-
8/12/2019 Federman - Physicians' Opinions About Reforming
Reimbursement
1/8
HEALTHCAREREFORM
ORIGINAL INVESTIGATION
Physicians Opinions About Reforming Reimbursement
Results of a National Survey
Alex D. Federman, MD, MPH; Mark Woodward, PhD; Salomeh Keyhani,
MD, MPH
Background:Several strategies have been proposed toreform
physician reimbursement while improving qual-ity of care. Despite
much debate, physicians opinions re-garding reimbursement reform
proposals have not beenobjectively assessed.
Methods:We conducted a national survey of ran-domly selected
physicians between June 25 and Octo-
ber 31, 2009. Physicians rated their support for
severalreimbursement reform proposals: rewarding quality
withfinancial incentives, bundling payments for episodes ofcare,
shifting payments from procedures to manage-ment and counseling
services, increasing pay to gener-alists, and offsetting increased
pay to generalists with areduction in pay for other specialties.
Support for the dif-ferent reform options wascompared with
physician prac-tice characteristics.
Results:The response rate was 48.5% (n=1222). Fourof 5
physicians (78.4%) indicated that under Medicare,
some procedures are compensated too highly and oth-ers are
compensated at rates insufficient to cover costs.Incentives were
themost frequently supportedreformop-tion (49.1%), followed by
shifting payments (41.6%) andbundling (17.2%). Shifting payments
and bundling weremore commonly supported by generalists than by
other
specialists. There was broad support for increasing payfor
generalists (79.8%), but a proposal to offset the in-crease with a
3% reduction in specialist reimbursementwas supported by only 39.1%
of physicians.
Conclusions:Physicians are dissatisfied with
Medicarereimbursement and show little consensus for major
pro-posals to reform reimbursement. The successful adop-tion of
payment reform proposals may require a betterunderstanding of
physicians concerns and their willing-ness to make tradeoffs.
Arch Intern Med. 2010;170(19):1735-1742
ACROSS THE POLITICAL SPEC-trum, there is generalagreement that
the cost ofhealth care has risen to un-tenablelevelsand is
threat-
ening the future of Medicare and the eco-nomic well-being of the
United States.1,2
These concerns have prompted various
proposals intended to bend the costcurve of health care
expenditures whilemaintainingor improving health carequal-ity.
Physicians account for only one-fifthof health care costs, but
their clinical de-cisions and patterns of use are a major fac-tor
in rising health care costs; thus, manyproposals have eyed
physician reimburse-ments as potential targets to promote
costsavings and establish incentives to im-prove care.3,4
A variety of strategies have been pro-posed to reform physician
payment.5 Onewidely advocated approach is the use offinancial
incentives, such as bonuses (payfor performance) for meeting
quality stan-dards that reflect good process of care or
good health outcomes6 or financialpenalties for delivering
substandard care,as measured by high hospital readmis-sion
rates.7,8 Also gaining considerable at-tention are 2 strategies to
promote greateraccountability by physicians or health caresystems
for quality andcost: bundling pay-ments and promotion of
accountable careorganizations.2,7,9 Bundling lays the
re-sponsibility for containing costs and en-suring quality on the
physician or healthcare system by paying a fixed amount for
See also page 1728
See Invited Commentaryat end of article
Author Affiliations:Division ofGeneral Internal Medicine(Drs
Federman, Woodward, andKeyhani) and Department ofHealth Policy (Dr
Keyhani),Mount Sinai School ofMedicine, New York, New York;and
James J. Peters VeteransAdministration Medical Center,Bronx, New
York (Dr Keyhani).
ARCH INTERN MED/ VOL 170 (NO. 19), OCT 25, 2010
WWW.ARCHINTERNMED.COM1735
2010 American Medical Association. All rights
reserved.(REPRINTED WITH CORRECTIONS)
wnloaded From: http://archinte.jamanetwork.com/ by a Johns
Hopkins University User on 01/22/2014
-
8/12/2019 Federman - Physicians' Opinions About Reforming
Reimbursement
2/8
an episode of care or for a set of services bundled undera
specific episode of care, much in the way that hospi-tals are
reimbursed for care bundled under the inpatientprospective care
system.10,11 Similarly, accountable careorganizations, which are
extended networks of hospi-tals and outpatient providers, would
have responsibilityfor total health care spending and quality of
care for aset of patients. Bundling of services and accountable
careorganizations are both promoted in the Patient Protec-tion and
Accountable Care Act of 2010.12
Finally, the Patient Protection and Accountable CareAct also
addresses the growing need for preventive careand care coordination
by inceasing Medicare and Med-icaid payments to generalist
physicians.12 Additionally,the Center for Medicare and Medicaid
Services recentlyannounced plans to expand multiple procedure
pay-ment reduction for imaging and therapy services.13 Com-bined,
these strategies aim to increase the provision ofpreventive health
care, promote health maintenance, andreduce excesive testing.14
Given the controversies in modifying paymentsto phy-sicians to
controlcosts,policymakers shouldconsider howphysicians view the
different options. Physicians expe-riences may help optimize the
design of reimbursementreforms. In addition, maximizing physicians
approval ofreforms would facilitate implementation. Although
pre-vious research has assessed physicians views on healthcare
system financing options, to our knowledge,15 therehave been no
systematic evaluations of physicians viewson reimbursement reform.
We, therefore, conducted anational survey to assess physicians
opinions about dif-ferent strategies to reform physician
reimbursement, pro-mote quality of care, and enhance health care
savings.
METHODS
SAMPLE
In April 2009, we obtained data on a stratified sample of
6000physicians randomly selected from among 849 213 physicians
inthe American Medical Association (AMA) Physician Masterfile.The
AMA Physician Masterfile includes current data on all USphysicians,
regardless of AMA affiliation. Physicians were strati-fied into 4
specialty groups:primary care(internists,familyprac-titioners, and
pediatricianswithout subspecialtytraining); medi-cal and pediatrics
subspecialists, neurologists, and psychiatrists;surgical
specialists and subspecialists (general surgeons, surgi-cal
subspecialists, and obstetrician/gynecologists); and the re-maining
specialties. Equal numbers of physicians were ran-domly sampled for
eachstratum. The study was approved by theMount Sinai School of
Medicine institutional review board.
