Embed Size (px)
Citation preview

C
12
3
4
A
2cuNs
1h
Critical Reviews in Oncology/Hematology 85 (2013) 193–205
Features of cancer management in obese patients
Hussam Hijazi a, Nicolas Magné b, Antonin Levy c, Pierre-Yves Marcy d, Alexis Lacout e,Axel Leysalle a, Jean-Michel Hannoun-Levi a, Stephane Schneider f, Jean-Louis Sadoul g,
Juliette Thariat h,∗a Department of Radiation Oncology, Centre Antoine Lacassagne – Université Nice Sophia Antipolis, 33 av Valombrose, 06189 Nice, France
b Department of Radiotherapy, Institut de Cancérologie Lucien Neuwirth, 42271 Saint Priest en Jarez, Francec Department of Radiation Oncology, Institut Gustave Roussy, Université Paris XI, 94800 Villejuif, France
d Department of Radiology, Centre Antoine Lacassagne – Institut Universitaire de la Face et du Cou – Université Nice Sophia Antipolis, 33 av Valombrose,06189 Nice, France
e Imaging Centre, 15000 Aurillac, Francef Division of Digestive Diseases, University Hospital of Nice, France
g CHU de Nice, hôpital de l’Archet, service d’endocrinologie-diabétologie-reproduction, BP 3079, 06202 Nice, Franceh Department of Radiation Oncology, Centre Antoine Lacassagne – Institut Universitaire de la Face et du Cou – Université Nice Sophia Antipolis, 33 av
Valombrose, 06189 Nice, France
Accepted 13 June 2012
ontents
. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 194
. Involvement of obesity in cancer management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1942.1. Medical imaging and image-guided intervention challenges in high BMI patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1942.2. Oncologic surgical results among high BMI patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1952.3. Dose uncertainty in obese patients receiving chemotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1972.4. Concerns in radiation accuracy for high BMI population . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 198
. Prospects: from biological assumption to new therapeutic strategies and toxicity prediction? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2013.1. Biological pathways implicated in tumorigenesis of obese patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2013.2. Biological prediction of toxicity: the example of radiotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202
. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202Biography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 205
bstract
There is worldwide increased in obesity prevalence and statistical almost half of United-States, including children, could be obese by050. Obesity in cancer patients is a major issue in oncology because weight gain and obesity account for approximately 20% of all cancerases. Indeed, increased obesity is linked with higher risk of various types of cancer and a poorer survival. Although biological mechanismsnderlying how obesity causes an increased risk of cancer are suggested, overweight as a putative direct cause of death is still debated.umerous confounding factors may impact on survival, including comorbidities and imaging limitations. Moreover, difficulties to achieve the
n may also be concerned. Herein, we examined the specific features and
tandard oncologic care with surgery, chemotherapy and/or radiatio∗ Corresponding author. Tel.: +33 492031269; fax: +33 492031570.E-mail address: [email protected] (J. Thariat).
040-8428/$ – see front matter © 2012 Elsevier Ireland Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.critrevonc.2012.06.003

1
pn©
K
1
wooDtlgcOfuahbdB[
ddrbcgcittpficjeiT
ousbtcTpa
94 H. Hijazi et al. / Critical Reviews in Oncology/Hematology 85 (2013) 193–205
otential adaptation of the cancer management in overweighed patients. Then, we reviewed how implicated molecular pathways may provideew strategies to decrease cancer risk and predict toxicities in an increasingly obese population.
2012 Elsevier Ireland Ltd. All rights reserved.
Treatment; Technical; Adaptation/limitation
Table 1Relative risks of cancer in obese patients [6,7].
Incidencea [6] Survivalb [7]
Men Women Men Women
Breast (postmenopausal) – 1.1 – 2Cervix – N/A – 3.2Colon 1.2 1.1 1.9c 1.5c
Endometrial – 1.6 – 6.2Esophagus adenocarcinoma 1.5 1.5 1.9Gallbladder 1.1 1.6 1.8 2.6Ovary N/A N/A N/A 1.5Leukemia 1.1 1.2 N/A N/ALiver N/A N/A 4.5 1.7Melanoma 1.1 1 N/A N/AMyeloma 1.1 1.1 1.7 1.4Non-Hodgkin’s lymphoma 1.1 1.1 1.5 2Pancreas 1.1 1.1 2.6 2.8Prostate 1 – 1.34 –Rectum 1.1 1 1.9c 1.5c
Renal 1.2 1.3 1.7 4.8Stomach N/A N/A 1.9 N/AThyroid 1.3 1.1 N/A N/AAll cancer N/A N/A 1.7 1.9
N/A, not available.a Relative risk is expressed per 5 kg/m2 increased in BMI.
2
2c
ptonduticofma
m
eywords: Obese; Overweight; Bariatric; Cancer risk; Incidence; Toxicity;
. Introduction
The past three decades have been characterized by a majororldwide increased in obesity prevalence. In 2010, one-thirdf United-States adults were obese, and nine states reportedbesity rates of 30% or more, compared to none in 2000.espite ambitious national plans, Centers for Disease Con-
rol and Prevention showed an annual 1% increase over theast five years. Moreover, statistical predictive model sug-ested that almost half of United-States, including children,ould be obese by 2050 [1,2]. According to the World Healthrganization, obesity is defined as abnormal or excessive
at accumulation that presents a risk to health. A crude pop-lation measure of obesity is the body mass index (BMI),person’s weight (in kilograms) divided by the square of
is or her height (in meters). BMI is closely related tooth percentage body fat and total body fat. Overweight isefined by a BMI of more than 25 kg/m2 and obesity by aMI over 30 kg/m2 (http://www.who.int/topics/obesity/en/)
1].Obesity is a costly health issue (hundreds of billions of
ollars yearly) and one of the leading preventable causes ofeath worldwide. Indeed, overweight and obesity are majorisk factors for a number of chronic diseases, including dia-etes, cardiovascular diseases and cancer [3–5]. Obesity inancer patients is a major issue in oncology because weightain and obesity account for approximately 20% of all cancerases [4]. Indeed, large prospective epidemiological stud-es support the association between obesity and variousypes of malignancies, including colic, pancreatic, endome-rial, renal, gallbladder or esophageal adenocarcinoma, andostmenopausal breast cancer [6]. Besides, historical datarom the past 25 years point obesity as a cause of approx-mately 14% of cancer deaths in men and up to 20% ofancer deaths in women. Compared to normal weight sub-ects, the relative death rates from all cancers reaches anxcess of 62% [4,7]. Relative risks of cancer in term ofncidence and prognosis in obese population are reported inable 1.
Because the exact biological mechanisms underlying howbesity causes an increased risk of cancer are still poorlynderstood, overweight as a putative direct cause of death istill debated. In fact, confounding factors may include comor-idities and limitations for diagnosis or difficulties to achievehe standard of oncologic care. Herein, we examined the spe-ific features of the cancer management in obese patients.
hen, we reviewed how molecular pathways of interest mayrovide new strategies to decrease cancer risk and toxicity inn increasingly obese population.san
b Relative risk is expressed for highest BMI category.c Colon and rectum were pooled.
