Embed Size (px)
Citation preview

99:163
MEDICAL BIOCHEMISTRY
LECTURER: PETER RUBENSTEIN
FATTY ACID METABOLISM

2

3
LEARNING OBJECTIVES
1. Describe how dietary fats are handled in the digestive system to allow their
ultimate introduction of dietary fatty acids into the blood.
2. Describe how fatty acids are mobilized from fat stores in adipose tissue.
3. Explain how fatty acids are removed from the blood and shuttled to the mitochondria for beta oxidation. How is the carnitine system regulated?
4. Describe the sequence of events called beta oxidation by which fatty acids are
degraded. Explain how metabolic energy is generated in the process.
5. Describe the symptoms that often accompany defects in fatty acid degradation and explain their origin.
6. Describe the pathway that leads to the generation of the three ketone bodies and
explain why their levels go up in response to increased fatty acid mobilization. Explain why elevated ketone body levels can lead to metabolic acidosis.
7. Explain how the substrates for fatty acid synthesis in the cytosol are generated.
8. Explain the way fatty acids are synthesized in terms of the reductive cycle that
occurs with every two carbon addition, the role of malonyl CoA in the process, and the two-site shuttling mechanism used by fatty acid synthase to accomplish this end.


5
III. Use of Dietary fatty acids Dietary triglyceride MOUTH STOMACH SMALL INTESTINE Bile Liver Pancreatic lipase Pancreas 2-Monoglyceride + Fatty acid SMALL INTESTINAL ENTEROCYTES Triglycerides Chylomicrons LYMPH BLOOD CAPILLARIES Lipoprotein lipase Fatty acids TISSUES

6
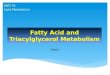
IV. Mobilization of Fatty Acids from Adipose Tissue Glucagon/ epinephrine Receptor Activated G-protein cAMP Adenylate cyclase
PKA Hormone Sensitive Lipase Glycerol MAG DAG TAG FA FA FA ________________________________________________________ BLOOD Serum Albumin FA—Albumin Complex Liver Extrahepatic FFA FFA -Oxidation Acetyl CoA Acetyl CoA Ketone CO2 + H2O CO2 +H2O
Bodies

7
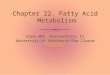
V. Fatty Acid Transfer to Cytosol and Activation FA FA-Albumin ___________________________________________________________ FAT plasma membrane _________________________(Fatty Acyl Transferase)_______________ FABP FA
CoASH, ATP AcylCoA Synthetase FA-CoA -Oxidation Phospholipids Triglycerides Sphingolipids
A. Coenzyme A
B. Derived from pantothenic acid (vitamin)
C. Active end is a thiol
O
D. Forms a thioester ( R-C-SCoA) with a carboxylate group following carboxylate activation.

8
E. Activation process is called adenylation which means the carboxyl is activated by the attachment of AMP (adenylate).
O O AMP R—C—O- + ATP R—C—O—P—OAdrib + PPi O O R—C—O—P—OAdrib +HS-CoA R—C—SCoA + AMP PPi + H2O 2Pi (Inorganic pyrophosphatase) Anytime PPi is produced as a product in the cell it is hydrolyzed, releasing an extra 8 kcal/mole of energy which drives the overall reaction forward. Overall Rxn: O R-COO- + ATP + CoASH + H2O R-C-SCoA + AMP + 2Pi
VI. Transport of Fatty Acyl CoA into Mitochondrial Matrix, the Site of FA Degradation (-Oxidation)
A. FA-CoA cannot go across inner mitochondrial membrane
B. Within membrane is an “Acyl Carnitine Transport System” for bring the activated FA moiety across
C. Depends on conversion of acyl-CoA to acyl-carnitine, an activated oxygen
ester form of the fatty acid.

