Embed Size (px)
Citation preview

relation to aortic diameter, the tim-ing of balloon inflation in diastoleand deflation in systole, and thepatient’s own blood pressure andvascular resistance.3,4
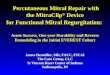
The Impella 2.5 (Figure 1) aspi-rates up to 2.5 L/min of blood fromthe left ventricle and displaces it intothe ascending aorta, rapidly unload-ing the left ventricle and increasingforward flow. It reduces myocardialoxygen consumption, improves meanarterial pressure, and reduces pul-monary capillary wedge pressure.2
The Impella provides a greaterincrease in cardiac output than theIABP provides. In one trial5 inwhich an IABP was compared withan Impella in cardiogenic shockpatients, after 30 minutes of ther-apy, the cardiac index (calculated ascardiac output in liters per minutedivided by body surface area insquare meters) increased by 0.5 inthe patients with the Impella com-pared with 0.1 in the patients withan IABP. Unlike the IABP, the Impelladoes not require timing, nor is atrigger from an electrocardiographicrhythm or arterial pressure needed(Table 1). The device received 510(k)clearance from the Food and DrugAdministration in June 2008 forproviding up to 6 hours of partial
Brenda McCulloch, RN, MSN
Impella 2.5, and discuss implica-tions for nursing care for patientsreceiving extended support froman Impella 2.5. Additionally, I shareour experiences as we developed ourImpella program at our communityhospital. Routine management ofpatients after PCI is not addressed.
IABP therapy has been in usesince the late 1960s and has beenwidely used in clinical practice sincethat time. The IABP decreases after-load, decreases myocardial oxygenconsumption, increases coronaryartery perfusion, and modestlyenhances cardiac output.1,2 The IABPcannot provide total circulatorysupport. Patients must have somelevel of left ventricular function foran IABP to be effective. Optimalhemodynamic effect from the IABPis dependent on several factors,including the balloon’s position inthe aorta, the blood displacementvolume, the balloon diameter in
©2011 American Association of Critical-Care Nurses doi: 10.4037/ccn2011293
The Impella 2.5 is a percutaneously placed partial circulatory assist device thatis increasingly being used in high-risk coronary interventional procedures to providehemodynamic support. The Impella 2.5 is able to unload the left ventricle rapidlyand effectively and increase cardiac output more than an intra-aortic balloon cathetercan. Potential complications include bleeding, limb ischemia, hemolysis, and infec-tion. One community hospital’s approach to establishing a multidisciplinary programfor use of the Impella 2.5 is described. (Critical Care Nurse. 2011;31[1]:e1-e16)
Use of the Impella 2.5 inHigh-Risk PercutaneousCoronary Intervention
Feature
Patients who undergo high-risk percutaneous coro-nary intervention (PCI),such as procedures onfriable saphenous vein
grafts or the left main coronaryartery, may have an intra-aorticballoon catheter placed if theyrequire hemodynamic support dur-ing the procedure. Currently, theintra-aortic balloon pump (IABP)is the most commonly used devicefor circulatory support. A neweroption that is now available for selectpatients is the Impella 2.5, a short-term partial circulatory supportdevice or percutaneous ventricularassist device (VAD).
In this article, I discuss theImpella 2.5, review indications andcontraindications for its use, delin-eate potential complications of the
e1 CriticalCareNurse OnlineNOW www.ccnonline.org
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

circulatory support. In Europe, theImpella 2.5 is approved for use up to5 days. Reports of longer durationof therapy in both the United Statesand Europe have been published.8,9
The Impella 2.5 has been usedfor hemodynamic support duringhigh-risk PCI and for hemodynamicsupport of patients with myocardialinfarction complicated by cardiogenicshock or ventricular septal defect,
cardiomyopathywith acutedecompensa-tion, postcar-diotomy shock,off-pump coro-nary arterybypass graftingsurgery, or hearttransplant rejec-tion and as abridge to thenext decision.9
ClinicalResearchand RegistryFindings
In Europe,the Impella 2.5has been in wideuse for severalyears.8,9 In theUnited States,several smalltrials5,6,9-12 havebeen completedor are underway
to evaluate the Impella 2.5. Abiomedhas sponsored several of these trials,including PROTECT I, PROTECT II,RECOVER I, RECOVER II, andISAR-SHOCK.
The PROTECT I study was doneto assess the safety and efficacy ofdevice placement in patients under-going high-risk PCI.10 Twenty patientswere enrolled in that prospective,multicenter study. All had poor
ventricular function (ejection frac-tion ≤35%) and had PCI on an unpro-tected left main coronary artery orthe last remaining patent coronaryartery or graft. The device was suc-cessfully placed in all patients, andthe duration of support ranged from0.4 to 2.5 hours. None of the patientshad hemodynamic instability developduring the procedure. Two patientshad transient hemolysis that wasnot clinically significant. Followingthis trial, the Impella 2.5 devicereceived its 510(k) approval fromthe Food and Drug Administration.
The ISAR-SHOCK trial was doneto evaluate the safety and efficacy ofthe Impella 2.5 versus the IAPB inpatients with cardiogenic shock dueto acute myocardial infarction.5
Patients were randomized to sup-port from an IABP (n=13) or anImpella (n=12). One patient diedbefore implantation of a device.The trial’s primary end point ofhemodynamic improvement wasdefined as improved cardiac indexat 30 minutes after implantation.Improvements in cardiac index weresignificantly greater in the patientswith the Impella than in patientswith the IABP (P=.02). The patients’diastolic pressure increased signifi-cantly more with Impella supportthan with IABP support (P=.002).Mean arterial pressure increased inpatients with an Impella more thanit increased in patients with an IABP,but the difference was not signifi-cant (P=.09). The use of inotropicagents and vasopressors was similarin both groups of patients. Serumlevel of lactate was lower in patientstreated with the Impella. Hemolysis,as measured by the plasma level offree hemoglobin, was higher inpatients treated with the Impella.
BrendaMcCulloch is a cardiovascular clinical nurse specialist at Sutter Heart and VascularInstitute, Sutter Medical Center, Sacramento, California.
Author
Corresponding author: Brenda McCulloch, RN, MSN, Sutter Heart and Vascular Institute, Sutter Medical Center,5301 F Street, Suite 304, Sacramento, CA 95819 (e-mail: [email protected]).
To purchase electronic or print reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656.Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected].
www.ccnonline.org CriticalCareNurse OnlineNOW e2
Figure 1 Impella 2.5 cardiac assist device in left ventricle.Image courtesy ABIOMED Inc, Danvers, Massachusetts.
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

