Embed Size (px)
Citation preview

ORIGINAL PAPER
Feasibility and influence of hTEE monitoring on postoperativemanagement in cardiac surgery patients
S. Treskatsch1 • F. Balzer1 • F. Knebel2 • M. Habicher1 •
J. P. Braun3 • M. Kastrup1 • H. Grubitzsch4 •
K.-D. Wernecke5 • C. Spies1 • M. Sander1
Received: 26 March 2015 / Accepted: 1 June 2015 / Published online: 6 June 2015
� Springer Science+Business Media Dordrecht 2015
Abstract Monoplane hemodynamic TEE (hTEE) moni-
toring (ImaCor�ClariTEE�) might be a useful alternative to
continuously evaluate cardiovascular function andwe aimed
to investigate the feasibility and influence of hTEE moni-
toring on postoperative management in cardiac surgery
patients. After IRB approval we reviewed the electronic data
of cardiac surgery patients admitted to our intensive care
between 01/01/2012 and 30/06/2013 in a case-controlled
matched-pairs design. Patients were eligible for the study
when they presented a sustained hemodynamic instability
postoperatively with the clinical need of an extended
hemodynamic monitoring: (a) hTEE (hTEE group, n = 18),
or (b) transpulmonary thermodilution (control group,
n = 18). hTEE was performed by ICU residents after
receiving an approximately 6-h hTEE training session. For
hTEE guided hemodynamic optimization an institutional
algorithm was used. The hTEE probe was blindly inserted at
the first attempt in all patients and image quality was at least
judged to be adequate. The frequency of hemodynamic
examinations was higher (ten complete hTEE examinations
every 2.6 h) in contrast to the control group (one examina-
tion every 8 h). hTEE findings, including five unexpected
right heart failure and one pericardial tamponade, led to a
change of current therapy in 89 % of patients. The cumula-
tive dose of epinephrine was significantly reduced
(p = 0.034) and levosimendan administration was signifi-
cantly increased (p = 0.047) in the hTEE group. hTEE was
non-inferior to the control group in guiding norepinephrine
treatment (p = 0.038). hTEE monitoring performed by ICU
residents was feasible and beneficially influenced the post-
operative management of cardiac surgery patients.
Keywords Goal directed therapy � Echocardiography �hTEE � Monoplane probe � Cardiac surgery � Postoperativemanagement
Abbreviations
GDT Goal-directed therapy
DO2 Delivery of oxygen
CO Cardiac output
LCOS Low cardiac output syndrome
hTEE Hemodynamic monoplane transesophageal
echocardiography
ICU Intensive care unit
PICCO� Pulse contour cardiac output (monitor)
ESC European Society of Cardiology
EACVI European Association of Cardiovascular
Imaging
EACTA European Association of Cardiothoracic
Anaesthesiologists
TG SAX Transgastric short axis (view)
Electronic supplementary material The online version of thisarticle (doi:10.1007/s10554-015-0689-8) contains supplementarymaterial, which is available to authorized users.
& S. Treskatsch
1 Department of Anesthesiology and Intensive Care Medicine,
Campus Charite Mitte and Campus Virchow Klinikum,
Charite - Universitatsmedizin Berlin, Chariteplatz 1,
10117 Berlin, Germany
2 Department of Cardiology, Campus Charite Mitte, Charite -
Universitatsmedizin Berlin, Berlin, Germany
3 Department of Anesthesiology, Intensive Care Medicine and
Pain Therapy, Klinikum Hildesheim GmbH, Hildesheim,
Germany
4 Department of Cardiovascular Surgery, Campus Charite
Mitte, Charite - Universitatsmedizin Berlin, Berlin, Germany
5 SOSTANA GmbH, Berlin, Germany
123
Int J Cardiovasc Imaging (2015) 31:1327–1335
DOI 10.1007/s10554-015-0689-8

4C Midesophageal four chamber (view)
SVC Superior vena cava (view)
LV Left ventricle
RV Right ventricle
IAS Interatriale septum
TEE Multiplane transesophageal echocardiography
SD Standard deviation
IQR Interquartiles
SAPS-II Simplified acute physiology score II
NYHA New York Heart Association
CPB Cardiopulmonary bypass
CABG Coronary bypass grafting
VR Valve reconstruction and/or replacement
EVLWI Extravascular lung water index
Introduction
Several studies in the last decade found benefit in ‘‘goal
directed therapy’’ (GDT) [1, 2]. Goal directed fluid
administration reduced the length of hospital stay [3] and
improved patient outcome after surgery [4, 5]. Excessive
fluid restriction consistently increased the level of hypov-
olemia and the incidence of postoperative complications
[6]. The fundamental principle behind GDT is optimization
of oxygen delivery to tissues (DO2) by optimizing car-
diovascular function using fluids, catecholamines, red
blood cells and supplementary oxygen [7].
Cardiac output (CO) is one of the major determinates of
oxygen delivery [8]. CO depends on: (a) preload,
(b) afterload, (c) myocardial contractility, (d) valve func-
tion and (e) heart rate/rhythm, all of which can be exam-
ined using echocardiography. Postoperative low cardiac
output syndrome (LCOS), especially in cardiac surgery,
thus results in deficient oxygen delivery. Therefore, in
cases of unexplained life-threatening hemodynamic insta-
bility—possibly persisting despite corrective therapy—a
multiplane transesophageal echocardiographic examination
is recommended (Class I indication) to identify the
underlying pathophysiological cause, e.g. hypovolemia,
reduced myocardial contractility, pericardial tamponade
[9], and to guide goal-directed therapy [10, 11].