SURVEY DEVELOPMENT
We empanelled 7 nationally recognized physician leaders
andhealth policy and survey research experts and engaged themin a
modified Delphi process to develop content for the sur-vey.16We
drafted survey questions and asked the expert panelto rank these
items by policy relevance. To refine the ques-tions and uncover new
themes, we conducted 1-to-1 cognitiveinterviews with 16 physicians
from 7 statesin personor by tele-phone.Physicianswere selected from
a variety of practice back-grounds (private practice, salaried
physicians, practice own-
ers, and hospitalists) and specialty backgrounds (primary
careproviders and medical and surgical subspecialists). The sur-vey
questions were refined through this process until no newcontent
themes and no misinterpretations of the survey itemswere
identified.The survey was pilot tested on 15 internal medi-cine
physicians at Mount Sinai Hospital and had an averagecompletion
time of less than 4 minutes.
SURVEY ADMINISTRATION
We adopted the total design method to optimize the
physiciansurvey response.17-22 This approach minimized respondent
bur-den by using a brief (3-page, 4-minute) survey with
personal-ized content (a personalizedletter, a signedcoverletter,
andpost-age stamps) and follow-up contacts. The survey was mailed
in 3waves. Thefirst wave included a cover letter,thesurvey,a
stampedreturn envelope, and a $2 bill. Subsequent waves didnot
includea monetary incentive. Physicians were called after eachwave
wasmailed to encourage them to complete thesurveyand to offer
themthe option of returning it by fax or by e-mail.
Physicians were randomly chosen to receive 1 of 2 ver-sions of
the survey. The 2 versions shared corecontent (eg, opin-ions about
insurance coverage expansions and practice and pro-fessional
characteristics) but differed by 4 to 6 supplementalquestions,
including questions about physician reimburse-ment. Thus,
approximately half of the sample was asked aboutreimbursement.
Thefirstof 3 survey waves of theNationalPhy-sicians Survey on
Health Care Reform began on June 25, 2009,and the third survey wave
was initiated on August 27, 2009.Data collection was completed on
October 31, 2009.
OUTCOME MEASURES
The survey included 6 questions about physicians opinions
re-garding reimbursement and reimbursement reform
proposals(eAppendix; http://www.archinternmed.com). The first
ques-tion addressed equitability of Medicare reimbursements by
ask-ing physicians to express their level of agreement with the
fol-lowing statement: With the current Medicare
reimbursementsystem, some proceduresare compensatedtoo highly and
oth-ers are compensated at rates insufficient to cover costs.
Re-sponseoptions on the 5-point Likert scale rangedfrom
stronglyagree (5) to strongly disagree (1). Next, we asked
physiciansto express their level of support for 3 proposals for
reformingreimbursement: rewardingquality withfinancial incentives,
bun-dling paymentsfor episodes of care, and shiftingpayments
fromprocedural care to management and counseling services.
Variables captured on both surveyversionsincluded time spenton
clinical dutieseachweek, practiceownership, paymentmecha-nism
(salary only, salary andbonus, from billing only, shift orhourly
wage, or other), and professional society affiliation. Dataobtained
from the AMA Physician Masterfile included date ofbirth, sex,
state,zip code, specialty, training level (current traineeor
training completed), and type of practice (office based, hos-pital
based, administrative, teaching, research, resident, locumtenems,
or other).Zip code data wereused to determine whether
the practice site was rural or urban.
STATISTICAL ANALYSIS
TheanalysesexcludedphysiciansfromUSterritoriesbecausehealthcarereformmaynotbeasrelevanttothemandphysiciansintrain-ing
because of their limited experience with reimbursement.
Wecalculatedtheresponse andrefusal rates using
standardmethods,23
and we compared the characteristics of respondents and
nonre-spondents usingt and2 tests anddata available in theAMA
Phy-sician Masterfile. The associations between support for the
pro-
ARCH INTERN MED/ VOL 170 (NO. 19), OCT 25, 2010
WWW.ARCHINTERNMED.COM1736
2010 American Medical Association. All rights
reserved.(REPRINTED WITH CORRECTIONS)
wnloaded From: http://archinte.jamanetwork.com/ by a Johns
Hopkins University User on 01/22/2014
-
8/12/2019 Federman - Physicians' Opinions About Reforming
Reimbursement
3/8
posedreformsand physicianspecialtyand practice
characteristicswereevaluatedusinglogisticregressionadjustingforphysicianprac-ticecharacteristics.Fortheregressionanalyses,the5outcomes(sup-portfordifferentpayment
reforms and increased payment for pri-mary care) were dichotomized
as strongly or somewhat supportvs unsure or do not support. Weights
were used to adjust for the
stratifiedsamplingdesign,andalltheanalyseswereperformedusingthe
survey sampling and analysis procedures in SAS version 9.1(SAS
Institute Inc, Cary, North Carolina).
RESULTS
SURVEY RESPONSE
Of the 6000 physicians, 794 (13.2%) were trainees, 218(3.6%) had
their surveys returned by the postal service
due to a wrong address, 49 (0.8%) lived in a US terri-tory, and
5 (0.1%) were reported as deceased. Of the4934eligible individuals,
2441 responded, for a final re-sponse rateof 49.5%. Of the 2518
eligible physicians whoreceived the survey addressing reimbursement
reform,there were 1222 respondents (response rate, 48.5%).There
were no significant differences between respon-dents and
nonrespondents regarding age, sex, specialtygroup, geographic
region, and office-based practice set-ting (Table 1).
PARTICIPANT CHARACTERISTICS
Themeanageofthesamplewas51.6years,73.1%weremen,and77.2%practicedin
office-basedsettings.More
thanhalfoftherespondentswerepracticeownersorpartners(58.4%),andmostreportedacceptingMedicare(82.0%);39%receivedperformance
bonuses in addition to their salary.