More blood products were adminis-tered to patients treated with theImpella.
Results from additional clinicaltrials are available (Table 2), but con-tinuing clinical trials are essential toevaluate the effectiveness of the Impella2.5 device in various subgroups.
Device DesignThe Impella 2.5 catheter (Figure 2)
contains a nonpulsatile microaxialcontinuous flow blood pump (Figure3) that pulls blood from the left ven-tricle to the ascending aorta, creatingincreased forward flow and increasedcardiac output. An axial pump is onethat is made up of impellar blades, orrotors, that spin around a centralshaft; the spinning of these blades iswhat moves blood through thedevice.13 The distal tip of pigtail curveis 6F in size (Figure 4). The Impella 2.5
catheter shaft size is 9F and is 12Fat its largest point, which is themicroaxial blood pump.
The Impella 2.5 catheter has 2lumens. A tubing system called theQuick Set-Up has been developedfor use in the catheterization labora-tory. It is a single tubing system thatbifurcates and connects to each portof the catheter. This arrangementallows rapid initial setup of the con-sole so that support can be initiatedquickly. When the Quick Set-Up isused, the 10% to 20% dextrose solu-tion used to purge the motor is notheparinized. One lumen carries fluidto the impellar blades and continu-ously purges the motor to preventthe formation of thrombus. Theproximal port of this lumen is yellow.The second lumen ends near themotor above the level of the aorticvalve and is used to monitor aortic
pressure. The console uses thispressure measurement to calculatethe catheter’s position. The proxi-mal port of this lumen is red.
If the Impella remains in placefor continued support after the PCI,the tubing system is changed to 2separate systems. For continueduse, the purge fluid is heparinized(50 units heparin per milliliter offluid) and infused via an integratedinfusion pump, the Braun Vistainfusion pump (Figure 5). The typi-cal infusion rate for the purge fluidis 7 to 20 mL/h.
The second lumen of the Impella2.5 is flushed with heparinizedsaline (500 mL normal saline with1000 units heparin) by using regular(not infusion pump) intravenoustubing. The heparinized saline isplaced in a pressure bag that isinflated to 300 mm Hg. Other
e3 CriticalCareNurse OnlineNOW www.ccnonline.org
Table 1 Comparing traditional intra-aortic balloon therapy with Impella 2.5 percutaneous ventricular assist device
Feature
Duration of use
How does it work?
Physiological impact
Contraindications
Cost
Potential complications
Impella 2.5
Approved by the Food and Drug Administration for use upto 6 hours; approved in Europe for up to 5 days
Increases cardiac output more than an intra-aortic balloonpump does
Works independently of cardiac rhythm or arterial pressureNo timing required because it is continuous flow
Increases forward flowUnloads left ventricleAugments cardiac outputIncreases mean arterial pressure
Mechanical aortic valveModerate to severe aortic diseeaseLeft ventricular thrombusModerate to severe peripheral arterial disease
$20 000-$25 000 for cost of device and associated supplies;console provided with catheter purchase
Limb ischemiaBleeding, hematoma at access siteVascular injuryHemolysisEmbolization of thrombus or plaqueInfectionDevice failure
Intra-aortic balloon therapy6,7
Short-term use: hours to days
Blood volume displacementRequires cardiac rhythm or arterialpressure for trigger
Requires intermittent timing to ensureoptimal inflation and deflation of balloon
Decreases afterloadAugments cardiac output modestlyModerate to severe aortic insufficiencyAbdominal or aortic aneurysm
Moderate to severe peripheral arterialdisease
$800-$1200 for cost of device andassociated supplies plus cost of console
Limb ischemiaBleeding, hematoma at access siteVascular injuryEmbolization of thrombus or plaqueInfectionBalloon rupture
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

components of the Impella 2.5catheter include the cable that con-nects the catheter to the console anda repositioning sheath for bedsiderepositioning of the Impella 2.5.
The components required torun the device are assembled on a
rolling cart (Figure 6) and includethe power source, the Braun Vistainfusion pump, and the Impellaconsole (Figure 7). The Impella con-sole powers the microaxial bloodpump and monitors the functioningof the device, including the purge
pressure and several other parame-ters. The console has 10 functionkeys, but not all of the function keysare used for the Impella 2.5. Somewere designed to support future ver-sions of Impella catheters. Functionkeys that are used with the Impella
www.ccnonline.org CriticalCareNurse OnlineNOW e4
Table 2 Review of the research
Study, year
Henriques et al,9 2006
Remmelink et al,6 2007
Seyfarth et al,5 2008ISAR–SHOCK,sponsored by Abiomed
Burzotta et al,11 2008
Ferreiro et al,12 2009
Findings
Successful placement achieved in all patientsNo major complications related to the Impelladeveloped in any patients
Bleeding developed in 1 patient who required ablood transfusion
2 patients died of causes not related to the Impella
Aortic and coronary pressures increased withImpella support (P = .001)
Primary end point of hemodynamic improvement(defined as improved cardiac index at 30 minutesafter implantation) was achieved in 25 patients
Mean arterial pressure increased more in patientswith Impella than in patients with the IABP, but thedifference was not significant (P = .09)
Improvement in cardiac index significantly greater inImpella patients (P = .02)
Diastolic pressure increased significantly more withImpella support than with IABP (P = .002)
Use of inotropic agents and vasopressors wassimilar in both groups of patients
Serum level of lactate was lower in patients treatedwith Impella
Hemolysis measured by plasma free hemoglobinwas higher in patients treated with Impella (P <.05)
More blood products were administered to patientstreated with Impella
Left ventricular ejection fraction at 6 month follow-up increased significantly (P = .02)
No access site complicationsNo blood products required
PCI was successfully performed in all patients:• 88.5% remained hemodynamically stable duringprocedure
• 3 patients had severe hypotension developbecause of no-reflow
• 1 patient died of intracranial hemorrhage 8 hoursafter the Impella was removed
• 3 patients had limb ischemia develop; 1 requiredsurgical intervention
• 1 patient had hemolysis develop that requiredblood transfusion
Purpose
To evaluate safety and fea-sibility of using Impellaafter percutaneous coro-nary intervention (PCI) inpatients with ST-elevationmyocardial infarction
Evaluate effects of leftventricular unloading bythe Impella 2.5 on coro-nary hemodynamics
Evaluate safety and effi-cacy of Impella 2.5compared with intra-aortic balloon pump(IABP) in cardiogenicshock after acutemyocardial infarction
To evaluate feasibility andlong-term safety ofImpella-assisted high-risk PCI
To evaluate the use andsafety of the Impella 2.5in elective high-risk PCI
Sample size
19 consecutivepatients undergoinghigh-risk PCI
11 consecutive patientswho underwent elec-tive high-risk PCI
26 patients with car-diogenic shock afteracute myocardialinfarction; random-ized to IABP (n = 13)or Impella (n = 12)
One patient died beforeimplantation
10 consecutivepatients undergoingelective high-risk PCI
All patients had ejec-tion fraction ≤30%and multivessel orleft main coronarydisease
26 of 30 consecutivepatients who under-went high-risk PCI;3 patients excludedbecause of cardio-genic shock; 1excluded because ofdevice malfunction
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

