Embed Size (px)
Citation preview

Favourable outcome in a case of endobronchial amyloidosis
D.E. SCHRAUFNAGEL, MD; L. KNIGHT, MD; W.L. YING, MD; N.S. WANG, MD
Fibreoptic bronchoscopy has madethe airways more accessible to en-doscopic examination, and uncom-mon diseases are consequently seenmore frequently. One of these un-usual entities is localized bronchialamyloidosis. It may mimic bron-chogenic carcinoma grossly and maybe missed at light microscopic ex-amination if it is not suspectedclinically and an adequate amountof submucosal tissue is not obtainedat the time of biopsy. Once the diag-nosis is correctly made it is difficultto determine the natural course ofthe disease and decide on the ap-propriate treatment.
Case reports
Case I
A 55-year-old woman was ad-mitted to hospital because of coughand fever for 1 month and right-sided pleuritic chest pain for severaldays. She denied purulent sputum orhemoptysis. She had smoked onepackage of cigarettes per day for30 years.The woman was having paro-
xysms of dry, hacking cough. Herblood pressure was 112/74 mm Hg,pulse rate 118 beats/min, respira-tory rate 22/min and temperature38°C. Breath sounds were reducedposteriorly over the middle onethird of the right side of the chest.The results of physical examinationwere otherwise normal.
Chest roentgenography revealeda wedge-shaped homogeneous areaof consolidation in the superiorsegment of the lower lobe of theright lung without an air broncho-gram, which suggested postobstruc-tive pneumonitis. The results ofarterial blood gas analysis were nor-mal. Multiple sputum cultures for
From the respiratory division, theMontreal Chest Hospital, the RoyalVictoria Hospital and the pathologyinstitute, McGill University, MontrealReprint requests to: Dr. D.E.Schraufnagel, Respiratory division,Royal Victoria Hospital, 687 Pine Ave.W, Montreal, PQ H3A lAI
Mycobacterium tuberculosis werenegative; only normal oropharyn-geal flora grew on the bacterial cul-tures. The hemoglobin level was 11g/dl and the leukocyte count 11.53x 109/1. Findings from blood bio-chemical tests and urinalysis werenormal. Skin testing with 5 tuber-culin units of purified protein de-rivative resulted in induration 20mm in diameter. One of 10 sputumspecimens undergoing cytologicexamination contained malignantsquamous cell's.
Fibreoptic bronchoscopy revealeda mound of reddish friable tissue ob-structing the superior segment of theright lower lobe, suggestive of bron-chogenic carcinoma. A biopsy wasnot done because of the possibilityof excessive bleeding. Several lymphnodes removed at mediastinoscopycontained no malignant cells. Thepatient underwent right lower lobec-tomy for suspected carcinoma andrecovered uneventfully.
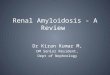
Pathological examination revealeda dense submucosal deposit of anamorphous pink substance that nar-rowed the entire circumference ofthe right lower lobe bronchus andits adjacent derivative bronchi (Fig.1). The amorphous substance de-monstrated green birefringence
FIG. 1-Case 1: lumen of subseg-mental bronchus narrowed by diffusethickening and protruding nodule(arrow) in submucosa (hematoxylin-eosin; X 6).
