Embed Size (px)
Citation preview
FDA Blood Products Advisory Committee 95th Meeting 21 July 2009
Update: 21st MeetingFDA Transmissible Spongiform Encephalopathies
Advisory Committee (TSEAC)12 June 2009
Recent Events Related to TSEs:Implications for Safety of Human Blood, Blood
Components and Plasma Derivatives
David M. Asher, MD
<[email protected]>Laboratory of Bacterial, Parasitic &
Unconventional AgentsDivision of Emerging & Transfusion-Transmitted
DiseasesOffice of Blood Research & Review
Center for Biologics Evaluation & ResearchUS Food & Drug Administration
2
UK Health Protection Agency17 February 2009
http://www.hpa.org.uk/webw/HPAweb&HPAwebStandard/HPAweb_C/1234859690542?p=1231252394302
see also HPA publication 09 June 2009http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_100357
CJD abnormal protein found in a patient with haemophilia at post mortem
“Evidence of infection with the agent (abnormal prion protein) that causes variant Creutzfeldt-Jakob disease (vCJD) has been found at post mortem in the spleen of a person with haemophilia [treated 11 yr earlier with UK “vCJD-implicated” pdFVIII].
The patient, who was over 70 years old, died of a condition unrelated to vCJD and had shown no symptoms of vCJD or any other neurological condition prior to his death. The vCJD abnormal protein was only identified during post mortem research tests. …
What was until now a theoretical risk may be an actual risk to certain individuals …”
3
Bovine spongiform encephalopathy (BSE)─ Accepted as source of food-borne vCJD─ Recent worldwide trends show decline in reported
cases─ Uncertainties (some at-risk countries did not report cases)
vCJD─ Recent trends
Declining cases in UK (PRNP-codon-129 MM clinical cases) Possible “second wave” (PRNP-codon-129 VV, MV: ?1st
case) Marked discrepancy in UK prevalence estimates from
1) lymphoid tissue survey of abnormal prion protein (PrPTSE) vs
2) case-based projections
─ Transfusion transmission (TT) of vCJD by RBC in UK 4 TT vCJD infections attributed to non-leukoreduced RBC No new report of TT vCJD since 2007
Presumptive transmission of vCJD by UK plasma derivative: reason for TSEAC meeting
4
TSEAC Meeting AgendaTransmission by plasma derivative:
implications for safety of US plasma derived factor VIII and von Willebrand factor. Review of modified FDA Risk Assessment (decisional issue)
BSE worldwide: US, Canadian and European regulatory responses (informational)
3 research topics related to TSEs and blood safety (informational):
─ Monkey model for BSE and vCJD infectivity in blood
─ Efforts to develop antemortem tests for identifying subjects during TSE incubation period
─ Problems in correlating abnormal prion protein and TSE agent infectivity
5
FDA TSEAC 21st Meeting Agenda 12 June 2009Decisional Issue:
Modified FDA Risk Assessment for Potential Exposure to vCJD Agent in US-licensed pdFVIII and vW factor
1. vCJD in UK, TMER. RG Will, UK CJD Surveillance Unit, Edinburgh
2. FDA vCJD geographic deferral guidance. A Williams, FDA CBER OBRR
3. Plasma derivatives, TSE agents and their clearance. D Scott, FDA CBER OBRR
4. Studies of TSE agent clearance by steps in the manufacture of plasma derivatives. A Gröner, (CSL Behring) PPTA
5. Modified FDA Risk Assessment for pdFVIII and von Willebrand factor. S Anderson, FDA CBER OBE
Open public hearing TSEAC discussions Vote on questions
6
FDA TSEAC 21st Meeting Agenda 12 June 2009Informational Presentations
1. US BSE surveillance, USDA and beef safety, OIE and BSE. JA Hughes, USDA APHIS
2. BSE in Europe. M Plantady, European Commission, Brussels
3. BSE in Canada. N Murray, Canadian Food Safety Inspection Agency, Ottawa
4. FDA BSE enhanced animal feed safety rule. B Pritchett, FDA CVM
5. FDA interim final food safety rule. A McGoig FDA CFSAN6. FDA proposed BSE medical products rule. T Finn, FDA
CBER OVRR7. Primate model of BSE and vCJD infectivity in blood. E
Comoy, Commissariat à l’Énergie Atomique, France8. Progress in developing antemortem TSE detection tests. L
Gregori, FDA CBER OBRR9. PrPTSE and TSE infectivity. P Piccardo, FDA CBER OBRR Discussion, open public hearing
7
Questions for TSEAC
Based on an updated risk assessment, FDA continues to believe that the risk of variant Creutzfeldt-Jakob disease (vCJD) to patients who receive US-licensed plasma-derived coagulation factor VIII (pdFVIII) products is likely to be extremely small, although we do not know the risk with certainty.
1. Does the Committee agree with the updated and new inputs to the FDA risk assessment model for US-licensed plasma-derived pdFVIII?
Updated inputs a. Estimated prevalence of UK vCJD infectionsb. Age at time of infectionc. Time during incubation period when infectivity is present in
blood New inputs
d. Genotype at PRNP codon 129: genetic susceptibility to vCJD infection and genotype proportions in US population
e. Distributions of vCJD incubation periods for persons of different PRNP-129 genotypes
f. Age distribution of persons with asymptomatic vCJD infections
8
Questions for TSEAC (continued)
2. Original question: Despite the finding of minimal additional risk in FDA’s
modified risk assessment, should the recent report from the UK Health Protection Agency, attributing a case of vCJD infection to treatment 11 years earlier with a “vCJD-implicated” pdFVIII, alter FDA’s interpretation of the risk for US-licensed preparations of pdFVIII?
Question modified during meeting: (responding to recent analysis concluding vCJD infection was much less likely from exposures to food, red blood cell transfusions or endoscopy but—considering probable prevalence of pre-clinical vCJD in UK plasma donors—at least as likely to have resulted from treatments with non-vCJD-implicated pdFVIII):
Despite the finding of minimal additional risk in FDA’s modified risk assessment, should the recent report from the UK Health Protection Agency, attributing a case of vCJD infection to treatment with UK-sourced pdFVIII, alter FDA’s interpretation of the risk for US-licensed preparations of pdFVIII?
9
Questions for TSEAC (continued)
3. Based on the available information, should FDA consider:
a. Recommending additional risk-reducing steps for manufacture of plasma derivatives (e.g., modifications to current donor deferral policies)?
b. Recommending revised warning labels for plasma derivatives?
c. Recommending modifications to FDA’s public communications (e.g., to Web postings) regarding the risk of vCJD associated with the use of FDA-licensed plasma derivatives?
