Embed Size (px)
Citation preview
Feasibility of Low-volume Injectionsof Contrast Material with a Body
Weight–Adapted Iodine-DoseProtocol in 320-Detector Row
Coronary CT Angiography
Fuminari Tatsugami, MD, Mitsuru Matsuki, MD, Yuki Inada, MD, Shuji Kanazawa, MD, Go Nakai, MD,Yoshihiro Takeda, MD, Hideaki Morita, MD, Haruhiko Takada, RT, Kenji Ashida, RT,Shushi Yoshikawa, RT, Katsunori Fukumura, RT, Yoshifumi Narumi, MD
Ac
FrS.O86co
ªdo
Rationale and Objectives: To investigate the feasibility of low-volume injections of contrast material with a body weight-adapted iodine-
dose protocol in computed tomography coronary angiography (CTCA) using a 320-detector row scanner.
Materials and Methods: Ninety-eight patients who underwent CTCA in a single heartbeat with electrocardiogram-gating were divided
into two groups, receiving 0.8 mL/kg of contrast material injected at a fixed duration of 12 seconds (A; n = 48) or 0.7 mL/kg of contrast
material injected at a fixed duration of 10 seconds (B; n = 50); all patients then received 20 mL of saline. Contrast densities were assessedfor the ascending aorta, left ventricle, right coronary artery (RCA), and left main coronary artery (LMA).
Results: The mean flow rate was 4.00� 0.56 mL/second in group A and 4.06� 0.57 mL/second in group B (P = .51). There were no signif-
icant differences in the mean enhancement values of the ascending aorta, LMA and proximal RCA between the two groups. Also, there wasno significant difference between the mean enhancement values at the three different levels of the RCA (proximal, middle, and distal
segments) (group A; P = .27, group B; P = .07).
Conclusion: The use of 0.7 mL/kg of contrast material injected at a fixed duration of 10 seconds was feasible for CTCA using 320-detectorrow CT, with a sufficient and reliable contrast enhancement in the ascending aorta and coronary artery.
Key Words: Cardiac CT; CT coronary angiography; contrast material; injection method; 320-detector row CT.
ªAUR, 2010
Computed tomography coronary angiography
(CTCA) has become a standard in the noninvasive
assessment of coronary arteries in the past few years
(1–4). In CTCA, high and consistent vascular enhancement
is a prerequisite for sufficient evaluation (5–8). Recently, it
has been reported that a patient weight–adapted iodine-dose
protocol with fixed injection duration yielded significantly
better image quality than the fixed-dose protocol in
64-detector row CTCA (9). An injection volume of 1.0
mL/kg body weight of contrast material (370 mgI/mL) is
necessary to achieve a sufficient contrast enhancement, and
ad Radiol 2010; 17:207–211
om the Departments of Radiology (F.T., M.M., Y.I., S.K., G.N., H.T., K.A.,Y., K.F., Y.N.), Internal Medicine I (Y.T.), and Internal Medicine III (H.M.),saka Medical College, 2-7 Daigaku-machi, Takatsuki City, Osaka 569-86, Japan. Received May 7, 2009; accepted August 19, 2009. Addressrrespondence to: F.T. e-mail: [email protected]
AUR, 2010i:10.1016/j.acra.2009.09.010
injection duration of 15 seconds is recommended in 64-
detector row CTCA (9).
Very recently, 320-detector row CT scanner has been devel-
oped with a z-coverage value of 160 mm; thus, the entire heart
can be scanned in a single rotation and within a single heartbeat
with a minimum temporal resolution of 175 ms (10,11). The
data acquisition time for 320-detector row CTCA is less
than 3 seconds, which is quite short compared with
64-detector row CTCA at less than 10 seconds. Because this
shorter scan time permits a decrease in the contrast dose or
the injection duration at CTCA (8,9), contrast material proto-
cols must be adjusted and optimized as CT technology evolves.
To our knowledge, no study has evaluated the optimal dose
of contrast material on the basis of patient body weight for
a reliable vessel enhancement in 320-detector CTCA. The
purpose of this study is to compare contrast injection proto-
cols with different volume of contrast material and to investi-
gate the feasibility of low-volume injections of contrast
material with a body weight–adapted iodine-dose protocol
in 320-detector row CTCA.