CURRENT OPINIONON MEDICARE REIMBURSEMENTS
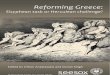
Most physicians (78.4%) indicated that Medicare reim-bursements
are inequitable. There was little differencein attitude about the
equitability of Medicare reimburse-ment across physician
specialties (P =.07) (Figure 1).Of physicians who accepted
Medicare, 40.2% stronglyagreed and 38.2% somewhat agreed that under
Medi-care, some procedures are compensated too highly andothers are
compensated at rates insufficient to cover costs.Only 11.5% of
physicians disagreed with the statement,and 10.2% were unsure.
There were no significant dif-
ferences in opinion regarding Medicare reimbursementacross any
of the physician variables (data not shown).
SUPPORT FOR PROPOSALS TO REFORMPHYSICIAN REIMBURSEMENT
Of the 3 reimbursement reform proposals, physiciansshowed the
highest level of support for the use of incen-tives to improve
quality, with approximately half (49.1%)strongly or somewhat
supporting this approach. Sup-port for incentive-based reform was
similar across phy-
Table 1. Characteristics of Respondentsand Nonrespondentsa
VariableRespondents
(n=1222)Nonrespondents
(n=1296)P
Value
Age, mean (SD), y 51.6 (11.9) 50.9 (12.0) .82
Male sex, % 73.1 71.5 .39
Specialty, %
.78
General practice 26.7 26.8
Medical subspecialty 24.6 25.8
Surgery 24.2 24.5
Other 24.6 22.9
Census region, %
.20
West 21.2 23.0
Midwest 20.5 21.5
South 35.6 31.6
Northeast 22.8 24.0
Census division, %
.15
Pacific 14.7 17.4
Mountain 6.5 5.6
West North Central 6.6 5.3
West South Central 10.3 9.4
East North Central 13.8 16.2
East South Central 5.0 4.7
South Atlantic 20.3 17.4
Middle Atlantic 16.6 17.7
New England 6.1 6.2Urban practice location, % 91.0 91.7 .55
Office-based practice, % 77.2 75.5 .31
Practice ownerb 58.4 NA NA
Patient care20 h, wkb 84.5 NA NA
Insurance/paymentaccepted, %b
NA
Medicare 82.0 NA
Medicaid 73.5 NA
Private 88.0 NA
Cash 86.5 NA
Other 18.4 NA
Not applicable 7.3 NA
Source of income, %b
NA
Salary only 26.2 NA
Salarybonus 39.0 NA
Billing only 18.9 NAShift work/hourly wages 5.3 NA
Other 10.6 NA
Abbreviation: NA, not available.a Values are based on unweighted
data.b These variables were not available in the American Medical
Association
Physician Masterfile.
100
90
80
70
60
50
40
30
1020
0Generalists Medical
SpecialistsSurgeons Other
Specialties
Specialty Group
Physicians,
%
Agree Unsure Disagree
Figure 1.Agreement with the statement that Medicare
reimbursement isinequitable by specialty group.
ARCH INTERN MED/ VOL 170 (NO. 19), OCT 25, 2010
WWW.ARCHINTERNMED.COM1737
2010 American Medical Association. All rights
reserved.(REPRINTED WITH CORRECTIONS)
wnloaded From: http://archinte.jamanetwork.com/ by a Johns
Hopkins University User on 01/22/2014
-
8/12/2019 Federman - Physicians' Opinions About Reforming
Reimbursement
4/8
sician specialties, geographic locations of the
practices,practice types, practice ownership, and the
physiciansmode of compensation (Table 2).
Overall, 41.6% of physicians supported shifting pay-ments
and46.4%opposed it.Most generalists (66.5%) sup-porteda shift
inreimbursement towardcounselingandman-agement compared with only
16.6% of surgeons (P .001for the difference across the 4 specialty
groups). In addi-
tion, support for shifting paymentswas less likely to be
ex-pressed by physiciansin office-basedpracticesettings,prac-tice
owners, and those with fewer patient care hours.
Most physicians viewed bundling of payments unfa-vorably, with
69.1% of physicians opposing it. Supportfor bundling payments was
low across all physician char-acteristics, with lower levelsof
support expressed by office-based practitioners, practice owners,
and physicians see-ing patients more than 20 hours per week.
In unadjusted regression analysis, surgeons,
medicalsubspecialists, and other physicians were markedly less
supportive of shifting payments to generalists than
weregeneralists themselves (Table 3). These associations werenot
appreciably altered by adjusting for practice charac-teristics and
census division. Nongeneralists were alsoless supportive of
incentives and bundling than were gen-eralists, although the
differences generally were not sta-tistically significant (Table
3). Practice owners were lesssupportive of shifting payments
(adjusted odds ratio[AOR], 0.72; 95% confidence interval [CI],
0.52-0.99)and bundling (AOR, 0.53; 95% CI, 0.38-0.76) than
werenonowners. Physicians who provided more than 20 hoursof patient
care per week were similarly less supportiveof shifting payments
(AOR, 0.59; 95% CI, 0.40-0.88) andof bundling (AOR, 0.56; 95% CI,
0.37-0.85).
SUPPORT FOR INCREASING PAYFOR GENERALISTS
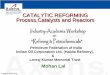
There was broad support for increasing pay for general-ists:
79.8% of respondents expressed support and only13.3% were opposed
(Figure 2). Even among sur-geons, three-quarters (76.6%) supported
increased pay-ments for generalists (Table 4). In contrast to
support
for the other reimbursement reform proposals,only17.2%of
physicians supported bundling. Fewer than half of thephysicians
(39.1%) supported such a strategy, and theleast support was
expressed by surgeons (21.7%).
Although there was broad support for increasing payfor
generalists, physicians in the nongeneralist special-ties were
considerably less supportive of this strategy, inunadjusted and
unadjusted analyses, and even less sowhen there was a cost offset
(Table 5).
COMMENT
In this national survey, we found that most
physiciansbelievethatMedicare reimbursements are inequitable,
andyet there was little consensus on strategies to reform pay-ment.