10
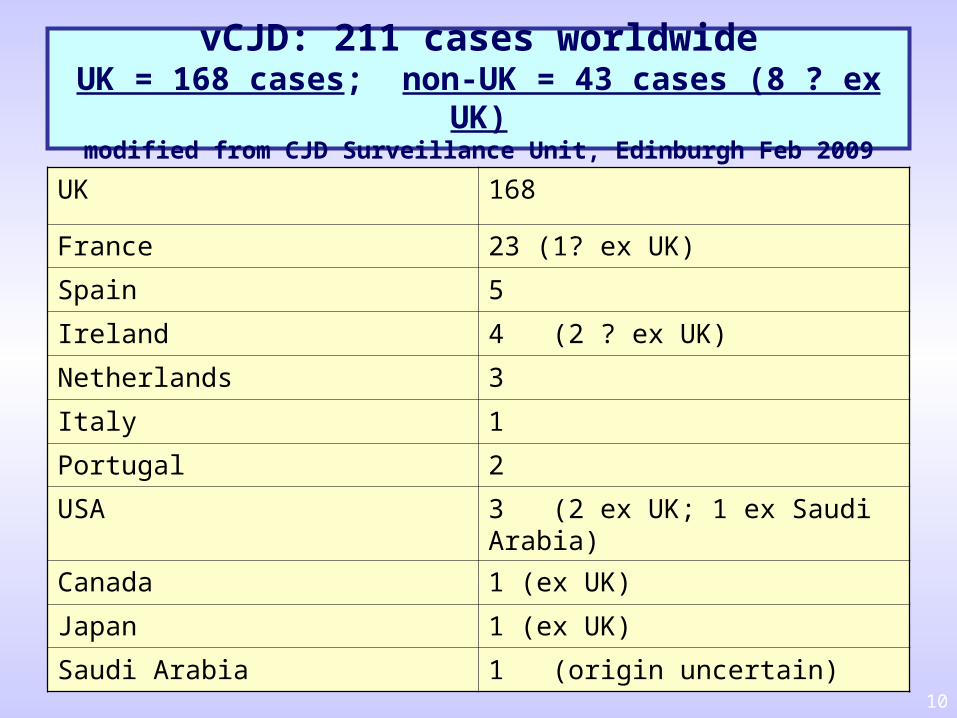
vCJD: 211 cases worldwideUK = 168 cases; non-UK = 43 cases (8 ? ex UK)
modified from CJD Surveillance Unit, Edinburgh Feb 2009
UK 168
France 23 (1? ex UK)
Spain 5
Ireland 4 (2 ? ex UK)
Netherlands 3
Italy 1
Portugal 2
USA 3 (2 ex UK; 1 ex Saudi Arabia)
Canada 1 (ex UK)
Japan 1 (ex UK)
Saudi Arabia 1 (origin uncertain)
11
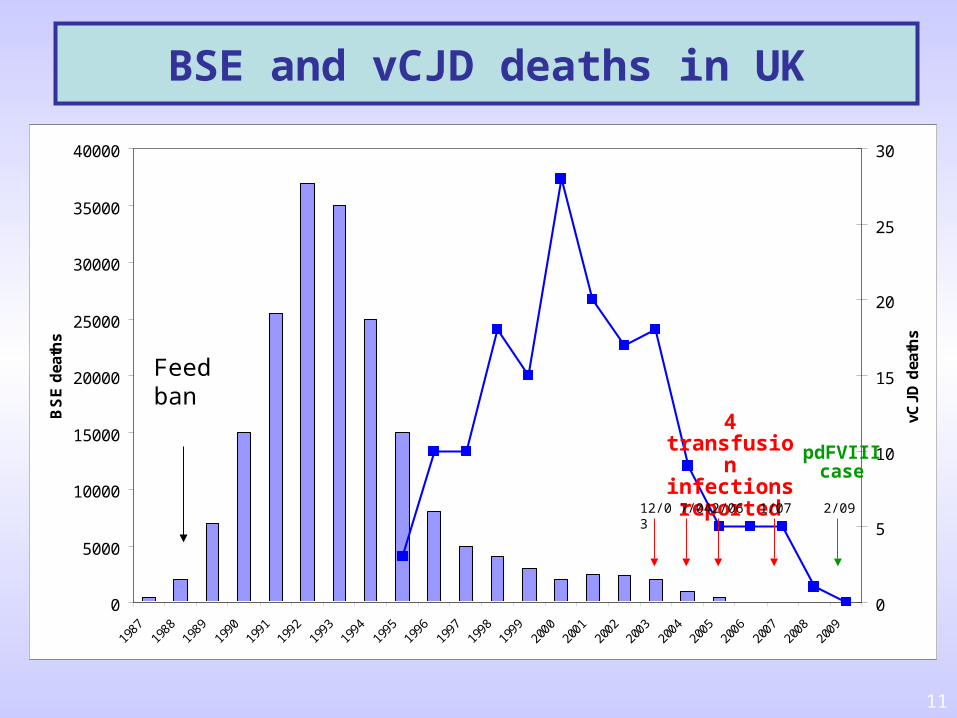
BSE and vCJD deaths in UK
0
5000
10000
15000
20000
25000
30000
35000
40000
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
BS
E d
eath
s
0
5
10
15
20
25
30
vCJD
dea
ths
Feedban
4 transfusion infections reported
pdFVIII case
12/03 7/04 2/06 1/07 2/09
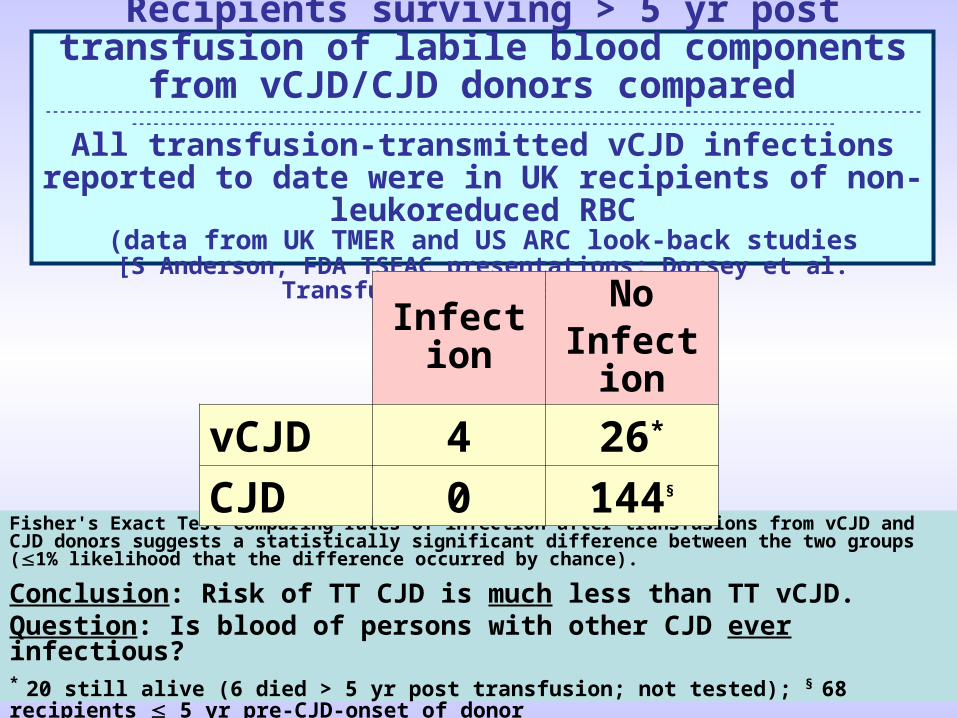
Recipients surviving > 5 yr post transfusion of labile blood components
from vCJD/CJD donors compared ----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
------------------------------------------
All transfusion-transmitted vCJD infections reported to date were in UK recipients of non-
leukoreduced RBC(data from UK TMER and US ARC look-back studies
[S Anderson, FDA TSEAC presentations; Dorsey et al. Transfusion 2009;49:977-84])
Fisher's Exact Test comparing rates of infection after transfusions from vCJD and CJD donors suggests a statistically significant difference between the two groups (1% likelihood that the difference occurred by chance).