. Involvement of obesity in cancer management
.1. Medical imaging and image-guided interventionhallenges in high BMI patients
Challenges for tumor assessment in imaging of obeseatients include the physical constraint, including the aper-ure opening diameter (∼70 cm) and table weight (∼250 kg)f CT (computed-tomography) and MR (magnetic reso-ance) scans. Although several adaptations of radiologicevices with portable (X-ray/ultrasound), as imaging orpgraded bariatric equipment, are being developed in this set-ing, obtaining high quality images remains a central point ofnterest in this population [8–10]. Undeniably, the radiologi-al anatomy of obese patients is modified by the accumulationf adipose tissue (retroperitoneal, subcutaneous fat) and theatty infiltration of a number of organs (liver, parotids, breast,uscle, etc.). Then, anatomical variant of normal imaging
nd limits are specific to each imaging technique [11,12].Although fat can be helpful in a few radiographs such as
ammography (improved visibility of a lesion relative to the
urrounding fat), increased BMI induces higher X-ray beamttenuation with lower image contrast. Moreover, body thick-ess increases exposure time and induces a higher potential
Oncolo
fHtiao
vsaaliwfs
vomarheitgctt[
Mgptosbufs1i
a(basdull
t
wrpapvw
2
ttHleobidahpb
ragorllwmaiw1rfpsatcBhstroa
H. Hijazi et al. / Critical Reviews in
or loss of geometric sharpness because of motion artifacts.igher tube current, voltage settings, using tight collima-
ion and a grid (filtering device that ensure the clarity of themage) of alternating radiopaque and radiolucent strips tovoid detection of scattered photons may improve the qualityf images [13].
Image quality issues due to attenuation and limited field ofiew are also observed in ultrasound imaging. Indeed, ultra-ound beam penetration is attenuated at a rate of 0.63 dB/cms it passes through the subcutaneous and intraperitonealbdominal fat. Using the lowest frequency transducer and aiver/spleen window may somewhat improve the image qual-ty. However, it is very hard to predict which obese patientsill be affected, as patients with predominately subcutaneous
at will have lower quality images compared those with lowerubcutaneous fat and more intraperitoneal fat [12].
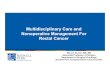
As in X-ray imaging, fat can be advantageous for theisualization of some organ structures on CT scan inverweight patients, such as head and neck tumors orediastinal/supra-clavicular adenopathies (Fig. 1). Addition-
lly, intra/retroperitoneal fat and liver steatosis play the sameole in spontaneously contrasting the tumor. On the otherand, limitations of CT scan in obese patients include inad-quate photon penetration and limited field of view resultingn image cropping and beam-hardening artifacts, respec-ively (Fig. 2). Increasing the tube voltage, decreasing theantry rotation speed or using scanners with automated tubeurrent modulation may improve image quality. Adjustinghe patient’s position or the use of specialized softwarehat allows field of view may decrease truncation artifacts12,14,15].
MRI image quality is least affected by obesity. TypicalRI equipments have a high signal-to-noise ratio and strong
radients (≥1.5 T). Nonetheless, MRI cannot accommodateatients weighing 150 kg or with aperture opening diame-er of 60 cm or more (Fig. 2). Also, the increased distancef inner organs from the coils in obese patients affects theignal-to-noise ratio and decreases image resolution. Using aody coil rather than a phased-array multicoil and using sat-ration bands could also decrease noise from subcutaneousat. Newer MR scanners, which offer larger (or open) bore,horter bore lengths, and higher table weight limits than in.5-T system, could help to improve the quality of radiolog-cal findings [11,12].
In nuclear medicine, obesity degrades image quality by thebsorption and the scatter of photons within the soft tissuesFig. 3). Also, because the administration of radioisotopes isased on weight, obese patients may exceed the maximumllowable dose may be exceeded in obese patients and con-equently they may not be able to receive the proportionateose of radionuclide for their body weight. Solutions includesing the maximum allowable dose of radionuclide and a
onger time of exposition to maximize counts. Nevertheless,imited irradiation should be encouraged [16].As other invasive procedures such as surgery, interven-ional radiology often requires high intravenous doses of
aimt
gy/Hematology 85 (2013) 193–205 195
eight-based sedative medications that increase the risk ofespiratory depression. Moreover, appropriate planning ofatient positioning, selection of target pathway and appropri-te instrument length are challenging in obese patients. Obeseatients are also at increased risk of technical failure rate ofenous port device access and related complications [17–19],hich can hinder the delivery of systemic treatments.
.2. Oncologic surgical results among high BMI patients
Poorer surgical access to tumor, contraindications to anes-hesia and higher rates of complications may partially explainhe higher mortality among overweight patients with cancer.owever, it remains difficult to determine whether onco-
ogic and functional results in obese patients differ to a largextent from those in non-obese patients. As an example, inncologic patients, oncologic post-op venous thromboem-olic events correlated with body mass index ≥35, but alsondependently with other comorbidities (pulmonary and renalisease), advanced age (≥60 years), reintubation, cardiacrrest, postoperative infectious complications, and prolongedospitalization [20,21]. For this purpose, we reviewed hereost-op observations for colo-rectal, prostate, uterus, andreast cancer.
Rectal cancer is usually treated with perioperativeadiation ± chemotherapy and conservative surgery orbdominoperineal resection. Subgroup analyses of the inter-roup 0114 prospective study (1700 patients, including 18%bese) showed that male obese patients had an increasedate of abdominoperineal resection, an increased risk ofocal recurrence (HR 1.6, 95% CI 1.0–2.6) and a trend forower disease-free survival when compared with normal-eight males [22]. Increased local recurrence after totalesorectal excision in obese rectal cancer patients has been
ttributed to technical difficulties associated with adipos-ty. Conversely, in a series of 596 patients (27% obese)ith T3/4 and/or N1 rectal adenocarcinoma treated from998 to 2007 with neoadjuvant therapy followed by radicalesection using total mesorectal excision, overall and disease-ree survival were similar between obese and non-obeseatients. Higher BMI neither significantly compromisedphincter preservation, complete resection nor negativelyffected long-term outcomes. These findings might be relatedo the fact that resection was performed in a specializedenter with dedicated oncologic surgeons. However, higherMI was associated with longer operative time and longerospital stay [23]. Concerning colon cancer, laparoscopicurgery has now appeared to be a feasible and safe alterna-ive to laparotomy. Makino et al. performed a comprehensiveeview for the years 1983–2010 to compare colon cancerbese (n = 1766) and non-obese (n = 7465) patients. In theirnalysis, despite obesity was associated with longer oper-
tive and higher conversion rate, there was no negativempact of obesity on intraoperative blood loss, perioperativeortality, reoperation, recovery of gastrointestinal func-ion rate by using laparoscopic procedure [24]. Moreover,

196 H. Hijazi et al. / Critical Reviews in Oncology/Hematology 85 (2013) 193–205
F ids andi
po
rgpe(bi
rrop2aw
Fo
ig. 1. Physiological modifications of obese patient anatomy. Enlarged parots shown without contrast medium injection.
athologically obesity does not increase wound healing dis-rders and infections involving the minilaparotomy site [25].
Although evidence suggests obesity as an independentisk factor for a less optimal control rate for patients under-oing prostatectomy, the direct role of BMI in relapse ofrostate cancer remains discussed [26,27]. While Freedlandt al. reported on 385 patients that moderate or severe obesity
2
BMI ≥ 35 kg/m ; n = 55) was an independent predictor ofiochemical failure (hazard ratio: 2.09), Amling et al. showedn 3162 patients that BMI did not influence biochemicalww[
ig. 2. Challenges in imaging of obese patients. Wraparound artifacts are shown onn the left side.
enlarged nodal areas. Retropectoral subclavicular lymphadenopathy (arrow)
ecurrence-free survival [28,29]. Nevertheless, complicationates seem to be higher in an obese population. In a seriesf 4500 patients undergoing radical surgery (open radicalrostatectomy in 75% and laparoscopic prostatectomy in5%, including 97 robotic-assisted procedures), symptomaticnastomotic strictures developed in 198 patients (4%) andere more likely in obese patients [30]. Overall, obesity
as associated with a slower recovery of bowel function,orse quality of life after radical retropubic prostatectomy31]. In addition, research has suggested that, among men
both sides of this obese prostate cancer. Patient (BMI: 38), predominantly

H. Hijazi et al. / Critical Reviews in Oncology/Hematology 85 (2013) 193–205 197
F reast ca ◦r MIP cod
ucp
c8aaipgrttlcmrt
wtopa
aoeir[cpr1oor[
tdp
2c
ig. 3. Diagnostic limitations in imaging of obese patients. A 73 year-old bight diaphragm retraction (A–C) with photon scatter (B). Contrary to theisclosing the distal pulmonary emboli (arrow).
ndergoing prostatectomy, surgical margins may not be aslean in obese men and they may have fewer nerve bundlesreserved [32].