207

TATSUGAMI ET AL Academic Radiology, Vol 17, No 2, February 2010
MATERIALS AND METHODS
Patients
Initially, 106 patients who were scheduled to undergo 320-
detector row CTCA were recruited in this study. Patients
who had previous allergic reaction to iodinated contrast mate-
rial, severe heart failure, valvular heart disease, or elevated serum
creatinine level (>1.5 mg/dL) were excluded, along with
women who were potentially pregnant. Patients were referred
because of suspected coronary artery disease (CAD) (n = 92)
based on the following symptoms such as dyspnea (n = 11), atyp-
ical chest pain (n = 48), pathological exercise test or electrocar-
diogram (n = 25), or high cardiovascular risk factors (n = 8).
Fourteen patients with known CAD were referred for stent
control. However, eight patients were excluded because of
severe calcification of the coronary arteries (n = 3) or manifest
arrhythmia (n = 5). The final study group consisted of 98
patients (57 men, 41 women) who were 37–84 years old
(mean, 69.0 � 9.3 years) with a body weight of 41–77 kg
(mean, 58.6 � 8.4 kg). This study was performed according
to the principles of the Declaration of Helsinki, and approved
by our institutional review board. Informed consent was
obtained from all patients before the CTexamination.
CT Scanning
CT was performed using a 320-detector row scanner (Aqui-
lion ONE, Toshiba Corporation Medical Systems, Tokyo,
Japan). Patients with a prescan heart rate of 65 beats per
minute (bpm) or higher were given 20–60 mg of metoprolol
(Selokeen; AstraZeneca, Zoetermeer, Netherlands) orally 1
hour before scanning. The scan parameters were a collimation
of 320 � 0.5 mm, a voltage of 120 kV, a tube current of 450–
580 mA, and a rotation time of 0.35 or 0.375 seconds. The
patient’s electrocardiogram was digitized and monitored
continuously during image acquisition.
The volume of contrast material was adapted to the patient’s
body weight. Patients were divided into two groups, receiving
0.8 mL/kg of nonionic contrast material (Iomeprol, Iomeron
350 mgI/mL; Eisai, Tokyo, Japan) injected at a fixed duration
of 12 seconds (group A; n = 48) or 0.7 mL/kg of contrast
material injected at a fixed duration of 10 seconds (group B;
n = 50). In both protocols, contrast administration was fol-
lowed by 20 mL of 0.9% saline solution injected at the same
flow rate as the contrast material. Using a dual shot injector
(Nemoto Kyorindo, Tokyo, Japan), the contrast material
and saline solution were injected through a 20-gauge intrave-
nous injection catheter (Termo, Tokyo, Japan) inserted into
the antecubital vein.
The scan delay was set with the use of automatic bolus-
tracking technology (Real Prep technique; Toshiba Corpora-
tion Medical Systems, Tokyo, Japan). As soon as the single
density level in the ascending aorta reached 150 Hounsfield
units, the patient was instructed to take a deep breath and
hold it. Five seconds after triggering, the contrast-enhanced
CT scan was performed. The phase window during which
208
the patient was exposed was limited to 70%–80% of the R-
R interval for all patients with a heart rate <60 bpm, to
65%–85% of the R-R interval for patients with a heart rate
60–65 bpm and to 30%–90% of the R-R interval for patients
with a heart rate >65 bpm. However, patients who required
visualization of the myocardial or valve motion throughout
the cardiac cycle were imaged with a dose modulation. The
effective radiation dose of CTCA was calculated as the
product of the dose-length product times a conversion coeffi-
cient for the chest (k = 0.017 mSv/mGy�cm) (12).
For evaluation of the coronary arteries, data was recon-
structed at 75% of the R-R interval with a slice thickness of
0.5 mm and a reconstruction interval of 0.25 mm. If motion
artifacts were still present in this phase, images were recon-
structed at each 2% interval around the 5% intervals with fewest
motion artifacts at the midlevel of the heart. The reconstructed
image data was transferred to a computer workstation (ZIO
Station System 610, Ziosoft, Tokyo, Japan) for postprocessing.