Conclusion: Risk of TT CJD is much less than TT vCJD.Question: Is blood of persons with other CJD ever infectious?* 20 still alive (6 died > 5 yr post transfusion; not tested); § 68 recipients 5 yr pre-CJD-onset of donor
InfectionNo
Infection
vCJD 4 26*
CJD 0 144§
13
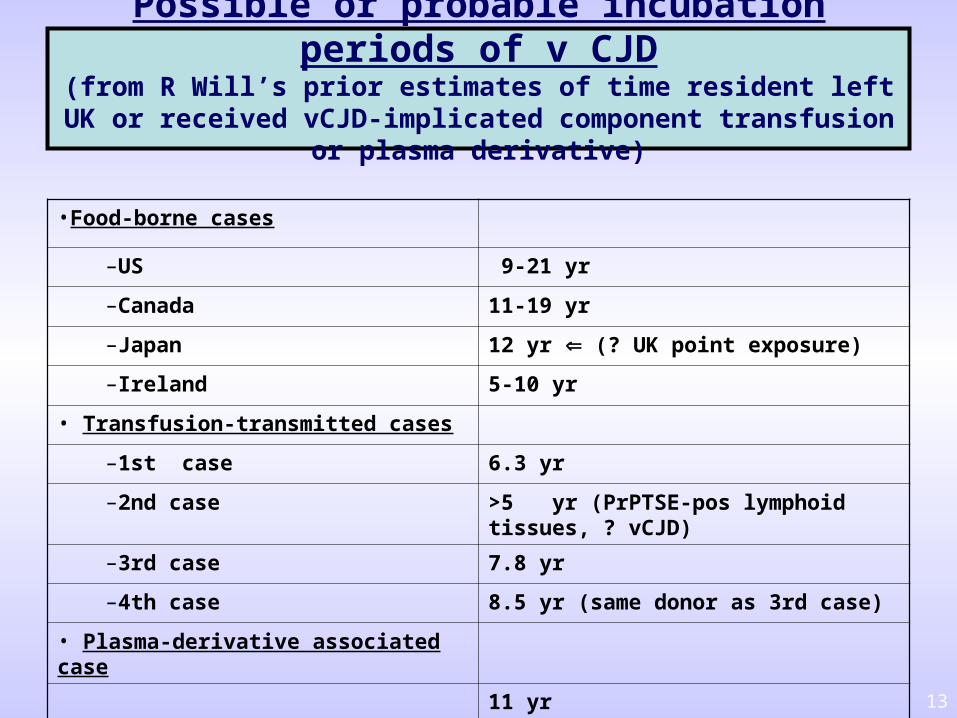
Possible or probable incubation periods of v CJD(from R Will’s prior estimates of time resident left UK or received vCJD-
implicated component transfusion or plasma derivative)
•Food-borne cases
–US 9-21 yr
–Canada 11-19 yr
–Japan 12 yr (? UK point exposure)
–Ireland 5-10 yr
• Transfusion-transmitted cases
–1st case 6.3 yr
–2nd case >5 yr (PrPTSE-pos lymphoid tissues, ? vCJD)
–3rd case 7.8 yr
–4th case 8.5 yr (same donor as 3rd case)
• Plasma-derivative associated case
11 yr
14
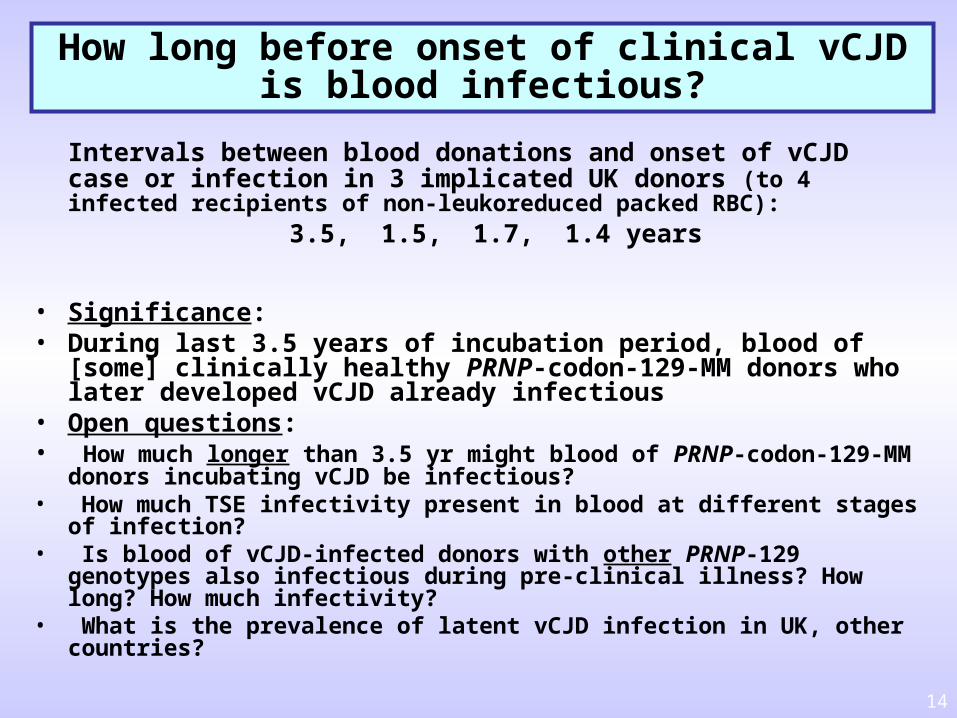
How long before onset of clinical vCJDis blood infectious?
Intervals between blood donations and onset of vCJD case or infection in 3 implicated UK donors (to 4 infected recipients of non-leukoreduced packed RBC):
3.5, 1.5, 1.7, 1.4 years
• Significance:• During last 3.5 years of incubation period, blood of [some]
clinically healthy PRNP-codon-129-MM donors who later developed vCJD already infectious
• Open questions:• How much longer than 3.5 yr might blood of PRNP-codon-129-MM donors
incubating vCJD be infectious?• How much TSE infectivity present in blood at different stages of
infection?• Is blood of vCJD-infected donors with other PRNP-129 genotypes also
infectious during pre-clinical illness? How long? How much infectivity?• What is the prevalence of latent vCJD infection in UK, other countries?
15
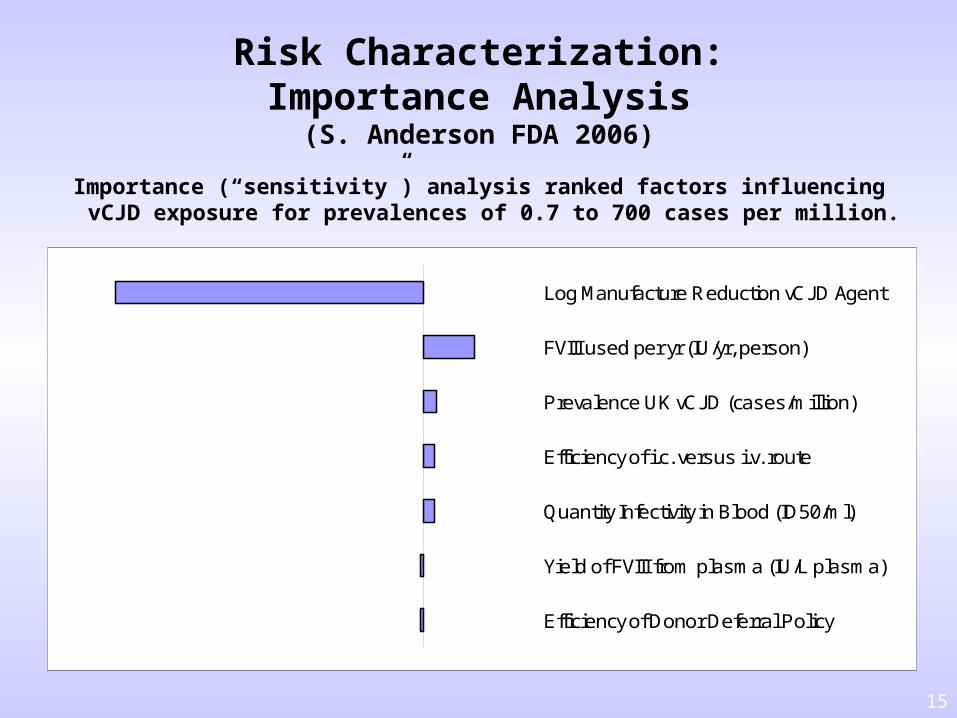
Risk Characterization:Importance Analysis
(S. Anderson FDA 2006)
Importance (“sensitivity”) analysis ranked factors influencing vCJD exposure for prevalences of 0.7 to 700 cases per million.
