Embed Size (px)
Citation preview
Eur J Orthop Surg Traumatol (2012) 22:423–426
DOI 10.1007/s00590-011-0792-zUP-TO DATE REVIEW AND CASE REPORT
Femoral shaft fracture below a pre-existing implant: a novel method of Wxation: a case report
Varatharaj Mounasamy · Jibananada Satpathy · Mark C. Willis Jr.
Received: 24 February 2011 / Accepted: 28 February 2011 / Published online: 12 March 2011© Springer-Verlag 2011
Abstract Femoral shaft fractures below or above a pre-existing implant in the elderly are not uncommon, and theideal management of these fractures is not well deWned. Wereport the use of a retrograde femoral nail for a femoralshaft fracture, linked to a pre-existing hip plate screw con-struct by locking the nail through the distal two holes of theplate. We were able to achieve a biomechanically stableconstruct with no gapped areas and no stress risers in oste-openic bone. This technique is one of the various methodsthat can be chosen to Wx a fracture with a pre-existingimplant proximally.
Keywords Fracture · Dynamic hip screw · Retrograde nail
Introduction
Fractures of the femur in the elderly are increasing as aresult of the longevity of the general population, and hipfractures constitute a signiWcant percentage of all femurfractures in the elderly. Femoral shaft fractures below a pre-existing hip fracture are not uncommon, and the bestmethod of management of these fractures is not well deW-ned. Removal of the hip implant if the fracture has healedand Wxation of the femoral shaft fracture with an antegradenail with a cephalomedullary screw would be ideal. Retro-grade nail and plate Wxation would be the other surgical
implants of choice. Pre-existing implants proximally or dis-tally limit implant selection and segments of femur that areunprotected by Wxation devices areas after Wxation createstress risers and are susceptible to fracture.
We present in this case report of an 86-year-old commu-nity ambulator with a relatively displaced midshaft femurfracture with a pre-existing dynamic hip screw in whom weextended the Wxation proximally and linked the retrogradenail to the pre-existing implant to create a biomechanicallystable construct.
Case report
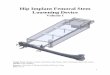
An 86-year-old female community ambulator presentedwith pain and swelling over her right thigh after a groundlevel fall. Her medical and family histories were noncon-tributory. She had undergone surgery for Wxation of a rightintertrochanteric fracture in the past. Physical examinationrevealed tenderness over the right thigh. There were nooverlying skin changes. Healed surgical scars were seenproximally over her right hip. The neurovascular status ofthe involved extremity was intact. Plain radiographsrevealed a right midshaft femur fracture with a butterXyfragment and signiWcant osteopenia (Fig. 1a–c). Radio-graphs of the pelvis revealed a healed intertrochantericfracture with dynamic hip screw construct in situ. Risk ben-eWts and alternatives of treatment were explained to thepatient, and she preferred operative intervention and earlyreturn to pre-injury level of ambulation.
In supine position on a radiolucent table, we incisedthrough the patient’s previous scar on the lateral side of theright hip, and after reaching the plate, we removed all thefour screws from the DHS plate. We then through the kneeplaced a retrograde nail in the usual fashion after reducingthe fracture and minimal reaming.