Physicians generally showed the least support forproposals that
carried the risk of reduced reimburse-ment, such as payments for
bundled care. For physi-cians who frequently perform procedures,
such as sur-geons, there was low support for shifting
somereimbursement from procedures to evaluation and man-agement
services, and there was very low support amongsurgeons and other
nonmedical specialists for a 3% re-duction in reimbursements to
offset increased pay-ments for primary care physicians.
Morethanthree-quartersof the physicians indicatedthatMedicare
reimbursements are inequitable, a finding that
was constant across physician specialties, practice set-tings,
and practice ownership. This observation is consis-tent with
previously published findings that physiciansbe-lieve that
timeliness and adequacy of reimbursements isbetter under private
insurers than it is under Medicare.24
They also echo the call for changes in Medicares rate-setting
policies.8,25,26 The Centers for Medicare and Med-icaid Services
establishes payment rates for physician ser-vices using a
resource-based relative value scale but alsoreceives adviceon
settingreimbursement rates fromthe Spe-cialty Society Relative
Value Scale Update Committee
Table 2. Characteristics of 1222 Physicians Who SupportSpecific
Payment Reform Proposalsa
Variable
Physicians Who Support, %
Incentives bShifting
Payments c Bundlingd
Specialty
General practice 52.7 66.5e 21.3
Medical subspecialty 45.4 54.0 16.0
Surgery 47.0 16.6 15.2Other 52.2 27.3 16.0
Census division
Pacific 55.2 52.0 22.8 f
Mountain 49.1 49.5 16.8
West North Central 45.5 48.5 14.0
West South Central 41.8 45.3 8.6
East North Central 50.5 46.2 26.6
East South Central 56.7 42.8 16.6
South Atlantic 50.4 42.9 14.5
Middle Atlantic 49.9 49.2 16.1
New England 38.3 59.2 22.4
Practice setting
Office based 47.5 45.9e 15.7e
Other 55.3 54.3 25.1
Practice owner
Yes 46.7 42.6e 13.3eNo 53.0 55.0 24.0
Patient care, h/wk20 51.9 f 45.4e 29.7e
20 48.8 61.1 15.8
Source of income
Salary only 53.6 51.2 20.0 f
Salarybonus 52.3 41.8 18.8
Billing only 45.6 53.4 14.6
Shift work/hourly wages 43.0 45.8 14.6
Other 38.3 50.4 12.9
a Weighted 2 test.b Incentivesindicates paying physicians a
higher rate for higher-quality
care (bonus) and a lower rate for lower-quality care (penalty).c
Shifting Paymentsindicates increasing payments for management
and
counseling while decreasing payments for procedures.d
Bundlingindicates paying physicians a fixed amount for all
services
associated with an episode of care.e P .001.f P .05.
ARCH INTERN MED/ VOL 170 (NO. 19), OCT 25, 2010
WWW.ARCHINTERNMED.COM1738
2010 American Medical Association. All rights
reserved.(REPRINTED WITH CORRECTIONS)
wnloaded From: http://archinte.jamanetwork.com/ by a Johns
Hopkins University User on 01/22/2014
-
8/12/2019 Federman - Physicians' Opinions About Reforming
Reimbursement
5/8
(RUC), which is composed of representatives of
medicalspecialties. The RUC has drawn criticism for overestimat-ing
the relative resource needs of physicians in specific spe-cialties
and for specific procedures.26,27 Physician
dissatis-factionwithMedicarereimbursements24 andconcernsaboutequity
of reimbursements suggest that the role of the RUCin advising
Medicare should be carefully evaluated. TheObama administration
andhealth policy experts havecalledfor the creationof an
independentMedicare advisory com-
mittee.
28
However, only 1 Congressional health care re-form proposal
included an independent Medicare com-mission.29Withoutan
independentarbiter,physicians andphysician groups are likely to
continue having complaintsabout the equitability of reimbursements
under Medicare.
There was little unity regarding support for physi-cian payment
reform proposals. Half of the physicianssupported financial
incentives to improve quality. Sup-port for incentives was more
common and more consis-tent acrossallspecialtiescompared with
shifting and bun-dling payments. Actual experience with
financial
incentives to improve quality could have directly in-formed
physicians generally more positive views of thesetypes of
reimbursement mechanisms. For example, higherapproval of incentives
may reflect the fact that incen-tives are already widely applied in
outpatient care, suchas in managed care organizations or in the
Medicare Phy-sician Quality Reporting Initiative.30
There was even less consensus among physicians re-garding
shifting some portion of payments from proce-
dures to management and counseling. As expected, thosewho
conduct procedures were against it, and those whodo more management
and counseling were for it. Nev-ertheless, some surgeons (17%) and
physicians in otherprocedurally oriented specialties (27%)
supported shift-ing payments toward evaluation and management
ser-vices, indicating that underpayment of management andcounseling
even in procedurally oriented specialties is aconcern for many
physicians.