Similar finding were suggested in surgery of endometrialancer. In a retrospective series, Craquant et al. described1 patients receiving hysterectomy with oophorectomynd pelvic lymphadenectomy by laparoscopic and vaginalpproach. In the 50% obese patients, operating times werencreased in comparison of non-obese patients but com-lications and disease-free survival were similar in bothroup. Of note, one patient treated by laparotomy nevereceived intended radiotherapy because of a delay greaterhan three months caused by a cutaneous necrosis. Authorshen concluded that, when compared with laparotomy, theaparoscopic approach was feasible with similar operativeomplications, shorter hospital stay and less abdominal wallorbidity, associated with a lower risk to delay adjuvant
adiotherapy in an obese population as compared with laparo-omy [33].
Regarding breast surgery, higher rates of complicationsere described in a series of 718 surgical breast reconstruc-
ion patients including 64 (9%) obese patients. The rates
f overall complications were significantly higher for obeseatients. Indeed, flap complications were 39% and 20%, over-ll donor-site complications 23% and 11%, infection 5%fh
ncer female patient (BMI: 41) presenting with dyspnea, fever (38 2C), andronal reformations (C), the axial native view (D) was the only technique
nd 1%, seroma 9% and 1%, and hernia 6% and 2% inbese and normal-weight patients, respectively [34]. Pinsollet al. also showed an increased risk of complications, namelynfection and capsular contracture, after immediate breasteconstruction using myocutaneous flaps in obese patients35]. Additionally, conservative breast surgery was also asso-iated with an increased risk of arm lymphedema in obeseatients in a series of 282 patients. Indeed, higher BMI waselated with a greater frequency (36% of obese patients vs.2% in the non-obese group) and severity of arm edema (9%f obese patient’s vs. 2% in the non-obese patients). Thisbservation corroborated prior studies showing an increasedisk of arm edema in obese patients undergoing mastectomy36].
Post-operative complications can also impact on adjuvantreatment, increasing the delay of administration. Moreover,osing of chemotherapy and radiation therapy among obeseatients is a key issue.
.3. Dose uncertainty in obese patients receivinghemotherapy
Evidence-based methods for determining suitable dosingor patients with high BMI are lacking. In this setting, theistorical assumption that metabolism is proportional to body

1 Oncolo
ssapvaact
itiNwnccsatsbpc
sdnpaoocrwaac(lwowwIcwhpbbifpd
awoacilbasu
nB
2p
mtoaaaiocms5tp(v(tc
tor(ocrc1rtci
98 H. Hijazi et al. / Critical Reviews in
urface area may not be true. A basic appreciation of how obe-ity alters volume of distribution and clearance of hydrophilicnd lipophilic drugs is still required for determining appro-riate dosage regimens. Broadly, obese patients have a largerolume of distribution for lipophilic drugs, increased clear-nce of hydrophilic drugs, and a decrease in lean body massnd tissue water, compared to non-obese controls [37]. Thesehanges potentially impact on therapy-related efficacy andoxicity [4,38–40].
With increasing attention being paid to chemotherapy dosentensity as a predictor of treatment response in numerousumor types, careful reconsideration of the optimal dosingn obese patients may be appropriate for some drugs [41].onetheless, chemotherapy dose is capped for the very obese,hich may confound the interpretation of outcomes and prog-osis [42]. It is also suggested that clinicians often reducehemotherapy doses when treating obese patients because ofoncerns about overdosing and toxicity. In fact, it has beenhown that systematic reduced dose of adjuvant chemother-py in obese patients with breast cancer may occurs in upo 40%, resulting in worse outcome [43–45]. However, in aeries of 1431 women receiving adjuvant chemotherapy forreast cancer initially dosed according to actual weight, obeseatients did not experience excess toxicity or poorer outcomeompared with non obese women [43].
Sparreboom et al. reevaluated pharmacokinetic data sub-ets from previously published studies of eight anticancerrugs and compared results for obese patients to those with aormal BMI. They concluded that there is no support for theractice of dose reduction based on sole obesity. This studylso supported the use of actual body weight rather somether alternate weight descriptors for dose calculation in thebese [46]. Similarly, in a study of 262 patients with small-ell lung cancer, no support for empiric chemotherapy doseeductions based on ideal body weight. Indeed, actual bodyeight used when determining initial doses of chemother-
py resulted in similar toxicity from treatment or survivalccording to BMI levels [47]. Overall, a panel of expertsonvened by the American Society of Clinical OncologyASCO) confirmed that up to 40% of obese patients receiveimited chemotherapy doses that are not based on actual bodyeight and that concerns about toxicity or overdosing basedn the use of actual body weight, are unfounded [48]. Any-ay, pharmacokinetic studies are still required to determinehether these subgroups have different drug dispositions.
ndeed, it was reported that the absolute clearance of certainhemotherapy such as cisplatin, paclitaxel, and troxacitabineas significantly increased in the obese [46]. Several studiesave shown the utility of toxicity-adjusted dose, and furtherrospective trials are underway. Appreciating the differentody shapes and sizes that contribute to a high BMI cannote overemphasized, and probably results in patient’s overdos-
ng. As an example, a tall, muscular patient with little bodyat may have a very different drug disposition from anotheratient with significant central obesity from metabolic syn-rome. Sarcopenic obesity is increasingly described in all2wis
gy/Hematology 85 (2013) 193–205
ge groups; it is associated with a poorer prognosis in patientsith solid tumors, compared with non-sarcopenic obese. Onef the reasons may be an increased toxicity of chemother-py drugs primarily metabolized by fat-free mass, such asapecitabine, leading to a reduction of chemotherapy doses,tself responsible for a worse prognosis [49]. Finally, the fol-owing rules (based on the ASCO guidelines) may most likelye useful: (1) body surface area should not be capped at anrbitrary value, (2) actual body weight should be used and (3)ome drugs have special specifications, such as carboplatin,sing the AUC formula [48,50].
Similarly, there are also concerns regarding the effective-ess incertitude and the ability to deliver radiation in highMI patients.
.4. Concerns in radiation accuracy for high BMIopulation
While post-operative complications previously describeday impact on the possible use of adjuvant radiation, radio-
herapy alone may also play a main curative-intent role inbese patients excluded from surgery. As a matter of fact, inseries of 766 consecutive women undergoing hysterectomynd bilateral salpingo-oophorectomy for endometrial cancer,djuvant pelvic radiation treatment was statistically admin-stered more often in non-obese women (p 0.01) [51]. At thepposite, Davies reported that in a large cohort of prostateancer patients, a significant trend toward nonsurgical treat-ent modalities was apparent with increasing BMI. In this
eries of over 5041 men (51% overweight, 17% obese, and% morbidly obese) with clinically localized prostate cancer,he adjusted odds ratio (OR) of receiving nonsurgical thera-ies rather than radical prostatectomy increased with obesityp 0.003). In fact, compared with normal-weight patients,ery obese patients were more likely to receive brachytherapyOR: 1.59), external radiation (OR: 1.29), primary androgenherapy only (OR: 1.77), or active surveillance (OR: 1.06)ompared with radical prostatectomy [52].