V. Mounasamy (&) · J. Satpathy · M. C. Willis Jr.Department of Orthopedics, Virginia Common Wealth University Health System, 1200 East Broad Street, 9th Floor West Hospital, PO Box 980153, Richmond, VA 23298-0153, USAe-mail: [email protected]
123
424 Eur J Orthop Surg Traumatol (2012) 22:423–426
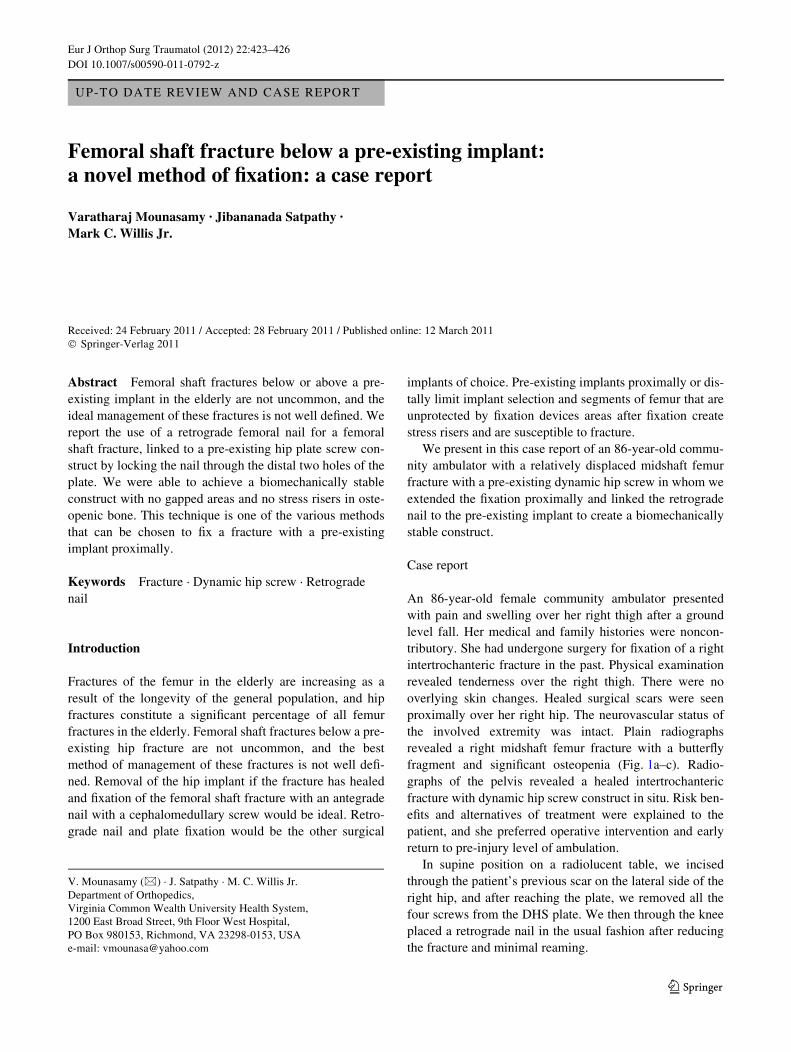
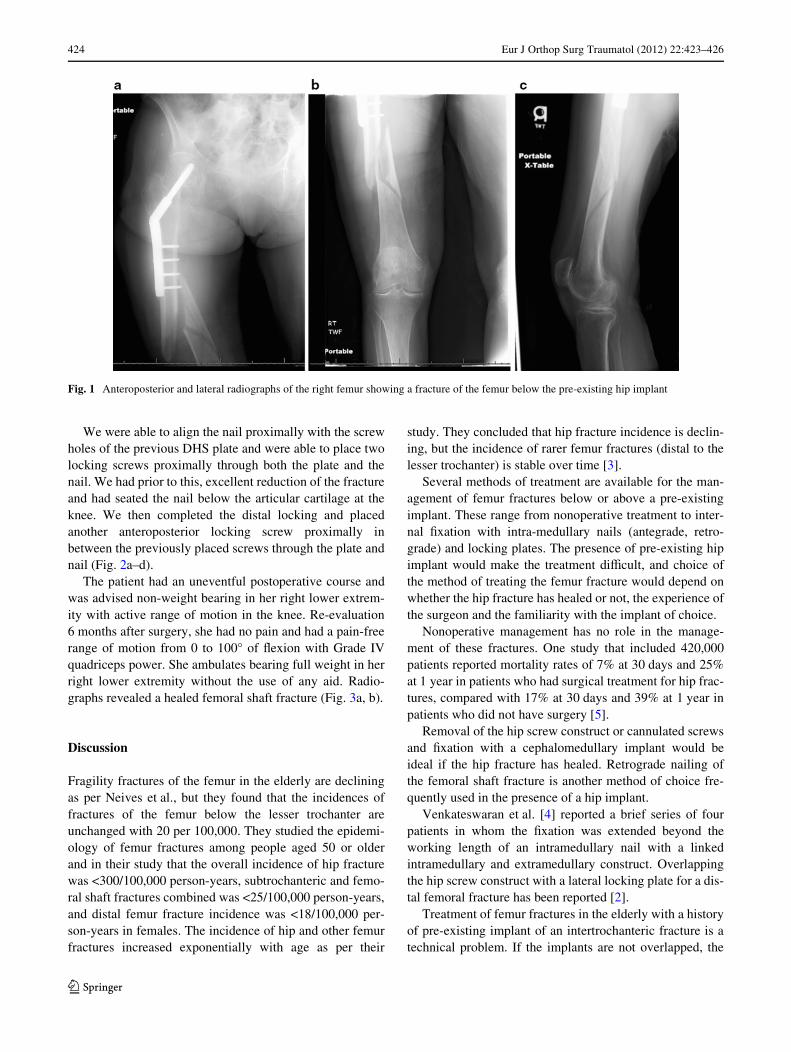
We were able to align the nail proximally with the screwholes of the previous DHS plate and were able to place twolocking screws proximally through both the plate and thenail. We had prior to this, excellent reduction of the fractureand had seated the nail below the articular cartilage at theknee. We then completed the distal locking and placedanother