9
D. Carnitine
1. Derivative of methionine and lysine: OH group for acyl attachment.
2. Obtained primarily in diet from meat products 3. Can be made in liver and kidney 4. Vast majority in body is found in skeletal and cardiac muscle.
E. System has three parts:
1. Carnitine palmitoyl transferase I (outer mitochondrial membrane) – Called CPT I
2. Acyl carnitine transporter (inner mitochondrial membrane) 3. Carnitine palmitoyl transferase II (mitochondrial matrix) Called CPT II

10
F. Short and medium chain FAs (<12 carbons) do not require carnitine system for
mitochondrial entry. G. Very long chain FAs first enter peroxisome where they are partially degraded
(discussed later). Partially shortened FAs finish degradation in mitochondrion. VI. Metabolic regulation involving the acyl-carnitine system.
A. Effects on carbohydrate utilization
1. Build-up of fatty acyl carnitines inhibits pyruvate dehydrogenase
2. This inhibition prevents entry of carbohydrate carbons into the mitochondrion as acetyl CoA since the excess of FA carnitine is a signal for surplus energy substrates in the mitochondrion.
B. Malonyl CoA inhibits CPT I
1. Malonyl CoA is a substrate for FA synthesis. Its presence indicates cell is in
a FA synthetic mode.
2. This inhibition prevents fatty acids from being degraded in the same cell that is geared to making them for transport to the rest of the body.
VII. Degradation of fatty acids in mitochondrion
A. Beta Oxidation
1. All reactions occur in the mitochondrial matrix
2. The set of four reactions sequentially clips 2-carbon fragments of the starting fatty acid as acetyl-CoA which can then be used in the Krebs Cycle.
3. 1 NAD, 1 FAD, and 1 CoASH needed for each 2-carbon fragment generated.
For each cycle, 1 NADH and 1 FADH2 produced.
4. For complete degradation, there is one fewer cycles than the number of 2-carbon fragments in the original fatty acyl CoA.

11

12
B. Energy yield in beta oxidation of palmitate (C16)
7 FADH2 produced 14 ATP (assume 2/ FADH2)
7NADH produced 21 ATP (assume 3/NADH)
8 acetyl CoA (Krebs Cycle: 12 ATP/acetyl CoA) 96 ATP
-2 P to make FA-CoA initially (adenylation rxn.)
Net yield: 129 ATP/ palmitate VII. Oxidation of Very Long FAs (C20 or larger)
A. Occur in peroxisome B. Carnitine system NOT involved C.Modified-Oxidation is utilized
1. Desaturation is carried out by an FAD-dependent oxidase 2. O2 is the terminal electron acceptor 3. The peroxide made (HO—OH ) is destroyed by catalase 4. NADH is returned to the cytosol 5. ATP is not generated 6. Shortened FAs go to mitochondrion for further degradation
VIII. Defects in the degradation of fatty acids (mitochondrial)
A. Systemic consequences
1. ATP shortage in cells that normally oxidize FAs 2. Hypoglycemia because of abnormally high reliance on blood glucose as
energy source. 3. Decreased levels of ketone bodies in blood (discussed later) called
hypoketonemia

13
4. Carnitine deficiency – undegraded fatty acids made into carnitine or glycine esters and eliminated from the body via the urine.
5. Symptoms include weight-loss, fatigue, vomiting, coma, can be fatal.
Exacerbated by driving body into a catabolic state.
6. Dicarboxylic aciduria
a. Undegraded FAs accumulate
b. Terminal methyl group oxidized to –CO2-
c. Reaction catalyzed by a cytochrome P450 isoform d. Occurs in the endoplasmic reticulum e. Product , - dicarboxylic acids eliminated in urine. f. Detected by column chromatographic analysis of urine.
B. Specific conditions
1. CPT deficiency
a. CPT I – Effects liver. Often fatal. Inability of liver to oxidize long chain
FAs to generate energy to fuel gluconeogenesis.
b. CPT II – Primarily in cardiac and skeletal muscle. Cardiomyopathy, muscle fatigue, myoglobinuria due to inability of muscle to oxidatively generate ATP to fuel muscle contraction.
c. Treatment: carbohydrate-rich diet, low in fats and supplemented with
medium chain FAs and carnitine.
2. MCAD Deficiency
a. Many of the enzymes of -oxidation scheme are found as isozymes with specificities for different chain length fatty acids.
b. Acyl CoA Dehydrogenases (Long chain, medium chain, short chain). c. Relatively common genetic defect (1 /12,000 births in West) is MCAD
deficiency (affects medium length FA utilization) d. Treatment: carbohydrate-rich diet, carnitine, short-chain FAs.