Anyway, the influence of obesity on radiotherapy effec-iveness is discussed. For example, in a retrospective studyf 111 head and neck obese who underwent surgery oradio-chemotherapy [53], comparable median follow up38 months) and five-year overall survival (50%) werebserved in non obese patients. Nevertheless, clinical out-ome studies on prostate cancer have suggested, as in patientseceiving prostatectomy, the influence of BMI on biochemi-al failure after radiotherapy. In a retrospective study with,868 patients of whom 21% were obese, external-beamadiotherapy alone was given on localized prostate cancer. Inhis population, BMI remained a significant predictor of bio-hemical relapse (p = .008). Palma et al. reported 706 patients,ncluding 28% with normal weight, 51% overweight and
2% obese with localized prostate adenocarcinoma treatedith radiotherapy. While the different groups did not differn terms of Gleason score, pre-treatment PSA, or stage, obe-ity correlated with a lower serum testosterone levels and

H. Hijazi et al. / Critical Reviews in Oncology/Hematology 85 (2013) 193–205 199
Fig. 4. Example of amputated field-of-view with bordering field artifacts. Uncertainties in dose delivery may necessitate radiation re-planning but with limitedo ajor dosd
b[aPoswwottr
mpaauilOtOba
bbtstwppciaChrtur[rTot
ptions for small anneal CT scanners. Two patients with a BMI over 44; mosimetry as planned for stereotactic radiation treatment.
iochemical relapse and prostate-cancer-specific mortality54]. Moreover, despite BMI correlated with younger agend increased prostate volume at diagnosis (P = 0.003 and= 0.002, respectively), no significant correlation between
besity measures and T-stage, Gleason score, prostate-pecific antigen or percentage of positive cores at biopsyas found [55]. Noteworthy, Wong et al. found that thereas a shift in the delivery of external-beam radiation inbese patients with prostate cancer, with consequently thearget location not receiving the full dose. This may explainhe higher recurrence rate with conventional external beamadiation therapy [56].
Indeed, technical limitations interfere with the manage-ent of obese patients in radiotherapy. Undeniably, similar
hysical constraint as in radiology described earlier exists,s the aperture opening diameter (Fig. 4), the table weightnd with X-ray setup. Multimodal imaging with PET or MRIsed for treatment planning may also be limited. Challengen terms of daily reproducibility is high and could probablyead to uncertainties in terms of accuracy of treatment (Fig. 5).ther adaptations include the use of back and side pointers,
he number and incidence of fields or additional time [57–61].
ther adaptation includes prone breast irradiation for mor-idly obese patients receiving radiation for breast cancer. Instudy on 110 patients with a median BMI of 34 treated withidc
e calculation illustrating uncertainties for beams entering through arms on
reast conserving surgery followed by 3D-conformal wholereast irradiation in prone position between showed favorableoxicity profiles and excellent cosmesis [62]. However, as thetandard remain supine position in breast radiation, prospec-ive assessment of tumor delivery in obese breast canceromen remains necessary [63]. Anyhow, the setup errors arearticularly high in pelvic radiation. In a recent series of 30atients (median BMI = 33, 27% obese) with endometrial car-inoma treated with intensity-modulated radiotherapy, dailymage guidance showed that daily shifts, systematic errorsnd margin requirements were greater in obese patients [64].onsequently, intra-operative irradiation and brachytherapyave been proposed as a feasible alternative to external beamadiation therapy in obese patients [65,66]. In fact, prospec-ive data on rectal dosimetry/toxicity of 407 patients whonderwent iodine-125 prostate implant did not show higherectal wall dose or higher Grade 3 toxicity in obese patients67]. Moreover, there was no evidence for higher rates ofecurrence among obese men undergoing brachytherapy [68].herefore, brachytherapy seems an attractive treatment forbese prostate cancer patients. Another technical question ishe use of special procedures such as stereotactic irradiation
n obese patients [69]. A new stereotactic frame system wasesigned at Indiana University to utilize the precision motionontrol of newer accelerator couches with promising results
200 H. Hijazi et al. / Critical Reviews in Oncology/Hematology 85 (2013) 193–205
Fig. 5. Example of difficulties in daily setup in obese patients. (a) Left: female BMI 48, anal cancer; right: male patient BMI 45 prostate cancer and (b) headand neck cancer female BMI 42.
[efi
tphbbw
iioh
bs
70]. On the other hand, advantages of other high-tech accel-rator such as tomotherapy include a large anneal with a largeeld of view [71,72].
New high-tech radiation device could also help decreaseoxicity in this perceptive population in which delayed com-lications may occur. In obese breast cancer patients, aigher rate of lymphedema, reduction in shoulder mobility,
rachial plexopathy, and radiation-induced pneumonitis haveeen described [66,73–75]. BMI also correlates with chestall pain in lung cancer patients treated with stereotacticprt
rradiation [76]. Impact of BMI on treatment-related toxicityn patients with stages II and III rectal cancer treated with peri-perative radiation ± chemotherapy and conservative surgeryave been presented above [22].
At this time, efforts are made to develop predictiveiological models for radiation-induced toxicity. Under-tanding these molecular links may also provide new
reventive and therapeutic strategies to decrease cancerisk and mortality in an increasingly obese popula-ion.
H. Hijazi et al. / Critical Reviews in Oncology/Hematology 85 (2013) 193–205 201
Fig. 6. Molecular pathways implicated in carcinogenesis in obese patients. Inflammatory cells of the adipose tissue secrete IL-6 and tumor necrosis factor-alpha(TNFa) that may activate JAK-signal transducer and activator of transcription (STAT) and nuclear factor-�B (NFKb) respectively. Increase hormonal releaseincludes adiponectin and leptin, both secreted from adipocytes. Obesity also results in higher levels of insulin and insulin-like growth factor (IGF). Activationof adiponectin receptor (ADIPOR) activates the AMP-activated kinase (AMPK) and phosphatidylinositol 3-kinases (PI3K) pathway. On the other hand, theleptin receptor (OBR) can activate JAK–STAT signaling and extracellular-signal-regulated kinases (ERK), implicated in carcinogenesis. Insulin and IGF bindI R pathm
3t
3o
aftssNmpppiai
stt
ea[cat[cfsvcgtmasdoIp
GF1 receptor (IGF1R) resulting in an activation of the PI3K–AKT–mTOonoacylglycerol lipase (MAGL) and the fatty acid synthase (FASN).
. Prospects: from biological assumption to newherapeutic strategies and toxicity prediction?
.1. Biological pathways implicated in tumorigenesis ofbese patients
The mechanisms through which obesity is associated withn increased cancer risk are probably complex and multi-actorial [77], with different pathways implicated in differentypes of malignancies [4]. Doubtless, physical mechanismsuch as the contribution of abdominal obesity to gastroe-ophageal reflux for esophageal adenocarcinoma exist [57].evertheless, understanding possible common fundamentalolecular pathways could lead to the development of crucial
reventive or curative intent therapies for the increasing obeseopulation with cancer. Currently, the convergences of threeotential mechanisms are involved in cancer developmentn obese patients: changes in hormone signaling (adipokinesnd insulin), increased availability of lipids, and increasednflammation (Fig. 6) [6,78].