Methods of Evaluation
One observer (F.T., with 7 years of experience in cardiovas-
cular radiology) collected all the measurements using
a circular region of interest (ROI) cursor. First, four represen-
tative slice levels were selected in each patient; level 1 was the
origin of the left main trunk, level 2 the origin of the RCA,
level 3 the center of the left ventricle, and level 4 the hori-
zontal part of the distal RCA (9). Examples of selected slices
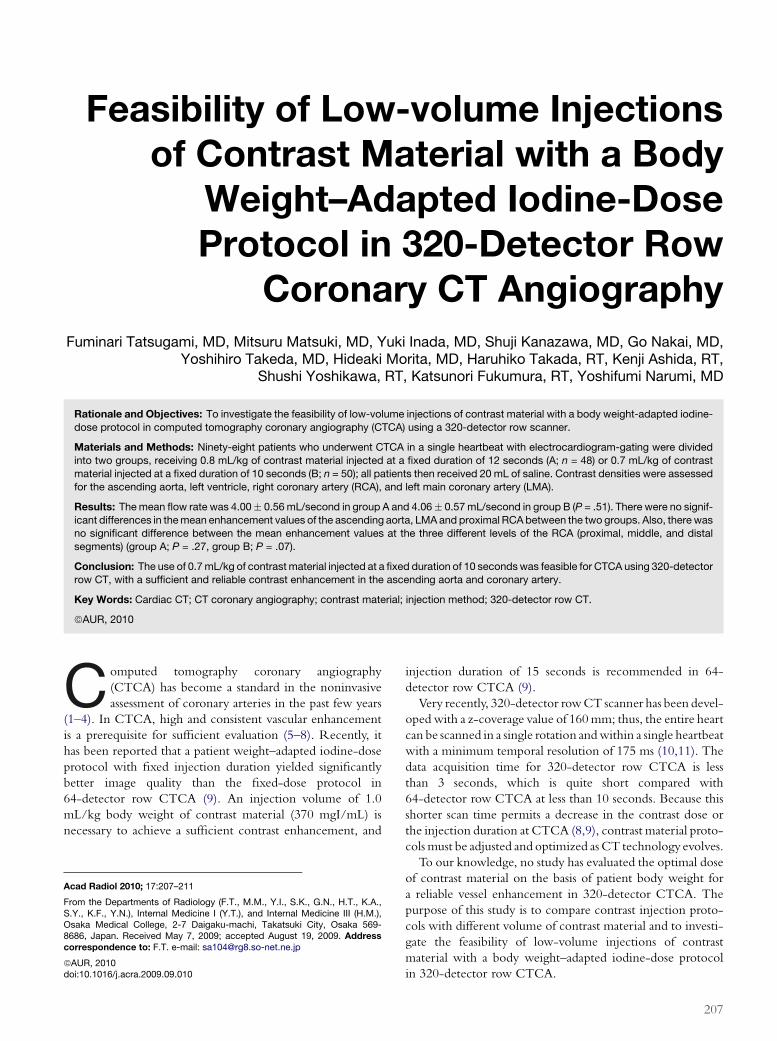
and ROIs are shown in Figure 1. Next, enhancement values
for the ascending aorta, pulmonary artery trunk and left main
coronary artery were measured at level 1 (Fig 1a), for the
proximal RCA at level 2 (Fig 1b), for the right and left
ventricle and the middle RCA at level 3 (Fig 1c), and for
the distal RCA at level 4 (Fig 1d) (9). ROIs for the coronary
arteries were plotted on a cross-sectional image at each slice
level (Fig 1). Calcifications, coronary artery stents, and soft
plaques were carefully excluded from the ROI measure-
ments.
Statistical Analyses
SPSS software (version 17.0, SPSS) was used for statistical
testing. Patients’ ages, body weights, the heart rate during
acquisition of CT scans, injection rate, and iodine delivery
rate were compared between the two groups with a one-
way analysis of variance. The quantitative results for the two
groups were compared using the Mann-Whitney U test.