Efficiency of Donor Deferral Policy
Yield of FVIII from plasma (IU/L plasma)
Quantity Infectivity in Blood (ID50/ml)
Efficiency of i.c. versus i.v. route
Prevalence UK vCJD (cases/million)
FVIII used per yr (IU/yr, person)
Log Manufacture Reduction vCJD Agent
16
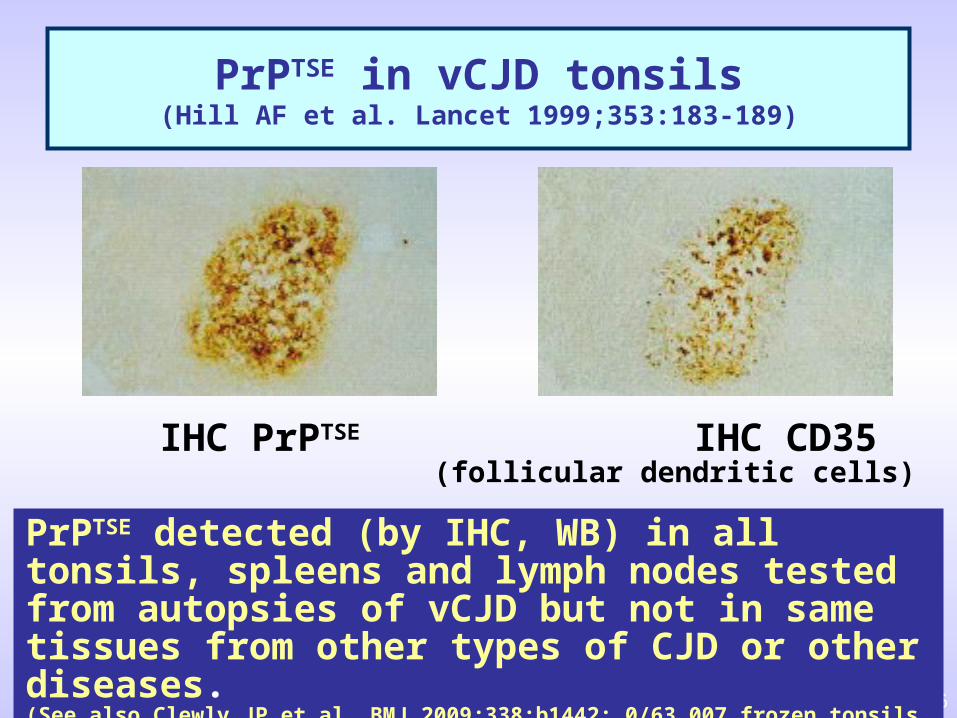
PrPTSE in vCJD tonsils(Hill AF et al. Lancet 1999;353:183-189)
IHC PrPTSE IHC CD35 (follicular dendritic cells)
PrPTSE detected (by IHC, WB) in all tonsils, spleens and lymph nodes tested from autopsies of vCJD but not in same tissues from other types of CJD or other diseases.(See also Clewly JP et al. BMJ 2009;338:b1442: 0/63,007 frozen tonsils confirmed PrPTSE-positive)
17
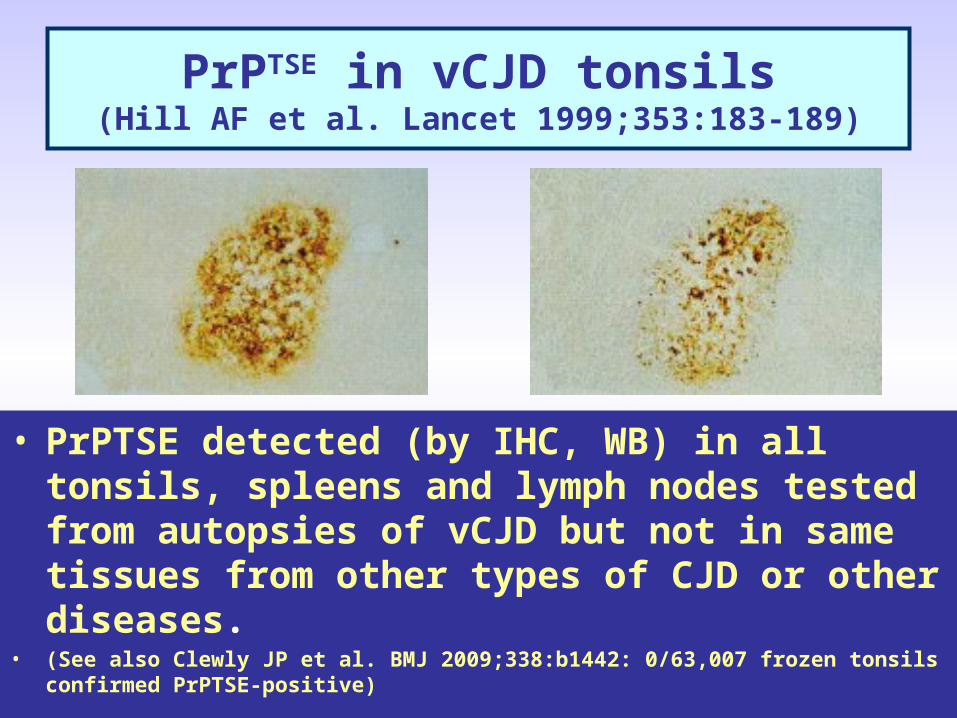
PrPTSE in vCJD tonsils(Hill AF et al. Lancet 1999;353:183-189)
• PrPTSE detected (by IHC, WB) in all tonsils, spleens and lymph nodes tested from autopsies of vCJD but not in same tissues from other types of CJD or other diseases.