14
e. Unusual case: Wilhelm, G. (2006). Sudden Death in a Young Woman from MCAD Deficiency. J. Emerg. Med. 30, 291-294. First diagnosed at age 19 following a bout of drinking.
3. Peroxisomal disorders
a. Zellweger’s syndrome (cerebrohepatorenal) – due to defect in
peroxisome biogenesis. Fatal b. X-linked adrenoleukodystrophy – defect in activation of VLFAs –
accumulate in serum – CNS effects, mental retardation – Lorenzo’s Oil.
KETONE BODIES I. Biological significance in normal conditions
A. Made in liver mitochondria from excess acetyl CoA
B. Excreted into blood C. Carry excess acetyl CoA carbons, H+ and electrons from the liver D. Used as fuels by other oxidative tissues such as brain, especially during
starvation when glucose is limiting. Normally, rate of production and clearance from blood are balanced.
II. Three components
A. Acetoacetate (parent compound) B.-Hydroxybutyrate (made from acetoacetate) C. Acetone (spontaneous decarboxylation product of acetoacetate in blood)
1. Occurs because of ease of decarboxylation of -ketoacids
2. Expelled from body via respiration

15
III. Ketone Body Synthesis
A. Competition for mitochondrial acetyl CoA between citrate synthase and the first enzyme in the ketone biosynthetic pathway.
B. Production of acetyl CoA greater than the Krebs Cycle can use will result in an
increase in ketone bodies.
C. Factors affecting Krebs Cycle clearance of Acetyl CoA
1. Increased acetyl CoA production due to increased beta oxidation
2. Saturation of the electron transfer chain due to increased beta oxidation causing a shortage of mitochondrial NAD and FAD
3. Decreased availability of OAA for condensation with acetyl CoA to make
citrate
D. Ratio of -hydroxybutyrate/ acetoacetate
1. Determined by NADH/NAD ratio in the mitochondrion.
2. By converting acetoacetate to -hydroxybutyrate, mitochondrion not only gets rid of two excess acetate units but also 2 electrons from NADH. Helps regenerate the NAD needed for continued Krebs Cycle and beta oxidation.
3. Virtually continuous operation of Krebs and beta oxidation ensures NADH is
always in excess.
4. Ratio of -HB/ acetoacetate in a normal individual is about 3:1

16
IV. Utilization of ketone bodies by nonhepatic tissues
A. Important fuels for muscle, heart, brain. Liver makes ketones, it does not use them
B. -Hydroxybutyrate reoxidized to acetoacetate in mitochondrion by NAD-
dependent -hydroxybutyrate dehydrogenase.
C. Acetoacetate-succinyl CoA transferase (thiophorase) transfers CoA to acetoacetate from succinyl CoA yielding succinate and acetoacetyl CoA (Enzyme not in liver).
D. Acetoacetyl CoA attacked by CoASH (-ketothiolase) yielding 2 Acetyl CoA VI. Abnormal ketone body production
A. Abnormally low production
1. Hypoketonemia
2. Defects in fatty acid oxidation or enzymes involved in ketone synthesis.
3. Severe hypoglycemia – causes increased dependence on ketone bodies as source of energy. Usage exceeds amount synthesized.
B. Abnormally high production
1. Ketosis – serum pH remains normal
2. Ketoacidosis – production levels are so high that the protons introduced into
the blood with the ketone bodies cannot be totally compensated by the blood bicarbonate buffer system, and the serum pH drops.
3. Detection:
a. Quick and dirty – dipstick analysis of urine. Only detects acetoacetate.
b. Better – analysis of -hydroxybutyrate in serum by -hydroxybutyrate
dehydrogenase. Especially important in case where NADH/NAD ratio is radically increased (types of alcohol usage) in which case the acetoacetate might only account for about 3-5% of the total ketone bodies present.