However, in practice conventional transesophgeal
echocardiography can only be performed intermittently
[12]. Hence, the new ImaCor� ClariTEE� might be a
useful alternative in daily clinical practice. Because of its
small size it can be introduced orally in the patients
esophagus and can remain up to 72 h in situ. With its
flexible probe tip the three most important two-dimensional
views of the heart can be obtained on demand to identify
and manage the pathophysiological causes of LCOS, thus
the name ‘‘hemodynamic TEE’’ (hTEE).
Up to now, there have only been a few clinical trials
investigating the possible benefit of using the ImaCor�
ClariTEE� to guide hemodynamic therapy in high-risk
surgical and/or critically ill patients [13–19]. Monoplane
TEE in the hands of intensivists has been shown to provide
clinically useful estimates of LV function, RV dilation,
hypovolemia and occurrence of pericardial effusion, as
shown evaluated by between experienced echocardiogra-
phers [16]. Furthermore, hTEE frequently led to changes in
clinical management of hemodynamic unstable patients on
ventilator support [15] and also of patients on ventricular
assist devices [14]. We were therefore interested in the
feasibility (=ease of insertion and technical operation) and
influence (=utility as hemodynamic monitor) of hTEE
monitoring on postoperative management in cardiac sur-
gery patients during its clinical implementation.
Methods
After approval of the Charite Ethics Committee, Berlin,
Germany (Study ID number: EA1-249-13; ClinGov. reg-
istration number: NCT02046954), we reviewed charts and
data derived from two electronic patient data management
systems (PDMS: COPRA GmbH, Sasbachwalden, Ger-
many and SAP AG, Walldorf, Germany) of cardiac surgery
patients admitted to our intensive care unit (ICU) of the
department of anesthesiology and intensive care medicine
at the Campus Charite Mitte, Berlin, between 01/01/2012
and 30/06/2013. Written informed consent was waived by
the ethics committee.
Patients were eligible for the study when they presented
with a sustained hemodynamic instability (i.e. lasting
longer than 1 h after ICU admission) despite corrective
therapy, and needed extended hemodynamic monitoring
according to current recommendations [20, 21]. Hemody-
namic instability was clinically defined as (two or more
criteria): persistent tachycardia (heart rate [100/min),
arterial hypotension (mean arterial pressure\60 mmHg),
need for catechlominergic support (norepinephrine
C0.1 lg/kg/min in combination with epinephrine C0.1 lg/kg/min and/or dobutamine C5 lg/kg/min and/or enoxi-
mone C1 lg/kg/min), lactate acidosis (pH\ 7.2) and/or
negative base excess (BE\-2 mmol/l), declining diure-
sis (\0.5 ml/kg/h), and/or suspicion of pericardial tam-
ponade. Those criteria were used to define ‘‘hemodynamic
instability’’ for the purpose of increasing assay sensitivity
by (a) detecting the most hemodynamic compromised
patients by means of (b) the most frequently documented
values in the local PDMS. In order to estimate the influence
of hTEE monitoring, we retrospectively investigated the
following time periods where (a) hTEE (01/10/2012–30/
06/2013), or (b) transpulmonary thermodilution (PICCO�,
1328 Int J Cardiovasc Imaging (2015) 31:1327–1335
123

bolus administration technique) (01/01/2012–30/09/2012,
e.g. before implementation of hTEE) was used. Exclusion
criteria were: (a) age less than 18 years, (b) use of pul-
monary artery catheter and (c) incomplete medical records.
In addition to comparing morphometric, demographic and
operative data, we evaluated (a) the feasibility (=ease of
insertion and technical operation) of hTEE, (b) its utility as
a hemodynamic monitor: amount and frequency of hemo-
dynamic evaluations per patient, use and cumulative doses
of catecholamines in the first week after extending hemo-
dynamic monitoring, postoperative lactate time course, net
fluid balance of the subsequent three postoperative days
(POD), and (c) overall in-hospital mortality.
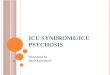
The ClariTEE� probe (Imacor, New York, USA) is a
single use, miniaturized, single-plane (angle = 0�), two-dimensional transesophageal probe, which was orally
inserted in the patients esophagus and remained up to 72 h
in situ for continuously available (‘‘on demand’’) use (as
approved by the Federal Drug Agency) (Fig. 1). The probe
has a flexible tip providing ante- and retroflexion, and was
connected to a standard echocardiographic system (Zura,
Imacor, New York, USA) including standard recording
capabilities (one loop consist of approximately five ECG
cycles), provided by the company (http://imacorinc.com/
htee/products/zura-evo-1-imaging-system.html). Two-di-
mensional measurements, e.g. left ventricular end-diastolic
dimension (LVEDD) and pericardial effusion, and color
Doppler mapping were possible.
