Embed Size (px)
Citation preview
FECAL-BORNE HEPATITIS
ETIOLOGY
Hepatitis A virus (HAV), Hepatovirus
Picornavirus, enterovirus 72
27 nm1 serotype only, although there are 4 genotypes
Hepatitis E virus (HEV)
Calicivirus-like virions
30 – 32 nm
Both are ssRNA, naked icosahedral viruses
EPIDEMIOLOGY
Natural hosts Humans
Distribution HAV is worldwide. High-prevalence areas: Africa, Asia, Central and
South America.
Epidemics of HEV have been reported in India (1955 with 29000 cases).
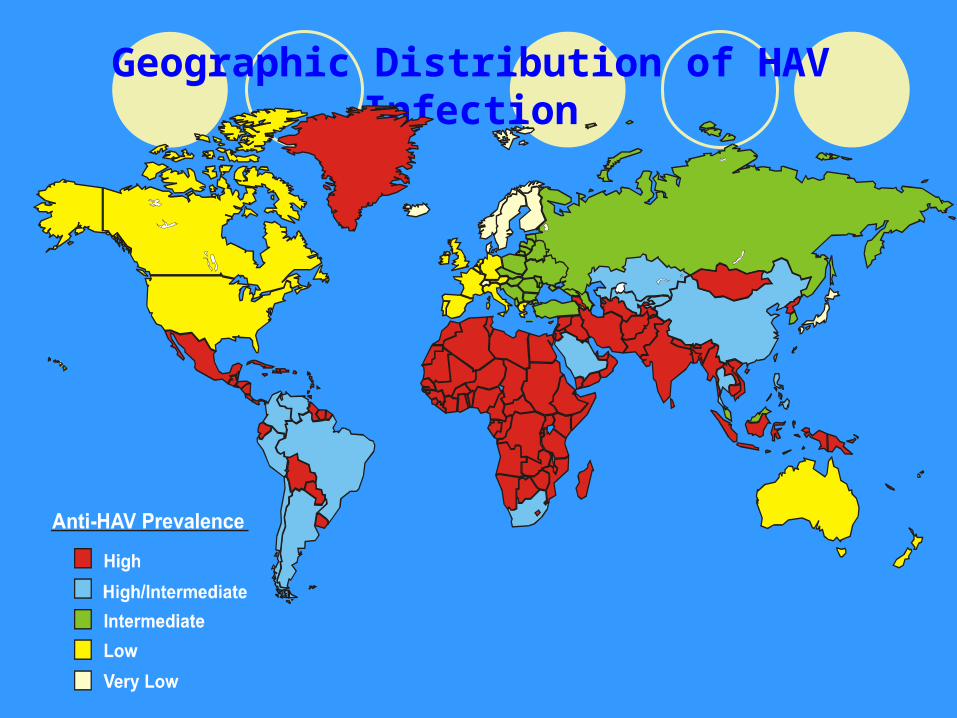
Geographic Distribution of HAV Infection
Fecal-oral route The virus survive in the environment for over 3
months. Daycares are good places for HAV infections to
spread.
Transmission
HAV Children 5-9 years Young adults 25-35 years
HEV Young and middle-aged adults
Prevalent Crowded living conditions Areas of low socioeconomic development
>90% of the population in underdeveloped countries has experienced HAV infection, vs. to <50% of the population in developed countries.