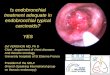
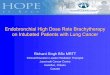
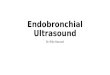
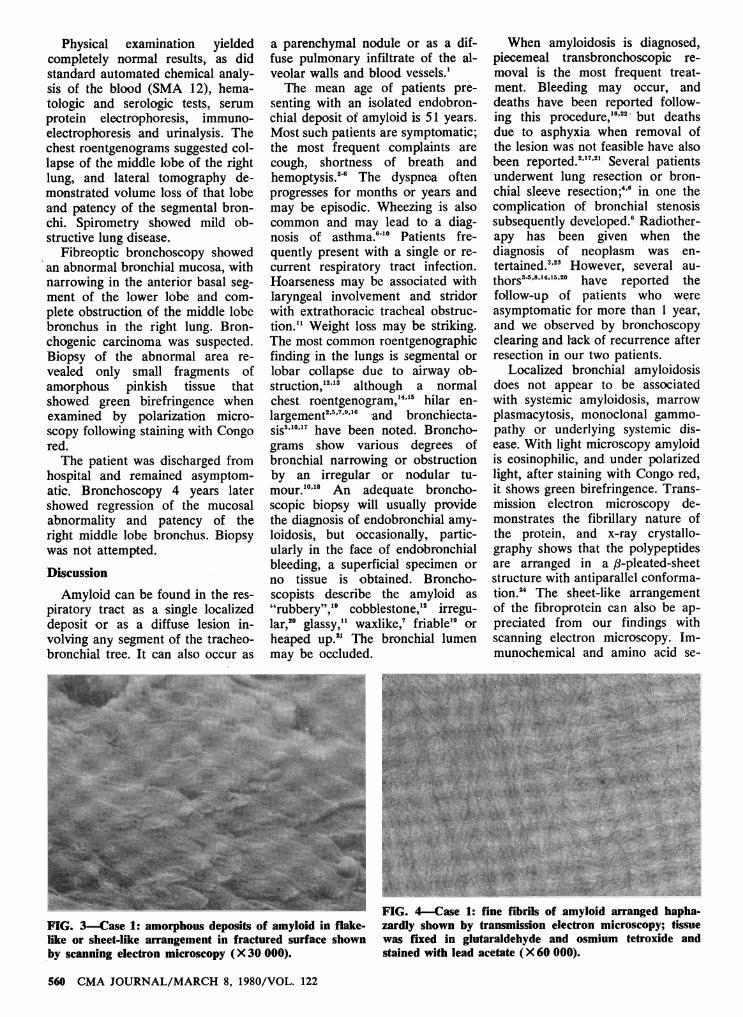
when examined by polarization mi-croscopy following staining withCongo red (Fig. 2). The amorphismof the substance was also appre-ciated by scanning electron micro-scopy at a lower power, but highermagnification showed a flake-likeor plate-like arrangement of amy-loid at the freeze-fractured surface(Fig. 3). Fine fibrils arranged hap-hazardly were obvious with trans-mission electron microscopy (Fig.4). The same material was foundaround the bronchial vessels.One year later lingular pneu-
monia developed. In view of theprevious positive results of cytologybronchoscopy was done again; thefindings were normal. The pneu-monia cleared completely with appropriate antibiotic therapy.
Case 2
A 61-year-old cabinetmaker wasadmitted to hospital because ofhemoptysis, which he had also ex-perienced 7 months prior to admis-sion. He had smoked, on average,2 packs of cigarettes per day for30 years. Chest pain, dyspnea andrespiratory tract infection weredenied. He had lost 4 kg in theprevious 9 months and had occa-sional night sweats, but no fever.
FIG. 2-Case 1: strong birefringenceof thickened submucosa of subseg-mental bronchus shown with polariza-tion microscopy (Congo red; X25).
CMA JOURNAL/MARCH 8, 1980/VOL. 122 559
Physical examination yieldedcompletely normal results, as didstandard automated chemical analy-sis of the blood (SMA 12), hema-tologic and serologic tests, serumprotein electrophoresis, immuno-electrophoresis and urinalysis. Thechest roentgenograms suggested col-lapse of the middle lobe of the rightlung, and lateral tomography de-monstrated volume loss of that lobeand patency of the segmental bron-chi. Spirometry showed mild ob-structive lung disease.
Fibreoptic bronchoscopy showedan abnormal bronchial mucosa, withnarrowing in the anterior basal seg-ment of the lower lobe and com-plete obstruction of the middle lobebronchus in the right lung. Bron-chogenic carcinoma was suspected.Biopsy of the abnormal area re-vealed only small fragments ofamorphous pinkish tissue thatshowed green birefringence whenexamined by polarization micro-scopy following staining with Congored.The patient was discharged from
hospital and remained asymptom-atic. Bronchoscopy 4 years latershowed regression of the mucosalabnormality and patency of theright middle lobe bronchus. Biopsywas not attempted.