2.5 include the P-PERF, MENU,SIGNAL, SCALE, and the ON keys.The console can run on a fullycharged battery for up to 1 hour.
Placement of the DeviceThe Impella 2.5 catheter is placed
percutaneously through the com-mon femoral artery and advanced
retrograde tothe left ventricleover a guidewire.Fluoroscopicguidance in thecatheterizationlaboratory oroperating roomis required. Afterthe device isproperly posi-tioned, it is acti-vated and bloodis rapidly with-drawn by themicroaxial bloodpump from theinlet valve in theleft ventricle and
moved to the aorta via the outletarea, which sits above the aorticvalve in the aorta (Figure 8).
If the patient tolerates the PCIprocedure and hemodynamic insta-bility does not develop, the Impella2.5 may be removed at the end ofthe case while the patient is still inthe catheterization laboratory. TheImpella device can be withdrawn,leaving the arterial sheath in place.The sheath can then be removedlater when the patient’s activatedclotting time or partial thrombo-plastin time has returned to nearnormal levels. For patients whobecome hemodynamically unstableor who have complications duringthe PCI (eg, no reflow, hypotension,or lethal arrhythmias), the devicecan remain in place for continuedpartial circulatory support, and thepatient is transported to the criticalcare setting.
ContraindicationsThe Impella 2.5 cannot be used
on all acutely ill patients who requirehemodynamic support.14 Becausethe device is designed to sit acrossthe aortic valve in the left ventricle,it should not be used in patientswho have prosthetic aortic valves,so as to prevent damage to the valve.It should not be used in patientswith moderate to severe aorticinsufficiency; it may worsen thedegree of insufficiency because theaortic valve cannot close completelywith the device in place. The Impellashould not be used in patients witha heavily calcified aortic valve. Thedevice may cause calcium to breakoff of the aortic valve and embolize,causing stroke. It cannot be used inpatients with documented left ven-tricular thrombus. The impellar
e5 CriticalCareNurse OnlineNOW www.ccnonline.org
Figure 2 Components of the Impella 2.5 cardiac assist device.Image courtesy ABIOMED Inc, Danvers, Massachusetts.
Infusion filter
Pigtail tip
Inlet area
Outlet area
Blood pump
Hemostasis sheath
Valve topurge fluid
Placement markingson the catheter shaft
Pressurereservoir
Plug to console
Red pressure sideportSideport tohemostasis sheath
Repositioning unit
Figure 3 Blood pump used in theImpella 2.5.Image courtesy ABIOMED Inc, Danvers, Massa-chusetts.
Figure 4 Detailed view of distal end of Impella 2.5.Image courtesy ABIOMED Inc, Danvers, Massachusetts.
Inlet area
Microaxial blood pump
Open pressure area
Outlet area
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

blades of themotor couldbreak up thethrombi, caus-ing arterialembolization.The device alsocannot be usedin patients withsevere peripheralarterial diseasebecause of thelarge sheath sizerequired for itsplacement, norcan it be used inpatients whocannot tolerateanticoagulationwith heparin.
Potential Complications ofImpella Therapy
The most commonly reportedcomplications of Impella 2.5 place-ment and sup-port includelimb ischemia,vascular injury,and bleedingrequiring bloodtransfusion.6,9
Hemolysis hasbeen reported.5,10
Other potentialcomplicationsinclude aorticvalve damage,displacement ofthe distal tip ofthe device intothe aorta, infec-tion, and sepsis.Device failure,although notoften reported,can occur.
Potential complications of use of theImpella 2.5 are detailed in Table 3.
Nursing Care of PatientsWith an Impella 2.5 forCirculatory Support
The nursing care of patientsremaining on Impella 2.5 supportrequires astute assessment andexpert nursing care (Table 4). Fre-quent hemodynamic evaluation isneeded. The use of continuous car-diac output monitoring may beuseful for patients with cardiogenicshock. Inotropic agents, such asdobutamine and milrinone, andvasopressors, such as dopamine andnorepinephrine, may still be neededafter the Impella 2.5 is placed tomaintain a cardiac index of at least2 and systolic blood pressure at 90mm Hg or higher. Some patients onImpella support may be intubatedand receiving mechanical ventilation.Implementation of the ventilator
www.ccnonline.org CriticalCareNurse OnlineNOW e6
Figure 5 Braun Vista infusion pump.Image courtesy ABIOMED Inc, Danvers, Massachusetts.
Figure 6 Rolling cart carrying compo-nents required to run the Impella 2.5.Image courtesy ABIOMED Inc, Danvers, Massa-chusetts.
Figure 7 Console of the Impella 2.5.Image courtesy ABIOMED Inc, Danvers, Massachusetts.
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

bundle is required for these patients,including elevation of the head ofthe bed to decrease the risk ofventilator-associated pneumonia, aswell as deep venous thrombosis andpeptic ulcer prophylaxis. Regularrepositioning of patients and assess-ment of their skin are necessary toprevent skin breakdown.
The patient with an Impella 2.5is at risk of limb ischemia because ofthe large size of the device. The arte-rial access site must be assessed reg-ularly for bleeding and developmentof a hematoma. Distal pulses of theaffected leg should be assessed at leasthourly. The use of anticoagulation isrequired, and bleeding may developin some patients. The partial throm-boplastin time should be monitoredevery 4 to 8 hours and maintainedat about 45 to 55 seconds, unless ahigher partial thromboplastin timeis required for some other reason.
Hemolysis can occur in patientswho are on the Impella 2.5. Hemolysis
can be mechani-cally inducedwhen red bloodcells are dam-aged as theypass through themicroaxialpump. Whenhemolysis occurs,hemoglobin leveland hematocritdecrease, hapto-globin leveldecreases, andplasma levels offree hemoglobinincrease. If thehemolysis issevere, hemoglo-binuria will beseen; if the
hemolysis is sustained, acute kidneyinjury will occur.
Patients on Impella 2.5 supportwho may require interrogation of apermanent pacemaker or implantablecardioverter defibrillator present aninteresting situation. In order forthe interrogator to connect with thepermanent pacemaker or implantablecardioverter defibrillator, the Impellaconsole must be turned off for a fewseconds while the signal is estab-lished. As soon as the signal hasbeen established, Impella supportis immediately restarted.
Impella 2.5 ConsoleManagement
The recommended maximumperformance level for continuoususe is P8. At P8, the flow rate is 1.9to 2.6 L/min and the motor is turn-ing at 50000 revolutions per minute.When activated, the console is silent.No sound other than alarms is audi-ble during Impella support, unlike
the sound heard with an IABP. Tendifferent performance levels rang-ing from P0 to P9 are available(Table 5). The performance leveldetermines the flow rate and thenumber of revolutions per minute.As the performance level increases,the flow rate and number of revolu-tions per minute increase. At maxi-mum performance (P9), the pumprotates at 50000 revolutions perminute and delivers a flow rate of2.1 to 2.6 L/min. P9 can be activatedonly for 5-minute intervals whenthe Impella 2.5 is in use.
Several parameters require regu-lar monitoring for the duration oftherapy. Regular documentation isessential, and review of trends isuseful when troubleshooting. Param-eters to assess regularly includeplacement signal, placement moni-toring (pump position), dual signal,purge pressure, motor current, andspeed (Table 6).
AlarmsSeveral console alarms may
require nursing intervention(Table 7). The most common includesuction, low purge pressure, andhigh purge pressure alarms. Infor-mation about the alarm can be seenon the console screen. An audiblealarm also will sound. Suctionalarms can occur if the performancelevel is too high for the patient; forexample, in a patient who is hypov-olemic or if the device is emptyingthe ventricle. A low purge pressurealarm indicates that the purge pres-sure to the Impella motor hasdecreased below 300 mm Hg. A lowpurge pressure can allow blood toenter the motor and damage themotor, rendering the device inoper-able. Low purge pressures require
e7 CriticalCareNurse OnlineNOW www.ccnonline.org
Figure 8 Fluoroscopic image of Impella 2.5 in place in the aorta.Image courtesy ABIOMED Inc, Danvers, Massachusetts.
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