During implementation of this transesophageal mono-
plane probe into clinical routine, residents of our ICU
received a training session of approximately 6 h on this
device in vivo and on a hTEE simulator under supervision
of a team of certified echocardiographers (EACVI/EACTA
Adult TEE accreditation and/or national certification by the
German Society of Anesthesiology and Intensive Care
Medicine)—available for 24 h 7 days a week. In addition,
hTEE loops presenting specific hemodynamic conditions
were shown on computer. Residents were trained to obtain
the three most important two-dimensional hTEE views to
determine hemodynamics: (a) transgastric short axis view
(TG SAX) to evaluate global systolic left ventricular (LV)
function, paradoxical septal motion, and pericardial effu-
sion; (b) midesophageal four chamber view (4C) to eval-
uate global systolic biventricular morphology/function,
paradoxical septal motion, mitral valve morphology, and
pericardial effusion; and (c) midesophageal superior vena
cava (SVC) view to evaluate volume responsiveness and
aortic valve morphology/function [17]. A complete exam-
ination was defined to consist of these three views. After
each examination residents had to complete a report with
their qualitative results: (1) global systolic function of the
left ventricle (LV): normal, slightly/moderately/severely
reduced; (2) systolic function of the right ventricle: normal,
reduced; (3) RV/LV-Index: normal, moderately/severely
dilated [22]; (4) position and mobility of the interatrial
septum (IAS): (hyper-)mobile, centered, right- or leftward
shift [23]; (5) position/motion of the interventricular sep-
tum: normal, paradoxical motion; (6) signs of hypov-
olemia: kissing papillary muscles, small cardiac chamber
areas, (hyper-)mobile IAS, collapse of SVC under
mechanical ventilation [24]; (7) presence of pericardial
effusion with potential signs of cardiac tamponade. Certi-
fied echocardiographers then reviewed findings and inter-
pretations of ICU residents. Additionally, overall image
quality was evaluated by the ICU residents as optimal,
adequate (not optimal but sufficient for hemodynamic
guidance), or inadequate and was further reviewed by
certified echocardiographers. ICU residents then had to
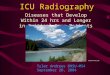
propose a therapy based on their findings according to an
institutional algorithm (Fig. 2). In case of unexpected
findings and/or difficulties in interpretation of the gained
images a cardiologist and/or a certified echocardiographer
had to be called to perform a multiplane TEE (‘‘seek expert
help’’). Patients who were monitored with transpulmonary
thermodilution were treated in a similar approach: therapy
was guided by the measured parameters (cardiac index,
Fig. 1 Comparison of an hTEE (blue) and a conventional multiplane TEE probe (black)
Int J Cardiovasc Imaging (2015) 31:1327–1335 1329
123

systemic vascular resistance, pulmonary artery pressure,
etc.) according to institutional standards guided by the
German S3 guidelines [20].
For informational purposes, cardiopulmonary bypass
(CPB) and anesthesia management were performed
according to our standard operating procedures [25]. Nor-
mothermic CPBwas established with a non-pulsatile flow of
2.5 l min-1 m2 and a mean arterial pressure[60 mmHg.
Cardioplegic arrest was induced and maintained by inter-
mittent administration of antegrade warm potassium enri-
ched blood [26]. After chest closure, the patient was
transferred intubated and mechanically ventilated (pressure-
controlled mode) to ICU. Patients were kept sedated with
propofol (1–3 mg kg-1 h-1) and opioid bolus administra-
tion until cardiopulmonary stabilitywas achieved, chest tube
drainage was insignificant (\100 ml/h), and the patient was
judged to be extubated. If mechanical ventilation was
required for C12 h, analgesic sedation was switched to
midazolam 0.01–0.2 mg kg-1 h-1 combined with sufen-
tanil 0.15–0.7 lg kg-1 h-1, and weaning from mechanical
ventilation was performed according to the standard
operating procedures at our hospital [27]. Further therapy
was based on actual medical standards.
Results are expressed as mean ± standard deviation
(SD), median ± interquartile range (IQR) or percentage, as
appropriate. Normality of continuous variables was checked
with the Kolmogorov–Smirnov test. The exact Mann–
Whitney U-test was used to analyze differences between
groups. The relative frequencies of variables were analyzed
by the exact Chi square test. Non-inferiority of guiding
norepinephrine therapy was based on the on the used
cumulative doses of norepinephrine in the first week after
extending hemodynamic monitoring using hTEE or
transpulmonary thermodilution and was tested by means of
the one-sided Schuirmann-test with an inferiority margin of
‘‘0.3 9 mean (control)’’. p\ 0.05 was considered statisti-
cally significant. All tests should be understood as consti-
tuting exploratory data analysis, such that no adjustments
for multiple tests have been made. Statistics were per-
formed using SPSS 20.0 software (IBM Corporation,
Armonk, New York, USA) and EquivTest 2.0 Copyright�2001 Statistical Solutions Ltd. Cork Ireland.
Fig. 2 Institutional echocardiography-based management-algorithm
1330 Int J Cardiovasc Imaging (2015) 31:1327–1335
123

Results
18 patients were eligible according to the aforementioned
criteria during the study period and were thus monitored
with hTEE (hTEE group). These patients were retrospec-
tively case-controlled matched based on their SAPS-II
admission score on ICU (score ± 5) to 18 patients moni-
tored with transpulmonary thermodilution before hTEE
implementation (control group).
Basic patient characteristics and surgical data are pre-
sented in Table 1. There were no significant differences in
preoperative functional status, e.g. NYHA classification,
surgical procedures, or other comorbidities between
groups. Concerning the nature of valve surgery (VR)
patients with reconstructive, replacement or redo of the
aortic valve due to aortic stenosis and/or insufficiency and/
or endocarditis were included.
