Embed Size (px)
Citation preview
FDA 7.00
Cardiovascular Drugs That Prolong The QT Interval
Douglas C. Throckmorton, M.D.
U.S. Food & Drug Administration
Division of Cardio-Renal Drug Products
FDA 7.00
Issues• Approval of anti-arrhythmic drugs that prolong
the QT interval– Sotalol and Dofetilide
• Approval of cardiac drugs that prolong the QT interval, excluding the anti-arrhythmics– Bepridil
• Relationship between QT prolongation, Torsade de Pointes (TdP), and Clinical Events– Sotalol and Dofetilide
FDA 7.00
I. Approval for Atrial Arrhythmias• Sotalol and Dofetilide have a dose-
dependent effect on QTc and cause TdP
• Effect on QT intrinsic to their effect as an anti-arrythmic
• Approval was based on – Demonstration of symptomatic benefit – Obtaining sufficient information to adequately
describe the nature of the arrhythmic risk
FDA 7.00
d, l,-Sotalol• Class III anti-arrhythmic
– Approved for • Treatment of life-threatening ventricular
arrhythmias • Maintenance of Normal Sinus Rhythmn in
patients with atrial arrhythmias
• Mean effect on QTc– 10 to 40 msecs at doses from 160 to 640
mg/ day
• Dose-dependent effect on QTc prolongation and TdP
FDA 7.00
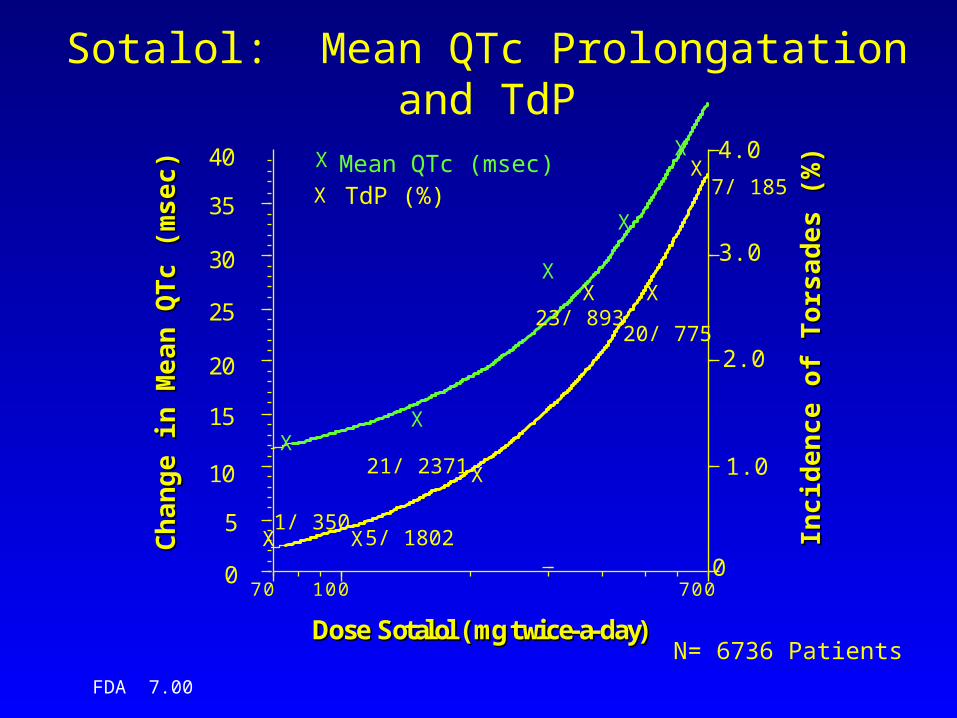
Sotalol: Mean QTc Prolongatation and TdP
XX
X
X
X
X X
X
X X
X
0
5
10
15
20
25
30
35
40
0
1.0
2.0
3.0
4.0
70 100 700
Ch
an
ge
in M
ea
n Q
Tc
(mse
c)
Ch
an
ge
in M
ea
n Q
Tc
(mse
c)
Inci
den
ce
of
To
rsa
de
s (%
)In
cid
enc
e o
f T
ors
ad
es
(%)
DDoossee SSoottaallooll ((mmgg ttwwiiccee--aa--ddaayy))
X
N= 6736 Patients
X
Mean QTc (msec)TdP (%)
21/ 2371
5/ 18021/ 350
23/ 89320/ 775
7/ 185
FDA 7.00
Sotalol: Effect on Mortality
• Post-Myocardial Infarction Trial (Julian Study); n=1,456– Early (<10 Days) Excess Mortality with
Sotalol
– Mortality on Sotalol at one year 7.3%– Mortality on Placebo at one year 8.9%
FDA 7.00
Sotalol: Effect on Mortality• Patients with Atrial Fibrillation and Atrial
Flutter*; n=1191– Sotalol: 3/747 (0.44%)
• 2 sudden deaths
– Quinidine: 1/86 (0.12%)• 0 sudden deaths
– Placebo: 2/358 (0.56%)• 1 sudden death
* Double-Blind portion of the trials only.