The quantitative results for the three different levels of the
RCA were compared using the Kruskal-Wallis test. All data
were expressed as means � SD, and differences were consid-
ered to be statistically significant at P < .05.
RESULTS
CT was successfully performed without complications on all
98 patients, of whom 30 were smokers (31%), 23 had diabetes
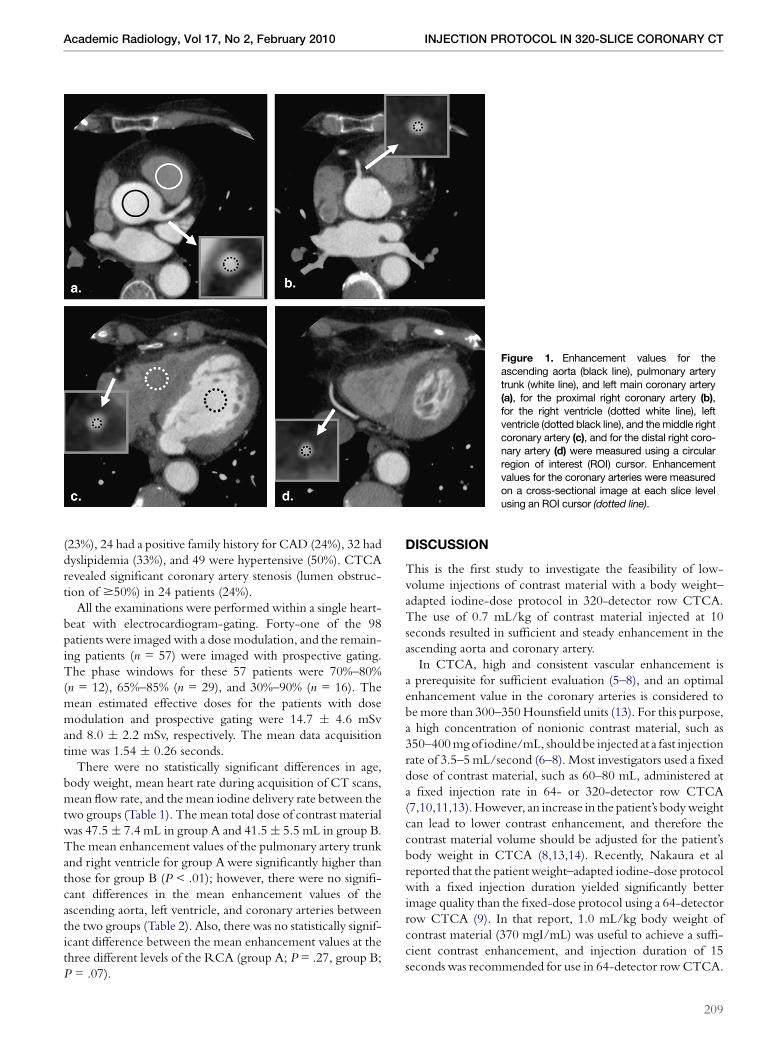
Figure 1. Enhancement values for the
ascending aorta (black line), pulmonary artery
trunk (white line), and left main coronary artery(a), for the proximal right coronary artery (b),for the right ventricle (dotted white line), left
ventricle (dotted black line), and the middle right
coronary artery (c), and for the distal right coro-nary artery (d) were measured using a circular
region of interest (ROI) cursor. Enhancement
values for the coronary arteries were measured
on a cross-sectional image at each slice levelusing an ROI cursor (dotted line).
Academic Radiology, Vol 17, No 2, February 2010 INJECTION PROTOCOL IN 320-SLICE CORONARY CT
(23%), 24 had a positive family history for CAD (24%), 32 had
dyslipidemia (33%), and 49 were hypertensive (50%). CTCA
revealed significant coronary artery stenosis (lumen obstruc-
tion of $50%) in 24 patients (24%).
All the examinations were performed within a single heart-
beat with electrocardiogram-gating. Forty-one of the 98
patients were imaged with a dose modulation, and the remain-
ing patients (n = 57) were imaged with prospective gating.