The adipokines (leptin and adiponectin) are cytokines
ecreted by adipose tissue. The ob or Lep gene codes forhe adipocyte-derived hormone leptin that acts as a nega-ive feedback “adipostatic” signal to brain centers to reduceabe
way. Finally higher neoplastic lipogenesis may implicate enzyme as the
nergy intake. Leptin regulates appetite and metabolismnd has been associated with obesity and inflammation79]. Interestingly, some authors suggested its role in car-inogenesis. Indeed, leptin may act as a growth factor byctivating ERK or JAK signal transducer and activator ofranscription (STAT3) pathways, both known as oncogenes80,81]. Another adipokine that may play a role in can-er is adiponectin: its levels inversely correlate with bodyat percentage in adults. Adiponectin also increases insulinensitivity, decreases inflammation and promotes cell sur-ival. As for leptin, evidence suggests that adiponectineould play a role in cancer promotion by activating onco-enic pathways such as PI3K–AKT–mTOR signaling andhe AMP-activated kinase (AMPK) [82,83]. The last hor-ones implicated in cancer among obese patients are insulin
nd possibly insulin-like growth factor (IGF), which shareequence homologies with insulin. Obese people have someegree of insulin resistance, associated with elevated levelsf circulating insulin. Downstream activation by insulin andGF may trigger the oncogenic RAS–MAPK and PI3K–AKTathways [78]. Because new available targeted therapies such
s mTOR inhibitors are in development, those findings mayecome of great interest for a therapeutic-intent strategy. Nev-rtheless, it remains unknown if such molecular deregulation
2 Oncolo
ip
iltctiinilaoidrsIftnr
3r
vmincfictaclpinlwlbigsenfi
cm
4
acacrhotptIta
C
d
R
P
O
R
02 H. Hijazi et al. / Critical Reviews in
s constantly associated in tumors affecting the overall obeseopulation.
Other evocated mechanisms implicate increased availabil-ty of lipids and inflammation. Increases in circulating lipidevels in obese patients are controlled by specific enzymeshat might play an oncogenic role. As an example, two impli-ated enzymes are the monoacylglycerol lipase (MAGL) andhe fatty acid synthase (FASN). MAGL is highly expressedn aggressive human cancer cells and primary tumors, wheret regulates a fatty acid network enriched in oncogenic sig-aling lipids that promotes migration, invasion, survival, andn vivo tumor growth [84]. Equally, FASN regulates de novoipogenesis, body weight, tumor growth, and correlates withn increased number of reactive oxygen species [85]. On thether hand, it is well described that the adipose tissue becomesnfiltrated with immune cells as monocytes and macrophagesuring obesity. It has been suggested that cell infiltration mayesult in higher levels of inflammatory cytokines secreteduch as IL-6 and tumor necrosis factor-� (TNF-a). WhileL6 activates JAK–STAT signaling, TNF-a activates nuclearactor-�B, both pathways being able to promote prolifera-ion and metastasis [86,87]. In this setting, aspirin and otheronsteroidal anti-inflammatory drugs might be effective ineducing cancer risks [88].
.2. Biological prediction of toxicity: the example ofadiotherapy
Because late effects from radiotherapy are often irre-ersible, efforts have been made to develop biologicalarkers to detect highly sensitive patients [89]. As toxicity
s often reported for high BMI patients receiving radiation,umerous preclinical studies evaluated such predictive indi-ators in this specific population. Indeed, obese mice lackingunctional leptin receptors have an increased susceptibil-ty to irradiation, poorer recovery and decreased leukocyteounts in peripheral blood in comparison to mice with func-ional receptors [79]. A genotype study on oxidative stressssessed the association of cutaneous toxicity in 466 breastancer Caucasian women who received radiotherapy fol-owing lumpectomy. Compared to non-obese patients, obeseatients with homozygous (GG) genotypes of nitric oxide hadncreased radiation-related toxicity. Overweight/obesity wasot a strong risk factor among women with other endothe-ial nitric oxide synthase and myeloperoxidase genotypes. Itas suggested that women with genotypes related to higher
evels of oxidative stress may help to reveal associationsetween BMI and radiotoxicity [90]. In two other large stud-es, the effect of genotypes of TP53, p21, and DNA repairenes were only observed in normal weight populations,
uggesting a specific pattern in obese patients [91–93]. Nev-rtheless, in a recent prospective trial, none of the singleucleotide polymorphisms in candidate genes were con-rmed. Future subsequent prospective trials are needed togy/Hematology 85 (2013) 193–205
onfirm the hypothesis that published single nucleotide poly-orphisms exert a clinically relevant effect [94].
. Conclusion
The obesity flaw has replaced the smoking epidemic, inn aging population at increased risk of cancer. Lifestylehanges and hygiene issue will be mandatory to counter-ct the epidemiologic wave of overweighed patients withancer. Indeed, weight loss and physical activity reduce theisk for breast and colon cancers [4,95,96]. Anyhow, obesityas clearly become a concern in the therapeutic managementf cancer and do require specific adaptations, not only forhe physician but also for the manufacturers. Future largerospective trials will definitely be warranted to validateherapeutic adaptations in the increasing obese population.ncreased knowledge in biology could be the cornerstone inhe future preventive intent strategies to reduce cancer risknd mortality in an increasingly obese population.
onflict of interest
The authors declare no conflict of interest or financialisclosure.
eviewers
Etienne Chatelut, Institut Claudius-Regaud, 20-24 rue duont Saint-Pierre, F-31052 Toulouse, France.
Cyrus Chargari, Department of Medical and Radiationncology, Val-de-Grâce Hospital, Paris, France.
eferences
[1] Bianchini F, Kaaks R, Vainio H. Overweight, obesity, and cancer risk.Lancet Oncology 2002;3(9):565–74.
[2] Rogers PC, Meacham LR, Oeffinger KC, Henry DW, Lange BJ. Obesityin pediatric oncology. Pediatric Blood and Cancer 2005;45(7):881–91.
[3] Berenson GS. Health consequences of obesity. Pediatric Blood andCancer 2012;58(1):117–21.
[4] Wolin KY, Carson K, Colditz GA. Obesity and cancer. Oncologist2010;15(6):556–65.
[5] Hyde R. Europe battles with obesity. Lancet 2008;371(9631):2160–1.[6] Renehan AG, Roberts DL, Dive C. Obesity and cancer: pathophys-
iological and biological mechanisms. Archives of Physiology andBiochemistry 2008;114(1):71–83.
[7] Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight,obesity, and mortality from cancer in a prospectively studied cohort ofU.S. adults. New England Journal of Medicine 2003;348(17):1625–38.
[8] Department of Health and Human Services Ws. Overweight and obe-
sity: obesity trends – 1991–2001. In: Prevalence of obesity among U.S.adults by state. Centers for Disease Control and Prevention; 2001.[9] Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, BalesVS, et al. Prevalence of obesity, diabetes, and obesity-related health

Oncolo
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
H. Hijazi et al. / Critical Reviews in
risk factors, 2001. Journal of the American Medical Association2003;289(1):76–9.
10] Polednak AP. Trends in incidence rates for obesity-associated cancersin the US. Cancer Detection and Prevention 2003;27(6):415–21.
11] Reynolds JV, Donohoe CL, Doyle SL. Diet, obesity and cancer. IrishJournal of Medical Science 2011;180(2):521–7.
12] Uppot RN. Impact of obesity on radiology. Radiologic Clinics of NorthAmerica 2007;45(2):231–46.