ICU residents at the first attempt in all patients blindly
inserted the hTEE probe. Image quality was judged to be
adequate to guide hemodynamic therapy or better in all
patients (adequate: n = 11, 61 %; optimal: n = 7, 39 %).
Image quality was never inadequate and we never had to
proceed to a conventional multiplane TEE based on hTEE
findings. In 4 patients (22 %) only 2 of the 3 views could
be obtained (no TG SAX: n = 3, no SVC: n = 1), how-
ever, these missing views were not assessed to have any
further influence on clinical decision-making. Therefore all
studies were rated to be complete. In addition, supervisors
were also not able to obtain these missing views and their
interpretations were equal with those of the residents.
30 ± 20 hTEE loops were recorded per patient with a
mean duration of probe insertion of 26.2 ± 17.6 h. This
resulted in approximately ten complete hTEE examinations
per patient, one every 2.6 h. In the control group,
extravascular lung water index (EVLWI) as a surrogate
parameter for the frequency of transpulmonary thermodi-
lutions was determined an average of 9 times per patients
in a 3 day period resulting in approximately one complete
examination every 8 h.
Results of the hTEE examination changed the current ther-
apy in nearly all cases (n = 16, 89 %): (1) administration of
levosimendan due to a severely reduced left ventricular func-
tion (n = 10, 56 %), (2) supporting right ventricular function,
i.e. administration of iloprost and/or PDE-III-inhibitors and/or
levosimendan, due to new/unexpected postoperative right heart
failure (n = 5, 28 %) (Fig. 2) (supplementary videos), and (3)
re-operation due to pericardial tamponade (n = 1, 6 %). The
first documented transpulmonary thermodilution led to a
change in current therapy in 44.4 % (n = 8): (a) volume
administration (n = 6) and (b) adding PDE-III-inhibitor
(n = 2). In addition, interpretation of the first transpulmonary
thermodilution parameters never triggered administration of
levosimendan (Fig. 3).
7 patients in the control group and only 3 patients in the
hTEE group died in hospital, but the difference did not
reach statistical significance (p = 0.264). Data on the
postoperative management in survivors (hTEE: n = 15;
control: n = 11) are presented in Table 2. Maximum
arterial lactate level and its decline in the observed post-
operative course were comparable in both groups. Net fluid
balance in the first three postoperative days was not sig-
nificantly different between groups. However, the cumu-
lative dose of epinephrine in the first week after extending
hemodynamic monitoring was significantly reduced
(p = 0.034) along with a significantly increased frequency
of levosimendan administration (p = 0.047) in the hTEE
group. There was a non-significant trend towards a lower
daily cumulative dose of enoximone in the hTEE group
(p = 0.051). Finally, hTEE was non-inferior to the control
group in guiding norepinephrine treatment (p = 0.038).
Discussion
The main findings of this retrospective, single center
analysis were that postoperative hTEE monitoring after
cardiac surgery is feasible and immediately influences
hemodynamic therapy and patient management.
After a short and intensive training programme, residents
of our ICU were able to achieve adequate or optimal quality
of obtainable images in all cases comparable to a previous
study [17]. In 22 % of the patients only two of the three
hTEE views could be acquired. However, in face of
hemodynamic guidance the missing views were not rated to
Table 1 Morphometric and demographic data and surgical
procedures
Control
(n = 18)
hTEE
(n = 18)
P value
Age (years) 69 ± 11 72 ± 9 0.389
Weight (kg) 77 ± 14 80 ± 16 0.521
Height (m) 1.73 ± 0.9 1.72 ± 0.8 0.621
Sex (men/women) 15/3 15/3 1.000
SAPS-II ICU admission 47 ± 20 49 ± 21 1.000
Procedure (n)
CABG 10 11 0.735
VR 11 6 0.095
CABG ? VR 4 1 0.148
Ventricle Rupture 0 1 0.310
NYHA III/IV (patients) 9 8 0.738
Coronary artery disease 14 15 0.674
Atrial fibrillation 10 9 0.738
Pulmonary arterial hypertension 6 6 1.000
Data are expressed as mean ± SD, numbers or percentage
Int J Cardiovasc Imaging (2015) 31:1327–1335 1331
123

have any further influence on clinical decision-making. This
is in line with a previous prospective trial in 94 ventilated
critically ill patients where image quality allowed hemo-
dynamic monitoring in 85 % [16]. Furthermore, the tech-
nical limitations of the small, monoplane hTEE probe were
the main cause for an overall lower image quality image
quality compared to a conventional multiplane probe in this
retrospective analysis [16]. This may be caused by (a) the
small, more flexible probe establishing too less surface
contact area and (b) the inability to rotate the probe
resulting in suboptimal cross-sections. In particular, at
times the lateral wall of the left ventricle was poorly visu-
alized in the midesophageal four chamber view, but always
optimal in the transgastric short axis view. However, image
quality was never inadequate for guiding hemodynamic
optimization. Indeed, residents of our department felt
quickly familiar with the probe focusing on only three
views and the possibility to frequently repeat the exami-
nation. Nevertheless, owing to these technical limitations, a
comprehensive echocardiographic evaluation cannot be
conducted with the ClariTEE� probe. Therefore, in case of
unexpected findings a multiplane TEE has to be performed
according to our institutional algorithm (Fig. 2: ‘‘Seek
expert help’’). This was never the case in this study. In
addition, we did not observe any harmful event related to
probe insertion in this retrospective analysis [28]. Espe-
cially, we saw no thermal injury since by design, imaging is
‘‘frozen’’ (the system is off) and pressure is removed (no
flexion) between two examinations (mean time interval
2.6 h).
