Embed Size (px)
Citation preview

POSTGRAD. MED. J. (I963), 39, 650
FATIGUE FRACTURES OF BOTHTIBIA AND FIBULA
RoY H. MAUDSLEY, F.R.C.S.Orthop&eedic Unit, Heatherwood Hospital, Ascot, Berks.
FATIGUE or stress fractures in the lower quarter ofthe fibula and of the tibia have been separatelyrecorded, but only in one case have they beenfound in the same leg (Murray, I957). Thefollowing two cases are therefore of some interest.
Case i.-E. G., a housewife and part-time domestic,aged 59, suddenly felt pain around the ankle whilewalking. Later the ankle became swollen but sheremained active for six weeks until she attended herdoctor, who referred her to Upton Hospital, Slough.On examination, the lower leg and ankle were
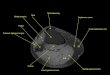
swollen, with maximal tenderness over the lower tibiaand fibula. Ankle movements were restricted slightlyand she walked with a limp. Radiographs were taken(see Fig. i).A walking plaster was applied for a month and fol-
lowed by a crepe bandage. Two months after her firstattendance she had no pain or limp and only a littleswelling at night. Four years later she had no symp-toms and radiographs revealed no trace of fracture.Case 2.-A. L., a housewife, aged 68, noticed the
onset of pain over the outer side of the right ankle, alsowhile walking. She regarded this as rheumatism butthree weeks later attended her doctor, who referred herto hospital. Radiographs revealed transverse fracturesabout two inches above the malleoli (see Fig. 2).A walking plaster was applied for six weeks. When
the plaster was removed there was no pain, but a littleswelling persisted in the ankle region together with aslight limp, and some increased valgus of the right footwas observed.
DiscussionFatigue fractures of the tibia or fibula are not
uncommon. Large series affecting the lowerquarter of the fibula have been recorded byBurrows (1948), Devas and Sweetnam (I956) andothers. In the lower tibia five cases were describedby Singer and Maudsley (I954) and nine inathletes by Devas (I958).These cases may be divided into (a) the young
and athletic and (b) the middle-aged and tired.The majority appear in the former group, as doesthe only previously recorded case of fatigue frac-tures in both tibia and fibula (Murray, I957). Thetwo cases described in this article are in the'middle-aged and tired' group. Neither of thesepatients attended until the symptoms had beenpresent for six weeks and then they were notsevere. It is possible that similar cases haveoccurred, but have not been radiographed nor
recognized. From the radiographs of these twopatients it will be seen that the callus in theantero-posterior view is fairly even, though in thelateral view it is wedge-shaped based posteriorly.This would suggest the stress fracture com-menced posteriorly, during dorsiflexion.
From the numerous descriptions of fatigue fracturesin many situations it is possible to describe severalstages through which a fracture may pass (see Fig. 3).
Stage i: The trabecular fracture in one cortex fol-lowed by callus formation but no visible fracture line.When the callus is adjacent to the periosteum, this islifted up.
Stage 2: The fracture is continued through onecortex and an infraction is seen.
Stage 3: The fracture extends to the opposite cortexand a triangular zone of callus formed.
Stage 4: The fracture being complete, the fragmentsmay become displaced.
In the event these stages are determined bywhether the activity is continued after the firstsigns of fracture occur, by the amount of activity,and by the rate of healing in the fracture zone.
If these stages are truly progressive, it wouldseem to follow that the site of maximum callus isthe site of first fracture. In the present cases andon review of the literature of cases in the lowerthird of the tibia the early callus appears pos-teriorly; this suggests that the bending strain isconvex posteriorly and that the repetition actionis dorsiflexion, or the forward thrust of the bodyweight through the knee.
Fatigue in metals is well understood and itmay be well to consider the common and differingfeatures. Any column of material when loadedvertically is subject to compression stress. If theload is off centre, as in walking, deflection willoccur due to bending, with compressive and tensilestrain on the inner or outer surfaces respectively.If this column is subjected to repeated loadingand relaxation there comes a time when thematerial reaches a point of fatigue. The numberof repetitive loadings to fatigue is very high inmetals, but less in bones, and for the human tibiahas been calculated by Evans (I957) to be about2,000,000 in the centre of the shaft, but diminish-ing towards each end of the bone. The fibular
copyright. on M
ay 12, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.39.457.650 on 1 N
ovember 1963. D
ownloaded from