13] Guest AR, Helvie MA, Chan HP, Hadjiiski LM, Bailey JE, RoubidouxMA. Adverse effects of increased body weight on quantitative measuresof mammographic image quality. American Journal of Roentgenology2000;175(3):805–10.
14] Yanch JC, Behrman RH, Hendricks MJ, McCall JH. Increased radiationdose to overweight and obese patients from radiographic examinations.Radiology 2009;252(1):128–39.
15] Schindera ST, Nelson RC, Lee ER, Delong DM, Ngyen G, TonchevaG, et al. Abdominal multislice CT for obese patients: effect on imagequality and radiation dose in a phantom study. Academic Radiology2007;14(4):486–94.
16] Masuda Y, Kondo C, Matsuo Y, Uetani M, Kusakabe K. Comparisonof imaging protocols for 18F-FDG PET/CT in overweight patients:optimizing scan duration versus administered dose. Journal of NuclearMedicine 2009;50(6):844–8.
17] Mansfield PF, Hohn DC, Fornage BD, Gregurich MA, Ota DM. Com-plications and failures of subclavian-vein catheterization. New EnglandJournal of Medicine 1994;331(26):1735–8.
18] Marcy PY, Magne N, Castadot P, Italiano A, Amoretti N, Bailet C,et al. Is radiologic placement of an arm port mandatory in oncol-ogy patients? Analysis of a large bi-institutional experience. Cancer2007;110(10):2331–8.
19] Bach F, Videbaek C, Holst-Christensen J, Boesby S. Cytostatic extrava-sation. A serious complication of long-term venous access. Cancer1991;68(3):538–9.
20] Khorana AA, Francis CW, Culakova E, Fisher RI, Kuderer NM, LymanGH. Thromboembolism in hospitalized neutropenic cancer patients.Journal of Clinical Oncology 2006;24(3):484–90.
21] De Martino RR, Goodney PP, Spangler EL, Wallaert JB, Corriere MA,Rzucidlo EM, et al. Variation in thromboembolic complications amongpatients undergoing commonly performed cancer operations. Journalof Vascular Surgery 2012;55(4):1035–400000.
22] Meyerhardt JA, Tepper JE, Niedzwiecki D, Hollis DR, McCollumAD, Brady D, et al. Impact of body mass index on outcomes andtreatment-related toxicity in patients with stage II and III rectal can-cer: findings from Intergroup Trial 0114. Journal of Clinical Oncology2004;22(4):648–57.
23] Chern H, Chou J, Donkor C, Shia J, Guillem JG, Nash GM, et al. Effectsof obesity in rectal cancer surgery. Journal of the American College ofSurgeons 2010;211(1):55–60.
24] Makino T, Shukla PJ, Rubino F, Milsom JW. The impact of obesity onperioperative outcomes after laparoscopic colorectal resection. Annalsof Surgery 2012;255(2):228–36.
25] Scheidbach H, Benedix F, Hügel O, Kose D, Köckerling F, Lippert H.Laparoscopic approach to colorectal procedures in the obese patient:risk factor or benefit? Obesity Surgery 2008;18:66–70.
26] Mitsuyama H, Wallner KE, Merrick GS. Treatment of prostate can-cer in obese patients. Oncology (Williston Park) 2006;20(10):1191–7[discussion 8, 206, 208].
27] Skolarus TA, Wolin KY, Grubb 3rd RL. The effect of body mass indexon PSA levels and the development, screening and treatment of prostatecancer. Nature Clinical Practice Urology 2007;4(11):605–14.
28] Freedland SJ, Aronson WJ, Kane CJ, Presti Jr JC, Amling CL, ElashoffD, et al. Impact of obesity on biochemical control after radical prosta-tectomy for clinically localized prostate cancer: a report by the Shared
Equal Access Regional Cancer Hospital database study group. Journalof Clinical Oncology 2004;22(3):446–53.29] Amling CL, Riffenburgh RH, Sun L, Moul JW, Lance RS, KusudaL, et al. Pathologic variables and recurrence rates as related to obesity
[
gy/Hematology 85 (2013) 193–205 203
and race in men with prostate cancer undergoing radical prostatectomy.Journal of Clinical Oncology 2004;22(3):439–45.
30] Sandhu JS, Gotto GT, Herran LA, Scardino PT, Eastham JA, Rabbani F.Age, obesity, medical comorbidities and surgical technique are predic-tive of symptomatic anastomotic strictures after contemporary radicalprostatectomy. Journal of Urology 2011;185(6):2148–52.
31] Montgomery JS, Gayed BA, Hollenbeck BK, Daignault S, Sanda MG,Montie JE, et al. Obesity adversely affects health related quality of lifebefore and after radical retropubic prostatectomy. Journal of Urology2006;176(1):257–61 [discussion 61-2].
32] Freedland SJ. Obesity and prostate cancer: a growing problem. ClinicalCancer Research 2005;11(19 Pt 1):6763–6.
33] Caquant F, Mas-Calvet M, Turbelin C, Lesoin A, Lefebvre D, NarducciF, et al. Endometrial cancer by laparoscopy and vaginal approach in theobese patient. Bull Cancer 2006;93(4):402–6.
34] Chang DW, Wang B, Robb GL, Reece GP, Miller MJ, Evans GR, et al.Effect of obesity on flap and donor-site complications in free transverserectus abdominis myocutaneous flap breast reconstruction. Plastic andReconstructive Surgery 2000;105(5):1640–8.
35] Pinsolle V, Grinfeder C, Mathoulin-Pelissier S, Faucher A. Compli-cations analysis of 266 immediate breast reconstructions. Journal ofPlastic, Reconstructive and Aesthetic Surgery 2006;59(10):1017–24.
36] Werner RS, McCormick B, Petrek J, Cox L, Cirrincione C, Gray JR,et al. Arm edema in conservatively managed breast cancer: obesity isa major predictive factor. Radiology 1991;180(1):177–84.
37] Hanley MJ, Abernethy DR, Greenblatt DJ. Effect of obesity onthe pharmacokinetics of drugs in humans. Clinical Pharmacokinetics2010;49(2):71–87.
38] Gurney H, Shaw R. Obesity in dose calculation: a mouse or an elephant?Journal of Clinical Oncology 2007;25(30):4703–4.
39] Dignam JJ, Polite BN, Yothers G, Raich P, Colangelo L, O’Connell MJ,et al. Body mass index and outcomes in patients who receive adjuvantchemotherapy for colon cancer. Journal of the National Cancer Institute2006;98(22):1647–54.
40] Ramos Chaves M, Boleo-Tome C, Monteiro-Grillo I, Camilo M,Ravasco P. The diversity of nutritional status in cancer: new insights.Oncologist 2010;15(5):523–30.
41] Griggs JJ, Sorbero ME, Lyman GH. Undertreatment of obese womenreceiving breast cancer chemotherapy. Archives of Internal Medicine2005;165(11):1267–73.
42] Dignam JJ, Wieand K, Johnson KA, Raich P, Anderson SJ, Somkin C,et al. Effects of obesity and race on prognosis in lymph node-negative,estrogen receptor-negative breast cancer. Breast Cancer Research andTreatment 2006;97(3):245–54.
43] Rosner GL, Hargis JB, Hollis DR, Budman DR, Weiss RB, Hender-son IC, et al. Relationship between toxicity and obesity in womenreceiving adjuvant chemotherapy for breast cancer: results from can-cer and leukemia group B study 8541. Journal of Clinical Oncology1996;14(11):3000–8.
44] Colleoni M, Li S, Gelber RD, Price KN, Coates AS, Castiglione-Gertsch M, et al. Relation between chemotherapy dose,oestrogen receptor expression, and body-mass index. Lancet2005;366(9491):1108–10.
