s s a r a
l l a e t a
l . [ 2 0 ] i n
c l u d i n g
f o u r g r o u p s a c c o r d
i n g t o t h e
h i n g e p o s i t i o n a n
d d e p t h p
l a t e ( D P ) — g r o u p
1 ,
n a s a
l h i n g e a n
d 1 3 0 μ m
D P ; g r o u p
2 ,
n a s a
l h i n g
e a n
d 1 6 0 μ m
D P ; g r o u p
3 ,
s u p e r i o r
h i n g e a n
d 1 6 0 μ m
D P ; g r o
u p
4 ,
s u p e r i o r
h i n g e a n
d 1 8 0 μ m
D P
360 Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366
7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 5/10
Table 2 Quality assessment of randomized trials based on Delphi list for quality assessment of randomized clinical trials [13]
Study Randomization Allocation
concealment
Baseline
group
similarity
Eligibility
criteria
specified
Blinded
outcome
assessor
Care
provider
blinded
Patient
blinded
Point estimates
and measure of
variability presented
Intention
to treat
analysis
Total
score
Donnenfeld et al. [8] Yes Yes Yes Yes Yes Yes Yes Yes DNK 9
Lee et al. [19] Yes Yes Yes Yes No No No Yes Yes 6
Mian et al. [10] Yes Yes Yes Yes No No No Yes Yes 6De Paiva et al. [20] Yes Yes Yes Yes Yes Yes Yes Yes Yes 9
Mian et al. [21] Yes Yes Yes Yes No No No Yes DNK 5
Ghoreishi et al. [9] Yes Yes Yes Yes Yes Yes Yes Yes Yes 9
Vroman et al. [22] Yes Yes Yes Yes Yes Yes Yes Yes Yes 9
Nassaralla et al. [23] Yes Yes Yes Yes Yes No No Yes Yes 7
DNK do not know
Fig. 1 Forest plot of comparison showing corneal sensitivity in studies
comparing for LASIK with vertical flap versus horizontal flap at
postoperative 1 week, 1, 3, and 6 months (Chi2 Chi-square statistic,
CI confidence interval, df degrees of freedom, I 2 I-square heterogeneity
statistic, IV inverse variance, Z Z-statistic)
Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366 361
7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 6/10
Discussion
Regarding the popularity of LASIK for the treatment of
refractive errors and the importance of ocular dryness com-
plaints after these procedures, we performed a meta-analysis
to compare different hinge positions of corneal flap making
for their effect on corneal sensation and dry eye. The present
study provided evidence that eyes with HF cause less loss of
sensation than VF and the difference reached significance at
postoperative 3 months; HF group had a significantly longer
TBUT and less percentage of patients with corneal staining
compared to VH group at postoperative 1 and 3 months;
Schirmer ’s I test values were also higher in the HF group,
although this difference was no statistically significant.
However, all the objective sings were not significantly dif-
ferent between the two groups at 6 months postoperatively.
Several mechanisms for dry eye symptoms after LASIK
have been proposed. These include damage to the goblet
cells by suction ring – induced pressure, decreased corneal
sensation and blink reflex, altered tear-film stability caused
by changes in corneal curvature, and medication-induced
effects [23]. Flap creation in LASIK severs all superficial
corneal nerves except at the hinge, which provides a route
for undisturbed innervation. Therefore, the location of the
hinge may be planned to afford the cornea the best sensory
advantage. Some previous studies found greater loss of
corneal sensation and increased dry eye signs and symptoms
in patients having surgery with VF than in those with HF [7,
8, 16]. These findings are supported by the traditional model
of corneal innervation that suggested that the long ciliary
nerves enter the cornea at the 3 o’clock and 9 o’clock
positions, with greater susceptibility to corneal nerve dam-
age with vertically hinged than with horizontally hinged [8].
Our meta-analysis of RCTs showed that compared to a
vertical-hinge location, a horizontal-hinge position lead to
less corneal sensory disturbance, which then resulted in
fewer dry eye complaints from patients. However, the true
distribution of corneal nerves is still controversial and is
Fig. 2 Forest plot of comparison showing tear break-up time in studies comparing LASIK with vertical flap versus horizontal flap at postoperative
1 week, 1, 3, and 6 months
362 Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366
7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 7/10
being elucidated. Müller et al. [24] reported the opposite
finding that leashes extend across the corneal apex prefer-
entially in the 6 to 12 o’clock direction and other leashes
approach the apex in the 5 to 11, 7 to 1, 9 to 3, 2 to 8, and 4
to 10 o’clock directions. Further basic studies are needed to
clear up the subject.
Subjective symptoms are important in the diagnosis and
management of dry eye. Seven studies, including our meta-
analysis, have compared the subjective dry eye symptoms
by a questionnaire method [8 – 10, 19 – 22]. The results were
generally consistent and showed that dry eye symptoms
were increased over preoperative values, but there was no
significant difference between the VF and HF groups at any
time point. However, we did not analyze the subjective
symptoms because not enough studies reported consistently
on the rates or extent in each group to perform a statistical
analysis. There is a limited consensus on how to define dry-
eye disease because symptoms often do not correlate with
clinical signs. Currently, an approach recommended by
Delphi for severity evaluation of dry eye was that combine
objective tests such as central corneal sensation, Schirmer
test with anesthesia, TBUT, corneal fluorescein staining,
and conjunctival lissamine green staining in conjunction
with subjective symptom assessment using the Ocular Sur-
face Disease Index (OSDI) questionnaire [25].