• (See also Clewly JP et al. BMJ 2009;338:b1442: 0/63,007 frozen tonsils confirmed PrPTSE-positive)
18
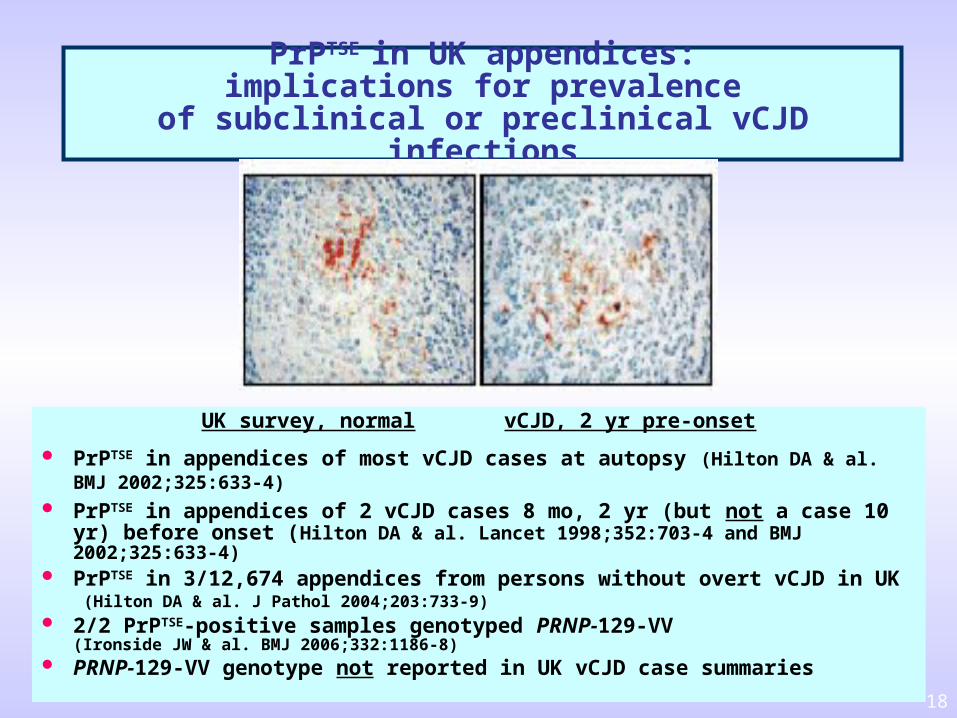
PrPTSE in UK appendices:implications for prevalence
of subclinical or preclinical vCJD infections
UK survey, normal vCJD, 2 yr pre-onset
PrPTSE in appendices of most vCJD cases at autopsy (Hilton DA & al. BMJ 2002;325:633-4)
PrPTSE in appendices of 2 vCJD cases 8 mo, 2 yr (but not a case 10 yr) before onset (Hilton DA & al. Lancet 1998;352:703-4 and BMJ 2002;325:633-4)
PrPTSE in 3/12,674 appendices from persons without overt vCJD in UK(Hilton DA & al. J Pathol 2004;203:733-9)
2/2 PrPTSE-positive samples genotyped PRNP-129-VV (Ironside JW & al. BMJ 2006;332:1186-8) PRNP-129-VV genotype not reported in UK vCJD case summaries
19
PPTA: Prion Reduction Capacity pdFVIII - TSEAC 120609 19
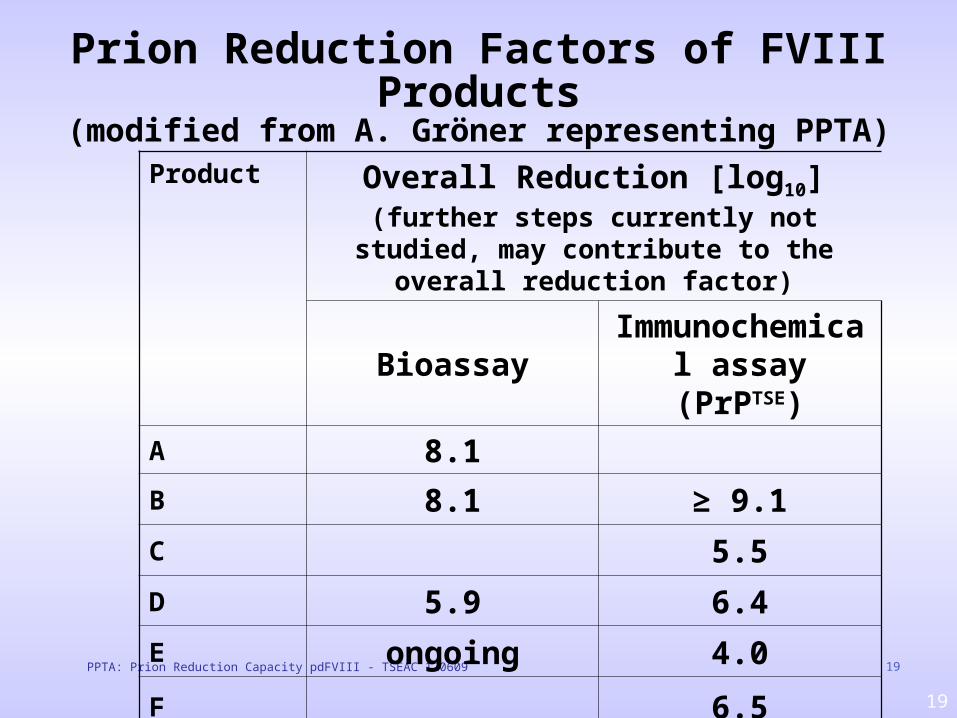
Prion Reduction Factors of FVIII Products(modified from A. Gröner representing PPTA)
Product Overall Reduction [log10](further steps currently not studied, may contribute to the overall reduction factor)
BioassayImmunochemi
cal assay (PrPTSE)
A 8.1B 8.1 ≥ 9.1C 5.5D 5.9 6.4E ongoing 4.0F 6.5
20
Summary(modified from A. Gröner representing PPTA)
• Manufacturing processes of plasma-derived FVIII products remove prions reduction factors of at least 4 log10 were
demonstrated [for all US-licensed products]
• PPTA members are not using UK [or other European] plasma [for manufacturing US-licensed plasma-derivative products]
Appropriate donor deferral procedures in place
PPTA: Prion Reduction Capacity pdFVIII - TSEAC 120609
21
PPTA Conclusion(modified from A. Gröner representing PPTA)
Recent report from UK Health Protection Agency regardingpatient with haemophilia has no bearing on the safety profileof products manufactured by PPTA members.
• The implicated product 8Y sourced from UK plasma • Public statement on low prion clearance capacity of 8Y
product (UK “vCJD-implicated product [assessment by Det Norske Veritas 2003])
Industry continues to be committed to research.
PPTA: Prion Reduction Capacity pdFVIII - TSEAC 120609
22
FDA Assessment of Possible Risks for Plasma-derived
Products in the US12 June 2009 21st TSEAC Meeting
Gaithersburg, MD
Steve Anderson, PhD, MPPwith
Hong Yang, PhDRichard Forshee, PhD
Mark Walderhaug, PhDOffice of Biostatistics and Epidemiology
FDA Center for Biologics Evaluation & Research
23
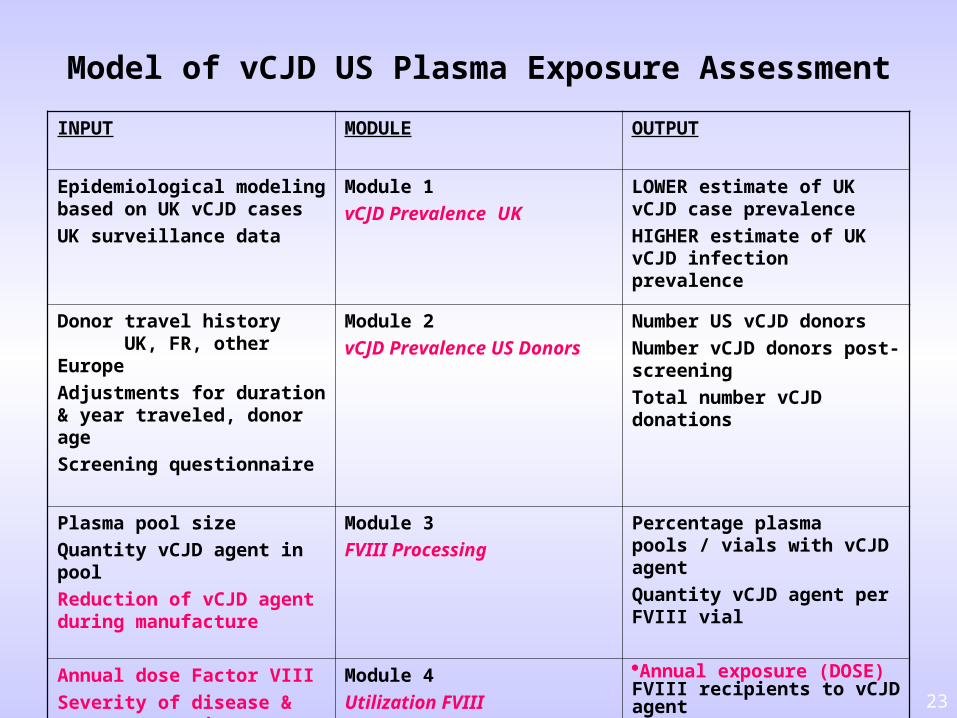
Model of vCJD US Plasma Exposure Assessment
INPUT MODULE OUTPUT
Epidemiological modeling based on UK vCJD cases
UK surveillance data
Module 1
vCJD Prevalence UK
LOWER estimate of UK vCJD case prevalence
HIGHER estimate of UK vCJD infection prevalence
Donor travel history UK, FR, other Europe
Adjustments for duration & year traveled, donor age
Screening questionnaire
Module 2
vCJD Prevalence US Donors
Number US vCJD donors
Number vCJD donors post-screening
Total number vCJD donations
Plasma pool size
Quantity vCJD agent in pool
Reduction of vCJD agent during manufacture
