Embed Size (px)
Citation preview

1/29/2014
1
Femur Fractures:Case-based solutions to common
problems with intramedullary nailingG Bl i d ll MDGreg Blaisdell, MD
New Hampshire Orthopaedic Center
I have no disclosures
ObjectivesReview common problems in femur fracture care
Pre-operative decision making
Case-based examples to help avoid complications with:
Subtrochanteric fractures
Femoral shaft fractures
Distal femur fractures
Subtrochanteric femur fractures
Don’t let these be your x-rays!
Subtrochanteric femur fractures
Flexion and external rotation of proximal fragment
Need more information pre-poperatively typically
Does it extend into the intertrochanteric zone?
-Has affect on nail choice
Subtrochanteric femur fractures
Traction Views are HELPFUL

1/29/2014
2
Positioning supine on fracture table
Good reduction! Quick Case!
Right?
Get a lateral or Prep and Drape?p
Options:
Supine vs. Lateral
Fracture table/Free leg
WRONG
Proximal guidewireposition CRITICAL
R d ti idReduction aids:
Percutaneous elevators, bone hooks, unicortical schanz pins, external manipulation, leg elevator
Reaming while in a malreduced position cannot be overcome by the nail
Opening reamer dictates nail pathway
Trochanteric start nails: Guidewire on medial slope of tip.
Fight the soft tissues!
Piriformis Greater Troch
Starting point: Does it matter?
Piriformis vs. trochanteric start point: No significant difference (Starr, JOT 2006)
Trochanteric entry on medial edge of trochanteric tip
Subtrochanteric femur fractures Clamp reduction +/- Cable for spiral fractures
Fracture table – Will this reduce?
Cables – Excellent reduction aid for spiral fractures
-Afsari et al, JBJS-A 2009

1/29/2014
3
Re-create the tube
Don’t crimp until nail is seated and proximal screw(s) are in
Femoral shaft fracturesAntegrade vs. Retrograde
Fracture table vs. Free-leg
Antegrade:
Piriformis vs. trochanteric
How many locking screws
Reamed vs. Unreamed
Gold Standard: Antegrade nailing,
statically locked, REAMED
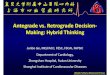
Shaft fracturesAvoiding Malrotation
Bråten et al. Acta Orthop Scand 1992
Normal variation in anteversion exists between sides
2 standard deviations is 11-13°
J t l J O th T 2004Jaarsma et al. J Orthop Trauma 2004
Clinical judgment alone is poor
Supine: 42% > 20° malrotation
Prone: 25% > 20° malrotation Not good!
Shaft fracturesAvoiding Malrotation
Tornetta et al. J Trauma 1995
Lateral only technique
Perfect lateral of uninjured hip
Perfect lateral of uninjured knee
Measure difference to get anteversion
Correct fractured limb
12 patients, avg 5° (0-8°)
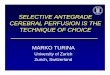
Shaft fracturesAvoiding Malrotation
Deshmukh et al. Injury 1998
Lesser trochanteric Profile
Start with perfect lateral knee
Rotate flouro 90 get AP hipRotate flouro 90, get AP hip
Compare lesser trochanter profiles
5 patients, all <10° variation
Occasionally not much of a profile!
Shaft fracturesAvoiding Malrotation
MOST IMPORTANT
GET PRE-OPERATIVE IMAGES OF UNINJURED LEG
BASE ALL PROFILE IMAGING OFF OF PERFECT LATERAL OF KNEE
AP KNEE AND AP HIP SHOULD BE 90° FROM PERFECT KNEE LATERAL
NOT SURE? GET A CT

1/29/2014
4
Shaft fracturesDealing with Malrotation
Lindsey and Krieg, JAAOS 2011
If unsure of rotation at index nailing procedure:
Consider single interlocking screw above and below fracture
Shaft fracturesAvoiding leg length inequality
Measure! Radiolucent ruler
Clinical check before extubation
CTCT scanogram
Discuss pre-operatively (Winquist 3 and 4 especially)
Shaft fracturesAvoiding leg length inequality
Vaiyda et al. Injury 2012
28 patients Winquist 3 or 4
Only 64% had <10 mm LLDy
16% LLD 10-15mm11% LLD 15-20mm11% LLD >20mm
5 patients underwent correction
What’s the cut-off?
Femoral shaft fracturesWinquist classification associated with malalignment
Malalignment:
Proximal/distal fractures worse than mid-diaphyseal
More likely when antegrade nailing distal fractures
More likely when retrograde nailing proximal fractures
Ricci JOT 2001
Blocking screws/wires
Krettek et al. JBJS-Br 1999
Success in preventing/treating malalignment in tibia fractures
Unreamed nailing technique
Diaphyseal blocking screw less successful in reamed nailing
Concave side of deformity
Extrapolated to femoral shaft fractures proximal/distal to diaphysis
Krettek et al., Injury 1999
Blocking screws/wires
Ostrum and Maurer JOT 2009
Blocking screw use in retrograde IMN distal 1/3 femur
No angular deformityNo angular deformity
Small group (5 patients)
Shahulhameed et al Injury 2011
Technical recommendation of Steinmann pins to effect blocking of nail malposition

1/29/2014
5
Blocking screws/wiresTechnical Example
Blocking screws/wiresTechnical Example
Blocking screws/wiresTechnical Example
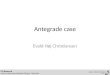
Starting point and guidewire direction are ESSENTIAL
Blocking screws/wiresTechnical Example
Re-establish posterior cortex Concave side of deformity
The Set-Up

1/29/2014
6
Anterior-posterior Steinmann pin leaves a mild deformityUse reduction tool to hold guidewire out of way for second Steinmann
Small adjustment of pin
Be careful inserting rod (can create new comminution)
Distal femur fractures:Combining ORIF with IMN
Thomson et al Orthopedics 2008Lower malunion, secondary bone grafting, nonunion compared to ORIF
Garnavos et al. Injury 2012Prospectively followed 17 patientsNo malunions or nonunionNo malunions or nonunionPartial weight-bearing by 6 weeks
Limitations:Extensive intra-articular comminutionInability to gain purchase with interlocks
Combining ORIF with IMNPerfect guidewire alignment
to avoid nail-induced malreduction
Lag screws recreate distal block
Keep lags out of nail path
Open reduction of joint, parapatellar vs. lateral
Choose a nail with multi-planar locking
Avoid short nails

1/29/2014
7
Reduction tool -Find proximal fragment easier-Better control of distal fragment than with external manipulationp
Can guide position of blocking screws if needed
Every company makes one – If it isn’t in the set in your hospital, it can be
Conclusions• Advanced femoral nailing techniques have provided
major advancements in femur fracture care
• Must respect limitations and overlooked problems with nailing
• Cannot treat all femoral nail cases like a mid-diaphyseal nailing of a simple fracture
• Use available techniques to make fractures straighter, better aligned, without rotational or length abnormalities
Thank You
Greg Blaisdell, MD
603-883-0091 work603 883 0091 work