Using the femtosecond laser allows creation of horizon-
tally or vertically oriented flaps with the same keratome.
Two articles included in this study reported that when
performing LASIK with the IntraLase laser and using the
same keratome, hinge position had no effect on corneal
sensation and dry-eye disease parameters [10, 21]. Never-
theless, the femtosecond laser may generate more consistent
and predictable flap diameters and thicknesses than micro-
keratomes [26]. There may also be fewer flap-related com-
plications, including reduced epithelial injury and faster
recovery of corneal sensation with use of femtosecond lasers
[27, 28]. One recent study found that eyes with femtosecond
flaps had a lower incidence of LASIK-associated dry eye
Fig. 3 Forest plot of comparison showing Schirmer's I test in studies comparing LASIK with vertical flap versus horizontal flap at postoperative1 week,1, 3, and 6 months
Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366 363
7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 8/10
and required less treatment for the disorder [29]. A deeper
lamellar dissection is expected to create a larger volume of
tissue through which nerves must regenerate, thus delaying
the return of corneal sensation. [22] Thus, the lower
Fig. 4 Forest plot of comparison showing corneal fluorescein staining in studies comparing for LASIK with vertical flap versus horizontal flap at
postoperative 1 week, 1, 3, and 6 months ( M-H Mantel-Haenszel)
Fig. 5 A funnel plot to explore
publication bias. The standard
error of mean difference of each
trial was plotted against the
mean difference for tear break-
up time. No skewed distribution
was observed, suggesting no
publication bias (the funnel plot
for other primary outcomes was
not represented here)
364 Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366

7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 9/10
incidence of dry-eye signs and symptoms with the femto-
second lasers may be attributed to the creation of thinner
flaps, resulting in greater residual stromal beds and de-
creased corneal denervation. [10, 29]
The present study has limitations that result from the
quality of the individual trials and the methods of the
meta-analysis itself. First, our research was restricted to
studies published in indexed journals or in certain trialregisters and conference proceedings. We did not search
for unpublished studies or original data. Second, the studies
included were heterogeneous in terms of study location,
population, number of patients from different studies, and
basal condition. We must acknowledge that the preoperative
incidence of dry-eye signs and symptoms was low, which
may predispose to a lower postoperative incidence of dry-
eye disease as preexisting dry eye is a risk factor for severe
postoperative dry-eye disease. Third, other factors such as
the degree of preoperative myopia, depth of laser treatment,
and flap thickness may also play a role for developing a dry
eye [7, 20]. This review unfortunately did not comprise a sufficient number of studies to perform subgroup meta-
analyses for these risk factors.
In summary, the present study suggests that hinge loca-
tion of corneal flap dose have some effects on corneal
sensation and the dry eye syndromes after LASIK. Compar-
ing with a vertical hinge flap, a horizontal hinge flap would
lead to less corneal sensory disturbance and dry eye syn-
dromes at early postoperative period, although there was no
significant difference between the groups at 6 months after
surgery. However, due to the fact that multiple factors may
contribute to the disorder, further elucidation of corneal
nerve organization and regrowth patterns may help us un-
derstand how to minimize dry eye after LASIK.
Acknowledgments This research was partly supported by the Fi-
nancing Project of Science and Technology Innovation Plan for Col-
lege Students of Zhejiang Province, China (2011R413047).