The phase windows for these 57 patients were 70%–80%
(n = 12), 65%–85% (n = 29), and 30%–90% (n = 16). The
mean estimated effective doses for the patients with dose
modulation and prospective gating were 14.7 � 4.6 mSv
and 8.0 � 2.2 mSv, respectively. The mean data acquisition
time was 1.54 � 0.26 seconds.
There were no statistically significant differences in age,
body weight, mean heart rate during acquisition of CT scans,
mean flow rate, and the mean iodine delivery rate between the
two groups (Table 1). The mean total dose of contrast material
was 47.5� 7.4 mL in group A and 41.5� 5.5 mL in group B.
The mean enhancement values of the pulmonary artery trunk
and right ventricle for group A were significantly higher than
those for group B (P < .01); however, there were no signifi-
cant differences in the mean enhancement values of the
ascending aorta, left ventricle, and coronary arteries between
the two groups (Table 2). Also, there was no statistically signif-
icant difference between the mean enhancement values at the
three different levels of the RCA (group A; P = .27, group B;
P = .07).
DISCUSSION
This is the first study to investigate the feasibility of low-
volume injections of contrast material with a body weight–
adapted iodine-dose protocol in 320-detector row CTCA.
The use of 0.7 mL/kg of contrast material injected at 10
seconds resulted in sufficient and steady enhancement in the
ascending aorta and coronary artery.
In CTCA, high and consistent vascular enhancement is
a prerequisite for sufficient evaluation (5–8), and an optimal
enhancement value in the coronary arteries is considered to
be more than 300–350 Hounsfield units (13). For this purpose,
a high concentration of nonionic contrast material, such as
350–400 mg of iodine/mL, should be injected at a fast injection
rate of 3.5–5 mL/second (6–8). Most investigators used a fixed
dose of contrast material, such as 60–80 mL, administered at
a fixed injection rate in 64- or 320-detector row CTCA
(7,10,11,13). However, an increase in the patient’s body weight
can lead to lower contrast enhancement, and therefore the
contrast material volume should be adjusted for the patient’s
body weight in CTCA (8,13,14). Recently, Nakaura et al
reported that the patient weight–adapted iodine-dose protocol
with a fixed injection duration yielded significantly better
image quality than the fixed-dose protocol using a 64-detector
row CTCA (9). In that report, 1.0 mL/kg body weight of
contrast material (370 mgI/mL) was useful to achieve a suffi-
cient contrast enhancement, and injection duration of 15