17
VII. Metabolic acidosis
A. Bicarbonate buffer system in blood
Carbonic anhydrase (Zn)
CO2 + H2O H2CO3 HCO3- + H+
B. Blood pH described by Henderson-Hasselbach Eqn.
pH = pK + log ((Anion)/(Acid)) For Bicarbonate system,
pH = 6.1 + log (HCO3-/ .03 PCO2)
C. Anion Gap
(Na+ + K
+) - (Cl
- + HCO3
-) 12-16 meq./dl if include K
+
8-12 meq./dl if do not include K+
D. Clinical scenario
1. Assume large amt. of organic acid (with its H+) is dumped into serum
2. H+ neutralizes HCO3- which ultimately becomes CO2 and blown off by the
lungs
3. Ratio of HCO3-/PCO2 decreases and pH decreases
4. Normal pH, 7.4; pH 7, life-threatening; <pH 7, often fatal
5. As bicarbonate decreases, anion gap increases. (Anion gap metabolic
acidosis
E. Build-up of H+ stimulates breathing in an attempt to acutely restore pH by
expelling CO2. Result is rapid, deep breathing called Kussmaul Respiration.


18
FATTY ACID BIOSYNTHESIS Introduction, overview Fatty acids are made in the cytosol from one acetyl CoA and many malonyl CoA molecules. Malonyl CoA comes from acetyl CoA. Acetyl CoA is made in the mitochondrion and must be transported to the cytosol as citrate before reconversion to acetyl CoA. I. Biosynthesis of cytoplasmic acetyl-CoA
A. Cytoplasmic acetyl-CoA is an important precursor for fatty acid biosynthesis which occurs entirely in the cytosol.
1. Acetyl-CoA cannot be synthesized de novo in the cytosol.
2. The source of cytosolic acetyl-CoA is mitochondrial acetyl-CoA, but acetyl-
CoA cannot cross the inner mitochondrial membrane.
B. Shuttling of acetyl-CoA equivalents across the inner mitochondrial membrane.
1. The acetyl-CoA is carried across as citrate (made in Krebs Cycle) under conditions where mitochondrial isocitrate dehydrogenase activity is low.
2. Shuttling is done by a specific tricarboxylic acid shuttle system.
3. In the cytosol, citrate is acted on by ATP-citrate lyase which uses ATP and
CoASH to split the citrate into acetyl CoA and oxaloacetate.

19
II. Synthesis of Malonyl-CoA
A. Major substrate for fatty acid synthesis
1. For an even chain fatty acid with n carbons, need 1 acetyl-CoA and (n-1)/2 malonyl CoA molecules
2. For every malonyl CoA used (3 carbon fragment) for fatty acid synthesis, a
CO2 is released
B. Synthesized by acetyl-CoA carboxylase
1. Biotin is a required cofactor; carboxybiotin is an intermediate form of “activated CO2”.
2. Reaction chemistry is like that used for pyruvate carboxylase which makes
oxaloacetate.
C. Regulation of acetyl-CoA carboxylase activity
1. Inactive dimer polymerizes to active polymer
a. Build-up of citrate causes polymerization and activation
b. Build-up of fatty acids cause depolymerization and inactivation
2. Covalent phosphorylation of enzyme leads to its depolymerization
a. Enzyme is phosphorylated in vivo by AMP kinase (not PKA) – leads to its depolymerization.
b. This phosphorylation is balanced by the action of a protein phosphatase
which acts to activate the carboxylase.
c. PKA, in response to epinephrine or glucagon causes inhibition of the phosphatase resulting in net inactivation of acetyl-CoA carboxylase.
d. Indirectly: PKA-dependent phosphorylation leads to acetyl-CoA
carboxylase inhibition, and dephosphorylation leads to acetyl-CoA carboxylase activation.