Most physicians from all specialties were opposed tobundled
payments (69%). Surgeons, who may have the
Table 3. Adjusted and Unadjusted Weighted Analyses of Support
for Payment Reform Proposals
Variable
Support, OR (95% CI)
Incentives a Shifting Paymentsb Bundlingc
Unadjusted Adjustedd Unadjusted Adjustedd Unadjusted
Adjustedd
Specialty
General practice 1 [Reference] 1 [Reference] 1 [Reference] 1
[Reference] 1 [Reference] 1 [Reference]
Medical subspecialty 0.77 (0.57-1.04) 0.72 (0.53-0.99)e 0.57
(0.42-0.78) f 0.51 (0.37-0.71) f 0.75 (0.51-1.10) 0.70
(0.45-1.03)
Surgery 0.73 (0.54-0.99)e
0.73 (0.53-1.01) 0.10 (0.07-0.14)f
0.09 (0.06-0.13)f
0.65 (0.44-0.97)e
0.68 (0.44-1.05)Other 0.91 (0.68-1.24) 0.87 (0.63-1.19) 0.18
(0.13-0.25) f 0.16 (0.11-0.23) f 0.70 (0.47-1.03) 0.68
(0.45-1.02)
Census division
Pacific 1 [Reference] 1 [Reference] 1 [Reference] 1 [Reference]
1 [Reference] 1 [Reference]
Mountain 0.69 (0.40-1.18) 0.68 (0.39-1.17) 1.02 (0.60-1.74) 0.91
(0.50-1.67) 0.72 (0.36-1.43) 0.78 (0.38-1.59)
West North Central 0.70 (0.41-1.18) 0.64 (0.37-1.10) 0.96
(0.57-1.62) 0.94 (0.50-1.79) 0.63 (0.31-1.27) 0.59 (0.29-1.21)
West South Central 0.55 (0.34-0.88) f 0.52 (0.32-0.84) f 0.77
(0.48-1.24) 0.65 (0.38-1.09) 0.28 (0.13-0.60)g 0.30
(0.14-0.63)f
East North Central 0.77 (0.51-1.19) 0.72 (0.46-1.11) 0.93
(0.61-1.43) 0.74 (0.46-1.19) 1.07 (0.65-1.77) 1.03 (0.60-1.75)
East South Central 0.87 (0.48-1.55) 0.87 (0.48-1.58) 0.71
(0.39-1.28) 0.61 (0.32-1.16) 0.77 (0.37-1.60) 0.81 (0.38-1.72)
South Atlantic 0.74 (0.50-1.10) 0.71 (0.47-1.07) 0.76
(0.51-1.12) 0.60 (0.38-0.94) f 0.57 (0.34-0.94)e 0.54
(0.31-0.91)e
Middle Atlantic 0.71 (0.47-1.08) 0.71 (0.46-1.09) 0.88
(0.58-1.33) 0.66 (0.41-1.05) 0.59 (0.35-1.00)e 0.53
(0.30-0.94)e
New England 0.50 (0.29-0.88)e 0.44 (0.25-0.77) f 1.26
(0.73-2.18) 1.00 (0.55-1.82) 1.04 (0.55-2.00) 0.90 (0.56-1.76)
Office-based practice
Yes 0.76 (0.59-0.98)e 0.88 (0.66-1.17) 0.77 (0.60-0.99)e 0.87
(0.63-1.19) 0.61 (0.44-0.83)f 0.78 (0.55-1.11)
No 1 [Reference] 1 [Reference] 1 [Reference] 1 [Reference] 1
[Reference] 1 [Reference]
Practice owner
Yes 0.72 (0.60-0.95)e
0.85 (0.64-1.13) 0.61 (0.48-0.77)f
0.72 (0.52-0.99)e
0.47 (0.34-0.64)f
0.53 (0.38-0.76)f
No 1 [Reference] 1 [Reference] 1 [Reference] 1 [Reference] 1
[Reference] 1 [Reference]
Patient care, 20 h/wk
Yes 0.89 (0.65-1.24) 0.92 (0.64-1.30) 0.53 (0.39-0.74)g 0.59
(0.40-0.88) f 0.47 (0.33-0.69) 0.56 (0.37-0.85)f
No 1 [Reference] 1 [Reference] 1 [Reference] 1 [Reference] 1
[Reference] 1 [Reference]
Source of income
Salary only 1 [Reference] 1 [Reference] 1 [Reference] 1
[Reference] 1 [Reference] 1 [Reference]
Salarybonus 0.88 (0.66-1.16) 0.96 (0.70-1.31) 0.67 (0.50-0.89)f
0.84 (0.59-1.19) 0.93 (0.65-1.33) 1.18 (0.80-1.73)
Billing only 0.71 (0.51-1.01) 0.80 (0.54-1.18) 1.08 (0.77-1.53)
1.54 (0.99-2.41) 0.70 (0.44-1.13) 1.04 (0.62-1.74)
Shift work/hourly wages 0.67 (0.38-1.17) 0.69 (0.39-1.24) 0.75
(0.43-1.32) 0.53 (0.27-1.02) 0.65 (0.30-1.40) 0.62 (0.28-1.39)
Other 0.50 (0.32-0.76) f 0.54 (0.35-0.86) f 0.94 (0.62-1.42)
1.11 (0.68-1.81) 0.66 (0.37-1.18) 0.74 (0.40-1.36)
Abbreviations: CI, confidence interval; OR, odds ratio.a
Incentivesindicates paying physicians a higher rate for
higher-quality care (bonus) and a lower rate for lower-quality care
(penalty).b Shifting Paymentsindicates increasing payments for
management and counseling while decreasing payments for
procedures.c Bundlingindicates paying physicians a fixed amount for
all services associated with an episode of care.d Adjusted for all
the independent variables listed in column 1.e P .05.f P .01.g P
.001.
ARCH INTERN MED/ VOL 170 (NO. 19), OCT 25, 2010
WWW.ARCHINTERNMED.COM1739
2010 American Medical Association. All rights
reserved.(REPRINTED WITH CORRECTIONS)
wnloaded From: http://archinte.jamanetwork.com/ by a Johns
Hopkins University User on 01/22/2014
-
8/12/2019 Federman - Physicians' Opinions About Reforming
Reimbursement
6/8
most experience with bundling,31 expressed the lowestlevels of
support for this strategy. With bundling, phy-sicians and health
care systems are at greater financialrisk, and uncertainty remains
about who would have re-sponsibility for controlling costs and how
savings gen-erated through greater efficiency in health care
provi-sion and better health outcomes would be divided
amongentities sharing in thecareofa patient.31,32 Because
bundledpayments are likely to be implemented in one form
oranother,1,2 this mechanism ought to be carefully ex-plained to
physicians to promote broad acceptance andsmooth implementation.
Research that further charac-terizes physicians experience with and
concerns aboutbundling could provide guidance toward these ends.
Ofnote, physicians in the West South Central census divi-sion of
the United States were less likely to support in-centives or
bundled payments. Additional research mighthelp determine which
factors contribute to this regionalvariation in views on payment
reform.