immediate intervention by a criticalcare nurse. A high purge pressurealarm indicates that the purge pres-sure is greater than 700 mm Hg andgenerally indicates a kink in thetubing or catheter.
If the device advances too far andboth the inflow and outflow areas arefully in the left ventricle, the pumpposition wrong alarm will occur. Onthe placement signal screen, the wave-form will show a ventricular, ratherthan an aortic, pressure waveform.
The motor current signal will be flat-tened. The placement monitoring dia-gram will show the aortic valvesymbols distal to the pump (Figure 9).The performance level should bedecreased to P2 and the physicianshould be notified to reposition thedevice by pulling it back slightly toobtain an aortic waveform. Reposi-tioning is best performed under fluo-roscopic guidance, whenever possible.
If the Impella 2.5 is completelyin the aorta, or if the inlet and outlet
areas are in the ventricle and the pres-sure port is in the aorta, the pumpposition alarm will sound. The place-ment signal will show a normalappearing aortic waveform withsystolic and diastolic pressures sim-ilar to those shown by the patient’sarterial catheter. The motor currentwill be flattened. The placementmonitoring diagram will continu-ously scroll through 3 differentimages because it is not able to dif-ferentiate the position of the catheter.
www.ccnonline.org CriticalCareNurse OnlineNOW e8
Table 3 Potential complications of Impella 2.5 support
Complication
Bleeding, vascular injury,ischemia of affectedextremity
Hemolysis
Device migration
Infection, sepsis
Aortic valve damage (rare)
Device failure (rare)
How it could develop
Lack of hemostasis atarterial access site
Large sheath (13F) canobstruct/impede flow toaffected extremity
Direct arterial damage canoccur during deviceplacement
Rupture of red blood cellsby impellar blades/highflow causing hemoglobinto leak into plasma
Catheter may inadvertentlyadvance or be withdrawnwith excessive move-ment, turning
Placement of Impella andother invasive monitoringcatheters
Trauma during deviceplacement
Defective device
How to recognize
Loss of pulses in affectedfoot/leg
Pain, pallor, coolness,paresthesia, and/or paral-ysis of affected foot/leg
Decreased hemoglobin andhematocrit
Laboratory specimens arehemolysed
Urine is red, burgundy,brown because of redblood cells in the urine
Decreased haptoglobin lev-els, elevated plasma lev-els of free hemoglobin
Positioning alarmsChanges in placementsignal parameters
Inflammation, tenderness,or purulent drainage ataccess site
Increased body temperature
Continued heart failure dueto aortic valve damage
Echocardiographic evidenceof aortic insufficiency
Loss of pump function,console alarms
Deterioration in patient’scondition
How to prevent/manage
Assess and monitor pulses, skin color,temperature, and capillary refill hourly
Notify physician of changes to the affectedextremity
Monitor results of laboratory testsAdminister blood and blood products asordered
Hemolysis is most pronounced whenImpella is not positioned well; notifyphysician of hemolysis
Anticipate echocardiography to assessrepositioning of Impella
Decrease flow levels on Impella when possible
Maintain elevation of head of bed at ≤30°After placement, note position markings oncatheter shaft and document for referenceeach shift
Secure device with tape; secure tubings tolower leg
Aseptic technique during placementSterile dressing changeDaily tubing changeMonitor patient for fever, elevated whiteblood cell count
Monitor placement signal hourlyNotify physician of Impella position alarms
Monitor and document console parametershourly
Respond promptly to console alarms andtrouble-shoot as indicated
Notify Impella coordinator and physician ofongoing alarms
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

e9 CriticalCareNurse OnlineNOW www.ccnonline.org
Table 4 Nursing care of patients with an Impella 2.5
Problem
Decreased cardiac outputrelated to decreased cardiaccontractility
Potential for bleeding relatedto device placement andanticoagulation
Potential for limb ischemiadue to device placement
Potential for hemolysisrelated to device placement
Potential for infection relatedto device placement
Potential for device malfunc-tion/device failure
Potential for discomfort relatedto pain, anxiety, bed rest
Knowledge deficit
Expected outcomes/goals
With the Impella in place, thepatient will• be hemodynamically stable,as evidenced by systolicblood pressure >90 mm Hg,heart rate >50/min and<100/min, cardiac indexa ≥2
• have warm and dry skin• maintain urine output >30 mL/h• be alert and oriented• be free of hemodynamicallycompromising arrhythmias
The patient will:• be free of bleeding/hematomaat the arterial access site
• have a partial thromboplastintime (PTT) between 45 and55 seconds
• maintain baseline hemoglo-bin, hematocrit, and plateletlevels
Patient will• maintain baseline circulationto affected extremity
Patient will• maintain integrity of redblood cells
• maintain urine free of redblood cells
Patient will• remain free of signs andsymptoms of infection
Patient will• be free of device failure
Patient will• be comfortable• report decreased anxiety
Patient/patient’s family will• verbalize understanding ofplan of care and need fordevice
Nursing intervention and rationale
Continuous cardiac monitoringMeasure vital signs and pulmonary artery pressures hourly; notifyphysician of changes
Determine cardiac output/cardiac index every 4 hours and withchanges in vasoactive medications; notify physician of changes
Administer and titrate vasoactive medications as orderedMonitor urine output hourly and notify physician if <30 mL/hEvaluate for changes in mental status, including confusion, rest-lessness, and decreased responsiveness
If patient requires cardiopulmonary resuscitation, decreaseImpella performance level to P2 for duration of chest compres-sions; after chest compressions, obtain chest radiograph orechocardiogram to assess placement of the Impella
Assess the arterial access site for bleeding/hematoma hourlyAdjust heparin infusion as needed to maintain PTT parameters;measure PTT every 6-8 hours while on Impella support
Notify physician of PTT outside of goal range and titrate heparininfusion as needed
Assess laboratory results, including hemoglobin level, hemat-ocrit, and platelet count
Notify physician of decreases in hemoglobin level, hematocrit, orplatelet count
Monitor presence and quality of distal pulses in the affectedextremity hourly
Assess sensation and movement of affected extremityNotify physician of loss of pulses, pallor, pain in leg/foot, loss ofsensation/movement
Monitor laboratory samples for presence of hemolysisMonitor plasma levels of free hemoglobin and haptoglobinMonitor urine for changes in color, as hemolysis breaks downred blood cells, urine becomes red to brown
Administer blood and blood products as ordered
Change sterile dressing daily by using strict aseptic technique;change more frequently if any drainage is present
Remove monitoring catheters as possibleEnsure adequate nutrition to promote healingNotify physician of elevated body temperature and other signs ofinfections, such as redness, tenderness, warmth at the site,purulent drainage, elevated white blood cell count
Elevate head of bed ≤30°, turn patient carefully to prevent inad-vertent pulling on the Impella catheter shaft and/or tubing
Assess and document exposed number of centimeter markingson the catheter shaft once each shift
Assess and troubleshoot positioning alarms (outlined in Table 7)Notify physician of suspected suboptimal positioning of device ordevice failure immediately
Administer analgesics as ordered for discomfortReposition patient for comfort as needed
Explain the need for the Impella device in assisting the heartHelp the patient and the patient’s family understand the need forbed rest, careful repositioning, frequent assessment, and dailytubing and dressing changes
a Calculated as cardiac output in liters per minute divided by body surface area in square meters.
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