Incidence
PATHOGENESIS
Portal: After ingestion, the rigid capsid withstands the harsh
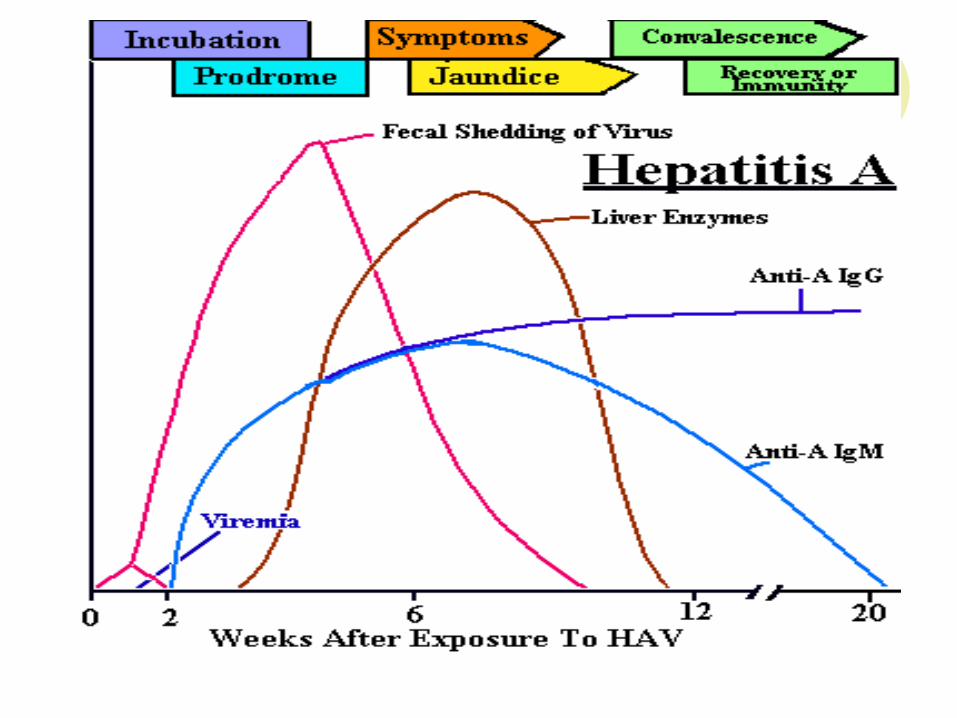
conditions in the stomach and intestines. Viremia:
HAV replicates in the oropharynx and epithelial lining of the intestines, where it initiates a transient viremia and infects the liver.
Replication: HAV binds to and replicates within liver parenchymal cells.
Virus shedding: Virus is released into the bile and eventually the stools. Virus
may be shed for 10 days before clinical symptoms appear.
Immunological role in pathology: Antibody-antigen complexes and complement fixation
contribute to inflammation and tissue damage.
Self-limited disease: All HAV infections are acute, being self-limited by the induction of IgM and IgG, which confers long-lasting immunity.
No chronic complications.
MANIFESTATIONS
Incubation: 14 - 45 days. Children: 84 - 94% are asymptomatic Adults: 5 - 25% are asymptomatic; 66% have jaundice
Initial symptoms: fever, malaise, fatigue, headache, anorexia, nausea, vomiting and pain in the right upper quadrant; and hepatosplenomegaly.
Classic symptoms: Cholestasis: Dark urine, clay-colored stools followed in 1 - 5 days by clinical jaundice. The liver is enlarged and tender. Liver damage produces increased blood levels of: Aspartate aminotransferase (AST=SGOT) Alanine aminotransferase (ALT = SGPT) Bilirubin
LABORATORY DIAGNOSIS
Elevated liver enzymes
High titer of anti-HAV IgM (only one serotype) in the serum during the acute phase of the illness using ELISA.
15% of people infected will have prolonged or relapsing symptoms over a 6 – 9 months period.
HEV is serologically unrelated and detection of IgM antibodies is available.
THERAPY
Supportive therapy and restHAV: low mortality (0.1-0.2%) HEV: Mortality rate 10 times HAV (1-2%).
Especially high mortality (20%) during pregnancy
PREVENTION
Passive immunization using pooled human immune serum globulin (ISG).
ISG is of no value once symptoms have appeared.
Vaccination of children 2 years of age and older; adolescents and adults is required for people who live in intermediate or high-risk areas.
Hepatitis A vaccine: inactivated (killed) vaccines.inactivated (killed) vaccines. The vaccine should be administered by intramuscular
injection into the deltoid muscle.

![Hepatitis B virus and hepatitis C virus play different ... · alcoholic cirrhosis, hepatitis viruses, tobacco and metabolic diseases[4]. Hepatitis viruses, including hepatitis B virus](https://img.pdfslide.us/doc/110x75/60e46cab5bd9101a6f539e91/hepatitis-b-virus-and-hepatitis-c-virus-play-different-alcoholic-cirrhosis.jpg)



