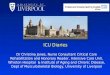
Fig. 3 Right heart failure detected by hTEE: Left dilated SVC; Middle left ventricular hypovolemia, normal global systolic left ventricular
function, paradoxical septal motion; Right right ventricular dilation, severely reduced systolic right ventricular
Table 2 Postoperative
hemodynamic parameters in
survivors during the observation
period
Control
(n = 11)
hTEE
(n = 15)
p value
Norepinephrineaverage (mg/kg/d) 0.16 ± 0.08 0.13 ± 0.11 0.311
Patients on norepinephrine (n) 10 15 0.234
Epinephrineaverage (mg/kg/d)* 0.04 ± 0.02 0.02 ± 0.02 0.034
Patients on epinephrine (n) 9 13 0.735
Levosimendanaverage (mg/kg/d) 0.05 ± 0.02 0.04 ± 0.01 0.811
Patients on levosimendan (n)* 3 10 0.047
Enoximoneaverage (mg/kg/d) 1.42 ± 0.56 0.91 ± 0.50 0.051
Patients on enoximone (n) 9 11 0.612
Net fluid balance
POD 1 ?2104 ± 2045 ?2143 ± 1214 0.959
POD 2 ?542 ± 1514 ?515 ± 1829 1.000
POD 3 -327 ± 2124 ?170 ± 1543 0.760
Lactatemax (mg/dl) 86 ± 34 86 ± 53 0.878
Interval ‘‘Lactatemax – Lactate\20mg/dl’’ (h) 13 ± 7 14 ± 8 0.936
Data are expressed as mean ± SD or numbers
POD postoperative day
* Significant differences between groups
1332 Int J Cardiovasc Imaging (2015) 31:1327–1335
123

As early as 1998 Benjamin et al. [29] demonstrated that
an additional multiplane transesophageal echocardiography
performed by intensivists changed pre-exam hemodynamic
therapy based on pulmonary artery catheter findings in
[50 % of patients. This was especially true in the case of
reduced left ventricular contractility. In the present study,
interpretation of hTEE findings after probe insertion pro-
voked changes of the current therapy in 89 % of patients.
Observers mostly reported echocardiographic findings
consistent with refractory left and/or right ventricular
failure due to chronic heart insufficiency, leading them to
administer levosimendan as ultima ratio add-on medication
[30]. This resulted in a significant reduction in the cumu-
lative dose of epinephrine. In addition, the cumulative dose
of enoximone was non-significantly reduced; however, this
may be explained in part because we do not administer
levosimendan and enoximone simultaneously in our ICU,
based on their pharmacodynamic and -kinetic profiles [31].
Furthermore, we did not observe an increase in the fre-
quency and dose of norepinephrine in the hTEE group
despite vasodilating properties of levosimendan [32]. This
is consistent with a previous study demonstrating that
levosimendan treatment did not lead to an increase in
norepinephrine when goal-directed volume therapy is
applied at the same time [30].
Interestingly, hTEE monitoring detected new and/or
clinically unexpected right ventricular (RV) dysfunction
[19, 33, 34] in approximately one-third of the patients,
comparable to a previous study [14]. Fletcher et al. [19]
also detected even more new right ventricular failure
(67.6 %) in ventilated patients with severe cardiogenic
shock requiring hemodynamic support using hTEE. Also,
one pericardial tamponade by monoplane hTEE was
detected in a very early postoperative time frame with
consequent re-operation [35–39]. In accord with the mean
duration of hTEE probe insertion [17], our results empha-
size the role of cardiac visualization early in the postop-
erative course in order to detect (new) cardiac dysfunction,
i.e. especially RV failure, optimize hemodynamics and
improve patients management [11, 16]. In this context, it is
worth noticing that we observed a non-significant trend
towards improved in-hospital mortality in the hTEE group.
We therefore conclude that the implementation of hTEE
monitoring into clinical practice following an approxi-
mately 6-h teaching session demonstrates that a focused
echocardiographic approach is feasible and sufficient to
enable physicians optimizing hemodynamics [40–43].
We did not detect a difference in the amount of volume
that has been administered between both groups. It may be
that hTEE monitoring only helps in detecting the right time
point when to administer volume, especially when atrial
fibrillation [8, 44–46] and/or right heart dysfunction are
present. In this context it has been shown that concomitant
tricuspid regurgitation is associated with underestimation
of cardiac output measured by thermodilution [47]. In
addition, clinically used parameters to estimate volume
responsiveness seem to be unreliable in patients with right
heart dysfunction [48, 49]. Finally, hTEE monitoring was
non-inferior to standard patient care in guiding nore-
pinephrine treatment.
This study stands out for its clinical approach, and as
such it has some limitations. As with all retrospective
studies, our analysis was limited by the variables available
in routine patient care. First, the number of patients ana-
lyzed in this study may also be regarded as relatively small.