20
III. Synthesis of saturated fatty acids
A. Major fatty acid synthesized in mammals is a C16 fatty acid with no double bonds: palmitate (16:0)
1 Ac CoA + 7 mal CoA + 14 NADPH palmitate + 14 NADP + 8 CoA + 7 CO2
1. 7 cycles of what is sort of the reverse of beta oxidation
2. In each cycle, there is a decarboxylation 3. In each cycle, there are two reductions
B. Reaction carried out by Fatty Acid Synthase
1. Single polypeptide chain with an active site for each step in the reductive
cycle. 2. Two chains come together in anti-parallel fashion such that each half of each
duplex contains all of the active sites necessary for synthesis of one fatty acid. Makes process much more spatially and temporally efficient.
3. Growing chain passed back and forth between two sites at one end. Sort of
like the ribosome during translation.
a. One site is the “condensing enzyme” site – Active site residue is a cysteine sulfhydryl group.
b. Second site is an ACP or acyl carrier protein site
i. Active site is the –SH of a 4-phosphopantetheinyl (4Pp) group
ii. 4Pp is attached covalently to the polypeptide chain of FA synthase iii. 4Pp is basically the SH half of Coenzyme A minus the nucleotide –
acts as a swinging arm attached to the protein.
4. Addition of new C2 units therefore occurs at the Carboxyl End of the growing fatty acid. The machinery does not have to keep moving to the new end. It stays put and reels out the fatty acid from the active site. Knitting needle model.

21
5. Differences between fatty acid synthesis and -oxidation
a. During -oxidation, 2-carbon units are released as acetyl CoA whereas during synthesis, 2-carbon units added come from a C3 compound, malonyl CoA accompanied by decarboxylation..
b. NAD is used to oxidize a hydroxyl to a ketone group in -oxidation while
NADPH is used to reduce a ketone to a hydroxyl group in synthesis.
c. FAD oxidizes a saturated C-C bond producing a double bond in -oxidation while in synthesis, NADPH reduces a double bond to a C-C single bond
d. This is an example of a more general phenomenon in which NADP(H)
tends to be used for biosynthetic purposes whereas NAD(H) tends to be used for catabolic purposes

22

23
FATTY ACID DESATURATION – endoplasmic reticulum Utilizes acyl CoA 3 human desaturases – insert double bonds in the cis configuration H H H R cis C = C C = C trans R R R H
Formed in food processing (hydrogenation) SCD – stearoyl CoA desaturase – fatty acid 9-desaturase – acts on saturated FA R-CH2-CH2-CH2-CH2-CH2-CH2-CH2-CH2-CH2-CO –CoA 10 9 O2, NADH, Cytochrome b5 R-CH = CH-CH2-CH2-CH2-CH2-CH2-CH2-CH2-CO –CoA
10 9
FADS1 – desaturates polyunsaturated fatty acids – fatty acid 5-desaturase R-CH = CH -CH2-CH = CH2-CH2-CH2-CH2-CH2-CH2-CH2-CO –CoA 13 12 9 8 6 5 O2, NADH, Cytochrome b5 R-CH = CH-CH 2-CH = CH2-CH2-CH = CH-CH2-CH2-CH2-CO –CoA
6 5
FADS2 – desaturates polyunsaturated fatty acids – fatty acid 6-desaturase R-CH = CH-CH2-CH = CH-CH2-CH2-CH2-CH2-CH2-CH2-CH2-CO –CoA 10 9 7 6 O2, NADH, Cytochrome b5 R-CH = CH-CH2-CH = CH-CH2-CH = CH-CH2-CH2-CH2-CH2-CO –CoA 7 6 ESSENTIAL FATTY ACIDS
Polyunsaturated fatty acids required for normal body function and health Cannot be completely synthesized by humans (and animals) Do not have necessary desaturases Plants have necessary desaturases – enter the food chain from plant products Two separate classes – cannot be interconverted – both required in diet 6 CH3 – CH2 – CH2 – CH2 – CH2 – CH = CH - - COOH 1 2 3 4 5 6 Most abundant in humans – 90% of essential fatty acid in Western diet 3 CH3 – CH2 – CH = CH - - COOH
1 2 3 < 10% of essential fatty acid in Western diet – high in brain, retina