FDA 7.00
Dofetilide• Class III anti-arrhythmic
– Approved for • Maintenance of normal sinus rhythmn (NSR) • Conversion of atrial fibrillation/flutter to NSR
• Mean effect on QTc– 34 msec placebo-subtracted QTc
prolongation in phase II/III trials (n=976)
• Dose-dependent effect on mean QTc– 5 to 20 msecs QTc prolongation at doses
of 125 to 500 mcg BID
FDA 7.00
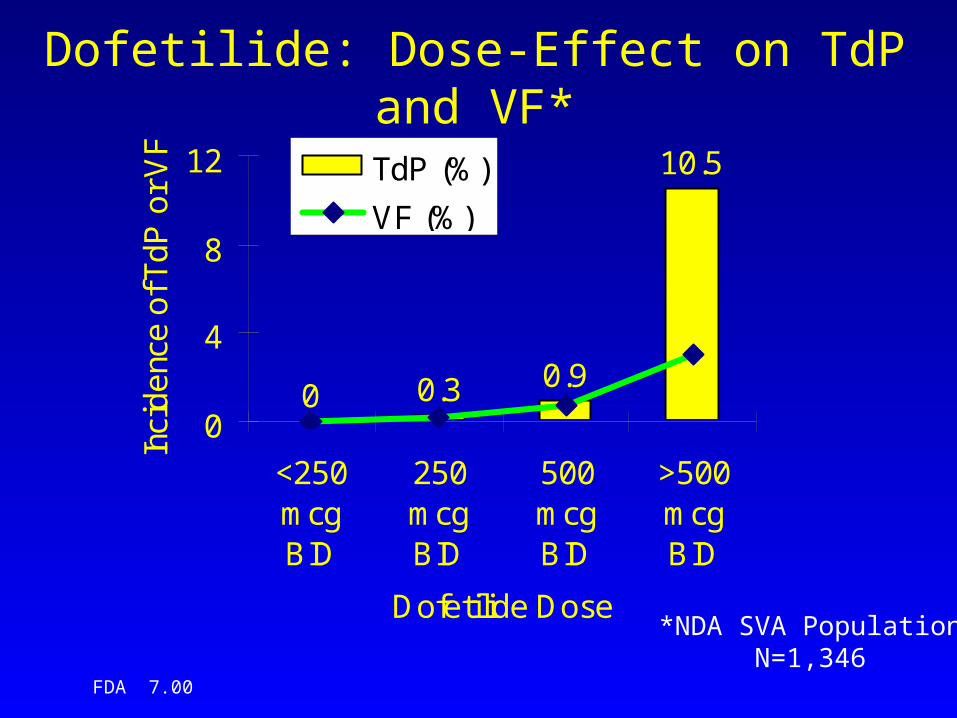
Dofetilide: Dose-Effect on TdP and VF*
0 0.3 0.9
10.5
0
4
8
12
<250mcgBID
250mcgBID
500mcgBID
>500mcgBID
Dofetilide Dose
Inci
de
nce
of T
dP
or
VF
TdP (%)
VF (%)
*NDA SVA PopulationN=1,346
FDA 7.00
Dofetilide: Mortality Effect in High-Risk Population
• DIAMOND CHF and MI– Patients with structural heart disease
and CHF• Dofetilide: 541/1511 (36%)• Placebo: 560/1517 (37%)
FDA 7.00
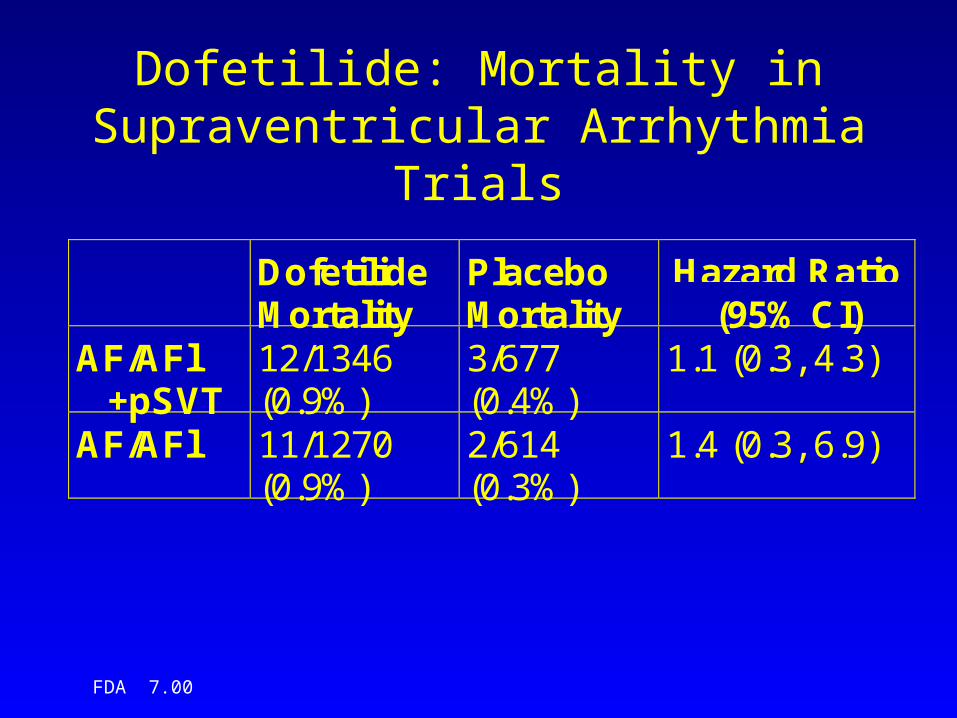
Dofetilide: Mortality in Supraventricular Arrhythmia Trials
DofetilideMortality
PlaceboMortality
Hazard Ratio(95% CI)
AF/AFl +pSVT
12/1346(0.9%)
3/677(0.4%)
1.1 (0.3, 4.3)
AF/AFl 11/1270(0.9%)
2/614(0.3%)
1.4 (0.3, 6.9)
FDA 7.00
Dofetilide: Dose-Adjustment to Minimize Cardiac Toxicity
• Measure baseline ECG, determine appropriateness of use
• Calculate creatinine clearance, choose appropriate starting dose