Module 3
FVIII Processing
Percentage plasma pools / vials with vCJD agent
Quantity vCJD agent per FVIII vial
Annual dose Factor VIII
Severity of disease & treatment regimen
Module 4
Utilization FVIII
Annual exposure (DOSE) FVIII recipients to vCJD agent
24
FDA has updated the pdFVIII-vCJD Risk Assessment from 2006
pdFVIII-vCJD Risk Assessment in 2009 incorporates new data suggesting susceptibility of entire population to vCJD infection and includes:
Three UPDATED inputs (added to Modules 1 and 2 of model)1. Estimation of UK vCJD prevalence (1)2. UK vCJD ages at time of infection (1)3. Time during incubation period when infectivity present in blood (2)75%
Three NEW inputs (added to Module 2 of model)4. Genotype susceptibility and genotype proportion in population 5. Distribution of incubation periods 6. Age distribution of asymptomatic infections
25
FDA vCJD Plasma-Derivative Risk Assessment:Scope and type of assessment
Scope of FDA pdFVIII Risk Assessment• Estimates potential vCJD risk for US pdFVIII recipients
– Severe Hemophilia A– Severe von Willebrand disease (Type 3)
• Potential vCJD risk estimated for 1 yr treatment (2002)
Analytic Approach • Quantitative risk assessment (QRA) • Input data usually statistical distributions• Probabilistic computer-based model• Monte Carlo methods
26
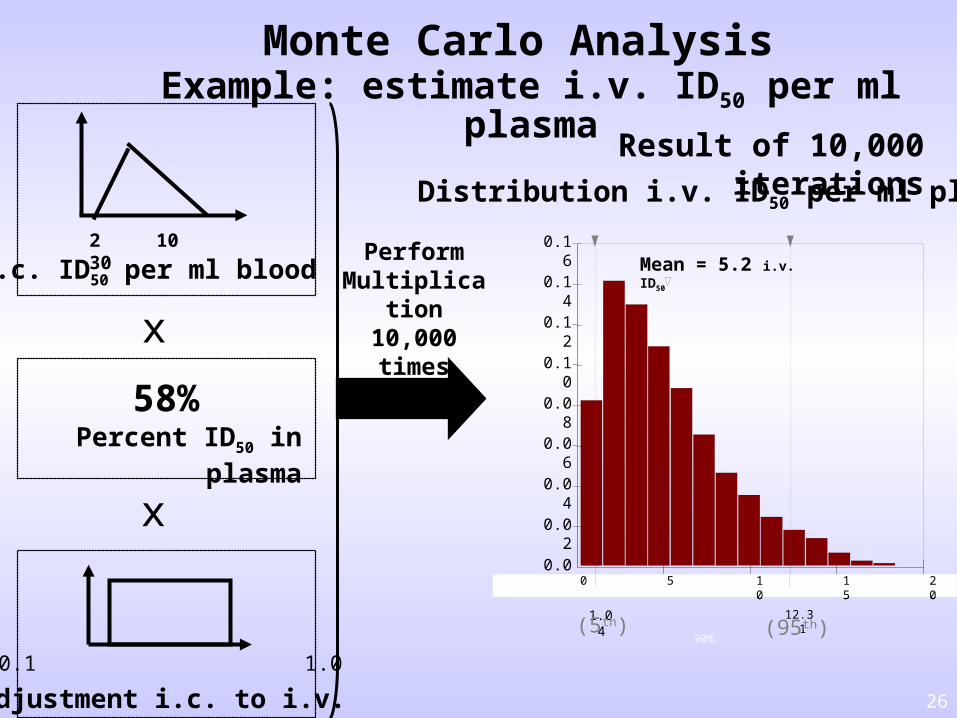
Monte Carlo Analysis Example: estimate i.v. ID50 per ml plasma
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
0.16
0 5 10
15
20
0 5 10
15
20
90%
1.04
12.31
Adjustment i.c. to i.v.
Distribution i.v. ID50 per ml plasma
Percent ID50 in plasma
Mean = 5.2 i.v. ID50
2 10 30
0.1 1.0
58%
i.c. ID50 per ml blood
x
x
Perform Multiplication
10,000times
Result of 10,000 iterations
(5th) (95th)
27
Exposure Assessment: Module 1Prevalence of vCJD in United Kingdom
A. Epidemiological modeling vCJD cases (LOWER estimate)from Clarke and Ghani 2005
FDA modeling estimated a vCJD prevalence of:
~1.8 per million UK population (2006) ~4.5 per million UK population (2009)
B. Tonsil/appendix tissue surveillance in UK patients (HIGHER estimate)
Hilton et al. 2004 3 PrPTSE-positive samples in UK 12,674 samples tested by
immunohistochemistry Mean of 1 positive in 4,225 individuals, or 237 per million
GOAL: Estimate UK prevalence; use to estimate vCJD prevalence for France, other W Europe, US military bases in Europe plasma donors in US
28
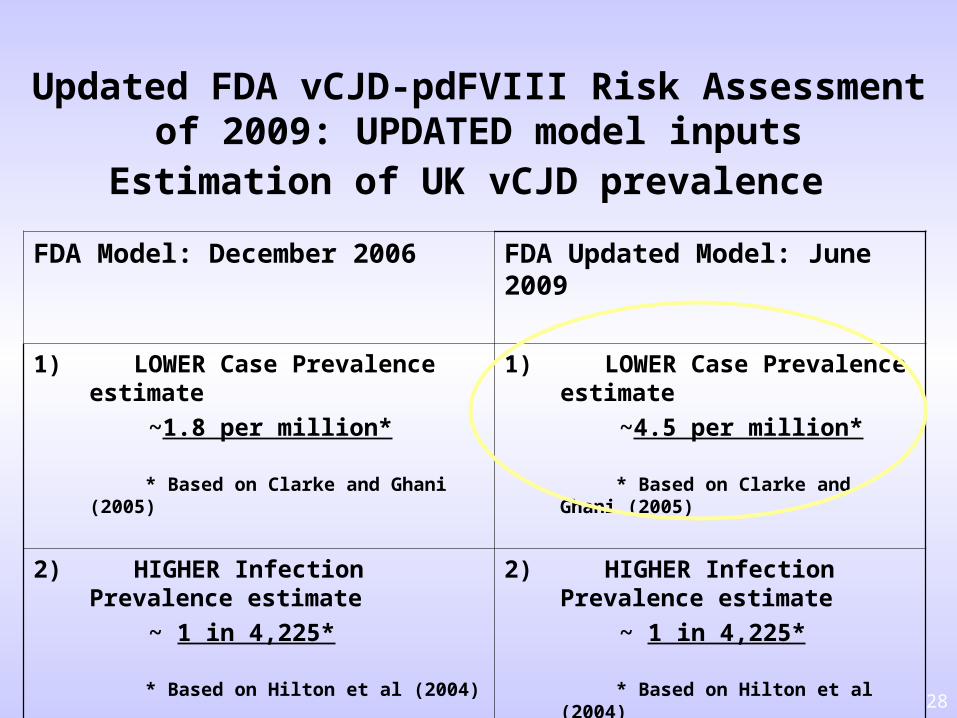
Updated FDA vCJD-pdFVIII Risk Assessment of 2009: UPDATED model inputs
Estimation of UK vCJD prevalence
FDA Model: December 2006 FDA Updated Model: June 2009
1) LOWER Case Prevalence estimate
~1.8 per million*
* Based on Clarke and Ghani (2005)
1) LOWER Case Prevalence estimate
~4.5 per million*
* Based on Clarke and Ghani (2005)
2) HIGHER Infection Prevalence estimate
~ 1 in 4,225*
* Based on Hilton et al (2004)
2) HIGHER Infection Prevalence estimate
~ 1 in 4,225*
* Based on Hilton et al (2004)
29
Exposure Assessment: Module 2 vCJD prevalence in US plasma donors (cont.)