In addition, EVLWI as a surrogate for the frequency of
transpulmonary thermodilutions might be inadequate in
patients with sinus rhythm and continuous pulse contour
analysis. However, there may exist some clinical scenarios
in which testing for validity of continuous pulse contour
analysis is still missing up to date. In this context it is
important to mention that C50 % of the patients of both
groups presented with atrial fibrillation (AF) preoperatively
or developed AF postoperatively. These findings represent
our first clinical experience with a new interesting device
during its implementation into daily routine. In contrast to
conventional hemodynamic monitors, the advantage of
hTEE might be the frequent ‘‘on demand’’ visualization of
the heart in combination with the here presented hemody-
namic optimization algorithm. Secondly, one might assume
that patients in the hTEE group were sicker and therefore
received significantly more often levosimendan. However,
patients functional status, all other comorbidities and their
clinical status upon arrival on ICU were comparable, and
all patients suffered sustained, life-threating hemodynamic
instability after cardiac surgery. Here, hTEE findings in
postoperative cardiac surgery patients lead to a change in
therapy in nearly all cases. Therefore, despite limitations of
its case-controlled matched-pairs approach, this study
clearly demonstrated the benefit of a focused trans-
esophageal echocardiography early in the postoperative
course if hemodynamic instability is present. Thirdly,
because assessment of volume responsiveness, the clear-
ance of lactate and the decrease in catecholaminergic
support is a compound of several factors and physician
expertise, the here presented impact of hTEE monitoring
has to be interpreted on that condition. However, there is a
need for individualized therapeutic strategies and algo-
rithms based on physiology [50, 51].
In conclusion, this retrospective analysis revealed a
beneficial influence of hTEE monitoring on the postoper-
ative management of cardiac surgery patients. Despite a
short training session, ICU residents achieved at least
adequate image quality to guide hemodynamic therapy.
hTEE monitoring is clinically feasible and can simply be
implemented into daily routine. It is not inferior to standard
Int J Cardiovasc Imaging (2015) 31:1327–1335 1333
123

patient care in guiding norepinephrine therapy. Besides one
urgent re-operation due to pericardial tamponade, hTEE
monitoring seemed to influence hemodynamic manage-
ment in patients with postoperative low cardiac output
syndrome. Finally, hTEE monitoring was useful in the
diagnosis and management of unexpected postoperative
right heart failure. Further prospective, randomized trials
are warranted to investigate the capabilities of this new
device.
Acknowledgments This study was performed within an institu-
tional Grant from Charite – Universitatsmedizin Berlin. ImaCor
provided the echocardiographic system (Zura, Imacor, New York,
USA) and the ClariTEE� probes without charge for this study, the
company provided no further financial support.
Conflict of interest S.T. received funding for experimental research
from B. Braun and honoraria for lectures from Edwards and Car-
inopharm. C.S. received (a) funding for research from the following
companies and societies: Abbott, Aspect, Baxter, Care Fusion, Del-
tex, Fresenius, Grunenthal, Hutchinson, Kohler Chemie, MSD, MCN,
Novartis, Pajunk, Pulsion, Roche, Sysmex, University Hospital Sta-
vanger, Argus, BDA, BMBF, DKH, DLR, German Research Society,
GIZ, Charite, Stifterverband, and (b) honoraria for lectures and travel/
accommodations/meeting expenses unrelated to activities listed from
Abbott, Essex Pharma, GSK, Bispebjerg Hospital, Aspect, and
(c) expert testimony from the ethical committee Vienna Faculty of
Medicine. J.P.B. received honoraria for lectures from Edwards, Car-
inopharm, Abbott, Orion and Pfizer. M.S. received funding for
research from Edwards Life Sciences, The Medicines Company and
Pulsion, honoraria for lectures from Edwards and Pulsion. For the
remaining authors none conflict of interests were declared.
References
1. Pearse R, Dawson D, Fawcett J, Rhodes A, Grounds RM et al
(2005) Early goal-directed therapy after major surgery reduces
complications and duration of hospital stay. A randomised,
controlled trial [ISRCTN38797445]. Crit Care 9:R687–R693
2. Hamilton MA, Cecconi M, Rhodes A (2011) A systematic review
and meta-analysis on the use of preemptive hemodynamic
intervention to improve postoperative outcomes in moderate and
high-risk surgical patients. Anesth Analg 112:1392–1402
3. Gan TJ, Soppitt A, Maroof M, el-Moalem H, Robertson KM et al
(2002) Goal-directed intraoperative fluid administration reduces
length of hospital stay after major surgery. Anesthesiology
97:820–826
4. Grocott MPW, Mythen MG, Gan TJ (2005) Perioperative fluid
management and clinical outcomes in adults. Anesth Analg
100:1093–1106
5. Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A et al (2001)
Early goal directed therapy in the treatment of severe sepsis and
septic shock. N Engl J Med 345:1368–1377
6. Futier E, Constantin JM, Petit A, Chanques G, Kwiatkowski F
et al (2010) Conservative vs restrictive individualized goal-di-
rected fluid replacement strategy in major abdominal surgery: a
prospective randomized trial. Arch Surg 145:1193–1200
7. Della Rocca G, Pompei L (2011) Goal-directed therapy in
anesthesia: any clinical impact or just a fashion? Minerva
Anestesiol 77:545–553
8. McGee WT, Raghunathan K (2013) Physiologic goal-directed
therapy in the perioperative period: the volume prescription for
high-risk patients. J Cardiothorac Vasc Anesth 27:1079–1086
9. Practice guidelines for perioperative transesophageal echocar-
diography (2010) An updated report by the American Society of
Anesthesiologists and the Society of Cardiovascular Anesthesi-
ologists Task Force on Transesophageal Echocardiograph.