References
1. Yu EYW, Leung A, Rao S, Lam DSC (2000) Effect of laser in situ
keratomileusis on tear stability. Ophthalmology 107:2131 – 2135
2. Jabbur NS, Sakatani K, O'Brien TP (2004) Survey of complica-
tions and recommendations for management in dissatisfied patients
seeking a consultation after refractive surgery. J Cataract Refract
Surg 30:1867 – 1874
3. Levinson BA, Rapuano CJ, Cohen EJ, Hammersmith KM, Ayres
BD, Laibson PR (2008) Referrals to the Wills Eye Institute Cornea
Service after laser in situ keratomileusis: reasons for patient dis-
satisfaction. J Cataract Refract Surg 34:32 – 39
4. Ambrosio R Jr, Tervo T, Wilson SE (2008) LASIK-associated dry
eye and neurotrophic epitheliopathy: pathophysiology and strate-
gies for prevention and treatment. J Refract Surg 24:396 – 407
5. Chuck RS, Quiros PA, Perez AC, McDonnell PJ (2000) Corneal
sensation after laser in situ keratomileusis. J Cataract Refract Surg
26:337 – 339
6. Situ P, Simpson TL, Fonn D, Jones LW (2008) Conjunctival and
corneal pneumatic sensitivity is associated with signs and symp-
toms of ocular dryness. Invest Ophthalmol Vis Sci 49:2971 – 2976
7. Vroman DT, Sandoval HP, Fernandez de Castro LE, Kasper TJ,
Holzer MP, Solomon KD (2005) Effect of hinge location on
corneal sensation and dry eye after laser in situ keratomileusis
for myopia. J Cataract Refract Surg 31:1881 – 18878. Donnenfeld ED, Solomon K, Perry HD, Doshi SJ, Ehrenhaus M,
Solomon R, Biser S (2003) The effect of hinge position on corneal
sensation and dry eye after LASIK. Ophthalmology 110:1023 –
1029, discussion 1029-1030
9 . G h or ei s hi M , A i de nl oo N S, P ey ma n A , P ey ma n M ,
Haghdoustoskoey M (2005) Does hinge position affect dry
eye after laser in situ keratomileusis? Ophthalmologica
219:276 – 280
10. Mian SI, Shtein RM, Nelson A, Musch DC (2007) Effect of hinge
position on corneal sensation and dry eye after laser in situ kera-
tomileusis using a femtosecond laser. J Cataract Refract Surg
33:1190 – 1194
11. Pogue J, Yusuf S (1998) Overcoming the limitations of current
meta-analysis of randomised controlled trials. Lancet 351:47 – 52
12. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF(1999) Improving the quality of reports of meta-analyses of rand-
omised controlled trials: the QUOROM statement. Quality of
Reporting of Meta-analyses. Lancet 354:1896 – 1900
13. Verhagen AP, de Vet HC, de Bie RA, Kessels AG, Boers M,
Bouter LM, Knipschild PG (1998) The Delphi list: a criteria list
for quality assessment of randomized clinical trials for conducting
systematic reviews developed by Delphi consensus. J Clin
Epidemiol 51:1235 – 1241
14. Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003)
Measuring inconsistency in meta-analyses. BMJ 327:557 – 560
15. Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in
meta-analysis detected by a simple, graphical test. BMJ 315:629 –
634
16. Kumano Y, Matsui H, Zushi I, Mawatari A, Matsui T, Nishida T,
Miyazaki M (2003) Recovery of corneal sensation after myopic
correction by laser in situ keratomileusis with a nasal or superior
hinge. J Cataract Refract Surg 29:757 – 761
17. Holzer MP, Vargas LG, Sandoval HP, Vroman DT, Kasper TJ,
Brown SJ, Apple DJ, Solomon KD (2003) Corneal flap complica-
tions in refractive surgery: Part 1: development of an experimental
animal model. J Cataract Refract Surg 29:795 – 802
18. Assil KK, McCall T (2005) Temporal hinge laser in situ kerato-
mileusis: maximizing treatable stromal bed area. J Cataract Refract
Surg 31:1139 – 1144
19. Lee KW, Joo CK (2003) Clinical results of laser in situ keratomi-
leusis with superior and nasal hinges. J Cataract Refract Surg
29:457 – 461
20. De Paiva CS, Chen Z, Koch DD, Hamill MB, Manuel FK, Hassan
SS, Wilhelmus KR, Pflugfelder SC (2006) The incidence and risk
factors for developing dry eye after myopic LASIK. Am J
Ophthalmol 141:438 – 445
21. Mian SI, Li AY, Dutta S, Musch DC, Shtein RM (2009) Dry eyes
and corneal sensation after laser in situ keratomileusis with fem-
tosecond laser flap creation. Effect of hinge position, hinge angle,
and flap thickness. J Cataract Refract Surg 35:2092 – 2098
22. Nassaralla BA, McLeod SD, Boteon JE, Nassaralla JJ Jr (2005)
The effect of hinge position and depth plate on the rate of recovery
of corneal sensation following LASIK. Am J Ophthalmol
139:118 – 124
23. Wilson SE (2001) Laser in situ keratomileusis-induced (presumed)
neurotrophic epitheliopathy. Ophthalmology 108:1082 – 1087
Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366 365

7/17/2019 Feng et al.pdf
http://slidepdf.com/reader/full/feng-et-alpdf 10/10
24. Muller LJ, Marfurt CF, Kruse F, Tervo TM (2003) Corneal nerves:
structure, contents and function. Exp Eye Res 76:521 – 542
25. Smith J, Nichols KK, Baldwin EK (2008) Current patterns in the
use of diagnostic tests in dry eye evaluation. Cornea 27:656 – 662
26. Friedlaender MH (2006) LASIK surgery using the IntraLase fem-
tosecond laser. Int Ophthalmol Clin 46:145 – 153
27. Binder PS (2004) Flap dimensions created with the IntraLase FS
laser. J Cataract Refract Surg 30:26 – 32
28. Lim T, Yang S, Kim M, Tchah H (2006) Comparison of the
IntraLase femtosecond laser and mechanical microkeratome
for laser in situ keratomileusis. Am J Ophthalmol 141:833 –
839
29. Salomao MQ, Ambrosio R Jr, Wilson SE (2009) Dry eye
associated with laser in situ keratomileusis: mechanical micro-
keratome versus femtosecond laser. J Cataract Refract Surg
35:1756 – 1760
366 Graefes Arch Clin Exp Ophthalmol (2013) 251:357 – 366





