• Start Dofetilide under continuous ECG monitoring, dose-adjust as needed
FDA 7.00
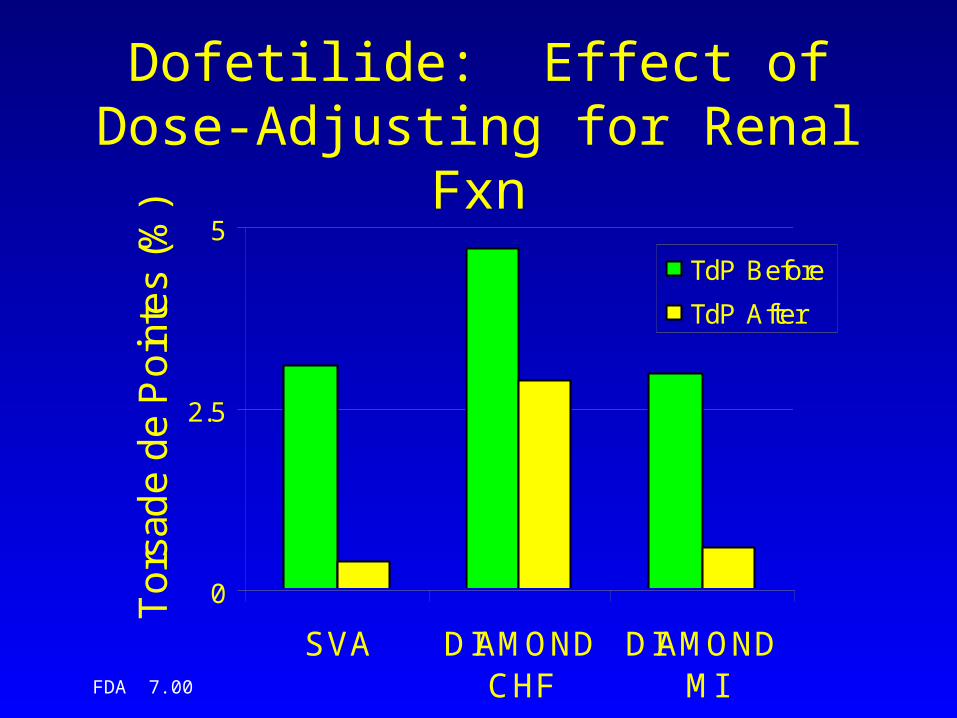
Dofetilide: Effect of Dose-Adjusting for Renal Fxn
0
2.5
5
SVA DIAMONDCHF
DIAMONDMI
To
rsad
e d
e P
oin
tes
(%)
TdP Before
TdP After
FDA 7.00
Dofetilide/ Sotalol Summary• Dose-dependent effect on QT, QTc, TdP and
Ventricular Fibrillation– Effects on QTc and TdP rate expected
• Overall mortality in high-risk and target populations not adverse
• Characterization of factors affecting risk of TdP– Exploration of broad dose-range– Exploration of other risk factors (e.g., Dofetilide and
Renal Fxn)
FDA 7.00
II. Approval As Second-Line Therapy
• Bepridil prolongs QT and causes TdP
• Not seen with other anti-anginals
• Approval based on demonstration of symptomatic benefit in a population resistant to available therapy
FDA 7.00
Bepridil• Calcium Channel Blocker
– Approved for treatment of chronic stable angina in patients intolerant or resistant to other anti-anginals
• Mean Effect on QTc– 30 to 70 msec– 5% of patients on Bepridil >25% increase
(appr. 100 msec)
• TdP: 7 cases in 840 angina patients in the U.S. population (0.8%), with 3 fatalities
FDA 7.00
Bepridil
• Effective in Resistant Populations– 86 patients with angina, refractory to Diltiazem,
randomized to Diltizem or Bepridil– Bepridil more effective anti-anginal in this
population, measured by exercise stress testing:• time to onset of angina• time to 1 mm ST-segment depression• total exercise time
FDA 7.00
Bepridil: Summary
• Dose-dependent effect on QT, QTc and clear association with TdP
• Effective in resistant patient population
FDA 7.00
Division of Cardio-Renal Drug Products Summary/Conclusions
• Use of cardiovascular drugs that prolong the mean QT in a dose-dependent fashion is associated with an increased risk for Torsade de Pointes and Sudden Death
FDA 7.00
Division of Cardio-Renal Drug Products Summary/Conclusions
• Cardiac drugs treating symptoms (e.g., atrial arrhythmias) have been approved with the following– Demonstration of symptomatic benefit – Sufficient information to adequately describe the
nature of the arrhythmic risk • Description of the drug-effect over a broad
dose-range• Exploration of potential factors that modify the
arrhythmic risk• Point estimates of total mortality in high-risk
population and in target population
FDA 7.00
Division of Cardio-Renal Drug Products Summary/Conclusions
• Cardiac drugs that cause QT prolongation can also be approved as second-line therapy by demonstrating a symptomatic benefit in a resistant population