The performance level should bereduced to P2 and the physicianshould be notified of the need toreposition the Impella.
If the patient’s ventricular func-tion is very poor, a positioning alarmcan occur. The alarm will read “pumpposition unknown due to low pul-satility.” The Impella console is notable to determine the pump posi-tion because the patient’s systolicand diastolic pressures are not verydifferent. The placement signal willshow depressed cardiac function,evidenced by a damped appearingwaveform. The motor current willbe flattened. The aortic valve symbolswill not be seen on the placementmonitoring diagram.
WeaningWeaning from the partial circula-
tory support provided by the Impella2.5 can be approached in differentways. When the device has been inonly for support during high-risk PCIand the patient’s condition is stableafter the procedure is completed,
rapid weaningcan be done.For rapid wean-ing, the per-formance levelis decreased by1 or 2 levelsevery 5 to 15minutes untilthe pump isset at P2. Thepatient’s hemo-dynamic statusis assessed afterevery decreasein performancelevel. P2 is thelowest perform-ance level that
can be used while the distal end ofthe Impella 2.5 is in the left ventri-cle. At the end of rapid weaning,the Impella device can then beremoved as described in the nextsection.
Patients who have had the devicein longer or who were in unstablecondition during the proceduremay benefit from a slower weaningprocess. Slow weaning is accom-plished by decreasing the perform-ance level by 1 or 2 levels every 2 or3 hours. If the patient tolerates thisslow weaning by remaining hemo-dynamically stable while at P2, thedevice is then removed.
In our facility, we often usetransthoracic echocardiography toaid in the assessment of our patients.With the physician at the bedside,transthoracic echocardiography isperformed and the pump’s perform-ance level is decreased. The physi-cian can evaluate left ventricularsize and function and can quicklyassess how well the patient toleratesdecreases in the performance level.
Device RemovalWhen the physician is ready to
discontinue the Impella 2.5 catheter,the groin dressing should beremoved, the site cleansed withchloroprep, and the sutures clipped.Immediately before removal of thedevice, decrease the performancelevel to P0. The catheter is thenpulled back from the left ventricleinto the ascending aorta and thencompletely withdrawn. The arterialsheath can be left in place to beremoved separately, or the catheterand the sheath can be removed as aunit, as is common when removingan intra-aortic balloon catheterplaced through a sheath.
The Impella 2.5 instructions foruse recommend a 40-minute man-ual hold to achieve hemostasis atthe arterial access site. We followour hospital’s protocol for achiev-ing hemostasis, using either manualor mechanical compression. Somefacilities may use what is referredto as a preclose method while thepatient is still in the catheterizationlaboratory; that technique uses 28F Perclose suture-mediated closuredevices (Abbott Laboratories,Abbott Park, Illinois). The Impella2.5 can also be removed in the sur-gical setting with direct visualiza-tion of the common femoral artery.A cutdown is performed, and thedevice is removed by the surgeon.Arterial repair is done at that time,and the incision is covered with asterile dressing.
Our ExperienceTo date, we have placed an
Impella 2.5 in about 40 patients.Our facility has a high-volumeinterventional cardiology programas well as a busy adult and pediatric
www.ccnonline.org CriticalCareNurse OnlineNOW e10
Table 5 Impella 2.5 performance level and flow rate
Performance level
P0
P1
P2
P3
P4
P5
P6
P7
P8a
P9b
Flow rate, L/min
0.0
0.0-0.5
0.4-1.0
0.7-1.3
0.9-1.5
1.2-1.8
1.4-2.0
1.6-2.2
1.9-2.5
2.1-2.6
Revolutions per minute
0
25 000
35 000
37 000
40 000
43 000
45 000
47 000
50 000
51 000
a Level P8 is recommended maximum performance for continuous use.b P9 is used for verification of catheter position only—can also be used to pro-vide maximum flow for up to 2 minutes (console will automatically default to P8after 5 minutes).
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

cardiovascular surgery service. Wehave extensive experience with theIABP and with surgically placedVADs, including the AbiomedAB5000, Thoratec CentriMag, XVE,and HeartMate II. Our use of theImpella 2.5 was our first experiencewith percutaneously placed partialcirculatory support devices. Wehave also placed the Impella 5.0 in
3 patients. We have gained muchknowledge since implementing ourImpella program in April 2008.Based on our experiences, we sharethe following recommendations.
1. Assign a point person whocan oversee and coordinate the pro-gram. In our facility, this role is filledby the interventional cardiologyclinical nurse specialist. All patients
with this device are observed bythis clinical nurse specialist duringtheir hospital stay. Additionally,patients are observed by the VADcoordinator.
2. Limit the physicians whocan place and manage the deviceand have them proctor one another.In our facility, physicians whocan place this device are thosewho have interventional cardiol-ogy and/or cardiac surgery privi-leges. All cases are also followedby the cardiac surgeon who over-sees our VAD program and a criti-cal care intensivist. We developedpreprinted orders for physiciansto use for patients remaining onsupport to ensure consistency incare (Table 8).
3. Train a core group of nursesand cardiovascular technologistsfrom the catheterization laboratoryfor initial setup of the console,catheter preparation, and assistingwith placement of the device. Con-sole and infusion pump setuprequires 2 to 3 minutes to complete.Our training for staff from thecatheterization laboratory consistedof a 3-hour session with didacticand hands-on training. Ongoingpractice is essential to develop andmaintain competency. The Impellacoordinator is present for implantsto assist the catheterization labora-tory staff as needed. The VAD coor-dinators also provide valuableassistance. We found it helpful forthe first few Impella placements tobe planned, elective placements forhigh-risk PCI. This arrangementallowed ample time for setting upthe console and infusion pumpbefore the Impella was placed.
4. Develop a nursing protocolthat outlines key strategies in patient
e11 CriticalCareNurse OnlineNOW www.ccnonline.org
Table 6 Console monitoring screens
Parameter What it means Screen display
Placement signal
This is a positioning aid. It evaluatesthe position of the device. The pressureis obtained from the pressure lumenthat ends near the motor. It should“see” an aortic waveform; however, ifthe device is too far in, a ventricularwaveform will be seen.
Motor current
Displays the amount of electrical cur-rent that is required to power the motorof the catheter device. The motor cur-rent increases as the flow increasesand decreases as the flow decreases.It should be a pulsatile waveform.
Purge pressureDisplays the current purge pressure.This pressure is measured in millime-ters mercury (mm Hg).
Speed Displays the rotations per minute ofthe impellar blades.
Flow
Displays the flow that is being aspi-rated from the left ventricle. This valuecan be found in the upper right cornerof all screens.
Placement monitoringThis graphic display shows aschematic of the pump position inrelationship to the aortic valve.
Dual signal
Displays 2 waveforms. The top wave-form is the motor current and the bot-tom waveform is the placement signal.This screen can be useful in advancedtroubleshooting.
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