45] Griggs JJ, Culakova E, Sorbero ME, van Ryn M, Poniewierski MS,Wolff DA, et al. Effect of patient socioeconomic status and body massindex on the quality of breast cancer adjuvant chemotherapy. Journalof Clinical Oncology 2007;25(3):277–84.
46] Sparreboom A, Wolff AC, Mathijssen RH, Chatelut E, Rowinsky EK,Verweij J, et al. Evaluation of alternate size descriptors for dose calcu-lation of anticancer drugs in the obese. Journal of Clinical Oncology2007;25(30):4707–13.
47] Georgiadis MS, Steinberg SM, Hankins LA, Ihde DC, Johnson BE.Obesity and therapy-related toxicity in patients treated for small-
cell lung cancer. Journal of the National Cancer Institute 1995;87(5):361–6.48] Griggs JJ, Mangu PB, Anderson H, Balaban EP, Dignam JJ, HryniukWM, et al. Appropriate chemotherapy dosing for obese adult patients

2 Oncolo
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
04 H. Hijazi et al. / Critical Reviews in
with cancer: American society of clinical oncology clinical practiceguideline. Journal of Clinical Oncology 2012;30(May (13)):1553–61.
49] Prado CM, Lieffers JR, McCargar LJ, Reiman T, Sawyer MB, MartinL, et al. Prevalence and clinical implications of sarcopenic obesity inpatients with solid tumours of the respiratory and gastrointestinal tracts:a population-based study. Lancet Oncology 2008;9(7):629–35.
50] Herrington JD, Tran HT, Riggs MW. Prospective evaluation of carbo-platin AUC dosing in patients with a BMI > or = 27 or cachexia. CancerChemotherapy and Pharmacology 2006;57(2):241–7.
51] Martra F, Kunos C, Gibbons H, Zola P, Galletto L, DeBernardo R,et al. Adjuvant treatment and survival in obese women with endome-trial cancer: an international collaborative study. American Journal ofObstetrics and Gynecology 2008;198(1), 89 e1–8.
52] Davies BJ, Walsh TJ, Ross PL, Knight SJ, Sadetsky N, Carroll PR,et al. Effect of BMI on primary treatment of prostate cancer. Urology2008;72(2):406–11.
53] Deneuve S, Tan HK, Eghiaian A, Temam S. Management and outcomeof head and neck squamous cell carcinomas in obese patients. OralOncology 2011;47(7):631–5.
54] Palma D, Pickles T, Tyldesley S. Obesity as a predictor of biochemicalrecurrence and survival after radiation therapy for prostate cancer. BJUInternational 2007;100(2):315–9.
55] Zilli T, Nguyen TV, Bahary JP, Chagnon M, Dufresne A, Taussky D.Prognostic impact of abdominal adiposity, waist circumference andbody mass index in patients with intermediate-risk prostate cancertreated with radiotherapy. International Journal of Obesity (London)2011;35(11):1421–6.
56] Wong JR, Gao Z, Merrick S, Wilson P, Uematsu M, Woo K, et al.Potential for higher treatment failure in obese patients: correlation ofelevated body mass index and increased daily prostate deviations fromthe radiation beam isocenters in an analysis of 1465 computed tomo-graphic images. International Journal of Radiation Oncology, Biology,Physics 2009;75(1):49–55.
57] Jacobson BC, Somers SC, Fuchs CS, Kelly CP, Camargo Jr CA. Body-mass index and symptoms of gastroesophageal reflux in women. NewEngland Journal of Medicine 2006;354(22):2340–8.
58] Rockhill J, Wallner K, Hoffman C, Merrick G, Simpson C,Arthurs S. Prostate brachytherapy in obese patients. Brachytherapy2002;1(1):54–60.
59] Kubo H. Use of oblique simulation films for estimating the maximumdose to the bladder and rectum in obese brachytherapy patients. MedicalPhysics 1995;22(4):441–2.
60] Sweigart KD. A simple method of alignment for pelvic irradiation inobese patients. Medical Dosimetry 2002;27(4):269–70.
61] Mohiuddin MM, Zhang B, Tkaczuk K, Khakpour N. Upright, standingtechnique for breast radiation treatment in the morbidly obese patient.Breast Journal 2010;16(4):448–50.
62] Bergom C, Kelly T, Morrow N, Wilson JF, Walker A, Xiang Q,et al. Prone whole-breast irradiation using three-dimensional confor-mal radiotherapy in women undergoing breast conservation for earlydisease yields high rates of excellent to good cosmetic outcomes inpatients with large and/or pendulous breasts. International Journal ofRadiation Oncology, Biology, Physics 2011;83(3):821–8.
63] Kirby AM, Evans PM, Helyer SJ, Donovan EM, Convery HM, YarnoldJR. A randomised trial of supine versus prone breast radiotherapy (SuPrstudy): comparing set-up errors and respiratory motion. Radiotherapyand Oncology 2011;100(2):221–6.
64] Lin LL, Hertan L, Rengan R, Kevin Teo BK. Effect of body mass indexon magnitude of setup errors in patients treated with adjuvant radio-therapy for endometrial cancer with daily image guidance. InternationalJournal of Radiation Oncology, Biology, Physics 2011;83(2):670–5.
65] Keshtgar MR, Vaidya JS, Tobias JS, Wenz F, Joseph D, Stacey C, et al.Targeted intraoperative radiotherapy for breast cancer in patients in
whom external beam radiation is not possible. International Journal ofRadiation Oncology, Biology, Physics 2011;80(1):31–8.66] Carmichael AR, Bates T. Obesity and breast cancer: a review of theliterature. Breast 2004;13(2):85–92.
[
gy/Hematology 85 (2013) 193–205
67] Patil N, Crook J, Saibishkumar EP, Aneja M, Borg J, Pond G, et al.The effect of obesity on rectal dosimetry after permanent prostatebrachytherapy. Brachytherapy 2009;8(2):218–22.
68] Freedland SJ, Sun L, Kane CJ, Presti Jr JC, Terris MK, Amling CL, et al.Obesity and oncological outcome after radical prostatectomy: impact ofprostate-specific antigen-based prostate cancer screening: results fromthe Shared Equal Access Regional Cancer Hospital and Duke ProstateCenter databases. BJU International 2008;102(8):969–74.
69] Welsh J, Thomas J, Shah D, Allen PK, Wei X, Mitchell K, et al. Obesityincreases the risk of chest wall pain from thoracic stereotactic body radi-ation therapy. International Journal of Radiation Oncology, Biology,Physics 2011;81(1):91–6.
70] Heinzerling JH, Papiez L, Chien S, Anderson J, Forster K, ZhangG, et al. Stereotactic body radiation therapy: evaluation of setupaccuracy and targeting methods for a new couch integrated immo-bilization system. Technology in Cancer Research and Treatment2008;7(3):197–206.
71] Sterzing F, Schubert K, Sroka-Perez G, Kalz J, Debus J, Herfarth K.Helical tomotherapy. Experiences of the first 150 patients in Heidelberg.Strahlentherapie und Onkologie 2008;184(1):8–14.
72] Ramsey CR, Scaperoth D, Seibert R, Chase D, Byrne T, Mahan S.Image-guided helical tomotherapy for localized prostate cancer: tech-nique and initial clinical observations. Journal of Applied ClinicalMedical Physics 2007;8(3):2320.
73] Kirby AM, Evans PM, Donovan EM, Convery HM, Haviland JS,Yarnold JR. Prone versus supine positioning for whole and partial-breast radiotherapy: a comparison of non-target tissue dosimetry.Radiotherapy and Oncology 2010;96(2):178–84.