anteroposterior locking screw proximally inbetween the previously placed screws through the plate andnail (Fig. 2a–d).
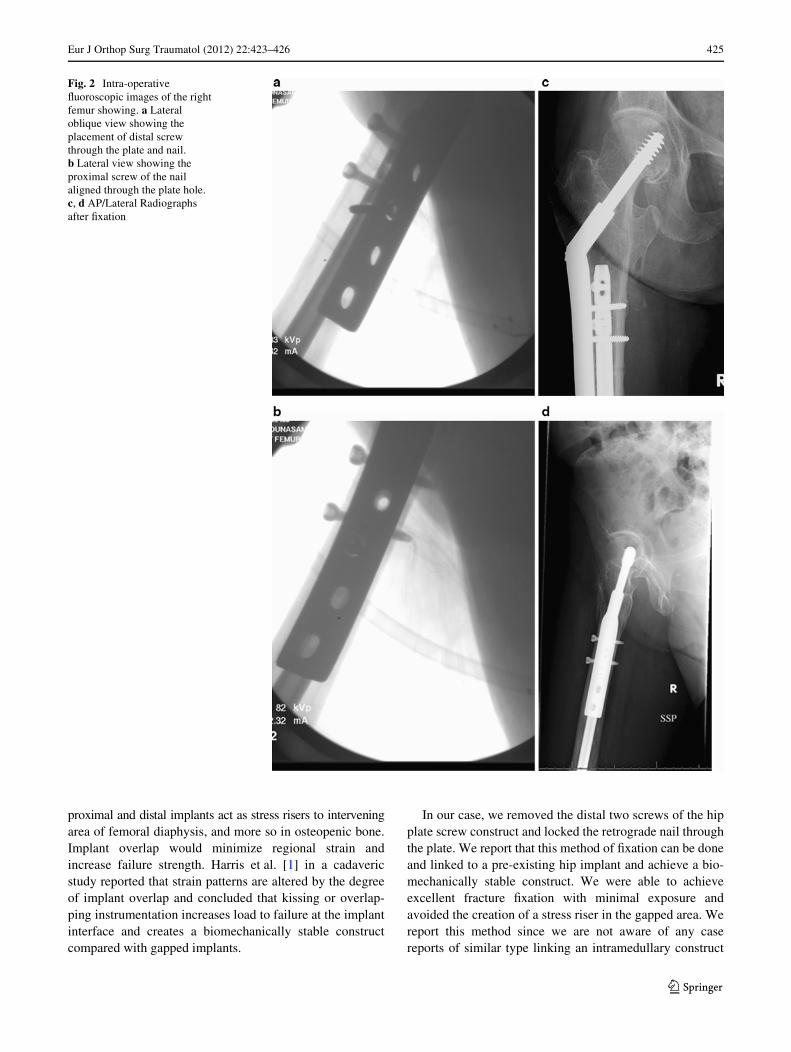
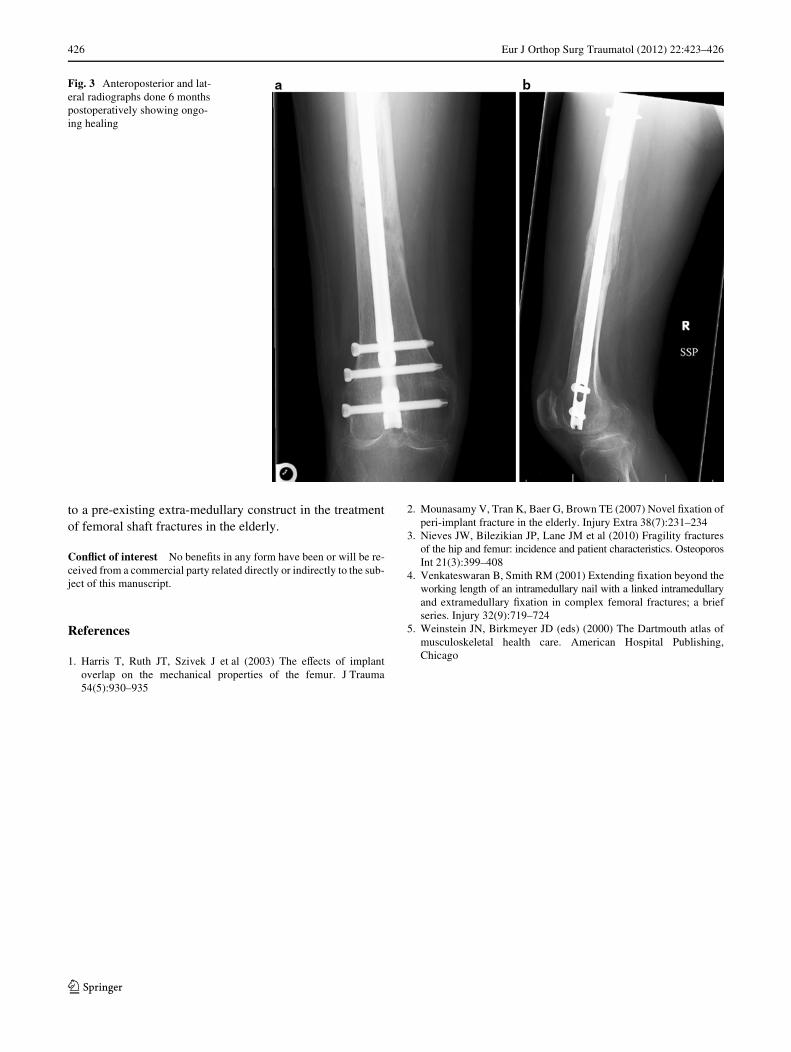
The patient had an uneventful postoperative course andwas advised non-weight bearing in her right lower extrem-ity with active range of motion in the knee. Re-evaluation6 months after surgery, she had no pain and had a pain-freerange of motion from 0 to 100° of Xexion with Grade IVquadriceps power. She ambulates bearing full weight in herright lower extremity without the use of any aid. Radio-graphs revealed a healed femoral shaft fracture (Fig. 3a, b).
Discussion
Fragility fractures of the femur in the elderly are decliningas per Neives et al., but they found that the incidences offractures of the femur below the lesser trochanter areunchanged with 20 per 100,000. They studied the epidemi-ology of femur fractures among people aged 50 or olderand in their study that the overall incidence of hip fracturewas <300/100,000 person-years, subtrochanteric and femo-ral shaft fractures combined was <25/100,000 person-years,and distal femur fracture incidence was <18/100,000 per-son-years in females. The incidence of hip and other femurfractures increased exponentially with age as per their
study. They concluded that hip fracture incidence is declin-ing, but the incidence of rarer femur fractures (distal to thelesser trochanter) is stable over time [3].