Reducing the fragmented provision of care throughimprovements in
care coordination and continuity of caremay be necessary before
bundling, and other strategiescould successfully contribute to
improvedhealth care andcost savings.7,31 To improve care
coordination and in-crease the delivery of preventive care and
counselingser-vices, several reform plans have proposed increasing
re-imbursement to generalist physicians, an idea supportedby most
physicians surveyed in this study. Surgeons andother specialists,
however, were considerably less sup-portive when the proposal
calledfor shifting some of theirreimbursement to meet the costs of
increased payments
to generalists, a strategy proposed for Medicare by theSenate
Finance Committee.7
This study is limitedby a 48.5% responserate. This rateis
slightly lower than the average for physician surveys33;however,
there were no differences between respondentsand nonrespondents on
important characteristics. Fur-thermore, we collected data during
just 4 months, a briefperiod intended to capture physician views
near the apexof thehealthcare reformdebate.Although physicians
opin-ions about strategies for expanding health insurance cov-erage
may have evolved across time, we found no signifi-
cant differences between opinions expressed in surveysreceived
at different time points during the period of datacollection.
Finally, duringthe period of data collection, pro-posals for
reimbursement reform were in flux as Congresstried to work out
legislation. For example, the Senate Fi-nance Committee proposed a
10% Medicare payment bo-nus for primary care providers with half of
the cost of thebonuses offsetby a 0.5% reduction in allother
services.Thetradeoff we used in the present study was a 3%
reduction
in reimbursementsfor nonprimary care physicians.
Phy-siciansrespondingto thissurveymighthavebeen more ame-nable to a
lower reduction in reimbursement, such as wasproposed by the Senate
Finance Committee.7 The PatientProtection and Accountable Care Act
did include a pay-ment bonus for primary care but no reductionin
paymentfor other services.
In conclusion, most physicians believe thatMedicare
re-imbursements are inequitable, yet there is little consensusamong
them regarding major proposals to reform reim-bursement. Bundling
of payments, in particular, was op-
100
75
25
50
0Increase Pay for
Primary Care
79.8
7.0
13.3
39.1
9.8
51.1
Decrease Pay to Specialistsby 3% to Increase Pay
for Primary Care
Respondents,
%
Support
Unsure
Oppose
Figure 2.Rates of support for increased pay for primary care
physicians(n=1222). Due to rounding, the percentages for the
increased pay section donot total 100.
Table 4. Characteristics of 1222 Physicians Who
SupportIncreasing Pay for Primary Care a
Variable
Support Increasing Payfor Primary Care, %
Without Changein Specialist
Reimbursement
With a 3% Reductionin Specialist
Reimbursement
Specialty
General practice 88.3b 63.0bMedical subspecialty 72.6 36.7
Surgery 76.6 21.7
Other 81.0 33.7
Census division
Pacific 82.4 45.9
Mountain 75.7 43.6
West North Central 77.5 45.4
West South Central 77.0 42.3
East North Central 80.1 41.9
East South Central 82.4 41.5
South Atlantic 79.6 37.2
Middle Atlantic 81.4 43.4
New England 86.1 52.2
Practice location
Urban 76.1 41.7
Rural 80.7 53.6Practice setting
Office based 79.9 40.7c
Hospital/other 81.6 50.1
Practice owner
Yes 79.1 37.8b
No 82.0 50.5
Patient care, h/wk
20 81.6 51.7c
20 80.0 41.3
Source of income
Salary only 80.7 47.2
Salarybonus 81.4 39.6
Billing only 79.4 45.9
Shift work/hourly wages 80.3 41.9
Other 76.4 38.9
a Weighted 2 test.bP .001.c P .05.
ARCH INTERN MED/ VOL 170 (NO. 19), OCT 25, 2010
WWW.ARCHINTERNMED.COM1740
2010 American Medical Association. All rights
reserved.(REPRINTED WITH CORRECTIONS)
wnloaded From: http://archinte.jamanetwork.com/ by a Johns
Hopkins University User on 01/22/2014
-
8/12/2019 Federman - Physicians' Opinions About Reforming
Reimbursement
7/8
posed by most physicians. Overall, physicians seem to beopposed
to reformsthatrisk lowering their incomes. Thus,finding common
ground among different specialties to re-form physician
reimbursement, reduce health care spend-ing, and improve health
care quality will be difficult. Re-search thatclarifiesthetradeoffs
physicianswould bewillingto accept in paymentreform, and
otherconcerns, may helprefine the design of payment reforms and
improve accep-tance among physicians.
Accepted for Publication:March 14, 2010.
Correspondence:Alex D. Federman, MD, MPH, Divi-sion of General
Internal Medicine, Mount Sinai Schoolof Medicine, PO Box 1087, One
Gustave L. Levy Place,New York, NY 10029
([email protected]).Author Contributions: Dr Federman had full
access to allthe data in the study andtakes responsibility for the
integ-rity of the data and the accuracy of the data analysis.
Studyconcept and design:Federman, Woodward, and Keyhani.Acquisition
of data:Federman and Keyhani.Analysis andinterpretation of data:
Federman, Woodward, and Key-hani.Drafting of the manuscript:
Federman and Keyhani.