74] Varga Z, Hideghety K, Mezo T, Nikolenyi A, Thurzo L, Kahan Z. Indi-vidual positioning: a comparative study of adjuvant breast radiotherapyin the prone versus supine position. International Journal of RadiationOncology, Biology, Physics 2009;75(1):94–100.
75] Patel RR, Becker SJ, Das RK, Mackie TR. A dosimetric compari-son of accelerated partial breast irradiation techniques: multicatheterinterstitial brachytherapy, three-dimensional conformal radiother-apy, and supine versus prone helical tomotherapy. InternationalJournal of Radiation Oncology, Biology, Physics 2007;68(3):935–42.
76] Woody NM, Videtic GM, Stephans KL, Djemil T, Kim Y, Xia P.Predicting chest wall pain from lung stereotactic body radiotherapyfor different fractionation schemes. International Journal of RadiationOncology, Biology, Physics 2011;83(1):427–34.
77] Roberts DL, Dive C, Renehan AG. Biological mechanisms linking obe-sity and cancer risk: new perspectives. Annual Review of Medicine2010;61:301–16.
78] Khandekar M, Cohen P, Spiegelman B. Molecular mecha-nisms of cancer development in obesity. Nature Reviews Cancer2011;24(1112):886–95, http://dx.doi.org/10.1038/nrc3174.
79] Gove ME, Sherry CL, Pini M, Fantuzzi G. Generation of leptin receptorbone marrow chimeras: recovery from irradiation, immune cellularity,cytokine expression, and metabolic parameters. Obesity (Silver Spring)2010;18(12):2274–81.
80] Banks AS, Davis SM, Bates SH, Myers Jr MG. Activation of down-stream signals by the long form of the leptin receptor. Journal ofBiological Chemistry 2000;275(19):14563–72.
81] Kanai M, Konda Y, Nakajima T, Izumi Y, Kanda N, Nanakin A,et al. Differentiation-inducing factor-1 (DIF-1) inhibits STAT3 activityinvolved in gastric cancer cell proliferation via MEK-ERK-dependentpathway. Oncogene 2003;22(4):548–54.
82] Cong L, Chen K, Li J, Gao P, Li Q, Mi S, et al. Regulation of adiponectinand leptin secretion and expression by insulin through a PI3K-PDE3Bdependent mechanism in rat primary adipocytes. Biochemical Journal2007;403(3):519–25.
83] Holland WL, Miller RA, Wang ZV, Sun K, Barth BM, Bui HH,et al. Receptor-mediated activation of ceramidase activity initiatesthe pleiotropic actions of adiponectin. Nature Medicine 2011;17(1):55–63.

Oncolo
[
[
[
[
[
[
[
[
[
[
[
[
[
B
tNsaAeapatthmGORTEC (Groupe d’Oncologie Radiotherapie des Tumeurs
H. Hijazi et al. / Critical Reviews in
84] Nomura DK, Long JZ, Niessen S, Hoover HS, Ng SW, Cravatt BF.Monoacylglycerol lipase regulates a fatty acid network that promotescancer pathogenesis. Cell 2010;140(1):49–61.
85] Nguyen PL, Ma J, Chavarro JE, Freedman ML, Lis R, Fedele G,et al. Fatty acid synthase polymorphisms, tumor expression, body massindex, prostate cancer risk, and survival. Journal of Clinical Oncology2010;28(25):3958–64.
86] Weisberg SP, McCann D, Desai M, Rosenbaum M, Leibel RL, FerranteJr AW. Obesity is associated with macrophage accumulation in adiposetissue. Journal of Clinical Investigation 2003;112(12):1796–808.
87] Park EJ, Lee JH, Yu GY, He G, Ali SR, Holzer RG, et al. Dietaryand genetic obesity promote liver inflammation and tumorigenesis byenhancing IL-6 and TNF expression. Cell 2010;140(2):197–208.
88] Rothwell PM, Fowkes FG, Belch JF, Ogawa H, Warlow CP, MeadeTW. Effect of daily aspirin on long-term risk of death due to can-cer: analysis of individual patient data from randomised trials. Lancet2011;377(9759):31–41.
89] Burnet NG, Elliott RM, Dunning A, West CM. Radiosensitivity,radiogenomics and RAPPER. Clinical Oncology (Royal College ofRadiologists) 2006;18(7):525–8.
90] Ahn J, Ambrosone CB, Kanetsky PA, Tian C, Lehman TA, KroppS, et al. Polymorphisms in genes related to oxidative stress (CAT,MnSOD, MPO, and eNOS) and acute toxicities from radiation ther-apy following lumpectomy for breast cancer. Clinical Cancer Research2006;12(23):7063–70.
91] Tan XL, Popanda O, Ambrosone CB, Kropp S, Helmbold I, vonFournier D, et al. Association between TP53 and p21 genetic polymor-phisms and acute side effects of radiotherapy in breast cancer patients.Breast Cancer Research and Treatment 2006;97(3):255–62.
92] Chang-Claude J, Ambrosone CB, Lilla C, Kropp S, Helmbold I, vonFournier D, et al. Genetic polymorphisms in DNA repair and damageresponse genes and late normal tissue complications of radiotherapyfor breast cancer. British Journal of Cancer 2009;100(10):1680–6.
93] Chang-Claude J, Popanda O, Tan XL, Kropp S, Helmbold I, von
Fournier D, et al. Association between polymorphisms in the DNArepair genes, XRCC1, APE1, and XPD and acute side effects ofradiotherapy in breast cancer patients. Clinical Cancer Research2005;11(13):4802–9.dcA
gy/Hematology 85 (2013) 193–205 205
94] Barnett GC, Coles CE, Elliott RM, Baynes C, Luccarini C, ConroyD, et al. Independent validation of genes and polymorphisms reportedto be associated with radiation toxicity: a prospective analysis study.Lancet Oncology 2012;13(1):65–77.
95] Jacquelin-Ravel N, Pichard C. Clinical nutrition, body composition andoncology: a critical literature review of the synergies. Critical Reviewsin Oncology/Hematology April 2012 [Epub ahead of print].
96] Brinksma A, Huizinga G, Sulkers E, Kamps W, Roodbol P, TissingW. Malnutrition in childhood cancer patients: a review on its preva-lence and possible causes. Critical Reviews in Oncology/HematologyJanuary 2012 [Epub ahead of print].
iography
Dr. Juliette Thariat, MD, PhD is an Assistant Professor inhe Department of Radiation Oncology at the University ofice Sophia Antipolis, France. She had her clinical fellow-
hip at the European Hospital Georges Pompidou in Paris,nd research fellowship with Pr Kian Ang as mentor at M.D.nderson Cancer Center, Houston, US. Her areas of inter-
st include head and neck, sarcoma, bladder, rare tumorsnd innovative radiation techniques including cyberknife androtons. Her research interests include the biology of headnd neck cancer, the use of mass spectrometry for transla-ional research and innovative radiation techniques. She ishe national organizer of the French “high tech diploma”. Sheas more than 100 peer reviewed papers and 100 oral com-unications or posters. She is the executive secretary of the
e la Tete et du Cou) and REFCOR (reseau d’expertise Fran-ais des Cancers ORL Rares) and member of the SFRO,STRO and GSF-GETO.























![4-Anesthesia and Obese Patients[1]](https://img.pdfslide.us/doc/110x75/577ce1b21a28ab9e78b605c5/4-anesthesia-and-obese-patients1.jpg)