24
SUMMARY – FATTY ACID UTILIZATION AND OXIDATION 1. Fats are degraded in the small intestine to fatty acids and monoglycerides. Intestinal cell reconverts them to fatty acids, incorporates them into chylomicrons, and introduces them into the lymph where they enter the circulation at the vena cava. 2. Fatty acids are mobilized from adipose tissue in response to hormone sensitive lipase. Albumin carries them to the liver where they enter the mitochondrion via the carnitine shuttle system and are ultimately converted to acetyl CoA by beta oxidation. With a saturated even-chain fatty acid, each round of beta oxidation produces 1 FADH2 and 1 NADH. 3. A buildup of fatty acyl carnitines, representative of too big a fatty acid load in the mitochondrion, will cause an inhibition of pyruvate dehydrogenase, thereby preventing additional acetyl CoA synthesis from carbohydrate carbons. 4. The acetyl CoA produced can be converted to citrate for shuttling to the cytosol for use in fatty acid synthesis or it can be further oxidized in the Krebs Cycle to produce reduced electron carriers for fuel in oxidative phosphorylation. 5. Excess acetyl CoA can be converted by the liver to one of three ketone bodies, acetoacetate, beta hydroxybutyrate or acetone. Acetoacetate and beta hydroxybutyrate are made in the mitochondrion via HMG CoA. Acetoacetate is reduced by NADH to beta hydroxybutryrate. The ratio of the two compounds is determined by the redox state of the mitochondrion. Acetone is generated nonenzymatically from acetoacetate. 6. Circulating ketone bodies are excellent fuel sources for oxidative tissues other than the liver. Beta hydroxybutyrate is re-oxidized to acetoacetate. Acetoacetate is converted to acetoacetyl CoA using a CoA from succinyl CoA. The acetoacetyl CoA is then split into two molecules of acetyl CoA. 7. Excess ketones in the blood produce a condition called ketosis. If the excess is large enough, the protons carried into the blood with the ketones will overcome the bicarbonate buffering system of the blood causing a drop in blood pH. This condition is ketoacidosis and is often seen in uncontrolled Type I diabetes. The drop in blood pH is accompanied by a drop in serum bicarbonate and an increased rate of respiration in order to reduce the acid load by CO2 expulsion. 8. Defects in fatty acid oxidation can lead to lethargy, CNS malfunction, and hypoglycemic hypoketonemia, especially during conditions of stress. Death can result.

25
SUMMARY – FATTY ACID SYNTHESIS 1. Fatty acids are synthesized from acetyl CoA and malonyl CoA in the cytosol. 2. Acetyl CoA is not made in the cytosol de novo but from acetyl CoA made in the mitochondrion. It is converted there to citrate, and citrate is shuttled into the cytosol. Whether acetyl CoA is oxidized in the Krebs Cycle or shuttled to the cytosol as citrate depends on the ATP/ADP ratio in the mitochondrion. 3. In the cytosol, citrate is reconverted to acetyl CoA and OAA in an ATP-dependent process catalyzed by ATP citrate lyase. The OAA can be reduced by malic dehydrogenase to malate in an NADH dependent process and reoxidized to pyruvate plus CO2 by malic enzyme in a reaction that uses NADP as an oxidizing agent producing NADPH. This can then be used in fatty acid synthesis. 4. Malonyl CoA is made from acetyl CoA and bicarbonate in an ATP-dependent process catalyzed by acetyl CoA carboxylase. Biotin is required for the reaction. This enzyme interconverts between an inactive monomer and an active polymer. Polymerization is caused by a build-up of citrate in the cytosol. A build-up of fatty acids causes depolymerization of the enzyme. Enzyme activity is also regulated by AMP-kinase and PKA activity. The phosphorylated state is inactive. 5. Fatty acids are made by fatty acid synthase. In mammals, this enzyme is an antiparallel dimer with an active site on each end of the protein complex. The major product of the enzyme is palmitate, a C16 saturated fatty acid that is made from 1 acetyl CoA, 7 malonyl CoAs and 14 NADPH molecules. The NADPH is made either by malic enzyme or by enzymes in the pentose phosphate shunt. 6. During the synthesis, malonyl CoA loses a CO2. The loss of this CO2 drives the reaction forward. New 2 carbon units are introduced at the carboxyl end of the growing fatty acid chain. During synthesis, the growing chain shuttles between the ACP and CE active sites on the enzyme. The fatty acid is held onto the ACP via 4-phosphopatetheine arm attached to a serine residue on the enzyme. 7. Once the fatty acid is released from the enzyme, it can be further elongated in the microsomes by a malonyl-CoA dependent process. Double bonds can also be introduced in a cytochrome b5-dependent process to make a 5, 6, or 9, bond.