Critical revision of the manuscript for important
intellectualcontent: Federman, Woodward, and
Keyhani.Statisticalanalysis: Federman, Woodward, and
Keyhani.Obtainedfunding: Federman and Keyhani.Administrative,
technical,and material support:Federman and Keyhani.Financial
Disclosure:None reported.Funding/Support: This project was
supported by a grantfrom the Robert Wood Johnson Foundation and
also bygrants from the National Institute on Aging; the Na-tional
Heart, Lung, and Blood Institute; and the Veter-ans Administration
Health Services Research and Devel-
opment Service (Drs Federman and Keyhani).Role of the Sponsors:
The Robert Wood Johnson Foun-dation played no role in thedesign or
conduct of thestudy;in the collection, management, analysis, or
interpreta-tion of the data; or in the preparation, review, or
ap-proval of the manuscript.Online-Only Material: An eAppendix is
available at http://www.archinternmed.com.Additional
Contributions:Helen Cole, MPH, providedproject management, and
Cathy Schoen, PhD; KennethShine, MD; Gerard Anderson, PhD; Thomas
Russell, MD;
Table 5. Adjusted and Unadjusted Weighted Analyses of Support
for Increasing Pay for Primary Care
Variable
Support Increasing Pay for Primary Care, OR (95% CI)
Without Changein Specialist Reimbursement
With a 3% Reductionin Specialist Reimbursement
Unadjusted Adjusteda Unadjusted Adjusteda
Specialty
General practice 1 [Reference] 1 [Reference] 1 [Reference] 1
[Reference]
Medical subspecial ty 0.38 (0.25-0.57)b
0.37 (0.24-0.57)b
0.33 (0.24-0.46)b
0.31 (0.22-0.43)b
Surgery 0.43 (0.28-0.65)b 0.43 (0.28-0.66)b 0.16 (0.11-0.22)b
0.16 (0.11-0.22)b
Other 0.53 (0.35-0.82)c 0.52 (0.33-0.80)c 0.29 (0.21-0.39)b 0.27
(0.19-0.38)b
Census division
Pacific 1 [Reference] 1 [Reference] 1 [Reference] 1
[Reference]
Mountain 0.67 (0.35-1.26) 0.62 (0.32-1.17) 0.96 (0.56-1.64) 0.85
(0.47-1.56)
West North Central 0.74 (0.39-1.42) 0.75 (0.38-1.47) 0.92
(0.54-1.58) 0.90 (0.49-1.64)
West South Central 0.77 (0.43-1.37) 0.73 (0.41-1.31) 0.79
(0.49-1.28) 0.68 (0.41-1.11)
East North Central 0.98 (0.57-1.69) 0.90 (0.51-1.57) 0.99
(0.65-1.52) 0.81 (0.50-1.30)
East South Central 1.11 (0.53-2.32) 1.00 (0.48-2.08) 0.77
(0.42-1.39) 0.67 (0.36-1.24)
South Atlantic 0.82 (0.50-1.34) 0.77 (0.46-1.30) 0.76
(0.51-1.14) 0.64 (0.41-1.01)
Middle Atlantic 0.96 (0.57-1.63) 0.94 (0.54-1.64) 0.86
(0.57-1.31) 0.72 (0.44-1.16)
New England 1.40 (0.65-3.02) 1.38 (0.62-3.05) 1.31 (0.77-2.26)
1.09 (0.63-1.89)
Office-based practice
Yes 0.79 (0.57-1.09) 0.79 (0.54-1.15) 0.71 (0.55-0.91)c 0.82
(0.60-1.11)
No 1 [Reference] 1 [Reference] 1 [Reference] 1 [Reference]
Practice ownerYes 0.84 (0.63-1.13) 0.94 (0.65-1.35) 0.60
(0.47-0.76)b 0.70 (0.51-0.95)d
No 1 [Reference] 1 [Reference] 1 [Reference] 1 [Reference]
Patient care, 20 h/wk
Yes 1.02 (0.68-1.53) 1.01 (0.65-1.56) 0.68 (0.49-0.94)d 0.74
(0.51-1.09)
No 1 [Reference] 1 [Reference] 1 [Reference] 1 [Reference]
Source of income
Salary only 1 [Reference] 1 [Reference] 1 [Reference] 1
[Reference]
Salarybonus 1.01 (0.71-1.45) 1.14 (0.76-1.71) 0.72 (0.54-0.96)d
0.87 (0.62-1.22)
Billing only 0.88 (0.57-1.35) 1.03 (0.62-1.69) 0.90 (0.64-1.28)
1.24 (0.80-1.91)
Shift work/hourly wages 0.96 (0.47-1.96) 1.05 (0.51-2.15) 0.74
(0.42-1.30) 0.67 (0.36-1.27)
Other 0.71 (0.43-1.16) 0.72 (0.41-1.24) 0.67 (0.44-1.04) 0.78
(0.48-1.27)
Abbreviations: CI, confidence interval; OR, odds ratio.a
Adjusted for all the independent variables listed in column 1.b P
.001.c P .01.d P .05.
ARCH INTERN MED/ VOL 170 (NO. 19), OCT 25, 2010
WWW.ARCHINTERNMED.COM1741
2010 American Medical Association. All rights
reserved.(REPRINTED WITH CORRECTIONS)
wnloaded From: http://archinte.jamanetwork.com/ by a Johns
Hopkins University User on 01/22/2014
-
8/12/2019 Federman - Physicians' Opinions About Reforming
Reimbursement
8/8
ShoshannaSofaer, DrPH; andLawrence Brown,PhD, pro-vided helpful
comments in developing this study.
REFERENCES
1. Luft HS. Health care reformtoward more freedom, and
responsibility, for
physicians.N Engl J Med. 2009;361(6):623-628.
2. Fisher ES, Bynum JP, Skinner JS. Slowing the growth of health
care costs
lessons from regional variation.N Engl J Med.
2009;360(9):849-852.
3. HenryJ Kaiser Family Foundation. HealthCareCosts: A Primer:
KeyInformation
on Health Care Costs and Their Impact.Menlo Park, CA: Henry J
Kaiser FamilyFoundation; 2009.
http://www.kff.org/insurance/upload/7670_02.pdf. Ac-
cessed March 1, 2009.
4. Bodenheimer T. High and rising health care costs: part 3: the
role of health care
providers.Ann Intern Med. 2005;142(12, pt 1):996-1002.
5. Rother J. A consumer perspective on physician payment
reform.Health Aff
(Millwood). 2009;28(2):w235-w237.
6. Kautter J, PopeGC, Trisolini M, Grund S.
Medicarephysiciangroup practicedem-
onstration design: quality and efficiency pay-for-performance.
Health Care Fi-
nanc Rev. 2007;29(1):15-29.
7. Senate Finance Committee.Framework for Comprehensive Health
Reform. US
Senate; September 8, 2009.
8. Milgate K, Cheng SB. Pay-for-performance: the MedPAC
perspective.Health Aff
(Millwood). 2006;25(2):413-419.
9. AntosJ,BertkoJ, ChernewM, etal. Bendingthe curve:
effectivestepsto addresslong-
term healthcare spending growth.AmJ ManagCare.