seconds was recommended for use in 64-detector row CTCA.
209
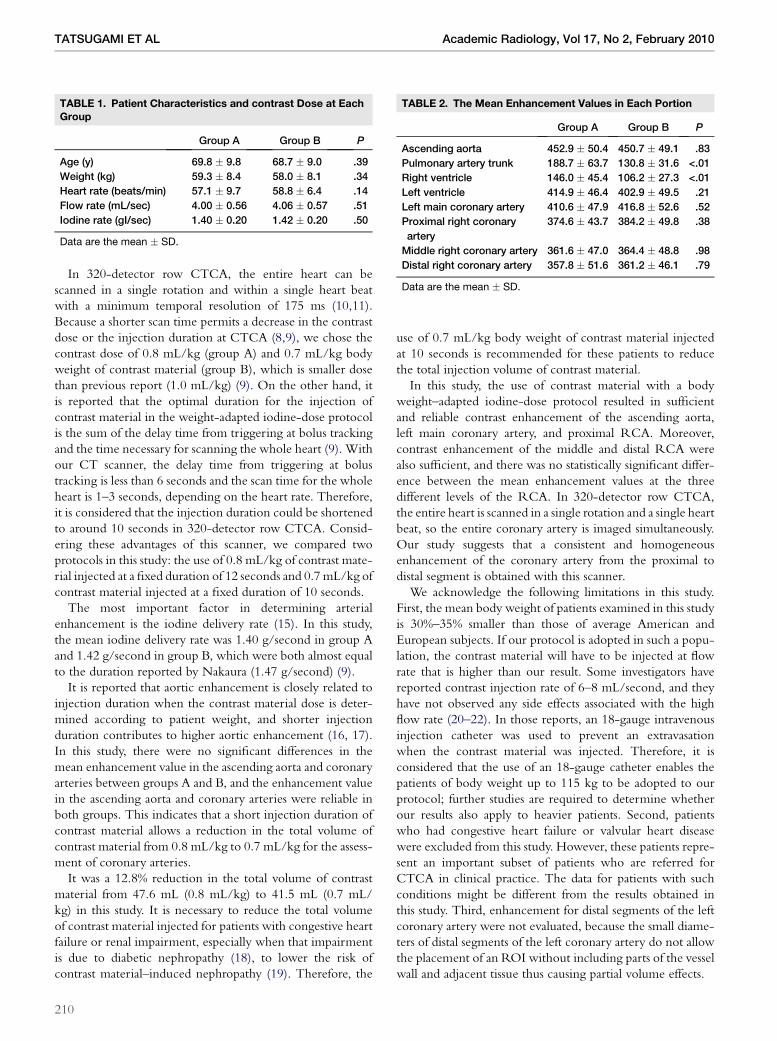
TABLE 2. The Mean Enhancement Values in Each Portion
Group A Group B P
Ascending aorta 452.9 � 50.4 450.7 � 49.1 .83
Pulmonary artery trunk 188.7 � 63.7 130.8 � 31.6 <.01
Right ventricle 146.0 � 45.4 106.2 � 27.3 <.01
Left ventricle 414.9 � 46.4 402.9 � 49.5 .21
Left main coronary artery 410.6 � 47.9 416.8 � 52.6 .52
Proximal right coronary
artery
374.6 � 43.7 384.2 � 49.8 .38
Middle right coronary artery 361.6 � 47.0 364.4 � 48.8 .98
Distal right coronary artery 357.8 � 51.6 361.2 � 46.1 .79
Data are the mean � SD.
TABLE 1. Patient Characteristics and contrast Dose at EachGroup
Group A Group B P
Age (y) 69.8 � 9.8 68.7 � 9.0 .39
Weight (kg) 59.3 � 8.4 58.0 � 8.1 .34
Heart rate (beats/min) 57.1 � 9.7 58.8 � 6.4 .14
Flow rate (mL/sec) 4.00 � 0.56 4.06 � 0.57 .51
Iodine rate (gI/sec) 1.40 � 0.20 1.42 � 0.20 .50
Data are the mean � SD.
TATSUGAMI ET AL Academic Radiology, Vol 17, No 2, February 2010
In 320-detector row CTCA, the entire heart can be
scanned in a single rotation and within a single heart beat
with a minimum temporal resolution of 175 ms (10,11).
Because a shorter scan time permits a decrease in the contrast
dose or the injection duration at CTCA (8,9), we chose the
contrast dose of 0.8 mL/kg (group A) and 0.7 mL/kg body
weight of contrast material (group B), which is smaller dose
than previous report (1.0 mL/kg) (9). On the other hand, it
is reported that the optimal duration for the injection of
contrast material in the weight-adapted iodine-dose protocol
is the sum of the delay time from triggering at bolus tracking
and the time necessary for scanning the whole heart (9). With
our CT scanner, the delay time from triggering at bolus
tracking is less than 6 seconds and the scan time for the whole
heart is 1–3 seconds, depending on the heart rate. Therefore,
it is considered that the injection duration could be shortened
to around 10 seconds in 320-detector row CTCA. Consid-
ering these advantages of this scanner, we compared two
protocols in this study: the use of 0.8 mL/kg of contrast mate-
rial injected at a fixed duration of 12 seconds and 0.7 mL/kg of
contrast material injected at a fixed duration of 10 seconds.
The most important factor in determining arterial
enhancement is the iodine delivery rate (15). In this study,
the mean iodine delivery rate was 1.40 g/second in group A
and 1.42 g/second in group B, which were both almost equal
to the duration reported by Nakaura (1.47 g/second) (9).