Anesthesiology 112:1084–1096
10. Giglio M, Dalfino L, Puntillo F, Rubino G, Marucci M et al
(2012) Haemodynamic goal-directed therapy in cardiac and
vascular surgery. A systematic review and meta-analysis. Interact
CardioVasc Thorac Surg 15:878–887
11. Aya HD, Cecconi M, Hamilton M, Rhodes A (2013) Goal-di-
rected therapy in cardiac surgery: a systematic review and meta-
analysis. Br J Anaesth 110:510–517
12. Geisen M, Spray D, Fletcher N (2014) Echocardiography-based
hemodynamic management in the cardiac surgical intensive care
unit. J Cardiothorac Vasc Anesth 28:733–744
13. Wagner CE, Bick JS, Webster BH, Selby JH, Byrne JG (2012)
Use of a miniaturized transesophageal echocardiographic probe
in the intensive care unit for diagnosis and treatment of a
hemodynamically unstable patient after aortic valve replacement.
J Cardiothorac Vasc Anesth 26:95–97
14. Maltais S, Costello WT, Billings FTt, Bick JS, Byrne JG et al
(2013) Episodic monoplane transesophageal echocardiography
impacts postoperative management of the cardiac surgery patient.
J Cardiothorac Vasc Anesth 27:665–669
15. Haglund NA, Maltais S, Bick JS, Costello W, Keebler M et al
(2014) Hemodynamic transesophageal echocardiography after
left ventricular assist device implantation. J Cardiothorac Vasc
Anesth 28:1184–1190
16. Vieillard-Baron A, Slama M, Mayo P, Charron C, Amiel JB et al
(2013) A pilot study on safety and clinical utility of a single-use
72-hour indwelling transesophageal echocardiography probe.
Intensive Care Med 39:629–635
17. Cioccari L, Baur HR, Berger D, Wiegand J, Takala J et al (2013)
Hemodynamic assessment of critically ill patients using a
miniaturized transesophageal echocardiography probe. Crit Care
17:R121
18. Cavarocchi NC, Pitcher HT, Yang Q, Karbowski P, Miessau J
et al (2013) Weaning of extracorporeal membrane oxygenation
using continuous hemodynamic transesophageal echocardiogra-
phy. J Thorac Cardiovasc Surg 146:1474–1479
19. Fletcher N, Geisen M, Meeran H, Spray D, Cecconi M (2015)
Initial clinical experience with a miniaturized transesophageal
echocardiography probe in a cardiac intensive care unit. J Car-
diothorac Vasc Anesth. doi:10.1053/j.jvca.2014.09.016
20. Carl M, Alms A, Braun J, Dongas A, Erb J et al (2010) S3
guidelines for intensive care in cardiac surgery patients: hemo-
dynamic monitoring and cardiocirculary system. Ger Med Sci 8.
doi:10.3205/000101
21. Cheitlin MD, Armstrong WF, Aurigemma GP, Beller GA, Bier-
man FZ et al (2003) ACC/AHA/ASE 2003 Guideline Update for
the Clinical Application of Echocardiography: summary article.
A report of the American College of Cardiology/American Heart
Association Task Force on Practice Guidelines (ACC/AHA/ASE
Committee to Update the 1997 Guidelines for the Clinical
Application of Echocardiography). J Am Soc Echocardiogr
16:1091–1110
22. Kukucka M, Stepanenko A, Potapov E, Krabatsch T, Redlin M
et al (2011) Right-to-left ventricular end-diastolic diameter ratio
and prediction of right ventricular failure with continuous-flow
left ventricular assist devices. J Heart Lung Transplant 30:64–69
23. Kusumoto FM, Muhiudeen IA, Kuecherer HF, Cahalan MK,
Schiller NB (1993) Response of the interatrial septum to
transatrial pressure gradients and its potential for predicting
1334 Int J Cardiovasc Imaging (2015) 31:1327–1335
123

pulmonary capillary wedge pressure: an intraoperative study
using transesophageal echocardiography in patients during
mechanical ventilation. J Am Coll Cardiol 21:721–728
24. Vieillard-Baron A, Chergui K, Rabiller A, Peyrouset O, Page B
et al (2004) Superior vena caval collapsibility as a gauge of
volume status in ventilated septic patients. Intensive Care Med
30:1734–1739
25. Spies C, Kastrup M, Kerner T, Melzer-Gartzke C, Zielke H, Kox
W (2013) SOPs in Anasthesiologie und Schmerztherapie: Alle
relevanten Standards und Techniken fur die Klinik. 1 ed. Thieme
26. Calafiore AM, Teodori G, Di Giammarco G, Bosco G, Mezzetti
A et al (1994) Intermittent antegrade cardioplegia: warm blood vs
cold crystalloid. A clinical study. J Cardiovasc Surg 35:179–184
27. Spies C, Kastrup M, Kerner T, Melzer-Gartzke C, Zielke H, Kox
W (2013) SOPs in Intensivmedizin und Notfallmedizin: Alle rel-
evanten Standards und Techniken fur die KLinik, 1 ed. Thieme
28. Hilberath JN, Oakes DA, Shernan SK, Bulwer BE, D’Ambra MN
et al (2010) Safety of transesophageal echocardiography. J Am
Soc Echocardiogr 23:1115–1127
29. Benjamin E, Griffin K, Leibowitz AB, Manasia A, Oropello JM
et al (1998) Goal-directed transesophageal echocardiography
performed by intensivists to assess left ventricular function:
comparison with pulmonary artery catheterization. J Cardiothorac
Vasc Anesth 12:10–15
30. Erb J, Beutlhauser T, Feldheiser A, Schuster B, Treskatsch S et al
(2014) Influence of levosimendan on organ dysfunction in
patients with severely reduced left ventricular function under-
going cardiac surgery. J Int Med Res 42:750–764
31. Nieminen MS, Fruhwald S, Heunks LM, Suominen PK, Gordon
AC et al (2013) Levosimendan: current data, clinical use and
future development. Heart Lung Vessel 5:227–245
32. Toller WG, Stranz C (2006) Levosimendan, a new inotropic and
vasodilator agent. Anesthesiology 104:556–569
33. Haddad F, Couture P, Tousignant C, Denault AY (2009) The
right ventricle in cardiac surgery, a perioperative perspective: II.