Discussion
Amyloid can be found in the res-piratory tract as a single localizeddeposit or as a diffuse lesion in-volving any segment of the tracheo-bronchial tree. It can also occur as
a parenchymal nodule or as a dif-fuse pulmonary infiltrate of the al-veolar walls and blood vessels.1The mean age of patients pre-
senting with an isolated endobron-chial deposit of amyloid is 51 years.Most such patients are symptomatic;the most frequent complaints arecough, shortness of breath andhemoptysis.`6 The dyspnea oftenprogresses for months or years andmay be episodic. Wheezing is alsocommon and may lead to a diag-nosis of asthma.6'0 Patients fre-quently present with a single or re-current respiratory tract infection.Hoarseness may be associated withlaryngeal involvement and stridorwith extrathoracic tracheal obstruc-tion."1 Weight loss may be striking.The most common roentgenographicfinding in the lungs is segmental orlobar collapse due to airway ob-struction,"2'," although a normalchest roentgenogram,"4" hilar en-largement2'5'7'9'16 and bronchiecta-sis',""7 have been noted. Broncho-grams show various degrees ofbronchial narrowing or obstructionby an irregular or nodular tu-mour.10"8 An adequate broncho-scopic biopsy will usually providethe diagnosis of endobronchial amy-loidosis, but occasionally, partic-ularly in the face of endobronchialbleeding, a superficial specimen orno tissue is obtained. Broncho-scopists describe the amyloid as"rubbery",'9 cobblestone," irregu-lar,20 glassy,'1 waxlike,7 friable'9 orheaped up.2' The bronchial lumenmay be occluded.
When amyloidosis is diagnosed,piecemeal transbronchoscopic re-moval is the most frequent treat-ment. Bleeding may occur, anddeaths have been reported follow-ing this procedure,'8"' but deathsdue to asphyxia when removal ofthe lesion was not feasible have alsobeen reported.",7"' Several patientsunderwent lung resection or bron-chial sleeve resection;46 in one thecomplication of bronchial stenosissubsequently developed.6 Radiother-apy has been given when thediagnosis of neoplasm was en-tertained.,"" However, several au-thors'4'814"520 have reported thefollow-up of patients who wereasymptomatic for more than 1 year,and we observed by bronchoscopyclearing and lack of recurrence afterresection in our two patients.
Localized bronchial amyloido-sisdoes not appear to be associatedwith systemic amyloidosis, marrowplasmacytosis, monoclonal gammo-pathy or underlying systemic dis-ease. With light microscopy amyloidis eosinophilic, and under polarizedlight, after staining with Congo red,it shows green birefringence. Trans-mission electron microscopy de-monstrates the fibrillary nature ofthe protein, and x-ray crystallo-graphy shows that the polypeptidesare arranged in a p-pleated-sheetstructure with antiparallel conforma-tion.' The sheet-like arrangementof the fibroprotein can also be ap-preciated from our findings withscanning electron microscopy. Im-munochemical and amino acid se-
FIG. 3-Case 1: amorphous deposits of amyloid in flake-like or sheet-like arrangement in fractured surface shownby scanning electron microscopy (X 30 000).
FIG. 4-Case 1: fine fibrils of amyloid arranged hapha-zardly shown by transmission electron microscopy; tissuewas fixed in glutaraldehyde and osmium tetroxide andstained with lead acetate (X 60 000).
560 CMA JOURNAL/MARCH 8, 1980/VOL. 122

quencing studies have shown thatthese proteins are frequently de-rived from the amino terminal endof light-chain immunoglobulins.24 Inour cases, like others of bronchialamyloidosis, plasma cells and lym-phocytes were observed within orat the border of the amyloid depo-sits.4,5,15,22,Ut
Localized endobronchial amy-loidosis presented like bronchogeniccarcinoma in our two patients. Inthe first patient lobectomy appearsto have been curative. In the secondthere was spontaneous regression ofthe disease. Review of the literatureindicates that only about half of thepatients have progressive disease. Itmay therefore be prudent to observepatients with endobronchial amy-loidosis, especially those that areasymptomatic.