Model considers effectiveness of US donor deferral policy (risk reduction measure)
Model assumes mean elimination of 92% vCJD risk (range: 85-99%) for US donors by current donor deferral policy for travel:
UK: 1980-1996, > 3 mos France: since 1980, > 5 years Other Europe: since 1980, > 5 years
(recovered plasma donors only) US military bases in Europe: 1980-1996
30
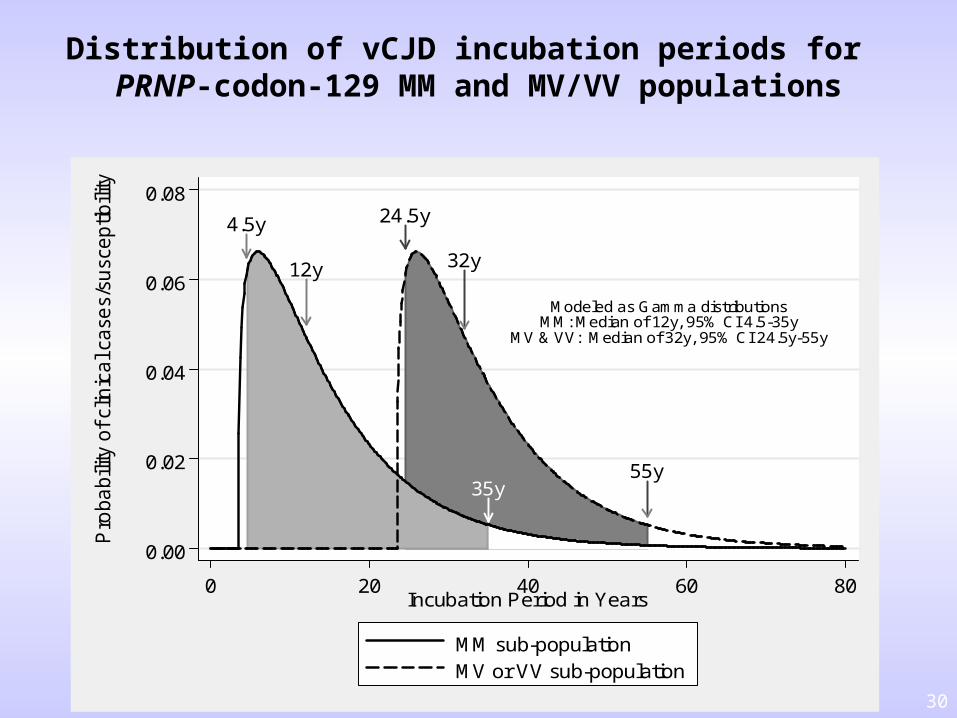
Distribution of vCJD incubation periods for PRNP-codon-129 MM and MV/VV populations
4.5y
12y
35y
24.5y
32y
55y
Modeled as Gamma distributionsMM: Median of 12y, 95% CI 4.5-35y
MV & VV: Median of 32y, 95% CI 24.5y-55y
0.00
0.02
0.04
0.06
0.08
Pro
ba
bili
ty o
f cl
inic
al c
ase
s/su
scep
tibili
ty
0 20 40 60 80Incubation Period in Years
MM sub-populationMV or VV sub-population
31
Exposure Assessment: Module 3
Factor VIII Processing
Modeling Approach for Module 3 Estimate probability plasma pool contains vCJD
donation(s) Estimate quantity vCJD ID50 per ml plasma, per pool Estimate log10 reduction in quantity of i.v. ID50
resulting from manufacturing process Adjust for “efficiency” of exposure by i.v. vs i.c. route
GOALEstimate: Percentage of pdFVIII vials containing vCJD agent Quantity vCJD agent per vial
32
Infectivity clearance from product plasma pools: problems Each product has different purification steps clearance Product-specific data: not available for all products Published data: not available for all purification steps; studies vary
FDA believes most (probably all) US-licensed pdFVIII ismanufactured by processes 4 log10 clearance.
FDA model stratified by 2 estimated
clearance levels: 7-9
log10 and 4-6 log10
Exposure Assessment: Module 3Factor VIII Processing (cont.)
33
Exposure Assessment: Module 4Utilization of Factor VIII
Inputs Percentage vials with vCJD agent Quantity vCJD agent per vial Annual utilization / doses of Factor VIII per patient
GOALSPredict: Annual potential dose vCJD ID50 per patient Risk of vCJD infection based on animal dose-response
information
34
Exposure Assessment: Module 4Utilization of FVIII
Factors considered for utilization─ Type of disease:
Severe Hemophilia A, Severe von Willebrand disease (vWD) (Type 3)
─ Treatment regimens: Prophylaxis or Episodic Treatment
─ Presence of FVIII inhibitor and immune tolerance
Data─ CDC estimated size of HA and vWD populations
─ CDC sponsored a 6-state hemophilia surveillance study, 1993-1998 (total records: 17,848) estimating product usage
35
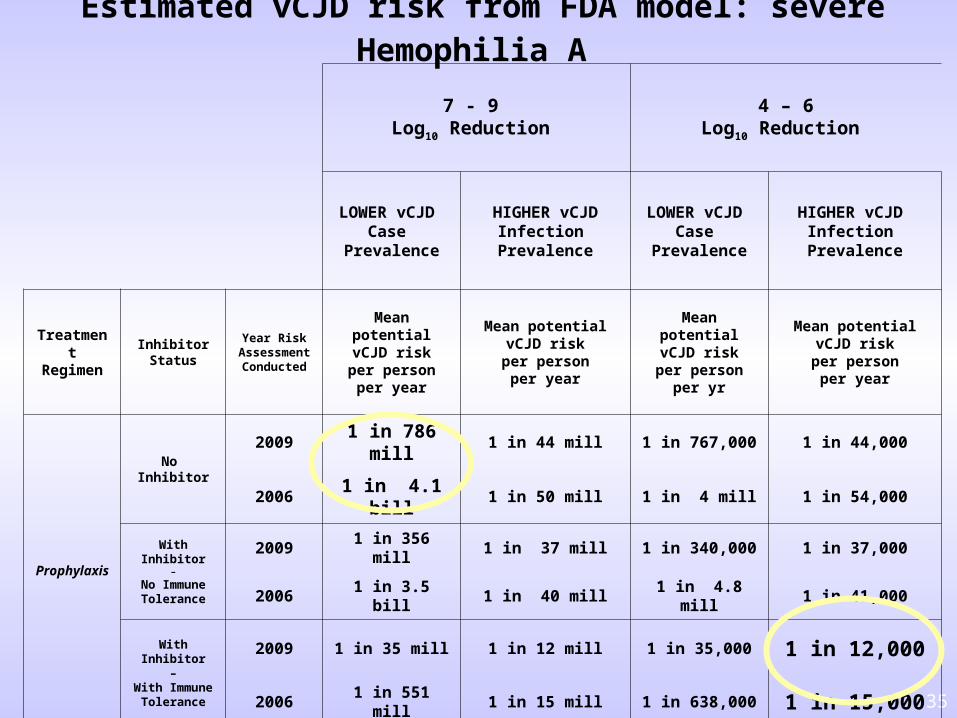
Estimated vCJD risk from FDA model: severe Hemophilia A
7 - 9 Log10 Reduction
4 – 6Log10 Reduction
LOWER vCJD Case
Prevalence
HIGHER vCJD Infection
Prevalence
LOWER vCJD Case
Prevalence
HIGHER vCJD Infection
Prevalence
TreatmentRegimen
InhibitorStatus
Year Risk Assessment Conducted
Mean potentialvCJD riskper person
per year
Mean potentialvCJD riskper person
per year
Mean potentialvCJD riskper person
per yr
Mean potentialvCJD riskper person
per year
Prophylaxis
No Inhibitor
2009 1 in 786 mill 1 in 44 mill 1 in 767,000 1 in 44,000
2006 1 in 4.1 bill 1 in 50 mill 1 in 4 mill 1 in 54,000
With Inhibitor–