management and a specific flowsheet (Figure 10) for documentation.
5. Train a core group of criticalcare nurses to care for the patient,monitor the device, change tubings,and troubleshoot alarms. We pro-vide 1-to-1 staffing for our patientswith an Impella 2.5 until they arehemodynamically stable. Our train-ing for our cardiac intensive careunit (CICU) nurses consisted of aseries of three 1-hour sessions,encompassing a review of pertinentphysiology and hemodynamics,Impella console management andtroubleshooting, and tubing changeswith hands-on practice and docu-mentation practice. Staff received1-to-1 mentoring from the Impellacoordinator. Review of patient care
www.ccnonline.org CriticalCareNurse OnlineNOW e12
Table 7 Impella 2.5 alarm troubleshooting
Alarm
Low purge pressure
High purge pressure
Suction likely
Pump position wrong
High motor current value
What to do
Correct the purge pressure quickly to prevent damage of themotor
Assess for leaks or loose connections in the purge system.Increase the purge pressure by delivering a bolus of 1 mL andincreasing the continuous rate on the Braun Vista Pump by 1 mL/h.
If maneuvers to increase the purge pressure to between 300 and700 mm Hg are not effective within 5 minutes, the Impella mayneed to be removed.
Look for kinks in the tubing or catheter.Decrease the flow rate of purge fluid by 1 mL/h on the BraunVista Pump. Do not decrease the flow rate to less than 4 mL/h.
May need to decrease the concentration of the purge fluid(eg, change from 20% dextrose to 10% dextrose).
If the alarm persists for more than 2 hours after the precedingsteps are taken, the device should be removed.
Reduce the performance level by 2 levels (for example, decreasefrom P8 to P6).
Assess hemodynamics and left ventricular filling; correct hypov-olemia if present.
Assess and support patient as indicated.Notify the physician/Impella coordinator.May assess placement by echocardiography/portable chestradiography.
Pump most likely needs to be repositioned by the physician.
If the motor current continues to increase, the catheter shouldbe removed.
What it means
Purge pressure is less than 300 mm Hg.With low purge pressure, blood canenter the motor and damage it.
Purge pressure is higher than700 mm Hg.
Tubing may be kinked.Concentration of purge fluid may betoo high.
The console has detected pump suction.The patient may be hypovolemic, andthe pump may be completely empty-ing the left ventricle.
Pump outlet is blocked—the pump istoo far in the ventricle and the outletmay be at the level of the aortic valve.
Reposition pump; wrong pump positionwas detected.
There are mechanical problems withthe pump. The motor current for theselected performance level has beenexceeded.
Figure 9 Placement monitoring screen display shows that pump position is wrong.Image courtesy ABIOMED Inc, Danvers, Massachusetts.
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

management strategies, consoletroubleshooting, and fluid/tubingsetup has also been added to ourannual VAD skills fair (Table 9).
6. Work with pharmacy and nurs-ing staff to develop a standardizedtime for fluid and tubing changes.We found performing such changesat a consistent time to be very help-ful. This arrangement ensured thatnew purge fluid was ready whenneeded and that the nurses hadmore staffing resources to assist withthe tubing change. The pharmacyprepares the heparinized 20% glucosepurge solution and sends it to theunit before our standard change timeof 3 PM daily. We have 2 nurses at thebedside for the tubing change. TheImpella coordinator is present toassist with tubing changes as neededby the nursing staff.
7. Include the cardiovascular sur-gery staff and perfusion staff in the
initial training. Patients with anImpella may go to the cardiovascularoperating room for bypass surgeryor valve repair/replacement. Coor-dination with the perfusionist isessential when patients are beingplaced on cardiopulmonary bypass.As the patient goes on cardiopul-monary bypass, the performance levelof the Impella must be decreased.When the patient is coming off ofcardiopulmonary bypass, the per-formance level of the Impella pump,if the pump remains in place, mustbe increased to provide adequateflow to the patient. In some facili-ties, the perfusionist manages boththe cardiopulmonary bypass andthe Impella. In our facility, we havea trained CICU nurse managing theImpella while the patient is in thecardiovascular operating room.
8. Partner with industry. Abiomedprovides strong clinical support as
well as excellent print and Web-basededucational materials. A consolesimulator is available that can be usedto practice troubleshooting. Abio-med also provides assistance withtroubleshooting via 24-hour-a-day,7-day-a-week telephone support.
SummaryThe Impella 2.5 device is an
alternative to an IABP that may bebeneficial in some patients whoneed hemodynamic support. It isuseful in patients undergoing high-risk PCIs. The Impella 2.5 shouldnot be used in patients with aorticvalve disease or known left ventric-ular thrombus. Potential complica-tions include bleeding, vascularinjury, hemolysis, infection, sepsis,and device malfunction or failure.Nursing care is directed towardsupport of critically ill patients,including frequent hemodynamicassessment, titration of vasoactivemedications as indicated, Impellaconsole troubleshooting, and moni-toring for potential complications.A multidisciplinary approach toestablishing a program for theImpella is useful in ensuring com-petency and good outcomes forpatients. The following 3 case stud-ies demonstrate the successful useof Impella 2.5 support during high-risk PCIs at our facility.
Case Study 1A 71-year-old man was referred
to our facility for saphenous veinbypass graft (SVG), a high-risk PCI.Diagnostic cardiac catheterizationand coronary angiography per-formed at the referring facilityshowed severe triple vessel coronarydisease and high-grade lesions in 2SVGs. He had a history of coronary
e13 CriticalCareNurse OnlineNOW www.ccnonline.org
Table 8 Physician orders for placement of Impella 2.5
Transfer to cardiac intensive care unit, continuous cardiac monitoring
See orders for after percutaneous coronary intervention for additional physician orders
Complete bed rest; may turn and reposition patient as needed; do not elevate head ofbed to >30°
Every hour and as needed: assess and document patient’s vital signs, access site,distal pulses, hemodynamic parameters, urine output, Impella performance level,flow, placement signal, motor current, pump position, and purge pressure
Perform the following diagnostic tests:On arrival in unit: complete blood cell count, renal panel, partial thromboplastin time,plasma free hemoglobin, portable chest radiograph, 12-lead electrocardiogram
Every 8 hours while on Impella support: partial thromboplastin timeIn morning: transthoracic echocardiography to assess placement of deviceDaily while on Impella support: plasma-free hemoglobin, complete blood cell count,renal panel
Notify Impella coordinator of changes in patient’s status or concerns regarding Impelladevice/Impella console
Notify physician if partial thromboplastin time <45 seconds; goal for partial thrombo-plastin time is 45-55 seconds
Daily at 3 PM:Change purge fluid/tubing system by using 500 mL dextrose 20% in water withheparin 25000 units
Change arterial fluid/tubing system, using 500 mL normal saline with heparin 1000 unitsSterile dressing change
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