We thank M. Charbonneau and J.Kroon-Vandor for technical assistanceand B. Ottoni and G. Pawelec forsecretarial assistance.
This study was supported in part bygrant MA-5305 from the MedicalResearch Council of Canada and theRoyal Edward Laurentian Foundation.
References1. SPENCER H: Pathology of the Lunr1g,
3rd ed. Pergamon, New York. 1977.pp 675-80
2. SCHOTTENFELD A. ARNOLD LM,GRUBN JG, et al: Localized amyloiddeposition in the lower respiratorytract. Am77 J AMed 11: 770, 1951
3. SCHMIDT HW. MCDONALD JR.CLAGETT OT: Amyloid tumors ofthe lower part of the respiratorytract and mediastinum. A r11 OtolRliiniol Larv1vgol 62: 880. 1953
4. CorrON RE. JACKSON JW: Localizedamyloid "tumours" of the lungsimulating malignant neoplasms.Thorax 19: 97. 1964
5. MCGURK FM: Primary bronchialamyloidosis. Br J Radiol 41: 795.1968
6. NAEF AP. SAVARY M. SCHMID DEGRUNECK JM. et al: Amyloid pseu-dotumor treated by tracheal resec-tion. Anr1J Tlorac Surg 23: 578.1977
7. SHINoi K. SHIRAISHI Y. YAHATA JD:Amyloid tumor of the trachea andlung, resembling bronchial asthma.Case report. Dis Chest 42: 442.1962
8. HOLINGER PH. JOHNSTON KC. DEL-GADO A: Amyloid tumors of thelarynx and trachea. AMIA Arch Oto-larngolrt 70: 555. 1959
9. HENRIKSSON P. LILJENBERG B:Bronchial asthma and tumour-form-ing amyloidosis of the trachea and
bronchi. Acta Allergol (Kb/i) 17:276, 1962
10. BONFILS-ROBERTS E, MARX AJ.NEALON TF JR: Primary amyloid-osis of the respiratory tract. AnnrThorac Suyrg 19: 313, 1975
11. PROWSE CB: Amyloidosis of thelower respiratory tract. Thorax 13:308, 1958
12. GORDONSON JS. SARGENT EN, JA-COBSON G, et al: Roentgenographicmanifestations of pulmonary amy-loidosis (classification and case illus-trations). J Can Assoc Radiol 23:269, 1972
13. RUBINOW A, CELLI BR, COHEN AS.et al: Localized amyloidosis of thelower respiratory tract. A)I RevRespir Dis 118: 603, 1978
14. KAMBERG S, LOITMAN BS, HOLTZ S:Amyloidosis of the tracheobronchialtree. N Enigi J Med 266: 587, 1962
15. GOTTLIEB LS, GOLD WM: Primarytracheobronchial amyloidosis. A inRev Respir Dis 105: 425, 1972
16. STARK DB, NEW GB: Amyloid tu-mors of the larynx, trachea orbronchi: report of 15 cases. An)1)Otol Rhiniol Larvingol 58: 117, 1949
17. GORDON W: Amyloid deposits in thebronchi. Br Med 1 1: 825, 1955
18. COOK AJ, WEINSTEIN M. POWELLRD: Diffuse amyloidosis of thetracheobronchial tree. Bronchograph-ic manifestations. Radiology 107:303, 1973
19. BOLSTAD DS: Primary amyloidosisin the lower respiratory tract. A iOtol Rhimiol Larvyngol 63: 200, 1954
20. GREGOR WM, LUCKE HH: Amyloid-osis of bronchus resembling carci-noma. Can Med Assoc J 99: 912,1968
21. ATTwOOD HD, PRICE CG, RIDDELLRJ: Primary diffuse tracheobronchialamyloidosis. Thorax 27: 620, 1972
22. MAINWARING AR, WILLIAMS G,KNIGHT EOW, et al: Localized amy-loidosis of the lower respiratorytract. Thorax 24: 441, 1969