It is reported that aortic enhancement is closely related to
injection duration when the contrast material dose is deter-
mined according to patient weight, and shorter injection
duration contributes to higher aortic enhancement (16, 17).
In this study, there were no significant differences in the
mean enhancement value in the ascending aorta and coronary
arteries between groups A and B, and the enhancement value
in the ascending aorta and coronary arteries were reliable in
both groups. This indicates that a short injection duration of
contrast material allows a reduction in the total volume of
contrast material from 0.8 mL/kg to 0.7 mL/kg for the assess-
ment of coronary arteries.
It was a 12.8% reduction in the total volume of contrast
material from 47.6 mL (0.8 mL/kg) to 41.5 mL (0.7 mL/
kg) in this study. It is necessary to reduce the total volume
of contrast material injected for patients with congestive heart
failure or renal impairment, especially when that impairment
is due to diabetic nephropathy (18), to lower the risk of
contrast material–induced nephropathy (19). Therefore, the
210
use of 0.7 mL/kg body weight of contrast material injected
at 10 seconds is recommended for these patients to reduce
the total injection volume of contrast material.
In this study, the use of contrast material with a body
weight–adapted iodine-dose protocol resulted in sufficient
and reliable contrast enhancement of the ascending aorta,
left main coronary artery, and proximal RCA. Moreover,
contrast enhancement of the middle and distal RCA were
also sufficient, and there was no statistically significant differ-
ence between the mean enhancement values at the three
different levels of the RCA. In 320-detector row CTCA,
the entire heart is scanned in a single rotation and a single heart
beat, so the entire coronary artery is imaged simultaneously.
Our study suggests that a consistent and homogeneous
enhancement of the coronary artery from the proximal to
distal segment is obtained with this scanner.
We acknowledge the following limitations in this study.
First, the mean body weight of patients examined in this study
is 30%–35% smaller than those of average American and
European subjects. If our protocol is adopted in such a popu-
lation, the contrast material will have to be injected at flow
rate that is higher than our result. Some investigators have
reported contrast injection rate of 6–8 mL/second, and they
have not observed any side effects associated with the high
flow rate (20–22). In those reports, an 18-gauge intravenous
injection catheter was used to prevent an extravasation
when the contrast material was injected. Therefore, it is
considered that the use of an 18-gauge catheter enables the
patients of body weight up to 115 kg to be adopted to our
protocol; further studies are required to determine whether
our results also apply to heavier patients. Second, patients
who had congestive heart failure or valvular heart disease
were excluded from this study. However, these patients repre-
sent an important subset of patients who are referred for
CTCA in clinical practice. The data for patients with such
conditions might be different from the results obtained in
this study. Third, enhancement for distal segments of the left
coronary artery were not evaluated, because the small diame-
ters of distal segments of the left coronary artery do not allow
the placement of an ROI without including parts of the vessel
wall and adjacent tissue thus causing partial volume effects.

Academic Radiology, Vol 17, No 2, February 2010 INJECTION PROTOCOL IN 320-SLICE CORONARY CT
In conclusion, the use of 0.7 mL/kg of contrast material
injected at a fixed duration of 10 seconds was feasible for
CTCA performed with a 320-detector row CT scanner and
a sufficient and reliable contrast enhancement was maintained
in the ascending aorta and coronary artery.
REFERENCES
1. Achenbach S, Giesler T, Ropers D, et al. Detection of coronary artery
stenoses by contrast-enhanced, retrospectively electrocardiographi-
cally-gated, multislice spiral computed tomography. Circulation 2001;
103:2535–2538.
2. Nieman K, Oudkerk M, Rensing BJ, et al. Coronary angiography with multi-
slice computed tomography. Lancet 2001; 357:599–603.
3. Beck T, Burgstahler C, Kuettner A, et al. Clinical use of multislice spiral
computed tomography in 210 highly preselected patients: experience
with 4 and 16 slice technology. Heart 2005; 91:1423–1427.
4. Bley TA, Ghanem NA, Foell D, et al. Computed tomography coronary angi-
ography with 370-millisecond gantry rotation time: evaluation of the best
image reconstruction interval. J Comput Assist Tomogr 2005; 29:1–5.