1
MOLECULAR ORIGINS OF SYMPTOMS ASSOCIATED WITH DIABETES
I. Diabetes mellitus (most common defect in regulation of carbohydrate metabolism)
A. Manifestations
1. Elevated blood glucose levels – water drawn from interstitial space to reduce osmotic imbalance caused by high blood glucose. Leads to:
2. Loss of glucose in urine with excessive urine and thirst
3. Fatigue, nausea, vomiting (acute onset)
4. Long-term uncontrolled disease leads to blindness, neuropathy, and vascular disease.
5. Accelerated release of and oxidation of fatty acids sometimes leading to ketoacidosis (generally Type 1).
6. Decreased insulin leads to increased glucagon which exacerbates
hyperglycemia (stimulates gluconeogenesis and subsequent body protein wasting) .
B. Type I diabetes
1. Insulin-dependent due to loss of insulin secreting b-cells of the pancreas or deficiency in one of the enzymes controlling insulin secretion.
a. Neonatal – enzyme deficiency.
b. Juvenile or sometimes adult onset- autoimmune in origin causing b-cell
destruction with a frequency of 1/200.
2. Hyperglycemia and other symptoms are due to inablility of muscle and adipose tissue to utilize blood glucose because of suppressed glucose transport. Short term acute metabolic problems and long term problems due to destruction of blood vessel endothelium

2
C. Type II diabetes
1. Used to be called adult onset- often associated with obesity. Now a large number of teenagers and young adults are presenting with this disease.
2. Insulin independent initially. In later stages can become insulin dependent-
insulin is made but is not biologically effective generally because of densitized insulin receptor system.
3. Insulin resistance causes additional insulin to be release (hyperinsulinemia)
which then activates IGF-1 receptors (lower affinity for these than insulin receptors but lowered affinity overcome by increased amount.). Promotes proliferation of smooth muscle cells in vascular wall aiding in build-up of occlusive deposits.
d. Incidence about 5/100 - Control with diet and drugs.
ORIGINS OF KETOACIDOSIS
II. Exaggerated starvation response of normal fatty acid metabolism in the liver
A. Increased glucagon, decreased insulin, and increased catecholamines cause massive liberation of fatty acids from extrahepatic tissues into blood (3-5 mM) via the hormone sensitive lipase (cAMP-dependent)
B. High glucagon and low insulin inhibit synthesis of malonyl CoA.
1. Fatty acid synthesis is shut down 2. Carnitine acyltransferase (cytosol) is fully activated allowing fatty acids to
enter mitochondrion.
C. High concentration of fatty acids in liver
1. Feedback inhibit synthesis of fatty acids from acetyl-CoA being produced 2. Saturate the carnitine system in the liver. 3. Fatty acyl CoA builds up in the mitochondrion and saturates the β-oxidation
enzymes. 4. NAD and FAD are largely converted to NADH and FADH2 as a result of
massive β-oxidation, thereby saturating the ETS and depleting the mitochondrion of NAD and FAD needed for the Krebs Cycle.