2009;15(10):676-680.
10. Mechanic RE, Altman SH. Payment reform options: episode
payment is a good
place to start.Health Aff (Millwood). 2009;28(2):w262-w271.11.
Guterman S, Davis K, Schoenbaum S, Shih A. Using Medicare payment
policy
to transform the health system: a framework for
improvingperformance. Health
Aff (Millwood). 2009;28(2):w238-w250.
12. Henry J. Focus on Health Reform: Summary of new health
reform law. http:
//www.kff.org/healthreform/upload/8061.pdf. Accessed August 13,
2010.
13. Federal Register.
http://edocket.access.gpo.gov/2010/pdf/2010-15900.pdf. Ac-
cessed August 13, 2010.
14. Barr M, Ginsberg J.The Advanced Medical Home:
Patient-Centered, Physician-
Guided Care for the Chronically Ill. Philadelphia, PA: American
College of Phy-
sicians; 2006.
15. McCormick D, Woolhandler S, Bose-Kolanu A, Germann A, Bor
DH, Himmel-
steinDUUS. U.S.physicians viewson financingoptions to expand
health insur-
ance coverage: a national survey. J Gen Intern Med.
2009;24(4):526-531.
16. Fink A, Kosecoff J, Chassin M, Brook RH. Consensus methods:
characteristics
and guidelines for use.Am J Public Health.
1984;74(9):979-983.
17. Ackermann RT, Carroll AE. Support for national health
insurance among U.S.
physicians: a national survey.Ann Intern Med.
2003;139(10):795-801.
18. CasalinoLP, AlexanderGC, JinL, Konetzka
RT.Generalinternistsviews onpay-
for-performance and public reportingof quality scores: a
national survey. Health
Aff (Millwood). 2007;26(2):492-499.
19. Freed GL, Cowan AE, Clark SJ. Primary care physician
perspectives on reim-
bursement for childhood immunizations. Pediatrics.
2008;122(6):1319-
1324.
20. McCormick D, Himmelstein DU, Woolhandler S, Bor DH.
Single-payer national
health insurance: physicians views.Arch Intern Med.
2004;164(3):300-
304.
21. McMahonSR, Iwamoto M, MassoudiMS, et al.Comparisonof
e-mail,fax, andpostal
surveysof pediatricians. Pediatrics. 2003;111(4, pt
1):e299-e303.http://pediatrics
.aappublications.org/cgi/content/full/111/4/e299. Accessed
August 25,
2010.
22. Meier DE, Emmons CA, Wallenstein S, Quill T, Morrison RS,
Cassel CK. A na-
tional survey of physician-assisted suicide and euthanasia in
the United States.
N Engl J Med. 1998;338(17):1193-1201.
23. American Association for Public Opinion Research.Standard
Definitions: Final
Dispositionsof CaseCodesand Outcome Rates for Surveys.Deerfield,
IL:Ameri-
can Association for Public Opinion Research; 2006.
24. Keyhani S, Federman A. Physician Views on the Public Health
Insurance Option
and MedicareExpansions.Princeton, NJ: RobertWood
JohnsonFoundation;Sep-
tember 2009.
25. Ginsburg PB, Berenson RA. Revising Medicares physician fee
schedule
much activity, little change.N Engl J Med.
2007;356(12):1201-1203.
26. Bodenheimer T, Berenson RA, Rudolf P. The primary
care-specialty income gap:
why it matters.Ann Intern Med. 2007;146(4):301-306.
27. Rich WL III. The primary care-specialty income gap.Ann
Intern Med. 2007;146
(12):895-896, author reply 896.
28. Pham HH, Ginsburg PB, Verdier JM. Medicare governance and
provider pay-ment policy.Health Aff (Millwood).
2009;28(5):1382-1394.
29. Congressional Budget Office analysis of the Americas Healthy
Future Act as
amended.
http://finance.senate.gov/issue/?id=82dd713a-cc17-425a
-a3ef-f05518995956. Accessed October 10, 2009.
30. Centers for Medicare and Medicaid Services.Physician Quality
Reporting Initia-
tive:2007 ReportingExperience. Baltimore,MD: Centers for
Medicare and Med-
icaid Services; December 3, 2008.
31. Miller HD. From volume to value: better ways to pay for
health care.Health Aff
(Millwood). 2009;28(5):1418-1428.
32. The Commonwealth Fund. MEDPAC probes effectiveness of
accountable care
organizations.
http://www.commonwealthfund.org/Content/Newsletters
/ Wa sh in g t on -H ea lt h- Po li c y- in - Re v ie w/ 20 09 /
A pr / Ap r il - 20 - 20 0 9
/MEDPAC-Probes-Effectiveness-of-Accountable-Care-Organizations.aspx.
Ac-
cessed October 11, 2009.
33. Asch DA, Jedrziewski MK, Christakis NA. Response rates to
mail surveys pub-
lished in medical journals.J Clin Epidemiol.
1997;50(10):1129-1136.
INVITED COMMENTARY
Reforming Payment for Health Care Services
American medicine has long been characterizedby fee-for-service
(FFS) payment. The FFSsystem has several merits. It rewards
hard
work and productivity and incentivizes physicians notto stint on
care. It avoids placing physicians at finan-cial risk if they care
for sick patients and facilitatesfinancing systems that allow
patients unconstrainedchoice of provider (eg, physicians, allied
health profes-sionals, and hospitals).
Yet the FFS system has come under attack lately asa primary
contributor to the ills of the American
health care system. A drawback of the FFS systemsincentive not
to stint on care is an incentive to overusecare. While physicians
are unlikely to intentionally
provide care that is unneeded or even harmful,payment rates in
most existing FFS systems are highenough to remove the incentives
to eliminate suchcare. Moreover, FFS systems can facilitate growth
of a
See also page 1728
ARCH INTERN MED/ VOL 170 (NO. 19), OCT 25, 2010
WWW.ARCHINTERNMED.COM1742
2010 American Medical Association. All rights
reserved.(REPRINTED WITH CORRECTIONS)