5. Cademartiri F, Mollet NR, Lemos PA, et al. Higher intracoronary attenua-
tion improves diagnostic accuracy in MDCT coronary angiography. AJR
Am J Roentgenol 2006; 187:W430–W433.
6. Cademartiri F, Mollet NR, van der Lugt A, et al. Intravenous contrast mate-
rial administration at helical 16-detector row CT coronary angiography:
effect of iodine concentration on vascular attenuation. Radiology 2005;
236:661–665.
7. Schoepf UJ, Zwerner PL, Savino G, et al. Coronary CT angiography. Radi-
ology 2007; 244:48–63.
8. Yamamuro M, Tadamura E, Kanao S, et al. Coronary angiography by
64-detector row computed tomography using low dose of contrast mate-
rial with saline chaser: influence of total injection volume on vessel
attenuation. J Comput Assist Tomogr 2007; 31:272–280.
9. Nakaura T, Awai K, Yauaga Y, et al. Contrast injection protocols for coro-
nary computed tomography angiography using a 64-detector scanner:
comparison between patient weight-adjusted- and fixed iodine-dose
protocols. Invest Radiol 2008; 43:512–519.
10. Rybicki FJ, Otero HJ, Steigner ML, et al. Initial evaluation of coronary
images from 320-detector row computed tomography. Int J Cardiovasc
Imaging 2008; 24:535–546.
11. Steigner ML, Otero HJ, Cai T, et al. Narrowing the phase window width in
prospectively ECG-gated single heart beat 320-detector row coronary CT
angiography. Int J Cardiovasc Imaging 2009; 25:85–90.
12. Einstein AJ, Moser KW, Thompson RC, et al. Radiation dose to patients
from cardiac diagnostic imaging. Circulation 2007; 116:1290–1305.
13. Bae KT, Seeck BA, Hildebolt CF, et al. Contrast enhancement in cardio-
vascular MDCT: effect of body weight, height, body surface area, body
mass index, and obesity. AJR Am J Roentgenol 2008; 190:777–784.
14. Tatsugami F, Husmann L, Herzog BA, et al. Evaluation of a body mass
index-adapted protocol for low-dose 64-MDCT coronary angiography
with prospective ECG triggering. Am J Roentgenol 2009; 192:635–638.
15. Yanaga Y, Awai K, Nakaura T, et al. Effect of contrast injection protocols with
dose adjusted to the estimated lean patient body weight on aortic enhance-
ment at CT angiography. AJR Am J Roentgenol 2009; 192:1071–1078.
16. Awai K, Hiraishi K, Hori S. Effect of contrast material injection duration and
rate on aortic peak time and peak enhancement at dynamic CT involving
injection protocol with dose tailored to patient weight. Radiology 2004;
230:142–150.
17. Ichikawa T, Erturk SM, Araki T. Multiphasic contrast-enhanced multidetec-
tor-row CT of liver: contrast-enhancement theory and practical scan
protocol with a combination of fixed injection duration and patients’
body-weight-tailored dose of contrast material. Eur J Radiol 2006; 58:
165–176.
18. Parfrey PS, Griffiths SM, Barrett BJ, et al. Contrast material-induced renal
failure in patients with diabetes mellitus, renal insufficiency, or both.
A prospective controlled study. N Engl J Med 1989; 320:143–149.
19. Solomon R. Contrast media nephropathy—how to diagnose and how to
prevent? Nephrol Dial Transplant 2007; 22:1812–1815.
20. Donnino R, Jacobs JE, Doshi JV, et al. Dual-source versus single-source
cardiac CT angiography: comparison of diagnostic image quality.
Am J Roentgenol 2009; 192:1051–1056.
21. Matsumoto M, Kodama N, Endo Y, et al. Dynamic 3D-CT angiography.
Am J Neuroradiol 2007; 28:299–304.
22. Schueller G, Schima W, Schueller-Weidekamm C, et al. Multidetector CT
of pancreas: effects of contrast material flow rate and individualized scan
delay on enhancement of pancreas and tumor contrast. Radiology 2006;
241:441–448.
211