3
5. Krebs cycle slows since
a. capacity for β-oxidation exceeds that for Krebs Cycle operation, so there is competition for limiting substrates.
b. since concentrations of electron carriers needed for oxidative
decarboxylation reactions are decreased c. Oxaloacetate needed for citrate synthase rxn. is being converted back to
malate due to high NADH/NAD ratio.
6. Result is large overabundance of acetyl-CoA molecules which nature converts into ketone bodies and exports them into the blood.
7. Every ketone body molecule brings 1 proton and the equivalent of 2 acetates
into the blood.
8. Ketone levels are high enough to overcome the HCO3 buffer system leading to ketoacidosis. – Occurs generally in Type1 diabetics or in end stage Type 2 when patients tend to become insulin dependent. Half of juvenile Type 2 patients can also exhibit ketoacidosis (reason unknown).
ABNORMAL CARBOHYDRATE METABOLISM IN TYPE I DIABETES
III .Absence of insulin leads to surplus of glucagon
A. Increased hepatic gluconeogenesis and glycogenolysis causes increased blood glucose
1. Absence of insulin means decreased recruitment of GLUT4 receptors to
muscle and adipose cell membranes
2. Decreased glucose uptake from blood
3. Rise in serum blood glucose
4. Above 180 mg./dl, glucose spills into urine
B. Acute effects of significantly elevated blood glucose
1. Spilling of glucose in urine leads to excess urine volume and wasting of energy, fatigue and weight loss. Too much water lost to be recaptured.

4
2. High glucose in blood leads to osmotic inbalance that draws water into the circulatory system leading to tissue dehydration and frequent urination. Manifest in diabetics as uncontrolled thirst.
C. Long-term effects of elevated blood glucose
1. Continuous high presence of elevated blood glucose leads to non-enzymatic
glycosylation of amino groups of membrane proteins and other proteins in the blood (Amadori rearrangement)
2. HbA1c.
a. Non-enzymatically glycosylated by free glucose as above. b. Normally in blood at levels < 6% of total Hb
c. Each percentage pt. increase = 35 mg./dl. of glucose
d. In uncontrolled diabetics, levels can reach as high as 18%.
e. Indicator of success of long term regulation of blood sugar control. Not
good for day-to-day monitoring. Elevations are predictive of long-term vascular complications.
3. Continued glycosylation Crosslinked protein complexes on membrane
called AGEs (advanced glycation endproducts).

5
a. Lead to vascular endothelial malfunction by altering the surface of vascular endothelial cells.
b. Modifications and resulting impaired circulation lead to long term vascular
complications of diabetes: neuropathy, ulcers, amputation, retinopathy, heart disease, infection, etc.
c. Other theories include redox stress and resulting lipid and protein
peroxidation; hyperglycemic activation of PKC (PKC inhibitors in phase III trials); inhibition of G6PDH (oxidative injury).
Treatment regimens
I. Type I:
A. Insulin
1. Injections 2. pumps.
B. Insulin shock: too much insulin leads to hypoglycemia which can produce
serious CNS complications II. Type 2
A. Inhibitors of gluconeogenesis (metformin = glucophage) B. Sulfonylureas (increase insulin secretion) C. Thiazolidinediones (increases sensitivity to insulin) D. Drugs such as glucokinase activators which promote storage of sugar in the liver.
E. α-glucosidase inhibitors (interfere with carbohyd. digestion in gut. Leads to lower
blood sugars and diarrhea.)
F. Insulin - used to be for end stage disease. Now considered as first or second line therapy depending on the severity of the disease.

6
III. Type 1 and 2
A. Drugs, such as aminoguanidines (no longer in trials because it causes B6 deficiency) and others are currently being developed to reverse AGEs thereby preventing or slowing down long-term damage resulting from diabetes.
B. Diet and exercise. Control food intake. Exercise increases mitochondrial
metabolism and decreases fat storage. Believed now to fight against processes that lead to glucose intolerance which may be precipated by or depend on increased activity in anabolic fat pathways.
Related References:
1. Biemel, KM., et. al. (2001) Formation Pathways for Lysine-Arginine crosslinks Derived from Hexoses and Pentoses by Maillard Processes (AGE formation). J. Biol. Chem. 276, 23405-23412.
2. Reddy, V.P., and Beyaz, A. (2006). Inhibitors of the Maillard Reaction and AGE
Breakers as Therapeutics for Multiple Diseases. Drug Discovery Today 11, 646-654.