23. HOLINGER PH, NOVAK FJ, JOHNSTONKC: Tumors of trachea. Larvngo-scope 60: 1086, 1950
24. GLENNER GG, TERRY WD, ISERSKYC: Amyloidosis: its nature and pa-thogenesis. Semin Hemnatol 10: 65,1973
BOOKScontinued from page 540
ATLAS OF EMERGENCY MEDICINE.Peter Rosen and George Sternbach. 165pp. Illust. The Williams & Wilkins Com-pany, Baltimore; the Macmillan Com-pany of Canada Limited, Toronto, 1979.$23.50. ISBN 0-683-07914-XCAHIERS D'ENSEIGNEMENT DE LASOFCOT. 9. Maladie luxante congenitalede la hanche. Traitement chez l'enfant.Redacteur en chef: J. Mallet avec lacollaboration de J. Bedouelle, M. Cam,H. Carlioz et autres. 159 pp. Illust. Ex-pansion Scientifique Francaise, Paris,1979. $53.10, broche. ISBN 2-7046-1037-1CAHIERS DENSEIGNEMENT DE LASOFCOT. 10. Conferences d'enseign'e-ment 1979. Sous la direction de J.Duparc avec la' collaboration de J.L.Alain, J.Y. Alnot, P. Boutin et autres. 140pp. Illust. Expansion Scientifique Fran-caise, Paris, 1979. $38.80, broche. ISBN2-7046-1 038-XCLINICAL ASPECTS OF NEUROIMMU-NOLOGY. Edward A. Neuwelt and W.Kemp Clark. 277 pp. Illust. The Williams& Wilkins Company, Baltimore; theMacmillan Company of Canada Limited,Toronto, 1978. $45.50. ISBN 0-683-06437-1COMMON SYMPTOMS -OF DISEASE INCHILDREN. 6th ed. R.S. lllingworth.370 pp. Illust. Blackwell Scientific Pub-lications, Oxford; the C.V. Mosby Com-pany, Saint Louis, 1979. $24. ISBN 0-632-00003-1EXERCISE ELECTROCARDIOGRAPHY:Practical Approach. Edited by EdwardK. Chung. 354 pp. Illust. The Williams& Wilkins Company, Baltimore; theMacmillan Company of Canada Lim-
ited, Toronto, 1979. $39.95. ISBN 0-683-01569-9EXTERNAL FIXATION. The Current Stateof the Art. Proceedings of the 6th In-ternational Conference on HoffmannExternal Fixation. Edited by Andrew F.Brooker, Jr. and Charles C. Edwards.419 pp. Illust. The Williams & WilkinsCompany, Baltimore; the MacmillanCompany of Canada Limited, Toronto,1979. S25.95, paperbound. ISBN 0-683-01073-5GASTRIC CANCER. Edited by Ch.Herfarth and P. Schlag. 374 pp. Illust.Springer-Verlag New York Inc., NewYork, 1979. $43.50. ISBN 0-387-09467-9THE GROWTH OF MEDICAL INFORMA-TION SYSTEMS IN THE UNITED STATES.Donald A.B. Lindberg. 194 pp. D.C.Heath Canada Ltd., Toronto, 1979. $23.ISBN 0-669-02911-4HANDBOOK OF DRUG THERAPY. Editedby Russell R. Miller and David J. Green-blatt. 1226 pp. Illust. Elsevier North-Holland, Inc., New York, 1979. $37.50,hardbound; $25, paperbound. ISBN0-444-00329-0, hardbound; ISBN 0-444-00253-7, paperboundHORMONES IN BLOOD. 3rd ed. Volume1. Edited by C.H. Gray and V.H.T.James. 707 pp. lllust. Academic PressInc. (London) Ltd., London, 1979. $86.50.ISBN 0-12-296201-XHORMONES IN BLOOD. 3rd ed. Volume2. Edited by C.H. Gray and V.H.T. James.463 pp. Illust. Academic Press Inc.(London) Ltd., London, 1979. S63.50.ISBN 0-12-296202-8
CMA JOURNAL/MARCH 8. 1980/VOL. 122 561