artery bypass grafting surgery severalyears prior as well as heart failure.His estimated ejection fraction wasmarkedly decreased at 20% (normal,55%-70%) on a recent echocardio-gram. He was experiencing progres-sion of his anginal symptoms, andhis functional capacity was poor.He declined repeat bypass surgery.After careful evaluation and opti-mization of pharmacological ther-apy for heart failure, the decisionwas made to proceed with high-riskPCI of the SVG to the left anteriordescending (LAD) artery with anImpella 2.5 used to provide partialcirculatory support during the PCI.
The patient was brought to thecatheterization laboratory and pre-pared for the procedure. On arrival,his blood pressure was 151/88 mmHg with a heart rate of 66/min.Sheaths were placed in the rightfemoral vein, the right femoralartery, and the left femoral artery.An SvO2 pulmonary artery cathetershowed that the patient’s baselinepulmonary artery pressures weremarkedly elevated at 69/40-47 mmHg (normal: 20-30/8-12 mm Hg;mean, 25 mm Hg). Heparin 7000units was administered intravenouslyfor anticoagulation. When the acti-vated clotting time was higher than
250 seconds, the Impella 2.5 wasadvanced into position via the leftcommon femoral artery and placedacross the aortic valve into the leftventricle. The catheter device wasconnected to the Impella console andsupport was initiated. The perform-ance level was increased from P0 toa maximum of P8 in a matter of min-utes. At P8, the flow was 2.5 L/minand the patient’s cardiac index was2.58 (normal, 2.5-4).
The PCI procedure of the LADSVG was then started. The SVG wasaspirated before a distal protectiondevice was placed. One bare metalstent (not a drug eluting stent) was
www.ccnonline.org CriticalCareNurse OnlineNOW e14
Figure 10 Impella 2.5 flowsheet.Abbreviations: ABGs, arterial blood gas analysis; AC, alternating current; Batt, battery; P-perf, pump performance level; PRN, as needed; PTT, partial thromboplastintime; RN, registered nurse; RPM, revolutions per minute.
Image courtesy Sutter Medical Center, Sacramento, California.
Time:
Infusion Rate (mL)(4-12 mL)
Flow L/min:
P-Perf Level:
Placement Signal:
Pump Position:
Dual Signal:
Purge Pressure:(300-700-mmHg)
Motor Current:
Speed RPM:
Power (AC / Batt):
Groin Check (✓)
Pulse Check (✓)
Initials
RN SIGNATUREDocument hourly and PRN
Every 8 hour labs: creatinie, ABGs with ionized calcium, PTTNotify physician if PTT < 45 seconds
Pump Serial Number:Access Site: Right / Left Femoral Artery# of exposed Hash Marks:Last sterile dressing change:Last tubing change:Use back of flow sheet for additional Impelladocumentation id needed
21781 (5/13/09)
PatientIdentification
FLOWSHEET
Date: ___________________________ ABIOMED 1-800-422-8666
Ventricular Assist DeviceFlowsheet for Impella 2.5
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

placed in the SVG to the LAD. Dur-ing this time, transient no-reflowdeveloped. No reflow is a phenome-non in PCI that can cause severehemodynamic compromise becausemyocardial perfusion through agiven segment of the coronary circu-lation is inadequate, yet no angio-graphic evidence of mechanicalobstruction of the vessel is apparent.15
The patient’s pulmonary artery pres-sures increased to 93/40-58 mm Hgand the cardiac index decreased to2.2. Despite the no-reflow, the arte-rial pressure, heart rate, and cardiacrhythm remained stable, and thepatient had no complaints of short-ness of breath or chest discomfort.Adequate blood flow was reestab-lished after the intracoronary admin-istration of 500 µg nitroglycerin.Because the patient was toleratingthe procedure well after this, thephysician decided to stent the seconddiseased SVG. With the Impella con-tinuing at maximum flow of 2.5 L,2 bare metal stents were deployed
in the SVG to the posterior lateralbranch. Pulmonary artery pressuresremained elevated after this stentwas placed, and the patient wasgiven furosemide and nitroglycerinto decrease preload and increasediuresis. Just before the patient’sreturn to the CICU, the pulmonaryartery pressure decreased to 70/41-48 mm Hg and the cardiac indexwas 2.69.
The patient was weaned fromthe Impella device, the device wasremoved in the catheterization labo-ratory, and the venous and arterialsheaths were secured in place. Thetotal duration of Impella supportwas slightly less than 2 hours. Thepatient was transferred to the CICUfor continued monitoring. Four hourslater, after the activated clotting timewas less than 150 seconds, the venousand arterial sheaths were removedand hemostasis was achieved after40 minutes of manual compression.
The patient’s remaining hospitalcourse was uneventful and he was
discharged 2 days later takingappropriate medications for afterPCI and to treat heart failure. Sixweeks later, the patient was painfree with no complaints of dyspnea.Transthoracic echocardiographyshowed increased contractility, andthe ejection fraction was 40%. Atfollow-up 12 months later, the patientremained symptom-free with a nor-mal ejection fraction of 55%.
Case Study 2A 74-year-old man was trans-
ferred to our facility after sustain-ing a non–ST-segment elevationmyocardial infarction. He had along history of diabetes and hadundergone coronary artery bypasssurgery 20 years prior. Diagnosticcardiac catheterization showedsevere triple vessel disease as wellas severe diffuse distal disease of hisleft internal mammary artery(LIMA) graft, his only remainingpatent graft. He had severe mitralregurgitation. His ventricular func-tion was poor with a calculatedejection fraction of 20%. His leftventricular end-diastolic pressurewas markedly elevated at 40 mm Hg(normal, 5-12 mm Hg), and his car-diac index was reduced at 1.98. Hewas evaluated by our cardiothoracicsurgery team and was deemed anextremely poor candidate for sur-gery. After a family conference thatincluded the patient, the decisionwas made to proceed with high-riskPCI of the LIMA graft, using theImpella 2.5 for hemodynamic sup-port during the procedure.
He returned to the catheterizationlaboratory the next day for coro-nary intervention. On arrival, hisblood pressure was 105/66 mm Hgwith a heart rate of 64/min. Sheaths
e15 CriticalCareNurse OnlineNOW www.ccnonline.org
Table 9 Impella competency checklist for nurses in the cardiac intensive careunit: critical elements for managing patients with an Impella 2.5
Lists resources for assistance (trained peers, clinical nurse specialists, ventricular assistdevice coordinators, ABIOMED toll-free phone line, reference binder on Impella cart)
Demonstrates use of Impella console:Verifies placement signalChanges performance level/pump speedVerifies purge pressure
Demonstrates troubleshooting of Impella components:Power supplyCommon alarms (low and high purge pressure, suction)Braun Vista infusion pump
Changes arterial flush fluid and tubing per checklist
Changes purge fluid and tubing per checklist
Describes required patient careAssessment/reassessment of findings, including hemodynamic profilePerforms sterile dressing changeStates potential complications and how to assess/prevent themReviews orders, communicates changes to cardiology/cardiothoracic surgeonIf cardiopulmonary resuscitation needed, decrease performance level to P2, andinitiate Advanced Cardiac Life Support protocols
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