MAUDSLEY: Fatigue Fractuires of Both Tibia and Fibiala
Fie.. i. Case I: Radiographs of transvers2 fatigue fracture of tibia and fibula with maximum callus posteriorly.
FIG. 2.- Case z: Radiographs showing considerable callus formation transversely in the tibia and fibula, maximalposteriorly.
Noveniber I963 651copyright.
on May 12, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.39.457.650 on 1 Novem
ber 1963. Dow
nloaded from

652 POSTGRADUATE MEDICAL JOURNAL November I963
ii-Rxx,IX,
--- .......
FIG. 3.-Stages in fatigue fracture of a bone.
specimen had a life of 3,000,000 cycles, all at5,ooo lb./sq. in. Evans has suggested that onereason for bone having a poorer fatigue life is itsporosity (Haversian canals, etc.) compared withmetals, and the increased porosity towards theends of the shaft of a long bone might well accountfor a reduced fatigue life. Whereas a metal may beconsidered homogeneous, bone may not, since ithas varying characteristics in stress at differentlevels and quadrants of the bone. Thus the stress-strain characteristics of the whole bone may notbe assumed from the determinations on a unitportion of bone. Nevertheless, bone has a built-inorganic capacity to repair that metal does notby virtue of osteoblastic action. Fatigue life istherefore likely to be reached only after excessiverepeated loadings within the time required forrepair, which may be prolonged in the case of themore elderly.
Individual trabecule may well be fractured atfirst and possibly lead to discomfort, which maydetermine rest and allow repair to occur. But ifthe activity be continued many trabeculk will befractured and lead to an infraction, though thismay not occur until callus has commenced inresponse to the first minute fractures. In this waythe well-known observation that callus is some-times seen either without or before a fracture linecan be explained. In a column such as bonethere is bending in response to loading and this isknown as elasticity. Devas and Sweetnam have
suggested that the bending of the fibula toward thetibia by resisted muscular effort may be respon-sible for fatigue fracture, but it would appearnormal for this to occur as part of the elasticity ofthe bone.
Burrows suggested that fatigue fractures occurin the section of fibula where it changes fromnarrow compact bone to wide cancellous bone,and this has also been noted in the tibia (Singerand Maudsley, I954). This level is a region ofincreasing porosity and marks the end of the shaftwhere fatigue life becomes reduced (Evans, I957).
TreatmentSince callus is often well advanced when the
patient is first seen, some restriction of activitywith immobilization to give comfort for a fewweeks is all that is required. Should an underlyingcause be suspected, a search for this should beundertaken, though in the vast majority of casesreported no positive findings have been made.
SummaryTwo cases of fatigue fractures of the lower ends
of both tibia and fibula of the middle-aged womenare described, and the mechanism of fatiguefractures is discussed.
I am grateful to Mr. W. Herschell for permission toquote the second case, to Miss Beckett for the drawingof Fig. 3, and to Miss D. Bannister for the radiographicprints.
REFERENCESBuRRows, H. J. (I948): Fatigue Fractures of the Fibula, 3'. Bone J7t Surg., 30B, 266.DEVAS, M. B. (1958): Stress Fractures of the Tibia in Athletes or 'Shin Soreness', Ibid., 40B, 227.
, and SWEETNAM, D. R. (1958): Runner's Fracture, Practitioner, I8o, 340.EvANs, F. GAYNOR (1957): 'Stress and Strain in Bone'. Springfield, Illinois: Charles C Thomas.MuRRAY, D. S. (I957): Fatigue Fractures of the Lower Tibia and Fibula in the Same Leg, J7. Bone Jt. Surg., 39B, 302.SINGER, M., and MAUDSLEY, R. H. (1954): Fatigue Fractures of the Lower Tibia, Ibid., 36B, 647.
copyright. on M
ay 12, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.39.457.650 on 1 N
ovember 1963. D
ownloaded from