Several methods of treatment are available for the man-agement of femur fractures below or above a pre-existingimplant. These range from nonoperative treatment to inter-nal Wxation with intra-medullary nails (antegrade, retro-grade) and locking plates. The presence of pre-existing hipimplant would make the treatment diYcult, and choice ofthe method of treating the femur fracture would depend onwhether the hip fracture has healed or not, the experience ofthe surgeon and the familiarity with the implant of choice.
Nonoperative management has no role in the manage-ment of these fractures. One study that included 420,000patients reported mortality rates of 7% at 30 days and 25%at 1 year in patients who had surgical treatment for hip frac-tures, compared with 17% at 30 days and 39% at 1 year inpatients who did not have surgery [5].
Removal of the hip screw construct or cannulated screwsand Wxation with a cephalomedullary implant would beideal if the hip fracture has healed. Retrograde nailing ofthe femoral shaft fracture is another method of choice fre-quently used in the presence of a hip implant.
Venkateswaran et al. [4] reported a brief series of fourpatients in whom the Wxation was extended beyond theworking length of an intramedullary nail with a linkedintramedullary and extramedullary construct. Overlappingthe hip screw construct with a lateral locking plate for a dis-tal femoral fracture has been reported [2].
Treatment of femur fractures in the elderly with a historyof pre-existing implant of an intertrochanteric fracture is atechnical problem. If the implants are not overlapped, the
Fig. 1 Anteroposterior and lateral radiographs of the right femur showing a fracture of the femur below the pre-existing hip implant
123
Eur J Orthop Surg Traumatol (2012) 22:423–426 425
proximal and distal implants act as stress risers to interveningarea of femoral diaphysis, and more so in osteopenic bone.Implant overlap would minimize regional strain andincrease failure strength. Harris et al. [1] in a cadavericstudy reported that strain patterns are altered by the degreeof implant overlap and concluded that kissing or overlap-ping instrumentation increases load to failure at the implantinterface and creates a biomechanically stable constructcompared with gapped implants.
In our case, we removed the distal two screws of the hipplate screw construct and locked the retrograde nail throughthe plate. We report that this method of Wxation can be doneand linked to a pre-existing hip implant and achieve a bio-mechanically stable construct. We were able to achieveexcellent fracture Wxation with minimal exposure andavoided the creation of a stress riser in the gapped area. Wereport this method since we are not aware of any casereports of similar type linking an intramedullary construct
Fig. 2 Intra-operative Xuoroscopic images of the right femur showing. a Lateral oblique view showing the placement of distal screw through the plate and nail. b Lateral view showing the proximal screw of the nail aligned through the plate hole. c, d AP/Lateral Radiographs after Wxation
123
426 Eur J Orthop Surg Traumatol (2012) 22:423–426
to a pre-existing extra-medullary construct in the treatmentof femoral shaft fractures in the elderly.
ConXict of interest No beneWts in any form have been or will be re-ceived from a commercial party related directly or indirectly to the sub-ject of this manuscript.
References
1. Harris T, Ruth JT, Szivek J et al (2003) The eVects of implantoverlap on the mechanical properties of the femur. J Trauma54(5):930–935
2. Mounasamy V, Tran K, Baer G, Brown TE (2007) Novel Wxation ofperi-implant fracture in the elderly. Injury Extra 38(7):231–234
3. Nieves JW, Bilezikian JP, Lane JM et al (2010) Fragility fracturesof the hip and femur: incidence and patient characteristics. OsteoporosInt 21(3):399–408
4. Venkateswaran B, Smith RM (2001) Extending Wxation beyond theworking length of an intramedullary nail with a linked intramedullaryand extramedullary Wxation in complex femoral fractures; a briefseries. Injury 32(9):719–724
5. Weinstein JN, Birkmeyer JD (eds) (2000) The Dartmouth atlas ofmusculoskeletal health care. American Hospital Publishing,Chicago
Fig. 3 Anteroposterior and lat-eral radiographs done 6 months postoperatively showing ongo-ing healing
123