No Immune Tolerance
2009 1 in 356 mill 1 in 37 mill 1 in 340,000 1 in 37,000
2006 1 in 3.5 bill 1 in 40 mill 1 in 4.8 mill 1 in 41,000
With Inhibitor–
With Immune Tolerance
2009 1 in 35 mill 1 in 12 mill 1 in 35,000 1 in 12,000
2006 1 in 551 mill 1 in 15 mill 1 in 638,000 1 in 15,000
36
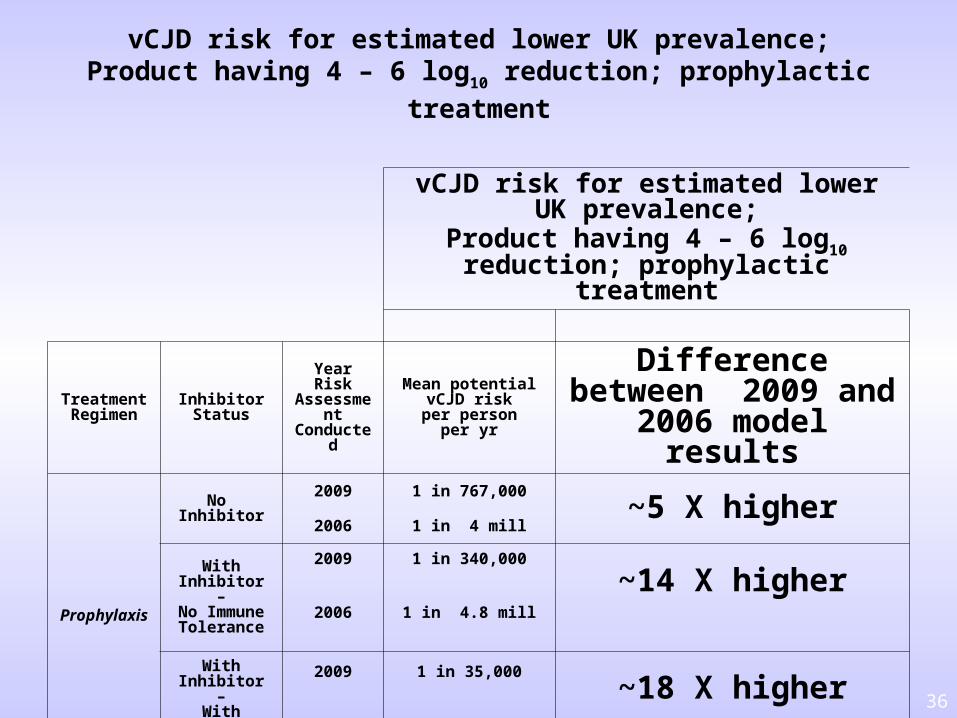
vCJD risk for estimated lower UK prevalence;Product having 4 – 6 log10 reduction; prophylactic treatment
vCJD risk for estimated lower UK prevalence;
Product having 4 – 6 log10 reduction; prophylactic treatment
TreatmentRegimen
InhibitorStatus
Year Risk Assessment Conducted
Mean potentialvCJD riskper person
per yr
Differencebetween 2009 and 2006
model results
Prophylaxis
No Inhibitor
2009 1 in 767,000~5 X higher
2006 1 in 4 mill
With Inhibitor–
No Immune Tolerance
2009 1 in 340,000
~14 X higher2006 1 in 4.8 mill
With Inhibitor–
With Immune Tolerance
2009 1 in 35,000~18 X higher
2006 1 in 638,000
37
Conclusions (interim: work in progress)
Updates to FDA 2009 model accounting for susceptibility of entire population have not caused important changes between the vCJD risk estimates for 2006 and 2009.
Results from the model indicate estimates of potential vCJD risk for 2009:─ Increased using a LOWER vCJD prevalence estimate by
approximately 5-fold to 18-fold─ However, results using a HIGHER vCJD prevalence were similar
to estimates from 2006 Does not substantially change FDA’s interpretation of risk
since the 2006 estimate was based on the HIGHER vCJD prevalence
Accordingly, as in 2006, FDA assumes current vCJD risk from use of US-licensed pdFVIII may not be zero but is most likely extremely small.
38
Questions for TSEAC Based on an updated risk assessment, FDA continues to believe that the risk of
variant Creutzfeldt-Jakob disease (vCJD) to patients who receive US-licensed plasma-derived coagulation factor VIII (pdFVIII) products is likely to be extremely small, although we do not know the risk with certainty.
1. Does the Committee agree with the updated and new inputs to the FDA risk assessment model for US-licensed plasma-derived pdFVIII?
Discussion: No disagreement (other improvements to model suggested).2. Despite finding minimal additional risk in FDA’s modified assessment,
should the recent report from the UK HPA, attributing a case of vCJD infection to treatment with UK-sourced pdFVIII, alter FDA’s interpretation of the risk for US-licensed preparations of pdFVIII?
Vote: Unanimous No (15 votes)—i.e., no changes suggested
3. Based on the available information, should FDA consider recommending:a. Additional risk-reducing steps for manufacture of plasma derivatives? Discussion: Encourage processes that clear more spiked TSE agent.b. Revised warning labels for plasma derivatives? Discussion: Yes (vCJD no longer just “theoretical” risk for pdFVIII)c. Modifications to FDA’s public communications about risk of vCJD
for FDA-licensed plasma derivatives? Discussion: Yes (include reference to case reported in UK)
39
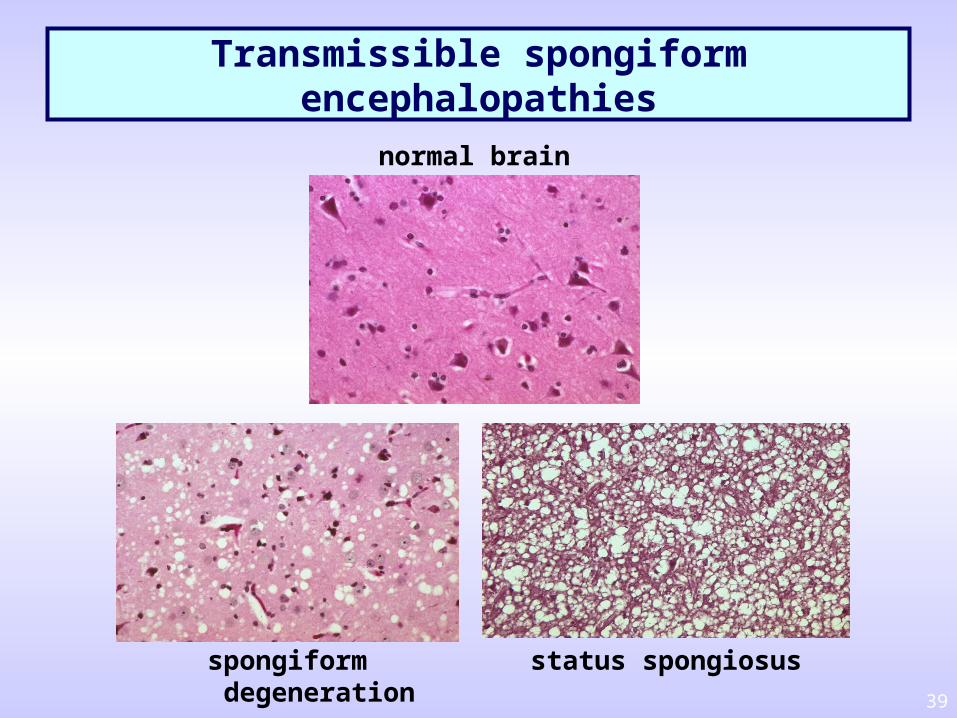
Transmissible spongiform encephalopathies
normal brain
spongiform degeneration
status spongiosus