Pathophysiology, clinical importance, and management. Anesth
Analg 108:422–433
34. Vlahakes GJ (2005) Right ventricular failure following cardiac
surgery. Coron Artery Dis 16:27–30
35. Imren Y, Tasoglu I, Oktar GL, Benson A, Naseem T et al (2008)
The importance of transesophageal echocardiography in diagno-
sis of pericardial tamponade after cardiac surgery. J Card Surg
23:450–453
36. Kuvin JT, Harati NA, Pandian NG, Bojar RM, Khabbaz KR
(2002) Postoperative cardiac tamponade in the modern surgical
era. Ann Thorac Surg 74:1148–1153
37. Bommer WJ, Follette D, Pollock M, Arena F, Bognar M et al
(1995) Tamponade in patients undergoing cardiac surgery: a
clinical-echocardiographic diagnosis. Am Heart J 130:1216–1223
38. Weitzman LB, Tinker WP, Kronzon I, Cohen ML, Glassman E
et al (1984) The incidence and natural history of pericardial
effusion after cardiac surgery—an echocardiographic study.
Circulation 69:506–511
39. Hirose H, GuptaS Pitcher H, Miessau J, Yang Q et al (2014)
Feasibility of diagnosis of postcardiotomy tamponade by minia-
turized transesophageal echocardiography. J Surg Res
190:27276–27279
40. Cholley BP, Vieillard-Baron A, Mebazaa nA (2006) Echocar-
diography in the ICU: time for widespread use! Intensive Care
Med 32:9–10
41. Manasia AR, Nagaraj HM, Kodali RB, Croft LB, Oropello JM
et al (2005) Feasibility and potential clinical utility of goal-di-
rected transthoracic echocardiography performed by noncardiol-
ogist intensivists using a small hand-carried device (SonoHeart)
in critically ill patients. J Cardiothorac Vasc Anesth 19:155–159
42. Jensen MB, Sloth E, Larsen KM, Schmidt MB (2004)
Transthoracic echocardiography for cardiopulmonary monitoring
in intensive care. Eur J Anaesthesiol 21:700–707
43. Kaul S, Stratienko AA, Pollock SG, Marieb MA, Keller MW et al
(1994) Value of two-dimensional echocardiography for deter-
mining the basis of hemodynamic compromise in critically ill
patients: a prospective study. J Am Soc Echocardiogr 7:598–606
44. Wittkowski U, Spies C, Sander M, Erb J, Feldheiser A et al
(2009) Haemodynamic monitoring in the perioperative phase.
Available systems, practical application and clinical data. Der
Anaesthesist 58(764–778):780–786
45. Habicher M, Perrino A Jr, Spies CD, von Heymann C, Wit-
tkowski U et al (2011) Contemporary fluid management in car-
diac anesthesia. J Cardiothorac Vasc Anesth 25:1141–1153
46. Ostergaard M, Nilsson LB, Nilsson JC, Rasmussen JP, Berthelsen
PG (2005) Precision of bolus thermodilution cardiac output
measurements in patients with atrial fibrillation. Acta Anaesthe-
siol Scand 49:366–372
47. Balik M, Pachl J, Hendl J (2002) Effect of the degree of tricuspid
regurgitation on cardiac output measurements by thermodilution.
Intensive Care Med 28:1117–1121
48. Wyler von Ballmoos M, Takala J, Roeck M, Porta F, Tueller D
et al (2010) Pulse-pressure variation and hemodynamic response
in patients with elevated pulmonary artery pressure: a clinical
study. Crit Care 14:R111
49. Ranucci M, Pazzaglia A, Tritapepe L, Guarracino F, Lupo M et al
(2009) Fluid responsiveness and right ventricular function in
cardiac surgical patients. A multicenter study. HSR Proc Inten-
sive Care Cardiovasc Anesth 1:21–29
50. Zhang Z, Ni H, Qian Z (2015) Effectiveness of treatment based
on PiCCO parameters in critically ill patients with septic shock
and/or acute respiratory distress syndrome: a randomized con-
trolled trial. Intensive Care Med 41:444–451
51. Boulain T, Cecconi M (2015) Can one size fit all? The fine line
between fluid overload and hypovolemia. Intensive Care Med
41:544–546
Int J Cardiovasc Imaging (2015) 31:1327–1335 1335
123