were placed in the right femoralvein, the right femoral artery, andthe left femoral artery. Heparin9000 units was administered intra-venously for anticoagulation, andthe Impella 2.5 was advanced intoposition in the left femoral artery.Support was established at P8. Thecoronary guidewire was advancedthrough the LIMA graft to the dis-tal LAD. Three sequential stentswere placed in the area of disease.The patient’s vital signs and cardiacrhythm remained stable throughoutthe procedure. The patient was rap-idly weaned from the Impella, whichwas removed in the catheterizationlaboratory. The 13F arterial sheathwas sutured in placed for removal4 hours later after the patient wasreturned to the CICU. He was dis-charged home 2 days later.
Case Study 3A 63-year-old woman was
admitted to our facility with anacute anteroseptal myocardialinfarction. She was treated withfibrinolytic therapy but continuedto have chest pain. She had a his-tory of hypertension complicatedby end-stage renal disease and wasreceiving dialysis treatments 3times per week. She was taken tothe catheterization laboratory,where she was found to have a sig-nificant obstruction of the left maincoronary artery complicated byplaque rupture. She was evaluatedby our cardiac surgery team, whothought that she was a very high-risk candidate for surgery based onthe recent fibrinolytic therapy, herrenal failure, and the remote his-tory of stroke. She was transferredto the CICU and supportive med-ical therapy was initiated.
She returned to the catheteriza-tion laboratory 3 days later for high-risk PCI of the left main coronaryartery. On arrival, her blood pres-sure was 127/72 mm Hg, and herheart rate was 54/min. Sheathswere placed in the right femoralvein, the right femoral artery, andthe left femoral artery. Bivalirudinwas administered for anticoagula-tion, and the Impella 2.5 wasadvanced into position in the leftfemoral artery. Support was estab-lished at P8.
The left main lesion was crossed,and one stent was deployed at thelesion. During stent deployment,the patient had severe chest painand showed ST-segment elevationin the anterior leads. Despite thesechanges, her blood pressure andcardiac rhythm remained stable.Intravascular ultrasound was per-formed to confirm optimal stentplacement. At the end of the proce-dure, she was symptom free, andshe was rapidly weaned from theImpella and the device was removed.The 13F arterial sheath was suturedin placed for removal 2 hours later,after the patient had returned to theCICU. She had no further chest painduring her hospitalization and wasdischarged home in stable condi-tion 3 days later. CCN
Financial DisclosuresBrenda McCulloch is a member of the AbiomedAdministrative Advisory Board.
References1. Vegas A. Assisting the failing heart. Anesthe-
siol Clin. 2008;26:539-564.2. Sarkar K, Kini AS. Percutaneous left ven-
tricular support devices. Cardiol Clin.2010;28:169-184.
3. Lee MS, Makkar RR. Percutaneous left ven-tricular support devices. Cardiol Clin.2006;24(2):265-275.
4. Kale P, Fang JC. Devices in acute heart failure.Crit Care Med. 2008;36(suppl):S121-S128.
5. Seyfarth M, Sibbing D, Bauer I, et al. A ran-domized clinical trial to evaluate the safetyand efficacy of a percutaneous left ventricu-lar assist device versus intra-aortic balloonpumping for treatment of cardiogenic shockcaused by myocardial infarction. J Am CollCardiol. 2008;52:1584-1588.
6. Remmelink M, Sjauw KD, Henriques JP, etal. Effects of left ventricular unloading byImpella Recover LP 2.5 on coronary hemo-dynamics. Catheter Cardiovasc Interv. 2007;70(4):532-537.
7. Reid MB, Cottrell D. Nursing care of patientsreceiving intra-aortic balloon counterpulsa-tion. Crit Care Nurse. 2005;25(5):40-49.
8. Weber DM, Raess DH, Henriques JPS, Siess T.Principles of Impella cardiac support. http://bmctoday.net/citoday/2009/09/supplement/article.asp?f=0909_supp_01.php.Accessed November 16, 2010.
9. Henriques JPS, Remmelink M, Baan J, et al.Safety and feasibility of elective high-riskpercutaneous coronary intervention proce-dures with left ventricular support of theImpella Recover LP 2.5. Am J Cardiol. 2006;97(7):990-992.
10. Dixon SR, Henriques JPS, Mauri L, et al. Aprospective feasibility trial investigating theuse of the Impella 2.5 system in patientsundergoing high-risk percutaneous coro-nary intervention (the PROTECT I trial):Initial U.S. experience. J Am Coll Cardiol.2009;2:91-96.
11. Burzotta F, Paloscia L, Trani C, et al. Feasi-bility and long-term safety of electiveImpella-assisted high-risk percutaneouscoronary intervention: a pilot two-centrestudy. J Cardiovasc Med. 2008;9:1004-1010.
12. Ferreiro JL, Gomez-Hospital JA, CequierAR, et al. Use of Impella Recover LP 2.5 inelective high risk percutaneous coronaryintervention [published online ahead ofprint September 2, 2009]. Int J Cardiol.doi:10.1016/j.ijcard.2009.08.003.
13. Stahl MA, Richards NM. Update on ventric-ular assist device technology. AACN Adv CritCare. 2009;20(1):26-34.
14. Impella: Instructions for Use for the Impella2.5 Circulatory Support System. Danvers, MA:Abiomed, Inc; 2007.
15. Eeckhout E, Kern MJ. The coronary no-reflowphenomenon: a review of mechanisms andtherapies. Eur Heart J. 2001;22:729-739.
www.ccnonline.org CriticalCareNurse OnlineNOW e16
Now that you’ve read the article, create or contributeto an online discussion about this topic using eLetters.Just visit www.ccnonline.org and click “Respond toThis Article” in either the full-text or PDF view ofthe article.
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from

Brenda McCullochUse of the Impella 2.5 in High-Risk Percutaneous Coronary Intervention
http://ccn.aacnjournals.org/Published online ©2011 American Association of Critical-Care Nurses
10.4037/ccn2011293 e1-e16 31 2011;Crit Care Nurse
http://ccn.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information:
http://ccn.aacnjournals.org/subscriptions/Subscription Information
http://ccn.aacnjournals.org/misc/ifora.xhtmlInformation for authors
http://www.editorialmanager.com/ccn Submit a manuscript
http://ccn.aacnjournals.org/subscriptions/etoc.xhtmlEmail alerts
362-2049. Copyright ©2016 by AACN. All rights reserved. bimonthly by AACN, 101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050, ext. 532. Fax: (949) Critical Care Nurse is an official peer-reviewed journal of the American Association of Critical-Care Nurses (AACN) published
by AACN on May 23, 2018http://ccn.aacnjournals.org/Downloaded from